Embed Size (px)
Citation preview

1
3
4
5
6
7
8 Q1
9
10
111213141516
17
1 9
20212223
24252627282930
3 1
5455
56
57
58
Human Immunology xxx (2014) xxx–xxx
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
Contents lists available at ScienceDirect
www.ashi-hla.org
journal homepage: www.elsevier .com/locate /humimm
A novel multiplex pyrosequencing assay for genotyping functionallyrelevant CTLA-4 polymorphisms: Potential applications in autoimmunityand cancer
http://dx.doi.org/10.1016/j.humimm.2014.04.0190198-8859/� 2014 Published by Elsevier Inc. on behalf of American Society for Histocompatibility and Immunogenetics.
Abbreviations: B-LCLs, B-lymphoblastoid cell lines; CTLA-4, cytotoxic T lymphocyte-associated antigen-4; HWE, Hardy Weinberg Equilibrium; IHWs, InteHistocompatibility Workshops; PB, peripheral blood; PSQ, pyrosequencing; SBT, sequence-based typing; SNPs, single nucleotide polymorphisms; SSc, systemic sclersequence specific primer; T-ARMS PCR, tetra-primer amplification refractory mutation system PCR.⇑ Corresponding author. Address: UOS Epigenetica dei Tumori, IRCCS A.O.U. San Martino-IST, Istituto Nazionale per la Ricerca sul Cancro, Largo Rosanna Benzi, 1
Genova, Italy. Fax: +39 0105737489.E-mail address: [email protected] (M.P. Pistillo).
1 These authors contributed equally to this work.
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequencing assay for genotyping functionally relevant CTLA-4 polymorpPotential applications in autoimmunity and cancer. Hum Immunol (2014), http://dx.doi.org/10.1016/j.humimm.2014.04.019
Barbara Banelli a,1, Anna Morabito a,1, Stefania Laurent a,b, Patrizia Piccioli c, Beatrice Dozin d,Massimo Ghio b, Paolo Antonio Ascierto e, Stefano Monteghirfo f, Vincenzo Ottaviano f, Paola Queirolo f,Massimo Romani a, Maria Pia Pistillo a,⇑a UOS Epigenetica dei Tumori, IRCCS A.O.U. San Martino-IST, Genova, Italyb Dipartimento di Medicina Interna e Specialità Mediche (DIMI), Università degli Studi di Genova, Genova, Italyc UOC Biologia cellulare, IRCCS A.O.U. San Martino-IST, Genova, Italyd UOC Epidemiologia Clinica, IRCCS A.O.U. San Martino-IST, Genova, Italye Unità di Oncologia Medica e Terapie Innovative, Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italyf UOC Oncologia Medica 2, IRCCS A.O.U. San Martino-IST, Genova, Italy
a r t i c l e i n f o a b s t r a c t
3233343536373839404142
Article history:Received 15 January 2014Accepted 27 April 2014Available online xxxx
Keywords:CTLA-4 single nucleotide polymorphismsPyrosequencingB-LCLsSclerodermic patientsMelanoma patients
434445464748495051
CTLA-4 expression/function can be affected by single nucleotide polymorphisms (SNPs) of CTLA-4 gene,which have been widely associated with susceptibility or progression to autoimmune diseases and cancerdevelopment.
In this study, we analyzed six CTLA-4 SNPs (�1661A > G, �1577G > A, �658C > T, �319C > T, +49A > G,CT60G > A) in 197 DNA samples from 43 B-lymphoblastoid cell lines (B-LCLs), 40 systemic sclerosis (SSc)patients, 14 pre-analyzed melanoma patients and 100 Italian healthy subjects.
Genotyping of �1661A > G, �1577G > A, �658C > T and CT60G > A was performed by newly developedmultiplex pyrosequencing (PSQ) assays, whereas �319C > T and +49A > G by T-ARMS PCR and directsequencing. Genotype/allele frequency were analyzed using v2 or Fisher exact test.
Our study provides the first multiplex PSQ method that allows simultaneous genotyping of two CTLA-4SNP pairs (i.e. �1661A > G/�658C > T and �1577G > A/CT60G > A) by two multiplex PSQ reactions.Herein, we show the CTLA-4 genotype distribution in the B-LCLs providing the first and best character-ized cell line panel typed for functionally relevant CTLA-4 SNPs.
We also report the significant association of the �1661A/G genotype, �1661 & �319 AC-GT diplotypeand �319 & CT60 TG haplotype with susceptibility to SSc without Hashimoto’s thyroiditis occurrence.Furthermore, we confirmed previous genotyping data referred to melanoma patients and providednew genotyping data for Italian healthy subjects.� 2014 Published by Elsevier Inc. on behalf of American Society for Histocompatibility and Immunoge-
netics.
52
5359
1. Introduction CTLA-4 may exert its inhibitory function through a variety of 6061
62
63
CTLA-4 is a transmembrane homodimer glycoprotein expressedby T cells upon activation, which negatively regulates their prolif-eration and effector functions [1].
molecular mechanisms, including: (i) recruitment of B7 (CD80/CD86) ligands on the surface of the antigen presenting cells [2]thus preventing their interaction with the co-stimulatory CD28molecule; (ii) interference with TCR-mediated signals [3] or
rnationalosis; SSP,
0, 16132
hisms:

64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
2 B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
association to signaling molecules [4] with subsequent attenuationof cell cycle progression, cytokine production and proliferation[5,6].
CTLA-4 is also constitutively expressed on regulatory T cells(Tregs) where it contributes to maintain their immunosuppressivefunction [7] and on different cellular types, both normal [6,8] andneoplastic [9–11].
The human CTLA-4 gene is located on chromosome 2q33 and iscomposed of 4 exons encoding for a leader sequence, an extracel-lular and a transmembrane domain and a cytoplasmic tail [12].CTLA-4 gene is highly polymorphic so that several single nucleo-tide polymorphisms (SNPs) have been identified, including�1661A > G, �1577G > A, �658C > T and �319C > T in the 50UTRand in the promoter region, +49A > G in the exon 1 and CT60G > Ain the 30UTR [13,14].
These CTLA-4 SNPs are functionally important as they mayinfluence the host immune response through alteration of CTLA-4expression levels and function in T cells. In particular, they canaffect the transcriptional efficiency of CTLA-4 gene [15], theprocessing and intracellular/surface transport of CTLA-4 protein[16], as well as the interaction between CTLA-4 and CD80 ligand[17].
CTLA-4 SNPs have been widely studied for their implication intwo major human diseases: autoimmune disorders [14] and cancer[17]. Considering that CTLA-4 optimal expression seems to be nec-essary for a safe and effective immune response, specific allelesassociated with a lower expression of CTLA-4 may induce hyperac-tivation of immune cells and confer susceptibility to autoimmunereactions, whereas other alleles associated with CTLA-4 overex-pression may suppress the immune cells and promote cancerdevelopment. Indeed, it has been reported that most autoimmunediseases are associated with the +49G allele, which appears todecrease CTLA-4 expression, whereas most cancers are associatedwith the +49A allele, which appears to increase CTLA-4 expression[18,19]. It is noteworthy that the above effects may occur in indi-viduals genetically and/or environmentally predisposed to autoim-munity or cancer [19].
Most of the published data are referred to the �319C > T,+49A > G and CT60G > A polymorphisms in different ethnic groups.However, other SNPs, such as �1661A > G, �1577G > A and�658C > T, are currently receiving attention for their link to auto-immune diseases [19–21] and cancer [17,19,22]. Indeed, the�1661A > G genotype has been found associated with a higher riskof development of Graves’ disease [23] and with lymph nodeinvolvement and estrogen receptor expression in breast cancer[22,24], whereas the influence of �1577G > A, �658C > T andCT60G > A in the clinical outcome of melanoma patients has beenrecently shown by our group [25] and other authors [26,27].CTLA-4 polymorphisms have been also implicated in the clinicaloutcome after allogeneic hematopoietic stem cell transplantationfrom HLA-identical sibling donors [28]. In this context, we havepreviously shown a significant association of the donor +49G/Ggenotype with longer overall survival [OS] and the number of+49G-alleles in the recipient with longer OS, longer disease-freesurvival and reduced relapse rate [28].
