Embed Size (px)
Citation preview

Journal of the American Podiatric Medical Association • Vol 97 • No 5 • September/October 2007 389Celebrating100years of continuous publication:1907–2007
Onychocryptosis is a pathologic condition of the nailapparatus in which the toenail damages the nail fold.It is a common condition that provokes pain, inflam-mation, and functional limitation. It principally af-fects the hallux, although it can also occur in thelesser toes. Onychocryptosis is more frequent in men(62%) than in women (38%). Although all age groupsare affected, most patients are adolescents in thefirst and second decades of life.1 The fibular canal ismore often affected than the tibial canal, in a propor-tion of 2:1.
The cause of the condition in childhood and adoles-cence is usually rounded trimming of the toenails, cut-ting with unsuitable instruments, or onychophagia.Other conditions conducive to the condition are hyper-hidrosis, wearing inappropriate footwear, direct trau-ma, biomechanical alterations, pathologic curvature ofthe nail plate, surgical iatrogenic conditions, excessiveweight, and the first toe being longer than the others.Congenital onychocryptosis is an infrequent form ofpresentation, believed to be due to intrauterine traumaor hereditary transmission.2 Heifitz3 divided onycho-cryptosis into three stages. Recently, Mozena4 refinedthis classification, establishing four stages:
• Stage I (inflammatory stage). This stage ischaracterized by the presence of erythema, slightedema, and pain when pressure is applied to the lat-eral nail fold. The nail fold does not exceed the limitsof the plate (Fig. 1).
• Stage II (abscess stage). This stage is dividedinto two substages. In stage IIa the pain increasesand there is edema, erythema, and hyperesthesia.There may be serum drainage and infection. The nailfold exceeds the nail plate and measures less than 3mm (Fig. 2). Stage IIb has symptoms similar to stageIIa. The hypertrophic fold exceeds the plate andmeasures more than 3 mm (Fig. 3).
• Stage III. In stage III, the symptoms worsen,with granulation tissue and chronic hypertrophy ofthe nail fold. The granulomatous or hypertrophic tis-sue largely covers the nail plate (Fig. 4). If onycho-cryptosis is not properly treated, it may progress evenfurther, resulting in serious chronic deformation ofthe toenail, nail folds, and distal fold.
We define a stage IV, which completes Mozena’sclassification. Stage IV results from evolution of stageIII, with serious chronic deformity of the toenail, bothnail folds, and the distal fold (Fig. 5). The differencebetween stages III and IV is the distal hypertrophy.
Indications for Nail Surgery
Nail surgery is indicated when the patient has painand functional disability; in cases of recurrent ony-chocryptosis, surgical relapse, or iatrogenic nail dis-
Onychocryptosis is a pathologic condition of the nail apparatus in which the toenail dam-ages the nail fold. It is a common condition provoking pain, inflammation, and functionallimitation. It principally occurs in the hallux. Onychocryptosis is one of the most frequentcomplaints regarding the foot and accounts for many clinical consultations. The disorderhas been classified in terms of the stages of the pathologic condition. In our practice, wediscovered a clinical entity that was not previously classified in the literature. We classifyonychocryptosis into stages I, IIa, IIb, III, and the new stage IV. A treatment plan is offeredfor each stage of this classification, with both general and specific indications given. Inonychocryptosis treatment, it is important to select the surgical technique best suited tothe patient’s particular clinical situation. (J Am Podiatr Med Assoc 97(5): 389-393, 2007)
*Podiatry, Department of Nursing, University of Extre-madura, Cáceres, Spain.
This article is a summary of the main part of Martínez-Nova A: Podología: Atlas de Cirugía Ungueal, EditorialMédica Panamericana, Madrid, 2006, and is adapted withpermission of the publisher.
Corresponding author: Alfonso Martínez-Nova, DPM,Centro Universitario de Plasencia, Avda. Virgen del Puertonº 2, 10600 Plasencia, Cáceres, Spain.
A New Onychocryptosis Classification and Treatment Plan
Alfonso Martínez-Nova, Lic Pod*Raquel Sánchez-Rodríguez, Lic Pod*
David Alonso-Peña, MD*
ORIGINAL ARTICLES

390 September/October 2007 • Vol 97 • No 5 • Journal of the American Podiatric Medical AssociationCelebrating100years of continuous publication:1907–2007
orders; and when conservative treatments have failed.The surgery should have several aims, with the over-all objective of restoring the integrity of the nail appa-ratus. The surgical procedure should correct the struc-
tural deformities of the nail, restore the longitudinaltrajectory of the nail plate, reestablish the morpholog-ical and normal physiologic features of the nail folds,prevent painful processes and infections, and con-serve the biomechanical function of the nail plate.The ultimate aim is to completely recover the func-tionality of the nail apparatus.4
Discussion
In the medical, dermatologic, and podiatric medicalliterature, various surgical techniques have been de-scribed to treat onychocryptosis. The ideal surgicalprocedure should result in a high level of patient satis-faction (both functional and aesthetic), a rapid returnto normal activities, and a low rate of recurrence. Al-though an attempt has been made to establish a “stan-dard technique” that will resolve onychocryptosis inmost cases, there is no scientific evidence that anysingle technique is the procedure of choice in all cases.
