Embed Size (px)
Citation preview
A Practical Approach to the Diagnosis and Treatment of Vitiligo in ChildrenKhaled Ezzedine, MD, PhD, a Nanette Silverberg, MDb
aDepartment of Dermatology, Henri Mondor Hospital and
EpiDermE, Université Paris-Est Créteil Val-de-Marne, Créteil,
France; and bDepartment of Dermatology and Pediatrics,
Mount Sinai St. Luke's-Roosevelt and Beth Israel Medical
Centers, New York, New York
Drs Ezzedine and Silverberg conceptualized and
designed the study, performed data collection,
drafted the initial manuscript, carried out the initial
analyses, reviewed and revised the manuscript, and
approved the fi nal manuscript as submitted.
DOI: 10.1542/peds.2015-4126
Accepted for publication Jan 27, 2016
Address correspondence to Khaled Ezzedine, MD,
PhD, Department of Dermatology, Henri Mondor
Hospital and EpiDermE, Université Paris-Est Créteil
Val-de-Marne, 94010 Créteil, France. E-mail: khaled.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright © 2016 by the American Academy of
Pediatrics
Vitiligo is a chronic, acquired
depigmenting condition of the
skin, and sometimes of the mucosa,
that results in the selective loss
of melanocytes.1 Vitiligo has been
reported since ancient times and a
description of it exists in the Latin
medical classic De Medicina of Celsus
during the second century.2, 3 The
name might come from the Latin
“vitium, ” meaning defect or blemish.4
Although vitiligo is not a rare disease,
it has been until recently an orphan
disease in terms of drug development
and a neglected one in the field of
dermatology. Moreover, patients often
complain that physicians are unaware
of treatment options and that most
of these physicians consider vitiligo
as a “cosmetic disease.”5 Despite
the lack of demonstrative physical
symptoms accompanying the disease
as compared with other common
chronic dermatological disorders,
such as eczema and psoriasis, vitiligo
causes emotional distress and impairs
patient and parental quality of life in
childhood.
EPIDEMIOLOGY OF PEDIATRIC VITILIGO
The prevalence of vitiligo worldwide
ranges from 0% to 2.16% of the
population, 6 with approximately one-
third to one-half of all cases having
onset in childhood.7 There appear to
be 2 subsets of patients with vitiligo:
those with early onset (12 years of age
or younger) who have more halo nevi,
Koebner phenomenon (KP) (lesional
development in response to trauma),
family history, segmental disease
and atopy, and those with late onset
who have more acrofacial lesions and
thyroid disease (in those older than 12
years).7–9 High estimates of prevalence
in pediatric vitiligo are noted when
analyzing groups of pediatric patients
attending a dermatology clinic. For
instance, in Nepal and India, 2.0%
and 2.6%, respectively, of children
attending a dermatology clinic were
diagnosed with vitiligo.10 In general
population-based studies, vitiligo
occurs in fewer than a half percent of
the population of children. In a large
Chinese population-based study in
abstractVitiligo is a common inflammatory skin disease with a worldwide
prevalence of 0.5% to 2.0% of the population. In the pediatric population,
the exact prevalence of vitiligo is unknown, although many studies
state that most cases of vitiligo are acquired early in life. The disease
is disfiguring, with a major psychological impact on children and their
parents. Half of vitiligo cases have a childhood onset, needing thus a
treatment approach that will minimize treatment side effects while avoiding
psychological impacts. Management of vitiligo should take into account
several factors, including extension, psychological impact, and possible
associations with other autoimmune diseases. This review discusses the
epidemiology of vitiligo and outlines the various clinical presentations
associated with the disorder and their differential diagnosis. In addition,
the pathophysiology and genetic determinants, the psychological impact of
vitiligo, and management strategies are reviewed.
STATE-OF-THE-ART REVIEW ARTICLEPEDIATRICS Volume 138 , number 1 , July 2016 :e 20154126
To cite: Ezzedine K and Silverberg N. A Practical
Approach to the Diagnosis and Treatment of Vitiligo
in Children. Pediatrics. 2016;138(1):e20154126
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from

EZZEDINE and SILVERBERG
which the prevalence overall was
0.56% of the population, a prevalence
of 0.1% in the 0 to 9 years age
group and 0.36% by 10 to 19 years
of age was recorded.11 Similarly a
Taiwanese study showed 0.09% of
children had vitiligo12 and a Danish
population-based study showed
0.09% and 0.15% prevalence for 0
to 9 and 10 to 20 years age groups,
respectively.13 In the Sinai desert,
a cohort of children younger than
18 years showed a prevalence of
0.18%.14
Disease onset increases through the
first 2 decades of life. Disease is quite
uncommon in children younger than
2 years as opposed to congenital
disorders of pigmentation, such
as nevus depigmentosus.15 Onset
before age 2 years represents 11%
of pediatric-onset cases, 28% of
cases start between 2 and 5 years,
40% of cases begin between 5 and
10 years, and 21% between 10 and
18 years, demonstrating that median
age of onset is between 5 and 10
years of age.16 In a cohort of Indian
children, 56.7% of pediatric cases
were noted in childhood between 8
and 12 years.17 Early-onset disease
(before age 12 years) represented
35.2% of cases in an Indian cohort.17
Children younger than 20 years
represent 35.5% of patients in a
Nigerian cohort18 and age of onset
before 20 years of age was noted
in 47.8% of patients in a Gujarati
cohort.19 Mean age of onset can be
as low as 6.9 years in Indian children
12 years and younger17 and as high
as 17.4 years in an unselected Saudi
Arabian mixed pediatric and adult
population.20 Family history appears
to be associated with earlier age of
onset.21
The prevalence of vitiligo by gender
is usually close to if not equal, with
some studies supporting female
predilection in the youngest age
groups. Vora et al19 described a
Gujarati cohort of 1100 patients
of all ages in which 57.3% were
female individuals and 42.7% were
male individuals. In a cohort of
268 Indian children 12 years and
younger, 56.7% were girls (n = 152)
and 43.3% were boys (n = 116).17
Similarly, in a Greek population,
two-thirds of the children ages 0
to 10 years were girls, whereas
by late adulthood, incidence was
similar between the genders.22
The breakdown of vitiligo types in
a pediatric population of patients
with vitiligo varies by population
reviewed. In a case series of 119
pediatric patients with vitiligo,
34% had generalized disease,
13% acrofacial, 3% mucosal, 29%
segmental, and 21% undetermined.
Lower estimates of segmental disease
include 17.6% of cases in children
who were 12 years or younger in an
Indian cohort.17
CLINICAL FEATURES
Recently, an international panel of
experts has proposed consensus
definitions of vitiligo.23 Overall,
vitiligo can be divided into
segmental vitiligo (SV) and vitiligo/
nonsegmental vitiligo (NSV), which
encompasses rare forms of vitiligo.
Typical vitiligo lesions can be defined
as whitish, nonscaly macules that
have usually distinct margins. When
first seeing a patient, it is of prime
importance to differentiate between
these 2 forms, as these are quite
different in terms of prognosis,
evolution, and response to treatment
patterns.
Nonsegmental Vitiligo
NSV is the most common variant of
vitiligo, and accounts for almost 80%
of all cases. NSV is characterized by
asymptomatic, well-circumscribed,
milky-white macules involving
multiple parts of the body, usually
in a symmetrical pattern (Fig 1).
The disease can start at any site of
the body, but the fingers, hands, and
face are frequently the initial sites.
Within NSV, several subphenotypes
have been well described, including
acrofacial, mucosal, generalized,
universal, mixed, and rare forms.
