Embed Size (px)
Citation preview

A retrospective study to the patient-reported outcome after an anterior cruciate ligament reconstruction:
a comparison between Endobutton® and TransFix®
Name: N.H. Hoefnagels Student number: 1638491 Supervisor: Dr. R.G. Zuurmond Isala Klinieken, orthopaedic department 15 February 2013 – 5 July 2013

2
Abstract Background. Traumatic injuries of the anterior cruciate ligament (ACL) are among the most common sports injuries to the knee. Treatment consists of conservative- or surgical treatment. In surgical ACL-reconstructions, currently there is no gold standard in the fixation method of the ACL-graft to the femur. Extracortical- and transfemoral fixation both show decent biomechanics. Thereby, both procedures give comparable stability and there is an indication that the functional outcome is similar as well. The purpose of this retrospective cohort study is to objectify and compare the patient-reported outcomes of an extracortical fixation (Endobutton®) and a transfemoral fixation (TransFix®), 2-3 years after ACL-reconstruction. Patients and methods. All 112 patients included in this study, underwent an ACL-reconstruction in the Isala Klinieken Zwolle in 2010. Femoral fixation was either with Endobutton® (n=53) or with TransFix® (n=59). Primary outcome was the patient-reported outcome measured by the Knee Injury and Osteoarthritis Outcome Score (KOOS). Secondary outcome was the patient-reported outcome, determined by the International Knee Documentation Committee (IKDC) subjective knee evaluation form, the Lysholm knee score and the Tegner Activity Scale (TAS). Furthermore, possible differences in the number of required additional surgical procedures, the duration of the ACL-reconstruction and the contentment of the patients were objectified. The possible correlation of these factors with the patient-reported outcome was objectified as well. Additionally, the surgeon and the patient characteristics (gender/age/BMI) were correlated to patient-reported outcome. Results. There was no significant difference in patient-reported outcome between Endobutton® and TransFix® measured by the KOOS (p-value >0.05). No major differences were seen in results of the IKDC, Lysholm and TAS. Patient characteristics, duration of surgical procedures and contentment of the patients were comparable between the two methods and did not correlate with patient-reported outcome. Patient-reported outcome of this study did not correlate with the individual surgeon. There were more re-operations required in the TransFix® group than in the Endobutton® group (respectively 20.34% and 7.55%), although differences were not considered significant. Patient-reported outcome is significantly lower in patients who underwent a re-operation. The mean follow-up was 2 year and 288 days after ACL-reconstruction. Conclusion. The patient-reported outcome of Endobutton® and Transfix® are comparable after 2-3 year follow-up. Results indicate that the number of required additional procedures is remarkably higher in the population with TransFix®. Since patient-reported outcomes are significantly lower in patients who underwent a re-operation, further analysis is clinically relevant.

3
Table of contents
ABSTRACT ........................................................................................................................................................ 2
INTRODUCTION ................................................................................................................................................ 4
ANATOMY AND FUNCTION OF THE ANTERIOR CRUCIATE LIGAMENT ..................................................................................... 4 INCIDENCE OF ACL-INJURIES ...................................................................................................................................... 4 MECHANISM OF AN ACL-INJURY ................................................................................................................................. 5 SIGNS AND SYMPTOMS OF AN ACL-TEAR ...................................................................................................................... 5 THERAPEUTIC OPTIONS: CONSERVATIVE OR SURGICAL TREATMENT? ................................................................................... 5 SURGICAL TREATMENT .............................................................................................................................................. 6 FACTORS INFLUENCING THE SUCCESS OF AN ACL-RECONSTRUCTION ................................................................................... 6 GRAFT SELECTION ..................................................................................................................................................... 7 FEMORAL FIXATION OF THE GRAFT ............................................................................................................................... 8 SURGICAL PROCEDURES BEING COMPARED IN THIS SPECIFIC STUDY ................................................................................... 11
TransFix® ........................................................................................................................................................ 12
Endobutton® .................................................................................................................................................. 12
PURPOSE AND HYPOTHESES OF THIS SPECIFIC STUDY ...................................................................................................... 13
PATIENTS AND METHODS .............................................................................................................................. 14
STUDY DESIGN ....................................................................................................................................................... 14 PATIENTS .............................................................................................................................................................. 14 QUESTIONNAIRES ................................................................................................................................................... 16 STATISTICAL ANALYSIS ............................................................................................................................................. 18
RESULTS ......................................................................................................................................................... 19
PRIMARY OUTCOME: THE KNEE INJURY AND OSTEOARTHRITIS OUTCOME SCORE (KOOS) .................................................... 19 SECONDARY OUTCOMES .......................................................................................................................................... 19
Questionnaires: IKDC, Lysholm and Tegner ................................................................................................... 19 Gender ........................................................................................................................................................... 20 Age ................................................................................................................................................................ 20 Body Mass Index (BMI) .................................................................................................................................. 20 Duration of surgery ....................................................................................................................................... 21 Required additional surgical procedures ....................................................................................................... 21 Correlation with the individual surgeon ........................................................................................................ 22 Contentment after the ACL-reconstruction ................................................................................................... 23
DISCUSSION AND CONCLUSION ..................................................................................................................... 24
REVIEW OF CURRENT LITERATURE .............................................................................................................................. 24 RESULTS ANALYZED IN THE LIGHT OF CURRENT LITERATURE ............................................................................................. 25 POSSIBLE CONFOUNDING FACTORS OF THIS STUDY ........................................................................................................ 26 ADVANTAGES OF THIS STUDY .................................................................................................................................... 28 IMPLICATIONS FOR FUTURE RESEARCH ........................................................................................................................ 28 CONCLUSIONS ....................................................................................................................................................... 29
ACKNOWLEDGEMENTS .................................................................................................................................. 30
DUTCH SUMMARY ......................................................................................................................................... 31
APPENDICES ................................................................................................................................................... 32
APPENDIX I: METC ................................................................................................................................................ 32 APPENDIX II: KNEE INJURY AND OSTEOARTHRITIS OUTCOME SCORE (KOOS) .................................................................... 33 APPENDIX III: INTERNATIONAL KNEE DOCUMENTATION COMMITTEE (IKDC) SUBJECTIVE KNEE EVALUATION FORM ................... 37 APPENDIX IV: LYSHOLM KNEE SCORING SCALE ............................................................................................................ 39 APPENDIX V: TEGNER ACTIVITY SCALE (TAS) .............................................................................................................. 40
REFERENCES ................................................................................................................................................... 41

4
Introduction
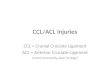
Anatomy and function of the anterior cruciate ligament The knee (or genual) joint is the largest joint in the body. By contracting various muscles, the knee is carried out to actively move the leg in flexion, extension, medial rotation and lateral rotation. The anterior cruciate ligament (ligamentum cruciatum anterius, ACL) is an important stabilizing ligament of the knee. Together with the posterior cruciate ligament (ligamentum cruciatum posterius, PCL), the ACL ensures stability by preventing the anterior movement of the tibia with respect to the femur. The tibia and femur are the largest bone of respectively the lower and upper leg. The cruciate ligaments are called cruciate, because they cross each other, and anterior and posterior from the position of their attachments to the tibia. Figure 1 shows the anatomy of the knee joint. The anterior cruciate ligament not only prevents the anterior movement of the tibia, but also the rotation of the tibia and varus-valgus angulations when the patient’s leg is in extension.1 This stabilizing function of the knee is primary required during heavy work or turning movements while participating in sports. Therefore ACL injuries are one of the most common sports injuries to the knee.2
Figure 1. Anterior view of the right knee in full extension, patella is reflected from anterior part.
1
Incidence of ACL-injuries The exact incidence of ACL-tears in the Netherlands is not known. Based on literature from the United States, it is estimated 1 on 3000 people, which is 95.000 patients per year in the United States.3 The estimated incidence of ACL-lesions in athletes is higher and is 1 on 556.4
In comparison to the PCL, the ACL is 10 times more often injured.5 Exact data about the number of surgical ACL-repairs in the Netherlands is also not precisely known, but is estimated around 6.000 operations per year. In the Isala Klinieken in Zwolle, the Netherlands, around 200 ACL-reconstructions are performed yearly. Women are more prone to develop an ACL lesion. The exact reason for the higher incidence is women is not fully cleared out, but is defined as a multifactorial matter.6,7

5
Mechanism of an ACL-injury There are two possible mechanisms of ACL injury, including both high-energy (e.g., motor vehicle collision) and low-energy (i.e., noncontact field sport). These mechanisms could both be divided in noncontact- and contactmechanisms. Noncontact mechanisms are classified as sudden deceleration prior to a change of direction or landing motion. Contact injuries occurred as a result of a direct valgus collapse of the knee. The most common mechanism of an ACL lesion is the low-energy noncontact mechanism during athletic activity. Noncontact mechanisms are in 72% the cause of the ACL rupture.8 There are studies performed by video-analysis to the movement of an ACL-injury. They conclude that the most common movement during an ACL-rupture is a forceful valgus movement of the leg from a position in which the knee is close to full extension combined with some rotation of the tibia (external or internal).9 Figure 2 shows this movement of the leg during an ACL-rupture.
Figure 2. Low-energy noncontact mechanism of an ACL-rupture: valgus movement of the knee, combined with internal (or external) rotation of the tibia.
10
Signs and symptoms of an ACL-tear At the moment of trauma, patients often complain about feeling or hearing a “plop” in their knee at the moment of injury. This is often followed by pain, an acute swelling and an unstable feeling of the knee. This mechanical instability is described as ‘giving way’ of the knee.2,11,12 An acute haemarthrosis is a sign for a possible ACL-tear. Approximately 50-70% of all the patients with haemarthrosis of the knee have an ACL lesion.13,14 Another, less common, possible presentation of an ACL-tear has a less acute character. Those patients have little complaints directly after the knee trauma. Over time, as a result of the ACL tear, patients develop an unstable feeling in their knee and symptoms of their knee ‘giving way’.
Therapeutic options: conservative or surgical treatment? In the treatment of a symptomatic ACL-tear, there are two possible therapeutic options: conservative- or surgical treatment. Conservative treatment consists of a physiotherapy exercise program which contains strength training, senso-motoric training (balance- and proprioception) and wearing a knee brace.15 Surgical treatment consists of an operational repair of the anterior cruciate ligament. It is worth mentioning that after surgical repair, it is also recommended to start with (non-surgical) treatment like strength training, combined with neuromuscular training.11 Because this study is focused on aspects of surgical therapy of an ACL-rupture, the present situation in literature about conservative treatment will not further be discussed.

