Embed Size (px)
Citation preview

A RETROspective Study of Combination Pyrimidine Nucleoside Therapy in Patients with Thymidine Kinase 2 (TK2) Deficiency
Joanne Quan,1 Christina Domínguez-González,2 Carmen Paradas,3 Marcos Madruga-Garrido,3 Andres Osorio Nascimento,4 Francina Munell,5 Hanna Mandel,6 Tzipora Falik Zaccai,6&7 Mira Ginzberg,8 Galit Tal,9 Caterina Garone,10 Emanuele Barca,11 Tristen Moors,1 Michio Hirano,11
1Modis Therapeutics (a Wholly Owned Subsidiary of Zogenix, Inc), Oakland, CA, USA; 2Hospital 12 de Octubre Instituto de Investigación, Madrid, Spain; 3Hospital Universitario Virgen del Rocío, Sevilla, Spain; 4Hospital Sant Joan de Déu, Barcelona, Spain; 5Hospital Vall d'Hebron, Barcelona, Spain; 6Western Galilee Medical Center, Israel; 7Azrieli faculty of Medicine, Bar Ilan, Israel; 8The Edith Wolfson Medical Center, Israel; 9The Ruth Rappaport Children's Hospital Rambam Medical Center, Israel; 10University of Cambridge, UK; 11Columbia University Medical Center, New York, USA
Modis would also like to acknowledge Myriam Ley Martos. Hospital Puerta del Mar. Cádiz and Javier Aguirre Rodríguez. Hospital Torrecárdenas. Almería
Ultra-rare autosomal-recessive mitochondrial DNA depletion/deletion syndrome caused by mutations in TK2 gene
Clinically characterized by severe progressive proximal limb, bulbar, and axial muscle weakness which often causes respiratory failure and death
Subjects with untreated TK2d show progressive decline which is often fatal. No spontaneous recovery has been reported
Age at onset is prognostic for outcome: younger subjects have high mortality There are no medicinal products indicated for treatment of TK2d. Treatment is
limited to supportive care
TK2 Deficiency
(TK2d)
TK2 mutations impair the mitochondrial nucleotide salvage pathway required for synthesis of deoxyribonucleotide triphosphates (dNTPs)
Treatment with the pyrimidine nucleosides (deoxycytidine [dC] and deoxythymidine [dT]; ie, substrate enhancement therapy) aims to (a) maximize residual TK2 activity to support mtDNA replication and (b) increase the levels of the substrates phosphorylated by TK1 and deoxycytidine kinase, thereby restoring the dNTP pool available for mtDNA synthesis
Mechanism
Study MT-1621-101 (RETRO) is a retrospective, GCP-compliant, medical chart review study of pyrimidine nucleosides administered as oral solution in patients with TK2d
The study comprises records from 38 pediatric and adult TK2d patients The primary objective of RETRO is to describe the safety and tolerability of pyrimidine
nucleosides in patients with TK2d The secondary objective is the assessment of efficacy (including survival) Patients were treated for a median of 71 weeks (range of 92 days-7 years) The survival analysis compared data to an untreated patient dataset extracted from
published natural history studies and individual case reports The responder analysis included a within-patient responder analysis that assessed changes
in the motor, respiratory, and feeding domains and compared these to the subject’s pretreatment baseline
Survival Analysis
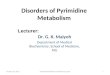
No subjects treated with pyrimidine nucleosides in Study MT-1621-101 died. Survival analysis compared treated subjects with untreated patient dataset that excluded subjects who died before age 1.3 years (youngest age of treated patient) The statistical models applied utilized methods to correct for potential length biased sampling Comparing RETRO subjects to a dataset of all published untreated cases of TK2d (n=68), there was a statistically significant improvement in survival (p = 0.0006), using the Cox regression model and age of
onset as a strata variable
FIGURE 1. Direct Adjusted Survival Curves Modeled from Treated and Untreated Data(Assuming Treatment from Time of Onset; Red = Untreated; Blue = Treated)
Responder AnalysisAnalysis Methods Clinical included endpoints (eg, EK2, HFMSE, 6MWT), motor milestones
(eg, walking), respiratory status, pulmonary function tests, and feeding tube status
Each subject was scored in the MOTOR, RESPIRATORY, and FEEDING domains according to predefined response thresholds
The last timepoint was compared with pretreatment baseline to determine the subject status: improved/remained stable/worsened
Overall Response Analysis In subjects administered pyrimidine nucleosides, most subjects (95%)
either improved (68%) or remained stable (26%). A low percentage of subjects (5%) worsened (Figure 2)
In each age of onset category, the majority of subjects improved or remained stable during the study (Table 1)
As TK2d is a progressive disease, subjects who improved or remained stable may both be considered as demonstrating clinical benefit
Safety
Examples of Functional ImprovementAmbulation: 3 subjects who had lost ambulation prior to treatment regained ambulation; 1 subjects who had never walked gained ambulation.Respiratory function: 1 subject receiving 24 hours/day of invasive mechanical ventilation prior to treatment discontinued all respiratory support following treatment. Feeding Support: 3 subjects had their feeding tubes removed, out of a total of 8 subjects on feeding tubes at study start
TABLE 1. MT-1621-101 Response Analysis
36 subjects (95%) had at least one AE reported Most AEs reported were considered not related to study drug (199 of 292) and were
Grade 1 (186 of 292 events) The most frequent AEs were diarrhea (63%, 24 of 38 subjects), increased blood
creatine phosphokinase (18%, 7 subjects), increased alanine aminotransferase (16%, 6 subjects), pyrexia (16%, 6 subjects), increased aspartate aminotransferase (13%, 5 subjects)
Serious AEs (SAEs) were reported in 14 subjects (37%). The majority of SAEs were deemed related to TK2d and study drug; 2 patients experienced 3 events related to study drug alone (kidney stone, kidney stone removal, diarrhea).
