Embed Size (px)
Citation preview

This CME activity is provided by Integrity Continuing Education.This CEU/CNE activity is co-provided by Postgraduate Institute for Medicine and Integrity Continuing Education.
A Hospital-based Approach to Achieving Better Health Outcomes in Heart Failure

FacultyLee Goldberg, MD, MPH
Medical DirectorHeart Failure and Cardiac Transplant Program
Associate Professor of MedicineCardiovascular Medicine Division
University of PennsylvaniaPhiladelphia, Pennsylvania

Consultant: Respircardia
Faculty Disclosures

Utilize an evidence-based approach to the diagnosis and evaluation of patients with heart failure (HF) that is consistent with current guideline recommendations
Summarize current clinical evidence regarding the efficacy and safety of new pharmacologic therapies for the treatment of heart failure with reduced ejection fraction (HFrEF)
Implement guideline-directed medical therapy for patients with HF
Identify transitional care strategies to prevent disease progression and future hospitalizations among patients with HF
Learning Objectives

Heart Failure in the Hospital Setting

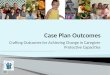
Trends in Primary HF Admissions and In-hospital Mortality (2001-2014)
Akintoye, et al. J Am Heart Assoc. 2017;6:e006955.
Rat
e of
Adm
issi
on (p
er 1
00,0
00 p
erso
ns)
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
600
550
500
450
400
350
% In
-hos
pita
l Mor
talit
y
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
5
4.5
4
3.5
3
2.5
2
1.5
Δ in trend in 2005 = -2.4 (95% CI: -4.4, -0.39); P=0.02
Δ in trend in 2009 = -1.0 (95% CI: -2.3, 0.30); P=0.14
Δ in trend in 2005 = 0.41 (95% CI: -1.3, 2.1); P=0.64
Δ in trend in 2009 = 3.2 (95% CI: 1.9, 5.4); P=0.002

Medicare Readmission Rates Among Patients Hospitalized for HF
Available at: http://kff.org/medicare/issue-brief/aiming-for-fewer-hospital-u-turns-the-medicare-hospital-readmission-reduction-program/
Despite recent decreases, a significant percentage (22%) of patients hospitalized with HF are readmitted within 30 days.
24.5 24.7 24.8 24.7
23.0 22.722.019.9 19.9 19.8 19.7
18.3 17.817.0
18.2 18.3 18.4 18.517.6 17.3 16.9
151617181920212223242526
July 2005-June 2008
July 2006-June 2009
July 2007-June 2010
July 2008-June 2011
July 2009-June 2012
July 2010-June 2013
July 2011-June 2014
Nat
iona
l Ave
rage
R
eadm
issi
on R
ate
(%)
Performance (Measurement) Time Period
Heart FailureHeart AttackPneumonia
Diagnosis for Initial Hospitalization

30-Day Risk Standardized HF Mortality Rates Under HRRP
RSMR, risk standardized mortality rate; RSRR, risk standardized readmission rate; CMS, Centers for Medicare and Medicaid Services.Abdul-Aziz AA, et al, J Cardiac Fail. 2017;23:S5-S6.
While 30-day readmission rates have improved for HF, 30-day HF mortality rates have increased at more than half of US hospitals since the advent of Centers for CMS readmission penalties.
0.5
0.0
-0.5
-1.0
Cha
nge
in R
SMR
2016
vs
2013
(%)
Change in RSRR 2016 vs 2013 (%)
CHF
AMI
Decreased >-1.0
-1.0 to 1.0 Increased >1.0

Opportunities to Improve Patient Outcomes: Principles for Successful HF Treatment
GDMT, guideline-directed medical therapy.Adapted from: Yancey, et al. J Am Coll Cardiol. 2018;71(2):201-230.
Implement GDMT
I. Initiate and switch treatment as appropriate
II. Titration to optimal dose
Address Specific Care Challenges
I. ReferralII. Care coordinationIII. AdherenceIV. Specific patient
cohortsV. Cost of care
Manage Other Aspects of HF
I. Increasing complexity of disease
II. ComorbiditiesIII. Palliative/hospice
care