For all the above reasons, the availability of efficient genotypingmethods, as well as, of a reference cell line panel, might be, ingeneral, of great interest for assessment and validation of genotypescreening and in particular for CTLA-4 polymorphisms which arerelevant both in research and in clinical practice.
In this study, we have developed a new multiplex pyrosequenc-ing (PSQ) assay that discriminates both alleles of two CTLA-4 SNPpairs (i.e. �1661A > G/�658C > T and �1577G > A/CT60G > A) bytwo multiplex PSQ reactions.
By means of this novel method, we investigated the genotypedistribution of �1661A > G, �1577A > G, �658C > T and CT60G > A
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
in a panel of human B-lymphoblastoid cell lines (B-LCLs) fromdifferent International Histocompatibility Workshops and ingroups of Italian subjects, i.e. patients with systemic sclerosis(SSc), patients with melanoma (pre-analyzed) and healthy sub-jects. Both B-LCLs and healthy subjects were also typed for�319C > T and +49A > G SNPs by previously set up methods, beingthe SSc patients previously analyzed for those SNPs [29].
Thus, this study provides a panel of B-LCLs, typed for the mostfunctionally relevant CTLA-4 SNPs, which may be suitable as afuture reference cell panel for investigating CTLA-4 gene polymor-phisms in autoimmunity and cancer. Furthermore, the studyreports a significant association of the �1661A > G and CT60A > GSNPs with SSc without Hashimoto’s thyroiditis (HT) and providesuseful information, not available so far in the literature, aboutCTLA-4 �1661A > G, �1577A > G and �658C > T SNP allelefrequencies in the Italian population.
2. Materials and methods
2.1. B-LCLs, PB and DNA samples
The B-LCLs were from the HLA homozygous and heterozygousreference cell line panels of different International Histocompati-bility Workshops (IHWs) including the 10th, 12th and 13th IHWs[30,31] and the 4th AOHW (Asia-Oceania IHW) [32]. The B-LCLswere obtained from the European Collection for BiomedicalResearch (ECBR) cell line bank (http://www.nettab.org/ecbr/ecbrsite.html) and were cultured in RPMI 1640 (Euroclone, Milano,Italy) supplemented with 10% heat-inactivated fetal bovine serum(FBS; Euroclone), 1% antibiotic mixture (5 mg/ml penicillin and5 mg/ml streptomycin stock solution; Euroclone), 2 mM L-gluta-mine (Euroclone), at 37 �C in a humidified 5% CO2 atmosphere.B-LCLs had been extensively typed for HLA-A Class I and Class IIalleles by our laboratory during different IHWs by sequence-basedtyping (SBT) [33,34] and authenticated by sequence specific prim-ers (SSP) (Olerup SSP AB, Biospa Società Prodotti Antibiotici,Milano, Italy) [35] before using for the present study. HLA high res-olution typing of B-LCLs is available at the HLA Informatics Groupweb site (http://www.ebi.ac.uk/imgt/hla/).
Peripheral blood (PB) samples were collected from unrelatedhealthy blood donors, including females (n = 52; median age60 years, range 30–79) and males (n = 48; median age 60 years,range 32–75) derived from both the Transfusion Service of GallieraHospital and IRCCS A.O.U. San Martino-IST (Genova, Italy) uponwritten informed consent
Genomic DNA was extracted from B-LCL and PB samples byconventional proteinase K protocol as previously described [25].Genomic DNA samples from a subgroup of BLCLs (n = 12) fromthe 13th IHW, from SSc (n = 40; all females; median age 55 years,range 35–77) and melanoma patients (n = 14; 5 females and 9males; median age 58 years, range 33–73) analyzed for CTLA-4gene polymorphisms in previous studies [25,29], were alreadyavailable in our laboratory. For demographic and clinical character-istics of SSc and melanoma patients, as well as for the ethics com-mittee approvals, refer to those studies [25,29].
2.2. CTLA-4 genotyping
Genotyping of four CTLA-4 SNPs, i.e. �1661A > G (rs4553808),�1577G > A (rs11571316), �658C > T (rs11571317) in the 50UTRand in the promoter region and CT60G > A (rs3087243), presentin the 30UTR of the gene, was performed by newly developedassays based on the PSQ technology.
The primer sets for the PSQ assays (including a PCR primer pairand a sequencing primer) were designed with the Pyrosequencing
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx 3
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
Assay Design software (Biotage, Uppsala, SW). The PCR reactionswere performed by amplifying �200 ng genomic DNA in a finalvolume of 50 ll containing 200 mol/L dNTPs, 1� GeneAmp buffer(1.5 mM MgCl2), 1.25U of Immolase Hot Start polymerase (Bioline,Milan, Italy) and 0.3 lM of the PCR primer pairs specific for eachSNP.
Genotyping of CT60 was performed either with PCR primersalready published by Wang et al. [27] or with two newly designedadditional primers. In one case, the primer pair was the samedescribed by Wang et al. except for the degeneration of the for-ward primer to consider a G > C polymorphism (rs35482731) thathas been reported in the African/African-American subpopulationwithin the SNP500 Cancer project (http://variantgps.nci.nih.gov/cgfseq/pages/snp500.do). The other new primer pair is not affectedby the presence of any polymorphism within their sequences. Allthe PCR amplicons were pyrosequenced with the same sequencingprimer used by Wang et al. [27].
The sequence of all primers, the PCR amplification conditionsand the sequence of the pyrosequenced fragments are indicatedin Table 1.
The assembly of the PCR reactions was performed with anEpMotion5070 liquid handling station (Eppendorf, Milan, Italy);the PSQ assay [36] was performed with a PSQ 96MA instrument(Qiagen, Milan, Italy); sequencing reactions were performed withthe Pyro Gold reagent kit PSQ 96MA, according to the manufac-turer instructions. The sequencing analysis was conducted withthe PSQTM 96MA software (version 2.02). We performed this SNPgenotyping by carrying out two multiplex PCR reactions (CT60with �1577 and �658 with �1661 SNPs), both of them sequencedwith two multiplex pyrosequencing reactions. The SNP pairs in thePCR reactions were defined on the basis of the similarity of theamplicon lengths and the annealing temperature.
Genotyping of CTLA-4 �1577G > A, �1661A > G, �658C > Tand CT60G > A was also performed by alternative methods, i.e.
Table 1Primers and conditions for the analysis of CTLA-4 �1661A > G, �1577G > A, �658C > T an
The IUB (International Union of Biochemistry) codes of the polymorphisms are indicated�1577G > A and �658C > T polymorphisms are pyrosequenced on the reverse strand ofAbbreviations: SNPs, single nucleotide polymorphisms; Ta, annealing temperature; F, for1Sequence of CT60 forward primer published by Wang et al. in Ref. [27].2Sequence of CT60 forward primer with a degenerate sequence (S) for the SNP rs354823Sequence of the newly designed CT60 forward primer.
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
Tetra-primer Amplification Refractory Mutation System (T-ARMS)-PCR (for �1661A > G, �658C > T [25] and CT60G > A [25,28]) andSBT (for �1661A > G and �1577G > A SNPs [25]).
Genotyping of �319C > T (rs5742909, in the promoter) and+49A > G (rs231775, in the exon 1) SNPs was performed by previ-ously described T-ARMS-PCR and direct SBT protocols [25,28,29].
2.3. Statistical analysis
Deviation from the Hardy Weinberg Equilibrium (HWE) wasanalyzed with the Pearson chi-square test by using the de Finettiprogram (http://ihg2.helmholtz-muenchen.de/cgi-bin/hw/hwa1.pl). A P-value <0.05 indicates a lack of HWE.