Of note, overlaps between these
forms may exist; for example, NSV
may initially have an acrofacial
pattern, with a later evolvement to
the generalized form. Interestingly,
a recent study based on latent class
analysis has distinguished 2 types
of vitiligo with probable different
pathophysiological pathways.8
2
FIGURE 1Typical nonsegmental vitiligo.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
PEDIATRICS Volume 138 , number 1 , July 2016
Acrofacial vitiligo is not very
common in children. In this form,
areas involved are often limited to
the face, hands, feet, and orifices.
The form may later evolve to typical
generalized vitiligo.
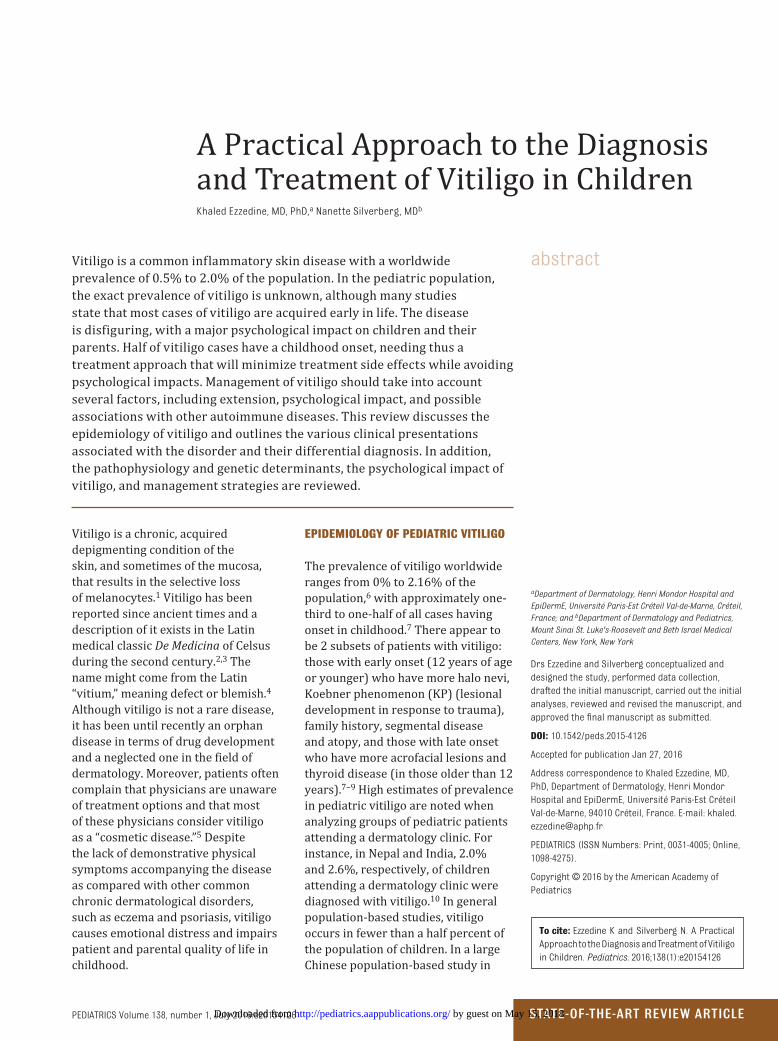
Vitiligo universalis is a widespread
form of the disease that is generally
seen in adults, although cases in
children are reported.24 The term
“universalis” refers to the almost
virtually universal depigmentation
(>60% to 90% of the body surface
area) (Fig 2). Hairs may be partially
spared. In general, vitiligo universalis
is the result of generalized vitiligo
that gradually progresses to nearly
complete depigmentation of
the skin.
Mucosal vitiligo states for oral and/
or genital mucosae involvement
in vitiligo as part of generalized
vitiligo or as an isolated condition.
When limited to mucosa, differential
diagnosis should include lichen
sclerosus. Moreover, the coexistence
of both conditions has also been
reported.25
Mixed vitiligo refers to the
concomitance of SV and NSV in a
single patient. Criteria proposed
for mixed vitiligo are detailed
elsewhere.26
Rare Forms
Several forms may fit into the
spectrum of rare vitiligo and all
should be considered as NSV forms.
Punctate vitiligo was first described
by Falabella et al27 and refers to pea-
sized depigmented macules that may
involve any area of the body.23
Vitiligo minor is rarely reported
in children. In this rare form,
hypopigmented macules are
distributed mainly on the face,
and the back has been recently
reported.28 Another striking rare
form is follicular vitiligo, which has
the particularity to primarily involve
the melanocyte follicular reservoir
with whitening of most of the body
hairs and rare depigmented
macules.29
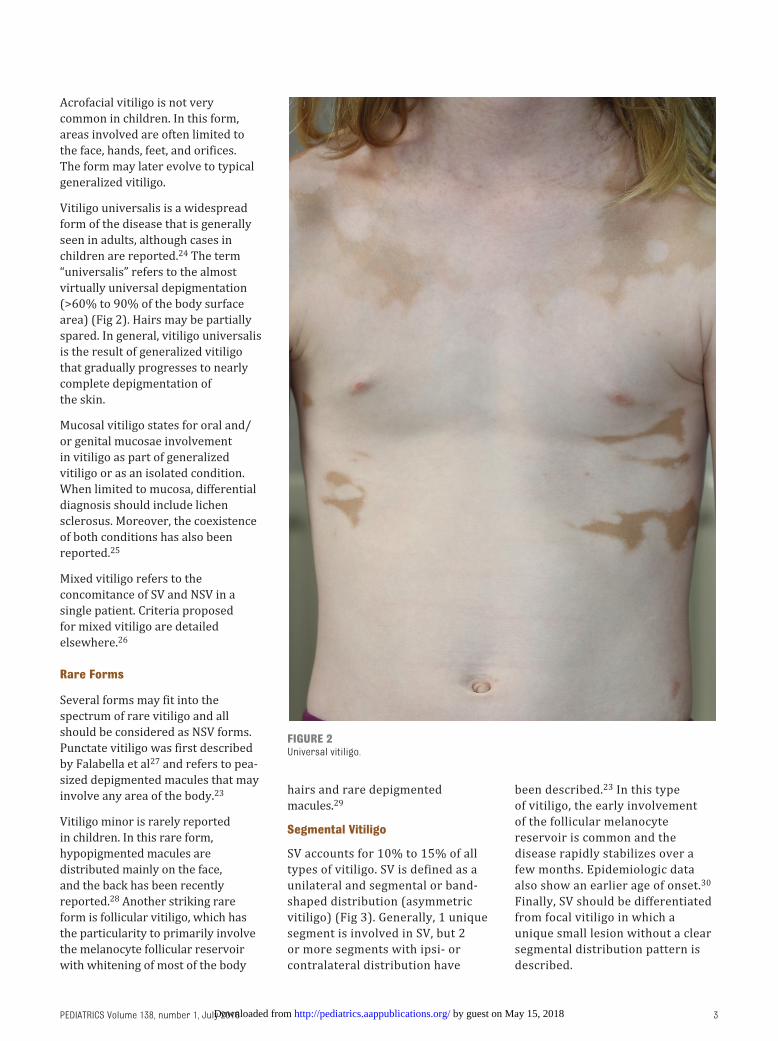
Segmental Vitiligo
SV accounts for 10% to 15% of all
types of vitiligo. SV is defined as a
unilateral and segmental or band-
shaped distribution (asymmetric
vitiligo) (Fig 3). Generally, 1 unique
segment is involved in SV, but 2
or more segments with ipsi- or
contralateral distribution have
been described.23 In this type
of vitiligo, the early involvement
of the follicular melanocyte
reservoir is common and the
disease rapidly stabilizes over a
few months. Epidemiologic data
also show an earlier age of onset.30
Finally, SV should be differentiated
from focal vitiligo in which a
unique small lesion without a clear
segmental distribution pattern is
described.
