Embed Size (px)
Citation preview

ORIGINAL ARTICLE
A randomized, double-blind, vehicle-controlled study of a novelliposomal dithranol formulation in psoriasis
ABIR SARASWAT1, RAVINDRA AGARWAL2, OM P. KATARE2, INDERJEET KAUR3 &
BHUSHAN KUMAR3
1Skin Clinic, Lucknow, India, 2University Institute of Pharmaceutical Sciences, Panjab University, Chandigarh, India, and3Department of Dermatology, Venereology & Leprology, Postgraduate Institute of Medical Education & Research,
Chandigarh, India
AbstractDithranol is infrequently used in psoriasis in spite of excellent efficacy due to its local adverse effects. We have synthesized anovel formulation of dithranol in which the drug is entrapped in phospholipid liposomes. This formulation has shownmarkedly low irritation and minimal staining of skin and clothes in preliminary studies. Twenty patients with bilaterallysymmetrical stable plaque psoriasis applied 0.5% dithranol lipogel to lesions over one side of the body. On the other side, 10patients were randomized to apply pure liposomal base and 10 applied a conventional cream containing 1.15% dithranol,1.15% salicylic acid and 5.3% coal tar in a 30-minute, short contact regimen for 6 weeks. Patients were assessed for diseaseseverity, perilesional erythema and skin staining, pruritus and any other adverse effects at baseline, 2, 4 and 6 weeks. Bothlipogel and the cream significantly reduced the total severity score compared to the liposomal base at 4 (p50.004) and 6(p50.01) weeks. There was no significant difference in the clinical response of dithranol cream and lipogel. Markedly lowincidence and severity of perilesional erythema (pv0.001) and skin staining (pv0.05) was seen with the lipogel incomparison with the cream.
Key words: Adverse effects, dithranol, liposome, psoriasis, topical therapy
Introduction
Since its introduction more than 80 years ago,
dithranol has been one of the most effective topical
treatments for psoriasis, but its side effects of
irritancy and staining of skin and clothes have
restricted its use. Several attempts have been made
to eliminate these troublesome side effects while
maintaining efficacy. Shorter application times have
been recommended (1), followed by washing the
skin with special cleansing agents (2), and aqueous
cream (3) and wax-ester-based preparations (4) have
been introduced. However, dithranol use remains
limited in spite of various modifications in thera-
peutic regimens and topical formulations.
In 1992, Gehring et al. (5) demonstrated
increased skin penetration and clinical effect of
dithranol when compounded in a vehicle containing
liposomes. However, that formulation did not
contain liposome-entrapped dithranol. We have
prepared a new, stable, liposome-entrapped formu-
lation of dithranol in an aqueous gel base. This
dithranol lipogel has shown good skin penetration
and pharmacokinetics on animal skin (6). Our
preliminary open-label studies on psoriasis patients
have revealed a marked lack of skin staining and
irritation coupled with good efficacy (7), and fabric-
staining studies have shown much lighter and easily
washable staining compared to conventional pre-
parations (8).
The aim of the present study was to test the
clinical efficacy and acceptability of dithranol lipogel
against the only commercially available dithranol
preparation in India, a conventional cream-based
product containing dithranol, salicylic acid and coal
tar.
Materials and methods
This trial was a randomized, double-blind, vehicle-
controlled, within-patient comparison. It was con-
ducted at the Dermatology outpatient department of
the Postgraduate Institute of Medical Education and
Research, Chandigarh, which is a tertiary-level
referral centre in northern India. This study was
Correspondence: Abir Saraswat, B 7, Indira Nagar, Lucknow (UP), PIN 226 016, India. E-mail: [email protected]
(Received 10 May 2006; accepted 1 July 2006)
Journal of Dermatological Treatment. 2007; 18: 40–45
ISSN 0954-6634 print/ISSN 1471-1753 online # 2007 Taylor & Francis
DOI: 10.1080/09546630601028729
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tha
mm
asat
Uni
vers
ity o
n 10
/09/
14Fo
r pe
rson
al u
se o
nly.

