Embed Size (px)
Citation preview

Introduction
In addition to anticancer vaccines, cytokines, and
immune checkpoint inhibitors, bispecific T cell engagers (BiTE) antibody (Ab) constructs, and chimeric antigen receptor T cells (CAR-T cells) represent alternative methods for harnessing the immune system to fight cancer. Immune checkpoint inhibitors, BiTEs, and CAR-T cells all utilize T cells in their fight against cancer, but in differing ways. Whereas immune checkpoint inhibitors amplify antigen-specific T cell response, BiTEs provide as-sistance in increasing T cell activity, and CAR-T cell therapy augments the capabilities of T cells. Both BiTEs and CAR-T cells provide targeted redirection of T cells against highly expressed tumor associated antigens (TAA). BiTEs have enjoyed some clinical success, with the recent approvals of catumaxomab and blinatumomab. The field of CAR-T has also grown significantly in recent years, there have been over 800 publications on CAR-T cells within the past five years and many clinical trials showing success, particularly for B cell malignancies[5]. These thera-pies offer novel treatment options, but have yet to be fully vetted for safety and efficacy. This report will provide a brief overview of BiTEs, as well as a more comprehensive review of CAR-T cell therapy. This report is part two of two of Kineticos’ series of research reports on cancer immunotherapies.
Bispecific T-Cell Engagers (BiTE) Antibody ConstructsBispecific T-cell engager antibody constructs (BiTEs) are a type of bispecific Ab which are engineered by combining two scFv domains of different Abs onto one polypeptide chain, with one scFv directed against the CD3 epitope of the T cell receptor (TCR) complex expressed on T cells, and the other scFv di-rected against a tumor-associated antigen (TAA)[6]. By simultaneously binding to both a T cell and can-cer cell, BiTEs form an “immunological synapse[7],” which results in target cell dependent polyclonal T cell activation and proliferation, followed by the release of IL-2 and IFNγ to induce the proliferation
and expansion of T cells at the tumor site[8], as well as the release of perforin and granzyme from the T cell to ultimately cause the destruction of the target cancer cell by apoptosis[5]. Perforin assembles into multimeric pores in the tumor cell membrane, which enables granzyme to enter into the target cancer cell. The “immunological synapse” formed by BiTEs are indistinguishable from those formed during the natu-ral cytotoxic T cell recognition process[7]. CD8+ and CD4+ TEM cells are the primary T cell subsets responsible for mediating the cytotoxic activity of BiTEs due to their large number of perforin and granzyme filled vesicles, as well as
their high capacity for proliferation[9]. It should be noted that BiTE-induced T cell activation, cytokine release, proliferation, and redirected lysis are target antigen-dependent and do not rely on the specific-ity of the TCR; thus, BiTEs are able to engage any T cell, regardless of the specificity of its TCR[9]. Furthermore, the size of the “synapse,” the distance between the anti-CD3 and anti-TAA moieties of the BiTE, determines the cytotoxicity of the BiTE as the apoptotic proteins perforin and granzyme must passively diffuse across the “synapse” from the T cell into the tumor cell[10]. Decreasing the size of the “synapse,” and thus the distance between the T cell and the tumor cell, results in increased cytotoxic activity. BiTEs are also able to induce T cells to enter into a “serial killing” mode, in which one T cell is able to sequentially induce apoptosis in multiple target cancer cells: it has been observed that, over a 9h period, one T cell was able to kill up to five target cancer cells[11]. Thus the formation of BiTE-induced “immunological synapses” are significantly more efficient than that of naturally occurring immu-nological synapses between TCRs and peptide MHC complexes[9].BiTEs may be able to circumvent certain common tu-
A Primer on Immuno-Oncology Part 2 - Targeted Redirection of T CellsSoo Kim, Mark Osterman, Shailesh Maingi
1
“[CAR-T cell] therapies offer novel
treatment options, but have yet to be fully
vetted for safety and efficacy.”

mor escape mechanisms such as loss of MHC Class I molecules or impaired antigen processing and/or transport; however, research into methods to increase the efficacy of BiTEs is ongoing and includes target antigen loss, expression of immune checkpoints (e..g PD1 or CTLA4), methods to increase T cell infil-tration into the tumor, and the immunosuppressive
tumor microenvironment. A combinatorial approach such as the use of BiTEs with immune checkpoint inhibitors may synergize and increase the efficacy of treatment[9]. BiTEs may have difficulty in reducing the size of a large tumor mass; however, BiTE treat-ment may be applied in a minimal residual disease or metastatic disease setting in order to kill the remain-ing population of cancer (stem) cells. In this setting, a combinatorial approach such as the addition of immune checkpoint inhibitors would be particularly useful to overcome the immunosuppressive tumor microenvironment[9].Blinatumomab, an anti-CD19 BiTE, has demon-strated clinical efficacy in Philadelphia chromosome-negative relapsed or refractory acute lymphoblastic leukemia, and received conditional approval by the FDA in 2014. Other BiTEs being developed in clini-cal trials include MT112, MT111, MED-565, AMG-330, AMG-110, AMG-211, and AMG-212.
Chimeric Antigen Receptor T Cells (CAR-T Cells)CAR StructureAnother strategy for redirecting T cells against can-cer cells is to engineer T cells to express a chimeric antigen receptor (CAR). CARs are composed of: 1) the scFv of a mAb fused to 2) a hinge/spacer region fused to 3) a transmembrane (TM) domain and 4) an intracellular signaling domain (ICD) which is able to activate the T cell. The scFv of a CAR directs CAR-T cells to tumor cells expressing the target neoantigen. Whereas T cell receptors traditionally recognize antigens on MHC Class I molecules, a CAR is able to recognize antigens in an MHC-independent manner[3]. In addition, CARs are able to recognize a wide variety of targets, including proteins, carbohydrates, ganglio-sides, proteoglycans, etc.[1]. The affinity of the scFv for its target may affect CAR-T cell function; low-affinity scFvs were shown to be specific for and sup-ported killing of tumor cells expressing high levels of antigen, but did not kill normal cells expressing low or normal levels of antigen[13]. This suggests that scFv affinity may be optimized based on antigen expression on tumor vs. healthy tissues to increase safety and targeting efficiency.
2
A Primer on Immuno-Oncology Part 2
BsAb Sponsor Targets ClinicalTrialIdentifier DiseasesBlinatumomab Amgen CD3×CD19 ApprovedinUSA ALL PhaseI,NCT00274742 RelapsedNHL PhaseII,NCT01207388 BcellALL PhaseII,NCT01209286 Relapsed/refractoryALL NationalCancer
Institute PhaseI,NCT02568553 NHL
PhaseII,NCT02143414 AdultB-ALLwitht(9;22)(q34;q11.2);BCR-ABL1;
untreatedadultALL PhaseIII,NCT02003222 BCR-ABL-negativeBlineageALLSolitomab(MT110,AMG110)
Amgen CD3×EpCAM CompletedphaseI,NCT00635596
Solidtumors
AMG330 Amgen CD33×CD3 PhaseI,NCT02520427 Relapsed/refractoryAMLMT112(BAY2010112)
Bayer PSMA×CD3 PhaseI,NCT01723475 Prostaticneoplasms
MT111(MEDI-565) MedImmune CEA×CD3 CompletedphaseI,NCT01284231
Gastrointestinaladenocarcinomas
BAY2010112 Bayer CD3×PSMA PhaseI,NCT01723475 ProstaticneoplasmsMEDI-565 MedImmune CEA×CD3 Completedphase
I,NCT01284231
Gastrointestinaladenocarcinomas
Table 1. BiTEs in Clinical Trials[12].