Figure 1. Stage I onychocryptosis. Figure 2. Stage IIa onychocryptosis.
Figure 3. Stage IIb onychocryptosis.
Figure 5. Stage IV onychocryptosis. (Reprinted withpermission from Martínez-Nova.1)
Figure 4. Stage III onychocryptosis.

Journal of the American Podiatric Medical Association • Vol 97 • No 5 • September/October 2007 391Celebrating100years of continuous publication:1907–2007
Despite this lack of scientific evidence for the su-periority of any one technique, many studies5-8 haveshown greater success with the phenol-alcohol tech-nique compared with other techniques. These studiesshow high rates of efficacy (80% to 95%) and low recur-rence rates (approximately 2% to 5%). On the negativeside is a 2- to 5-week recovery time,9 with the incon-venience that this represents for the patient. More-over, chemical matrixectomy may destroy too muchor too little tissue because it is not a precise tech-nique. Many other variables can influence the effec-tiveness of chemical matrixectomy, including tissuehydration; bleeding, which can cause dilution of theapplication; and the shelf life of the chemical used,which can affect its concentration. Nonetheless, thephenol-alcohol technique is clearly the most exten-sively studied and practiced technique. It is simple toperform, requires no complex instruments, has abroad range of indications, and is widely endorsed inthe dermatologic and podiatric medical literature.
The phenol-alcohol technique can be performed inthe presence of concomitant infection,10 and Giaca-lone11 demonstrated that it can be applied to diabeticpatients, for whom it presents no differences in heal-ing time or postsurgical complications. The use ofsodium hydroxide, less prevalent in the podiatricmedical community, has the same advantages as phe-nol, but with considerably less tissue destruction.12
Other studies, however, have found no significant dif-ferences between mechanical resection of the matrixand phenolization of the matrix.13 This last study rec-ommends resection of the matrix to avoid the use ofa toxic substance such as phenol. Persichetti et al14
affirm that simple excision of the matrix using me-chanical procedures (with a curet or scalpel) is mosteffective, leading to fewer complications and infec-tions and with a shorter healing time.
The use of physical methods to perform the ma-trixectomy, such as carbon dioxide laser dissectionor electrodissection, have also been discussed.15, 16 Al-though they are important and effective surgicalmethods, they are relatively expensive.
Most of the reports we found in the medical litera-ture were retrospective studies; only two were prospec-tive. They consisted of randomized controlled clinicaltrials comparing two techniques (phenol versus me-chanical resection of the matrix with curet or scalpel).One of these two studies suggests using the phenoltechnique,15 and the other recommends mechanicalresection of the nail matrix.13 The findings differ be-cause the aesthetic and functional results depend notonly on the technique used but also on the skill of theprofessional, the recovery protocol, the appropriateselection of the patient, and other factors. The podi-
atric medical community must undertake scientificstudies and controlled clinical trials to obtain demon-strable scientific parameters as part of evidence-based podiatric medical research.17 It is important tooffer a surgical solution for each stage of onycho-cryptosis, selecting the appropriate technique for thepatient’s particular clinical situation.
Treatment Algorithm According to theStage of Onychocryptosis
The surgical techniques used are classified into fourgroups according to the stage of onychocryptosis(Fig. 6).
Excision of the Spicule and Partial Matrixectomy: Suppan I Technique
General Indication. Onychocryptosis affecting thenail plate without hypertrophy of the nail fold. Thetechnique consists of excision of the affected portionof the toenail and partial mechanical matrixectomy(with curet or scalpel).18, 19
Indications According to Stage
• Stage I• Adult or elderly patients, in whom tissue-regen-
eration capacity is reduced and likelihood of recur-rence is lower.
• Patients with insulin-dependent diabetes. In pa-tients with some vascular risk or poor control of theirdiabetes, after previous stabilization of the vascularsituation and glycemia, this technique is preferred tophenol-alcohol to avoid complications caused by theburn.
Chemical Partial Matrixectomy:Phenol-Alcohol Technique
General Indication. Onychocryptosis affecting thenail plate with hypertrophy of the nail fold of lessthan 3 mm. In these cases, excision of the portion ofaffected toenail and phenol partial matrixectomy areperformed.20-22
Indications According to Stage
• Stage I• Stage IIa• Young or adolescent patients because they have
great tissue-regeneration capacity. The phenolizationensures a low recurrence rate.