3
FIGURE 2Universal vitiligo.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
EZZEDINE and SILVERBERG
PATHOPHYSIOLOGY AND GENETIC DETERMINANTS
SV occurs focally, based on localized
susceptibility to disease and is
not associated with autoimmune
phenomena unless nonsegmental
disease or a generalized autoimmune
condition such as alopecia areata
occurs concurrently.31, 32 The
leading theory is that generalized
vitiligo is a multifactorial, polygenic
autoimmune disorder that occurs
in only a minority of genetically
susceptible individuals and is
therefore believed to have a strong
component of environmental
triggering. Other theories of vitiligo
development include biochemical
defects in the tetrahydrobiopterin
pathway/oxidative damage,
adhesion defects, and neural
induction33; however, generalized
disease at this point in time is
usually presumed autoimmune
in nature, with demonstrable
autoantibodies against pigment
cells in patients with vitiligo.34 In
a survey of 2624 primarily White
probands, frequency was 6.1%
in siblings, and concordance only
23% in identical twins. Early-onset
disease was associated with more
family members, suggesting that
this subgroup carries more genetic
susceptibility determinants.35
Associated autoimmune diseases
in family members in this cohort
were vitiligo itself, autoimmune
thyroid disease (particularly
hypothyroidism), pernicious anemia,
Addison disease, systemic lupus
erythematosus, and inflammatory
bowel disease. Other studies have
demonstrated personal and familial
association of vitiligo with canity, 21
atopic dermatitis, 36, 37 rheumatoid
arthritis, types 1 and 2 diabetes
mellitus, alopecia areata, psoriasis,
chronic urticaria, lichen sclerosis
et atrophicus, Celiac disease,
systemic lupus erythematosus, and
sarcoidosis.38 Extensive disease and
increasing years with disease are the
factors most associated with vitiligo-
associated autoimmune disease.38
At this time, there is no genetic
test for vitiligo. The genetics of
vitiligo are complex, as there are
multiple determinants found in most
genome-wide association studies.
Consistent association with genes
such as DDR1, XBP1, NLRP1, PTPN22
and COMT has been noted. Other
studies have noted association with
ACE, AIRE, CD4, COX2, ESR1, EDN1, FAS, FOXD3, FOXP3, IL1-RN, IL-10,
MBL2, MC1R, MYG1, Nrf2, PDGFRA, PRO2268, SCF, SCGF, TXNDC5, UVRAG, and VDR genes.39 These genes can
be broken down into 6 categories
of genes: (1) pigmentation gene
polymorphisms believed to create
increased risk of autoimmune
attack and susceptibility to damage:
TYR, TRP 1 and 2, OCA2 and its
transcription down regulator HERC2,
MC1R, and DDR1, which affects
melanocyte cellular adhesion; (2)
MHC loci (eg, HLA-A*02:01, HLA-DR4,
and HLA-DR7 alleles) and XBP1,
which regulates MHC expression;
(3) B- and T-cell developmental
genes, which promote activity and/
or repression promoting immune
response against melanocytes (eg,
CTLA4, BACH2, CD44, IKZF4, LNK); (4)
genes involved in innate immunity
(eg, NLRP-1, formerly NALP-1); (5)
apoptosis determinants (CASP7);
and (6) polymorphisms in genes
that regulate antiinflammatory
activity (eg, glutathione S transferase,
vitamin D receptor).40
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
The diagnosis of vitiligo is
generally made clinically through
the appearance of reduced or lost
pigmentation of the skin in a typical
distribution, including periorificial,
segmental, lips and tips of the
fingers, toes and/or penis, flexural
surfaces, and frictional areas, such
as waistbands.40, 41 Clues to the
presence of generalized vitiligo
include multiple halo nevi, poliosis
(loss of pigmentation in the hairs),
canity, family history of vitiligo
and canity, and lesions in sites of
trauma, so-called KP.42, 43 SV is often
corroborated by the presence of
linear lesions, broadly in the Lines
of Blaschko or on the face in typical
segments.44 Colocalization of poliosis
is common, whereas alopecia areata
overlap may be noted as well. In
vitiligo, biopsy will demonstrate
in the center of a lesion the loss of
melanocytes (pigment cells) with
4
FIGURE 3Segmental vitiligo with hair whitening in the depigmented area.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from

PEDIATRICS Volume 138 , number 1 , July 2016
special stains of the epidermis. The
border of a lesion may be noted
visually to be inflamed (inflammatory
vitiligo), and a notable inflammatory
infiltrate of CD 4+ and CD 8+ T
lymphocytes may be seen on biopsy
of an “active” border, 39 although the
inflammation may be clinically absent.
The differential diagnosis of vitiligo
is broad and includes inflammatory,
postinflammatory, neoplastic,
and primary pigmentary genetic
disorders (Table 1).
The first step is to determine whether
the lesion is inherited or not. Indeed,
if the lesion is present at birth,
inherited or genetically induced
hypomelanoses should be ruled
out. This is quite easy in patients
with dark phototype. However, in
patients with fair skin complexion,
hypopigmented patches are usually
revealed after the first sun exposure
due to tanning of normal surrounding
skin, sometime in the first 2 years
of life. In this case, family history,
ethnic background/consanguinity
history, and a detailed family tree are
of prime importance. Several genetic
diseases may be misdiagnosed as
vitiligo, but the most frequent are
piebaldism and tuberous sclerosis.
In piebaldism, the combination of
white forelock, anterior body midline
depigmentation, and bilateral shin
depigmentation is the hallmark of the
disease. Differential diagnosis with
tuberous sclerosis might be trickier
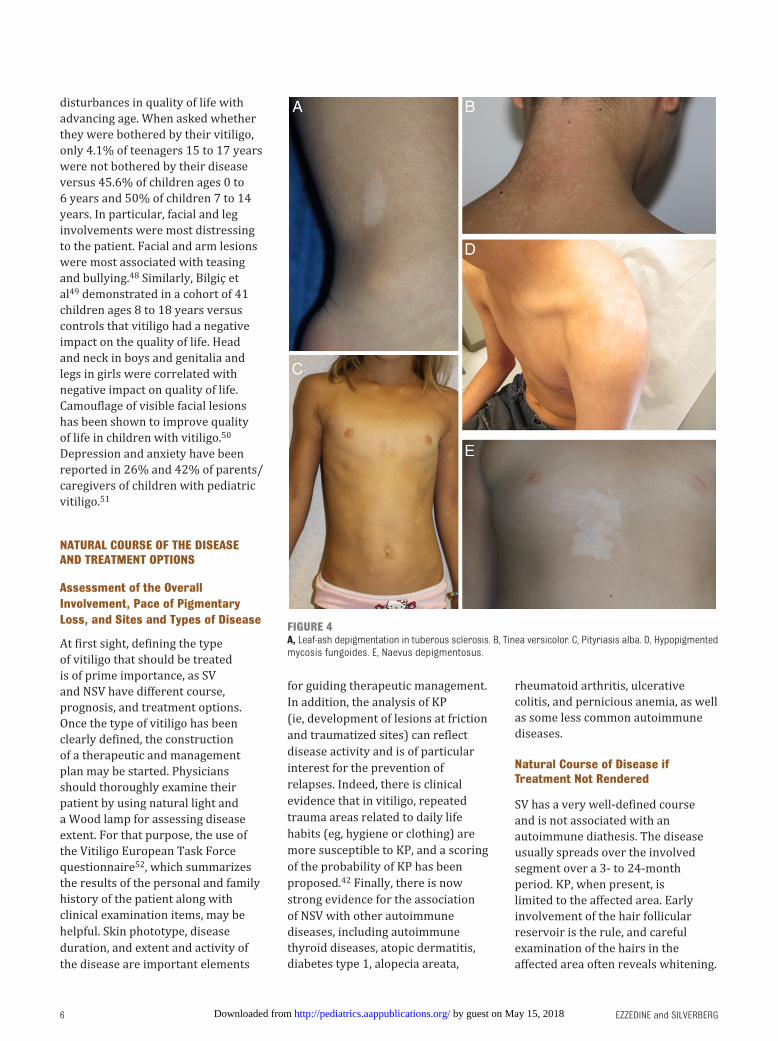
in case of ash-leaf hypopigmented
spots (Fig 4A) without seizures
or other usually later cutaneous
symptoms, such as shagreen patches,
or angiofibromas.