3
The scFv of CARs are typically derived from murine immunoglobulins; this may result in an immune re-sponse, and binding of human anti-mouse Abs to the CAR may block antigen recognition by the CAR[1]. The spacer/hinge domain of a CAR joins the scFv to the T cell membrane and is commonly derived from IgG subclasses or CD8; IgG1 is most commonly used, although not all CAR-T cells utilize a spacer/hinge domain[1]. Membrane-proximal epitope binding requires the use of a spacer/hinge domain; however, they have been found to reduce CAR-T cell function when the epitope is expressed near the amino terminal portion of the target antigen[14]. The spacer/hinge domain of a CAR affects CAR func-tion; the distance between the CAR-T cell and the cancer cell is determined by the position of the target epitope and the length of the spacer region. This distance affects tumor recognition and T cell cyto-kine production and proliferation, as well as synapse formation between the CAR-T cell and the target cancer cell[15].The transmembrane (TM) domain affects CAR expression on the cell surface, using a CD28 TM do-main has been shown to result in high expression of the CAR as compared to the CD3ζ TM domain[16].There have been multiple iterations of improved CAR design based on upgrading the intracellular signaling domain (ICD). First generation CARs pos-sessed only the ICD of the CD3ζ chain and lacked in vivo efficacy. This led to the creation of second and third generation CARs, which added on single or multiple co-stimulatory molecules, respectively, such as OX40, CD28ζ or 4-1BBζ to improve CAR signaling, cytokine production, and T cell prolifera-tion, differentiation, and survival[17]. Different co-stimulatory domains may be utilized for to achieve different results; the use of CARs with CD28ζ demonstrated increased IL-2 production and cyto-toxicity, whereas CARS containing 4-1BBζ demon-strated improved persistence in vitro[18, 19]. A CAR containing CD28 and OX40 demonstrated increased survival of the CAR-T cells, as compared to a CAR-T cell containing only CD28[20]. ICOS is a co-stimulatory receptor involved in TH17 polarization; integration of ICOS into the ICD of a CAR resulted in increased in vivo persistence of TH17-polarized CAR-T cells, compared to CAR-T cells containing CD28 or 4-1BB[21]. Duong et al. assessed the anti-tumor activity of various CAR-T cells with differing
costimulatory domains, and found that using DAP10 and CD27 with CD3ζ produced CAR-T cells with the greatest antitumor activity[22].Each component of the CAR plays a unique role which affects the performance of the CAR and the CAR-T cells Different indications may require their own unique combination of scFv, hinge, transmem-brane, ICD, and co-stimulatory domains to achieve efficacy[23].
In addition to engineering the “right” CAR, efficient delivery and persistent expression of the CAR is crucial for achieving clinical efficacy. The T cell population must be isolated, stimulated, expanded, transduced with the CAR, and then reintroduced into the patient, ideally following lymphodepletion pre-conditioning in order to maximize CAR T-cell expan-sion and engraftment[3].
CAR-T Cell ProductionMethods for introducing the CAR transgene into T cells include nonviral gene transfer for DNA plasmids, in vitro transcribed mRNA species, or viral-mediated transduction. Initially, nonviral DNA transfection was used to produce CAR-T cells due to its low immunogenicity and low risk of insertional mutagenesis. However, cells produced using this
A Primer on Immuno-Oncology Part 2
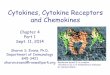
Figure 1. Evolution of CAR Signaling Capacities[4]. First generation CARs transmitted activating signals only via ITAM-bearing signaling chains like CD3ζ or FcεRIγ, licensing the engrafted T cells to eliminate tumor cells. Second generation CARs contain an additional costimulatory domain (CM I), predominantly the CD28 domain. Signaling through these costimula-tory domain leads to enhanced proliferation, cytokine secretion, and renders engrafted T cells resistant to immunosuppression and induction of AICD. Recent developments fused the intracellular part of a second costimulatory molecule (CM II) in addition to CD28 and ITAM-bearing signaling chains, thus generating tripartite signaling CARs. T cells engrafted with third genera-tion CARs seem to have superior qualities regarding effector functions and in vivo persistence.

4
method were short-lived[1]. Now, almost all stud-ies of CAR-T cells have utilized retroviral vectors such as gamma-retroviral and lentiviral vectors to introduce the CAR gene into T cells[24]. Both of these methods are able to efficiently and permanently transduce T cells, and lentiviral vectors are also able to transduce nondividing cells. T cells are usually activated with either anti-CD28 Ab, Ab costimula-tion, or coculture with peripheral blood
mononuclear cells (PBMCs) derived from antilo-gous patients or donors[1]. IL-2 is typically used to induce T cell expansion ex vivo, however, other cytokines such as IL-7, IL-15, or IL-21 may be used to modify the T cells for the desired effector func-tion.Research has shown that the addition of IL-7 and IL-15 resulted in CAR-T cells with a more favorable T memory stem cell phenotype[25]. After removing and selection for a subpopulation of T cells from the patient, expanding the cells, and transducing them with a CAR gene, the cells are infused back into the patient. The dosage of cells given to cancer patients has typically been up to 10^11 T cells.
CAR-T Cell TargetsThe most studied and successful target for CAR-T cell therapy has been CD19. CD19 is an ideal target because it is expressed by most B cell malignan-cies, but not in normal tissues and has been targeted
for the treatment of acute lymphoblastic leukemia (ALL), chronic lymphoblastic leukemia (CLL), mul-tiple myeloma (MM), and lymphoma[1]. Trials using CAR-T cell therapy have had differing outcomes which were affected by the CAR-T cell strategy used, but the exact effect these differences had remain unclear. Differences include vector de-sign (e.g. the use of a CD28/CD3ζ signaling domain vs. a 4-1BB/CD3ζ signaling domain), the manufac-turing process, conditioning chemotherapy strategy,
the timing of CAR-T cell infusion, and CAR-T cell dosage and derivation[26]. For example, a trial targeting Her-2 failed due to “on-target, off-tumor”
effects caused by low-level expression of Her-2 on normal lung epithelium; in addition, the high dose of CAR-T cells may have precluded a potential therapeutic window[27]. Another trial targeting Her-2 (for a different indication) used a different scFv, administered a lower dose of CAR-T cells, and did not co-administer IL-2 or use lymphodepleting chemotherapy prior to transfusion. Patients in this study did not experience any toxicity, and some pa-tients exhibited stable disease or partial response[28]. These two trials show the importance of mAb selec-tion, CAR generation, target distribution, and host preconditioning[27].
“Armored” CAR-T CellsCAR-T cells may lose their cytotoxic ability in the immunosuppressive tumor microenvironment, much
like endogenous T cells. This has been shown in vivo; injection of CAR-T cells into mice bearing large solid tumors resulted in the upregulation of the T cell inhibitory enzymes diacylglycerol
“The most studied and successful target for
CAR-T cell therapy has been CD19. CD19
is an ideal target because it is expressed
by most B cell malignancies, but not in
normal tissues...”
A Primer on Immuno-Oncology Part 2
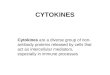
Figure 2. Overview of CAR Adoptive Cell Transfer[3]. T cells are collected via apheresis, expanded ex vivo and genetically modified to express a desired CAR construct before they are infused back into the patient.