• Patients with controlled type 1 or 2 diabetes. Thephenol-alcohol technique is safe in diabetic patientswho have no vascular risk and good control of theirdiabetes.

392 September/October 2007 • Vol 97 • No 5 • Journal of the American Podiatric Medical AssociationCelebrating100years of continuous publication:1907–2007
Wedge Resection of the Toenail and Nail Fold
Aesthetic Reconstruction Technique. General In-
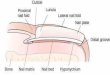
dication. Onychocryptosis affecting the nail platewith hypertrophy of the nail fold exceeding 3 mm.These cases involve excision of the affected portionof the nail plate, partial matrixectomy, and wedge ex-tirpation of the hypertrophic nail fold and the nailbed. The hypertrophic fold is cleared from the matrixzone, below the eponychium to the distal end of thetoenail (Fig. 7). No cutaneous incision is made, andtherefore no stitches are required.23, 24
Indication According to Stage
• Stage IIbWinograd Technique. General Indication. Ony-
chocryptosis affecting the nail plate with hypertrophyof the nail fold greater than 3 mm. These cases in-volve excision of the affected portion of the nailplate, partial matrixectomy, and extirpation of the hy-pertrophic tissue.25, 26
Indication According to Stage
• Stage III
Figure 6. Stage and treatment algorithm. DM indicates diabetes mellitus.
Onychocryptosis
Stage IIb
Increased pain,edema, erythema,hyperesthesia,serum drainage,and/or infection.
Nail fold exceedsthe nail plate > 3 mm.
Stage IIa
Increased pain,edema, erythema,hyperesthesia,serum drainage,and/or infection.
Nail fold exceedsthe nail plate < 3 mm.
Stage I
Erythema, slightedema, and pain.
Nail fold does notexceed the limits ofthe nail plate.
Stage III
Granulation tissueand chronic hyper-trophy of the nailfold.
Granulomatous orhypertrophic tissuewidely covers thelateral nail plate.
Stage IV
Serious chronicdeformity of the toe-nail, both nail folds,and distal fold.
Hypertrophic tissuecompletely coverslateral, medial, anddistal nail plate.
Adults
Suppan I
Type 1 DM
Suppan I
Youngpatients
Phenol
Young patients
Phenol
ControlledType 1 or 2 DM
Phenol
Aestheticreconstruction Winograd
Young patients with tibial/fibu-lar/distal hypertrophy
Winograd
Adults
Phenol totalmatrixectomy
Figure 7. Wedge resection of the lateral fold using theaesthetic reconstruction technique. (Reprinted withpermission from Martínez-Nova.1)

Journal of the American Podiatric Medical Association • Vol 97 • No 5 • September/October 2007 393Celebrating100years of continuous publication:1907–2007
Total Matrixectomy
General Indication. Onychocryptosis with dystro-phy of the nail folds and distal folds. Nail dystrophy.Nail excision and total matrixectomy with phenol isperformed.27-30
Indication According to Stage
• Onychocryptosis in stage IV adult patients• Onychogryphosis, onychodystrophy• Chronic hypertrophy of the distal and lateral foldsIn this stage of our classification (stage IV), the lat-
eral and distal folds are considerably hypertrophied,and the nail is affected. There are two treatment op-tions. The first option is three Winograd proceduresfor tibial/fibular/distal hypertrophy. This procedure isindicated in young patients to conserve the integrityand function of the nail apparatus. The second optionis phenol total matrixectomy, which must be per-formed in adult patients. If other disorders are pres-ent, such as onychomycosis or onychodystrophy,phenol total matrixectomy might be the better option.If the nail fold is widely affected, the Kaplan31 tech-nique should be considered.
Conclusion
Correct management of onychocryptosis requiresidentification of the stage and evaluation of the af-fected tissues. Nail surgery should be considered incases of pain, recurrent onychocryptosis, surgical re-lapse, and failure of conservative treatment. It is im-portant to select the surgical technique that is bestsuited to the patient’s particular clinical situation.
Financial Disclosures: None reported.Conflict of Interest: None reported.
References
1. MARTÍNEZ-NOVA A: Podología: Atlas de Cirugía Ungueal,
Editorial Médica Panamericana, Madrid, 2006.2. KREFT B, MARSCH WC, WOHLRAB J: Congenital and post-
partum ungues incarnati. Hautarzt 54: 1083, 2003.3. HEIFITZ CJ: Ingrown toenail: a clinical study. Am J Surg
38: 298, 1937.4. MOZENA JD: The Mozena Classification System and treat-
ment algorithm for ingrown hallux nails. JAPMA 92: 131,2002.
5. HEROLD N, HOUSHIAN S, RIEGELS-NIELSEN P: A prospectivecomparison of wedge matrix resection with nail matrixphenolization for the treatment of ingrown toenail. JFoot Ankle Surg 40: 390, 2001.