Patient Evaluation

A careful history and physical examination remain the cornerstones of assessment
Assessment for HF
ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.
Patient history
Physical examination
Diagnostic laboratory
testing
Cardiac imaging
Invasive evaluation

Risk factors– Family history– Other conditions (eg, HTN, CAD/MI,
thyroid disease, & diabetes)
Duration of illness Symptoms
– Type– Severity
Recent/frequent prior hospitalizations for HF
Diet– Sodium intake
Medication– Discontinuation or nonadherence – Agents that may exacerbate HF
De novo HF indicators– Inadequate BP control– New-onset or poorly controlled AF– New ischemia– Metabolic, respiratory, & other stressors
Patient History
HTN, hypertension; CAD, coronary artery disease; MI, myocardial infarction; BP, blood pressure; AF, atrial fibrillation.ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.

Shortness of breath Chronic coughing/
wheezing Edema Fatigue/lightheadedness Nausea/lack of appetite
Confusion/impaired thinking
Elevated HR
Symptoms of HF
HR, heart rate.
Available at: http://www.heart.org/HEARTORG/Conditions/HeartFailure/WarningSignsforHeartFailure/Warning-Signs-of-Heart-Failure_UCM_002045_Article.jsp#.V7YfgFsrL4Z.

Physical Examination Weight loss or gain BP (supine and upright) Pulse JVP at rest (sitting or standing)
and/or positive Kussmaul’s sign
Presence of extra heart sounds and murmurs
Size and location of PMI Presence of RV heave Pulmonary status: RR and
pleural effusion Hepatomegaly and/or ascites Peripheral edema Presence of cool lower
extremities
JVP, jugular venous pressure; PMI, point of maximal impulse; RV, right ventricular; RR, respiratory rate.ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.

Recommendations for the Use of Biomarkers in the Evaluation of Patients with HF
Biomarker, Application Setting COR LOENatriuretic peptides
Diagnosis or exclusion of HF Ambulatory, Acute I A
Prognosis of HF Ambulatory, Acute I A
Achieve GDMT Ambulatory IIa B
Guidance for ADHF therapy Acute IIb C
Biomarkers of myocardial injuryAdditive risk stratification Acute, Ambulatory I A
Biomarkers of myocardial fibrosisAdditive risk stratification Ambulatory IIb B
Acute IIb A
ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.

Association Between Discharge BNP and Clinical Outcomes
OPTIMIZE-HF
BNP, brain natriuretic peptide.Kociol RD, et al. Circ Heart Fail. 2011;(4) 628-636.
CI UpperHR CI Lower
3
2.75
2.5
2.25
2
1.75
1.5
1.25
1300 800 1300 1800 2300 2800 3300 3800 4300
Discharge BNP
Haz
ard
Rat
io
Death at 1 Year
Haz
ard
Rat
io300 800 1300 1800 2300 2800 3300 3800 4300
Discharge BNP
Death or hospitalization at 1 Year2
1.9
1.8
1.7
1.6
1.5
1.4
1.3
1.2
1.1
1

NT-proBNP Reduction Lowers the Rate of CV Death or HF-related Hospitalization
NT-proBNP, N-terminal pro b-type natriuretic peptide.Zile MR, et al. J Am Coll Cardiol. 2016;68:2425-36.
Ris
k of
Prim
ary
Endp
oint
Af
ter
1 M
onth
0 1 2 3Years
0.5
0.4
0.3
0.2
0.1
0.0
Did not achieve NT-proBNP ≤1000 pg/mL
AchievedNT-proBNP ≤1000 pg/mL

Stage Characteristics Class Characteristics
A Significant risk factors for HF No known structural heart disease No signs or symptoms of HF
None
B Structural heart disease No signs or symptoms of HF I No functional limitation
C Structural heart disease Prior or current symptoms of HF
IIIIIIIV
No functional limitation Symptoms with activity beyond
ADLs Symptoms with ADLs Symptoms of HF at rest
D Refractory HF requiring specialized
interventions (eg, transplant, VAD, palliative care/hospice, and experimental therapies)
IV Symptoms of HF at rest
ACCF/AHA Stages and NYHA Functional Classes of HF
ACCF/AHA, American College of Cardiology Foundation/American Heart Association; VAD, ventricular assist device; ADLs, activities of daily living.ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.

