Embed Size (px)
Citation preview

A modified longitudinally split segmental rectusfemoris muscle flap transfer for facial reanimation:Anatomic basis and clinical applications
Daping Yanga,*, Steven F. Morrisb, Maolin Tangb, Christopher R. Geddesb
aDivision of Plastic Surgery, Department of Surgery, The 2nd Hospital of Harbin Medical University, HarbinHLJ 150086, ChinabDepartment of Anatomy and Neurobiology and Department of Surgery, Dalhousie University Halifax, NovaScotia, Canada
Received 25 April 2005; accepted 19 October 2005
S0do
KEYWORDSRectus femorismuscle;Facial reanimation;Surgical flap;Neurovascularanatomy
007-1226/$ - see front matter q 20i:10.1016/j.bjps.2005.10.015
* Corresponding author.E-mail address: dapingyang@hotma
Summary The present study was conducted to investigate the intra-muscularneurovascular anatomy and the intra-muscular tendon distribution of the rectusfemoris muscle to reassess the reliability of technique of harvesting a longitudinallysplit segmental muscle flap, and to present our clinical experience on usefulness ofthe longitudinally split segmental rectus femoris muscle flap as a method forreconstruction of the paralysed face in a series of 25 patients. Twenty fresh cadaverswere systemically injected with lead oxide, gelatin and water. Based on the anatomyof intra-muscular neurovascular structure in the rectus femoris muscle, 25consecutive patients with established facial paralysis were treated by using a two-stage method combining neurovascular free-muscle transfer with cross-face nervegrafting. Follow-ups were 15–24 months. All of the 25 patients showed significantlyimprovement in the appearance of the oral commissure and oral competence.Satisfactory results of facial reanimation were obtained in 23 patients. Among thesecases, near-natural facial expression was achieved. Recovery continued up to 2 yearspostoperatively. There were two cases having poor movement of transferred muscle2 years postoperatively. No complications occurred in the donor site. In conclusion,the present study has demonstrated the suitability for subdivision of the segmentmuscle flap of the rectus femoris into two functional units with a commonneurovascular pedicle. This series has further demonstrated the safety and reliabilityof using the rectus femoris muscle flap for facial reanimation.q 2006 Published by Elsevier Ltd on behalf of The British Association of PlasticSurgeons.
06 Published by Elsevier Ltd on
il.com (D. Yang).
Since, Harii et al. first reported free gracilis muscletransfer for facial reanimation,1 the technique ofthe free gracilis muscle transfer has been adopted
Journal of Plastic, Reconstructive & Aesthetic Surgery (2006) 59, 807–814
behalf of The British Association of Plastic Surgeons.

D. Yang et al.808
and refined by others to achieve both an aestheticand a functional reconstruction.2–7 The modifiedmethods included substantial debulking, thinning,and splitting of the muscle to achieve satisfactoryresults. However, these additional procedurescarried the risk of denervation and devascularisa-tion of the muscle flap. Hemostasis control withcautery tends to cause excessive muscle injury.Another problem with the gracilis muscle thatsurgeons faced was lack of an adequate and strongtendon for attachment to the recipient site duringthe muscle flap inset, so that many patientsrequired a subsequent procedure to shorten themuscle or adjust its insertion.7,8
To overcome these drawbacks, Taylor et al. hasproposed the coracobrachialis muscle as an idealdonor muscle because they considered certainfeatures of the muscle would allow it to improveon the overall result. These features include its longproximal tendon, the thick intermuscular septumalong its lateral surface, and the ligament ofStruthers.8
The rectus femoris muscle has been used for one-stage reconstruction of the established paralysedface.9,10 Our previous anatomical study of the rectusfemoris muscles has been conducted to assess thepotential of the rectus femoris as an alternativedonor muscle for facial reanimation.11 In the presentstudy, our attention was focused on the intra-muscular neurovascular anatomy and the intra-muscular tendon distribution to reassess thereliability of the technique of harvesting a long-itudinally split segmental muscle flap. Our clinicalexperience on usefulness of combining the long-itudinally split segmental rectus femoris muscle flaptransferwith cross-face nerve grafting as a two-stagemethod for reconstruction of the paralysed face in aseries of 25 patients is also presented in this paper.