Two subjects discontinued study drug due to AEs of increased GGT and increased liver enzymes. The elevations were reversible and did not meet criteria for drug-induced liver injury
There were no deaths in the study Overall, study treatment was well tolerated
Age of Onset≤ 2 Years 2-12 Years >12 Years All Subjects
Overall ResponseImproved 11 (73%) 11 (79%) 4 (44%) 26 (68%)Remained Stable 4 (27%) 3 (21%) 3 (33%) 10 (26%)Worsened 0% 0% 2 (22%) 2 (5%)Motor DomainImproved 12 (80%) 10 (71%) 5 (56%) 27 (71%)Remained Stable 3 (20%) 4 (29%) 3 (33%) 10 (26%)Worsened 0% 0% 1 (11%) 1 (3%)Respiratory DomainImproved 6 (40%) 4 (29%) 0% 10 (26%)Remained Stable 8 (53%) 10 (71%) 7 (78%) 25 (66%)Worsened 1 (7%) 0% 2 (22%) 3 (8%)Feeding DomainImproved 2 (13%) 1 (7%) 0% 3 (8%)Remained Stable 13 (87%) 13 (93%) 9 (100%) 35 (92%)Worsened 0% 0% 0% 0%
FIGURE 2. Responder Analysis – All Subjects
SUMMARY Treatment with pyrimidine nucleosides significantly improved survival in subjects with TK2d Greater than 90% of subjects experienced improvement in response or no further decline overall A number of subjects regained milestones that were previously lost. These regained milestones
included 4 subjects that gained ambulation, 1 subject discontinuing respiratory support, and 3 subjects had feeding tubes removed
Pyrimidine nucleosides were generally safe and well tolerated. No deaths occurred in TK2d subjects treated with pyrimidine nucleosides
Pyrimidine nucleosides may provide an effective treatment option for patients with TK2d Modis Therapeutics is developing MT1621, a GMP fixed dose combination of dC/dT for the
treatment of TK2d
Generated from 2 comprehensive natural history studies (Wang 2018, Garone 2018), 1 large case series (Domínguez-González, 2019) and systematic PubMed literature search through July 2019
Search terms included thymidine kinase 2 deficiency, TK2, thymidine kinase 2, TK2 mitochondrial DNA maintenance defects
Dataset was curated to remove treated subjects, duplicates and to resolve discrepancies.
Data on age at loss of ambulation, age at loss of independent ventilation, and age at death were captured.
Subject Demographics in Study MT-1621-101n 38 subjectsAge of Onset
≤ 2 years 15 (40%)2-12 years 14 (37%)>12 years 9 (24%)
Median Age of Onset (Q1, Q3) 2.5 (1.4,11.7) yearsMale 21 (55%)Female 17 (45%)Baseline Status
Ambulatory 16 (42%)Ventilator Support Yes 19 (50%)Feeding Tube Yes 8 (21%)
Study MT-1621-101
Background
0 20 40 60 80
Percentage of Subjects
Improved
RemainedStable
Worsened
Untreated Patient Dataset
ReferencesWang J, Kim E, Dai H, et al (2018) Clinical and molecular spectrum of thymidine kinase 2-related mtDNA maintenance defect. Mol Genet Metab:124(2):124-130.Garone C, Taylor RW, Nascimento A, et al (2018) Retrospective natural history of thymidine kinase 2 deficiency. J Med Genet:55(8):515-521.Domínguez-González C, Hernández-Laín A, Rivas E et al (2019) Late-onset thymidine kinase 2 deficiency: a review of 18 cases. Orphanet J Rare Dis:14(1):100.
Figure 1B: >2 to ≤ 12 years at age of onset
Time to Event (Years)
Surv
ival
Pro
babi
lity
Figure 1A: ≤ 2 years at age of onset Figure 1C: > 12 years at age of onset
Time to Event (Years) Time to Event (Years)