Embed Size (px)
Citation preview

See discussions, stats, and author profiles for this publication at:
https://www.researchgate.net/publication/236777599
A Review of Three Controversial Educational
Practices: Perceptual Motor Programs, Sensory
Integration, and Tinted Le....
Article in Education and Treatment of Children · January 2009
DOI: 10.1353/etc.0.0054
CITATIONS
33
READS
1,783
3 authors, including:
Some of the authors of this publication are also working on these related projects:
Cognitive-Behavioral Approach for Children with Autism Spectrum Disorders View project
Oral Narrative in Children with Disability View project
Keith J. Hyatt
Western Washington University
9 PUBLICATIONS 110 CITATIONS
SEE PROFILE
Jennifer Stephenson
Macquarie University
108 PUBLICATIONS 969 CITATIONS
SEE PROFILE
All content following this page was uploaded by Jennifer Stephenson on 17 November 2014.
The user has requested enhancement of the downloaded file.
EDUCATION AND TREATMENT OF CHILDREN Vol. 32, No. 2, 2009
A Review of Three Controversial EducationalPractices: Perceptual Motor Programs, Sensory
Integration, and Tinted Lenses
Keith J. HyattWestern Washington University, Bellingham
Jennifer Stephenson and Mark CarterMacquarie University
Sydney, Australia
Abstract
Children with disabilities have frequently participated in various interventionsbefore the efficacy of those practices was scientifically validated. Whensubsequent scientific evidence failed to support particular practices, those thathad already made inroads into the educational arena frequently continuedto be used. Given the current emphasis on the use of empirically validatedinterventions, a review of research on the efficacy of educational interventionsis consistent with guidelines from the No Child Left Behind Act (2001) andthe Individuals with Disabilities Education Act (2004). The research findingsregarding three relatively common, yet controversial, practices failed tosupport the continued use of perceptual motor programs, sensory integrationtherapy, and tinted lenses. Educators are encouraged to become informedconsumers of research and implement evidence-based practices.
In recent years, journal articles and entire books have been writtento alert educators, parents, physicians, psychologists, and other
professionals of the inherent problems associated with the useof nonvalidated practices in the treatment of individuals withdisabilities (e.g., Jacobson, Foxx & Mulick, 2005; Lilienfeld, Lynn,& Lohr, 2003; Rooney 1991; Sieben, 1977; Silver, 1995; Stephenson,2004). in spite of efforts of those in the field to ensure that scientificallyvalidated interventions are the treatments of choice, nonvalidatedapproaches continue to hold a considerable amount of influence onthe perceptions of many professionals and the public. The AmericanAcademy of Pediatrics (1999) recommended training new physiciansabout discredited practices, such as the Doman-Delacato patterningtreatment, to avoid repeating mistakes of the past. This is an importantrecommendation that is just as relevant for educators as it is forphysicians.
Correspondence to Keith j . Hyatt, EdD, Chair, Department of Special Education,Western Washington University, Miller Hall 318a, Bellingham, WA 98225-9040; e-mail:ktMth.hyatt#w wu.edu.
Pages 313-342
314 HYATT, STEPHENSON and CARTER
While the use of a nonvalidated approach may not pose an im-minent threat to the safety of individuals, it could deprive people ofexposure to effective interventions, waste valuable time, and providefalse hopes that may lead to feelings of discouragement after the ap-proach fails to produce the desired outcome. An internet search on thepractices discussed in this paper would lead the reader to many sitescontaining persuasive advertisements and testimonials claiming theeffectiveness of the treatments without citing support from empiri-cal research reported in peer-reviewed papers. To this end, it is im-perative that professionals become informed consumers of researchto ensure that those seeking assistance are provided with treatmentsor interventions that will most likely result in improved learning andan increased quality of life.
The purposes of this paper are twofold. Eirst, the review willconsolidate available research evidence and inform professionals ofthe lack of scientific substantiation for the continued use of three con-troversial practices: perceptual motor programs (PMPs), sensory in-tegration, and tinted lenses. Second, parallels will be drawn betweenthese three approaches with the intent of assisting consumers of re-search to understand why they continue to be employed and how toidentify potentially ineffective practices. The three practices discussedin this review have been selected among the many unsupported orcontroversial practices because there is a long history of their use withstudents with disabilities and learning difficulties (Kavale & Mostert,2004; Whitely & Smith, 2001). It is our intention to draw to the atten-tion of practitioners the nature of the evidence available on the effi-cacy of these practices. To achieve this goal, definitions of each prac-tice, a description of the procedures along with a rationale for thoseprocedures and relevant research findings will be presented for eachpractice. Where systematic meta-analyses have been conducted (i.e.,PMPs and sensory integration), key reviews will be synthesized andrecent studies will be considered where relevant. Unlike PMPs andsensory integration, tinted lenses have not been subject to systematicmeta-analysis so primary sources of research will be examined. Final-ly, some common characteristics of these approaches will be discussedalong with an exploration of reasons they continue to be employed.
Perceptual Motor Programs
Definition
Perceptual motor skills are those that require the integration ofsensory input (visual, auditory, and kinesthetic) with fine or grossmotor responses. Perceptual Motor Programs (PMPs) for students

A REVIEW OF THREE CONTROVERSIAL PRACTICES 315
who have difficulty learning are based on the notion that neurologicalproblems causing particular processing deficits related to the integra-tion of perceptual and motor skills interfere with academic learning(Blythe, 2000; Dore, 2006). Despite professional concerns regardingthe existence of processing deficits, interventions for learning diffi-culties that purport to remediate these underlying process deficitsremain popular. Perceptual-motor training has been the most preva-lent type of process training and remains alive and well (Kavale &Forness, 2000). Many older PMPs such as the Doman-Delacato pat-terning program continue to be advertised, although they have beendiscredited (American Academy of Pediatrics, 1999; Jacobson, Mulick,& Foxx, 2005), and many newer programs such as the Dore/DDAT,Primary Movement Program and Brain Gym® have emerged with arange of theorefical underpinnings.
Description of Practice for Perceptual Motor Programs
Currently widely advertised programs such as the Dore Achieve-ment Center's individualized Dyslexia, Dyspraxia and AttentionTreatment (DDAT) are based on the claim that the difficuUies lie inthe cerebellum (Dore, 2006). Treatment consists of exercise programsthat are claimed to improve the ability of the cerebellum to processinformation. It is purported that children with dyslexia have a coredifficulty with skill automizafion, which impacts language and read-ing. This difficulty has been called Cerebellar Developmental Delay(DDAT, 2006a) by the Dore centers, a label that is not used by anyother group. Dore centers claim that their individually designed exer-cise programs improve cerebral functioning thereby overcoming au-tomization deficits and subsequently improving academic and socialskills (DDAT, 2006b; Fawcett, Nicolson, & Maclagan, 2001; Reynolds,Nicolson, & Hambly, 2003)
Other current perceptual-motor theories ascribe difficulfies inlearning to the persistence of primitive refiexes which then impedenormal development and the ability to learn skills such as readingand writing (Goddard-Blythe, 2000; Insfitute for Neuro-PhysiologicalPsychology, n.d.; Jordan-Black, 2005; McPhillips, Hepper & Mulhem,2000). These theories underlie the Primary Movement program devel-oped by McPhillips and programs promoted by the Insfitute for Neu-ro-PhysioIogical Psychology (INPP). Programs such as Brain Gym®,which are promoted as improving learning, sport and self manage-ment skills in anyone (Brain Gym®, 2006a), rely on much more gen-eral and simplistic notions of improving brain funcfion. Brain Gym®promotes exercises claimed to facilitate the integration of the frontand back parts of the brain, the right and left hemispheres, and the top