Materials and methods
Part A. Anatomical study
The study was carried out on 20 fresh humancadavers (18 men, 2 women; mean age 74 years).The cadaver underwent arterial injection by meansof the carotid artery with a lead-oxide, gelatin, andwater mixture. Thereafter, the rectus femorismuscle was dissected. The muscle was radio-graphed. Radiographs revealed the intra-musculararterial pattern.
Further dissection was then carried out by long-itudinally splitting the muscle through the midline ofthe bipennate structure (landmark of intra-muscular
tendon) to harvest a segment of muscle flap with adominant neurovascular pedicle and the intra-muscular tendon from the mid-third of the muscle.The segment muscle flap was radiographed. Thesecond radiograph revealed the intra-muscular vas-cular branches of the segment muscle flap.
Finally, careful dissection was performed bysubdividing the segment muscle flap into twofunctional units through the neurovascular hilumof the medial border of the muscle, each with itsneurovascular supply. The superficial segmentconsists of the superficial branch of the dominantneurovascular pedicle and the intra-musculartendon; the other deep segment contains theposterior branch of the dominant neurovascularpedicle and the posterior aponeurosis (Fig. 1). Bothlongitudinally split segmental rectus femorismuscle flaps were radiographed again. All radio-graphs were then analysed.
Part B. Patients and surgical technique
Patient profilesBetween 1999 and 2004, 25 patients with estab-lished facial paralysis underwent surgical correc-tion using the rectus femoris muscletransplantation. Nine were male patients and 16were female patients. Patients ranged in age from15 to 54-year-old (mean 27-year-old). Facialparalysis was incomplete in four of the 25 patients,and the remaining patients had complete facialparalysis. The mean duration of facial paralysis was8 years (range 1.5–12 years). Causes of facialparalysis include complication of tumour surgery(such as acoustic neuroma or preauricular or infra-auricular tumour excision), unresolved Bell’s palsy,intra-cranial seventh nerve damage, trauma, orcongenital dysfunction. All patients received aclassic two-stage procedure: cross-face nervegrafting followed by the rectus femoris functioningmuscle flap transplantation. Photographs andvideotapes were obtained for all patients beforeand after surgery and every 6 months thereafter.Outcome was assessed by clinical examination andpatient questionnaire for facial appearance at restand during voluntary and involuntary movementsand muscle tone.
Surgical techniqueThe operative procedure is divided into two stages.The first stage consists in a classic cross-face nervegraft. A modified parotidectomy incision withsubmandibular extension is used to expose thebranches of the facial nerve on the nonparalysedside. Two of these branches is divided and joined to

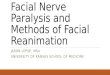
Figure 1 The anterior (A) and the posterior (B) view of the rectus femoris muscle show the intra-muscular tendon andthe aponeurosis are included with the superficial and deep sections of segment muscle flaps. (1) Rectus femoris muscle;(2) superficial section of segment muscle; (3) deep section of segment muscle flap; (4) dominant vascular pedicle; (5)neural branch; flap; (6) intra-muscular tendon; and (7) aponeurosis.
Segmental rectus femoris muscle flap transfer for facial reanimation 809
the nerve graft. Making sure that the buccal branchis one of these donor branches. Simultaneously, thesural nerve graft is harvested using multiple smalltransverse incisions. The sural nerve graft isanastomosed to the donor facial nerve branchesand is tunnelled through the upper lip to theparalysed side. The graft is anchored to the dermisby silk suture. Tinel’s sign is followed, and about8–12 months later the vascularized muscle istransferred and its neural branch is sutured to thedistal end of the cross-face nerve graft.
For the second stage, the two-team approach isused. One team prepares the facial nerve graft andrecipient vessels, and the other harvests andprepares the donor muscle on its neurovascularpedicle. The patients are placed in the supineposition. An s-shaped skin incision is made on theanterior thigh from the midpoint of the inguinalligament to the point of 15 cm proximal to thesuperior pole of the patellar. The femoral trianglearea is dissected to identify the branches of thefemoral nerve and the lateral circumflex femoralartery. The motor branch of the rectus femoris isidentified through careful dissection from thefemoral nerve trunk. Dissection proximally alongthe femoral nerve trunk increases the length of thenerve pedicle to 12–15 cm. The rectus femoris islongitudinally split through the midline of thebipennate structure for harvesting a segment ofmuscle flap with a dominant neurovascular pedicle(6–8 cm in length) and the intra-muscular tendonfrom the mid-portion of the muscle. The remainingpart of the muscle is then left in the thigh, havingits blood supply from the other minor vascular
pedicle. Careful dissection is performed by sub-dividing the segment muscle flap into twofunctional units through the neurovascular hilumof the medial border of the muscle. The superficialsegment flap consists of the superficial branch ofthe dominant neurovascular pedicle and the intra-muscular tendon; the other deep segment flapcontains the posterior branch of the inferiordominant neurovascular pedicle and posterioraponeurosis. Dimensions of the muscle flap are2–3 cm in width and approximately 8–10 cm inlength.