6
Surgical treatment In the past 25 years, surgical treatment of ACL-tears developed considerably. In literature there are many studies described about both the internal and external factors possibly affecting the result of an ACL-surgery. Besides these factors, various different surgical options have been compared, described and analyzed. To optimize the success-ratio of an ACL-reconstruction, it is important to practice evidence-based medicine. Because of numerous studies on ACL-reconstruction in the past decades, numbers of failing ACL-reconstructions are decreasing.16,17
Factors influencing the success of an ACL-reconstruction As mentioned earlier, the results of an ACL-reconstruction are influenced by different factors. In the decision whether to choose for a surgical ACL-reconstruction or not, the expectations of an operational treatment should be considered by both patient and physician. This contributes to the right indication for a surgical repair of the ACL and thereby the rate of success. The most important parameter for the indication of an ACL reconstruction is the patients’ activity level. The more the patient is participating in sports, the higher the chance that surgery is necessary to ensure an (for the patient) acceptable level of activity.18 On the other hand, patients who participate in sports with a higher risk of ACL-injury, have higher chance of a re-rupture, secondary surgery and osteoarthritis.2,19
Sports with a higher risk of ACL-injury are ‘pivoting’ sports or sports with physical contact (like football, American football, basketball, volleyball, gymnastics, handball or downhill skiing). In general, younger patients have higher level of activities. That is why younger patients are more eligible for an ACL-repair than older patients.20-22 Nevertheless, the effect of the patients’ age should not be considered in the decision for anterior cruciate ligament reconstruction. There is no significant difference in outcome between different ages.21,22 Although women are more at risk for an ACL injury, there is no evidence that difference in gender of the patient influences the clinical outcome or the chance of failure of an ACL-reconstruction.2,6,7,23,24 Other patient-relevant factors on the outcome of an ACL-reconstruction are the pre-existing degenerative damage of the knee or the meniscus. Patients with existing chondropathy have significant lower clinical outcome after ACL-surgery.25,26 There are indications that ACL insufficiency and medial osteoarthritis have negative influence on each other.27
Also a high body mass index (BMI) and smoking have a negative influence on the rate of success of the ACL-reconstruction. In current literature could be found that patients with a BMI greater than 30 have 0.35 times the odds of success as subjects with a lower BMI. Also smokers have 0.36 times the odds of success, compared to as patients who do not smoke.25 The right timing of surgical treatment does influence the clinical outcome of the ACL-reconstruction as well. In current literature there is not a clear consensus about the optimal timing of an ACL-repair. However in the acute phase after injury, when there is still synovial reaction and a full extension of the knee is not possible, ACL reconstruction is contraindicated.28 It is described that a sub-acute reconstruction (within 6 weeks) gave

7
better outcome for range of motion, work participation, and degenerative change than late reconstruction.29 Besides this, in younger patients it is preferred to wait for an ACL- reconstruction until the growth plates are nearly closed.11
Another important factor of the success of an ACL-reconstruction is the surgeon. Menetrey et al. concluded in an overview article that technical and mechanical aspects, which influence the outcome of a surgical treatment, are directly depended of the surgeon and his skills.30 Additionally, intra-operational technical failures are the most common cause of the failure of an ACL-reconstruction.31
Graft selection In historical perspective, repair of the anterior cruciate ligament once was performed by only suturing the injured ligament. A major disadvantage of suturing the native ACL, is that a high percentage of the sutures will rupture and a considerable amount of patients experience instability after this operation. The reported percentage of revision surgery of sutured ACL’s is 24%.16 Nowadays, reconstructions of the anterior cruciate ligament are arthroscopic procedures. The ruptured ACL is substituted by a graft. ACL-reconstructions have been described and performed with different kinds of grafts: autografts, allografts and synthetic grafts. Table 1 shows an overview of the various types of grafts. An autograft is tissue from the patient itself, used as a substitute for the ruptured anterior cruciate ligament. An allograft is donor tissue from another individual than the patient. Synthetic grafts are manufactured made out of various materials like carbon fibre, polypropylene and polyester.32 ACL-reconstructions with synthetic grafts are not very common because they reported a higher rate of complications compared tot autograft and allograft. Reported problems of synthetic grafts are synovitis, lack of fibrous tissue ingrowth, failed adhesion to bone tunnels with subsequent poor biomechanical properties and chronic instability.32,33 The short-term clinical outcomes of anterior cruciate ligament reconstruction with allograft are not significantly different from those with autograft.17,34 In the Netherlands, only autografts are being used for ACL-reconstructions.3,11 There are four different types of autografts that are being used in the ACL-reconstruction. Those are bone-patella-tendon-bone (BPTB-graft), the tendon of the hamstrings (m. gracilis and m. semitendinosus), the m. quadriceps tendon or the fascia lata.
Autograft Allograft Synthetic graft
Bone-pattela-tendon-bone Bone-pattela-tendon-bone Scaffolds
Hamstrings Hamstrings Stents
Quadriceps tendon Quadriceps tendon Prostheses
Fascia lata Tibialis anterior/posterior tendon
Achilles tendon
Fascia lata
Table 1. Different types of graft for ACL-reconstruction: autograft, allograft and synthetic grafts.
The auto-transplantations of patella tendon and hamstring grafts are most common in reconstructive ACL surgery. An often-reported disadvantage of a BPTB-graft is anterior knee pain, which is present in a significant higher percentage of patients than with hamstring-

8
grafts. Various systematic reviews suggest that hamstring tendon autografts are superior for preventing anterior knee pain.35 Regarding functional outcome, meta-analyses show that BPTB-grafts and hamstring grafts are equal.17,36-38 There is also no difference in percentage of rupture, complications and loss of strength in extensors or flexors of the knee.37,39 In literature is described that BPTB-grafts generate more stability than hamstring grafts.36,40,41 However, in these studies they do not differentiate in the fixation technique of the graft in the femur. Poolman et al. made subgroups in those studies and concluded there is limited evidence that bone-patella-tendon-bone autografts provide better stability if you differentiate in the various methods of fixation of the graft to the femur.35 With extracortical fixation (see ‘Femoral fixation of the graft’) there is no difference in stability between the BPTB and the hamstring-graft. There is even a study where, with extracortical fixation, the hamstring graft has a better stability than the BPTB-graft.42
Femoral fixation of the graft There are many different techniques for the fixation of the ACL-graft to the femur.43,44 Figure 3 shows an overview of various femoral fixation methods that are being used. The femoral fixation techniques could be classified according to their fixation mechanism: compression (figure 3A and 3B); expansion (figure 3C); cortical suspension (figure 3D, 3E and 3F); cancellous suspension (figure 3G); and cortical-cancellous suspension (figure 3H and 3I).44 (Current techniques include suspensory fixation, transfemoral fixation with cross-pins (cortico-cancellous suspension) and joint line fixation with interference screws.45-47 Currently, there is no gold standard for the femoral fixation of grafts in ACL reconstruction. A direct stabile fixation of the ACL-graft to the femur after the ACL-reconstruction is required to avoid slippage of the graft and allow graft healing. It could take 8-12 weeks until the soft tissue graft is healed to the osseous tunnel.45 Strong fixation of the graft is necessary for using current rehabilitation protocols, which allow full ‘range of motion’, early weight bearing, and return of neuromuscular function.48 During rehabilitation, forces as high as 450–500 Newton are usually applied to the ACL-graft. The rate of failure of an ACL-reconstruction is difficult to calculate and may be underreported, but in literature rates in the range from 4% to 27.3% are described. 43,49

9
Figure 3. Overview of the different graft fixation complexes in the femur. (A) Bioscrew
®; (B) RCI screw
®; (C) Rigidfix
®; (D)
Ligament Anchor®; (E) Endobutton
®; (F) Swing Bridge
®; (G) Linx-HT
®; (H) Transfix
® and (I) Bio-Transfix
®.44
In current literature, various studies are available to the different femoral fixation techniques in ACL-reconstruction. Important aspects of a decent fixation are biomechanical strength of the fixation of the graft, stability of the joint, the iatrogenic risks of anatomical structures, the effect of the graft to the bone (‘tunnel widening’), and functional outcome. Ahmad et al. performed a study on thirty-three porcine femora, where they tested the biomechanical strength of four different fixation techniques that are also shown in figure 3.44 The interference screw (figure 3A and 3B) and the Rigidfix® fixation (figure 3C) demonstrated significantly inferior fixation biomechanics compared to the Bio-Transfix® and the Endobutton® techniques (figure 3I and 3E). They showed more slippage of the graft in the osseous tunnel and there was a lower load to failure.50 Milano et al. also performed a cadaver study and found that cortical-cancellous suspension fixation (figure 3H and 3I) offered the best and most predictable results in terms of elongation, fixation strength, and stiffness.44 The weakest fixation was attained with cancellous fixation devices (figure 3G). By determining the anterior translation of the tibia, the stability of the ACL could be objectified. This could be performed with an instrument, the KT-1000TM arthrometer (MEDmetric Corp, San Diego, CA) and by physical examination with the Lachman test and the pivot shift.51-53 The results in stability of the ACL were comparable in various studies. In current literature, there was no clinical difference described in stability measured between the different fixation techniques.54-60

10
The movement of the tendon graft in the bone tunnel, the ‘bungy-cord’ effect and the ‘windshield-wiper’ effect, may cause widening of the osseous tunnel.61 Figure 4 shows the possible mechanisms of tunnel widening. However, the exact cause of widening of the osseous tunnel of the femur remains unclear. Most authors favor a multifactorial biomechanical and biological process.62 The clinical significance of this tunnelwidening is not yet fully cleared out. It has not been correlated with short-term clinical outcome. However, there has been concern that widening of the tunnels could pose clinical problems by delaying incorporation of the soft tissue graft into bone, decreasing graft stability, or by causing difficulty with future revision surgery.63
Figure 4. A possible cause of tunnelwidening: the ‘bungy-cord’(4a) and ‘windshield-wiper’(4b) effect of movement of the hamstring graft in the femoral tunnel.
61
Various studies have been described about the influence of the femoral fixation technique to tunnelwidening. In a prospective randomized computed tomography-based study, Sabat et al. compared an extracortical suspension method (Endobutton®) with a transfemoral cross-pin technique (Transfix®). They found significantly more tunnelwidening in the Endobutton® variant.62 Fauno and Kaalund et al. also compared Endobutton® with Transfix® and described similar results.64 Other studies performed a comparable study to the differences between the interference screw and the Endobutton®. These studies found considerably more tunnel widening in the grafts fixed with the Endobutton® as well.55,60 However in all these studies there was no correlation between tunnelwidening and the clinical scores or laxity measurements.55,60,64 In a meta-analysis, eight different studies were shown that investigated whether there is any difference in patient-reported outcome between various different fixation methods as measured by the International Knee Documentation Committee (IKDC) score.43 They did not find femoral fixation influenced postoperative IKDC score. However, seven of the eight studies compared the interference screw with another method of femoral fixation. Yet, in various studies is shown that on the aspect of biomechanical stability, the interference screw is inferior to suspensory fixation and transfemoral fixation with crosspins.44,50 Only one of these eight studies compared the functional outcome of a suspensory fixation technique (Endobutton®) with a cortico-cancellous transfemoral cross-pin (TransFix®).64 This study was a prospective randomized controlled trial with 87 patients who were assessed at 1-year follow-up. No significant difference was found on the functional outcome (measured by the Lysholm score and IKDC).