316 - HYATT, STEPHENSON and CARTER
and bottom parts of the brain to improve a wide array of unrelated be-haviors such as reading, surfing, golf, and sales. (Brain Gym®, 2006b;Hyatt, 2007). In essence, PMPs imply that relatively simple exercisescan fundamentally change the neural structure of the brain and facili-tate learning.
PMP programs prescribe particular motor activities and exer-cises. Some, such as in the Dore/DDAT program maybe individuallyprescribed and adjusted (Reynolds et al., 2003), while others may begeneric (Brain Gym®, 2006b). They often include activities, such asthrowing and catching, purported to improve balance, gross and finemotor skills, and academic achievement. The exercises may involvedoing two things at once; for example, one exercise in the Dore/DDATprogram involves sitting and bouncing on a large air filled ball whiletossing a bean bag from hand to hand (DDAT, 2006a).
The persistence of primitive reflexes is another rationale givenfor programs that prescribe exercises that mimic the activities of fetus-es and infants such as crawling and stretching or movements based onthose reflexes (Goddard-Blythe, 2005; Jordan-Black, 2005; McPhillipset al., 2000). The claim is made that movements that follow the patternof the reflexes will work to inhibit those reflexes and somehow im-prove the ability to acquire reading and other academic skills (McPhil-lips et al.).
Research Findings for Perceptual Motor Programs
Kavaîe and Mattson (1983) completed a meta-analysis of 180studies of PMPs and found a very small overall effect size of .08. Ef-fect sizes were reported for outcome measures (reading, intelligence,general achievement as well as perceptual and motor skills), specifictraining programs, different groups of children, and different gradelevels and no important positive effects were found. Indeed the effectsize for perceptual-motor outcomes was only 0.17 which is also verysmall and suggests that the programs examined had little impact evenon perceptual-motor skills themselves. The Board of the Trustees ofthe Council for Learning Disabilities (Council for Learning Disabili-ties, 1987) issued a strong statement in 1986 against the use of per-ceptual motor testing and training to improve academic performance,perceptual, and perceptual-motor functions in students with learningdisabilities. They based this recommendation on the lack of scientificevidence supporting such practices.
Hyatt (2007) reviewed the research on Brain Gym® and foundthat the limited peer-reviewed research available failed to supportclaims that Brain Gym® resulted in improvements in academiclearning. There are two reported studies of the DDAT exercise-based
A REVIEW OF THREE CONTROVERSIAL PRACTICES 317
approach (Reynolds et al, 2003; Reynolds & Nicolson, 2007) but theflawed research design and difficulties with the analysis and inter-pretation of results make the evidence supporting the efficacy of theapproach unconvincing (Alexander & Slinger-Constant, 2004; Rack,Snowling, Hulme & Gibbs, 2007; SnowUng & Hulme, 2003). Summa-ries of several small, in-house studies in schools in the UK and Ger-many on the effects of a program designed by the INPP to reducethe persistence of primitive and postural reflexes and to improveacademic performance, particularly reading, were presented by God-dard-Blythe (2005). None of these studies showed that the programhad important effects on reading, and in most sites there was no effecton reading.
There are two research studies (Jordan-Black, 2005; McPhilUpset al, 2000) that reported positive effects on reading and math but notspelling after the use of the Primary Movement Programme devel-oped by McPhillips, but there are limitations to these studies and theresults need to be replicated by other researchers prior to acceptance.The assessment of the persistence of primitive reflexes was carriedout using observation and scoring on a four point scale of the move-ment of the arms in response to having the head turned (Schildertest). Neither McPhillips et al nor Jordan-Black provide informationon the origins, reliability, or validity for this test nor did they carryout inter-observer agreement measures in their studies which wouldestablish that the same actions would be scored the same way by twoindependent observers. Both reports also note that the reduction inthe reflexes is claimed only to increase "readiness" to learn and theprogram is not a substitute for instruction. Given the lack of impactof older PMPs on reading and that the exhaustive review of the cor-relates of reading carried out by Hammill (2004) found only small cor-relations between reading and perceptual-motor skills, it is hard tobe optimistic that these newer programs will be any more successfulthan the older programs.
Sensory Integration
Definition ^
Sensory integration arose from the work of Ayres (see Ayres,1972) and was popularized in the 197O's. It has been applied to a vari-ety of groups including those with learning difficulties (Hoehn & Bau-meister, 1994), cerebral palsy (Chu, 1989), intellectual disability (Ar-endt, MacLean, & Baumeister, 1988a) and autism (Dawson & Watling,2000). Much ofthe early research addressed children with learning dis-abilities, with the expectation that underlying academic performance

318 HYATT, STEPHENSON and CARTER
would improve with sensory integrative therapy (Vargas & Camilli,1999). More recent research has often focused on addressing unusualresponses to sensory input, particularly in children with autism spec-trum disorders (see Baranek, 2002; Dawson & Watling, 2000). A fun-damental assumption underlying sensory integration is that learningand other problems arise, at least in part, from difficulties in the neu-rological processing of vestibular, tactile and proprioceptive sensoryinformation (Arendt et al., 1988a; Ayres, 1972; Bundy & Murray 2002;Hoehn & Baumeister, 1994). Higher-level functions, such as those in-volved in traditional academic skills, are assumed to be dependent onlower-level processing of sensory information (Hoehn & Baumeister,1994). The basic premise that higher cognitive and functional skills aredependent on more fundamental abilities is common among percep-tual motor programs. Sensory integration, however, is distinguishedby the apparent complexity of its underlying neurophysiological the-ory and thus it warrants separate consideration.
Description of Practice for Sensory Integration
Sensory integrative therapy is usually conducted by occupationaltherapists and treatment is costly, with intervention sometimes lastingmore than a year (Vargas & Camilli, 1999). In a review of sensory inte-gration research, Vargas and Camilli reported that intervention aver-aged 60 hours (range 13-180), involving between two and five sessionsper week, each of 25-45 min duration. Interventions involve a range ofactivities that typically include the combination of controlled sensorystimulation and "purposeful" motor activity (Ayres, 1972; Bundy &Murray, 2002; Hoehn & Baumeister, 1994). Therapy may involve theuse of equipment such as hammocks and scooter boards to providevestibular stimulation, use of weighted vests, manual compression ofjoints, as well as brushing and rubbing of the body with materials ofvarious textures (see Ayres, 1972; Hoehn & Baumeister, 1994; Smith,Mruzek, & Mozingo, 2005). A related intervention involves the use of"sensory diets", including activities and environmental adjustments,which are presumed to match the individual's sensory needs (Smithet al., 2005). For example, if a child is over-aroused, calming vestibu-lar activities such as rocking or riding a bike might be advised (Yee,2007).
Research Findings for Sensory Integration
The ongoing interest in sensory integration has resulted in re-views of its efficacy in several areas and key reviews will now besynthesized. In examining the application of sensory integration toindividuals with intellectual disability, Arendt et al. (1988a) described

A REVIEW OE THREE CONTROVERSIAL PRACTICES 319
a small and deeply flawed body of research that provided no empiri-cal support for the continued use of the procedure in clinical contexts.Hoehn and Baumeister (1994) found similar results in their review ofresearch on sensory integration with individuals with learning dis-abilities. Following analysis of seven outcome studies published after1982, they concluded that the "current fund of research findings maywell be sufficient to declare SI therapy as not merely unproven, but ademonstrably ineffective, primary or adjuncfive remedial treatmentfor learning disabilities and other disorders" (p. 348).
Sensory issues affecting individuals with autism have been ofinterest in recent years and sensory integration has been suggestedas a possible strategy to address these problems (Dawson & Watling,2000). Dawson and Watling located four relevant studies in their re-view and concluded that "these were of such small scale that no firmconclusions regarding efficacy could be made" (p. 415), although eventhis interpretation may have been overly generous (see Goldstein,2000). In a later review, Baranek (2002) examined only three studies,identifying important weaknesses in each that made it difficult to as-cribe any observed changes to sensory integration per se. Baranek'srecommendation supporting the cautious use of sensory integrativetherapy seems unjustifiable given the number of studies examined,acknowledged flaws, and inconsistent treatment effects. Substantialintegrative reviews of intervention options in autism (Lord & McGee,2001; New York State Department of Health, 1999; Perry & Condillac,2003; Roberts, 2004) have consistently concluded that there is no cred-ible empirical base to support the application of sensory integrativetherapy. Even those recommending the use of sensory integration inautism (e.g., Baranek, 2002) or suggesting it may have promise (e.g.,Heflin & Simpson, 1998) concede that there is currently no valid em-pirical evidence base for the technique.
In addition to descriptive reviews of sensory integration in spe-cific areas, quantitative meta-analytic syntheses have been conducted.Ottenbacher (1982) provided a meta-analysis of the small body ofearly research on sensory integration, examining eight studies pub-lished prior to 1982. These initial findings were encouraging with anoverall effect size of .79. Unfortunately, this very early promise hasbeen comprehensively disconfirmed in later and larger analyses. Var-gas and Ciamilli (1999) provided a meta-analysis of 23 studies com-paring sensory integration to no treatment controls or other interven-tions. When compared with no treatment, the mean effect size was.29. While this was statistically significant, it fell short of the third ofa standard deviation difference that is typically used as the thresh-old for educational significance. Vargas and Camilli confirmed the