A preauricular incision is performed on theparalysed side to create a subcutaneous cheekpocket to accept subsequent neurovascular muscletransfer. The facial vessels and the cross-face nervegraft are identified and prepared for anastomosis.
The split segmental muscle flaps are thentransferred to the malar pocket of the paralysedface. The superficial segment flap is used toreconstruct paralysed face muscle. The proximalend of the intra-muscular tendon and muscle are,respectively, anchored to the periosteum of thezygomatic prominence and to the fascia deep to thesubmuscular aponeurotic system; its distal intra-muscular tendon is sutured to oral commissure andthe distal end of the muscle flap is then separatedinto two equal sections that are, respectively,anchored to the paralysed orbicularis oris musclein the upper and lower lip.
The deep segment flap is used to reconstruct theparalysed orbicularis oculi muscle and the nasola-bial fold. The proximal end of the deep segmentflap is sutured to the temporal muscle. The distal

D. Yang et al.810
aponeurosis is also divided into two strips. One stripis fixed to the inner canthal ligament through alower eyelid incision, and the other to the paralysednasolabial fold.
The transferred muscle is placed in enoughtension so that under anaesthesia it is tight enoughto place the paralysed oral commissure in balancewith 1 cm higher than the normal side. The commonvascular pedicle of two muscle grafts is anasto-mosed to the facial vessels. Its neural branch issutured to the distal end of the cross-face nervegraft.
Results
Part A. Anatomical study
Intra-muscular neurovascular supplyThree different vascular patterns in 40 muscleswere observed based on Mathes’ classification.
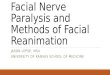
Figure 2 Arteriogram showing that the rectus femoris muspedicle (A). A segment of muscle flap is separated from the mtwo functional units through the neurovascular hilum (C).
The most of the rectus femoris muscles (80%)were classified as type II, with a dominant vascularpedicle and a minor pedicle from the differentbranches of the lateral circumflex femoral artery. Aminor pedicle arose from an ascending branch orthe transverse branch, which entered the deepsurface of the rectus femoris and supplied theproximal muscle. The dominant vascular pediclearose from the descending branch and entered themuscle at the junction of the upper and middlethirds. Within the muscle, it divided into two mainbranches that ran straight down to supply the distaltwo-thirds of the muscle. The superficial branch ofthe dominant vascular pedicle ran superficiallyalong the medial border of the rectus femoris,and the other posterior branch coursed behind theintra-muscular tendon. There were few anasto-moses between the dominant artery and the minorartery (Fig. 2).
Twelve percent rectus femoris muscles wereclassified as type I, having a single vascular pedicle,without regard to some tiny branches supplying the
cle receives a dominant vascular pedicle and one minoruscle (B). The segment of muscle flap is subdivided into

Segmental rectus femoris muscle flap transfer for facial reanimation 811
tendons of origin and insertion. This vascularpedicle was derived from the descending branchof the lateral circumflex femoral artery. Beforeentering the muscle, the vascular pedicle generallydivided into a superior minor branch and an inferiordominant branch.
Eight percent muscles received two dominantvascular pedicles from two different branches ofthe lateral circumflex femoral artery as type III. Thesuperior dominant arterial pedicle arose from theascending branch or the transverse branch of thelateral circumflex femoral artery, and the inferiordominant pedicle stemmed from the descendingbranches of the lateral circumflex femoral artery.
In general, the intra-muscular vascular pattern intype I or type III was similar to that in type II. Thethree different vascular patterns were presentedonly based on the number of vascular pedicles,whether or not arising from different branches ofthe lateral circumflex femoral artery, and theirrelative dominance within the muscle.