Comparison of genotype and allele frequencies between groupswas performed by using the Pearson chi-square test or the Fisher’sexact test, as appropriate. The association between genotype fre-quency in the two subgroups of SSc patients (with and withoutHashimoto’s thyroiditis) was expressed as odds ratio (OR) with95% confidence intervals (CI) and estimated with the Fisher’s exacttest.
All statistical tests were two-sided and they were carried outusing the SPSS package (version 19.0 for Windows). Statistical sig-nificance was accepted for any P-value <0.05.
3. Results
3.1. Set up and validation of a multiplex PSQ assay for genotypingCTLA-4 �1661A > G, �1577G > A, �658C > T and CT60G > Apolymorphisms
In this study, we developed a PSQ-based genotyping assay forthe detection of CTLA-4 �1661A > G, �1577G > A, �658C > T andCT60G > A polymorphisms.
d CT60G > A polymorphisms.
in bold and in rectangles in the PCR primers and sequence to analyze (�1661A > G,DNA).
ward; R, reverse; Bio, biotinylated.
731 (see Section 2).
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
4 B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
This assay was designed to minimize DNA usage, economiceffort and time for screening studies. With the dedicated softwaredescribed in the Method section we designed the PCR and thesequencing reaction for each polymorphism separately. The PCRand the sequencing primers were designed in order to avoid anyknown polymorphism which could alter the genotyping, beingthe only exception that for the pyrosequencing assay for CT60polymorphism which was already described by Wang et al. [27].We have carefully evaluated whether the rare rs35482731 (G > C)SNP, described in the Method section and not considered in the for-ward primer, could affect the genotyping analysis.
To this purpose, we compared the genotyping results obtainedby introducing in this primer a degenerate base to take intoaccount the SNP rs35482731 or by designing an alternative PCRprimer pair without any known SNP in their sequence. In both ofthese approaches, we confirmed the genotyping results.
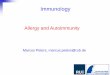
The four single assays were tested separately to check the opti-mal quality score after the PSQ reaction. The pyrograms of repre-sentative homozygous and heterozygous genotypes for each ofthe 4 SNPs analyzed are shown in Fig. 1, panel A.
Having defined the robustness of the four single assays, we setup the multiplex PCR and PSQ reactions to test simultaneously the�1577G > A/CT60G > A and �1661A > G/�658C > T, respectively. A
Fig. 1. Analysis of CTLA-4 �1661A > G, �1577G > A, �658C > T and CT60G > A polymorphthe heterozygote are shown for each polymorphisms. Panel A. Pyrograms showing CThomozygous genotypes carrying the �1661A, �1577G, �658C and CT60A alleles and thethe heterozygous genotypes relative to each SNP. Highlighted in yellow are the sequencesPSQ 96MA instrument. Sequencing reactions were performed with the Pyro Gold reagentwas conducted with the PSQTM 96MA software (�1661A > G, �1577G > A and �658C > TPCR showing genotypes of �1661A > G, �658C > T, CT60G > A SNPs and SBT showing geMolecular weight marker. (A) Product sizes of �1661A > G SNP were 290 bp for non-allelectropherograms for �1577G > A SNP. Representative analysis of homozygous G/G (ugenotypes. Arrows indicate the position of single nucleotide polymorphisms; (c) productallele and 145 bp for C allele band, respectively; (d) product sizes of CT60G > A SNP were 2band, respectively.
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
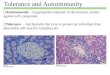
schematic representation of the procedure followed for the multi-plex PCR/PSQ assay is described in Fig. 2.
We tested two multiplex PCR reactions taking into account theamplicon length and the annealing temperature changes of thefragments considering every known polymorphism [37]. TheCTLA-4 genotyping performed by the multiplex PCR/PSQ was incomplete agreement with the single PCR/PSQ assay and previouslyset up protocols, as shown in Fig. 1, panel B, for each of the 4 SNPs.
The multiplex PSQ method was validated in a subgroup of B-LCLs (n = 12) from the 13th IHW and in a cohort of 14 melanomapatients already typed using other validated methods (i.e. T-ARMS-PCR and/or SBT) [25].
3.2. Genotype analysis of CTLA-4 �1661A > G, �1577G > A, �658C > Tand CT60G > A polymorphisms in a panel of B-LCLs by multiplex PSQ
Multiplex PSQ genotyping of �1661A > G, �1577A > G,�658C > T and CT60G > A was performed in a panel of 43 HLA-typed reference B-LCLs, derived from subjects of different genderand ethnic groups and included in different IHWCs.
To provide a reference panel of cell lines typed for the mostfunctionally relevant CTLA-4 SNPs, the B-LCLs were also genotypedfor the additional �319C > T and +49A > G SNPs, using protocols
isms by PSQ, T-ARMS PCR and SBT. Analysis of each one of the homozygotes and ofLA-4 genotypes of 4 representative B-LCLs. Upper and lower pyrograms show the�1661G, �1577A, �658T and CT60G alleles, respectively. Middle pyrograms showcorresponding to the polymorphism analyzed. The PSQ assay was performed with a
kit PSQ 96MA, according to the manufacturer’s instructions. The sequencing analysispolymorphisms are pyrosequenced on the reverse strand of DNA). Panel B. T-ARMSnotypes of �1577G > A SNP for the 4 representative B-LCLs of panel A. Mw: 50 bpele-specific control band, 181 bp for G allele and 159 bp for A allele; (b) Sequencepper panel), heterozygous G/A (middle panel) and homozygous A/A (lower panel)sizes of �658C > T SNP were 366 bp for non-allele-specific control band, 270 bp for T76 bp for non-allele-specific control band, 208 bp for G allele and 118 bp for A allele
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
Fig. 2. Schematic representation of the multiplex PCR/PSQ analysis of the 4 CTLA-4 polymorphism pairs: (A) CT60G > A & �1577G > A and (B) �658C > T & �1661A > G. Thetwo double PCR reactions are checked on a 3% agarose gel. The amplicons are purified, denaturated in a semi-automated work-station and only the biotinylated strands areretained and successively released to be annealed to the sequencing primers. In the black rectangles, the multiplex PSQ reactions are depicted; it is noteworthy that except forCT60 polymorphism, the other pyrosequencing reactions take place on the reverse strand. Below, some representative multiplex pyrograms of different B-LCLs: three sampleswith different genotyping for the four polymorphisms are analyzed with our multiplex PCR/PSQ assay: the three pyrograms on the left analyze the genotyping of CT60G > A &�1577G > A; the three pyrograms on the right analyze the genotyping of �658C > T & �1661A > G. The yellow rectangles represent the polymorphic sites to be interrogated.
B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx 5
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
previously described [25,28,29]. The genotype distribution of thesix CTLA-4 SNPs analyzed in this B-LCL panel is reported in Table 2.
The IHWC B-LCLs constitute a well-characterized reference cellline panel for polymorphisms of the HLA [30–32] and the killer-cellimmunoglobulin-like receptor gene [38]. Thus, this panel providesB-LCLs representative of some major HLA alleles, B⁄38, C⁄3, C⁄15and DRB1⁄15, indicated in Table 3 according to the nomenclatureassigned by the WHO Nomenclature Committee for Factors of theHLA System [39], that are associated to autoimmune diseases[40]. Interestingly, these HLA alleles, either single or in combina-tion with the CTLA-4 CT60 G/G genotype of CTLA-4, have also beenreported to represent a five-marker genotyping signature able topredict OS in melanoma patients receiving adjuvant IFN-c [27].