HF Type by Ejection Fraction
*HFrEF has been defined across different guidelines by left ventricular ejection fraction 35%, <40%, and 40%.
EF, ejection fraction; HFpEF, heart failure with preserved ejection fraction.ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239; Tannenbaum S, et al. Curr Opin Cardiol. 2015;30(3):250-258.
HF
HFrEF(Systolic HF)
HFpEF(Diastolic HF)
EF ≤40%* EF ≥50%
Focus on risk factor controlPharmacologic and nonpharmacologic therapies

Treatment Options for HFrEF

Conventional Guideline-recommended Pharmacologic Treatments
() For select patients.ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; NYHA, New York Heart Association.ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.
TherapyNYHA Class
1 2 3 4
ACE inhibitors, ARBsBeta-blockersAldosterone antagonistsDiureticsDigoxin
Hydralazine and isosorbide dinitrate
()
()
() () ()
() ()()

Newer Therapies for the Treatment of HF
*The metallopeptidase neprilysin hydrolyzes natriuretic peptides.RAAS, renin-angiotensin-aldosterone system; NP, natriuretic peptide.von Lueder TG, et al. Pharmacol Ther. 2014;144(1):41-49; DiFrancesco D. Circ Res. 2010;106(3):434-446; Rosa GM, et al. Expert Opin Drug Metab Toxicol. 2014;10(2):279-291. Corlanor [prescribing information]. Amgen; 2015.
Therapy Mechanism of Action
Ivabradine• Selective inhibition of sinus node If channel (decreases HR)• Does not affect cardiac ionotropy and can be used with a
beta blocker
AngiotensinReceptor–Neprilysin
Inhibitor (ARNI)
• Angiotensin receptor blockade + inhibition of neprilysin*(inhibits RAAS and augmenting NP activity)

Impact of Ivabradine Treatment on CV Death or Hospital Admission for Worsening HF
Swedberg K, et al. Lancet. 2010;376(9744):875-885.
0 6 12 18 24 30Months
Patients with Primary Composite Endpoint (%)
Placebo (937 events)Ivabradine (793 events)
HR 0.82 (95% CI 0.75–0.90), P<.0001
0 6 12 18 24 30Months
Patients with First Hospital Admission for Worsening HF (%)
30 Placebo (672 events)Ivabradine (514 events)
HR 0.74 (95% CI 0.66–0.83), P<.0001
40
30
20
0
1010
20
0
CV, cardiovascular; HR, hazard ratio; CI, confidence interval.

Ivabradine Added on to Standard of Care Therapy Reduces the Risk of Hospitalizations for HF
Borer JS, et al. Eur Heart J. 2012;33(22):2813-2820.
HospitalizationIvabradine(N=3241)
Placebo(N=3264)
HR (95% CI) P value
First 514 (16%) 672 (21%) 0.75 (0.65–0.87) P<.001
Second 189 (6%) 283 (9%) 0.66 (0.55–0.79) P<.001
Third 90 (3%) 128 (4%) 0.71 (0.54–0.93) P<.012
0.4 0.6 0.8 1.0 1.2Favors Ivabradine Favors Placebo

Heart Rate Reduction with Ivabradine Improves Outcomes Independently of HF Duration
Bohm M, et al. Eur J Heart Fail. 2018;20:373–381.
Patie
nts,
%
0 6 12 18 24 30 36Time from Randomization, Months
50
40
30
20
10
0
Log rank P <.0001
Placebo
Patie
nts,
%
0 6 12 18 24 30 36Time from Randomization, Months
50
40
30
20
10
0
Log rank P <.0001
Ivabradine