320 HYATT, STEPHENSON and CARTER
results of the earlier Ottenbacher meta-analysis but found that effectsizes fell to .03 in post-1982 studies. When compared with alternafivetreatments, the overall effect size was .09, which was not stafisticallysignificant from zero. A similar pattern of results was presented byShaw (2002) in summarizing a meta-analysis of 41 sensory integrationstudies employing random assignment. Effect sizes for improvementin language (-.08), behavior (.02) and sensory motor funcfions (-.10)were not stafistically significant. Small but significant effects werefound for motor skills (.24) and psychoeducational performance (.26)but these dropped to near zero for studies that controlled for matura-tion. Sensory integration is an expensive intervenfion and availablereview data overwhelmingly suggests it is manifestly ineffective.
Sensory integration has sometimes been defended by reversingthe conventional scientific burden of proof. Conventionally, the onusof proof rests with those proposing an intervention to demonstratethat it does work. In the case of sensory integrafion, it is sometimes ar-gued that critics have failed to demonstrate that it does not work (e.g.,Ottenbacher, 1988). The end point of this line of reasoning is demon-strated by Miller (2003) with an argument that amounts to the justifi-cation of continued clinical use of sensory integrative therapy on thebasis of a perceived lack of interpretable scientific evidence. Indeed,Shaw's (2002) suggesfion that sensory integration exhibits many corefeatures of pseudoscience should not be dismissed lightly.
Despite a consistent lack of supporting evidence, sensory inte-gration has been highly enduring (Smith et al., 2005). For example.Green et al. (2006) reported a survey of over 500 parents of childrenwith autism in which sensory integration was reported as the thirdmost commonly implemented treatment, ahead of interventions withsolid empirical support such as applied behavior analysis. It is pos-sible that this resilience may be a product of incorrect percepfions ofparents and educators that sensory integrative therapy may be havingan effect. Mason and Iwata (1990) have clearly demonstrated experi-mentally that apparent effects of sensory integrative therapy may beartifacts and unrelated to the therapy itself. Part of the basis for thisresilience may also relate to the view that research on sensory integra-tion is in its infancy (Miller, 2003) and that research will eventuallycatch-up with professional beliefs (Schaaf & Miller, 2005; Smith et al.,2005). This would seem increasingly unlikely noting that sensory in-tegration theory and research now dates back around 40 years. To putthis in context, sensory integration emerged as a field of research ataround the same time as applied behavior analysis. Even if the con-tentious argument that sensory integrafion is unproven rather thandisproved is accepted, the question arises as to whether the publicshould continue to be exposed to an unproven intervention?

A REVIEW OF THREE CONTROVERSIAL PRACTICES 321
Tinted Lenses and Overlays
Definition
Irlen (1991) reported that during the 1980s she had chanced uponan amazing discovery when working with adults with reading prob-lems, the identification of a previously unknown visual-perceptualproblem that interfered with a person's ability to process full spectrumlight. She coined the condition Scotopic Sensitivity Syndrome (SSS),which is also known as Irlen Syndrome (The irlen Institute, n.d.) andMeares-Irlen Syndrome (The Institute of Optometry, n.d.). Some of thepostulated symptoms of SSS included text appearing blurred, spacedas if a river were running down the page, and letters appearing toswirl or shake. Irlen theorized that SSS was the reason many peopleexperienced difficulty in a wide range of important life activities thatincluded reading, attitude, motivation, self-esteem, depth percepHon,sports, movement, coordination, music, math, handwriting, and writ-ing composition, and claimed that the perceptual difficulties of indi-viduals with SSS could be ameliorated with the use of colored overlaysor tinted lenses. Unlike the reviews of PMP and sensory integration,the following discussion is based on primary sources, because therewere no meta-analyses identified in a search of the ERIC, PsychlNFO,and MEDLINE databases between 1990 and 2006.
Description of Practice for Tinted Lenses and Overlays
The use of tinted lenses and overlays has been promoted by twoagencies, the Irlen Institute for Perceptual and Learning Developmentin the United States and The Institute of Optometry in the UnitedKingdom. It is unclear how widespread the use of tinted lenses is;however, the Irlen International Newsletter (New Screeners, 2006)listed the following number of new screeners in various countries:United States, 402; England, 93; Canada, 30; Australia, 24; South Ko-rea, 17; Austria, 8; New Zealand, 5; Hong Kong, 2; Jordan, 2, Slovenia,1, Switzerland, 1, Slovenia, 1. The estimated the number of screen-ers is approximately 7000 worldwide with over 100.000 people usingIrlen lenses (Othmer, 2006).
Both organizations claim that colored overlays are effectivetreatments for visual-perceptual problems and SSS. They also assertthat the colored overlays must be specifically manufactured and notethat colored overlays purchased from office supply stores would notsuffice; however, they provide no research support for this contention(The Institute of Optometry, n.d.; The Irlen Institute, n.d.).
The two session assessment conducted by Irlen examiners is onlybriefly described in Irlen materials. In the first session, an interview
322 HYATT, STEPHENSON and CARTER
is conducted, visual-perceptual tasks are administered, and for thosedeemed to have SSS, colored overlays are provided. The individualis told to use the overlays and return for a Tinting Assessment if theuse of colored overlays significantly improved reading. The assess-ment conducted by The Institute of Optometry is similar and mayinclude an eye examination, an interview, and a Colorimetry assess-ment if necessary. The Colorimetry assessment is conducted with anIntuitive Colorimeter, a device developed to prescribe colored over-lays and lenses. However, identification of colored overlays in thestudies reviewed was frequently done through a subjective processof elimination where subjects were shown various tints and asked toselect the best. Kriss and Evans (2005) noted difficulties with objectiveassessment of Irlen syndrome and stated that diagnosis is typicallybased upon whether the individual reported immediate improvementor voluntarily used the overlays for a sustained period of time. Whileindividual reporting may reflect actual change for the person, reli-ance on subjective reporting could be misleading, because an indi-vidual may provide a report to please the investigator, the positivereport may be a result of the placebo effect, or it could represent actualchange. It would be important to clarify this issue in future researchusing controlled measures.
Research Findings for Tinted Lenses and Overlays
Before reviewing research studies that investigated the use ofcolored lenses, a few background issues must be addressed. First, sev-eral researchers have noted the absence of objective scientific evidencethat Scotopic Sensitivity Syndrome actually exists (Blaskey et al, 1990;Rooney, 1991; Royal College of Ophthalmologists, 2002; Silver, 1995;Stone & Harris, 1991; Woerz & Maples, 1997). Second, Irlen and TheInstitute of Optometry claimed that the symptoms of SSS are not de-tectable by standard vision examinations; however. Solan (1990) andWilliams, Kitchener, Press, Scheiman, and Steele (2004) noted that theidentified symptoms of SSS are related to identifiable vision anoma-lies. Furthermore, while vision problems must be corrected so thatchildren can see the printed word, the contention that neurologicallybased visual-perceptual problems are one cause of learning disabili-ties has not been substantiated (American Academy of Pediatrics,1998; Helveston, 1987; Metzger & Werner, 1984). When consideringthat SSS is supposedly related to the visual sy.stem, it is of interestto note that the majority of studies reviewed did not require a visionexamination as part of the study. If addressed, most noted that thesubjects had received an exam in the past. For example, Kriss and Ev-ans (2005) stressed the importance of vision examinations, but still
A REVIEW OF THREE CONTROVERSIAL PRACTICES 323
failed to conduct vision exams prior to conducting their study. Finally,while both the Irlen institute and the Institute of Optometry claim tohave unique procedures for diagnosing and manufacturing the ap-propriate tint, no research was located comparing the effectivenessof the different assessment procedures or tints prescribed by eitherorganization.
In addition to the disagreement regarding the existence of SSSas a unique perceptual disorder, there is a lack of documentation sup-porting the consistency in which individuals select overlays (Fletcher& Martinez, 1994). Woerz and Maples (1997) conducted a study with41 high school students to determine the consistency of student selec-tion of tinted overlays. In a visual activity in which 24 differently col-ored overlays were used, students self-selected the overlay that madethe task easier to complete. Two weeks later, the students were againasked to select a preferred overlay, and only fourteen students (34%)selected the same color. When comparing the performance of the 19students identified as SSS symptomatic, the results were even worsewith only 5 (26%) of 19 choosing the same color on retest. Anotherstudy conducted by Wilkins, Lewis, Smith, Rowland, and Tweedie(2001) examined the consistency of color selection of 87 students ingrades four through six in one school. They reported that 47% selectedthe same color on the second assessment. Unlike Woerz and Maples,they did not report data on SSS symptomatic students separately.
In spite of the absence of scientific evidence supporting the ex-istence of SSS or the consistency of colored overlay selection proce-dures, a considerable number of studies were conducted to evaluatethe efficacy of colored overlays. In 1990, the Journal of Learning Dis-abilities published a special issue that provided intensive coverage ofIrlen lenses. In the preface to the issue, the editor in chief. Wiederholt,noted that each of the studies had serious theoretical, medical/physi-cal, and methodological ñaws, but were published along with articlescritiquing the studies to provide readers with an overview of the Irlenprocedures as well as guidance for conducting quality research stud-ies. He, along with Hoyt (1990), Parker (1990), and Solan (1990), notedthat these initial studies by Blaskey et al. (1990), O'Connor, Sofo, Ken-dall, and Olsen (1990), and Robinson and Conway (1990) failed to sup-port the treatment validity of colored overlays.
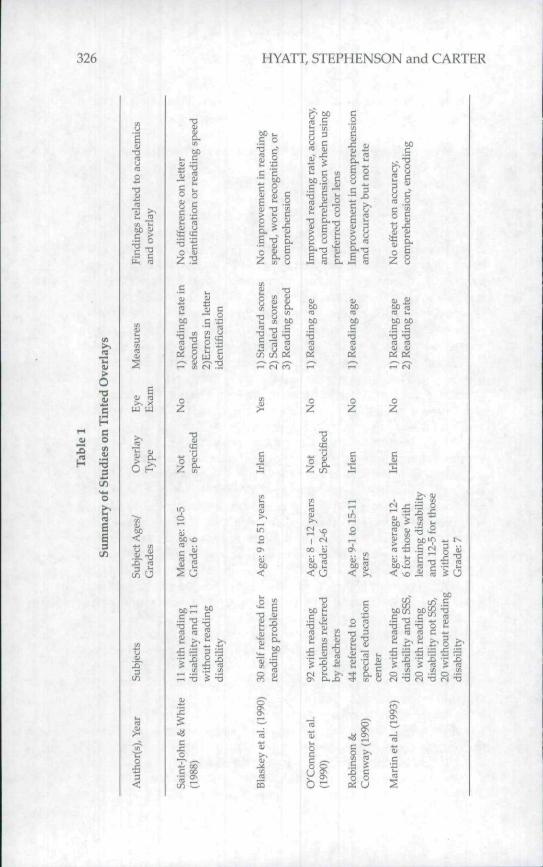
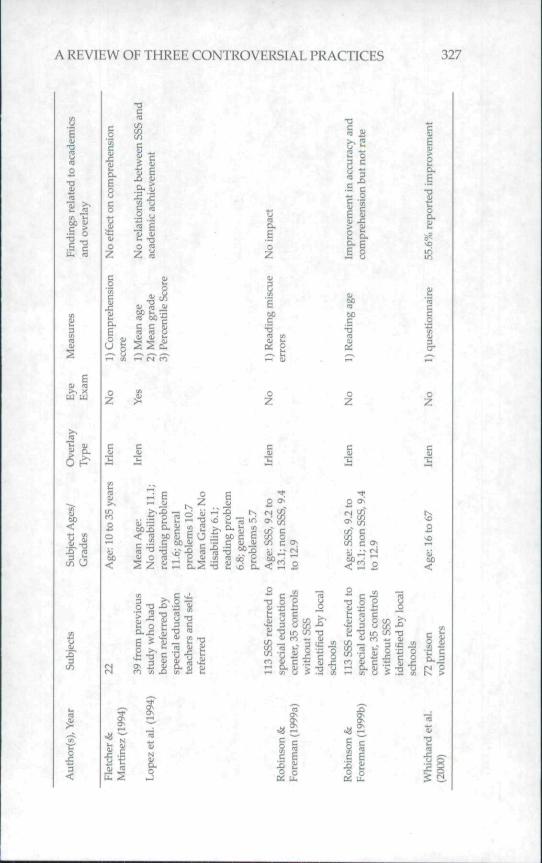
A brief description of representative studies conducted on bothIrlen and Intuitive overlays is contained in Table 1. The considerablevariability in the findings may be a result of methodological flawssimilar to those identified by Parker (1990). Some of the inadequaciesincluded: subjective and anecdotal reporting, failure to control for pla-cebo effect, lack of control groups, failure to determine equivalence of
324 HYATT, STEPHENSON and CARTER
!groups at pre-test phase, use of multiple treatments with one group,application of multiple statistical analyses without correction for falsepositives, failure to control for external threats to validity, possible ex-perimenter bias, and use of inappropriate measurement metrics, suchas reading age-equivalent scores. Given these concerns with the re-search designs, it should not be surprising that there is considerablevariability in findings reported in Table 1.
Some key issues arising from the research on Irlen overlays willbe discussed followed by a review of research on Intuitive overlays.None of the studies included a control group who met the criteria forSSS. In fact, Robinson and Conway (1990) stated, "A control groupwas not included, due to the ethical concerns of denying treatmentfor 1 year" (p. 590). Hoyt (1990) expressed concern that this statementimplied that the researchers were convinced of the validity of Irlenlenses as a treatment approach prior to conducting the study, whichraised a fundan^ental concern related to researcher bias. Despite thisconcern, future studies by Robinson and Foreman (1999a, 1999b) alsoincluded the same justification for exclusion of a control group withSSS symptoms. In addition to problems inherent with lack of control,Robinson and Eoreman (1999a, 1999b) subjected two of three experi-mental groups to more than one treatment, so any findings for thosegroups could not be attributed to a single experimental condition.They also failed to control for internal and external threats to validitysuch as subject maturation or changes in schooling conditions.
Several studies also used inappropriate measurement metricsand statistical analyses. Reading age was used as a measure of per-formance in several studies (Christenson, Griffin, & Taylor, 2001; Mar-tin, Mackenzie, Lovegrove, & McNicol, 1993; O'Connor et al., 1990;Robinson & Conway, 1990; Robinson & Eoreman, 1999b, Saint-John &White, 1988). Salvia, Ysseldyke, and Bolt (2007) provided strong cau-tions regarding the use of developmental equivalents, such as readingage, noting that the ordinal nature of these measures precludes theiruse in most statistical computations. Other researchers also used non-standard measurements in their studies. Eor example, Lopez, Yolton,Kohl, Smith, and Saxerud (1994) conducted statistical analyses usingpercentile rankings, which were inappropriate for the statistical anal-yses conducted. Due to the nature of ordinal scores, the findings inthese studies must be viewed with extreme caution.
In an additional study on Irlen overlays, Whichard, Eeller, andKastner (2000) evaluated the effectiveness of Irlen overlays on 72 pris-on inmates. Based on subjective reports from the volunteers, they de-termined that the lenses were effecHve as 40 of the subjects reportedconsiderable improvement in reading. However, this report cannot be