336
337
338
339
340
341
342
343
344
345
346
347
348
349
3.3. Genotype analysis of CTLA-4 �1661A > G, �1577G>, �658C > Tand CT60G > A SNPs in Italian SSc patients and healthy controls bymultiplex PSQ
We performed genotyping of CTLA-4 �1661A > G, �1577G > A,�658C > T and CT60G > A SNPs, by the multiplex PSQ assay, inDNA specimens from 40 SSc female patients and 52 sex- andage-matched healthy Italian subjects. All the healthy donors werealso genotyped for �319C > T and +49A > G SNPs as already donefor the SSc patients [29]. Genotyping of SSc samples by multiplexPSQ was repeated twice and a perfect concordance between resultswas obtained for each SNP analyzed.
The genotype distribution and allele frequencies of the CTLA-4variants analyzed in SSc patients and in healthy controls arereported in Table 4.
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
As shown, no deviation from the Hardy–Weinberg Equilibriumwas observed for any of the polymorphisms both in SSc patientsand in healthy controls. Similar frequencies of genotypes and ofalleles were found in both groups of subjects, for all the 6 CTLA-4SNPs analyzed.
It is of note that the rare homozygotes for the �658T/T weredetected amongst the SSc and/or the healthy subjects studied, thusconfirming the ability of our PSQ method to identify this genotype.
The Italian controls in Table 4 included only sex-matched sub-jects; however no statistical differences in CTLA-4 genotype fre-quencies were also found between SSc patients and a panel of100 Italian controls which included 48 male subjects, as shownin Supplementary Table 1.
The allele and the genotype frequencies in our healthy controlsare similar to those previously reported by our [25] and othergroups for the healthy Italian [41,42] and European populations[43]. Moreover, our results show the frequency of three SNPs ana-lyzed (�1661A > G, �1577G > A and �658C > T) that was notreported, so far, for the Italian population.
3.4. Genotype frequencies of CTLA-4 SNPs in SSc clinical subsetsaccording to the Hashimoto’s thyroiditis status
The SSc patients were subdivided into 2 groups according to thepositivity for the anti-thyroperoxidase (TPO) and anti-thyroglobu-lin (TGA) auto-antibodies which define a group of clinically pecu-liar SSc patients with the associate occurrence of Hashimoto’sthyroiditis (HT), as previously described [29]. In our series, 20patients were negative (SSc/HT�) and 20 were positive (SSc/HT+)
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
Table 2Genotyping of CTLA-4 polymorphisms in B-LCLs from the 10th to the 13th IHWs and from the 4th AOHW.
IHW No. B-LCLs Sex Origin CTLA-4 polymorphisms
�1661 A > G �1577 G > A �658 C > T �319 C > T +49 A > G CT60 G > A
9002 MZO70782 M 1a A/A A/A C/C C/C A/A A/A9007 DEM M 1b A/G G/G C/C C/C A/G G/G9014 MGAR F 1c A/A G/A C/C C/C A/G G/A9023 VAVY F 1d A/A G/A C/C C/C A/A A/A9024 KT17 F 2a A/A G/A C/C C/C A/G G/A9025 DEU M 1e A/A A/A C/T C/C A/A A/A9042 TISI F 1d A/G G/A C/C C/C A/A G/A9044 BR1P M 1d A/A G/G C/C C/C G/G G/G9045 TUBO F 1d A/G G/A C/C C/T A/A G/A9047 PLH F 1g G/G G/G C/C C/C A/A G/G9057 TEM M 1h A/A G/G C/C C/C G/G G/G9058 OMW M 3a A/A G/G C/C C/C A/G G/G9063 WT47 M 1f A/G G/G C/C C/C A/A G/A9064 AMALA F 4a A/A G/G C/C C/C G/G G/G9066 TAB089 M 2a A/A G/G C/C C/C G/G G/G9068 BM9 F 1f A/A A/A C/T C/C A/A A/A9071 OLGA F 4a A/A G/G C/C C/C G/G G/G9077 T7527 F 2b A/A G/A C/C C/C A/G G/A9084 CALOGERO M 1f A/A G/A C/C C/C A/G G/A9085 EJ32B F 1i A/G G/G C/C C/T A/G G/G9089 BOB F 1b A/A G/G C/C C/C G/G G/G9092 BM92 M 1f A/A A/A C/C C/C A/A A/A9095 WIN M 1b A/A G/G C/C C/C A/G G/G9101 SPL M 4a A/A A/A C/C C/C A/A A/A9103 KT14 M 2a A/A G/A C/C C/C A/G G/A9107 LKT3 M 2a A/A G/A C/C C/C A/G G/A9111 TAI 034 M 2c A/A G/A C/T C/C A/A A/A9114 WIL,M F 1 A/A G/A C/C C/C A/G G/A9115 BAT,J Un Un G/G G/G C/C C/C A/A G/G9121 CHI013 M 2c A/G G/G C/C C/T A/G G/G9122 WOO,EM F 4b A/A G/A C/C C/C A/G G/A9202 BYD,A F 1 A/A G/A C/C C/C A/G G/A9222 KY M 2a A/G G/A C/C C/T A/A G/A9224 RSA-ND M 2d A/G G/G C/C C/T A/A G/G9231 32511 F 3c A/G G/G C/C C/C A/A G/G9238 VEN Un 1 A/A A/A C/C C/C A/A A/A9239 SHJO Un 3b A/A G/G C/C C/C G/G G/G9253 THAI742 M 2c A/G G/A C/C C/T A/A G/A9254 BJ M Un A/G G/A C/C C/C A/A G/A9273 LADA F 3c A/A G/G C/C C/C A/G G/G9278 31708 F 3c A/G G/G C/C C/C A/A G/G9286 AKIBA F 2a A/A G/G C/C C/C G/G G/G9287 JY M 4c A/G G/G C/C C/C A/G G/G
The cell line panel from the 10th IHW (9002 to 9107 B-LCLs), the 12th IHW (9222 to 9287 B-LCLs) and the 4th AOHW (9111 to 9202 B-LCLs), consists of B-LCLs from subjectsof different gender and ethnic groups including Caucasians (46%), Orientals (25%), Blacks (12%), others (12%) and unknown (Un; 5%) ethnicities. This panel includes at leasttwo examples of every homozygous and heterozygous genotype for each of the SNP analyzed, except for the �658C > T and �319C > T SNPs (http://www.ncbi.nlm.nih.gov/projects/SNP) for which no homozygotes for the rare T allele were detected.Genotyping of �1661A > G, �1577A > G, �658C > T and CT60G > A was performed by the newly developed PSQ method and validated by previously set up T-ARMS PCR andSBT protocols. Genotyping of �319C > T and +49A > G was performed by T-ARMS PCR and SBT.Numbers in the origin column indicate the B-LCL ethnicity as follows: 1Caucasian: aAshkenazi Jew, bGerman, cHispanic/North American, dFrench, eDutch, fItalian, g-
Scandinavian, hJewish, iAustralian; 2Oriental: aJapanese, bChinese, cThai, dFilipino; 3Black: aAfrican, bAmerican, cAfrican American; 4Others: aIndian/Warao/South American;bAustralian /Aboriginal; cAmish.
6 B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
for the presence of such antibodies. The comparison of these twogroups (Table 5) has shown that the percentage of subjects carry-ing the homozygous �1661A/A genotype was lower in SSc/HT�patients (40%) than in SSc/HT+ patients (80%), whereas thepercentage of heterozygous �1661A/G genotype was significantlyhigher in SSc/HT� patients (55%) than in SSc/HT+ patients (15%)(Fisher’s test, A/G vs A/A, OR 7.33 95% CI 1.58–33.96; P = 0.011).This difference was confirmed at the level of the�1661G allele thatshowed a significant difference between SSc/HT� and SSc/HT+patients (Fisher’s test, G vs A, OR 3.37 95% CI 1.07–10.61;P = 0.038). Concerning the �319C > T polymorphism, the signifi-cant frequencies, previously described [29] for the �319C/T geno-type (P = 0.022) and for the T allele (P = 0.037) in SSc/HT� ascompared to SSc/HT+ patients, are also shown.