kinase and SHP-1, as well as upregulation of immune checkpoint receptors such as PD1, ultimately leading to an inability to kill the tumor[29]. Modifying CAR-T cells to express immune-modulatory proteins, such as cytokines and ligands, represents one strategy to overcome the immunosuppressive tumor microenvi-ronment. One such method is to fuse the PD-1 extra-cellular receptor domain to the CD28 intracellular sig-naling domain. CAR-T cells may also be engineered to constitutively express stimulatory ligands such as CD40L or 4-1BBL. CD40L enhances the immunoge-nicity of CD40+ tumor cells, and stimulates dendritic cells[30]; 4-1BBL binds to T cell co-stimulatory receptors and stimulates the transduced cells, as well as adjacent T cells[31]. One other method includes engineering CAR-T cells to secrete pro-inflammatory cytokines such as IL-2, IL-15, and IL-12[32]. Hoyos et al. found that CAR-T cells expressing IL-15 and a suicide gene had increased proliferation, reduced PD-1 expression, and resulted in increased antitumor activ-ity in a mouse model of B-cell lymphoma[33]. While systemic administration of IL-12 has been shown to be toxic, local administration via CAR-T cells engineered to secrete IL-12 may provide the beneficial effects of IL-12 without systemic toxicity[32]. Localized administration of IL-12 via CAR-T cells has been shown to remove the need for preconditioning che-motherapy, enhance CAR-T cell persistence, provide resistance to Treg cell and MDSC mediated inhibition, and increase antitumor efficacy[34-36]. A clinical trial (NCT02498912) using CAR-T cells which secrete IL-12 for the treatment of ovarian cancer is currently ongoing.
Key Companies and Collabora-tions in the CAR-T Cell Therapy Space[37]Table 2 shows a list of companies and assets in the CAR-T cell space. Major players are discussed below.
NovartisIn 2015, Novartis and UPenn showed success in a trial of CTL019, a CAR-T cell therapy targeting CD19, for the treatment of acute lymphoblastic leukemia (ALL).
They reported a 92% remission rate, with a six-month duration of response of 76% and six-month event-free survival rate of 70%. In another study for diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma, they reported an overall response rate at 3 months of 47% for DLBCL and 73% for follicular lymphoma. Novartis plans on filing a marketing application for CTL019 for the treatment of pediatric relapsed/refrac-tory ALL in 2017. In early September 2016, Novartis closed down its Cell and Gene Therapy Unit. However, Novartis released a statement saying that they will continue to develop their CAR-T cell therapies and plans to sub-mit CTL019 for FDA approval to treat relapsed/refrac-tory B-cell ALL early this year. In addition, Novartis stated that they planned to submit KTE-C19 for EMA approval in 2017 as well, having already received the Agency’s PRIME (Priority Medicines) designation which may speed up the time needed for review and approval.
Juno TherapeuticsJuno, in partnership with Memorial Sloan Ketter-ing, reported positive results from their trial of their CD19 targeted CAR-T cell therapy, JCAR015, for the treatment of adult relapsed/refractory ALL. They reported an 82% complete response, and minimal residual disease-negative complete response in 83% of those patients. JCAR014 also had positive re-sults, with a 93% complete response rate in patients receiving monotherapy, and 100% complete response rate in patients who received JCAR014 with fludara-bine. JCAR015 was in a Phase II clinical trial with cyclophosphamide preconditioning for the treatment of all – however, recently, Juno halted this trial due to several patient deaths from cerebral edema. The trial had been previously halted by the FDA due to patient deaths, but was resumed with a modified preconditioning regimen which Juno asserted would minimize patient deaths. This most recent hold on the trial was imposed by Juno themselves, rather than by the FDA. In March 2017, Juno announced that they were permanently halting all future development of JCAR015, and will instead focus on developoing their other CAR-T cell therapy products such as JCAR016, JCAR018, and JCAR014, which are being developed for other blood cancers such as acute myeloid leu-kemia and chronic lymphocytic leukemia. This puts Juno behind rivals Kite Pharma and Novartis.
5
“...local administration (of IL-12) via CAR-T cells engineered to secrete IL-12 may provide the beneficial effects of IL-12 without systemic toxicity.”
A Primer on Immuno-Oncology Part 2

6
A Primer on Immuno-Oncology Part 2
Company AcademicCenter ProjectName Antigen Co-stim Transfection ScFv SuicideGene Addedfeature(s)Aurora BaylorCollegeofMedicine AU105 Her2 CD28 retrovirus murine none –Autolus UniversityCollege,London 1RG-CART GD2 CD28 unknown unknown suicidegene
cassette–
Bellicum BaylorCollegeofMedicine BPX-601 PSCA none(1st-gen)
retrovirus murine none GoCAR-separateinducibleMyD88/CD40
BluebirdBio&Celgene
BaylorCollegeofMedicine bb2121 BCMA 4-1BB lentivirus murine none –
BluebirdBio UppsalaUniversity 3rd-genCD19CAR
CD19 CD28&4-1BB
retrovirus unknown none –
BluebirdBio BaylorCollegeofMedicine CD30.CAR CD30 CD28 gamma-retro-virus
murine none –
Cellectis,Pfizer&Servier
UniversityCollege,London UCART19 CD19 4-1BB lentivirus murine RQR8 TCRα&CD52knockout;allogeneic
CellularTherapeuticsLtd
ChristieHospitalNHSFoundationTrust
aCD19z CD19 none(1st-gen)
retrovirus murine none –
CellularTherapeuticsLtd
CancerResearchUK anti-CEAMFEz CEA none(1st-gen)
unknown murine none –
Juno FredHutchinson&NCI JCAR014 CD19 4-1BB lentivirus murine EGFRt –Juno MemorialSloanKettering JCAR015 CD19 CD28 gamma-
retrovirusmurine none –
Juno SeattleChildren’sHospital JCAR017 CD19 4-1BB lentivirus murine EGFRt defined-compositionproduct
Juno,viaOpusBio NCI JCAR018 CD22 4-1BB lentivirus human none –Juno SeattleChildren’sHospital JCAR023 L1CAM
(=CD171)4-1BB lentivirus murine EGFRt –
Juno MemorialSloanKettering JCAR020 MUC16 CD28 gamma-retrovirus
fullyhuman
EGFRt IL12-secreting“armoredCAR”
Juno FredHutchinsonCancerCenter
JCAR024 ROR1 4-1BB retrovirus rabbit EGFRt mightbeCD4+:CD8+definedcellproduct
KitePharma ZeligEshhar(CabaretBiotech)
KTE-C19 CD19 CD28 gamma-retrovirus
murine none –
KitePharma NCI Anti-EGFRvIIICAR
EGFRvIII CD28 gamma-retrovirus
murine none –
LeucidBio King'sCollegeLondon LEU-001(T1E28z)
ErbBdimers
CD28 gamma-retrovirus
murine none IL4receptortoaidexpansion
Mustang(FortressBio)
CityofHopeMedicalCenter
MB-102 CD123 CD28 lentivirus murine EGFRt –
Mustang(FortressBio)
CityofHopeMedicalCenter
MB-101 IL13Rα2 4-1BB lentivirus murine truncatedCD19
–
Novartis UniversityofPennsylvania CART-BCMA BCMA 4-1BB lentivirus murine none –
Novartis UniversityofPennsylvania CTL019 CD19 4-1BB lentivirus murine none –Novartis UniversityofPennsylvania CTL119 CD19 4-1BB lentivirus humanised none –Novartis UniversityofPennsylvania CART22cells CD22 4-1BB lentivirus murine none –Novartis UniversityofPennsylvania CART-
EGFRvIIIEGFRvIII 4-1BB lentivirus murine none –
Novartis UniversityofPennsylvania CART-meso mesothelin 4-1BB lentivirus murine none –Ziopharm,Intrexon&MerckKGaA
MDAndersonCancerCenter
CD19CAR CD19 CD28 SleepingBeauty
murine none Includesdonor-derivedmatchedallo”
Table 2. Clinical-Stage CAR-T Projects with Commercial Licensees (Excluding China)[38].