A REVIEW OF THREE CONTROVERSIAL PRACTICES 325
accepted with any level of confidence as there was no control groupand no objective measure of reading skill before or after selection ofcolored overlays.
Several studies listed in Table 1 were conducted to evaluate theeffectiveness of the Intuitive colored overlays. As with the studies onIrlen overlays, the research studies on Intuitive overlays did not in-clude control groups, did not ensure group equivalence prior to inter-ventions, and included the use of questionable statistical procedures.For example, Bouldoukian, Wilkins, and Evans (2002) noted that someof the subjects had been using overlays for several weeks prior to par-ticipating in that study and approximately one-third had been per-forming eye exercises prior to the study. So group equivalence couldnot be assumed. In addition, Wilkins et al. (2001) in the third studyreported in that article stated "To save time on testing, only childrenwho chose an overlay were tested" (p. 55), thus, there was no compar-ison group. The statistical analyses were also of concern and includedthe use of multiple t-tests without controlling for Type I error and theuse of one-tailed t-tests (Scott et al., 2002; Wilkins et al, 2001). Bothof these procedures increase the chance of finding a significant dif-ference where one did not exist, thereby, limiting the confidence thatcould be afforded to these findings.
In contrast to studies using Irlen lenses, the studies involvingIntuifive overlays tended to demonstrate an increase in reading speedas measured by the Rate of Reading Test (RRT). Wilkins, Jeanes, Pum-frey, and Laskier (1996) described the RRT, developed by Wilkins, as atest that minimized the linguistic aspects of reading by using only 15common words and maximized visual difficulties due to spacing, fonttype, and font size. They stated that multiple equivalent forms wereavailable but provided no evidence of alternate form reliability.
A reliability study of the RRT described by Wilkins et al. (1996)was conducted with 77 students who ranged in age from 8-8 to 11-9 and were in the fourth, fifth, or sixth grade. No other informafionregarding the sample was provided. While they did find an accept-able correlafion, the study was not conducted in the same manner forall students, which brings into question the level of reliability theyreported. Due to the varied nature of the assessment, the small experi-mental group, nonexistent alternate forms reliability measurement,and limited demographic data, one cannot accept the reliability of theRRT as presented. In addition to questions about the reliability, thereremain quesHons regarding the concurrent and predicfive validity ofthe RRT; perhaps most pressing is whether performance on the RRTis related to actual reading tasks and school performance. The RRTmay in fact be an acceptable measure of reading speed, and future
326 HYATT, STEPHENSON and CARTER
1 «
O
vuO
ss
o
Ö0<
.S
a; ESo
S -n •—
"re § ïï
1R
ead
M)
[ing
Rea
d
2 en
i
b o C>C
IIra ta
year
s
(M
00
Age
:in
g
<u
5r-i
•at;lid
o
O'C
ȣ)es
m
Gra
d
QJ)H ^lA Ge _£
"s Í
15-1
1
o,_cr
Age
:
o
J QJ- L .
- u,
inso
nR
obye
ars
cosnu3
T3
^ fe
[ X EUi/i O
S~O^
re
Con
(Ñai00rev.<
>
Age
:w
ith
3!o
6 fo
r
tri
M"
3;
al.
tin e
t
re
S
C
bill
re
'•B
sabi
lit D
•S
lea
m
re
and
1
en"
oc£^
bili
ra
'•B
^^
with
c
c"re
• o
/§S
(M
Gra
dbi
li
S
A REVIEW OF THREE CONTROVERSIAL PRACTICES 327
• f 2
JS sO 0)
C C
"O vcí ' S f̂ id "ö "Ç
O' o^
tn o _If) G O)
T3 o& "13
B Oj Cu S 's;
1 acc
ura
but
noi
b cc -21 SË wS 'S
s &.û. ËË p
impr
ovpo
rted
S?i n
Da
t/î qtn c
ç .-t;
SSS
o
wit
h
u_oj:i
xs
fie
•r
iden
o
scho
TS
113Í
o-Vm
duc
a>f^
Spec
"p,pcooinm
§
SSS
ao
wit
h
Xo
T3
fie
• r
iden
O
scho
[^
oVi
a,Pi
U1Ut
1)ai
C
O