11
In another study, TransFix® and Endobutton® are being compared on the functional outcome and other aspects.56 There was no difference in functional outcome after 1 year follow-up, as deficits in hamstring-quadriceps muscle strength, motor coordination and proprioception were still found in both groups. They recommended that long-term follow-up and rehabilitation including neuromuscular exercises should be continued for longer than one year after ACL reconstruction. Another prospective randomized study concluded there was no statistically different clinical outcome between Endobutton® (n=13) and TransFix® (n=16) measured by the IKDC.65 They measured after 1-year and 2-year follow-up. This study also noticed an indication that additional procedures were required more frequently in the TransFix® group.
Surgical procedures being compared in this specific study The patient is in supine position with his or her thigh secured in a holder with either a general or spinal block anesthetic. A tourniquet is applied and used as needed to control bleeding.46 An oblique incision two finger-breadths below the medial joint-line over the pes anserinus tendons was used to harvest the tendons of the m. semitendinosus and m. gracilis, as they are used as an autologous graft. An incision above the pes anserinus was used to elevate the insertion site of the tendons. Tendons were identified and harvested with a tendon stripper and all muscle remnants were removed. The grafts were tensioned with 15 lbs for at least 5 minutes on the table with a graft-tensioning system.56 Figure 5 shows the position of the portals. An anterolateral introduction of the arthroscope is performed. An anteromedial working portal is created and a cannula is inserted proximal-medial or proximal-lateral. The knee is arthroscopically inspected to determine the status of the joint: suprapattelar, pattelar-femoral, medial and lateral compartiment of the meniscus and the cruciate ligaments. Figure 6 shows the arthroscopic view of the knee. Tibial and femoral tunnels were drilled.
Figure 5: three-portal arthroscopy of the knee. The arthroscope on the anterolateral side, the cannula on the proximal-lateral side and the arthroscopic instrument directly medial of the patella tendon.
56

12
Figure 6 (a-c) Knee joint arthroscopy. 6a: distal view into the femoropatellar joint, 6b: medial view of the free inner edge of the lateral meniscus with the retractor depressing the anterior part of the meniscus, 6c: anterolateral view of the distal part of the anterior cruciate ligament (ACL), which is drawn medially by a retractor.
66
TransFix®
The graft is pulled into the osseous tibial and femoral tunnel and is femorally fixated by the TransFix® device (as in shown in figure 7). Femoral fixation strength is tested by flexing the knee 130 degrees. The surgeon checks if the TransFix® device is not sticking out of the lateral femurcondyl. Now that the graft is properly fixated, the tendons are secured in the tibia by a bio-interference screw. Stabilization and movement tests are being performed and show a stabile knee joint with a normal range of motion.
Figure 7. Femoral fixation of the ACL-graft by the TransFix
®-technique (transfemoral fixation with cross-pins or cortico-
cancellous fixation.67
Endobutton® After creating the osseous tunnels in the tibia and femur, the prepared grafts were embedded intra-articularly through the tibial tunnel and fixed using an Endobutton® loop at the femoral site. The Endobutton® is a ligament suspensory device that works as a tissue anchor by locking itself against the cortex of the femoral condyle (as seen in figure 8).68
The graft is fixated with a bio-absorbable screw at tibial site. Testing of stabilization, fixation strength and range of motion is performed as described above.

13
8a 8b Figure 8 (a,b) 8a: Endobutton
® technique (suspensory or extracortical fixation)of femoral fixation of the ACL-graft
67 8b: the
Endobutton®
works as a tissue anchor by locking itself extracortical of the femoral condyle.68
Purpose and hypotheses of this specific study In current literature, there is not much research to be found on the difference of clinical outcome and activity of patients on longer term between femoral fixation of the ACL-graft by a transfemoral cross-pin and an extracortical suspensory fixation. The main purpose of this study is to compare these two different methods of femoral fixation of the ACL-graft in ACL-reconstruction. In this study, the specific surgical procedures are the Endobutton®
(Smith & Nephew, Andover, MA, USA) and the Transfix® (Arthrex Inc., Naples, FL, USA). The
two procedures will be compared on various aspects in patients who have been operated in the year 2010, thus the follow-up will be 2-3 years. The primary outcome of this study is the patient-reported outcome, measured by the Knee Injury and Osteoarthritis Outcome Score (KOOS). As secondary outcome, the patient-reported outcome is determined by using the International Knee Documentation Committee (IKDC) subjective knee evaluation form, the Lysholm knee score and the Tegner Activity Scale (TAS). Furthermore, possible differences in the number of required additional surgical procedures, in the duration of the primary ACL-reconstruction, in the contentment of the patients and the possible correlation of these factors with the patient-reported outcome was tested as well. Besides this, patient characteristics (gender/age/BMI) were analyzed if they possibly were a factor of influence on the results. Because three different surgeons did all the ACL-reconstructions in the year 2010, the influence of the surgeon on the outcomes was objectified and analyzed as well. The hypothesis of this study is that there is no difference between the Endobutton® and the Transfix® procedure in patient-related outcome of patients with 2-3 year follow-up. It is also hypothesized that there will be no difference between Endobutton® and TransFix® in the duration of the surgical procedure, the number of additional procedures that are required and rate contentment of patients. It is expected that these factors could not be correlated to patient-related outcome as well. Patient characteristics are not considered as factors of influence on the patient-related outcome. Neither are the results expected to be dependent on the individual surgeon.

14
Patients and Methods
Study design The study design is a single-centre retrospective cohort study with a 2-3 year follow-up of patients who have had an ACL-reconstruction. The reconstruction was performed in 2010 by one of the three experienced ACL-surgeons of the Isala Klinieken in Zwolle, the Netherlands. All the ACL-grafts were autologous hamstring-grafts, which were femoral fixated by a transfemoral corticocancellous fixation implant (Transfix®) or an extracortical suspensory fixation (Endobutton®). Patients were contacted by telephone and were requested to participate in this study. If they were willing to take part of this study, they subsequently received the questionnaires by e-mail. Patient characteristics were withdrawn from their digital hospital file. This study is approved by the Medical Ethical Committee (METC) of the Isala Klinieken in Zwolle, the Netherlands. (Appendix I)
Patients The inclusion of this study took place in a period of 10 weeks. In total, 112 patients were included. Patients aged between 18 and 55 and who have had a primary ACL-reconstruction in the Isala Klinieken in Zwolle in 2010 were eligible for inclusion in the present study. They should have had an ACL-reconstruction by the Endobutton® or Transfix® fixation technique. All patients have had their ACL-surgery after the acute phase since their injury. Excluded from this study were patients who have had one of the following situations at the same knee as the primary ACL-reconstruction in 2010:
a (multi) ligamentary reconstruction before 2010
a (sub)total meniscectomy
a (total or hemi) knee-arthroplasty
a fracture of the tibia or femur at the trauma of ACL-injury
immobilizing neurological or systemic pathology All patients got recruited by phone and subsequently were sent an e-mail with the questionnaires. Participation in this study was completely voluntary. The patients were reminded by an extra notification by email if they had not filled in the questionnaires. In the year 2010, 168 patients have had an ACL-reconstruction. From these 168 patients, 17 subjects were excluded: seven patients have had a (sub) total meniscectomy, seven patients had a revision ACL-reconstruction in 2010, two patients were excluded because of their age at the time of inclusion (<18 or >55 years old) and one patient has had a hemi-prosthesis of the knee between 2010 and the time of inclusion. In total, 135 patients were reached by phone. Two patients did not want to participate in this study. The reason for not participating was not reported. From the 133 patients who received the e-mail with questionnaires, 112 patients activated and filled in the questionnaires. Figure 9 shows a schematic view of the inclusion process.

15
Figure 9. Algorithm of the inclusion process.
The population of this study consists of 65 men and 47 women. In the Endobutton® group 53 patients (47.32%) are included and in the TransFix® group 59 patients (52.68%) are included. Demographic data is schematically shown in table 2. The population is considered relatively homogenic with regard to age and BMI. With regard to gender, a relatively high percentage of men (64.41%) is included in the TransFix® group. The mean follow-up after surgery of the 112 patients is 2 year and 288 days.
Endobutton®
n = 53
TransFix®
n = 59
Total n = 112
Gender: Men Women Age Median (Q1-Q3) Min-Max BMI (mean ± sd)
n = 27 (50.94%) n = 26 (49.06%)
33 (24-45)
18-51 24.88 ± 3.94
n = 38 (64.41%) n = 21 (35.59%)
31 (23-40)
18-55 24.09 ± 3.85
n = 65 n = 47
Table 2. Demographic data of study population. Number and percentage of different genders, median age with first quartile (Q1) - third quartile (Q3) and minimum-maximum. Mean BMI (body mass index) with standard deviation is shown per group.
ACL-reconstruction in 2010: n = 168
Excluded patients: n = 17 - (sub) total meniscectomy (n = 7) - Revision surgery (n = 7) - Age (n = 2) - (hemi)prosthesis of knee (n = 1)
Included: n = 149
Patients reached by phone: n = 135
Patients did not want to participate: n = 2
Patients that activated questionnaires: n = 112