7
A Primer on Immuno-Oncology Part 2
In May 2015, Juno partnered with Editas to utilize their CRISPR/Cas9 technology to develop Juno’s CAR-T cell therapies. Juno paid Editas an up-front payment of $25M, with additional milestone pay-ments. In April 2016, Celgene partnered with Juno to develop JCAR015, JCAR014, and JCAR017. Cel-gene paid $150M in an up-front payment to Juno, plus an $864M equity stake. The deal gave Celgene com-mercial rights outside of North America and China. After the most recent halt of Juno’s JCAR015 trial in ALL due to patient deaths, shares of Juno’s stock have plummeted by ~30%.
Kite PharmaKite has a cooperative research and development agreement with the NCI surgery branch to develop KTE-C19, their CD19 targeted CAR-T cell therapy product. In their phase I trial (ZUMA-1) of KTE-C19 for the treatment of DLBCL, they reported an overall response rate of 71% after treatment with KTE-C19. Furthermore, treatment durability was higher than expected, the number of patients in complete remis-sion remained unchanged from 3mo to 6mo post-study. KTE-C19 is currently in Phase II clinical trials, and has received Breakthrough Therapy Designation and Orphan Drug status from the U.S. Food and Drug Administration for the treatment of patients with chemorefractory DLBCL, primary mediastinal B-cell lymphoma, and transformed follicular lymphoma. The European Medicines Agency has also granted KTE-C19 access to regulatory support under its Priority Medicines (PRIME) initiative for the treatment of DLBCL and Orphan Drug Designation for various hematological indications. Unlike the Juno trials, Kite has not seen any patient deaths from cerebral edema, but one patient did die from KTE-C19 related cytokine release syndrome and another from a fungal infection unrelated to KTE-C19. In December 2016, Kite initiated a rolling submission of the US FDA Biologics License Application (BLA) for KTE-C19,
and announced the US Adopted Name for KTE-C19, “axicabtagene ciloleucel”.Other notable collaborations with Kite include Adimab for the discovery and optimization of fully humanized Abs against CAR targets, Alpine Immune Sciences to use their AIS Transmembrane Immunomodulatory Protein Technology for Kite’s CAR-T cell program, Amgen to utilize their oncology targets, Cell Design Labs to use their suicide switch in CAR-T cells, Genentech for a clinical trial utilizing both KTE-C19 CAR-T cell product and atezolizumab (Genentech’s anti-PDL1 Ab), the Leukemia and Lymphoma Society to develop KTE-C19, and the Tel-Aviv Sourasky Medical Center to develop CAR-T cell products.
Bluebird BioBluebird and Celgene, along with Baylor College of Medicine, entered into a collaboration to treat multiple myeloma using CAR-T cells by targeting the B-cell maturation antigen (BCMA), which is expressed on the surface of most multiple myeloma cells. Celgene and Bluebird reached a deal wherein Cel-gene agreed to pay $225M in milestone payments to Bluebird, and Celgene has an option to exclusive rights to any BCMA related CAR-T cell therapies. In May 2015, Bluebird entered into an exclusive license agreement with Five Prime to research, develop, and commercialize Juno’s CAR-T cell therapies using Five Prime’s proprietary lentiviral gene therapy platform and proprietary human Abs to an undisclosed can-cer target for hematological malignancies and solid tumors. Five Prime received $1.5M up-front, with subsequent milestone payments totaling up to over $130M per licensed product, as well as tiered royal-ties to Five Prime. In December 2015, ViroMed and Bluebird entered into an exclusive license agreement to research, develop, and commercialize CAR-T cell therapies using ViroMed’s proprietary humanized Ab to an undisclosed cancer target for solid tumors. ViroMed received an up-front payment of $1M with milestone payments of up to $48M and tiered royal-ties. Bluebird started their first CAR-T clinical trial for bb2121 (NCT02658929) targeting BCMA for the treatment of multiple myeloma in February 2016. Preliminary results showed an overall response rate of 78% with no grade 3 or higher neurotoxicities or cytokine release syndrome resulting from treatment.
“In March 2017, Juno announced that they were permanently halting all future development of JCAR015, and will instead focus on developoing their other CAR-T cell therapy products
such as JCAR016, JCAR018, and JCAR014, which are being developed for other blood cancers such as acute myeloid
leukemia and chronic lymphocytic leukemia. This puts Juno behind rivals Kite Pharma and Novartis.”