Effect of ARNI Treatment on the Risk of Death or First-time Hospitalization for HF
McMurray JJ, et al. N Engl J Med. 2014;371(11):993-1004.
HR, 0.80 (95% CI, 0.71–0.89)P<.001
0 180 360 540 720 900 1080 1260Days Since Randomization
Cum
ulat
ive
Prob
abili
ty
0 180 360 540 720 900 1080 1260Days Since Randomization
1.0 Primary Endpoint
HR, 0.80 (95% CI, 0.73–0.87)P<.001
Cum
ulat
ive
Prob
abili
ty
0 180 360 540 720 900 1080 1260Days Since Randomization
1.0 Death From CV CausesC
umul
ativ
e Pr
obab
ility
0 180 360 540 720 900 1080 1260Days Since Randomization
1.0 Hospitalization for HF
HR, 0.79 (95% CI, 0.71‒0.89)P<.001
Cum
ulat
ive
Prob
abili
ty 1.0 Death from Any Cause
HR, 0.84 (95% CI, 0.76‒0.93)P<.001
EnalaprilARNI
0.60.50.40.30.20.10.0
0.60.50.40.30.20.10.0
0.60.50.40.30.20.10.0
0.60.50.40.30.20.10.0

ARNI Treatment Reduces the Incidence of Hospital Readmissions
Desai AS, et al. J Am Coll Cardiol. 2016;68(3):241-248.
21
13.4
30.5
20.317.8
9.7
27.8
17.1
0
5
10
15
20
25
30
35
30-day All-cause 30-day HF 60-day All-cause 60-day HFReadmission
EnalaprilARNI
Inve
stig
ator
-Rep
orte
d H
ospi
taliz
atio
ns
Asso
ciat
ed w
ith R
eadm
issi
on (%
)

ARNI Treatment Reduces CV Death and HF Hospitalization Across the LVEF Spectrum
LVEF, left ventricular ejection fraction.Solomon SD, et al. Circ Heart Fail. 2016;9(3):e002744.
Favors ARNI Favors Enalapril
OverallP interaction = 0.87
≤28>28 to 33≥33
Primary Endpoint
Hazard Ratio
Favors ARNI Favors Enalapril
.5 .75 1 1.25 1.5
CV Death
OverallP interaction = 0.55
≤28>28 to 33≥33
Hazard Ratio
Favors ARNI Favors Enalapril
.5 .75 1 1.25 1.5
.5 .75 1 1.25 1.5
OverallP interaction = 0.78
≤28>28 to 33≥33
HF Hospitalization
Hazard Ratio
All-Cause Death
OverallP interaction = 0.93
≤ 28> 28 to 33≥ 33
Hazard Ratio
Favors ARNI Favors Enalapril
.5 .75 1 1.25 1.5

How Should Newer Therapies Be Incorporated into GDMT?
Yancey, et al. J Am Coll Cardiol. 2018;71(2):201-230.
HFrEF Stage C Treatment
ACEI / ARB ANDbeta blocker with diuretic as needed
Titrate
Diuretics
Add
Hydralazine + isosorbide
dinitrate
Switch
ARNI
Add
Aldosterone Antagonist
Add
Ivabradine
For patients with persistent volume
overload, NYHA class II-IV
For persistently symptomatic African
Americans, NYHA class III-IV
For patients stable on ACEI/ARB,
NYHA class II-III
For patients with eGFR≥30 mL/min/1.72 m2,
K+ <5.0 mEq/dL,NYHA class II-IV
For patients with resting HR ≥70, on maximally tolerated beta blocker dose in sinus rhythm,
NYHA class II-III

Multi-center, patient-level, randomized, open-label study Patient population (N=~450)
– Reduced LVEF of 35% – HR 70 bpm – Discharged following stabilization from acute HF
Predischarge initiation of ivabradine or usual care Post-discharge follow-up at 7-14 days, 6 weeks,
and 180 days HR, systolic BP, and quality of life to be assessed
PRIME-HF: When Should Therapy Be Initiated?
Available at: https://clinicaltrials.gov/ct2/show/NCT02827500

Testing and Medication Titration for Patients with HFrEF
*BNP/NT-proBNP, complete blood count, basic metabolic panel, liver function tests, iron and thyroid studies, HbA1c, x-ray, echocardiogram, coronary angiogram, cardiac MRI, biopsy, other imaging.Yancey et al. J Am Coll Cardiol. 2018;71(2):201-230.
Consider initial evaluation studies*
End-intensification/ maintenance
Assess response to therapy and cardiac remodeling
Serial evaluation and titration of medications
Lack of response/instability
Referral for advanced care
Intensification 2-4 months
(1-4 week cycles)
Stabilization ~3 months