16
Questionnaires
Knee Injury and Osteoarthritis Outcome Score (KOOS) (Appendix II)
The KOOS questionnaire was developed by Roos et al in 1998.69 Main purpose of this evaluation form is to assess short- and long-term patient-relevant outcomes following knee injury.70 Content and scoring. The KOOS is self-administered and assesses five outcomes: Pain, Symptoms, Activities of daily living, Sport and recreation function and Knee-related quality of life. These five outcomes are scored separately: 9 questions related to pain; 7 questions related to symptoms; 17 questions related to activities of daily life function; 5 questions related to sport and recreation function; and 4 questions about knee-related quality of life. All items could be scored from 0 to 4, and each of the five outcome scores are calculated as the sum of the items included. Scores were then transformed to a 0-100 scale, with 0 representing extreme knee problems and 100 representing no knee problems. Scores between 0 and 100 represent the percentage of total possible score achieved. Reliability. The reliability of the questionnaire was considered to be good.71 Validity: In multiple studies is reported that the KOOS strongly correlates with subscales of the Short Form-36 (SF-36) that measures similar constructs, but less strongly with SF-36 subscales that measure mental health.70 Translation. The questionnaire was translated to Dutch by de Groot et al. in 2008.71 The Dutch translation of the KOOS is validated and recommended in the Dutch guideline of ACL-lesions as a measure of functional outcome.3,11
International Knee Documentation Committee (IKDC) subjective knee evaluation form (Appendix III)
Irrgang et al. developed the definitive version of the IKDC Subjective Knee Evaluation Form 2001.72 The purpose of the IKDC is to detect improvement or deterioration in symptoms, function, and sports activities due to knee impairment.70 Evidence based on item-response theory, indicates that the function of this instrument is the same for patients with a variety of knee problems, including ligament and meniscal injuries, articular cartilage lesions, arthritis, and patellofemoral problems. Thus, the IKDC Subjective Knee Form can be used to reliably and validly measure outcome for patients with a variety of knee problems and allows for comparison of the effect of different knee problems on patient’s symptoms, function, and sports activity.72 Content and scoring. The questionnaire is based on three outcomes. The first outcome is symptoms, including pain, stiffness, swelling, locking/catching and giving way. The second outcome is sports and daily activities and the third outcome is current knee function and knee function prior to knee injury. The IKDC consists of 18 items (7 items for symptoms, 1 item for sport participation, 9 items for daily activities, and 1 item for current knee function). The response to each item is scored using an ordinal method (i.e., 0 for responses that represent lowest level of function or the highest level of symptoms). Scores for each item are summed to give a total score, which could be then transformed to a 0-100 scale.70 Reliability. Internal consistency of the IKDC is adequate for patients with knee injuries and mixed knee pathologies.70,73 Validity. The IKDC score was highly correlated with other knee-scores.70,73 Translation. The questionnaire is translated by Haverkamp et al. in 2006 and is recommended in the Dutch guideline of ACL-lesions as a measure of functional outcome.3,11,73

17
Lysholm Knee Scoring Scale (Appendix IV)
The Lysholm Knee Scoring Scale is developed in 1982 and revised in 1985.12,47 The purpose of this questionnaire is to evaluate outcomes of knee ligament surgery, particularly symptoms of instability. Content and scoring. The revised Lysholm Knee Scoring Scale includes 8 items: limp, support, locking, instability, pain, swelling, stair climbing and squatting. Each item is scored using individual scoring scales. The total score is the sum of each response to the 8 items, of a possible score of 100, where 100 indicates no symptoms or disability. Scores are categorized as excellent (95–100), good (84 –94), fair (65– 83), and poor (<64). Reliability. Reliability of the Lysholm Score is adequate for use in groups with knee injuries in general, but is less than adequate for groups with mixed knee pathologies.75 Validity. Multiple studies have reported convergent validity for the Lysholm score, finding significant correlations with various other tests.70 Translation. The questionnaire is translated, but is not validated in Dutch.3,11
Tegner Activity Scale (TAS) (Appendix V)
The Tegner Activity Scale (TAS) is developed to complement the Lysholm Scale and is originally intended for use in patients with anterior cruciate ligament injury to provide a standardized method of grading work and sporting activities.74 Content and scoring. The TAS consists out of graduated list with 11 activity levels of daily living, competitive sports and recreation. Patients select the level of participation that best describes their current level of activity.70 A score of 0 represents “sick leave or disability pension because of knee problems,” whereas a score of 10 corresponds to participation in national and international elite competitive sports.70,74 Reliability. The reliability of the TAS for groups was considered acceptable.75 Validity. The TAS covers a wide variety of activity levels that may be applicable to patients with ACL and other knee injuries. At construct validity value, significant correlations have been shown with the other knee scores (e.g. IKDC).70 Translation: The TAS is translated to Dutch, but the translation is not validated. The Dutch Orthopaedic Association approves usage of the TAS, as it is an internationally valid and valuable activity score in ACL-injury.3,11
Contentment patients after the ACL-reconstruction
The contentment of patients is obtained by asking every participant of this study the following question: “Would you choose for the same operation again?”. Possible answers are ‘Yes’ or ‘No’. This question is used as an indication.

18
Statistical analysis All statistical analyses were performed using IBM SPSS Statistics 20. A power analysis was not performed, due to the retrospective design of this study. Discrete variables are summarised and described in frequencies and percentages. Continuous data were analyzed and described as number of observations and mean scores with standard deviations. If the continuous data were not normally distributed, median scores were shown, with first- and third quartile or minimum and maximum scores. To determine whether data were normally distributed or not, a histogram was assessed and specific tests as the Kolmogorov-Smirnoff test or the Shapiro-Wilk test were performed. If the obtained data of the questionnaires were not normally distributed, the Mann-Whitney U test was performed to test the null hypothesis on the scores between the two different groups (TransFix® and Endobutton®). The Mann-Whitney U test is a non-parametric test and has a greater efficiency than the t-test on non-normal distributions. The student-t test was performed if data were normally distributed. These tests were also used in analyzing the influence of gender, the impact of re-operations on the patient-reported outcome. To objectify the possible correlation between continuous data (not normally distributed scores derived from the questionnaires) and nominal or ordinal data, the Spearman’s rank correlation was performed. This test is a nonparametric measure of statistical dependence between two variables. Correlation was objectified of the patient-related outcome with age, body mass index, duration of the surgical procedure and the individual surgeon. Fisher’s exact test was used to test the difference between two proportions (e.g. the number of re-surgeries per group and the number of content patients). In the results of this study, p-values of <0.05 were considered statistically significant.

19
Results
Primary outcome: the Knee Injury and Osteoarthritis Outcome Score (KOOS) There is no significant difference in patient-relevant outcome between Endobutton® and TransFix® on the KOOS-questionnaire. As the data is not normally distributed, the Mann-Whitney U test was performed on the difference between Endobutton® and TransFix®. The median scores on the different subscales of the KOOS are shown in table 3. Table 3. Median scores of the different subscales of the KOOS in the Endobutton
®- and TransFix
®-group (with first- and third
quartile). P-values are shown (Abbreviations: ADL = Activities of Daily Living, QOL = Quality of Life).
Secondary outcomes
Questionnaires: IKDC, Lysholm and Tegner There is no significant difference to be found between patients with Endobutton® and patients with TransFix® in the scores of the IKDC, the Lysholm knee score and the Tegner Activity Scale (p-value >0.05). The Mann-Withney U test is performed and p-values are shown in table 4. These results indicate there is no significant difference in symptoms, function and level of (work and sport) activities between Endobutton® and TransFix® in patients, 2-3 years after the primary ACL-reconstruction.
Endobutton® (n = 53) TransFix® (n = 59) p-value
IKDC Median (Q1-Q3)
Lysholm Median (Q1-Q3) Tegner
Median (Q1-Q3)
70.74 (62.77-75)
83.5 (10-93.5)
6 (4-7)
69.68 (60.64-77.66)
89 (75-96)
5 (4-7)
0.825
0.131
0.316
Table 4. Median scores on the IKDC, Lysholm Knee Scoring Scale and Tegner. P-values are shown. Medians are given with first quartile (Q1) and third quartile (Q3).
Endobutton® (n = 53) TransFix® (n = 59) p-value
KOOS Pain Symptoms ADL Sport/Recreation QOL
93.06 (62.77-75) 85.71 (71.43-92.86) 98.68 (96.71-100) 80 (62.5-95) 75 (62.5-87.5)
94.44 (86.11-100) 89.29 (71.43-96.43) 100 (94.74-100) 90 (70-100) 75 (56.25-87.5)
0.304 0.379 0.384 0.060 0.856

Gender There are no significant differences between men and women in the TransFix group. Between Endobutton® and TransFix® there are no differences in patient-reported outcome within the gender ‘men’ or within the gender ‘women’. The Mann-Whitney U test was performed on all the subscales of the KOOS, the IKDC, the Lysholm and the Tegner and differences were not significant. Within the Endobutton® group, there is a significant difference between men and women in the KOOS questionnaire on the subscale Activities of Daily living (p-value 0.041). Men score higher than women, thus have a better outcome on this subscale. In the Endobutton® group, there is a near significant difference (p-value 0.051) between men and women on the subscale Symptoms of the KOOS. Women score higher, which indicates lower presence of ‘Symptoms’ in women. Scores are shown in table 5. No differences between men and women were found in the Endobutton® group on other subscales of the KOOS, the IKDC, the Lysholm and the Tegner. These results indicate that gender does not influence the outcome in patients after ACL-reconstruction with a mean follow-up of 2 year and 288 days. With the exception of two subscales of the KOOS in the Endobutton® group, since the results indicates that men perform better than women on the activities of daily living and women have lower presence of symptoms than men.
Table 5: Median scores on the KOOS-Activities of Daily living and KOOS-symptoms of men and women in the Endobutton®
-group. P-values are shown. Medians are given with first quartile (Q1) and third quartile (Q3) and minimal/maximal scores (Min-max).
Age Of all the analyzed patients in the study population (n=112), there is no correlation between age and patient-reported outcome. Correlations between age and functional outcome are being objectified with the Spearman Rank Test on the scores of the KOOS, IKDC, Lysholm and Tegner. In the TransFix® group (n=59), there is no correlation with age and scores as well. In the Endobutton® group (n=53), there only is a significant negative correlation between age and the Tegner score (correlation coefficient -.359, p-value 0.041). Older patients in the Endobutton® group have significant lower scores on the Tegner than younger patients in the Endobutton® group. This indicates that in Endobutton® group, older patients have lower grades of activities in work or sports.
Body Mass Index (BMI) Correlations between BMI and patient-reported outcomes were objectified on all the questionnaires. There is no correlation between BMI and patient-reported outcome after an
Endobutton® Men (n=27) Women (n=26) p-value
KOOS ADL Median (Q1-Q3) Min-max
KOOS Symptoms Median (Q1-Q3) Min-max
100 (97.37-100)
47.37-100
82.14 (64.29-89.29) 25-100
98.68 (96.05-99.01)
47.37-100
89.29 (82.14-97.32) 50-100
0.047
0.051