performed in accordance with standard operating
procedures with the permission of the Drug
Controller General of India.
Inclusion criteria
Male or female patients aged 12 years or older, with
bilaterally symmetrical stable plaque psoriasis invol-
ving less than 10% of the body surface area, who
were registered at the Psoriasis Clinic of the
Dermatology outpatient department, were eligible
for enrolment in the study. The nature of the study
was explained to the patients. Twenty-three patients
satisfying these criteria were recruited. After a 2-
week wash-off period, during which only topical
bland emollients were allowed, 20 patients were
randomized to receive treatment.
Exclusion criteria
Patients who had ever used dithranol in the past, or
had taken any systemic anti-psoriatic treatment in
the 8-week period to randomization were excluded
from the study. Known intolerance to the ingredi-
ents of the topical agents used was also an exclusion
criterion. During the study period, patients were
allowed only topical bland emollients apart from the
medications given. Systemic antihistamines were
allowed in patients with moderate to severe pruritus.
Study design
Patients who met the study criteria were randomized
to either of the two treatment arms at a 1:1 ratio.
The investigator and patients were blinded as to the
composition of the topical medication dispensed.
The study duration was 6 weeks.
Treatment
Dithranol lipogel was produced by optimal entrap-
ment of dithranol in multilamellar liposomes com-
posed of phosphatidyl choline and cholesterol, with
minimal free drug. The mean diameter of liposomes
was 5¡1.25 mm. Further details of the preparation
and in vitro evaluation of dithranol lipogel have been
published earlier (6). Each patient was given two
identical 25 g tubes, one of which contained 0.5%
dithranol lipogel. The other tube contained either
pure liposomal base without dithranol, or Derobin
ointment (1.15% dithranol, 1.15% salicylic acid,
5.3% decolourized coal tar in a cream base)
depending on the treatment arm. To ensure
adequate blinding, a yellow food-grade dye was
added to the liposomal base, which resembled the
yellow colour of the dithranol-loaded product.
Each patient was randomly assigned to apply one
of the tubes to all lesions on the right side of the
body, and the other to the left side. Patients were
instructed to apply the medication with a plastic/
wooden applicator, carefully avoiding perilesional
skin, and to wash off both the sides with ordinary
bathing soap after 30 minutes of application.
Following this, topical emollients were applied to
the lesions immediately and ad libitum thereafter.
Treatment was continued for 6 weeks or until a total
sign score of 0 was reached, whichever was earlier.
Clinical evaluation
Patients were examined at screening, baseline and at
weeks 2, 4 and 6. The signs evaluated were
erythema, induration and scaling. The severity of
each sign was scored on a 0–3 scale (05absent,
15mild, 25moderate and 35severe) and the sum of
the scores constituted the total severity score (TSS).
If different lesions on the same side showed differing
sign scores, the mean of all lesional sign scores was
used. Perilesional erythema was also scored on a
similar 0–3 score, and lesional and perilesional
brown staining of skin was scored on the 0–3 score
given by Mustakallio (9). Lesional itching was
scored on a 0–10 visual analog scale (VAS) by the
patients. For each of the above parameters, separate
scoring for left and right sides was done at each visit.
Patients were also asked about any burning sensation
on application, overall cosmetic acceptability and
cloth staining on both sides.
Statistical methods
The efficacy analysis was conducted on the intent-
to-treat (ITT) population on patients with at least
one post-baseline assessment. The primary efficacy
variable was the fall in TSS, which was analysed at
each visit by the Kruskal–Wallis one-way analysis of
variance on ranks, which does not require a normal
distribution of observations. This was followed by all
pairwise multiple comparison procedure (Student–
Newman–Keuls method). Multiple comparisons
taking the dithranol lipogel group as the control by
Dunn’s method were also performed. The power of
all performed tests was more than 80% with
alpha50.05%. Non-parametric data were compared
by the chi-squared test. All statistical tests were
performed using Sigma StatH software.