The rectus femoris was innervated by a branchfrom the posterior division of the femoral nerve.The neural branch divided into two branches beforeit reached the muscle. These branches were,respectively, accompanied by arterial branches toform two neurovascular hila. The superior branchentered the muscle on its proximal posteriorsurface with the superior vascular pedicle. Theinferior branch entered the medial border of themuscle with the inferior dominant vascular pedicle,and split into two branches, respectively, accom-panying the superficial branch and the posteriorbranch of the dominant vascular pedicle before orafter entering the muscle. The intra-muscularneural pattern, like the vascular pattern, isoriented longitudinally. Once the nerve separatedinto two individual fascicles within the muscle, theyrun parallel to the muscle fibers and vascularbranches.
Intra-muscular structure related to segmentmuscle flap harvestingThe rectus femoris is a fusiform muscle with itssuperficial fibers arranged in a bipennate pattern,and its deep fibers run parallel to the long axis ofthe muscle. Its straight tendinous head is attachedto the anterior inferior iliac spine and formed thesuperficial tendon on the muscle’s anterior aspectof the proximal third. The intra-muscular tendonarose from the tendon of the reflected head. Distalto the superficial tendon, the bipennate structurewas formed by the muscle fibers arising from theintra-muscular tendon. From the cross-sectionview, the intra-muscular tendon lay in the anteriorportion of the middle muscle belly, and travelled
through the majority of the muscle length. Itsanatomic landmark was the midline of the bipen-nate structure. A broad aponeurosis was seen on theposterior aspect of the muscle’s distal two-thirds.
Taken together, these findings could providesome potential insights regarding the segmentalrectus femoris muscle transfer as follows.
1. The lengths of the intra-muscular tendon of therectus femoris and the aponeurosis along itsposterior surface enable them to be includedwith any segment of muscle located along themedial surface of the muscle (Fig. 1).
2. The longitudinally oriented pattern of neurovas-cular supply of the muscle makes it an idealchoice for longitudinal subdivision (Fig. 2).
3. The superficial and deep sections of the musclecan be easily identified at the dominant neuro-vascular hilum, as its superficial fibers arrange ina bipennate pattern and its deep fibers runparallel to the long axis of the muscle.Dissection through the neurovascular hilum cansubdivide a segmental muscle flap into twofunctional units, each with its neurovascularsupply.
Part B. Clinical study
All of the 25 patients underwent transfer of themuscle without any complications. No musclenecrosis was observed. All of the 25 patientsshowed significantly improvement in the appear-ance of the oral commissure and oral competence.Satisfactory results of facial reanimation wereobtained in 23 patients, evaluated at 15 months to2 years after second operation. Among these cases,near-natural facial expression was achieved.Recovery continued up to 2 years postoperatively.There were two cases out of 25 cases only withstatic symmetry of the lips and without the move-ment of transferred muscle 2 years postoperatively.
Case reports
Case 1
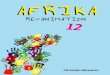
A 24-year-old man presented with left completefacial paralysis resulting from intra-cranial damage2 years previously. The rectus femoris muscle wastransplanted for facial reanimation combined withcross-face nerve grafting which was joined to twocontralateral buccal branches. Seven months afterthe surgery, the patient felt a weak contraction ofthe transferred muscle, and 2 years after surgery,

Figure 3 A 24-year-old man presented with left facial paralysis resulting from intra-cranial damage 2 years previously.Seven months after the surgery, the patient felt a weak contraction of the transferred muscle, and 2 years after surgery,the muscle contracted with considerable power. Smiling before treatment (A); 2 years after muscle flap transfer at rest(B), and 2 years after muscle flap transfer with muscle contraction (C).
D. Yang et al.812
the muscle contracted with considerable power(Fig. 3).
Case 2
A 31-year-old woman presented with a left com-plete facial paralysis of 4 years’ duration thatresulted from resection of a recurrent intra-cranialcholesteatoma. Two-stage method combining neu-rovascular free-muscle transfer with cross-facenerve grafting was performed. A strip fromaponeurosis of rectus femoris muscle was used tosuspend the left lower eyelid, because the lefttemporal muscle had already been used to fill in adead space when the cholesteatoma was removed.Muscle contraction was not observed 2 years afterneurovascular free muscle transfer. Only staticsymmetry of the face was shown (Fig. 4).