8
A Primer on Immuno-Oncology Part 2
CellectisIn 2014, Pfizer and Cellectis entered into a global strategic collaboration to develop Cellectis’ CAR-T cell therapies. Cellectis received an up-front payment of $80M and up to $185M in milestone payments, as well as tiered royalties. The deal gave Pfizer exclusive rights to pursue development and commercialization of CAR-T cell therapies directed towards 15 targets selected by Pfizer. In 2015, Pfizer obtained the rights to Cellectis’ UCART19 CAR-T cell therapy through an intermediary, Servier. Servi-er paid Cellectis $38M in an up-front payment, with up to $300M in milestone payments, for global rights to UCART19. Shortly after the deal was reached, Servier sold the US rights to Pfizer for an undis-closed sum. UCART19 is an off-the-shelf CAR-T cell therapy which uses allogeneic cells rather than the patient’s own cells, Cellectis is the only company to utilize this allogeneic approach.
ChallengesImmunogenicityCAR-T cells may elicit severe toxicities; thus, safety is a major concern. CARs have mostly been derived from mouse Abs, and both Ab and T cell responses against CARs have been reported in clinical tri-als[39]. In order to minimize the immunogenicity of CAR-T cells, one may utilize humanized or fully human Abs[40].
Increasing Engraftment and SurvivalInfused CAR-T cells must survive and also possi-bly proliferate in order to exert therapeutic efficacy and disease clearance. Choosing a specific popula-tion of T cells for transducing the CAR gene may offer certain benefits; CD19-specific CD8+ central memory T-enriched cells expressing naïve markers such as CD62L may have improved engraftment as compared to effector/more differentiated T cells[41]. Alternatively, using cytokines such as IL-12 may increase T cell proliferation and survival. CAR-T cells engineered to express IL-12 were shown to retain a central memory effector phenotype and had increased antitumor activity[42]. Similarly, CAR-T cells expressing IL-15 were shown to have increased persistence and no loss of antitumor activity[33].
Solid TumorsAlthough CAR-T cell therapy was first utilized to
treat solid tumors, most of the successes of CAR-T cell therapy has been from the treatment of he-matological malignancies[43]. Trials using first generation CAR-T cells for the treatment of solid tumors mostly failed to achieve an effective antitu-mor response[1]. However, HER2.CD28ζ CAR-T cells have showed some success in clinical trials for HER2+ sarcoma: four patients experienced disease stabilization for 12wks – 14mos[28]. Challenges for the treatment of solid tumors using CAR-T cell therapy includes inefficient tumor targeting, the ab-sence of unique TAA, the immunosuppressive tumor microenvironment, and limited persistence of CAR-T cells[1]. Approaches for addressing these challenges, and others, are discussed below.
SpecificityOne major concern of CAR-T cell therapy is “on-target, off-tumor” toxicity[1]. This refers to CAR-T cells targeting normal, healthy tissues which express low or normal levels of the target antigen, resulting in immune-mediated destruction of healthy tissues. One such example is the development of B-cell aplasia in patients receiving CD-19 targeted CAR-T cells[44]. Mutated tumor antigens may be targeted to minimize “on-target, off-tumor” toxicity as they are expressed only on cancer cells; these include EGFRvIII, EphA2 epitopes, and tumor-specific glycosylation patterns of MUC-1[43]. Recently, re-searchers at the University of Pennsylvania have tar-geted truncated carbohydrate molecules on MUC-1 protein, which is not expressed on healthy tissue, but is expressed on cancer cell’s surface of many types of solid tumors and leukemias. Their efforts showed antitumor efficacy in a mouse model of pancreatic cancer and leukemia.
“One major concern of CAR-T cell
therapy is “on-target, off-tumor” toxicity. This refers to CAR-T cells targeting
normal, healthy tissues which express low or normal levels of the target antigen, resulting in immune-mediated
destruction of healthy tissues.”

9
A Primer on Immuno-Oncology Part 2
Another strategy to increase the specificity of CAR-T cells is to engineer CAR-T cells to express ad-ditional receptors. Chemokines have been shown to play a role in influencing lymphocyte migration; thus engineering T cells to express certain chemokine receptors may alter the migration pattern of the T cells so that they traffic to those tumor chemokine recep-tors[1]. CAR-T cells specific for CD30 (Hodgkin’s Lymphoma) were engineered to express CCR4, result-ing in increased localization to the tumor site[45]. Similarly, in a strategy targeting the tumor stroma, CAR-T cells have also been engineered to express CCR2b for neuroblastoma[46] and VEGFR2 which is expressed in tumor blood vessels[35]. Targeting the tumor stroma via targets such as VEGFR2 or FAP has shown antitumor efficacy[43]. In addition, inducing expression of heparanase in CAR-T cells has been shown to improve their ability to degrade the extracel-lular matrix of tumors, and increase their infiltration into tumors without affecting CAR-T cells’ viability, expansion, or effector function while increasing antitu-mor efficacy[47].
Recent research has shown that bispecific CARs, which require binding to two distinct antigens, may have increased safety while maintaining antitumor efficacy[48]. In this strategy, the activating and co-stimulatory domains are separated onto two separate CARs located on one T cell. Binding to just one of the target antigens does not result in activation of the CAR-T cell; rather, the CAR-T cell must bind to both target antigens in order to become activated. In a similar strategy used to increase the safety of CAR-T cells, two CARs are again used, with one CAR specific for an antigen expressed by normal tissues and conjugated to a suppressive domain. Binding of this inhibitory, bispecific CAR (iCAR to normal, healthy tissue results in inhibition of T cell function, and thus increased safety[49].Local delivery may also be utilized to deliver CAR-T cells to tumors. Intra-tumoral delivery of CAR-T cells targeted towards ErbB for head and neck squamous cell carcinoma is currently in Phase I clinical trial. Ovarian cancer and malignant pleural mesothelioma may also be candidates for local delivery of CAR-T cells as they possess a propensity for localized dis-semination within peritoneal and pleural cavities[43].
Immunosuppressive Tumor Microenviron-mentAfter CAR-T cells are infused into the patient, they must infiltrate the tumor and the tumor microenvi-ronment in order to exert their therapeutic effect. The tumor microenvironment possesses a variety of immunosuppressive factors used to defeat the host’s immune system response to the tumor and can limit the efficacy of CAR-T cell therapy. Thus, researchers have explored different methods for overcoming the immunosuppressive tumor microenvironment. One such method is engineering CAR-T cells to express a dominant-negative form of TGFβ receptor in order to overcome the inhibitory effects of TGFβ[50]. CAR-T cells have also been engineered to target NKG2D in order to recognize NKG2D ligands expressed by im-munosuppressive cells[1]. Granulocyte-macrophage colony-stimulating factor (GM-CSF) has been shown to be secreted at high levels by tumor cells in vivo and is implicated in myeloid-derived suppressor cells’ (MDSCs) recruitment. MDSCs have been shown to expand in response to liver metastases and inhibit the antitumor efficacy of CAR-T cells; thus,
Figure 4. Schematic Representation of the Chimeric Antigen Receptor (CAR) Structure[1]. A) CAR T-cells redirected for universal cytokine killing (TRUCKs) employ a vector encoding the CAR construct that also possesses a cytokine expression cassette. These cytokines such as IL-12 can ef-fectively recruit other components of the immune system to enhance the antitumor immune response toward those cancer cells that are invisible to CAR T-cells. B) To increase the specificity of the CAR T-cells, T-cell signal 1 is separated from signal 2. Both target antigens that are expressed on tumor cells must be engaged to deliver signals 1 and 2 and fully activate CAR T-cells. Normal cells that express only one of two antigens do not signal T-cells sufficiently to accomplish full activation. C) A CAR that delivers a dominant inhibitory signal such as PD-1 and CTLA-4 is coexpressed with a CAR capable of full T-cell activation. Engaging both antigens on normal cells could inhibit T-cell function, whereas encountering only the activating ligand on tumor cells generates a sustained T-cell response. CAR = chimeric antigen receptor; CCR = chimeric costimulatory receptor; iCAR = inhibi-tory CAR.