Results
A total of 23 patients entered the 2-week pre-study
washout period and three patients dropped out at
the end of this period due to unrelated reasons.
Twenty patients were randomized to two treatment
arms (dithranol lipogel versus liposomal base, n510;
dithranol lipogel versus cream, n510). Two patients
in the lipogel versus cream group discontinued the
treatment: one had severe irritation on only the site
treated with cream at 2 weeks and the other had
Liposomal dithranol in psoriasis 41
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tha
mm
asat
Uni
vers
ity o
n 10
/09/
14Fo
r pe
rson
al u
se o
nly.

moderate to severe irritation on both sides at 4
weeks. Both patients were advised to stop treatment
on both sides and periodic assessments were
continued until the end of the study (6 weeks).
None of the patients stopped treatment in the lipogel
versus liposomal base group.
Key demographic data and disease characteristics
at baseline are presented in Table I. All demo-
graphic and disease parameters were similar between
both treatment groups.
Efficacy
Complete clearance of disease (TSS50) was seen in
5/20 (25%) dithranol lipogel-treated sides (at 3
weeks in one patient, 4 weeks in three patients, and 6
weeks in one patient), 3/10 (33.3%) cream-treated
sites (at 3 weeks in all) and none of the liposomal
base-treated sites (pw0.05) (Figure 1A and B). Only
mild erythema (score51) without any induration or
scaling remained at 6 weeks in a further five patients
on the lipogel-treated side. The fall in erythema,
induration and scaling scores over the treatment
period with the three preparations is presented in
Figures 2A, B and C. All three treatments reduced
scaling the most, followed by induration and
erythema. In all three parameters, there was no
significant difference between the dithranol lipogel
versus liposomal base and dithranol lipogel versus
cream groups or individually between the three
treatments at baseline and 2 weeks. However, both
dithranol lipogel- and cream-treated sites showed
significantly less erythema, induration and scaling
than liposomal base-treated sites at 4 and 6 weeks
(pv0.05). There was no significant difference in the
mean scores of the cream- and lipogel-treated sites at
any point in the study. The changes in the TSS in
the three groups are presented in Table II.
Safety and tolerability
Perilesional erythema was observed at any visit on 1/
20 lipogel-treated sides, 7/10 cream-treated sides
and none of the liposomal base-treated sides (x2 test,
pv0.01). Erythema was mild in the dithranol
lipogel-treated side, whereas it was mild in three
patients, moderate in three patients and severe in
one patient on the cream-treated side.
Lesional/perilesional staining of skin was seen in 8/
20 dithranol lipogel-treated sites and it was scored 1
(brownish hue) in all of them. Skin staining was seen
Table I. Patient demographics and disease characteristics at
baseline.
Dithranol lipogel
versus liposomal
base n510
Dithranol lipogel
versus DerobinH
n510a
Mean age, years (¡SD) 40.1¡16.2 44.7¡14.9
Sex (male:female) 7:3 8:2
Median duration of
disease, years (range)
6 (0.6–32) 8 (1–47)
Mean % body surface
area involved (¡SD)
5.3¡2.1 6.1¡1.9
aTwo patients withdrew from the study after 2 weeks.
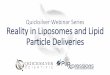
(A) (B)
Figure 1. (A) Pretreatment appearance of a patient in the dithranol lipogel (right) versus dithranol cream (left) group; (B) almost total
clearance with dithranol cream and more than 90% improvement with dithranol lipogel at 4 weeks.
42 A. Saraswat et al.
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tha
mm
asat
Uni
vers
ity o
n 10
/09/
14Fo
r pe
rson
al u
se o
nly.

in 9/10 cream-treated patients (x2 test, pv0.05). It
was scored 1 in one patient, 2 (reddish brown) in
seven patients and 3 (dark brown) in one patient
(Figure 3). The only patient with no staining had
discontinued treatment at 2 weeks due to severe
irritation.