When to Refer Patients for Advanced HF Care: I-NEED-HELP
Yancey, et al. J Am Coll Cardiol. 2018;71(2):201-230.
IV inotropes
NYHA IIIB/IV or persistently elevated natriuretic peptides
End-organ dysfunction
Ejection fraction ≤35%
Defibrillator shocks
Hospitalizations >1
Edema despite escalating diuretics
Low blood pressure, high heart rate
Prognostic medication - progressive intolerance or down-titration of GDMT

Therapies for HFrEF Under Investigation

Effects of Omecamtiv Mecarbil on Cardiac Function and Structure
Teerlink JR, et al. Lancet. 2016;388:2895-903.
COSMIC-HFC
hang
e in
Sys
tolic
R
ejec
tion
Tim
e (m
s) 302520151050
-5
P=0.0007
P<0.0001A
Cha
nge
in
LVES
D(m
m) 0
-1-2-3-4-5
P=0.1732
P=0.0027
C
Placebo 25 mg Fixed Dose PK TitrationStudy Group
Cha
nge
in H
eat R
ate
(bea
ts p
er m
in) 2
10
-1-2-3-4
P=0.2177
P=0.0070
E
Cha
nge
in S
trok
e Vo
lum
e (m
l)
6420
-2-4
P=0.0036P=0.0217
B
Cha
nge
in
LVED
D(m
m)
1.51.00.5
0-0.5-1.0
P=0.1899
P=0.0128
D
Cha
nge
in N
T-pr
oBN
PC
once
ntra
tion
(ng/
L) 1000
500
0
-500
-1000Placebo 25 mg Fixed Dose PK Titration
Study Group
P=0.0205P=0.0069
F

Effect of Vericiguat Treatment in Patients with Worsening HFrEF
Gheorghiade M, et al. JAMA. 2015;314(21):2251-2262.
SOCRATES-REDUCED
Rat
io o
f Geo
met
ric M
eans
for C
hang
efr
om B
asel
ine
of N
T-pr
oBN
PLe
vel 1.3
1.2
1.1
1.0
0.9
0.8
0.7
0.6
0.51.25 mg 2.5 mg 2.5 to 2.5 to Pooled
5 mg 10 mg 2.5/5/10 mg
Vericiguat Group
P<.02
P<.05
Prop
ortio
n of
Pat
ient
s Ex
perie
ncin
g th
eC
ompo
site
of C
V D
eath
and
HF
Hos
pita
lizat
ion
0 28 56 84Day
0.25
0.20
0.15
0.10
0.05
0
1.25 mg2.5 mg2.5 to 5 mg2.5 to 10 mgPooled 2.5/5/10 mg groups
PlaceboVericiguat

Treatment of HFpEF

Increasing incidence
Frequent in elderly female patients
Comorbidities include obesity, CAD, DM, AF, and hyperlipidemia
HTN is the most important cause (60%-89% prevalence)
Represents a growing proportion of patients with HF requiring hospitalization
Significance of HFpEF
DM, diabetes mellitus.
ACCF/AHA Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.

Efficacy of Spironolactone Treatment of HFpEF Across the LVEF Spectrum
Solomon SD, et al. Eur Heart J. 2016;37:455–462.
TOPCAT Trial
P = 0.02In
cide
nce
Rat
e
40 50 60 70 80Ejection Fraction (%)
8
6
4
2
0
Primary Outcome
P = 0.79
Inci
denc
e R
ate 8
6
4
2
0
HF Hospitalization
40 50 60 70 80Ejection Fraction (%)
P = 0.002
Inci
denc
e R
ate 8
6
4
2
0
CV Death
40 50 60 70 80Ejection Fraction (%)
P = 0.004
Inci
denc
e R
ate 8
6
4
2
0
All-Cause Death
40 50 60 70 80Ejection Fraction (%)