10
A Primer on Immuno-Oncology Part 2
neutralization of GM-CSF may prevent MDSC expan-sion and increase the antitumor efficacy of CAR-T cells[43]. An alternative strategy is to use combinatorial therapy, CAR-T cell therapy may be used in conjunction with immune checkpoint inhibitors such as a PD-1 Ab[51] or a chimeric PD1-CD28 receptor, which can convert PD-L1 to a ligand, which transmits a CD28 costimu-latory signal to CD8+ T cells, thus enhancing their antitumor activity[52]. Conditioning chemotherapy (e.g. fludarabine and cyclophosphamide) may also be used to achieve resistance to immunosuppressive
factors such as indoleamine 2,3-dioxygenase[53]. In addition, “armored” CAR-T cells expressing cytokines such as IL-2, IL-12, IL-15 or TGFβ may also be used, this strategy has been discussed above.
ToxicityCAR-T cell therapy may result in cytokine release syndrome (CRS); this is caused by the production of pro-inflammatory cytokines such as IL-6, TNFα, and IFNγ by large numbers of activated T cells and is characterized by high fever, hypotension, hypoxia, and potentially results in organ failure[1]. Inhibition of IL-6 using the IL-6 receptor antagonist tocilizumab has been used to control severe CRS without affect-ing CAR-T cell therapy efficacy[54]. The severity of CRS may directly correlate with the tumor burden at the time of therapy; thus, treating patients with pre-infusion conditioning chemotherapy combined with intensive chemotherapy to reduce the tumor burden
may significantly reduce the risk of severe CRS[55].On-target, off-tumor toxicity and strategies for mitigat-ing such toxicity has been discussed above. The use of safety switches or suicide genes to avoid T cell medi-ated toxicity is discussed below.
Safety SwitchesIn the event of T-cell mediated toxicity, elimination of the CAR-T cells from the circulation would be useful. For this purpose, safety switches may be engineered into the CAR-T cells. Early approaches used ex-pression of a protein which metabolized an inactive prodrug into a cytotoxic metabolite to kill the CAR-T cells. In a later approach, a membrane bound protein was expressed on the surface of CAR-T cells, and an Ab against that protein was used to deplete cells expressing that protein[56]. Recently, the inducible caspase-9 (iCasp9) system has
been utilized for this purpose. This system uses an incomplete pro-apoptotic caspase-9 lacking its caspase recruitment domain fused to a mutated peptide derived from FKBP12 protein. When the mutated FKBP12 domain interacts with a specific small molecule, it induces dimerization of the fusion protein and, subsequently, activates caspase-9 induced apopto-sis[57]. Wu et al. presented another approach in which they produced a dissociated CAR, with one protein possessing the antigen binding and transmembrane
domains, and another protein with the intracellular signaling domains[58]. Both of the subunits also pos-
sess a heterodimerization module which assembles the CAR into one fully functional unit in the presence of a specific small molecule; thus this CAR-T cell requires both antigen binding and the dimerizing agent to be present in order to activate the T cell, allowing for both real-time and dose-dependent control of CAR-T cell activity[56].
Choosing the Right TherapyAs tumor cells evolve, they are eliminated from the body by immune surveillance; in particular, by T cells responding to tumor neoantigen-derived peptides presented by MHCs. Certain types of tumors, such as melanoma or NSCLC, which have a high frequency of somatic mutations leading to an increased presenta-tion of neoantigens, and may be more likely to escape immune surveillance via co-evolution in the immuno-suppressive tumor microenvironment[32]. In addition, the immunosuppressive tumor microenvironment
inhibits CAR-T cell function, as discussed above. In this type of environment, inducing an immune-medi-ated antitumor response may best be achieved through
the use of immune-modulating mAbs such as anti-PD1
“CAR-T cell therapy may result in cytokine
release syndrome (CRS); this is caused by the production of pro-inflammatory cytokines such as IL-6, TNFα, and IFNγ by large numbers of activated T cells and
is characterized by high fever, hypotension,
hypoxia, and potentially results in organ
failure.”

11
A Primer on Immuno-Oncology Part 2
or anti-CTLA4 checkpoint inhibitors[32]. In tumors with low antigen presentation and a non-immunosup-pressive tumor microenvironment, immune modulat-ing mAbs may not be sufficient and instead, CAR-T cells may represent a more efficacious option. In tumors with a phenotype in between these extremes, a combinatorial approach may be most efficacious. In a preclinical model of sarcoma and breast cancer, PD-1 blockade alone or CAR-T cell therapy alone had significantly less antitumor response as compared to a combinatorial approach utilizing both strategies[51]. However, it should be noted that there is an increased risk of toxicity when utilizing a combinatorial ap-proach such as this. There is currently an ongoing clinical trial using a combination of CTLA-4 mAb and CAR-T cell therapy (NCT00586391).
Regulatory Considerations[59]CAR-T cells are unique in that they are somatic cells, and thus fall under the guidelines for cell therapy; however, they are also genetically modified, and thus also fall under the guidelines of gene therapy prod-ucts. Different nations have their own guidelines for clinical trials utilizing CAR-T cells, and herein we will discuss the US FDA and the EU EMA.The US FDA classifies CAR-T cells as 351 biologi-cal products regulated under “Considerations for the design of early-phase clinical trials of cellular and gene therapy products” and “Guidance for industry: preclinical assessment of investigational cellular and gene therapy products” (Nov. 2013, OCTGT CBER). CAR-T cell therapies should meet the CMC criteria under the “Guidance for FDA reviewers and sponsors: content and review of chemistry, manufac-turing, and control (CMC) information for human
somatic cell therapy investigational new drug (IND) applications” (Apr. 2008) and “Guidance for FDA reviewers and sponsors: content and review of chem-istry, manufacturing, and control (CMC) information for human gene therapy investigational new drug
applications (INDs).” The EU EMA issued a guideline, “Guideline on quality, non-clinical and clinical aspects of medici-nal products containing genetically modified cells” (2012). The guideline focuses on the quality, safety, and efficacy requirements of genetically modified cells to be used as a medicinal product. The manu-facture of CAR-T cells is regulated by the regula-tion on advanced therapy medicinal products No 1394/2007 and guidance on quality, preclinical and clinical aspects of gene transfer medicinal products (CPMP/BWP/3088/99).
Patent DisputesCAR-T cell therapies have been in development for decades, primarily in academic centers. However, now that the technology has begun to reach the com-mercialization stage, patent issues have arisen, al-though several disputes have recently been resolved. Juno settled a dispute with UPenn and Novartis in 2015 over a patent licensed from St. Jude Children’s Research Hospital. The settlement gave Juno and St. Jude’s $12.25M, plus future milestone payments and royalty payments on relevant CAR-T cell products.
ConclusionWhile CAR-T cell therapy is an exciting and growing field, challenges associated with CAR-T cell thera-pies, such as safety and toxicity, must be addressed prior to commercialization. Some strategies to miti-gate these challenges, such as bispecific CAR-T cells or armored CAR-T cells, have been discussed in this report. In addition, before CAR-T cell therapies can reach the market, patent disputes over CAR-T cell therapy products must be resolved and may require cross-licensing deals between academic groups and corporations, as companies in the CAR-T cell space often own technologies for just one part of CAR-T cell therapies (such as gene editing technology or a suicide switch). This hints at the possibility, or even the necessity, of more deals between pharma and biotech companies in this space. Mark Osterman, Senior VP at Kineticos, recently published a Kineti-cos Insight regarding the movement of innovation away from big pharma to smaller biotech/pharma companies. Similarly, companies in the CAR-T cell space may follow such a trend, with smaller biotech companies that possess the rights for one compo-nent of CAR-T cell therapies being acquired by or
“CAR-T cells are unique in that they are somatic cells, and
thus fall under the guidelines for cell therapy; however, they are also genetically modified, and thus also fall under the guidelines of gene therapy products.”