A significantly higher frequency was observed for the CT60Gallele between SSc/HT� patients (0.65) and SSc/HT+ patients
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
(0.42) (Fisher’s test, G vs A, OR 2.52 95% CI 1.02–6.20; P = 0.046)(Table 5).
3.5. Haplotype and diplotype frequencies of CTLA-4 �1661A > G,�319C > T and CT60G > A polymorphisms in SSc/HT� and SSc/HT+patients
The frequencies of haplotypes and diplotypes have been ana-lyzed within the two groups of SSc patients (Table 6). Since wehave previously shown a significant association of the �319T posi-tive genotypes (genotypes C/T and T/T) with SSc without HT [29],we also included this polymorphism in the haplotype and diplo-type analysis.
Haplotype analysis of �1661 & �319 showed a trend towards asignificantly higher frequency of the GT haplotype in SSc/HT� thanin SSc/HT+ patients (22.5% vs 5%; v2 test: P = 0.060) whereas the TG
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
Q2
Table 3B-LCLs showing the major HLA alleles with clinical relevance in autoimmune diseasesand melanoma.
IHW No. B-LCLs HLA alleles CTLA-4 CT60 genotype
B⁄ C⁄ DRB1⁄
9057 TEM 38:01:01 G/G9224 RSA-ND 38:02:01 G/G9024 KT17 03:039064 AMALA 03:03 G/G9238 VEN 03:039253 THAI742 03:039071 OLGA 03:04 G/G9045 TUBO 15:029089 BOB 15:02 G/G9014 MGAR 15:019122 WOO,EM 15:019111 TAI 034 15:029286 AKIBA 15:02 G/G
The indicated HLA-B⁄, C⁄ and DRB1⁄ alleles have been typed by SSP and direct SBT.Alleles have been indicated according to the official allele designations given by theWHO Nomenclature Committee for Factors of the HLA System (2010). Genotypingof CT60G > A was performed by the newly developed PSQ method and validated bypreviously set up protocols.The HLA alleles shown, alone or in combination with CTLA-4 CT60G/G genotype,may have prognostic significance on OS of melanoma patients as reported in Ref.[27].Abbreviations: B-LCLs, B-lymphoblastoid cell lines; IHW, International Histocom-patibility Workshop.
B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx 7
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
haplotype frequency of �319 & CT60 was significantly different inSSc/HT� and SSc/HT+ groups (22.5 vs 5.0%; v2 test: P = 0.034;Table 6). A trend was observed for a higher frequency of the
Table 4Frequencies of six CTLA-4 polymorphisms in SSc patients and in sex- and age-matched co
n (%)
Genotypes SSc patients (n = 40) Controls (n = 52) P–
�1661A > GA/A 24 (60.0) 29 (56.0) 0.845A/G 14 (35.0) 19 (36.0)G/G 2 (5.0) 4 (8.0)HWE P = 0.982 P = 0.720
�1577G > AG/G 16 (40.0) 19 (36.6) 0.918G/A 16 (40.0) 21 (40.4)A/A 8 (20.0) 12 (23.0)HWE P = 0.291 P = 0.201
�658C > TC/C 33 (82.5) 46 (88.4) 0.449C/T 6 (15.0) 6 (11.6)T/T 1 (2.5) 0 (-)HWE P = 0.292 P = 0.659�319C > T*
C/C 29 (72.5) 42 (80.8) 0.188C/T 11 (27.5) 8 (15.4)T/T 0 (-) 2 (3.8)HWE P = 0.313 P = 0.076
+49A > G*
A/A 15 (37.5) 25 (48.1) 0.555A/G 23 (57.5) 24 (46.1)G/G 2 (5.0) 3 (5.8)HWE P = 0.072 P = 0.370
CT60G > AG/G 13 (32.5) 18 (34.6) 0.973G/A 17 (42.5) 21 (40.4)A/A 10 (25.5) 13 (25.0)HWE P = 0.358 P = 0.183
Genotyping of �1661A > G, �1577A > G, �658C > T and CT60G > A was performed byGenotyping of �319C > T and +49A > G was performed by T-ARMS PCR and SBT. HWE wP– value as estimated by the Pearson’s v2 test and P⁄ as estimated by the Fisher’s test. SAbbreviations: SSc, systemic sclerosis; HWE, Hardy–Weinberg Equilibrium.* For SSc patients, the frequencies of �319C > T and +49A > G genotypes are those prev
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
�1661 & CT60 haplotype GG in SSc/HT� as compared to SSc/HT+patients (32.5% vs 12.5%; v2 test: P = 0.055; Table 6).
In addition, the analysis of diplotypes (haplotype combinations)has shown a significant difference in the frequency of individualscarrying the �1661 & �319 AC-GT diplotype (HT�: 40.0% vsHT+: 5%; v2 test: P = 0.040) and a trend towards a significantlyhigher frequency of individuals carrying the �319 & CT60 CA-TGdiplotype (HT�: 20.0% vs HT+: 0%; v2 test: P = 0.050; Table 6).
No significant differences were observed for the �1661 & CT60diplotypes, as well as for the other SNP haplotypes/diplotypes,between SSc/HT� and SSc/HT+ patients. The frequencies of haplo-types and diplotypes were not statistically different betweenpatients and controls (data not shown).
4. Discussion
Several studies have shown that specific CTLA-4 gene polymor-phisms are associated with susceptibility to autoimmune diseases[14,19–21] and to cancer development or progression [24–27].
All these findings point out the increasing importance of detect-ing CTLA-4 gene polymorphisms by accurate and sensitive geno-typing methodologies.
In this study, we describe the development of a specific andrapid multiplex PSQ-based method that allows the simultaneousamplification and discrimination of both alleles of two CTLA-4SNP pairs (i.e. �1661A > G/�658C > T and �1577G > A/CT60G > A)in a panel of extensively studied IHW B-LCLs and Italian controls.Both the B-LCLs and Italian controls were also analyzed for twoadditional CTLA-4 SNPs (�319C > T and +49A > G). Therefore, the
ntrol subjects.
n (frequency)
Alleles SSc patients (2n = 80) Controls (2n = 104) P⁄
�1661A > GA 62 (0.78) 77 (0.74) 0.609G 18 (0.22) 27 (0.26)
�1577G > AG 48 (0.60) 59 (0.57) 0.763A 32 (0.40) 45 (0.43)
�658C > TC 72 (0.90) 98 (0.94) 0.401T 8 (0.10) 6 (0.06)
�319C/TC 69 (0.86) 92 (0.88) 0.660T 11 (0.14) 12 (0.12)
+49A/GA 53 (0.66) 74 (0.71) 0.522G 27 (0.34) 30 (0.29)
CT60 > GAG 43 (0.54) 57 (0.55) 1.000A 37 (0.46) 47 (0.45)
the newly developed PSQ method and validated by previously set up protocols.as tested by the Pearson v2 test (P < 0.05 indicates a lack of HWE).tatistical significance: P < 0.05.
iously reported in Ref. [29].
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
Table 5Frequencies of CTLA-4 �1661A > G and CT60G > A polymorphisms in SSc patients according to anti-TPO/TGA status.