Case 3
A 23-year-old man with left complete facialparalysis 2 years after a left acoustic neuromapreviously removed was treated by cross-face nervegrafting and split segmental rectus femoris muscletransfer. The patient felt voluntary movement ofthe transferred muscle 8 months after the surgery,and the muscle obtained considerable contraction 2years after the operation. A distal aponeurosis stripwas used to suspend the left lower eyelid (Fig. 5).
Discussion
Although reanimation of the paralysed face is one ofthe challenges for the reconstructive surgeon, aconsiderable progress has been made over the lasttwo decades. Neurovascular free muscle transfer is
now a standard procedure for the dynamic smilereconstruction of longstanding facial paralysis.Surgeons have obtained a good result in thetreatment of facial paralysis with cross-facialnerve grafts in combination with free vascularisedmuscle flaps in recent years. Surgeons havefavoured the gracilis muscle for its reliable vascularsupply, the ease being harvested, and its expend-ability. In addition to the gracilis, the extensordigitorum brevis,12,13 serratus anterior,14 latissimusdorsi,15,16 rectus abdominis,17 and pectoralisminor18,19 muscles have been used in attempts torestore spontaneous symmetrical movements to theface to achieve both an aesthetic and a functionalreconstruction. However, inadequate cosmeticresult is problematic because many patients requiresubsequent procedures to debulk the muscle,shorten it, or adjust its insertion.8 An ideal splittingsegment muscle flap, therefore, should have notonly a consistent neurovascular pedicle, but alsoinclude an adequate and strong tendon for attach-ment to the recipient site.
Transfer of the rectus femoris has been per-formed to improve facial smile function in patientswith unilateral established facial paralysis in one-stage.9,10 We preferred cross-face nerve graftfollowed by free-muscle transplantation as a two-stage procedure, because of the better resultsachieved with more synchronous, natural, andsymmetric facial movement. We modified Koshi-ma’s method to a longitudinally split segmentalrectus femoris muscle flap transfer with an intra-muscular tendon. The rectus femoris as an alterna-tive donor muscle has the common advantages thesame as the gracilis, including a reliable neurovas-cular supply, minimal donor-site morbidity, and theoption of having two teams operate simultaneously.In addition, it has a few unique features, such as the

Figure 4 A 31-year-old woman presented with a left complete facial paralysis of 4 years’ duration that resulted fromresection of a recurrent intra-cranial cholesteatoma. Muscle contraction was not observed 2 years after neurovascularfree muscle transfer. Only static symmetry of the face was shown. Before treatment (left) and after treatment (right).
Segmental rectus femoris muscle flap transfer for facial reanimation 813
intra-muscular tendon and broad aponeurosis,which can be included with the split segment ofmuscle harvested for facial reanimation to facili-tate attachment of the muscle in the face toimprove the facial asymmetry.
Figure 5 A 23-year-old man with left complete facial paremoved was treated by cross-face nerve grafting and split soperation (A). Two years after muscle transfer (B).
The intra-muscular tendon was found in ourexperience to be helpful not only for anchoring themuscle flap to the fascia and periosteum, but alsofor splitting and thinning the segmental muscleflap. Careful dissection through the intra-muscular
ralysis 2 years after a left acoustic neuroma previouslyegmental rectus femoris muscle transfer. Smiling before

D. Yang et al.814
tendon can reduce the likelihood of tissue injuryand ensures that the segment of muscle harvestedcan be safely performed in an expeditious andreliable manner.
Because the rectus femoris is relatively thickcompared with the facial muscles, a splittingsegment muscle flap is required for facial reanima-tion. The lengths of the intra-muscular tendon ofthe rectus femoris and the aponeurosis along itsposterior surface enable them to be included withany segment of muscle located along the medialsurface of the muscle used for facial reanimation.The intra-muscular tendon is of significancebecause it can be used as a fascial sling for staticsupport in the face when it is harvested with themuscle. On the other hand, the technique ofharvesting a segmental muscle flap using theintra-muscular tendon as a landmark can minimisethe chances of intra-muscular nerve and vesseldamage, since there are no vascular anastomosesbetween the bipennate muscles. However, the riskof vessel damage exists during splitting thesuperficial and deep segment flaps. The success ofthis procedure depends on precise knowledge of theintra-muscular neurovascular anatomy. Care shouldbe taken when dissecting through the neurovascularhilum, where two sections of the muscle can beeasily identified, as its superficial fibers arrange in abipennate pattern and its deep fibers run parallel tothe long axis of the muscle.