The VAS for itching showed a bilaterally symme-
trical flat or downward trend in all patients except
two in the dithranol cream versus dithranol lipogel
group, in whom the cream-treated side experienced
increased itching at 2 weeks, followed by subsidence
of pruritus. There was no significant difference in
pruritus at 6 weeks between any of the three
treatments.
Two patients reported a transient burning sensa-
tion after application: one on only the cream-treated
side and the other on both cream- and dithranol
lipogel-treated sides. Fifteen patients preferred the
lipogel preparation for overall acceptability and
efficacy and five reported no particular preference.
Overall, five patients reported accidental staining of
clothes: two in the liposomal base versus dithranol
lipogel group and three in the cream versus dithranol
lipogel group. All of them reported that stains on the
side of dithranol lipogel application were easily and
almost completely washable with soap and water,
whereas the latter three commented on the deep,
permanent staining due to cream.
Discussion
This study showed that 0.5% liposome-entrapped
dithranol in an aqueous gel base has comparable
efficacy to a 1.15% commercially available dithranol
ointment, and this difference is exclusive of the
beneficial effect of the liposomal base itself.
Moreover, we have seen a remarkable difference
between the two products with regard to skin
irritation and staining. Similar to our observations
in a preliminary study (7), the dithranol lipogel had
significantly lighter skin staining compared to con-
ventional dithranol cream, even when both were
applied for identical 30-minute contact periods. A
marked reduction was also observed in the incidence
and severity of perilesional erythema with the
lipogel. These effects may be explained based on
the novel drug delivery mechanisms used in this
preparation.
Efficacy
Dithranol is highly unstable and is degraded quickly
in a pH-dependent manner in the presence of water
and oxygen to inactive metabolites like danthron and
dithranol dimer (10). Previous attempts to enhance
stability have involved the addition of a-hydroxy
acids such as salicylic acid (e.g. in the conventional
cream product used in this study) and antioxidants
such as ascorbyl palmitate (11,12). Dithranol has
been embedded in crystalline monoglycerides in a
relatively recent formulation (MicanolH) to enhance
stability and reduce perilesional spread (4). In the
liposomal gel used in this study, we have ensured
stability by two means: efficient liposomal drug
loading with minimum free drug, and the addition
of butylated hydroxytoluene, which is a potent
antioxidant. Stability is further enhanced by lipo-
some encapsulation, which protects dithranol mole-
cules from oxygen and water. Liposomes also
provide targeted delivery with slow and sustained
drug release, acting as ‘drug localizers’, and not
only as ‘drug transporters’. This is because simi-
larly to biological membranes, they can store both
Figure 2. (A) Fall in mean erythema score with the three
treatments; (B) fall in mean induration score with the three
treatments; (C) fall in mean scaling score with the three
treatments.
Liposomal dithranol in psoriasis 43
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tha
mm
asat
Uni
vers
ity o
n 10
/09/
14Fo
r pe
rson
al u
se o
nly.

water-soluble and lipophilic substances in their
different phases (13,14). These properties can
explain the comparable effect of the test formulation
with conventional dithranol cream in spite of having
a 56% lower dithranol concentration. Similar results
have been reported with liposomal formulations of
tretinoin, showing no loss of efficacy even with a
significantly reduced drug concentration (15).
A limitation of this study is the lack of a treatment
arm with a 0.5% conventional cream preparation of
dithranol. This means that the comparable efficacy
between 0.5% dithranol lipogel and 1.15% cream
cannot be attributed to the liposomal vehicle with
certainty.
Irritation
Histopathological studies done by us on normal rat
skin have shown that dithranol lipogel causes
minimal epidermal or dermal inflammatory changes
in comparison with other commercially available
dithranol formulations (submitted for publication).