12
A Primer on Immuno-Oncology Part 2
licensing the rights to big pharma, who is then able to further develop and commercialize the technol-ogy. Such a trend may foster increased innovation by encouraging the growth and conception of smaller, novel, and innovative biotech companies, ultimately leading to improved therapies.

13
A Primer on Immuno-Oncology Part 2
References1. Dai, H., et al., Chimeric Antigen Receptors Modified T-Cells for Cancer Therapy. J Natl Cancer Inst, 2016. 108(7).2. Guo, Y., Y. Wang, and W. Han, Chimeric Antigen Receptor-Modified T Cells for Solid Tumors: Challenges and Prospects. J Immunol Res, 2016. 2016: p. 3850839.3. Frigault, M.J. and M.V. Maus, Chimeric antigen receptor-modified T cells strike back. Int Im-munol, 2016. 28(7): p. 355-63.4. Cartellieri, M., et al., Chimeric antigen receptor-engineered T cells for immunotherapy of cancer. J Biomed Biotechnol, 2010. 2010: p. 956304.5. Zhukovsky, E.A., R.J. Morse, and M.V. Maus, Bispecific antibodies and CARs: generalized immunotherapeutics harnessing T cell redirection. Curr Opin Immunol, 2016. 40: p. 24-35.6. Nagorsen, D. and P.A. Baeuerle, Immuno-modulatory therapy of cancer with T cell-engaging BiTE antibody blinatumomab. Exp Cell Res, 2011. 317(9): p. 1255-60.7. Offner, S., et al., Induction of regular cytolyt-ic T cell synapses by bispecific single-chain antibody constructs on MHC class I-negative tumor cells. Mol Immunol, 2006. 43(6): p. 763-71.8. Haas, C., et al., Mode of cytotoxic action of T cell-engaging BiTE antibody MT110. Immunobiol-ogy, 2009. 214(6): p. 441-53.9. Klinger, M., et al., Harnessing T cells to fight cancer with BiTE(R) antibody constructs--past devel-opments and future directions. Immunol Rev, 2016. 270(1): p. 193-208.10. Bluemel, C., et al., Epitope distance to the target cell membrane and antigen size determine the potency of T cell-mediated lysis by BiTE antibodies specific for a large melanoma surface antigen. Cancer Immunol Immunother, 2010. 59(8): p. 1197-209.11. Hoffmann, P., et al., Serial killing of tumor cells by cytotoxic T cells redirected with a CD19-/CD3-bispecific single-chain antibody construct. Int J Cancer, 2005. 115(1): p. 98-104.12. Fan, G., et al., Bispecific antibodies and their applications. Journal of Hematology & Oncology, 2015. 8: p. 130.13. Caruso, H.G., et al., Tuning Sensitivity of CAR to EGFR Density Limits Recognition of Normal Tissue While Maintaining Potent Antitumor Activity. Cancer Res, 2015. 75(17): p. 3505-18.
14. Guest, R.D., et al., The role of extracellular spacer regions in the optimal design of chimeric im-mune receptors: evaluation of four different scFvs and antigens. J Immunother, 2005. 28(3): p. 203-11.15. Dustin, M.L. and D. Depoil, New insights into the T cell synapse from single molecule tech-niques. Nature reviews. Immunology, 2011. 11(10): p. 672-684.16. Pule, M.A., et al., A chimeric T cell antigen receptor that augments cytokine release and supports clonal expansion of primary human T cells. Mol Ther, 2005. 12(5): p. 933-41.17. Maher, J., et al., Human T-lymphocyte cyto-toxicity and proliferation directed by a single chimeric TCRzeta /CD28 receptor. Nat Biotechnol, 2002. 20(1): p. 70-5.18. Loskog, A., et al., Addition of the CD28 signaling domain to chimeric T-cell receptors en-hances chimeric T-cell resistance to T regulatory cells. Leukemia, 2006. 20(10): p. 1819-28.19. Milone, M.C., et al., Chimeric receptors con-taining CD137 signal transduction domains mediate enhanced survival of T cells and increased antileuke-mic efficacy in vivo. Mol Ther, 2009. 17(8): p. 1453-64.20. Hombach, A.A., et al., Adoptive immuno-therapy with redirected T cells produces CCR7- cells that are trapped in the periphery and benefit from com-bined CD28-OX40 costimulation. Hum Gene Ther, 2013. 24(3): p. 259-69.21. Guedan, S., et al., ICOS-based chimeric antigen receptors program bipolar TH17/TH1 cells. Blood, 2014. 124(7): p. 1070-80.22. Duong, C.P., et al., Engineering T cell func-tion using chimeric antigen receptors identified using a DNA library approach. PLoS One, 2013. 8(5): p. e63037.23. Gill, S. and C.H. June, Going viral: chime-ric antigen receptor T-cell therapy for hematological malignancies. Immunol Rev, 2015. 263(1): p. 68-89.24. Suerth, J.D., A. Schambach, and C. Baum, Genetic modification of lymphocytes by retrovirus-based vectors. Curr Opin Immunol, 2012. 24(5): p. 598-608.25. Xu, Y., et al., Closely related T-memory stem cells correlate with in vivo expansion of CAR.CD19-T cells and are preserved by IL-7 and IL-15. Blood, 2014. 123(24): p. 3750-9.