CTLA-4 genotypes n (%) OR (95% CI) P⁄ Alleles n (frequency) OR (95% CI) P⁄
HT� (n = 20) HT+ (n = 20) HT� (2n = 40) HT+ (2n = 40)
�1661A > G �1661A > GA/A 8 (40.0) 16 (80.0) A/G vs A/A 0.011 A 27 (0.67) 35 (0.88) G vs A 0.038A/G 11 (55.0) 3 (15.0) 7.33 (1.58–33.96) G 13 (0.33) 5 (0.12) 3.37 (1.07–10.61)G/G 1 (5.0) 1 (5.0)
�319C > T �319C > TC/C 11 (55.0) 18 (90.0) C/T vs C/C 0.022 C 31 (0.77) 38 (0.95) T vs C 0.037C/T 9 (45.0) 2 (10.0) 7.36 (1.33–40.55) T 9 (0.23) 2 (0.05) 5.52 (1.11–27.43)T/T 0 (-) 0 (-)
CT60G > A CT60G > AG/G 9 (45.0) 4 (20.0) G/G vs A/A 0.070 G 26 (0.65) 17 (0.42) G vs A 0.046G/A 8 (40.0) 9 (45.0) 5.25 (0.87–31.55) A 14 (0.35) 23 (0.58) 2.52 (1.02–6.20)A/A 3 (15.0) 7 (35.0)
The SSc patients were subdivided into HT� and HT+ groups according to the positivity for the anti-thyroperoxidase (TPO) and anti-thyroglobulin (TGA) auto-antibodies, aspreviously described [29].P⁄value was referred to the OR (95% CI) and estimated by the Fisher’s test. Statistical significance: P < 0.05.Abbreviations: anti-TPO, anti-thyroperoxidase auto-antibodies; anti-TGE, anti-thyroglobulin auto-antibodies; SSc, systemic sclerosis; HT�, SSc patients negative for anti-TPO/TGA; HT+, SSc patients positive for anti-TPO/TGA; OR, Odds ratio; 95% CI, 95% confidence interval.
Table 6Frequencies of haplotypes and diplotypes of �1661A > G, �319 C > T and CT60G > ACTLA-4 polymorphisms in SSc/HT� and SSc/HT+ patients.
n (%) P–
HT� (2n = 40) HT+ (2n = 40)
Haplotypes �1661 & �319AC 27 (67.5) 35 (87.5)GC 4 (10.0) 3 (7.5) 0.060GT 9 (22.5) 2 (5.0)
Diplotypes (n = 20) (n = 20)AC-AC 8 (40.0) 16 (80.0) 0.040AC-GC 3 (15.0) 2 (10.0)AC-GT 8 (40.0) 1 (5.0)GC-GT 1 (5.0) 1 (5.0)
Haplotypes �319 & CT60 (2n = 40) (2n = 40)CA 14 (35.0) 23 (57.5) 0.034CG 17 (42.5) 15 (37.5)TG 9 (22.5) 2 (5.0)
Diplotypes (n = 20) (n = 20)CA-CA 3 (15.0) 7 (35.0) 0.050CG-CA 4 (20.0) 9 (45.0)CG-CG 4 (20.0) 2 (10.0)CG-TG 5 (25.0) 2 (10.0)CA-TG 4 (20.0) 0 (-)
Haplotypes �1661 & CT60 (2n = 40) (2n = 40)AA 14 (35.0) 23 (57.5) 0.055AG 13 (32.5) 12 (30.0)GG 13 (32.5) 5 (12.5)
Diplotypes (n = 20) (n = 20)AA-AA 3 (15.0) 7 (35.0) 0.185AA-GG 4 (20.0) 1 (5.0)AG-AA 4 (20.0) 8 (40.0)AG-AG 1 (5.0) 1 (5.0)AG-GG 7 (35.0) 2 (10.0)GG-GG 1 (5.0) 1 (5.0)
Haplotypes and diplotype analysis including the �319C > T SNP previously foundassociated with SSc without HT [29].P value as estimated by the Pearson’s v2 test. Statistical significance: P < 0.05.Abbreviations: HT�, SSc patients negative for anti-TPO/TGA; HT+, SSc patientspositive for anti-TPO/TGA.
8 B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
B-LCLs provide the first and best characterized IHW cell line paneltyped for functionally relevant CTLA-4 SNPs useful for test develop-ment, validation and comparison of the results obtained in differ-ent laboratories.
The PSQ method was further used for typing a group of sclero-dermic patients and sex and age-matched healthy control subjects.
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
In this context we demonstrated that the frequency of �1661A/Ggenotype and of GT (�1661G and �319T) and TG (�319T andCT60G) haplotypes are higher in SSc/HT� patients than in SSc/HT+ patients, thus suggesting that individuals carrying these geno-type and haplotypes may be protected from the development ofSSc with a concomitant HT. Although, further studies on largerSSc patient cohorts are needed to definitely confirm these findings,these results underlie the possible relevance of other two CTLA-4polymorphisms in the pathogenesis of SSc in addition to the previ-ously described �319C > T SNP [29].
In the context of cancer, the perfect correlation between thegenotyping results of melanoma patients obtained by the PSQand T-ARMS PCR, or other alternative methodologies [25,28,29],confirms the robustness and reproducibility of the PSQ method,thus providing its validation.
The PSQ method may therefore find application to assess CTLA-4 polymorphisms as biomarkers of response to CTLA-4 blockadetherapy not only in melanoma patients where this therapy isalready being used [25], but also in tumors of different histotypesfor which the CTLA-4 blockade approach is still under investigationin ongoing trials [44].
The �1661A > G, �1577G > A, �658C > T and CT60G > A SNPshave been predominantly analyzed, in previous studies, by RFLP[45,46], SBT [25], real-time quantitative PCR (QRT-PCR) [47],T-ARMS PCR [25,28] or SNaP shotTM Multiplex Kit [21]. To ourknowledge, PSQ has not been used to date for the single or simul-taneous analysis of �1661A > G, �1577G > A, �658C > T SNPs,whereas it has been used for the analysis of CT60 SNP [27,48].although using different primers and PCR conditions and not inmultiplex assays with other SNPs.
One advantage of the PSQ technique, over the other approaches,is that PSQ is an extremely robust and sensitive technique. Forinstance, genotyping by sequencing requires that the SNPs arelocalized within a distance that can be accurately read by theinstrument; on the contrary, the multiplex PSQ is independentfrom the relative position of the target sequences; moreover PSQhas a limit of detection, for mutations, of approximately 5% as com-pared to the 15–20% of the conventional sequencing [49]. An addi-tional advantage of PSQ over PCR-based techniques is that it is alargely automated procedure that, if the assay is properly opti-mized, provides absolute results without internal references anddoes not require subjective data interpretation.
The chemistry at the basis of PSQ is very reliable and robust.As we have already noted, this technique, utilized for a very
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530531532533534535536537538539540541542543544545546547548549550551552553554555556557
B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx 9
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
demanding multiplex assay for methylation analysis, is very repro-ducible [50]. Similarly, the reproducibility of the multiplex geno-typing of CTLA-4 is very high and we did not observe discordantresults among replicates and repeated assays.
The cost of PSQ genotyping strictly depends from the number ofpatients analyzed at the same time and is comparable to that of theother techniques with the exception of T-ARMS which ischeaper and does not require the use of special equipment.Moreover, PSQ can be fully automated and is more versatile, notonly to detect two SNPs simultaneously, but also to analyzepolymorphisms characterized by insertions/deletions of repeatedsequences [51].
The entire procedure of our PSQ approach, starting from puri-fied DNA, takes about 3.30 h (PCR amplification, gel electrophore-sis, sample purification, set up of the reaction and PSQ reaction).Data acquisition is available immediately after completion of thePSQ reaction.
Our novel assay halves the time-consuming and the economiceffort respect to the same genotyping performed with four PSQ sin-gle assays. This multiplex assay could be useful to rapidly genotypea high number of samples in screening studies or in large geneticpopulation studies.
CTLA-4 genotyping by PSQ requires a proprietary platform andthe cost of the instrument might be a limitation of this assay. How-ever, PSQ-based diagnostic and research procedures are becomingvery common in many different areas (cancer, microbiology, phar-macogenomics etc.) and PSQ is becoming the reference method forthe clinical detection of site-specific mutations like those of BRAFand KRAS genes [52,53].
In conclusion, our results show a rapid and sensitive pyrose-quencing-based method that may represent a reliable and repro-ducible tool for determining CTLA-4 �1661A > G, �1577G > A,�658C > T and CT60G > A polymorphisms in patients with autoim-mune diseases, as well as in cancer patients and in control subjects.In particular, the simplicity of the method makes it particularlyuseful for assessing the SNPs, within few hours after genomicDNA isolation, also in large cohorts of patients.