ARNI for the Treatment of Patients with HFpEF: PARAGON-HF
Solomon, et al. JACC Heart Fail. 2017;5(7):471-482.
Sequential Single-Blind Run-In Period
Eligible patients who meet tolerability criteria at each safety/tolerability check visit are switched to the next study period
Randomized Double-Blind Long-Term Follow-Up Period
Follow-up visits occurred at 4, 16, 32, and 48 weeks and every 12 weeks thereafter. All patients are followed until target number of primary composite (CV deaths and total HF hospitalizations) occur or 26 months after randomization of the last patient elapse, whichever occurs last.
Screening period
Valsartan single-blind run-in
Sacubitril/Valsartan single-blind run-in
-2 weeks 1-4 weeks* 2-4 weeks† Sacubitril/Valsartan at a target dose of 97/103 mg bid
Valsartan at a target dose of 160 mg bid
N~4800
Safety/tolerabilitycheck
Safety/tolerability checkand randomizations (if eligible)
*Eligible patients are exposed to valsartan 80 mg bid for 1 to 2 weeks. Patients on low pre-study angiotensin converting enzyme inhibitors or angiotensin receptor blocker doses or those with tolerability concerns are first started on valsartan 40 mg bid 1 to 2 weeks and then up-titrated to valsartan 80 mg bid for 1 to 2 weeks.†Patients tolerating valsartan 80 mg bid for 1 to 2 weeks are switched to sacubitril/valsartan 49/51 mg bid for 2 to 4 weeks.

Management of Comorbidities

Target an optimal BP of <130/80 mm Hg in those with HTN and at increased risk (stage A HF)
Titration of GDMT to attain SBP <130 mm Hg in patients with HFrEF and HTN
Titration of GDMT to attain SBP <130 mm Hg in patients with HFpEF and persistent HTN after management of volume overload
Management of Hypertension in Patients with HF
BP, blood pressure; SBP, systolic blood pressure.
Yancey CW, et al. Circulation. 2017;136(6):e137-e161.

Use of Intravenous Iron for Patients with Symptomatic HF and Iron Deficiency
Ponikowski P, et al. Eur Heart J. 2015;36:657–668.
Odd
s R
atio
(95%
CI)
6 12 18 24 30 36 42 48 52Weeks Since Randomization
4
3.5
3
2.5
2
1.5
1
0.5
0Plac
ebo
bette
rFC
Mbe
tter
Self-reported Patients Global Assessment
P=0.29
P=0.035 P=0.047
P=0.001 P=0.001
NYHA Functional Class
Odd
s R
atio
(95%
CI)
6 12 18 24 30 36 42 48 52Weeks Since Randomization
12
10
8
6
4
2
0
Plac
ebo
bette
rFC
Mbe
tter
P=0.067P=0.093
P=0.004
P<0.001P<0.001

Impact of Intravenous Iron Therapy on Hospitalization Due to Worsening HF
Ponikowski P, et al. Eur Heart J. 2015;36:657–668.
Hos
pita
lizat
ion
Rat
e (p
er 1
00 S
ubje
cts)
0 90 180 270 360Time in Days
30
20
10
0
Placebo FCM
Log-rank testP=0.009

Benefits of Phrenic Nerve Stimulation in the Treatment of Central Sleep Apnea
Costanzo M, et al. Am J Cardiol 2018;121:1400–1408.
12 Months Active AHI Reduced ≥50%
SubgroupTreatment
% (n/N) Proportion (95% CI)Age
<65 58% (18/31)65 to <75 67% (10/15)≥75 100% (8/8)
SexFemale 71% (5/7)Male 66% (31/47)
Heart failureNo 61% (14/23)Yes 71% (22/31)
NYHA ClassI 60% (3/5)II 71% (10/14)III 75% (9/12)
DefibrillatorNo 69% (24/35)Yes 63% (12/19)
AHI severityModerate (15 - <30) 57% (4/7)Severe (≥30) 68% (32/47)
Prior SDB therapyNo 66% (21/32)Yes 68% (15/22)
Atrial fibrillationNo 66% (23/35)Yes 68% (13/19)
0 25 50 75 100

