Embed Size (px)
Citation preview

Dear Sir,
Allergic granulomatous angiitis (Churg-Strauss syn-drome, CSS) is characterized by the triad of asthma,eosinophilia, and systemic vasculitis [1]. In addition tothese classical findings, pulmonary infiltrates, skin le-sions, eye, gastrointestinal, and lymph node involvementhas been reported [5]. There are rare cases of limitedform of CSS with no clinical evidence of asthma [6].The patient presented here had no history of asthma orpulmonary symptoms. The patient’s disease was limitedto gastrointestinal system and the lymph nodes drainingthe involved bowel segment.
The patient had an elevated white blood cell count(16,800/ml) with normal red cell indices. On peripheralsmear eosinophils were significantly elevated (38%). Se-rological tests for hepatitis B virus and human immuno-deficiency virus were negative, as were those for anti-nuclear antibodies, anti-neutrophil cytoplasmic antibod-ies (ANCA), and rheumatic factor. Urinalysis showed noproteinuria or hematuria. Renal and liver function testswere within normal limits. IgE levels were normal. Thepatient’s neurological examination and electromyographicfindings were normal. Chest computed tomography re-vealed multiple pulmonary nodules on both lungs. Aller-gy tests were performed and no allergic response wasobserved on screening tests.
The patient was a 19-year-old man who had experi-ence nausea, diarrhea, and fatigue for 1–2 weeks. Thepatient presented to the emergency room with abdomi-
nal colic. Following initial work-up the clinical suspi-cion of acute appendicitis was established. Emergencylaparotomy was performed. On gross inspection the ap-pendix was found to be normal. However, multiplehemorrhagic serosal and mesenteric nodules and necrot-ic appearing ileum, cecum, and transverse colon wereobserved. A right hemicolectomy including the ileoce-cal region was performed followed by an ileotransver-sostomy.
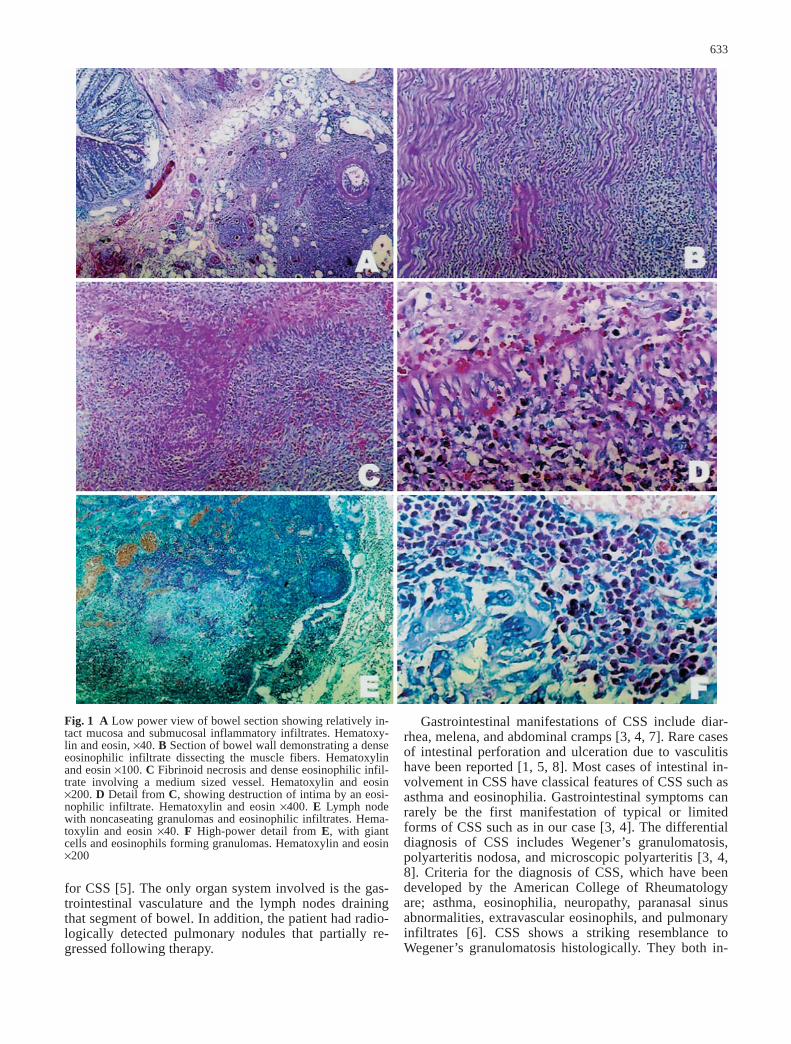
On gross inspection the bowel serosa appeared hem-orrhagic and focally necrotic. On sectioning the bowelmucosa appeared pale but not ulcerated. The serosalnodules were hemorrhagic. No tumor was identified. Theappendix appeared normal. On microscopic evaluation anecrotizing eosinophilic vasculitis involving small andmedium-sized arteries was seen (Fig. 1C, D). The bowelmucosa showed ischemic changes but no crypt abscesseswere observed (Fig. 1A). In addition, there was a denseeosinophilic infiltrate throughout the bowel wall and thelymph node capsules, sparing the mucosa (Fig. 1B). Theregional lymph nodes showed partial involvement withthe vasculitic