In noninherited lesions, which
are the most common differential
diagnoses in children with vitiligo,
pityriasis versicolor (Fig 4B) and
postinflammatory hypomelanoses
(hypopigmentation) should be
ruled out. A Wood lamp can be
used to highlight lesions of vitiligo
for confirmation distinguishing
vitiligo from pityriasis alba (Fig
4C); on the other hand, one of the
neoplastic hypomelanoses to exclude
is mycosis fungoides (Fig 4D), and
that may highlight on Wood lamp
examination.45, 46 Therefore, biopsy
may be required in atypical cases
and where mycosis fungoides is
suspected; in that setting, T cell gene
rearrangement studies on the biopsy
may be helpful.
For segmental vitiligo, naevus
depigmentosus (Fig 4E) is the most
common lesion in the differential
diagnosis. Naevus depigmentosus
is usually congenital and stable in
size, growing in proportion to the
child’s growth. The lesion generally
holds a normal or subnormal number
of melanocytes with a reduced
production of melanin pigment.
Where biopsy is needed, the inclusion
of a specimen of normal skin for
comparison may be needed for
definitive reading.
THE PSYCHOLOGICAL IMPACT OF VITILIGO
The psychological impact of vitiligo
is profound in childhood. Associated
negative experiences can include
fear of being questioned about one’s
appearance, teasing and bullying,
anxiety over the potential for
disease spread, interference with
emotional maturation, depression,
and interference with socialization
(eg, sexual debut). Of the 25% of
children with vitiligo evaluated for
psychological issues, 60% reported
psychological problems in a cohort
of 119 Brazilian children.16 A recent
review article of quality-of-life issues
in childhood skin disease stated:
“In general, patients with vitiligo
experience low self-esteem, social
stigmatization, shame, avoidance
of intimacy, anxiety, depression,
adjustment disorder, fear, suicidal
ideation, and other psychiatric
morbidity.”47 Recent studies have
suggested that childhood vitiligo
impacts quality of life similarly
to psoriasis, as children enter
adulthood.
An Internet-based survey of vitiligo
probands ages 0 to 17 years and their
families showed that pediatric vitiligo
was associated with increasing
5
TABLE 1 Common Mimics of Vitiligo in Childhood
Differential diagnosis with nonsegmental vitiligo
Congenital depigmentation (often with appearance by 2 y of age)
Albinism
Piebaldism (white forelock + ventral depigmentation)
Waardenburg syndrome
Tuberous sclerosis (leaf-ash depigmentation) (Fig 4A)
Postinfl ammatorya
Chemical depigmentation
Psoriasis
Atopic dermatitis
Lichen sclerosis et atrophicus
Morphea
Pityriasis alba (Fig 4B)
Pityriasis rosea
Sarcoidosis
Seborrheic dermatitis
Postinfl ammatory hypopigmentation
Infectious
Progressive macular hypomelanosis
Tinea versicolor (Fig 4C)
Tinea incognito
Neoplastic
Mycosis fungoides (Fig 4D)
Differential diagnosis with segmental vitiligo
Nevus depigmentosus/hypochromic nevus (Fig 4E)
a Associations between vitiligo and other infl ammatory dermatoses may exist. In particular association of vitiligo and
atopic dermatitis is frequently reported.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
EZZEDINE and SILVERBERG
disturbances in quality of life with
advancing age. When asked whether
they were bothered by their vitiligo,
only 4.1% of teenagers 15 to 17 years
were not bothered by their disease
versus 45.6% of children ages 0 to
6 years and 50% of children 7 to 14
years. In particular, facial and leg
involvements were most distressing
to the patient. Facial and arm lesions
were most associated with teasing
and bullying.48 Similarly, Bilgiç et
al49 demonstrated in a cohort of 41
children ages 8 to 18 years versus
controls that vitiligo had a negative
impact on the quality of life. Head
and neck in boys and genitalia and
legs in girls were correlated with
negative impact on quality of life.
Camouflage of visible facial lesions
has been shown to improve quality
of life in children with vitiligo.50
Depression and anxiety have been
reported in 26% and 42% of parents/
caregivers of children with pediatric
vitiligo.51
NATURAL COURSE OF THE DISEASE AND TREATMENT OPTIONS
Assessment of the Overall Involvement, Pace of Pigmentary Loss, and Sites and Types of Disease
At first sight, defining the type
of vitiligo that should be treated
is of prime importance, as SV
and NSV have different course,
prognosis, and treatment options.
Once the type of vitiligo has been
clearly defined, the construction
of a therapeutic and management
plan may be started. Physicians
should thoroughly examine their
patient by using natural light and
a Wood lamp for assessing disease
extent. For that purpose, the use of
the Vitiligo European Task Force
questionnaire52, which summarizes
the results of the personal and family
history of the patient along with
clinical examination items, may be
helpful. Skin phototype, disease
duration, and extent and activity of
the disease are important elements
for guiding therapeutic management.
In addition, the analysis of KP
(ie, development of lesions at friction
and traumatized sites) can reflect
disease activity and is of particular
interest for the prevention of
relapses. Indeed, there is clinical
evidence that in vitiligo, repeated
trauma areas related to daily life
habits (eg, hygiene or clothing) are
more susceptible to KP, and a scoring
of the probability of KP has been
proposed.42 Finally, there is now
strong evidence for the association
of NSV with other autoimmune
diseases, including autoimmune
thyroid diseases, atopic dermatitis,
diabetes type 1, alopecia areata,
rheumatoid arthritis, ulcerative
colitis, and pernicious anemia, as well
as some less common autoimmune
diseases.
Natural Course of Disease if Treatment Not Rendered
SV has a very well-defined course
and is not associated with an
autoimmune diathesis. The disease
usually spreads over the involved
segment over a 3- to 24-month
period. KP, when present, is
limited to the affected area. Early
involvement of the hair follicular
reservoir is the rule, and careful
examination of the hairs in the
affected area often reveals whitening.
6
FIGURE 4A, Leaf-ash depigmentation in tuberous sclerosis. B, Tinea versicolor. C, Pityriasis alba. D, Hypopigmented mycosis fungoides. E, Naevus depigmentosus.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
PEDIATRICS Volume 138 , number 1 , July 2016
One characteristic feature in SV
is that once repigmentation has
occurred, relapse is rare.
On the other hand, the course of NSV
is unpredictable. The natural history
of the disease tends to be cyclic and
includes a silent phase, during which
melanocyte destruction is minimal,
and a so-called acceleration phase
with rapid disease progression over
a few weeks or months followed by a
stabilization phase. Whitening of the
hairs may appear later in the course
of the disease. Repigmentation
may occur without any therapeutic
intervention or after sun exposure.
The number of lifetime cycles and
triggering factors are different in
each patient and yet still to be clearly
elucidated. Epidemiologic studies
support the role of stress episodes as
a trigger of disease and/or relapse.