328 HYATT, STEPHENSON and CARTER
OO)
•a2
en
¥ a.
00 ïï
~ 'a2 Si
er o
I I
o ^ —.
ooo<
S ¿^¿-2
il^ (fi
-c EC
00<
c 2P
pr CL.
00<
L.
a!
ipto
m
Ü
o
c
stud
e
mm
in5 j
CO
c
stud
e
UUlOJ
cO
I >, .s •;, -§o
> B > B o S
— 4-. a
J2 -5
e o ä
c 3 3
gr rea
T Í.OJ• ^ in
S ^ OJ
0
2
<uX
B
c2
ac
;S
>•a
tui
c
>
'is
to m ; ^
>•a
tui
c
._ s*'
' ^ -C 1
>•X!
2
Q. .^in 5
Û-TJ C
?i T3
¿ 3 ï

A REVIEW OF THREE CONTROVERSIAL PRACTICES 329
comparative research could confirm or disaffirm its use as a readingassessment instrument.
Northway (2003) identified changes in reading rate on the RRTthat were accompanied by large standard errors of measurement. Inthis study, subjects v̂ 'ho did not choose an overlay actually demon-strated a decrease in rate of -2.4 words per minute ± 4, those whochose an overlay but didn't use it also demonstrated a decrease of-4.4 ± 9, and those who reported frequent use of the overlays dem-onstrated an increase of 10.2 ±. 13. In all cases, the standard error ofmeasure was greater than the change in performance. It is possiblethat the large standard error of measure could be related to the use ofgain scores which are not recommended for analyses due to unknownreliability of gain scores (Thorndike & Dinnel, 2001). Additionally, testresults which demonstrate large standard errors of measure shouldbe interpreted cautiously because the large error could be due to lowreliability of the measure (Salvia et al., 2007).
In summary, the research conducted on tinted lenses has failedto demonstrate the efficacy of the practice. The often conflicting find-ings between research studies conducted on Irlen lenses with thoseconducted on Intuitive lenses may be related to study designs, partici-pants, the use of different reading assessments, or even the overlaysthemselves. The Royal College of Ophthalmologists {2002} noted thatthe majority of studies in the literature were poorly designed, but didencourage controlled research to seriously investigate the issue, as didthe American Optometric Association (Williams et al., 2004). Howev-er, neither organization implicitly recommended the use of coloredlenses at the present time. The American Academy of Pediatrics in ajoint statement with the Committee on Children with Disabilities, theAmerican Academy of Ophthalmology, and the American Associationfor Pédiatrie Ophthalmology and Strabismus (1998) took a strongerposition and firmly repudiated the use of lenses, stating that therewas no scientific evidence supporting their use. In fact, they notedthat the expense of such treatment is unwarranted and may provideparents and teachers with a false sense of hope. Following a reviewof research related to Irlen lenses, Kavale and Mostert (2004) stated,"Irlen lenses need to take their place in the history of interventionsthat have been tried in the name of special education but failed" (p.173). Despite these concerns from noted professional organizations,Kriss and Evans (2005) stated that many individuals without readingdifficulties would benefit from the use of colored overlays.

330 HYATT, STEPHENSON and CARTER
Discussion
Summary ;
This review has focused on three practices that have generatedcontroversy regarding their efficacy. Research on the oldest of thethree, PMPs has failed to support their use for remediation of aca-demic difficulties since the original Kavale and Mattson (1983) review,yet many still persist in various guises. Sensory Integration has beenresearched for over 40 years and there has been a failure to provideconvincing evidence suggesting it is effective with any diagnosticgroup. The more recent entrant, tinted lenses, shares the same prem-ise as the older practices: It appears to assume that there is some un-derlying deficit in students with disabilities that can be addressed andthat the proposed intervention will lead to improvement in academicfunctioning.
These practices share other common features, such as uniqueclinical constructs, terminology, and assessment practices, which havealso been identified as characteristic of other controversial treatments(Vyse, 2005), The use of clinical constructs, such as Sensory IntegrativeDysfunction, Cerebellar Developmental Delay and Scotopic Sensitiv-ity Syndrome which are claimed to underlie and "cause" particulardifficulties provides a plausible rationale for the treatments, but theseconditions are not generally recognized outside the particular contro-versial practice. For example, none of the disorders are recognized inDSM-IV'TR (American Psychiatric Association, 2000) and they are notconsistent with accepted neurological theory. It is often specificallyargued that sensory integration is consistent with our understandingof neuroscience (e.g., Dunn, 1988; Heflin & Simpson, 1998). In reality,however, sensory integration theory is highly speculative and thereare significant reasons to question its conceptual foundation (see Ar-endt et al., 1988a; Arendt, MacLean, & Baumeister, 1988b; Hoehn &Baumeister, 1994; Smith et al, 2005). Similarly, as has been illustrat-ed in this paper, the conceptual and theoretical foundations for bothPMPs and colored lenses are highly questionable. The range of symp-toms of these disorders casts a broad net and opposing symptomsmay be included (e.g., under- and over-sensitivity to sensory stimu-lation for sensory integration) or the conditions, such as eye fatigue,may be symptomatic of widely recognized visual disorders. Alignedwith these purported conditions are assessment procedures that maybe questionable or subjective, such as the Schilder test to establishthe presence of persistent reflexes in assessment procedures for somePMPs, postrotary nystagmus in sensory integration (see Hoehn &Baumeister, 1994) or procedures used to select the colors of overlays