process. The lymph node sinuses werefilled with eosinophils. Eosinophilic infiltrates extendedto pericapsular areas. The lymph node cortexes retainedthe follicular architecture but focal areas contained eosi-nophilic and necrotizing granulomas (Fig. 1E, F). Eosi-nophilic vasculitis of the lymph node arterioles was alsoevident. Based on these pathological and laboratory find-ings, the diagnosis of limited form of CSS was estab-lished.
The patient responded well to steroids and cyclophos-phamide and is on remission with no evidence of any or-gan involvement. Following therapy the patient’s periph-eral eosinophilia was reversed and the pulmonary nod-ules detected by chest computed tomography decreasedin diameter.
The case presented here lacks some of the classicalfeatures of CSS such as asthma and p-ANCA positivity.However, presence of eosinophilia in the peripheralblood, eosinophilic infiltrates in the tissues, and eosino-philic vasculitis and necrotizing granulomas are specific
F. Kacar (✉) · E. Levi · E. Dikicioglu · I. Meteoglu · M. UyarDepartment of Pathology, Adnan Menderes University Medical School, Aydin 09100 Turkeye-mail: [email protected].: +90-256-2124078Fax: +90-256-2120146
H. ErpekDepartment of Pathology, Adnan Menderes University Medical School, Aydin 09100 Turkey
Virchows Arch (2002) 441:632–634DOI 10.1007/s00428-002-0688-8
L E T T E R T O T H E E D I T O R
Füruzan Kacar · Edi Levi · Emel DikiciogluIbrahim Meteoglu · Hakan Erpek · Meral Uyar
A limited form of Churg-Strauss syndrome presenting as acute abdominal catastrophe
Received: 13 December 2001 / Accepted: 18 June 2002 / Published online: 12 July 2002© Springer-Verlag 2002
633
Fig. 1 A Low power view of bowel section showing relatively in-tact mucosa and submucosal inflammatory infiltrates. Hematoxy-lin and eosin, ×40. B Section of bowel wall demonstrating a denseeosinophilic infiltrate dissecting the muscle fibers. Hematoxylinand eosin ×100. C Fibrinoid necrosis and dense eosinophilic infil-trate involving a medium sized vessel. Hematoxylin and eosin×200. D Detail from C, showing destruction of intima by an eosi-nophilic infiltrate. Hematoxylin and eosin ×400. E Lymph nodewith noncaseating granulomas and eosinophilic infiltrates. Hema-toxylin and eosin ×40. F High-power detail from E, with giantcells and eosinophils forming granulomas. Hematoxylin and eosin×200
for CSS [5]. The only organ system involved is the gas-trointestinal vasculature and the lymph nodes drainingthat segment of bowel. In addition, the patient had radio-logically detected pulmonary nodules that partially re-gressed following therapy.