21
ACL-reconstruction. Neither is there a correlation found in the Endobutton®- or in the TransFix® group. The mean BMI of the study population was 24.73 with a standard deviation of 3,88.
Duration of surgery There is no difference in duration of the surgical procedure between the Endobutton® and TransFix® femoral fixations (p-value 0.482) in ACL-reconstructions. The median duration of an ACL-reconstruction with Endobutton® was 62 minutes (first- and third quartile 55-69.5) and in TransFix® 61 minutes (Q1-Q3: 54-67). Duration of the surgery was not correlated with the scores on the questionnaires (Spearman correlation coefficient). This indicates that the duration of the procedure does not influence patient-reported outcome.
Required additional surgical procedures Of all the patients included (n=112), 18 re-operations were performed on 16 different patients. In the Endobutton® group, 4 of the 53 patients (7.55%) have had one re-operation since 2010. Among the 59 patients in the TransFix® group, 12 patients (20.34%) have had a re-operation since 2010. In the TransFix® group, there are 10 patients (16.95%) that have one re-operation and 2 patients (3.68%) that have two re-operations. The difference of number of re-surgeries between Endobutton® and TransFix® is not considered to be significant (Fisher’s exact probability test, p-value 0.121). Primary indications for a re-operation are shown in table 6.
Table 6. Primary indication for re-operation after an ACL-reconstruction in 2010 * wound abscess
All the additional required surgical procedures in the Endobutton® group (n=4) were performed arthroscopically. The one patient with indication ‘Pain’ in the Endobutton® group had complaints of small pieces of the resorbable tibia screw inside the joint, which were arthroscopically removed. The one patient with complaints of laxity of the ACL underwent a ‘shrinkage-procedure’ of the neo-ACL. Patients with impingement of the ACL received a ‘Notchplasty’, which is a surgical procedure performed to reshape the intercondylar of the femur in case of impingement. Meniscal lesions were the reason for partial meniscectomies.
Primary indication for a re-operation after ACL-reconstruction
Endobutton® (n = 53) One re-operation: n = 4 Two re-operations: n = 0
TransFix® (n =59) One re-operation: n = 10 Two re-operations: n = 2
First surgery (n =16) - Pain - Re-rupture - Laxity of ACL - Impingement - (Suspected) meniscus lesion - Other*
Second surgery (n=2)
- Pain - Re-rupture
1
0 1 1 1 0
0 0
5 2 0 2 2 1
1 1

22
In the TransFix® group 7 patients (11.86%) have had an arthroscopic intervention and 5 patients (8.47%) an open approach of their knee (table 6). The 5 open procedures consisted of debridement of screws (2 tibial screws and 2 TransFix®-screws in the femur) and drainage of an abscess. In total, there were 3 revisions of a ruptured neo-ACL in the TransFix® group. The reasons for the second re-operation were different in the two patients. In one patient, the primary indication of surgery was pain, based on fibrosis anterolateral and a cyclops of the neo-ACL. In the first re-operation of this patient, the femur screw was removed because of pain. The other patient with a second re-operation had complaints of laxity, based on a failed ACL-reconstruction. That is why an ACL-reconstruction was performed. In the first re-operation of this patient, there were complaints of impingement based on a cyclops of the neo-ACL.
There is a significant difference in presence of symptoms and in functional outcome of patients who did have a re-operation and patients who did not. The Mann-Whitney U test was performed and p-values were significant (p-value <0.05) on every subscale of the KOOS, the IKDC, the Lysholm and the Tegner as shown in table 7. Patients who did not have a re-operation scored significantly higher on all the questionnaires and thereby have a better patient-reported outcome.
No re-operation
(n=96) Re-operation
(n =16) p-value
KOOS Pain Symptoms ADL Sport/Recreation QOL IKDC Lysholm Tegner
94.44 (88,89-100) 89.29 (78.57-96.43) 100 (97.37-100) 90 (70-100) 75 (62.5-87.5) 71.28 (63.03-76.60) 85.50 (74.25-95) 6 (4-7)
84.72 (58.33-93.75) 62.50 (50.89-89.29) 94.74 (63.49-100) 72.5 (31.25-88.75) 43.75 (32.81-71.88) 57.45 (39.36-68.88) 69 (44-87.75) 4 (2-6)
.001 .002 .012 .023 .000 .005 .007 .007
Table 7. Median scores of the patients who did and who did not have a re-operation. With first quartile (Q1) and third quartile (Q3). P-values are shown.
Correlation with the individual surgeon There is no correlation between surgeon and patient-reported outcome. Spearman's rho showed no significant correlation of the factor ‘surgeon’ with any of the questionnaires (p-value >0.05). Data is shown in table 8.
Surgeon N total EB (n) TF (n) N satisfied
patients One re-operation
(n = patients) Two re-operations
(n = patients)
Median duration
(min-max)
A
B
C
45
10
59
43
10
0
2
0
59
42
10
55
4
0
10
0
0
2
60 (45-107)
70 (56-90)
61 (41-92)
Table 8. Data of the different surgeons (A,B,C). Total number of ACL-reconstructions performed (N total), number of operations with Endobutton
® (EB) and TransFix
® (TF), number of satisfied patients, the account of re-operations per
surgeon who performed the primary reconstruction and median duration in minutes are shown.

23
Contentment after the ACL-reconstruction To analyse the contentment of the patients, the following question was asked: ‘Would you choose for the same surgical procedure again?’. Possible answers were ‘Yes’ or ‘No’. Of a total of 112 patients, seven patients answered ‘No’ (6.25%). Those were three patients (5.70%) of the Endobutton® group (n=53) and four patients (6.80%) of the TransFix® group (n=59). One of the four patients in the TransFix® group has had a re-operation of his or her knee; the other six patients did not. There is no significant difference in the number of content of patients with Endobutton® and patients with TransFix ® (Fisher’s exact test p-value 1.000).

24
Discussion and conclusion This single-centre retrospective study investigated the patient-reported outcome after an ACL-reconstruction with a mean follow-up of 2 year and 288 days (± 105). A comparison is performed between two types of femoral fixation of the ACL-graft: Endobutton® and TransFix®. As hypothesized, there was no relevant difference in patient-reported outcome and patient characteristics (gender, age, BMI) did not influence the patient-reported outcome. As expected, there was no significant difference in duration of the surgical procedure and in contentment-rate of patients. These factors could also not be correlated to the patient-reported outcome. In the TransFix® group the percentage of patients with additional required surgeries was clearly higher than in the Endobutton® group (20.34% versus 7.55%), but differences were not considered significant (p-value 0.121). Patients who underwent a re-operation had a significantly lower patient-report outcome (p-value <0.05).
Review of current literature This study focused on two variants of surgical intervention of an ACL-injury. However, there is some evidence in current literature that conservative treatment alone, can also result in a satisfactory outcome.76
In a systemic review is shown that there is insufficient evidence from randomized trials comparing surgical- with conservative treatment of ACL ruptures to inform current practice. Nevertheless, there is some limited evidence from two outdated, heterogeneous and poor quality trials that surgical intervention does improve knee stability more efficient than conservative treatment.77,78 As these studies have been performed in the early 1980s, these results are less relevant and less valuable. Surgical procedures have been changed and improved in the past decades. Another benefit of surgical intervention is an ACL-reconstruction could decrease the further damaging of the menisci and cartilage. 20
Thereby is it important to determine the patient his care demands and to individualize the choice for the right therapy to attain the best outcome. In this decision, the physician and patient should define the present quality of life of the patient, the level of current activities, the functional limitations, and her or his fear of recurrence.3 In current literature, there are only three studies to be found which also compare the outcome of Endobutton® with TransFix®. Fauno and Kaalund performed a prospective randomized study to compare the fixation methods on tunnel widening and IKDC-scores.64 They included 87 patients and assessed them 1-year postoperative. Considerably more tunnel widening was found in the Endobutton® group, but there was no correlation between tunnel widening and clinical outcome. Thus no difference between Endobutton® and TransFix® in the IKDC-scores could be found. Another study, performed by Yosmaoğlu et al., is a prospective study in which 40 patients after an ACL-reconstruction were being compared 1 year postoperative on functional outcome (lower extremity muscle strength, joint position sense and knee stability).56 There was no statistically difference to be found between Endobutton® (n=20) and TransFix® (n=20), 1 year after surgery. Also in the study of Price et al. there are no differences in clinical outcome between these two femoral fixation methods.65

25
Results analyzed in the light of current literature The results of the patient-related outcome in this study are comparable with other studies comparing methods of femoral fixation of the ACL-graft.53-60,84 As hypothesized, there are no major differences in the patient-reported outcome between Endobutton® and TransFix®. On the subscale ‘Sport and recreation’ of the KOOS-questionnaire, there is a near significant difference (p-value 0.06) between the two methods. Patients with TransFix® have a slightly higher score, which indicates a better performance on this subscale. The main reason for this near significant difference could not be found. A factor of influence to the results could be the small number of questions in this subscale. This subscale consists of only 5 questions. Compared to the scales ‘Symptoms’, ‘Pain’ and ‘Activities of daily living’ (with respectively 7, 9 and 17 questions), this number is rather small. However, the subscales of the KOOS are validated to be used individually. There are a few single subscales where significant differences could be found. Conform current literature, the results in this study also indicate that gender does not influence results of the clinical outcome. As hypothesized, there was no difference between men with Endobutton® or TransFix® and between women with Endobutton® or TransFix®. However, within the Endobutton® group there is a minor difference (p-value 0.047) between men and women on the ‘Activities of daily living’. Men score higher. Also within the Endobutton® group, there is a near significant difference (p-value 0.051) in subscale ‘Symptoms’ between different genders: scores indicate women have less symptoms in this group. Both differences are minor and only showing on one particular subscale of one questionnaire. These differences could not be found in the other questionnaires that are being used in this study. A larger study population and more consistent results are needed to acknowledge the clinical relevance of these differences. As expected, there were no correlation between age and patient-reported outcome measured by all the questionnaires (KOOS, IKDC, Lysholm and Tegner) after an ACL-reconstruction. Also in the TransFix® group, no correlation could be found. In the Endobutton® group, there only was a negative correlation found on the Tegner, which indicates that young patients with an Endobutton® fixation have a higher grade of activities in sports or work compared to older patients. It is remarkable that this result indicates a difference between the fixation methods on this subject. This result could not be declared, as no significant correlation with age could be found on the other questionnaires and age is relatively equally distributed in both groups. The clinical relevance of this is considered low, as these differences are only found on the Tegner Activity Scale. In literature, lower patient-reported outcome after an ACL-reconstruction is seen in patients with obesity.25 A low outcome in patients with a BMI above 30 is described. In our study, there is no significant correlation between BMI and outcome as was hypothesized. In the population of this study, the BMI is normally distributed with a low percentage of subjects with a BMI above 30 (5.36%). Only 6 of the 112 patients included were having a BMI above 30. No negative correlation could be found in the patients with a BMI above 30. A larger study population with a higher frequency of patients with a BMI above 30 should be performed to confirm significant correlation of BMI with patient-reported outcome.