Clinically, this was seen as almost no irritation in 19
of the 20 patients in this study. One patient who
reported irritation with the lipogel was found to be
sensitive to dithranol on a patch test and Repeated
Open Application Testing (ROAT). The explana-
tion of the reduced irritancy may lie in the
mechanism of dithranol irritation. It has been shown
that dithranol-derived free radicals are principally
responsible for perilesional erythema and inflamma-
tion, whilst paradoxically they mediate key antipsor-
iatic effects in lesional skin (16). Kersey et al. (17)
have suggested that dithranol-induced inflammation
could be due to an oxidation metabolite formed by
aryl hydrocarbon hydroxylase, an enzyme which is
induced in human skin by dithranol. Experimental
studies have shown that dithranol inhibits the
activity of endogenous free radical scavengers such
as superoxide dismutase and catalase in skin (18).
Thus, a combination of free radical-induced damage
and suppressed endogenous antioxidant activity
produces skin irritation. In this liposomal gel, slow
release of the drug from the multilamellar liposomes
and reduced dithranol-derived free radicals due to
enhanced stability may contribute to lowering the
irritancy. However, the exact reason for this effect is
a matter of conjecture.
Staining of skin
Brown discolouration of lesional and perilesional
skin is cosmetically the major adverse effect of
dithranol and is caused by the formation of insoluble
dithranol metabolites which cannot be easily washed
off. Danthron and dithranol dimer are orange and
pale yellow in colour and it is known that the violet-
brown skin staining is due to these and other
uncharacterized products derived from extensive
oxidation of dithranol (19). Therefore, it is expected
that enhancing the stability of dithranol will reduce
its oxidation and minimize skin staining. Moreover,
staining and irritation are concentration-dependent
and, therefore, 0.5% dithranol would be intrinsically
less staining and irritating than a 1.15% formulation.
Other adverse effects
The vehicle may be responsible for the local stinging,
itching, burning sensation and dryness of skin, as is
seen with conventional dithranol products (20). Co-
ingredients such as salicylic acid, which is present in
the conventional cream used in this study, are also
Table II. Fall in total severity score (¡SE) in the treatment groups.
Weeks
0 2 4 6
Dithranol lipogel 6.1¡1.3 3.8¡0.3 2.5¡0.3 1.6¡0.2
Conventional cream 6.3¡1.2 3.7¡0.3 2.3¡0.2 1.5¡0.2
Liposomal base 6.2¡1.2 5.3¡0.5 4.7¡0.5 4.1¡0.4
The inter-group differences were statistically significant at 4 and 6 weeks.
Figure 3. Perilesional pigmentation in a patient after 6 weeks of
treatment with dithranol cream (right) and dithranol lipogel (left).
44 A. Saraswat et al.
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tha
mm
asat
Uni
vers
ity o
n 10
/09/
14Fo
r pe
rson
al u
se o
nly.

known to produce local adverse effects. However,
the liposomal base has intrinsic emollient activity,
which was reflected in the slow, but steady improve-
ment in disease severity on the base-treated sites in
this study. These properties of liposomes and the
water-based gel formulation may account for the
excellent cosmetic acceptability and negligible local
adverse effects of the lipogel.
To conclude, this study has demonstrated that
0.5% liposomal dithranol gel is as effective as 1.15%
dithranol cream in the treatment of stable plaque
psoriasis and produces almost negligible local
adverse effects. Coupled with its low fabric and skin
staining and its easy washability, dithranol lipogel
has the potential to be much more acceptable to
patients and physicians than currently available
formulations. However, the extremely low irritation
and staining of the skin seen in this study needs to be
confirmed in larger studies.
Acknowledgement
We are grateful to Natterman Phospholipids GmbH,
Cologne, Germany, who supplied the liposomes and
GSK Pharmaceuticals (India), who provided pure
dithranol for this study free of charge.
References
1. Schaefer H, Farber EM, Goldberg L, Schalla W. Limited
application period for dithranol in psoriasis: Preliminary
report on penetration and clinical efficacy. Br J Dermatol.
1980;102:571–3.