558559560561562563564565566567568569570571572573574
Disclosure
Dr. Paola Queirolo participated to Advisory Board from BristolMyers Squibb, Merck Sharp and Dohme, Roche-Genentech, GlaxoSmith Kline. She received honoraria from Bristol Myers Squibband Roche-Genentech.
Dr. Paolo Ascierto is consultant for Merck Sharp and Dohme. Heparticipated to Advisory Board from Bristol Myers Squibb, MerckSharp and Dohme, Roche-Genentech, Glaxo Smith Kline, Amgen,Celgene, Medimmune, Novartis. He received honoraria from BristolMyers Squibb, Merck Sharp and Dohme, Roche-Genentech.
575576577578579580581582583584585586587588589590591592593594595
Authors’ contributions
BB developed assays based on the PSQ technology andperformed PSQ assays; AM collected samples, performed Tetra-ARMS PCR, SBT and PSQ assays, SL cultured B-LCLs and performedTetra-ARMS PCR, PP performed Tetra-ARMS PCR and SBT; MG coor-dinated systemic sclerosis patients; PAA, SM, VO and PQ coordi-nated melanoma patients; MR participated in the design of thestudy; MPP conceived the study and drafted the manuscript. Allauthors read and approved the final manuscript.
Acknowledgements
This work was supported by grants from Ricerca Sanitaria Reg-ione Liguria (Dgr 563/2009). The authors thank the blood donors
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
and staff of both the Transfusion Centers of Galliera Hospital andthe IRCCS A.O.U. San Martino-IST, Genova, Italy, for kindly provid-ing buffy coats. They also thank P. Peirano for collection of bloodsamples from melanoma patients and G. Allemanni for technicalsupport. B.B. is the recipient of the ‘‘Young Investigators’’ grantGR-2008-1143408 from the Italian Ministry of Health.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.humimm.2014.04.019.
References
[1] Walunas TL, Lenschow DJ, Bakker CY, Linsley PS, Freeman GJ, Green JM, et al.CTLA-4 can function as a negative regulator of T cell activation. Immunity1994;1:405–13.
[2] Masteller EL, Chuang E, Mullen AC, Reiner SL, Thompson CB. Structural analysisof CTLA-4 function in vivo. J Immunol 2000;164:5319–27.
[3] Chikuma S, Imboden JB, Bluestone JA. Negative regulation of T cell receptor-lipid raft interaction by cytotoxic T lymphocyte-associated antigen 4. J ExpMed 2003;197:129–35.
[4] Teft WA, Chau TA, Madrenas J. Structure-Function analysis of the CTLA-4interaction with PP2A. BMC Immunol 2009;30:10–23.
[5] Krummel MF, Allison JP. CTLA-4 engagement inhibits IL-2 accumulation andcell cycle progression upon activation of resting T cells. J Exp Med1996;183:2533–40.
[6] Teft WA, Kirchhof MG, Madrenas J. A molecular perspective of CTLA-4 function.Annu Rev Immunol 2006;24:65–97.
[7] Jonuleit H, Schmitt E, Stassen M. Identification and functional characterizationof human CD4(+)CD25(+) T cells with regulatory properties isolated fromperipheral blood. J Exp Med 2001;193:1285–94.
[8] Laurent S, Carrega P, Saverino D, Piccioli P, Camoriano M, Morabito A, et al.CTLA-4 is expressed by human monocyte-derived dendritic cells and regulatestheir functions. Hum Immunol 2010;71:934–41.
[9] Laurent S, Queirolo P, Boero S, Salvi S, Piccioli P, Boccardo S, et al. Theengagement of CTLA-4 on primary melanoma cell lines induces antibody-dependent cellular cytotoxicity and TNF-alpha production. J Transl Med2013;11:108–21.
[10] Pistillo MP, Tazzari PL, Palmisano GL, Pierri I, Bolognesi A, Ferlito F, et al. CTLA-4 is not restricted to the lymphoid cell lineage and can function as a targetmolecule for apoptosis induction of leukemic cells. Blood 2003;101:202–9.
[11] Contardi E, Palmisano GL, Tazzari PL, Martelli AM, Falà F, Fabbi M, et al. CTLA-4is constitutively expressed on tumor cells and can trigger apoptosis uponligand interaction. Int J Cancer 2005;117:538–50.
[12] Dariavach P, Mattéi MG, Golstein P, Lefranc MP. Human Ig superfamily CTLA-4gene: chromosomal localization and identity of protein sequence betweenmurine and human CTLA-4 cytoplasmic domains. Eur J Immunol1988;18:1901–5.
[13] Johnson GC, Esposito L, Barratt BJ, Smith AN, Heward J, Di Genova G, et al.Haplotype tagging for the identification of common disease genes. Nat Genet2001;29:233–7.
[14] Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, et al.Association of the T-cell regulatory gene CTLA4 with susceptibility toautoimmune disease. Nature 2003;423:506–11.
[15] Wang XB, Zhao X, Giscombe R, Lefvert AK. A CTLA-4 gene polymorphism atposition -318 in the promoter region affects the expression of protein. GenesImmun 2002;3:233–4.
[16] Anjos S, Nguyen A, Ounissi-Benkalha H, Tessier MC, Polychronakos C. Acommon autoimmunity predisposing signal peptide variant of the cytotoxic T-lymphocyte antigen 4 results in inefficient glycosylation of the susceptibilityallele. J Biol Chem 2002;277:46478–86.
[17] Sun T, Zhou Y, Yang M, Hu Z, Tan W, Han X, et al. Functional genetic variationsin cytotoxic T-lymphocyte antigen 4 and susceptibility to multiple types ofcancer. Cancer Res 2008;68:7025–34.
[18] Zhang Y, Zhang J, Deng Y, Tian C, Li X, Huang J, et al. Polymorphisms in thecytotoxic T-lymphocyte antigen 4 gene and cancer risk: a meta-analysis.Cancer 2011;117:4312–24.
[19] Ghaderi A. CTLA4 gene variants in autoimmunity and cancer: a comparativereview. Iran J Immunol 2011;8:127–49.
[20] Almasi S, Erfani N, Mojtahedi Z, Rajaee A, Ghaderi A. Association of CTLA-4gene promoter polymorphisms with systemic sclerosis in Iranian population.Genes Immun 2006;7:401–6.
[21] Palacios R, Comas D, Elorza J, Villoslada P. Genomic regulation of CTLA4 andmultiple sclerosis. J Neuroimmunol 2008;203:108–15.
[22] Li D, Zhang Q, Xu F, Fu Z, Yuan W, Li D, et al. Association of CTLA-4 genepolymorphisms with sporadic breast cancer risk and clinical features in Hanwomen of northeast China. Mol Cell Biochem 2012;364:283–90.
[23] Chistiakov DA, Savost’anov KV, Turakulov RI, Efremov IA, Demurov LM.Genetic analysis and functional evaluation of the C/T(�318) and A/G(�1661)
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019

596597598599600601602603604605606607608609610611612613614615616617618619620621622623624625626627628629630631632633634635636637638639640641642643644645646647
648649650651652653654655656657658659660661662663664665666667668669670671672673674675676677678679680681682683684685686687688689690691692693694695696697698699
10 B. Banelli et al. / Human Immunology xxx (2014) xxx–xxx
HIM 9369 No. of Pages 10, Model 5G
9 May 2014
polymorphisms of the CTLA-4 gene in patients affected with Graves’ disease.Clin Immunol 2006;118:233–42.
[24] Erfani N, Razmkhah M, Talei AR, Pezeshki AM, Doroudchi M, Monabati A, et al.Cytotoxic T lymphocyte antigen-4 promoter variants in breast cancer. CancerGenet Cytogenet 2006;165:114–20.