14
A Primer on Immuno-Oncology Part 2
26. Davila, M.L., et al., How do CARs work?: Early insights from recent clinical studies targeting CD19. Oncoimmunology, 2012. 1(9): p. 1577-1583.27. Spear, T.T., K. Nagato, and M.I. Nishimura, Strategies to genetically engineer T cells for cancer immunotherapy. Cancer Immunol Immunother, 2016. 65(6): p. 631-49.28. Ahmed, N., et al., Human Epidermal Growth Factor Receptor 2 (HER2) -Specific Chi-meric Antigen Receptor-Modified T Cells for the Immunotherapy of HER2-Positive Sarcoma. J Clin Oncol, 2015. 33(15): p. 1688-96.29. Moon, E.K., et al., Multifactorial T-cell hypofunction that is reversible can limit the efficacy of chimeric antigen receptor-transduced human T cells in solid tumors. Clin Cancer Res, 2014. 20(16): p. 4262-73.30. Curran, K.J., et al., Enhancing antitumor efficacy of chimeric antigen receptor T cells through constitutive CD40L expression. Mol Ther, 2015. 23(4): p. 769-78.31. Zhao, Z., et al., Structural Design of Engi-neered Costimulation Determines Tumor Rejection Kinetics and Persistence of CAR T Cells. Cancer Cell, 2015. 28(4): p. 415-28.32. Khalil, D.N., et al., The future of cancer treatment: immunomodulation, CARs and combina-tion immunotherapy. Nat Rev Clin Oncol, 2016. 13(6): p. 394.33. Hoyos, V., et al., Engineering CD19-specific T lymphocytes with interleukin-15 and a suicide gene to enhance their anti-lymphoma/leukemia ef-fects and safety. Leukemia, 2010. 24(6): p. 1160-70.34. Pegram, H.J., et al., Tumor-targeted T cells modified to secrete IL-12 eradicate systemic tumors without need for prior conditioning. Blood, 2012. 119(18): p. 4133-41.35. Chinnasamy, D., et al., Local delivery of in-terleukin-12 using T cells targeting VEGF receptor-2 eradicates multiple vascularized tumors in mice. Clin Cancer Res, 2012. 18(6): p. 1672-83.36. Kerkar, S.P., et al., IL-12 triggers a pro-grammatic change in dysfunctional myeloid-derived cells within mouse tumors. J Clin Invest, 2011. 121(12): p. 4746-57.37. Plieth, J., Not For the Faint of CAR-T: The CAR-T Landscape in 2015. 2015.38. Plieth, J.E., Edwin, Shifting CAR-Ts to a Higher Gear. 2016.
39. Lamers, C.H., et al., Immune responses to transgene and retroviral vector in patients treated with ex vivo-engineered T cells. Blood, 2011. 117(1): p. 72-82.40. June, C.H., S.R. Riddell, and T.N. Schum-acher, Adoptive cellular therapy: a race to the finish line. Sci Transl Med, 2015. 7(280): p. 280ps7.41. Wang, X., et al., Phenotypic and functional attributes of lentivirus-modified CD19-specific hu-man CD8+ central memory T cells manufactured at clinical scale. J Immunother, 2012. 35(9): p. 689-701.42. Pegram, H.J., et al., IL-12-secreting CD19-targeted cord blood-derived T cells for the immu-notherapy of B-cell acute lymphoblastic leukemia. Leukemia, 2015. 29(2): p. 415-22.43. Zhang, B.L., et al., Hurdles of CAR-T cell-based cancer immunotherapy directed against solid tumors. Sci China Life Sci, 2016. 59(4): p. 340-8.44. Kalos, M., et al., T cells with chimeric anti-gen receptors have potent antitumor effects and can establish memory in patients with advanced leuke-mia. Sci Transl Med, 2011. 3(95): p. 95ra73.45. Di Stasi, A., et al., T lymphocytes coex-pressing CCR4 and a chimeric antigen receptor targeting CD30 have improved homing and antitu-mor activity in a Hodgkin tumor model. Blood, 2009. 113(25): p. 6392-402.46. Craddock, J.A., et al., Enhanced tumor trafficking of GD2 chimeric antigen receptor T cells by expression of the chemokine receptor CCR2b. J Immunother, 2010. 33(8): p. 780-8.47. Caruana, I., et al., Heparanase promotes tumor infiltration and antitumor activity of CAR-redirected T lymphocytes. Nat Med, 2015. 21(5): p. 524-9.48. Kloss, C.C., et al., Combinatorial antigen recognition with balanced signaling promotes selec-tive tumor eradication by engineered T cells. Nat Biotechnol, 2013. 31(1): p. 71-5.49. Fedorov, V.D., M. Sadelain, and C.C. Kloss, Novel approaches to enhance the specificity and safety of engineered T cells. Cancer J, 2014. 20(2): p. 160-5.50. Foster, A.E., et al., Antitumor activity of EBV-specific T lymphocytes transduced with a dominant negative TGF-beta receptor. J Immunother, 2008. 31(5): p. 500-5.

15
A Primer on Immuno-Oncology Part 2
51. John, L.B., et al., Anti-PD-1 antibody therapy potently enhances the eradication of estab-lished tumors by gene-modified T cells. Clin Cancer Res, 2013. 19(20): p. 5636-46.52. Prosser, M.E., et al., Tumor PD-L1 co-stimulates primary human CD8(+) cytotoxic T cells modified to express a PD1:CD28 chimeric receptor. Mol Immunol, 2012. 51(3-4): p. 263-72.53. Ninomiya, S., et al., Tumor indoleamine 2,3-dioxygenase (IDO) inhibits CD19-CAR T cells and is downregulated by lymphodepleting drugs. Blood, 2015. 125(25): p. 3905-16.54. Grupp, S.A., et al., Chimeric antigen recep-tor-modified T cells for acute lymphoid leukemia. N Engl J Med, 2013. 368(16): p. 1509-18.55. Maude, S.L., et al., Chimeric antigen recep-tor T cells for sustained remissions in leukemia. N Engl J Med, 2014. 371(16): p. 1507-17.56. Abate-Daga, D. and M.L. Davila, CAR models: next-generation CAR modifications for en-hanced T-cell function. Mol Ther Oncolytics, 2016. 3: p. 16014.57. Fan, L., et al., Improved artificial death switches based on caspases and FADD. Hum Gene Ther, 1999. 10(14): p. 2273-85.58. Wu, C.Y., et al., Remote control of thera-peutic T cells through a small molecule-gated chime-ric receptor. Science, 2015. 350(6258): p. aab4077.59. Wang, W., et al., Establishing guidelines for CAR-T cells: challenges and considerations. Sci China Life Sci, 2016. 59(4): p. 333-9.

16
Authors
3005 Carrington Mill BlvdSuite 510Morrisville, NC 27560Office: 919.678.3206Email: [email protected]
www.kineticos.com
Soo Kim, PhDAnalyst
Kineticos
About KineticosKineticos is a specialized management consulting firm serving the life science industry. The firm is focused on identifying opportunities to drive strategic growth and achieve operational excellence for it clients.
Through its three practice areas - Biopharmaceutical, Biopharmaceutical Services, and Diagnostics - Kineticos has experience working with companies across the life science industry ecosystem.
Dr. Kim recently graduated from the Eshelman School of Pharmacy, Division of Molecular Pharmaceutics at UNC–Chapel Hill. His research involved a novel approach to formulating exosomes, nano-sized extracellular vesicles used in intracellular communication, to deliver poorly soluble anticancer drugs for the treatment of pulmonary metastases.
Prior to earning his PhD, Dr. Kim received a BS in Biology from UNC–Chapel Hill.
A Primer on Immuno-Oncology Part 2
Mark OsternanSenior Vice President
Kineticos
Mr. Osterman adds more than 25 years of experience in the biopharmaceutical industry to the team.
Mr. Osterman held roles in sales, clinical, and marketing at GlaxoSmithKline before moving to Johnson & Johnson, where he launched their stem cell internal venture and was responsible for the cardiovascular, pulmonary, metabolic, and mimetibody therapeutic areas in the Global Biologic Strategic Marketing.
Mr. Osterman earned a dual BA in Business Management and Economics from North Carolina State University.
Shailesh MaingiFounder and CEO
Kineticos
Mr. Maingi founded Kineticos Life Sciences in 2012 and develops long-term and day-to-day execution strategies.
Mr. Maingi serves on the Board of Directors at Gallus Biopharmaceutical and he serves on the advisory boards of Novolipid and Enci Therapeutics.
Prior to founding Kineticos Life Sciences, Mr. Maingi was a senior executive at Cardinal Health/PTS and Sigma-Aldrich/Supelco, where he held leadership roles in strategy, business development, and marketing.