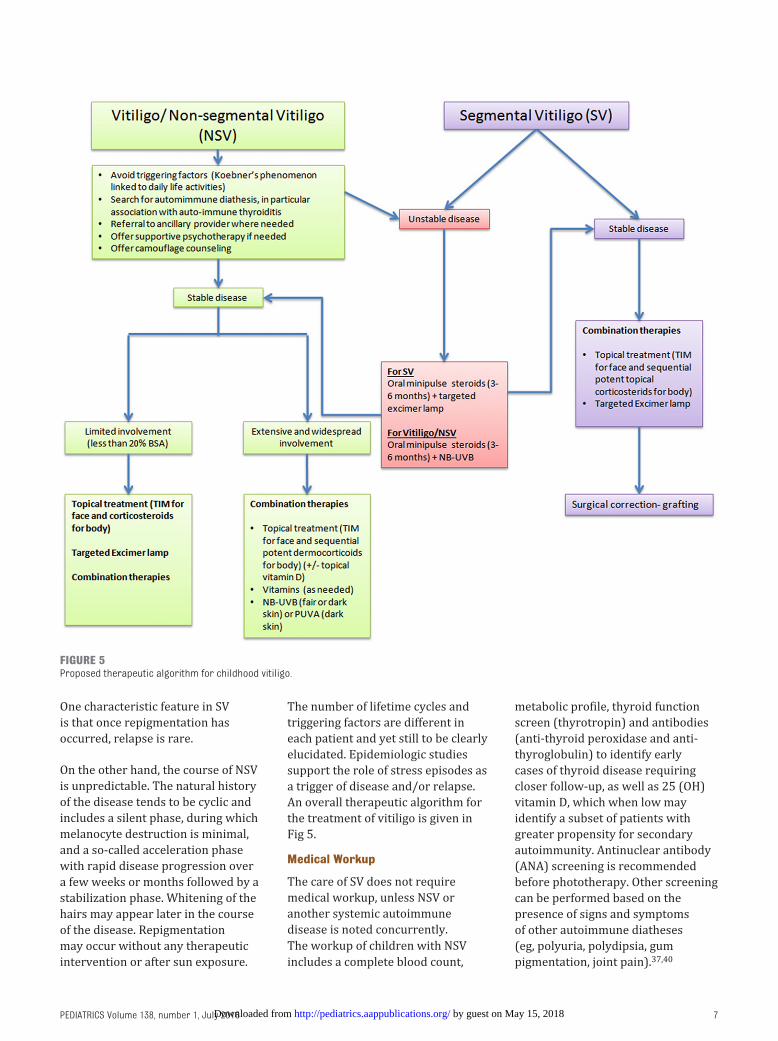
An overall therapeutic algorithm for
the treatment of vitiligo is given in
Fig 5.
Medical Workup
The care of SV does not require
medical workup, unless NSV or
another systemic autoimmune
disease is noted concurrently.
The workup of children with NSV
includes a complete blood count,
metabolic profile, thyroid function
screen (thyrotropin) and antibodies
(anti-thyroid peroxidase and anti-
thyroglobulin) to identify early
cases of thyroid disease requiring
closer follow-up, as well as 25 (OH)
vitamin D, which when low may
identify a subset of patients with
greater propensity for secondary
autoimmunity. Antinuclear antibody
(ANA) screening is recommended
before phototherapy. Other screening
can be performed based on the
presence of signs and symptoms
of other autoimmune diatheses
(eg, polyuria, polydipsia, gum
pigmentation, joint pain).37, 40
7
FIGURE 5Proposed therapeutic algorithm for childhood vitiligo.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from

EZZEDINE and SILVERBERG
Topical Therapies
There is no approved or labeled
treatment of vitiligo. Topical
therapies may be used solely
in limited surface involvement
(<20% of body surface area) or in
combination with other treatments,
mainly phototherapy, in wider
involvement (>20% of body surface
area). There are 3 main classes of
topical drugs that are used in vitiligo:
topical steroids, topical calcineurin
inhibitors, and topical vitamin D.
The site of involvement should be
taken into account for the choice
between these different treatments.
Hence, the European Dermatology
Forum consensus group has recently
published guidelines favoring the
use of topical calcineurin inhibitors
as a first-line option for face and
neck on a bidaily basis, as these have
fewer side effects in these particular
areas.53
Midpotency topical corticosteroids
may be used for the rest of the body
on a daily basis and in a sequential
discontinuous scheme (eg, 1 week
treatment and 1 week off for 6
months) to prevent local side effects
(ie, skin atrophy, telangiectasia,
hypertrichosis, acneiform eruptions,
and striae). The use of topical
vitamin D derivatives should be in
combination with topical steroids.
Mineral Complex Cream
Mineral complex creams have
been developed and tested in a
broad age group of patients largely
adjunctive to phototherapy. The
principle of therapy has been the
reduction of oxidative pigment
cell damage that is felt to occur
through tetrahydrobiopterin
pathway breakdown. Variable
results have been seen, with some
centers reporting good outcomes
with proprietary products. The
initial clinical report54 described
33 patients ages 4 to 68 years.
Pseudocatalase and calcium topically,
combined with narrowband UVB
or climatotherapy at the Dead Sea,
has been described to be effective
at repigmentation of facial and
dorsal hand vitiligo. Not all mineral
complexes benefit patients with
vitiligo. For example, topical co-Q10
application is not advised because of
potential triggering vitiligo through
a putative mechanism of peroxide
generation.55 Therefore, mineral
complex cream is generally used
adjunctively and should be used only
when the product efficacy can be
confirmed.
Sun Protection
Sun protection is generally advised in
all patients, but is needed more so for
areas of depigmentation. As a result,
any sun exposure that is not sought
for purposes of repigmentation
should be paired with sun protection,
including age-appropriate sun block
or sunscreen, hats, sunglasses, and
clothing.
Oral Vitamins and Supplements
There have been a few studies that
suggest vitamin supplementation
can enhance vitiligo outcomes.
First, vitamin deficiencies have
been noted in patients with vitiligo,
including vitamin D, which has been
linked to comorbid autoimmunity, 56
and B-complex vitamins,
including folate and B12.57
Hyperhomocysteinemia, which
can be associated with vitamin B
deficiencies, has also been linked
to vitiligo.58, 59 Low-dose vitamin
supplementation, such as 400 IU
Vitamin D3 daily, is common in
childhood, but high-dose vitamin
supplementation in childhood has
limited data supporting its usage
for childhood vitiligo, and in fact
there are few safety data for usage
of herbal remedies, such as gingko in
childhood. One clinical trial that has
looked at safety and efficacy of the
amino acid phenylalanine in high
dosage for vitiligo (a precursor to
melanin) showed modest benefit in
repigmentation.60, 61
Minipulse Oral Steroids
Steroid pulse therapy refers to
the intermittent administration
of suprapharmacological doses of
steroids. This method is weighted to
reduce the side effects of steroids.
No randomized placebo-controlled
clinical trial has yet confirmed the
interest of low-dose oral minipulse
(OMP) steroids in vitiligo/NSV.
However, several retrospective
studies have underlined the
interest of OMP of low doses of
betamethasone or dexamethasone
for 3 to 6 months in rapidly evolving
vitiligo with the principal aim to
halt disease progression.62, 63 In
addition, in a recent retrospective
study, the early use of short-term
systemic steroids in combination with
targeted phototherapy and topical
tacrolimus has shown to be effective
in repigmenting SV.63 Although
uncommon, side effects such as weight
gain and acneiform eruptions have
been described with the use of OMP.
Phototherapy
A variety of phototherapy modalities
exist that have been shown to
be beneficial in pediatric vitiligo.
Generalized phototherapy is often
performed in extensive disease and
in disease that is spreading rapidly.