[25] Queirolo P, Morabito A, Laurent S, Lastraioli S, Piccioli P, Ascierto PA, et al.Association of CTLA-4 polymorphisms with improved overall survival inmelanoma patients treated with CTLA-4 blockade: a pilot study. Cancer Invest2013;3:336–45.
[26] Breunis WB, Tarazona-Santos E, Chen R, Kiley M, Rosenberg SA, Chanock SJ.Influence of cytotoxic T lymphocyte-associated antigen 4 (CTLA4) commonpolymorphisms on outcome in treatment of melanoma patients with CTLA-4blockade. J Immunother 2008;3:586–90.
[27] Wang E, Zhao Y, Monaco A, Uccellini L, Kirkwood JM, Spyropoulou-Vlachou M,et al. A multi-factorial genetic model for prognostic assessment of high riskmelanoma patients receiving adjuvant interferon. PLoS ONE2012;7(7):e40805.
[28] Piccioli P, Balbi G, Serra M, Morabito A, Lamparelli T, Gobbi M, et al. CTLA-4+49A>G polymorphism of recipients of HLA-matched sibling allogeneic stemcell transplantation is associated with survival and relapse incidence. AnnHematol 2010;89:613–8.
[29] Balbi G, Ferrera F, Rizzi M, Piccioli P, Morabito A, Cardamone L, et al.Association of �318 C/T and +49 A/G cytotoxic T lymphocyte antigen-4 (CTLA-4) gene polymorphisms with a clinical subset of Italian patients with systemicsclerosis. Clin Exp Immunol 2007;149:40–7.
[30] Prasad VK, Yang SY. Allele assignment for HLA-A, -B, and -C genes to the TenthInternational Histocompatibility Workshop cell lines. Tissue Antigens1996;47:538–46.
[31] Hansen JA, Dupont B, editors. Proceedings of the 13th internationalhistocompatibility workshop and congress. Seattle, WA: IHWG Press; 2004.vols. I & II.
[32] 4th Asia-Oceania Histocompatibility Workshop. April 22–29, 1993. Perth,Western Australia. Proceedings. Hum Immunol 1993 Sep; 38(1);1–852.
[33] Delfino L, Longo A, Morabito A, Parodi A, Pera C, Pozzi S, et al. HLA class Isequence-based typing for high resolution matching in bone marrowtransplantation. J Biol Regul Homeost Agents 1999;13:42–6.
[34] Pera C, Delfino L, Longo A, Pistillo MP, Ferrara GB. Novel associations amongHLA-DQA1 and -DQB1 alleles, revealed by high-resolution sequence-basedtyping (SBT). Tissue Antigens 2000;55:275–9.
[35] Olerup O, Zetterquist H. HLA-DR typing by PCR amplification with sequence-specific primers (PCR-SSP) in 2 h: an alternative to serological DR typing inclinical practice including donor-recipient matching in cadaverictransplantation. Tissue Antigens 1992;39:225–35.
[36] Ronaghi M, Shokralla S, Gharizadeh B. Pyrosequencing for discovery andanalysis of DNA sequence variations. Pharmacogenomics 2007;8:1437–41.
[37] Banelli B, Merlo DF, Allemanni G, Forlani A, Romani M. Clinical potentials ofmethylator phenotype in stage 4 high-risk neuroblastoma: an open challenge.PLoS ONE 2013;8(5):e63253. http://dx.doi.org/10.1371/journal.pone.0063253.
[38] Cook MA, Norman PJ, Curran MD, Maxwell LD, Briggs DC, Middleton D,et al. A multi-laboratory characterization of the KIR genotypes of 10thInternational Histocompatibility Workshop cell lines. Hum Immunol2003;64:567–71.
700
Please cite this article in press as: Banelli B et al. A novel multiplex pyrosequePotential applications in autoimmunity and cancer. Hum Immunol (2014), htt
[39] Marsh SG, WHO Nomenclature Committee for Factors of the HLA System.Nomenclature for factors of the HLA system, update December 2010. TissueAntigens 2011;77:362–3.
[40] Gough SC, Simmonds MJ. The HLA region and autoimmune disease:associations and mechanisms of action. Curr Genomics 2007;8:453–65.
[41] Svahn J, Capasso M, Lanciotti M, Marrone A, Haupt R, Bacigalupo A, et al. Thepolymorphisms �318C>T in the promoter and 49A>G in exon 1 of CTLA4 andthe risk of aplastic anemia in a Cau population. Bone Marrow Transplant2005;35(Suppl. 1):S89–92.
[42] Brozzetti A, Marzotti S, Tortoioli C, Bini V, Giordano R, Dotta F, et al. Cytotoxic Tlymphocyte antigen-4 Ala17 polymorphism is a genetic marker ofautoimmune adrenal insufficiency: Italian association study and meta-analysis of European studies. Eur J Endocrinol 2010;162:361–9.
[43] Ramírez-Soriano A, Lao O, Soldevila M, Calafell F, Bertranpetit J, Comas D.Haplotype tagging efficiency in worldwide populations in CTLA4 gene. GenesImmun 2005;6:646–57.
[44] Grosso JF, Jure-Kunkel MN. CTLA-4 blockade in tumor models: an overview ofpreclinical and translational research. Cancer Immun 2013;13:5. Epub 2013Jan 22.
[45] Wang L, Li D, Fu Z, Li H, Jiang W, Li D. Association of CTLA-4 genepolymorphisms with sporadic breast cancer in Chinese Han population. BMCCancer 2007;7:173.
[46] Pincerati MR, Dalla-Costa R, Pavoni DP, Petzl-Erler ML. Genetic polymorphismsof the T-cell coreceptors CD28 and CTLA-4 in Afro- and Euro-Brazilians. Int JImmunogenet 2010;37:253–61.
[47] Idris ZM, Yazdanbakhsh M, Adegnika AA, Lell B, Issifou S, Noordin R. A pilotstudy on cytotoxic T lymphocyte-4 gene polymorphisms in urinaryschistosomiasis. Genet Test Mol Biomarkers 2012;16:488–92.
[48] Metaxas Y, Bertz H, Spyridonidis A, Spyroupoulou-Vlachou M, Porzelius C,Finke J. CT60 single-nucleotide polymorphism as a surrogate marker for donorlymphocyte infusion outcome after allogeneic cell transplantation for acuteleukemia. Bone Marrow Transplant 2012;47:411–5.
[49] Tsiatis AC, Norris-Kirby A, Rich RG, Hafez MJ, Gocke CD, Eshleman JR, et al.Comparison of Sanger sequencing, pyrosequencing, and melting curve analysisfor the detection of KRAS mutations: diagnostic and clinical implications. J MolDiagn 2010;12:425–32.
[50] Banelli B, Brigati C, Di Vinci A, Casciano I, Forlani A, Borzì L, et al. Apyrosequencing assay for the quantitative methylation analysis of the PCDHBgene cluster, the major factor in neuroblastoma methylator phenotype. LabInvest 2012;92:458–65.
[51] Rouits E, Boisdron-Celle M, Dumont A, Guérin O, Morel A, Gamelin E.Relevance of different UGT1A1 polymorphisms in irinotecan-inducedtoxicity: a molecular and clinical study of 75 patients. Clin Cancer Res2004;10:5151–9.
[52] Colomba E, Hélias-Rodzewicz Z, Von Deimling A, Marin C, Terrones N, PechaudD, et al. Detection of BRAF p. V600E mutations in melanomas: comparison offour methods argues for sequential use of immunohistochemistry andpyrosequencing. J Mol Diagn 2013;15:94–100.
[53] Weidlich S, Walsh K, Crowther D, Burczynski ME, Feuerstein G, Carey FA, et al.Pyrosequencing-based methods reveal marked inter-individual differences inoncogene mutation burden in human colorectal tumours. Br J Cancer2011;12(105):246–54.
ncing assay for genotyping functionally relevant CTLA-4 polymorphisms:p://dx.doi.org/10.1016/j.humimm.2014.04.019