Furthermore, this present study has demon-strated that the rectus femoris muscles have poorlydeveloped vascular anastomoses between thevascular territories. The phenomenon could beexplained on the basis of our intra-musculardissection. We have found that the intra-musculartendon influence vascular connections between thevascular territories within the muscle, which mightbe beneficial to reduce vessel damage during intra-muscular dissection.
In conclusion, the present anatomical study hasdemonstrated the availability of two neurovascularhila in the rectus femoris muscle and its suitabilityfor subdivision of the segment muscle flap into twofunctional units with a common neurovascularpedicle for functioning muscle transfer. Moreover,this series has further demonstrated the safety andreliability of using the rectus femoris muscle flapfor facial reanimation.
References
1. Harii K, Ohmori K, Torii S. Free gracilis muscle transplan-tation, with microneurovascular anastomoses for the treat-ment of facial paralysis. Plast Reconstr Surg 1976;57:133–43.
2. O’Brien BM, Franklin JD, Morrison WA. Cross-facial nervegrafts and microneurovascular free muscle transfer for longestablished facial palsy. Br J Plast Surg 1980;33:202–15.
3. Sassoon EM, Poole MD, Rushworth G. Reanimation for facialpalsy using gracilis muscle grafts. Br J Plast Surg 1991;44:195–200.
4. Manktelow RT, Zuker RM. Muscle transplantation by fasci-cular territory. Plast Reconstr Surg 1984;73:751–7.
5. Giordano PA, Abbes M, Pequignot JP. Gracilis blood supply:anatomical and clinical re-evaluation. Br J Plast Surg 1990;43:266–72.
6. Morris SF, Yang D. Gracilis muscle: arterial and neural basisfor subdivision. Ann Plast Surg 1999;42:630–3.
7. Turowski GA, Koshima I, Upton J. Muscle stapling techniquefor free muscle transfer to the face. Plast Reconstr Surg1998;102:1639–41.
8. Taylor GI, Cichowitz A, Ang SG, et al. Comparativeanatomical study of the gracilis and coracobrachialismuscles: implications for facial reanimation. Plast ReconstrSurg 2003;112:20–30.
9. Koshima I, Moriguchi T, Soeda S, et al. Free rectus femorismuscle transfer for one-stage reconstruction of establishedfacial paralysis. Plast Reconstr Surg 1994;94:421–30.
10. Koshima I, Umeda N, Handa T, et al. A double-muscletransfer using a divided rectus femoris muscle for facial-paralysis reconstruction. J Reconstr Microsurg 1997;13:157–62.
11. Yang D, Morris SF. Neurovascular anatomy of the rectusfemoris muscle related to functioning muscle transfer. PlastReconstr Surg 1999;104:102–6.
12. O’Brien BM, Franklin JD, Morrison WA. Cross-facial nervegrafts and microneurovascular free muscle transfer for longestablished facial palsy. Br J Plast Surg 1980;33:202–15.
13. O’Brien BM, Pederson WC, Khazanchi RK, et al. Results ofmanagement of facial palsy with microvascular free-muscletransfer. Plast Reconstr Surg 1990;86:12–22.
14. Whitney TM, Buncke HJ, Alpert BS, et al. The serratusanterior free-muscle flap: experience with 100 consecutivecases. Plast Reconstr Surg 1990;86:481–90.
15. Dellon AL, Mackinnon SE. Segmentally innervated latissimusdorsi muscle: microsurgical transfer for facial reanimation.J Reconstr Microsurg 1985;2:7–12.
16. Mackinnon SE, Dellon AL. Technical considerations of thelatissimus dorsi muscle flap: a segmentally innervatedmuscle transfer for facial reanimation. Microsurgery 1988;9:36–45.
17. Hata Y, Yano K, Matsuka K, et al. Treatment of chronic facialpalsy by transplantation of the neurovascularized free rectusabdominis muscle. Plast Reconstr Surg 1990;86:1178–87.
18. Harrison DH. The pectoralis minor vascularized muscle graftfor the treatment of unilateral facial palsy. Plast ReconstrSurg 1985;75:206–16.
19. Terzis JK. Pectoralis minor: a unique muscle for correctionof facial palsy. Plast Reconstr Surg 1989;83:767–76.