Psoralens and UVA (PUVA) has been
historically used in vitiligo with
good benefit, but there is difficulty
with nausea, compliance of eyewear,
office visits, and many side effects
including phototoxic reactions.64
Therefore, PUVA has been largely
replaced by narrowband UVB (NB
UVB). Furthermore, in head-to-head
study, there has been demonstrable
increased repigmentation that was
not significant over PUVA.65 In
children, NB UVB has become the
therapy of choice and can produce
2 types of benefits: (1) repigmentation,
and (2) stabilization, the latter
being an important way to gain
control over widespread disease.
Njoo et al demonstrated >75%
repigmentation in 53% of children
8 by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
PEDIATRICS Volume 138 , number 1 , July 2016
and 80% stabilization with twice-
weekly NB UVB in children.66 Some
benefit can be achieved with the
addition of topical corticosteroids.
Other forms of phototherapy that
have been described as safe and
effective for long-term therapy of
pediatric vitiligo include excimer laser,
targeted UVB, and targeted UVA1.67
Side effects of phototherapy include
itch, burning, erythema, stinging,
blistering, and phototoxicity.67
Targeted phototherapy may not allow
for disease stabilization in extensive
disease, but does limit side effects to
the local site treated.41 Excimer laser is
most beneficial in SV when performed
early on in disease.68 Phototherapy is
often more effective in darker patients
and the benefits of phototherapy in
Fitzpatrick type I skin (lightest skin
type) do not outweigh the risk.53
Although long-term follow-up of
pediatric patients with vitiligo who
received phototherapy has not been
conducted, the risk of carcinogenesis
after phototherapy probably persists
lifelong, requiring on-going full body
skin examinations for screening after
therapy. As some patients with vitiligo
will have circulating ANAs, which
could sensitize them, screening for
ANAs before systemic phototherapy
can be helpful.
Psychotherapy
Vitiligo has a strong and sustained
impact on the sufferer with long-term
fear of disease exacerbation, poor
self-perception, low quality of life,
poor interpersonal relationships,
depression, and anxiety (see
section The Psychological Impact
of Vitiligo).69–73 Psychotherapy,
including cognitive-behavioral
therapy and hypnosis, has been
described to aid in quality of
life, reduce anxiety, improve
coping with disease, and enhance
repigmentation.70, 74–76 Children with
extensive or visible disease, especially
adolescents, must be screened for
psychological symptomatology and
referred appropriately.
Cosmetics
Cosmetic camouflage, ranging from
self-tanners to clothing alterations
to concealers including stage-type
make-up, have been used to reduce
the clinical appearance of disease.77
Cosmetic camouflage make-up can
be color matched to the skin, and
children/parents can learn how to
apply these on a daily basis or before
major events to improve overall
quality of life.50
Surgical Grafting
Autologous grafting should be
reserved to stable vitiligo lesions
(ie, lesions with no progression
for at least 1 year). The best
indication for grafting is stable
SV. Different grafting techniques
have been described, including
punch grafting, split-thickness
skin graft, and the most recent is
melanocyte transfer grafting. The
main side effect of punch grafting
is a cobblestoning effect.78 All these
techniques remain painful, with
potential scarring and/or mottled
pigmentation side effects on the
recipient area and possible KP on
the donor site. Grafting techniques
have shown great results, although
there is a concern about the long-
term maintenance of these results in
vitiligo/NSV.79
Clinical Consultation and Comanagement
Comanagement of vitiligo with
the following practitioner types
may be advisable at times. These
include endocrinology (eg, thyroid
management), rheumatology (eg,
ANA-positive photosensitivity),
nutrition (eg, known vitamin
deficiencies), psychology/psychiatry
(eg, anxiety), developmental
specialists (eg, school-based
difficulties arising from vitiligo),
hematology (eg, pernicious anemia),
gastroenterology (eg, suspected
ulcerative colitis), and pediatrics (eg,
for coordination of care).
Furthermore, patients and parents
may benefit from referral to a
support group whether online or in
person. The following is a list of some
support sites for patients with vitiligo
worldwide:
1. Vitiligosupport.org
2. http:// vrfoundation. org/
3. www. mynvfi. org
Conclusions
Vitiligo is a frequent cause of
consultation and pediatricians and
general physicians play a central
role in its management. Indeed, as
the disease should be referred early
to potentialize treatment outcomes,
they are at the frontline for
referring patients to dermatologists
and managing further treatment
follow-up. Moreover, once the
diagnosis has been confirmed by a
dermatologist, early recognition of
new flare-ups by pediatricians and
general physicians will allow rapid
therapeutic intervention to prevent
the wide spread of the disease.
Although there is no approved drug
for the treatment of vitiligo, there is
now an arsenal of therapeutic options
that have proven efficacy in the
management of the disease. Parents
should be advised that the treatment
is often long term and requires
their adherence. The association
of vitiligo with other autoimmune
diseases should prompt physicians
to carefully seek any autoimmune/
autoinflammatory-associated disease.
Finally, as the disease is disfiguring,
one should not neglect its potential
psychological impact, especially if the
onset occurs during adolescence.
9
ABBREVIATIONS
ANA: antinuclear antibody
KP: Koebner phenomenon
NB UVB: narrowband UVB
NSV: nonsegmental vitiligo
OMP: oral minipulse
PUVA: psoralens and UVA
SV: segmental vitiligo
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
EZZEDINE and SILVERBERG
REFERENCES
1. Ezzedine K, Eleftheriadou V, Whitton
M, van Geel N. Vitiligo. Lancet.
2015;386(9988):74–84
2. Nair BK. Vitiligo—a retrospect. Int J
Dermatol. 1978;17(9):755–757
3. Gauthier YBL. Historical Aspects.
Heidelberg, Germany: Springer Verlag;
2010
4. Koranne RV, Sachdeva KG. Vitiligo. Int J
Dermatol. 1988;27(10):676–681
5. Ezzedine K, Sheth V, Rodrigues M, et al;
Vitiligo Working Group. Vitiligo is not a
cosmetic disease. J Am Acad Dermatol.
2015;73(5):883–885
6. Krüger C, Schallreuter KU. A review
of the worldwide prevalence of
vitiligo in children/adolescents and
adults. Int J Dermatol. 2012;51(10):
1206–1212
7. Silverberg NB. The Epidemiology
of Vitiligo. Curr Dermatol Rep.
2015;4:36–43
8. Ezzedine K, Le Thuaut A, Jouary T,
Ballanger F, Taieb A, Bastuji-Garin
S. Latent class analysis of a series
of 717 patients with vitiligo allows
the identifi cation of two clinical
subtypes. Pigment Cell Melanoma Res.
2014;27(1):134–139
9. Ezzedine K, Diallo A, Léauté-Labrèze
C, et al. Multivariate analysis of
factors associated with early-onset
segmental and nonsegmental vitiligo:
a prospective observational study
of 213 patients. Br J Dermatol.
2011;165(1):44–49
10. Shrestha R, Shrestha D, Dhakal AK,
Shakya A, Shah SC, Shakya H. Spectrum
of pediatric dermatoses in tertiary
care center in Nepal. Nepal Med Coll J.
2012;14(2):146–148
11. Wang X, Du J, Wang T, et al. Prevalence
and clinical profi le of vitiligo in China:
a community-based study in six cities.
Acta Derm Venereol. 2013;93(1):
62–65
12. Chen GY, Cheng YW, Wang CY,
et al. Prevalence of skin diseases
among schoolchildren in Magong,
Penghu, Taiwan: a community-based
clinical survey. J Formos Med Assoc.
2008;107(1):21–29
13. Howitz J, Brodthagen H, Schwartz
M, Thomsen K. Prevalence of vitiligo.
Epidemiological survey on the Isle of
Bornholm, Denmark. Arch Dermatol.
1977;113(1):47–52
14. Yamamah GA, Emam HM, Abdelhamid
MF, et al. Epidemiologic study of
dermatologic disorders among
children in South Sinai, Egypt. Int J
Dermatol. 2012;51(10):1180–1185
15. Tey HL. A practical classifi cation of
childhood hypopigmentation disorders.