26
Results of our study also show that re-operations are relatively frequently needed after an ACL-reconstruction and there is a difference between the two methods. There is only one other study to be found in current literature that compares Endobutton® with TransFix® on the number of needed required additional procedures after an ACL-reconstruction.65 In this prospective trial, 29 patients were included and randomized into either Endobutton® (n=13) or into TransFix® (n=16). Their results concur with this present study, as in their study 4 patients (25%) with TransFix® had interaoperative complications and 4 patients (25%) had postoperative complications. In the Endobutton® group only 2 patients (15.38%) required a re-operation. Furthermore, there is a remarkable difference between Endobutton® and TransFix® on this subject. There is a strong indication that the chance of a re-operation after TransFix® is a lot higher than after an ACL-reconstruction with Endobutton®. In this specific study, 20.34% of the patients required a re-operation in the TransFix® group. Compared to the 7.55% in the Endobutton® group, this is a relatively large difference. The difference in number of re-surgeries is not considered significant, but there is a strong indication that ACL-fixation with TransFix® leads to more re-surgeries. As numbers are small, but concur between two studies, this should be further investigated in a larger, randomized prospective trial. Causation of the more required additional procedures should be further analyzed. However, it is described that the use of the TransFix®-method has a specific iatrogenic risk which may contribute to the number of re-surgeries. This fixation method may lead to a lesion of the lateral collateral ligament (LCL) of the knee. This risk has been analyzed and can be reduced with a correct depth of the tunnel and a maximum knee flexion during the surgery, in order to move the LCL insertion.79 Exact numbers of this risk are not described in literature, but the extracortical fixation (Endobutton®) does not have the disadvantage of this iatrogenic risk.80
The clinical relevance of number of additional required surgical procedures is high, as there is a significant difference in patient-reported outcome on all of the used questionnaires of patients who did have a re-operation and patients who did not. Patients who did not have a re-operation, score significantly higher on all the questionnaires and thereby have a better patient-reported outcome. A larger trial is necessary to confirm the relevance of our results, because our groups differ strongly in number. Only 16 patients (14.29%) with re-surgeries have been included versus 96 patients (85.71%) without re-surgeries. As was hypothesized, the rate of contentment among the study population is similar in Endobutton® and in TransFix®. However, the difference in number of re-surgeries, did not reflect in the results about the contentment after the ACL-reconstruction.
Possible confounding factors of this study A probable confounding factor of this study is the dependency on the skills of the individual surgeon. In current literature is found that the clinical outcome and success of an ACL-reconstruction is strongly dependent on the skills of the surgeon.30 Besides this, technical failures are the most common cause of failure of the ACL and thereby the reason for revision surgery.31 This study evaluates the follow-up of patients who have had surgery by one of the three orthopaedic surgeons who performed ACL-reconstructions in the Isala

27
Klinieken in 2010. Each of these surgeons perform particularly one different technique of femoral fixation (as is shown in table 8). That is why the work of the individual surgeon, may influence our data. However, there is no significant correlation found between the surgeon and patient-reported outcome in this study (Spearman Rank test, p-value >0.05). Nevertheless, it remains unclear what the influence of this factor is on the results of this study. With the used criteria of exclusion in this study, there is attempt to minimize the influence of other pathologies on the results as a bias. That is the reason why subjects with a (multi) ligamentary reconstruction before 2010, a history of (sub-) total meniscectomy before or after 2010, an ipsilateral (total or hemi) knee-arthroplasty or fracture of the tibia or femur at the trauma of ACL-injury were excluded. Furthermore, patients who were immobilized because of neurological or systemic pathology were excluded as well. The patients with an ACL-injury in 2010 had the possibility to choose for their preferred surgeon. The individual surgeon made the choice for the used femoral fixation method. Thus, there was no selection bias in this study, which could have been a possible confounding factor and thereby influencing the results. As described earlier, all subjects of this study were operated in the year 2010. As a consequence, follow-up differs in patients between a minimum of 2.25 year and a maximum of 3.23 year at the time of inclusion. This means that difference in duration of follow-up could be a confounding factor, possibly influencing the results. However, there is no correlation found between the length of follow-up and patient-reported outcome (Spearman Rank test p>0.05). This study did not compare the difference in tunnel widening between Endobutton® and TransFix®. In literature is found that extracortical suspension of the ACL-graft (e.g. Endobutton®) gives more widening of the osseous tunnel than an interference screw55,60 or than an extracortical method of fixation (Transfix®).62,64 As described earlier, the clinical significance of tunnel widening is not fully cleared out. There has been concern that widening of the tunnels could pose clinical problems by delaying incorporation of the soft tissue graft into bone, decreasing graft stability, or by causing difficulty with future revision surgery.63 Nevertheless, in literature is found that there is no correlation of tunnel widening and clinical outcome on short term. Therefore, longer term follow-up is recommended.55,60,64 The method of tibial fixation of the ACL-graft is not discussed in this study. In literature is described that failure of the graft in ACL-reconstructions may be dependent on the combination of femoral and tibial fixation, rather than on either fixation alone.81 If the tibial fixation is stronger than the femoral fixation, the femoral fixation may actually be the weak point in the construction. All ACL-reconstructions in this study are performed with a tibial fixation by an interference screw. This method of tibial fixation is reportedly associated with ultimate failure strength, greater than what the native ACL is subjected during most activities of daily living. However, graft failure can occur via slippage of the graft.82 Since all included subjects have had tibial fixation by the same method, it does not influence the results in the comparison of femoral fixation between Endobutton® and TransFix®.

28
Nevertheless, the method of tibial fixation may have effect on the overall outcome of the ACL-reconstruction in this study population. There is no clear consensus in literature about the optimal timing of an ACL-reconstruction. It is known that in the acute phase, when there is still synovial reaction and full extension is not possible, ACL reconstruction is contra-indicated.28 Patients in this study were not operated in this during the acute phase after their ACL-injury, so this could not be a bias is this study. Another possible confounding factor is the distribution of patient characteristics in the two groups. The Endobutton® and TransFix® are relatively homogenic with regard to age and BMI. Within the TransFix® group, a relatively high percentage of men (64.41%, n=38) is included, which could be influencing our data. Subjects who did not fill in the questionnaire (n=21) received telephone calls and multiple e-mails were sent to remind them of this study. The reason for not participating is unknown.
Advantages of this study In the Dutch guideline on anterior cruciate ligament injury, the Dutch orthopaedic association recommends how to evaluate the follow-up of patient-related outcome measures of patients with an anterior cruciate ligament injury. They recommend the combination of the Lachman test, pivot shift test and the anterior drawer test as a clinical outcome measurement. Thereby, they advise the use of the IKDC subjective and the KOOS as patient-related outcome measures. They also allege it could be useful tot adopt the Tegner score as an outcome measurement for activity.11 As this study only consists of questionnaires, it is impossible to objectify the status of patients after an ACL-injury with the all measurements that were recommended to evaluate the clinical outcome. On the other hand, the information obtained from the Lachman test, pivot shift and drawer test is less relevant than the opinion and experience of the patient. An advantage of this study is the use of multiple questionnaires. The questionnaires recommended in the guideline, plus the Lysholm knee score, are being used in this study. The Lysholm knee score is added to this study, because it is a test specially designed to evaluate outcomes of knee ligament surgery, particularly symptoms of instability.12 It is noteworthy that the Dutch translation is not validated. A major advantage of this study is that the study population is larger than in all of the other comparable studies that could be found in literature.53-60,64,65
Implications for future research A prospective randomized trial should be performed, ideally with multiple surgeons who are capable of performing both surgical methods. This will amplify the results of found patient-reported outcome, as the performance of the individual surgeon has a lower impact in the results. The focus of further research should be on the number of required re-surgeries after the ACL-reconstruction. Causation of the re-operation should be further investigated. Possible causations could be the iatrogenic risk or irritation of the implanted material (femoral- or tibial screw). The clinical relevance of further research is high, as number of resurgeries is frequent and results indicate these numbers differ between methods. Additionally, results implicate lower patient-reported outcome in patients with required re-

29
surgeries in comparison to patients without additionally needed procedures. The effect of tunnel widening on the long term and effect of the femoral fixation on the tunnel widening is also an aspect that should be investigated.64
Conclusions In conclusion, there are no major differences in the patient-reported outcome between patients with Endobutton® and patients with Transfix® in a study population with 2-3 year follow-up. Data indicated patient characteristics like gender, BMI and age have no clinically relevant influence on the patient-reported outcome after an ACL-reconstruction. Thereby, results did not show an obvious specific femoral fixation method in favour of certain patient characteristics. Our results show a remarkably higher percentage of patients that require an additional surgical procedure after femoral fixation with Transfix®, than after an ACL-reconstruction with Endobutton®. Patient who underwent a re-operation have a significantly lower patient-reported outcome. Taken together, these findings suggest the need for further investigation to the causation and the influence of the femoral fixation method on the number of re-operations.

30
Acknowledgements
First and foremost, I would like to thank my main supervisor Dr. R.G. Zuurmond for his enthusiastic encouragements, critical view and friendly guidance during this study. His critical attitude towards scientific research combined with his competency to express certain issues distinctly, makes him the ideal supervisor of a research project. Advice given by Dr. Mireille Edens has been a great help with the statistical analysis of this study. I also wish to acknowledge the help of David de Jong with the logistic matter of gaining data. I would like to say thanks to all fellow researchers, friends and housemates for their (mostly empirical derived) advices about research during all our coffee breaks and bike-rides. Last but not least, my girlfriend Guusje Teeuwen receives my deepest gratitude and love for her critical view on this manuscript and her unconditional support during this study.