Improving Outcomes Through Effective Transitional Care

Obstacles to Effective Transitions of Care in HF
HCPs, health care providers; TOC, transitions of care. AHA Scientific Statement. Circ Heart Fail. 2015;8(2):384-409.
TOCConcerns
HCP Communication
• Poor handoff among HCPs• Insufficient patient
education
Medical Management
• Reconciliation issues• Unclear instructions• Transportation issues
Non-medication signs/symptoms (S/S) Management
• Nonadherence to diet, activity, exercise, & fluid management
• Not recognizing S/S requiring medical attention • Primary HCP is unclear about who to contact for
assistance
Follow-up Appointment
• No appointment scheduled within 7 days • Lack of transportation• HCP failure to follow GDMT• Patient unsure of location• Patient unaware

Frequency of Discharge Summary Transmission to Follow-up Providers
0
10
20
30
40
50
60
70
80
90
100
Site11
Site20
Site14
Site21
Site2
Site3
Site10
Site18
Site5
Site29
Site17
Site9
Site4
Site12
Site22
Site25
Site15
Site28
Site16
Site24
Site6
Site1
Site13
Site8
Site26
Site23
Site7
Site19
Site27
Dis
char
ge S
umm
arie
s Tr
ansm
itted
to
Fol
low
-up
Phys
icia
n (%
)
Sites
Salim Al-Damluji M, et al. Circ Cardiovasc Qual Outcomes. 2015;8(1):77-86.

Intervention Impact EvidenceHome-visiting programs and multidisciplinary HF (MDS-HF) clinic interventions
All-cause 3 to 6 months readmission High
Structured telephone support (STS) interventions
HF-specific and all-cause readmissions
High (HF-specific)Moderate (all-cause)
Home-visiting programs HF-specific readmission and composite end point* Moderate
Home-visiting programs, MDS-HF clinics, and STS interventions Mortality Moderate
High-intensity home-visiting program All-cause 30 day readmission and composite end point* at 30 days Low
Telemonitoring and primarily educational interventions
Did NOT reduce readmissions or mortality Low
Systematic Review of Transitional Care Interventions
*All-cause readmission or deathFeltner C, et al. Annals Intern Med. 2014;160(11):774-784.

Sytematic Review of Transitional Care Interventions Cont’d
Intervention Impact EvidenceHome-visiting programs and multidisciplinary HF (MDS-HF) clinic interventions
All-cause 3 to 6 months readmission High
Structured telephone support (STS) interventions
HF-specific and all-cause readmissions
High (HF-specific)Moderate (all-cause)
Home-visiting programs HF-specific readmission and composite end point* Moderate
Home-visiting programs, MDS-HF clinics, and STS interventions Mortality Moderate
High-intensity home-visiting program All-cause 30 day readmission and composite end point* at 30 days Low
Telemonitoring and primarily educational interventions
Did NOT reduce readmissions or mortality Low

AHA Recommended Strategies for Improving Transitional Care in HF Patient education Phone follow-up (48-72
hours) Early postdischarge
follow-up visit (7-10 days) Early assessment after
admission
Medication reconciliation Caregiver inclusion Home visits Handoff communication
to post-hospital providers
AHA Scientific Statement. Circ Heart Fail. 2015;8(2):384-409.

Recognition of escalating symptoms/concrete plan for response Activity/exercise Indications, use, and need for medication adherence Daily weight monitoring Modification of risk factors for HF progression Diet End-of-life considerations Follow-up Discharge instructions
Enhanced HF Patient Education: What Domains Should Be Covered?
Available at: http://www.heart.org/idc/groups/heart-public/@private/@wcm/@hcm/@gwtg/documents/downloadable/ucm_428949.pdf

Lee KK, et al. Med Care. 2016; 54(4): 365–372.
Risk of 30-Day Readmission by PostdischargeFollow-up Contact
Type
of F
irst
Cont
act Telephone
Clinic
Num
ber o
f Co
ntac
ts > 2 Contacts
1 or 2 Contacts
Tim
e to
Firs
t Co
ntac
t 8-30 Days
1 to 7 Days
No Contact
12.1%
10.7%
7.3%
13.1%
8.9%
12.0%
29.3%
Unadjusted Risk of 30-Day Readmission

Case Evaluations

Judy is a 68-year-old woman who presents to the ED for acute distress due to breathlessness and uncontrolled coughing. She reports that over the past 4 months, she has had some difficulty climbing stairs and breathing when lying down (having to sit back up to catch her breath). Judy’s medical history includes a remote history of smoking and alcohol consumption. She is dyslipidemic and moderately obese.
Case Evaluation #1: Patient Description
ED, emergency department.