Acta Derm Venereol. 2010;90(1):6–11
16. Marinho FS, Cirino PV, Fernandes NC.
Clinical epidemiological profi le of
vitiligo in children and adolescents.
An Bras Dermatol. 2013;88(6):
1026–1028
17. Agarwal S, Gupta S, Ojha A, Sinha R.
Childhood vitiligo: clinicoepidemiologic
profi le of 268 children from the
Kumaun region of Uttarakhand, India.
Pediatr Dermatol. 2013;30(3):348–353
18. Ayanlowo O, Olumide YM, Akinkugbe
A, et al. Characteristics of vitiligo
in Lagos, Nigeria. West Afr J Med.
2009;28(2):118–121
19. Vora RV, Patel BB, Chaudhary AH,
Mehta MJ, Pilani AP. A clinical study
of vitiligo in a rural set up of Gujarat.
Indian J Community Med. 2014;39(3):
143–146
20. Alissa A, Al Eisa A, Huma R, Mulekar
S. Vitiligo-epidemiological study
of 4134 patients at the National
Center for Vitiligo and Psoriasis in
Central Saudi Arabia. Saudi Med J.
2011;32(12):1291–1296
21. Pajvani U, Ahmad N, Wiley A, et al. The
relationship between family medical
history and childhood vitiligo. J Am
Acad Dermatol. 2006;55(2):238–244
22. Kyriakis KP, Palamaras I, Tsele E,
Michailides C, Terzoudi S. Case
detection rates of vitiligo by
gender and age. Int J Dermatol.
2009;48(3):328–329
23. Ezzedine K, Lim HW, Suzuki T, et al;
Vitiligo Global Issue Consensus
Conference Panelists. Revised
classifi cation/nomenclature of vitiligo
and related issues: the Vitiligo Global
Issues Consensus Conference. Pigment
Cell Melanoma Res. 2012;25(3):
E1–E13
24. Nicolaidou E, Antoniou C, Miniati A,
et al. Childhood- and later-onset vitiligo
have diverse epidemiologic and clinical
characteristics. J Am Acad Dermatol.
2012;66(6):954–958
25. Osborne GE, Francis ND, Bunker CB.
Synchronous onset of penile lichen
sclerosus and vitiligo. Br J Dermatol.
2000;143(1):218–219
26. Ezzedine K, Gauthier Y, Léauté-Labrèze
C, et al. Segmental vitiligo associated
with generalized vitiligo (mixed
vitiligo): a retrospective case series
of 19 patients. J Am Acad Dermatol.
2011;65(5):965–971
27. Falabella R. Surgical treatment of
vitiligo: why, when and how. J Eur Acad
Dermatol Venereol. 2003;17(5):
518–520
28. Ezzedine K, Mahé A, van Geel N,
et al. Hypochromic vitiligo: delineation
of a new entity. Br J Dermatol.
2015;172(3):716–721
29. Ezzedine K, Amazan E, Séneschal J,
et al. Follicular vitiligo: a new form of
vitiligo. Pigment Cell Melanoma Res.
2012;25(4):527–529
30. Mazereeuw-Hautier J, Bezio S, Mahe
E, et al; Groupe de Recherche Clinique
en Dermatologie Pédiatrique (GRCDP).
Segmental and nonsegmental
childhood vitiligo has distinct clinical
characteristics: a prospective
observational study. J Am Acad
Dermatol. 2010;62(6):945–949
10
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: Dr Ezzedine has indicated he has no potential confl icts of interest to disclose. Dr Silverberg has been an investigator for
Astellas Pharmaceuticals.
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
PEDIATRICS Volume 138 , number 1 , July 2016
31. Pagovich OE, Silverberg JI, Freilich E,
Silverberg NB. Thyroid abnormalities
in pediatric patients with vitiligo in
New York City. Cutis. 2008;81(6):
463–466
32. Silverberg N. Segmental vitiligo
may not be associated with risk of
autoimmune thyroiditis. Skinmed.
2011;9(5):329–330, author reply 330
33. Tarlé RG, Nascimento LM, Mira MT,
Castro CC. Vitiligo—part 1. An Bras
Dermatol. 2014;89(3):461–470
34. Naughton GK, Eisinger M, Bystryn
JC. Antibodies to normal human
melanocytes in vitiligo. J Exp Med.
1983;158(1):246–251
35. Alkhateeb A, Fain PR, Thody A, Bennett
DC, Spritz RA. Epidemiology of
vitiligo and associated autoimmune
diseases in Caucasian probands
and their families. Pigment Cell Res.
2003;16(3):208–214
36. Ezzedine K, Diallo A, Léauté-Labrèze C,
et al. Pre- vs. post-pubertal onset of
vitiligo: multivariate analysis indicates
atopic diathesis association in pre-
pubertal onset vitiligo. Br J Dermatol.
2012;167(3):490–495
37. Silverberg JI, Silverberg NB.
Association between vitiligo and
atopic disorders: a pilot study. JAMA
Dermatol. 2013;149(8):983–986
38. Silverberg JI, Silverberg NB. Clinical
features of vitiligo associated with
comorbid autoimmune disease:
a prospective survey. J Am Acad
Dermatol. 2013;69(5):824–826
39. Faria AR, Tarlé RG, Dellatorre G,
Mira MT, Castro CC. Vitiligo—Part
2—classifi cation, histopathology
and treatment. An Bras Dermatol.
2014;89(5):784–790
40. Silverberg NB. Recent advances in
childhood vitiligo. Clin Dermatol.
2014;32(4):524–530
41. Ezzedine K, Eleftheriadou V, Whitton
M, van Geel N. Vitiligo. Lancet.
2015;386(9988):74–84
42. Diallo A, Boniface K, Jouary T, et
al. Development and validation of
the K-VSCOR for scoring Koebner’s
phenomenon in vitiligo/non-segmental
vitiligo. Pigment Cell Melanoma Res.
2013;26(3):402–407
43. van Geel N, Speeckaert R, Taieb A,
et al; VETF members. Koebner’s
phenomenon in vitiligo: European
position paper. Pigment Cell Melanoma
Res. 2011;24(3):564–573
44. Kim DY, Oh SH, Hann SK. Classifi cation
of segmental vitiligo on the face:
clues for prognosis. Br J Dermatol.
2011;164(5):1004–1009
45. Ducharme EE, Silverberg NB. Selected
applications of technology in the
pediatric dermatology offi ce. Semin
Cutan Med Surg. 2008;27(1):94–100
46. Silverberg JI, Silverberg NB. False
“highlighting” with Wood’s lamp.
Pediatr Dermatol. 2014;31(1):109–110
47. Brown MM, Chamlin SL, Smidt AC.
Quality of life in pediatric dermatology.
Dermatol Clin. 2013;31(2):211–221
48. Silverberg JI, Silverberg NB. Quality
of life impairment in children and
adolescents with vitiligo. Pediatr
Dermatol. 2014;31(3):309–318
49. Bilgiç O, Bilgiç A, Akiş HK, Eskioğlu
F, Kiliç EZ. Depression, anxiety and
health-related quality of life in children
and adolescents with vitiligo. Clin Exp
Dermatol. 2011;36(4):360–365
50. Ramien ML, Ondrejchak S, Gendron R,
et al. Quality of life in pediatric patients
before and after cosmetic camoufl age
of visible skin conditions. J Am Acad
Dermatol. 2014;71(5):935–940
51. Manzoni AP, Weber MB, Nagatomi AR,
Pereira RL, Townsend RZ, Cestari TF.