31
Dutch summary Achtergrond. Traumatische letsels van de voorste kruisband (VKB) behoren tot een van de meest voorkomende sportletsels van de knie. Behandeling bestaat uit conservatieve therapie of chirurgische reconstructie. Bij chirurgische VKB-reconstructies is er geen gouden standaard voor de fixatie van het VKB-transplantaat aan het femur. Extracorticale- of transfemorale fixatie hebben beiden goede biomechanische eigenschappen. De stabiliteit is vergelijkbaar en er zijn aanwijzingen dat de functionele uitkomst gelijk is. Het doel van dit retrospectieve cohort onderzoek is het objectiveren en vergelijken van de patiënt gerapporteerde uitkomst na een extracorticale fixatie (Endobutton®) en na een transfemorale fixatie (TransFix®), 2-3 jaar na een VKB-reconstructie. Materiaal en methode. Alle 112 geïncludeerde patiënten ondergingen een VKB-reconstructie in de Isala Klinieken Zwolle in 2010. Femorale fixatie van het VKB-transplantaat was middels Endobutton® (n=53) of TransFix® (n=59). De primaire uitkomstmaat was de patiënt gerapporteerde uitkomst gemeten met de Knee Injury and Osteoarthritis Outcome Score (KOOS). Secundaire uitkomstmaten waren de patiënt gerapporteerde uitkomst gemeten met de International Knee Documentation Committee (IKDC) subjective knee evaluation form, the Lysholm knee score and the Tegner Activity Scale (TAS). Verder werden mogelijke verschillen in de benodigde heroperaties, de duur van de operaties en de tevredenheid van patiënten geobjectiveerd. De mogelijke correlatie van deze factoren met de patiënt gerapporteerde uitkomst werd ook bekeken. Hiernaast werd er gekeken of er correlatie was tussen patiëntkarakteristieken (geslacht/leeftijd/BMI) en de patiënt gerapporteerde uitkomst. Resultaten. De gemiddelde follow-up was 2 jaar en 288 dagen na de VKB-reconstructie. Er was geen significant verschil in patiënt gerapporteerde uitkomst tussen Endobutton® en TransFix® in de KOOS (p-value >0.05). Er werden geen grote verschillen gevonden in de resultaten van de IKDC, Lysholm en TAS. Patiëntkarakteristieken, duur van de operaties en de tevredenheid van patiënten was vergelijkbaar en correleerde niet met de patiënt gerapporteerde uitkomst. Er waren meer heroperaties nodig in de TransFix® groep dan in de Endobutton® groep (respectievelijk 20.34% en 7.55%). De patiënt gerapporteerde uitkomst was significant lager in patiënten die een heroperatie ondergingen. Conclusie. De patiënt gerapporteerde uitkomst bij Endobutton® en TransFix® zijn gelijk na 2-3 jaar follow-up. Verdere resultaten wijzen er op dat het aantal benodigde heroperaties duidelijk hoger is in de TransFix® groep. Gezien de lagere patiënt gerapporteerde uitkomst van patiënten die een heroperatie hebben ondergaan, is verdere analyse hiervan klinisch relevant.

32
Appendices
Appendix I: METC

33
Appendix II: Knee Injury and Osteoarthritis Outcome Score (KOOS)

34

35

36

37
Appendix III: International Knee Documentation Committee (IKDC) subjective knee evaluation form

38

39
Appendix IV: Lysholm Knee Scoring Scale

40
Appendix V: Tegner Activity Scale (TAS)

41
References (1) Drake V, Mitchell. Lower limb, Cruciate ligaments. Gray's Anatomy: Elsevier Inc; 2005. p. 536-537. (2) Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K. Incidence and risk factors for graft rupture and
contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy 2005 Aug;21(8):948-957. (3) DBF Saris, RL Diercks, DE Meuffels, AWFM Fievez, TW Patt, CP van der Hart, et al. Richtlijn Voorste
kruisbandletsel. 's-Hertogenbosch, The Netherlands: Nederlandse Orthopaedische Vereniging; 2011. (4) Roos H, Ornell M, Gardsell P, Lohmander LS, Lindstrand A. Soccer after anterior cruciate ligament injury--an
incompatible combination? A national survey of incidence and risk factors and a 7-year follow-up of 310 players. Acta Orthop Scand 1995 Apr;66(2):107-112.
(5) Schunke M. Prometheus, Algemene anatomie en bewegingsapparaat. second ed. Houten: Bohn Stafleu van
Loghum; 2005. (6) Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and
review of literature. Am J Sports Med 1995 Nov-Dec;23(6):694-701. (7) Myklebust G, Maehlum S, Holm I, Bahr R. A prospective cohort study of anterior cruciate ligament injuries in elite
Norwegian team handball. Scand J Med Sci Sports 1998 Jun;8(3):149-153. (8) Boden BP, Dean GS, Feagin JA,Jr, Garrett WE,Jr. Mechanisms of anterior cruciate ligament injury. Orthopedics
2000 Jun;23(6):573-578. (9) Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team
handball: a systematic video analysis. Am J Sports Med 2004 Jun;32(4):1002-1012. (10) A.D.A.M. Medical Encyclopedia:http://www.nlm.nih.gov/medlineplus/ency/article/001074.htm. (11) Meuffels DE, Poldervaart MT, Diercks RL, Fievez AW, Patt TW, Hart CP, et al. Guideline on anterior cruciate
ligament injury. Acta Orthop 2012 Aug;83(4):379-386. (12) Lysholm J, Gillquist J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale.
Am J Sports Med 1982 May-Jun;10(3):150-154. (13) Noyes FR, Bassett RW, Grood ES, Butler DL. Arthroscopy in acute traumatic hemarthrosis of the knee. Incidence
of anterior cruciate tears and other injuries. J Bone Joint Surg Am 1980 Jul;62(5):687-95, 757. (14) Sarimo J, Rantanen J, Heikkila J, Helttula I, Hiltunen A, Orava S. Acute traumatic hemarthrosis of the knee. Is
routine arthroscopic examination necessary? A study of 320 consecutive patients. Scand J Surg 2002;91(4):361-364.
(15) Cooper RL, Taylor NF, Feller JA. A randomised controlled trial of proprioceptive and balance training after surgical
reconstruction of the anterior cruciate ligament. Res Sports Med 2005 Jul-Sep;13(3):217-230. (16) Grontvedt T, Engebretsen L, Benum P, Fasting O, Molster A, Strand T. A prospective, randomized study of three
operations for acute rupture of the anterior cruciate ligament. Five-year follow-up of one hundred and thirty-one patients. J Bone Joint Surg Am 1996 Feb;78(2):159-168.
(17) Foster T, Wolfe B, Ryan S, Silvestri L, Kaye E. Does the graft source really matter in the outcome of patients
undergoing anterior cruciate ligament reconstruction? An evaluation of autograft versus allograft reconstruction results: a systematic review. . ;Am J Sports Med. 2010;38(1):189.
(18) Daniel DM, Fithian DC. Indications for ACL surgery. Arthroscopy 1994 Aug;10(4):434-441. (19) Fink C, Hoser C, Hackl W, Navarro RA, Benedetto KP. Long-term outcome of operative or nonoperative treatment
of anterior cruciate ligament rupture--is sports activity a determining variable? Int J Sports Med 2001 May;22(4):304-309.

42
(20) Dunn WR, Lyman S, Lincoln AE, Amoroso PJ, Wickiewicz T, Marx RG. The effect of anterior cruciate ligament reconstruction on the risk of knee reinjury. Am J Sports Med 2004 Dec;32(8):1906-1914.
(21) Sloane PA, Brazier H, Murphy AW, Collins T. Evidence based medicine in clinical practice: how to advise patients on the influence of age on the outcome of surgical anterior cruciate ligament reconstruction: a review of the literature. Br J Sports Med 2002 Jun;36(3):200-3; discussion 204.
(22) Barber FA, Elrod BF, McGuire DA, Paulos LE. Is an anterior cruciate ligament reconstruction outcome age
dependent? Arthroscopy 1996 Dec;12(6):720-725. (23) Heijne A, Ang BO, Werner S. Predictive factors for 12-month outcome after anterior cruciate ligament
reconstruction. Scand J Med Sci Sports 2009 Dec;19(6):842-849. (24) Salmon LJ, Refshauge KM, Russell VJ, Roe JP, Linklater J, Pinczewski LA. Gender differences in outcome after
anterior cruciate ligament reconstruction with hamstring tendon autograft. Am J Sports Med 2006 Apr;34(4):621-629.
(25) Kowalchuk DA, Harner CD, Fu FH, Irrgang JJ. Prediction of patient-reported outcome after single-bundle anterior
cruciate ligament reconstruction. Arthroscopy 2009 May;25(5):457-463. (26) Meunier A, Odensten M, Good L. Long-term results after primary repair or non-surgical treatment of anterior
cruciate ligament rupture: a randomized study with a 15-year follow-up. Scand J Med Sci Sports 2007 Jun;17(3):230-237.
(27) Williams RJ,3rd, Wickiewicz TL, Warren RF. Management of unicompartmental arthritis in the anterior cruciate
ligament-deficient knee. Am J Sports Med 2000 Sep-Oct;28(5):749-760. (28) Ferrari JD BB. Isolated anterior cruciate ligament injury. Chapman's Orthopedic surgery Philadelphia: Lippincott,
Williams & Wilkins; 2001. p. 2347. (29) Jarvela T, Nyyssonen M, Kannus P, Paakkala T, Jarvinen M. Bone-patellar tendon-bone reconstruction of the
anterior cruciate ligament. A long-term comparison of early and late repair. Int Orthop 1999;23(4):227-231. (30) Menetrey J, Duthon VB, Laumonier T, Fritschy D. "Biological failure" of the anterior cruciate ligament graft. Knee
Surg Sports Traumatol Arthrosc 2008 Mar;16(3):224-231. (31) George MS, Dunn WR, Spindler KP. Current concepts review: revision anterior cruciate ligament reconstruction.
Am J Sports Med 2006 Dec;34(12):2026-2037. (32) Legnani C, Ventura A, Terzaghi C, Borgo E, Albisetti W. Anterior cruciate ligament reconstruction with synthetic
grafts. A review of literature. Int Orthop 2010 Apr;34(4):465-471. (33) Zoltan DJ, Reinecke C, Indelicato PA. Synthetic and allograft anterior cruciate ligament reconstruction. Clin Sports
Med 1988 Oct;7(4):773-784. (34) Carey JL, Dunn WR, Dahm DL, Zeger SL, Spindler KP. A systematic review of anterior cruciate ligament
reconstruction with autograft compared with allograft. J Bone Joint Surg Am 2009 Sep;91(9):2242-2250. (35) Poolman RW, Farrokhyar F, Bhandari M. Hamstring tendon autograft better than bone patellar-tendon bone
autograft in ACL reconstruction: a cumulative meta-analysis and clinically relevant sensitivity analysis applied to a previously published analysis. Acta Orthop 2007 Jun;78(3):350-354.
(36) Biau DJ, Tournoux C, Katsahian S, Schranz P, Nizard R. ACL reconstruction: a meta-analysis of functional scores.
Clin Orthop Relat Res 2007 May;458:180-187. (37) Goldblatt JP, Fitzsimmons SE, Balk E, Richmond JC. Reconstruction of the anterior cruciate ligament: meta-
analysis of patellar tendon versus hamstring tendon autograft. Arthroscopy 2005 Jul;21(7):791-803. (38) Gifstad T, Sole A, Strand T, Uppheim G, Grontvedt T, Drogset JO. Long-term follow-up of patellar tendon grafts or
hamstring tendon grafts in endoscopic ACL reconstructions. Knee Surg Sports Traumatol Arthrosc 2013 Mar;21(3):576-583.
(39) Dauty M, Tortellier L, Rochcongar P. Isokinetic and anterior cruciate ligament reconstruction with hamstrings or
patella tendon graft: analysis of literature. Int J Sports Med 2005 Sep;26(7):599-606.