Gastrointestinal manifestations of CSS include diar-rhea, melena, and abdominal cramps [3, 4, 7]. Rare casesof intestinal perforation and ulceration due to vasculitishave been reported [1, 5, 8]. Most cases of intestinal in-volvement in CSS have classical features of CSS such asasthma and eosinophilia. Gastrointestinal symptoms canrarely be the first manifestation of typical or limitedforms of CSS such as in our case [3, 4]. The differentialdiagnosis of CSS includes Wegener’s granulomatosis,polyarteritis nodosa, and microscopic polyarteritis [3, 4,8]. Criteria for the diagnosis of CSS, which have beendeveloped by the American College of Rheumatologyare; asthma, eosinophilia, neuropathy, paranasal sinusabnormalities, extravascular eosinophils, and pulmonaryinfiltrates [6]. CSS shows a striking resemblance toWegener’s granulomatosis histologically. They both in-

diagnose. However, when the classical manifestations ofCSS such as asthma are lacking, and the patient presentswith gastrointestinal symptoms, the vasculitic syndromesincluding limited forms of CSS should also be includedin the differential diagnosis.
References
1. Churg J, Strauss L (1951) Allergic granulomatosis, allergic an-giitis and periarteritis nodosa. Am J Pathol 27:277–294
2. Cualing H, Schroder L, Perme C (2001) Allergic granulomato-sis secondary to a limited form of Churg-Strauss syndrome.Arch Pathol Lab Med 125:954–957
3. Kaneki T, Kawashima A, Hayano T, Honda T, Kubo K,Koizumi T, Sekiguchi M, Ichikawa H, Matsuzawa K, Katsuyama T (1998) Churg-Strauss syndrome (allergic granulo-matous angiitis) presenting with ileus caused by ischemic ilealulcer. J Gastroenterol 33:112–116
4. Lin TL, Wang CR, Liu MF, et al (2001) Multiple colonic ulcerscaused by Churg-Strauss syndrome in a 15-year-old girl. ClinRheumatol 20:362–364
5. Masi AT, Hunder GG, Lie JT (1990) The American College ofRheumatology 1990 criteria for the classification of Churg-Strauss syndrome. Arthritis Rheum 33:1094–1099
6. Ohwada S, Yanagisawa A, Joshita T, et al (1997) Necrotizinggranulomatous vasculitis of transverse colon and gallbladder.Hepatogastroenterology 44:1090–1094
7. Shimamato C, Hirata I, Ohshiba S, Fujiwara S, Nishio M(1990) Churg-Strauss syndrome [allergic granulomatous angii-tis] with peculiar multiple colonic ulcers. Am J Gastroenterol85:316–319
8. Solans R, Bosch JA, Perez-Bocanegra C, et al (2001) Churg-Strauss syndrome: outcome and long-term follow-up of 32 pa-tients. Rheumatology (Oxf) 40:763–771
9. Suen KC, Burton JD (1979) The spectrum of eosinophilic infil-tration of the gastrointestinal tract and its relationship to otherdisorders of angiitis and granulomatosis. Hum Pathol 10:31–43
634
volve the lungs presenting with necrotizing granulomas[2]. CSS is characterized by prominent eosinophilic in-filtrates and peripheral eosinophilia. Wegener’s granulo-matosis is characterized by c-ANCA (anti-proteinase III)as opposed to p-ANCA (anti-myeloperoxidase) com-monly found in CSS [5]. The absence of ANCA isagainst a diagnosis of Wegener’s granulomatosis. Theabsence of ANCA and the presence of eosinophilia isagainst a diagnosis of microscopic or macroscopic PAN[5]. The examination of the bowel did not reveal any in-flammatory lesions of the mucosa, and therefore a diag-nosis of inflammatory bowel disease was unlikely. Ex-amination of the feces and the tissues by special stainsdid not reveal any micro-organisms or parasites, there-fore an infectious cause was also eliminated. The pres-ence of vasculitis spreading to the lymph nodes excludesa diagnosis of eosinophilic gastroenteritis [9].
The cause of CSS is not known, however, ANCA(anti-myeloperoxidase) have been detected in approxi-mately 75% of the cases, and they are thought to play arole in the pathogenesis of this syndrome [8]. Associa-tion with asthma suggests the presence of an allergenicstimulus. The histopathological features of involvementof lymph nodes in CSS have been rarely reported [2]. Inour case the presence of dense eosinophilic infiltrates inthe lymph node sinuses and capsule and the presence ofnecrotizing epithelioid granulomas cuffed by dense eosi-nophilic infiltrates was striking.
We believe that this case is unique because most casesof CSS vasculitis with gastrointestinal involvement re-ported in the literature have a history of asthma and pe-ripheral eosinophilia [3, 4, 7]. These cases which presentwith the classical manifestations of disease are easier to