A REVIEW OF THREE CONTROVERSIAL PRACTICES 331
or lenses. These assessment procedures are typically unique to thespecific approach and do not have broader scientific acceptance.
In the absence of empirical research, proponents rely heavily ontestimonials, anecdotal evidence and in-house unpublished researchstudies (see for example, DDAX n.d.; Irlen Institute, n.d.). The pre-sentation of anecdote and professional experience in the absence ofscientific evidence (e.g., Evans et al, 1999; Irlen, 1991; Kimball, 1988;Pheloung, 1997) is undoubtedly a factor in the persistence of theseapproaches. Reliance on anecdotes and testimonies is recognized asone of the signs of pseudoscience (Park, 2003) and as a characteristicof controversial or fad treatments in special education (McWilliam,1999). A clear belief that personal perceptions are inherently reliable,even when they are in conflict with objective evidence, is a key featureof pseudoscientifíc thinking (Sagan, 1997; Shermer, 1997). The powerof testimonials as persuaders is recognized by the advertising indus-try (Cialdini, 2001). Newman (2003) provided some compelling ac-counts of the power of personal stories over hard scientific data in thefield of medicine and concluded that a conscious effort is required tomake decisions based on scientific evidence.
Implications for Educators
In the area of education, problems in forming considered judg-ments about the relative value of intervenfions may be exacerbatedby teacher education programs. Postmodernist relativism is common,wherein all information is considered to simply reflect a particularperspective and anecdote and opinion is often given the same weight-ing as controlled empirical research. Teachers are encouraged throughacfion research paradigms to appropriately view themselves as activeresearchers, but perhaps without understanding the very significantlimitations of these methodologies. There is little doubt that teachersmust be taught to be critical consumers of research but this necessar-ily involves understanding what research paradigms are appropriateto what sorts of quesfions as well as the limitations of these episte-mologies. Mostert and Crockett (1999-2000) also argue for the inclu-sion of historical knowledge about failed or discredited interventionsin teacher education. As we have seen, interventions like PMPs havea long history and keep reappearing with different names, differentrationales but essentially the same practices.
In order to become informed consumers of research, educatorsneed to be able to recognize some of the common characteristics ofpseudoscience, as illustrated in the preceding discussion. Warningsigns to the informed consumer may include interventions that arenot consistent with verified theory, that use unique clirucal constructs
332 HYATT, STEPHENSON and CARTER
and assessment practices, and those that rely on anecdotes and tes-timonials, particularly in the absence of solid research evidence. In-formed consumers should eschew unproven interventions or thosewith weak support in favor of those with more substantive evidence.They also have a professional responsibility to monitor developmentsin research, such that practices can be adjusted to reflect change inthe evidence base. While it is likely to be a thankless task, informedconsumers should also endeavor to educate others about the researchbase for interventions, including controversial ones, as well as theprinciples of scientific decision making.
Controversial practices are now widely advertised on the inter-net, often directly to parents and care-givers - another sign of ques-tionable science, according to Park (2003) is by-passing peer reviewand going straight to the media. Despite lack of data supporting theirefficacy, some controversial programs can involve substantial directcosts. For example, the Dore program was recently reported to costaround 1,900 pounds or approximately $3,700 US (Nicholls, 2006).Parents will attempt to search out the most compelling interventionfor their child, but are likely to be uninformed about standards forscientific decision making and the past history of unproven inter-ventions. Thus, professionals will undoubtedly encounter situationswhere parents elect to pursue ineffective or unproven interventionsagainst advice and sometimes at great financial cost. One approachto this dilemma may be to agree with parents on objective expectedoutcomes, time frames and criteria for decisions about effectiveness.Smith et al. (2005) provide several excellent examples of how smalln designs can be used to simply monitor controversial interventionsand assist parents in objective and rational decision-making.
Educators will certainly find themselves in uncomfortable posi-tions during meetings when practices they know are lacking in empir-ical evidence are advocated by other members of the IndividualizedEducation Program (IEP) team. There is no single or simple responseto such a dilemma, but educators must be prepared to meet the chal-lenge with a professional demeanor. Some suggestions could includethe following. First, if an educator learns through prior experiencein meetings or just discission that a professional member of the IEPteam will be recommending a "controversial" practice, the educatorcould meet with the other team member prior to the IEP to disaissany concerns with the "controversial" practice. The discussion maylead to an agreement to collect data on child progress should the in-tervention be implemented, the adoption of a different intervention,or result in a stalemate. If the discussion results in a stalemate andthe "controversial" practice is ultimately accepted by the IEP team.

A REVIEW OF THREE CONTROVERSIAL PRACTICES 333
then there is a legal obligation to provide the service or intervention.However, as with all interventions, a careful monitoring should beconducted to determine the efficacy of the practice, and the lEP teammay even agree to try a practice for a short period of time and reviewthe data before deciding whether to continue with the interventionor not. Second, if a practice is clearly not supported by the researchand, after consultation, the provider insists on recommending thepractice at the meeting, the educator could request a meeting withthe service provider and the administrator to discuss the procedureand determine whether the school administrator would support thatrecommendation during an IEP meeting. Third, an educator couldalso serve in a problem-solving capacity by identifying exactly whatoutcome is to be expected from implementing the specific practice,discuss the research findings, and suggest other alternatives that holdmore promise in achieving the desired outcome. These recommen-dations certainly place a higher level of responsibility on the educa-tor, who must know what may be recommended at and IEP meeting,whether the practice is supported by research, and if not, alternativesthat would more likely achieve the desired outcome.
It is critical that educators become informed consumers of re-search, because school districts must comply with the ÍEP. Certainly,administrative support at an IEP meeting can help the district fromagreeing to unnecessary programming, but part of that result requiresthat the administrator be educated about the controversial practices.Educators should be reminded that the law requires the IEP to providea student with educational benefit, not maximize a student's potential.Ciangreco (2006) provided useful guidelines for determining whethera particular related service was required. Since many of the "contro-versial" practices will be provided as related services, his suggestionsare useful for determining what must be provided. First, some IEPteam members assume that more service is better, but this really con-fuses quantity with quality. Too much of a service could actually bedetrimental, because it could interfere with the student's participationin school activities with typically developing peers, result in stigmati-zation, and create undesired dependencies on the adults who providethe service or the service itself. Second, any service should only be asspecialized as necessary, because this approach lends itself to draw-ing upon natural supports available to the student and also decreasesstudent dependence on supports that are not typical of peers withoutdisabilities. Finally, supports must be educationally relevant and nec-essary. To be relevant, a support must be directly linked to educationaloutcomes, that is, the goals and objecäves on the IEP. If a service is ed-ucationally relevant, then the next question must be whether it is also

334 " HYATT, STEPHENSON and CARTER
necessary for the student to achieve the educational outcomes. If thestudent is receiving the desired benefit without the service, then theservice would not be an educational necessity and the school wouldnot have to provide it.
There is a pressing need for a very visible and accessible sourceof information on the internet about scientific evaluation of interven-tions in special education, similar to the Cochrane Collaboration in thearea of medicine. Such a source could provide balanced informationabout effective and controversial interventions and educate consum-ers about scientific decision making procedures and the characteris-tics of controversial and unproven practices.
In conclusion, there has been a clear shift toward adoption of ev-idence-based practice in the area of education in recent years. Hope-fully, more critical thinking and higher standards of evidence will seea decrease in the use of unproven and disproven interventions, suchas those reviewed in this paper. In order for this to become a reality,professionals must ensure they are informed about evidence-basedpractice and take an active role in disseminating research to consum-ers.
References
Alexander, A. W., & Slinger-Constant, A. (2004). Current status of treat-ments for dyslexia, journal of Child Neurology, 19, 744-758.
American Academy of Pediatrics. (1998). Learning disabilities, dyslex-ia, and vision: A subject review [Electronic version]. Pediatrics,102,1217-1219.
American Academy of Pediatrics. (1999). The treatment of neurologi-cally impaired children using patterning. Pediatrics, 104,1149-1151.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders (Revised 4th ed.). Washington, DC:Author.
Arendt, R. E., MacLean, W. E., & Baumeister, A. A. (1988a). Critique ofsensory integration therapy and its application to mental re-tardation. American Journal on Mental Retardation, 92, 401-411.
Arendt, R. E., MacLean, W. E., & Baumeister, A. A. (1988b). Sensoryintegration theory and practice: An uncertain connection.American journal on Mental Retardation, 95, 427-429.
Ayres, A. J. (1972). Sensory integration and learning disorders. Los Ange-les, CA: Western Psychological Services.
A REVIEW OF THREE CONTROVERSIAL PRACTICES 335
Baranek, G. T. (2002). Efficacy of sensory and motor interventions forchildren with autism, journal of Autism and Developmental Dis-orders, 32, 397-422.
Blaskey, P., Scheiman, M., Parisi, M., Ciner, E. B., Gallaway, M., & Sel-znick, R. (1990). The effectiveness of Irlen filters for improv-ing reading performance: A pilot study, journal of LearningDisabilities, 23, 604-612.
Blythe, S. G. (2000). Early learning in the balance: Priming the firstABC. Support for Learning, 15,154-158.
Bouldoukian, J., Wilkins, A. J., & Evans, B. J. W. (2002). Randomisedcontrolled trial of the effect of coloured overlays on the rate ofreading of people with specific learning difficulties. Ophthal-mic & Physiological Optics, 22, 55-60.
Brain Gym® (2006a). About Brain Gym ®. Retrieved 25th July, 2006from http://www.braingym.org/about.html
Brain Gym® (2006b). What are Edu-K's three dimensions? Retrieved25th July, 2006 from http://www.braingym.org/FAQ.html
Bundy, A. C, & Murray, E. A. (2002). Sensory integration: A. JeanAyres' theory revisited. In A. C. Bundy, S. J. Lane, & E. A. Mur-ray (Eds.), Sensory Integration: Theory and practice. (2nd ed., pp.3-33). Philadelphia, PA: F. A. Davis.
Christenson, G. N., Griffin, J. R., Taylor, M. (2001). Failure of blue-tinted lenses to change reading scores of dyslexic individuals.Optometry, 72, 627-633.
Chu, S. K. H. (1989). The application of contemporary treatment ap-proaches in occupational therapy for children with cerebralpalsy. British journal of Occupational Therapy, 52, 343-348.
Cialdini, R. B. (2001). ¡nßuence: Science and practice (4* ed.). Boston,MA: Allyn & Bacon.
Council for Learning Disabilities (1987). Measurement and training ofperceptual and perceptual-motor functions, journal of Learn-ing Disabilities, 20, 350.
Dawson, G. D., & Watling, R. (2000). Interventions to facilitate audi-tory, visual, and motor integration in autism: A review of theevidence, journal of Autism und Developmental Disorders, 30,415-421.
Dunn, W. (1988). Basic and applied neuroscience research provides abase for sensory integration theory. American journal on Men-tal Retardation, 92, 420-422.