43
(40) Freedman KB, D'Amato MJ, Nedeff DD, Kaz A, Bach BR,Jr. Arthroscopic anterior cruciate ligament reconstruction:
a metaanalysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med 2003 Jan-Feb;31(1):2-11.
(41) Yunes M, Richmond JC, Engels EA, Pinczewski LA. Patellar versus hamstring tendons in anterior cruciate ligament
reconstruction: A meta-analysis. Arthroscopy 2001 Mar;17(3):248-257. (42) Prodromos CC, Joyce BT, Shi K, Keller BL. A meta-analysis of stability after anterior cruciate ligament
reconstruction as a function of hamstring versus patellar tendon graft and fixation type. Arthroscopy 2005 Oct;21(10):1202.
(43) Colvin A, Sharma C, Parides M, Glashow J. What is the best femoral fixation of hamstring autografts in anterior
cruciate ligament reconstruction?: a meta-analysis. Clin Orthop Relat Res 2011 Apr;469(4):1075-1081. (44) Milano G, Mulas PD, Ziranu F, Piras S, Manunta A, Fabbriciani C. Comparison between different femoral fixation
devices for ACL reconstruction with doubled hamstring tendon graft: a biomechanical analysis. Arthroscopy 2006 Jun;22(6):660-668.
(45) Hoher J, Livesay GA, Ma CB, Withrow JD, Fu FH, Woo SL. Hamstring graft motion in the femoral bone tunnel
when using titanium button/polyester tape fixation. Knee Surg Sports Traumatol Arthrosc 1999;7(4):215-219. (46) Clark R, Olsen RE, Larson BJ, Goble EM, Farrer RP. Cross-pin femoral fixation: a new technique for hamstring
anterior cruciate ligament reconstruction of the knee. Arthroscopy 1998 Apr;14(3):258-267. (47) McGuire DA, Barber FA, Elrod BF, Paulos LE. Bioabsorbable interference screws for graft fixation in anterior
cruciate ligament reconstruction. Arthroscopy 1999 Jul-Aug;15(5):463-473. (48) Brand J,Jr, Weiler A, Caborn DN, Brown CH,Jr, Johnson DL. Graft fixation in cruciate ligament reconstruction. Am J
Sports Med 2000 Sep-Oct;28(5):761-774. (49) Kamath GV, Redfern JC, Greis PE, Burks RT. Revision anterior cruciate ligament reconstruction. Am J Sports Med
2011 Jan;39(1):199-217. (50) Ahmad C, Gardner T, Groh M, Arnouk J, Levine W. Mechanical properties of soft tissue femoral fixation devices
for anterior cruciate ligament reconstruction. Am J Sports Med 2004 Apr-May;32(3):635. (51) Benjaminse A, Gokeler A, van der Schans CP. Clinical diagnosis of an anterior cruciate ligament rupture: a meta-
analysis. J Orthop Sports Phys Ther 2006 May;36(5):267-288. (52) Scholten RJ, Opstelten W, van der Plas CG, Bijl D, Deville WL, Bouter LM. Accuracy of physical diagnostic tests for
assessing ruptures of the anterior cruciate ligament: a meta-analysis. J Fam Pract 2003 Sep;52(9):689-694. (53) Stengel D, Matthes G, Seifert J, Tober V, Mutze s, Rademacher G, et al. SPOT Group. Resorbable screws versus
pins for optimal transplant fixation (SPOT) in anterior cruciate ligament replacement with autologous hamstring grafts: rationale and design of a randomized, controlled, patient and investigator blinded trial. 2005; 21:1(BMC Surg.).
(54) Capuano L, Hardy P, Longo UG, Denaro V, Maffulli N. No difference in clinical results between femoral
transfixation and bio-interference screw fixation in hamstring tendon ACL reconstruction. A preliminary study. Knee 2008 Jun;15(3):174-179.
(55) Buelow JU, Siebold R, Ellermann A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament
reconstruction with hamstrings: extracortical versus anatomical fixation. Knee Surg Sports Traumatol Arthrosc 2002 Mar;10(2):80-85.
(56) Yosmaoglu HB, Baltaci G, Kaya D, Ozer H, Atay A. Comparison of functional outcomes of two anterior cruciate
ligament reconstruction methods with hamstring tendon graft. Acta Orthop Traumatol Turc 2011;45(4):240-247. (57) Harilainen A, Sandelin J. A prospective comparison of 3 hamstring ACL fixation devices--Rigidfix, BioScrew, and
Intrafix--randomized into 4 groups with 2 years of follow-up. Am J Sports Med 2009 Apr;37(4):699-706.

44
(58) Harilainen A, Sandelin J, Jansson KA. Cross-pin femoral fixation versus metal interference screw fixation in
anterior cruciate ligament reconstruction with hamstring tendons: results of a controlled prospective randomized study with 2-year follow-up. Arthroscopy 2005 Jan;21(1):25-33.
(59) Rose T, Hepp P, Venus J, Stockmar C, Josten C, Lill H. Prospective randomized clinical comparison of femoral
transfixation versus bioscrew fixation in hamstring tendon ACL reconstruction--a preliminary report. Knee Surg Sports Traumatol Arthrosc 2006 Aug;14(8):730-738.
(60) Ma CB, Francis K, Towers J, Irrgang J, Fu FH, Harner CH. Hamstring anterior cruciate ligament reconstruction: a
comparison of bioabsorbable interference screw and endobutton-post fixation. Arthroscopy 2004 Feb;20(2):122-128.
(61) Galla M, Uffmann J, Lobenhoffer P. Femoral fixation of hamstring tendon autografts using the TransFix device
with additional bone grafting in an anteromedial portal technique. Arch Orthop Trauma Surg 2004 May;124(4):281-284.
(62) Sabat D, Kundu K, Arora S, Kumar V. Tunnel widening after anterior cruciate ligament reconstruction: a
prospective randomized computed tomography--based study comparing 2 different femoral fixation methods for hamstring graft. Arthroscopy 2011 Jun;27(6):776-783.
(63) Schultz WR, McKissick RC, DeLee JC. Tibial tunnel widening after hamstring tendon anterior cruciate ligament
reconstruction: the effect of supplemental aperture fixation with autogenous bone cores. Am J Sports Med 2007 Oct;35(10):1725-1730.
(64) Fauno P, Kaalund S. Tunnel widening after hamstring anterior cruciate ligament reconstruction is influenced by
the type of graft fixation used: a prospective randomized study. Arthroscopy 2005 Nov;21(11):1337-1341. (65) Price R, Stoney J, Brown G. Prospective randomized comparison of endobutton versus cross-pin femoral fixation
in hamstring anterior cruciate ligament reconstruction with 2-year follow-up. ANZ J Surg 2010 Mar;80(3):162-165.
(66) Paulsen. Sobotta / deel 1 Anatomie van het bewegingsapparaat. November 2011:http://www.elsevier-
data.de/SobottaRed/Daten/bilder/zoom/1289_100.jpg. (67) Noyes FR. ACL graft failure due to problems in graft tensioning and fixation. 2008 march 29. (68) Schindler OS. Surgery for anterior cruciate ligament deficiency: a historical perspective. Knee Surg Sports
Traumatol Arthrosc 2012 Jan;20(1):5-47. (69) Roos EM, Roos HP, Ekdahl C, Lohmander LS. Knee injury and Osteoarthritis Outcome Score (KOOS)--validation of
a Swedish version. Scand J Med Sci Sports 1998 Dec;8(6):439-448. (70) Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International Knee
Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res (Hoboken) 2011 Nov;63 Suppl 11:S208-28.
(71) de Groot IB, Favejee MM, Reijman M, Verhaar JA, Terwee CB. The Dutch version of the Knee Injury and
Osteoarthritis Outcome Score: a validation study. Health Qual Life Outcomes 2008 Feb 26;6:16-7525-6-16. (72) Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, et al. Development and validation of the
international knee documentation committee subjective knee form. Am J Sports Med 2001 Sep-Oct;29(5):600-613.
(73) Haverkamp D, Sierevelt IN, Breugem SJ, Lohuis K, Blankevoort L, van Dijk CN. Translation and validation of the
Dutch version of the International Knee Documentation Committee Subjective Knee Form. Am J Sports Med 2006 Oct;34(10):1680-1684.
(74) Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 1985
Sep;(198)(198):43-49.

45
(75) Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR. The reliability, validity, and responsiveness
of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med 2009 May;37(5):890-897.
(76) Linko E, Harilainen A, Malmivaara A, Seitsalo S. Surgical versus conservative interventions for anterior cruciate
ligament ruptures in adults. Cochrane Database Syst Rev 2005 Apr 18;(2)(2):CD001356. (77) Andersson C, Odensten M, Good L, Gillquist J. Surgical or non-surgical treatment of acute rupture of the anterior
cruciate ligament. A randomized study with long-term follow-up. J Bone Joint Surg Am 1989 Aug;71(7):965-974. (78) Sandberg R, Balkfors B, Nilsson B, Westlin N. Operative versus non-operative treatment of recent injuries to the
ligaments of the knee. A prospective randomized study. J Bone Joint Surg Am 1987 Oct;69(8):1120-1126. (79) Pujol N, David T, Bauer T, Hardy P. Transverse femoral fixation in anterior cruciate ligament (ACL) reconstruction
with hamstrings grafts: an anatomic study about the relationships between the transcondylar device and the posterolateral structures of the knee. Knee Surg Sports Traumatol Arthrosc 2006 Aug;14(8):724-729.
(80) Plaweski S, Rossi J, Merloz P. Anterior cruciate ligament reconstruction: assessment of the hamstring autograft
femoral fixation using the EndoButton CL. Orthop Traumatol Surg Res 2009 Dec;95(8):606-613. (81) Monaco E, Labianca L, Speranza A, Agro AM, Camillieri G, D'Arrigo C, et al. Biomechanical evaluation of different
anterior cruciate ligament fixation techniques for hamstring graft. J Orthop Sci 2010 Jan;15(1):125-131. (82) Micucci CJ, Frank DA, Kompel J, Muffly M, Demeo PJ, Altman GT. The effect of interference screw diameter on
fixation of soft-tissue grafts in anterior cruciate ligament reconstruction. Arthroscopy 2010 Aug;26(8):1105-1110.