2. Ramsay B, Lawrence CM, Bruce JM, Schuster S. The effect
of triethanolamine application on anthralin-induced inflam-
mation and therapeutic effect in psoriasis. J Am Acad
Dermatol. 1990;23:73–6.
3. Wilson JD, Ive FA. Dithrocream in psoriasis. Br J Dermatol.
1980;103:105–6.
4. Volden G, Bjomberg A, Tegner E, Pedersen NB, Arles UB,
Agren S, et al. Short-contact treatment at home with Micanol.
Acta Derm Venereol Suppl (Stockh). 1992;172:20–2.
5. Gehring W, Ghyczy M, Gloor M, Scheer T, Roding J.
Enhancement of the penetration of dithranol and increase of
effect of dithranol on the skin by liposomes.
Arzneimittelforschung. 1992;42:983–5.
6. Agarwal R, Katare OP, Vyas SP. Preparation and in-vitro
evaluation of liposomal/niosomal delivery systems of anti-
psoriatic drug dithranol. Int J Pharm. 2001;228:43–52.
7. Agarwal R, Saraswat A, Kaur I, Katare OP, Kumar B. A novel
liposomal formulation of dithranol in psoriasis: Preliminary
results. J Dermatol. 2002;29:286–8.
8. Saraswat A, Agarwal R, Kaur I, Katare OP, Kumar B.
Fabric staining properties and washability of a novel
liposomal dithranol formulation. J Dermatol Treat. 2002;13:
119–22.
9. Mustakallio KK. Irritation, staining and antipsoriatic activity
of 10-acyl analogue of anthralin. Br J Dermatol.
1981;105(suppl 20):23–7.
10. Hiller C, Campbell C, Smeaton I. How stable is dithranol?
An investigation into the degradation of different dithranol
formulations. Pharm Pract. 1995;5:428–31.
11. Van Scott EJ, Yu RJ. New chemical stabilizers, vehicles
and delivery systems to enhance efficacy of low strength
anthralin formulations. Br J Dermatol. 1981;105(suppl 20):
35–8.
12. Whitefield M. Pharmaceutical formulations of anthralin. Br J
Dermatol. 1981;105(suppl 20):28–32.
13. Schmid MH, Korting HC. Therapeutic progress with topical
liposome drugs for skin disease. Adv Drug Deliv Rev.
1996;18:335–42.
14. Lasch J, Bouwstra J. Interaction of external lipid vesicles with
the skin. J Liposome Res. 1995;5:543–69.
15. Schafer-Korting M, Korting HC, Ponce-Poschl E. Liposomal
tretinoin for uncomplicated acne vulgaris. Clin Investig.
1994;72:1086–91.
16. Muller K. Antipsoriatic and proinflammatory action of
anthralin. Implications for the role of oxygen radicals.
Biochem Pharmacol. 1997;53:1215–21.
17. Kersey P, Chapman P, Rogers S, Rawlins M, Schuster S. The
inflammatory response to anthralin and its relation to aryl
hydrocarbon hydroxylase. Br J Dermatol. 1981;105(suppl
20):64–7.
18. Muller K, Gawlik I. Inactivation of mouse epidermal 12-
lipoxygenase by anthralin: Implications for the role of oxygen
radicals. Biochem Pharmacol. 1996;51:1173–9.
19. Mustakallio KK. The history of dithranol and related
hydroxyxanthrones, their efficacy, side effects and different
regimens employed in the treatment of psoriasis: A review.
Acta Derm Venereol Suppl (Stockh). 1992;172:7–9.
20. Kraft S, Maibach HI, Shroot B. Dithranol (Anthralin). In:
Roenigk HH, Maibach HI, editors. Psoriasis. New York:
Marcel Dekker, 1998. p. 435–52.
Liposomal dithranol in psoriasis 45
J D
erm
atol
og T
reat
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tha
mm
asat
Uni
vers
ity o
n 10
/09/
14Fo
r pe
rson
al u
se o
nly.