336 ' HYATT, STEPHENSON and CARTER
DDAT (2006a). How does it work? Retrieved 25th July, 2006 fromhttp://www.ddat.co.uk/how.aspx.
DDAT (2006b). Frequently asked questions. Retrieved 27th July, 2006from http://www.ddat.co.uk/faq/aspx .
DDAT (n.d.). Independent research. Retrieved 27th July 2006 fromhttp://www.dore.com.au/content/research.html.
Dore, W. (2006). Dyslexia: Vie miracle cure. London: John BlakePublishing.
Evans, B. J. W., Patel, R., Wilkins, A. J., Lightstone, A., Eperjesi, R,Speedwell, L., & Duffy, J. (1999). A review of the managementof 323 consecutive patients seen in a specific learning difficul-fies clinic. Ophthalmic & Physiological Optics, 19, 454-466.
Fawcett, A. J., Nicolson, R. 1., & Maclagan, F. (2001). Cerebellar testsdifferenfiate between groups of poor readers with and with-out IQ discrepancy. Journal of Learning Disabilities, 34, 119-135.
Fletcher, J., & Martinez, G. (1994). An eye-movement analysis of theeffects of scotopic sensitivity correction on parsing and com-prehension. Journal of Learning Disabilities, 27, 67-70.
Giangreco, M. F. (2006). Foundafional concepts and practices for ed-ucating students with severe disabilities. In M. E. Snell & F.Brown (Eds.), Instruction of students with severe disabilities (6thed., pp. 1-27). Upper Saddle River, NJ: Pearson.
Goddard-Blythe, S. (2000). Early learning in the balance: Priming thefirst ABC. Support for Learning, 15,154-158.
Goddard-Blythe, S. (2005). Releasing educational potential throughmovement: A summary of individual studies carried out us-ing the INPP test battery and developmental exercise pro-gramme for use in schools with children with special needs.Child Care in Practice, 11,415-432.
Goldstein, H. (2000). Commentary: Interventions to facilitate auditory,visual, and motor integration: "Show me the data". Journal ofAutism and Developmental Disorders, 30. 423-425.
Green, V. A., Pituch, K. A., Itchon, J., Choi, A., O'Reilly, M., & Siga-foos, J. (2006). Internet survey of treatments used by parentsof children with autism. Research in Developmental Disabilities,27, 70-84.
Hammill, D. D. (2004). What we know about the correlates of reading.Exceptional Children, 70, 453-469.

A REVIEW OF THREE CONTROVERSIAL PRACTICES 337
Heflin, L. J., & Simpson, R. L. (1998). Interventions for children andyouth with autism: Prudent choices in a world of exaggeratedclaims and empty promises. Part I: hitervention and treat-ment option review. Focus on Autism and Other DevelopmentalDisabilities, 13, 194-211.
Helveston, E. M. (1987). Vol III module 1; Management of dyslexiaand related learning disabilities, journal of Learning Disabili-ties, 20, 415-421.
Hoehn, T P., & Baumeister, A. A. (1994). A critique of the applicationof sensory integration therapy to children with learning dis-abilities. Journal of Learning Disabilities, 27,338-350.
Hoyt, C. S. (1990). Irlen lenses and reading difficulties./ournfl/o/Liflr«-ing Disabilities, 23, 624-626.
Hyatt, K. J. (2007). Brain gym: Building stronger brains or wishfulthinking. Remedial and Special Education, 28,117-124.
Individuals with Disabilities Education Improvement Act of 2004, 20U.S.C. § 1400 et seq.
The Institute for Neuro-Physiological Psychology (n.d.) INPP Neuro-developmental factors in dyslexia. Retrieved 25th July 2006from http://www.inpp.org.uk/lNPP_5_l_NDD_factors_dys-lexia.php.
The Institute of Optometry. (n.d.) Coloured overlays and colouredlenses: Frequently asked questions. Retrieved August 6, 2006,from http://www.ioo.org.uk/appoint4.htin.
Irlen, H. (1991). Reading by the colors. Garden City Park, NY; AveryPublishing Group. j '
The Irien Institute, (n.d.). Irlen syndrome/scotopic sensitivity: Most fre-quently asked questions. Available from Irlen Institute Web site,h ttp ://w w w.ir len. com/ind ex_sss. h tml.
Jacobson, R. M. Foxx, & J. A. Mulick (Eds.). (2005). Controversial thera-pies for developmental disabilities: Fads, fashions, and science inprofessional practice. Mahwah, NJ; Lawrence Erlbaum.
Jacobson, J. W., Mulick, ]. A., & Foxx, R. M. (2005). Historical approach-es to developmental disabilities. In J. W. Jacobson, R. M. Foxx,& J. A. Mulick (Eds.), Controversial therapies for developmentaldisabilities: Fads, fashions, and science in professional practice (pp.61-84). Mahwah, NJ: Lawrence Erlbaum.
Jordan-Black, J. (2005). The effects of the Primary Movement pro-gramme on the academic performance of children attenclingordinary primary school. Journal of Research on Special Educa-tion Needs, 5, lOl-lU.

338 • HYATT, STEPHENSON and CARTER
Kavale, K. A., & Forness, S. R. (2000). Policy decisions in special educa-tion: The role of meta-analysis. In R. Gersten, E. P. Schiller, &S. Vaughn (Eds.), Contemporary special education research: Syn-theses of the knowledge base on critical instructional issues, (pp.251-262). Mahwah, NJ: Lawrence Erlbaum.
Kavale, K. A., & Mattson, P D. (1983). "One jumped off the balancebeam": Meta-analysis of perceptual-motor training. Journal ofLearning Disabilities, 16,165-173.
Kavale, K. A., & Mostert, M. P. (2004). The positive side of special edu-cation: Minimizing its fads, fancies, and follies. Lanaham, MD:Sea rercrow Education.
Kimball, J. G. (1988). The emphasis is on integration, not sensory.American Journal on Mental Retardation, 92, 423-424.
Kriss, I., & Evans, B. J. W. (2005). The relationship between dyslexiaand Meares-Irlen syndrome. Journal of Research in Reading, 28,350-364.
LiUenfeld, S. O., Lynn, S. }., & Lohr, J. M. (Eds.). (2003). Science andpseudoscience in clinical psychology. New York: Guilford Press.
Lord, C, & McGee, J. P (Eds.). (2001). Educating children with autism.Washington, DC: National Academy Press.
Lopez, R., Yolton, R. L., Kohl, P, Smith, D. L., & Saxerud, M. H. (1994).Comparison of Irlen scotopic sensitivity syndrome test resultsto academic and visual performance data, journal of the Ameri-can Optometric Association, 65, 705-712.
Martin, F., Mackenzie, B., Lovegrove, W., & McNicol, D. (1993). Irlenlenses in the treatment of specific reading disability: An eval-uation of outcomes and processes. Australian journal of Psy-chology, 45(3), 141-150.
Mason, S. A., &: Iwata, B. A. (1990). Artifactual effects of sensory-inte-grative therapy on self-injurious behavior, journal of AppliedBehavior Analysis, 23, 361-370.
McPhillips, M., Hepper, P. G., & Mulhem, G. (2000). Effects of replicat-ing primary-reflex movements on specific reading difficultiesin children: A randomised, double-blind, controlled trial. TheLancet, 355, 537-5^1.
McWilliam, R. A. (1999). Controversial practices: The need for a reac-culturation of early intervention fields. Topics in Early Child-hood Special Education, 19,177-185.
Metzger, R. L., & Werner, D. B. (1984). Use of visual training for read-ing disabilities: A review. Pediatrics, 73, 824-829.
A REVIEW OF THREE CONTROVERSIAL PRACTICES 339
Miller, L. J. (2003). Empirical evidence related to therapies for sen-sory processing impairments. NASP Communiqué, 31 (5).Retrieved August 9, 2006, from http://www.nasponline.org/publications/cq315sensory.html.
Mostert, M. P., & Crockett, I. B. (1999-2000). Reclaiming the history ofspecial education for more effective practice. Exceptionality, 8,133-143.
New Screeners. (2006, September). Irlen International Newsletter, 16(2),11-12. Available from Irlen Institute Web site, http://irlen.com/index.php?s=inewsletters.
Newman, T. B. (2003). The power of stories over statistics. British Med-ical journal, 327, U24-U27.
New York State Department of Health. (1999). Clinical practice guide-line - Report of the guideline recommendations: Autism / Per-vasive Developmental Disorders assessment and interventionfor young children (age 0-3 years). Retrieved August 8, 2006,from http://www.health.state.ny.us/community/infants_chil-d ren/ea r ly_intervention/au tism/ind ex .htm.
Nicholls, K. (2006, 24 October). Dyspraxia: Severe developmental co-ordination disorder explained. The Independent. RetrievedOctober 25, 2006 from http://news.independent.co.uk/uk/health_medical/article]919584.ece.
No Child Left Behind Act of 2001, 20 U.S.C. § 6301 et seq.Northway, N. (2003). Predicting the continued use of overlay s in school
children - a comparison of the developmental eye movementtest and the rate of reading test. Ophthalmic & Physiological Op-tics, 23, 457-464.
O'Connor, P. D., Sofo, F., Kendall, L., & Olsen, G. (1990). Reading dis-abilities and the effects of colored filters, journal of LearningDisabilities, 23, 597-603.
Ottenbacher, K. (1982). Sensory integration therapy: Affect or effect.American journal of Occupational Therapy, 36, 571-578.
Ottenbacher, K. J. (1988). Sensory integration - myth, method, and im-perative. American journal on Menial Retardation, 92, 425-426.
Othmer, S. (2006, January). Irlen North American Conference. IrlenInternational Newsletter, 16(1), 1,4-5. Retrieved June 30, 2007,from http://irlen.com/index.php?s=inewsletters.
Park, R. L. (2003). The seven warning signs of bogus science. Chronicleof Higher Education, 49, 20-21