6. ESPENSEN EH, NIXON BP, ARMSTRONG DG: Chemical ma-trixectomy for ingrown toenails: is there an evidencebasis to guide therapy? JAPMA 92: 287, 2002.
7. ANDREASSI A, GRIMALDI L, D’ANIELLO C, ET AL: Segmental phe-nolization for the treatment of ingrowing toenails: a review
of 6 years experience. J Dermatol Treat 15: 179, 2004.8. ROUNDING C, HULM S: Surgical treatments for ingrowing
toenails. Cochrane Database Syst Rev 2: CD001541, 2000.9. BOSTANCI S, EKMEKCI P, GURGEY E: Chemical matricec-
tomy with phenol for the treatment of ingrowing toe-nail: a review of the literature and follow-up of 172treated patients. Acta Derm Venereol 81: 181, 2001.
10. KIMATA Y, UETAKE M, TSUKADA S, ET AL: Follow-up studyof patients treated for ingrown nails with the nail ma-trix phenolization method. Plast Reconstr Surg 95: 719,1995.
11. GIACALONE VF: Phenol matricectomy in patients with di-abetes. J Foot Ankle Surg 36: 264, 1997.
12. OZDEMIR E, BOSTANCI S, EKMEKCI P, ET AL: Chemical ma-tricectomy with 10% sodium hydroxide for the treat-ment of ingrowing toenails. Dermatol Surg 30: 26, 2004.
13. GERRITSMA-BLEEKER CL, KLAASE JM, GEELKERKEN RH, ET
AL: Partial matrix excision or segmental phenolizationfor ingrowing toenails. Arch Surg 137: 320, 2002.
14. PERSICHETTI P, SIMONE P, LI VECCHI G, ET AL: Wedge ex-cision of the nail fold in the treatment of ingrown toe-nail. Ann Plast Surg 52: 617, 2004.
15. YANG KC, LI YT: Treatment of recurrent ingrown greattoenail associated with granulation tissue by partial nailavulsion followed by matricectomy with sharpulse car-bon dioxide laser. Dermatol Surg 28: 419, 2002.
16. ZUBER TJ: Ingrown toenail removal. Am Fam Physician65: 2547, 2002.
17. PORTHOUSE J, TORGERSON DJ: The need for randomizedcontrolled trials in podiatric medical research. JAPMA94: 221, 2004.
18. SUPPAN RJ, RITCHLIN JD: A non-disabling surgical proce-dure for ingrown toenail. JAPA 52: 900, 1962.
19. KUWADA G: “Cirugía de los Dedos Menores,” in Atlas a
Color y Texto de Cirugía del Antepié, ed by R Butter-worth, G Dockery, Ortocen, Madrid, 1992.
20. KURU I, SUALP T, GUNDUZ T: Factors affecting recurrencerate of ingrown toenail treated with marginal toenailablation. Foot Ankle Int 25: 410, 2004.
21. BOBERG JS, FREDERIKSEN MS, HARTON FM: Scientific analy-sis of phenol nail surgery. JAPMA 92: 575, 2002.
22. MARTÍNEZ NOVA A, ALONSO PEÑA D, ALONSO PEÑA J, ET AL:Efecto de la irrigación con alcohol en la técnica quirúr-gica del fenol. Rev Esp Podol 15: 166, 2004.
23. GIRALT DE VECIANA E: Tratamiento de la onicocriptosismediante la técnica de reconstrucción estética. Rev EspPodol IV: 398, 1993.
24. PERSICHETTI P, SIMONE P, LI VECCHI G, ET AL: Wedge ex-cision of the nail fold in the treatment of ingrown toe-nail. Ann Plast Surg 52: 617, 2004.
25. WINOGRAD AMA: Modification in the technique of oper-ation for ingrown toe-nail. JAMA 92: 229, 1929.
26. DOCKERY GL: “Nails,” in Comprehensive Textbook of Foot
Surgery, 2nd Ed, Vol 1, ed by ED McGlamry, AS Banks,MS Downey, p 203, Williams & Wilkins, Baltimore, 1992.
27. DE BERKER DA, DAHL MG, COMAISH JS, ET AL: Nail surgery:an assessment of indications and outcome. Acta DermVenereol 76: 484, 1996.
28. MCINNES BD, DOCKERY GL: Surgical treatment of mycotictoenails. JAPMA 87: 557, 1997.
29. SUGDEN P, LEVY M, RAO GS: Onychocryptosis-phenol burnfiasco. Burns 27: 289, 2001.
30. BARAN R, HANEKE E: Matricectomy and nail ablation.Hand Clin 18: 693, 2002.
31. KAPLAN EG: Elimination of onychauxis by surgery. JAPA50: 110, 1960.