Case Evaluation #1: Question 1
A. Blood testing for BNP/NT-proBNPB. Invasive hemodynamic monitoringC. Endomyocardial biopsy
Judy’s physical exam confirms dyspnea on exertion and reveals significant ankle edema. Her BP = 130/86 mm Hg, HR = 90 bpm, JVD 12 cm, and she has a positive Kussmaul sign. Which of the following tests would you order to further aid in your diagnosis?
A. B. C.
0% 0%0%
:8

Case Evaluation #1: Question 2
A. Maintain current treatment regimenB. Switch to ARNIC. Switch to ivabradine
Judy is diagnosed with NYHA III Stage C HFrEF. Following stabilization, she is initiated on a regimen that includes lisinopril and carvedilol. At her 3 month follow-up, clinical and laboratory assessments indicate that she is stable with her current treatment plan. Which of the following would you recommend for Judy?
A. B. C.
0% 0%0%
:8

Case Evaluation #1: Question 3
A. 12 hoursB. 36 hoursC. 3 days
If you were to switch Judy to ARNI, how long would wait before initiating ARNI after discontinuing lisinopril?
A. B. C.
0% 0%0%
:8

Jim is a 73-year-old man who presents with breathlessness over the past 2 days. His history includes 3 prior hospital admissions for worsening HF over 2 years. He has difficulty with ADLs. Previous echocardiograms have shown moderate LV systolic dysfunction (EF 26%, PASP 55 mm Hg, EDD 6.7 cm). Physical exam reveals BP 98/78 mm Hg, HR100 bpm, RR 25/min, S4, and displaced point of maximal impulse. Jim’s EMR reveals that he has a history of iron deficiency as well. His current medications include aspirin, furosemide, enalapril, and carvedilol.
Case Evaluation #2: Patient Description
PASP, pulmonary artery systolic pressure; S4, fourth heart sound; EMR, electronic medical record.

Case Evaluation #2: Question 1
A. Addition of ARNI to Jim’s current treatment regimen
B. Increase the dose of carvedilolC. Switch Jim from enalapril to
ivabradine
Which of the following changes to Jim’s therapeutic regimen would you recommend for Jim?
8A. B. C.
0% 0%0%
8

Case Evaluation #2: Question 2
A. Dietary iron supplementationB. Intravenous iron therapyC. Erythropoietin therapy D. No therapy
What type of intervention, if any, would you consider for the treatment of Jim’s iron deficiency?
8A. B. C.
0% 0%0%
8

Despite recent progress in the reduction of HF-related readmission rates, the health outcomes of many patients with HF remain suboptimal
Optimal management of HF requires thorough and accurate patient evaluation along with the implementation of guideline-directed medical therapy to control symptoms and improve prognosis
New treatment options have expanded the range of strategies toachieve therapeutic goals and demonstrated the capacity to significantly improve patient outcomes over standard therapy
Summary

For patients with symptoms of HF, apply a multifaceted evaluation approach to identify underlying causes and risk for disease progression
Implement guideline-directed medical therapy for all patients with HF
Consider treatment using a newer agent with a novel mechanism of action for any patients who remain symptomatic despite their current regimen as well as those who are stable but may benefit from a switch in therapy
Prior to discharge, evaluate patients’ clinical status, comorbid conditions, and current medication regimen, and adjust the care plan accordingly
Schedule timely follow-up and ensure adequate communication of the care plan to the nursing home team, home healthcare team, PCP, or family caregiver
Clinical Pearls

Questions and Answers

Thank You!