Assessing depression and anxiety in
the caregivers of pediatric patients
with chronic skin disorders. An Bras
Dermatol. 2013;88(6):894–899
52. Taïeb A, Picardo M; VETF Members. The
defi nition and assessment of vitiligo:
a consensus report of the Vitiligo
European Task Force. Pigment Cell Res.
2007;20(1):27–35
53. Taieb A, Alomar A, Böhm M, et al;
Vitiligo European Task Force (VETF);
European Academy of Dermatology and
Venereology (EADV); Union Européenne
des Médecins Spécialistes (UEMS).
Guidelines for the management of
vitiligo: the European Dermatology
Forum consensus. Br J Dermatol.
2013;168(1):5–19
54. Schallreuter KU, Wood JM, Lemke KR,
Levenig C. Treatment of vitiligo with a
topical application of pseudocatalase
and calcium in combination with
short-term UVB exposure: a case
study on 33 patients. Dermatology.
1995;190(3):223–229
55. Schallreuter KU. Q10-triggered
facial vitiligo. Br J Dermatol.
2013;169(6):1333–1336
56. Silverberg JI, Silverberg AI, Malka E,
Silverberg NB. A pilot study assessing
the role of 25 hydroxy vitamin D levels
in patients with vitiligo vulgaris.
J Am Acad Dermatol. 2010;62(6):
937–941
57. Montes LF, Diaz ML, Lajous J, Garcia
NJ. Folic acid and vitamin B12 in
vitiligo: a nutritional approach. Cutis.
1992;50(1):39–42
58. Silverberg JI, Silverberg NB. Serum
homocysteine as a biomarker of
vitiligo vulgaris severity: a pilot study.
J Am Acad Dermatol. 2011;64(2):
445–447
59. Karadag AS, Tutal E, Ertugrul
DT, Akin KO, Bilgili SG. Serum
holotranscobalamine, vitamin B12,
folic acid and homocysteine levels
in patients with vitiligo. Clin Exp
Dermatol. 2012;37(1):62–64
60. Schulpis CH, Antoniou C, Michas
T, Strarigos J. Phenylalanine plus
ultraviolet light: preliminary report
of a promising treatment for
childhood vitiligo. Pediatr Dermatol.
1989;6(4):332–335
61. Antoniou C, Schulpis H, Michas T,
et al. Vitiligo therapy with oral and
topical phenylalanine with UVA
exposure. Int J Dermatol. 1989;28(8):
545–547
62. Singh A, Kanwar AJ, Parsad D,
Mahajan R. Randomized controlled
study to evaluate the effectiveness
of dexamethasone oral minipulse
therapy versus oral minocycline in
patients with active vitiligo vulgaris.
Indian J Dermatol Venereol Leprol.
2014;80(1):29–35
63. van Geel N, Speeckaert R, De Wolf J,
et al. Clinical signifi cance of Koebner
phenomenon in vitiligo. Br J Dermatol.
2012;167(5):1017–1024
64. Veith W, Deleo V, Silverberg N.
Medical phototherapy in childhood
skin diseases. Minerva Pediatr.
2011;63(4):327–333
11 by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from

EZZEDINE and SILVERBERG
65. Whitton ME, Pinart M, Batchelor J, et al.
Interventions for vitiligo. Cochrane
Database Syst Rev. 2015;(2):CD003263
66. Njoo MD, Bos JD, Westerhof W.
Treatment of generalized vitiligo in
children with narrow-band (TL-01) UVB
radiation therapy. J Am Acad Dermatol.
2000;42(2 Pt 1):245–253
67. Koh MJ, Mok ZR, Chong WS.
Phototherapy for the treatment of
vitiligo in Asian children. Pediatr
Dermatol. 2015;32(2):192–197
68. Do JE, Shin JY, Kim DY, Hann SK, Oh
SH. The effect of 308nm excimer laser
on segmental vitiligo: a retrospective
study of 80 patients with segmental
vitiligo. Photodermatol Photoimmunol
Photomed. 2011;27(3):147–151
69. Gawkrodger DJ, Ormerod AD,
Shaw L, et al; Therapy Guidelines
and Audit Subcommittee, British
Association of Dermatologists;
Clinical Standards Department, Royal
College of Physicians of London;
Cochrane Skin Group; Vitiligo Society.
Guideline for the diagnosis and
management of vitiligo. Br J Dermatol.
2008;159(5):1051–1076
70. Shah R, Hunt J, Webb TL, Thompson AR.
Starting to develop self-help for social
anxiety associated with vitiligo: using
clinical signifi cance to measure the
potential effectiveness of enhanced
psychological self-help. Br J Dermatol.
2014;171(2):332–337
71. Krüger C, Smythe JW, Spencer JD,
et al. Signifi cant immediate and long-
term improvement in quality of life
and disease coping in patients with
vitiligo after group climatotherapy at
the Dead Sea. Acta Derm Venereol.
2011;91(2):152–159
72. Kossakowska MM, Cieścińska C,
Jaszewska J, Placek WJ. Control of
negative emotions and its implication
for illness perception among psoriasis
and vitiligo patients. J Eur Acad
Dermatol Venereol. 2010;24(4):429–433
73. Ongenae K, Van Geel N, De Schepper
S, Vander Haeghen Y, Naeyaert JM.
Management of vitiligo patients
and attitude of dermatologists
towards vitiligo. Eur J Dermatol.
2004;14(3):177–181
74. Papadopoulos L, Bor R, Legg C. Coping
with the disfi guring effects of vitiligo:
a preliminary investigation into
the effects of cognitive-behavioural
therapy. Br J Med Psychol. 1999;72(pt
3):385–396
75. Papadopoulos L, Bor R, Legg C, Hawk
JL. Impact of life events on the onset
of vitiligo in adults: preliminary
evidence for a psychological dimension
in aetiology. Clin Exp Dermatol.
1998;23(6):243–248
76. Shenefelt PD. Hypnosis in dermatology.
Arch Dermatol. 2000;136(3):393–399
77. Tedeschi A, Dall’Oglio F, Micali G,
Schwartz RA, Janniger CK. Corrective
camoufl age in pediatric dermatology.
Cutis. 2007;79(2):110–112
78. Linthorst Homan MW, Spuls PI,
Nieuweboer-Krobotova L, et al. A
randomized comparison of excimer
laser versus narrow-band ultraviolet
B phototherapy after punch grafting
in stable vitiligo patients. J Eur Acad
Dermatol Venereol. 2012;26(6):690–695
79. Parsad D, Pandhi R, Dogra S, Kanwar
AJ, Kumar B. Dermatology Life Quality
Index score in vitiligo and its impact on
the treatment outcome. Br J Dermatol.
2003;148(2):373–374
12 by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2015-4126 originally published online June 21, 2016; 2016;138;Pediatrics
Khaled Ezzedine and Nanette SilverbergA Practical Approach to the Diagnosis and Treatment of Vitiligo in Children
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/138/1/e20154126including high resolution figures, can be found at:
References
f-list-1http://pediatrics.aappublications.org/content/138/1/e20154126.full#reThis article cites 77 articles, 1 of which you can access for free at:
Subspecialty Collections
_psychology_subhttp://classic.pediatrics.aappublications.org/cgi/collection/psychiatryPsychiatry/Psychologyy_subhttp://classic.pediatrics.aappublications.org/cgi/collection/dermatologDermatologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
. ISSN:60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print
American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from
DOI: 10.1542/peds.2015-4126 originally published online June 21, 2016; 2016;138;Pediatrics
Khaled Ezzedine and Nanette SilverbergA Practical Approach to the Diagnosis and Treatment of Vitiligo in Children
http://pediatrics.aappublications.org/content/138/1/e20154126located on the World Wide Web at:
The online version of this article, along with updated information and services, is
. ISSN:60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print
American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 15, 2018http://pediatrics.aappublications.org/Downloaded from