340 HYATT, STEPHHNSON and CARTER
I I
Parker, R. M. (1990). Power, control, and validity in research, journal ofLearning Disabilities, 23, 613-620.
Perry, A., & Condillac, R. (2003). Evidence-based practices for children andadolescents with autism spectrum disorders: Review ofthe litera-ture and practice guide. Toronto, Canada: Children's MedicalHealth Ontario.
Pheloung, B. (1997). Help your class to learn: Effective perceptual move-ment programs for your classroom. Manly, NSW: Author.
Rack, J. P, Snowling, M. J., Hulme, C, & Gibbs, S. (2007). No evidencethat an exercise-based treatment programme (DDAT) hasspecific benefits for children with reading difficulties. Dys-lexia, 13, 97-104.
Reynolds, D., Nicolson, R. 1., & Hambly, H. (2003). Evaluation of anexercise-based treatment for children with reading difficulty.Dyslexia, 9, 48-71.
Reynolds, D., & Nicolson, R. J. (2007). Follow-up of an exercise-basedtreatment for children with reading difficulties. Dyslexia, 13,78-96.
Roberts, J. M. (2004). A review ofthe research to identify the most effectivemodels of best practice in the management of children with autismspectrum disorders. Sydney, Australia: Centre for Developmen-tal Disability Studies.
Robinson, G. L. W., & Conway, R. N. F. (1990). The effects of Irlencolored lenses on students' specific reading skills and theirperception of ability: A 12-month validity study, journal ofLearning Disabilities, 23, 589-596.
Robinson, G. L., & Foreman, P. J. (1999a). Scotopic sensitivity/Irlensyndrome and the use of coloured filters: A long-term pla-cebo-controlled study of reading strategies using analysis ofmiscue. Perceptual and Motor Skills, 88, 35-52.
Robinson, G. L., & Foreman, P. J. (1999b). Scotopic sensitivity/Irlensyndrome and the use of coloured filters: A long-term place-bo controlled and masked study of reading achievement andperception of ability. Perceptual and Motor Skills, 88, 83-113.
Rooney, K. J. (1991). Controversial therapies: A review and critique.Intervention in School and Clinic, 26(3), 134-142.
Royal College of Ophthalmologists. (2002, Autumn). Developmentaldyslexia. Retrieved July 3, 2006 from http://www.rcophth.ac.uk/docs/members/focus/FocusAutumn02.pdf.
Sagan, C. (1997). The demon haunted world: Science as a candle in the dark.London: Headline Book Publishing.

A REVIEW OF THREE CONTROVERSIAL PRACTICES 341
Salvia, J., Ysseldyke, J. E., & Bolt, S. (2007). Assessment in special andinclusive education (10th ed.). Boston, MA: Houghton MifflinCompany.
Saint-John, L. M., & White, M. A. (1988). The effect of coloured trans-parencies on the reading performance of reading-disabledchildren. Australian Journal of Psychology, 40, 403-411.
Schaaf, R. C, & Miller, L. J. (2005). Occupational therapy using a sen-sory integrative approach for children with developmentaldisabilifies. Mental Retardation and Developmental DisabilitiesResearch Reviews, 11, 143-148.
Scott, L., McWhinnie, H., Taylor, L., Stevenson, N., Irons, P., Lewis, E.,Evans, M., Evans, B., & Wilkins, A. (2002). Coloured overlaysin schools: Orthoptic and optometric findings. Ophthalmic &Physiological Optics, 22,156-165.
Shaw, S. R. (2002). A school psychologist investigates sensory integra-tion therapies: Promise, possibility, and the art of placebo.NASP Communiqué, 31 (2). Retrieved August 9, 2006, fromhttp://www.nasponline.org/publications/cq312si.html.
Shermer, M. (1997). Why people believe loeird things: Pseudoscience, super-stition, and other confusions of our time. New York: Henry Holt.
Sieben, R. L. (1977). Controversial medical treatments of learning dis-abilities. Academic Therapy, 13,133-147.
Silver, L. B. (1995). Controversial therapies. Journal of Child Neurology,10,96-100.
Smith, T., Mruzek, D. W., & Mozingo, D. (2005). Sensory integrafivetherapy. In J. W. Jacobson, R. M. Foxx, & J. A. Mulick (Eds.),Controversial therapies for developmental disabilities: Fad, fashion,and science in professional practice, (pp. 331-350). Mahwah, NJ:Lawrence Erlbaum. ,
Snowling, M-, & Hulme, C. (2003). A critique of claims from Reynolds,Nicolson & Hambly (2003) that DDAT is an effective treat-ment for children with reading difficulfies - 'Lies, dammedlies and (inappropriate) statistics?' Dyslexia, 9,127-133.
Solan, H. A. (1990). An appraisal of the Irlen technique of correctingreading disorders using tinted overlays and tinted lenses.Journal of Learning Disabilities, 23, 621-623, 626.
Stephenson, J. (2004). A teacher's guide to controversial pracfices. Spe-cial Education Perspectives, 13, 66-74.
Stone, J., & Harris, K. (1991). These coloured spectacles: What are theyfor? Support for Learning, 6(3), 116-118.
342 HYATT, STEPHENSON and CARTER
I i' - , ,
Thomdike, R. M., & Dinnel, D. L. (2001). Basic statistics for the behav-ioral sciences. Upper Saddle River, NJ: Prentice Hall, Inc.
Vargas, S., & Camilli, G. (1999). A meta-analysis of research on sen-sory integration treatment. American Journal of OccupationalTherapy, 53,189-198.
Vyse, S. (2005). Where do fads come from? In J. W. Jacobson, R. M.Foxx, & J. A. Mulick (Eds.), Controversial therapies for develop-mental disabilities: Fads, fashions, and science in professional prac-tice (pp. 3-17). Mahwah, NJ: Lawrence Erlbaum.
Whitely, H. E., & Smith, C. D. (2001). The use of tinted lenses to al-leviate reading difficulties, journal of Research in Reading, 24,30-40.
Whichard, J. A., Feller, R. W., & Kastner, R. (2000). The incidence ofscotopic sensitivity syndrome in Colorado inmates, journal ofCorrectional Education, 51, 294-299.
Wiederholt, J. L. (1990). A preface to the special series. Journal of Learn-ing Disabilities, 23, 588.
Williams, G. J., Kitchener, G., Press, L. J., Scheiman, M. M., & Steele, G.T. (2004). The use of tinted lenses and colored overlays for thetreatment of dyslexia and other related reading and learningdisorders. Optometry, 75, 720-722.
Wilkins, A. J., Jeanes, R. J., Pumfrey, P. D., & Laskier, M. (1996). Rate ofReading Test: Its reliability, and its validity in the assessmentof the effects of coloured overlays. Ophthalmic & PhysiologicalOptics, 6, 491-497.
Wilkins, A. J., Lewis, E., Smith, F., Rowland, E., & Tweedie, W. (2001).Coloured overlays and their benefit for reading. Jourîtal of Re-search in Reading, 24, 41-64.
Woerz, M., & Maples, W. C. (1997). Test-retest reliability of coloredfilter testing. Journal of Learning Disabilities, 30, 214-221.
Yee, C. E. (2007). Sensory diet. Retrieved October 16,2007, from http://www.autism-mi.org/aboutautism/generalll.html.






























