Embed Size (px)
DESCRIPTION
This study presents the results of a randomized treatment trial of family therapy and two control treatments for 119 outpatient opiate users. All treatments were combined with a methadone reduction programme.
Citation preview

A comparative study of family therapy in the treat-ment of opiate users in a London drug clinic
Dennis Yandoli,a Ivan Eislerb, Claire Robbins,c
Geraldine Mulleadyd and Christopher Daree
This study presents the results of a randomized treatment trial of familytherapy and two control treatments for 119 outpatient opiate users. Alltreatments were combined with a methadone reduction programme. Thecontrol treatments were: (1) a ‘standard’ treatment (supportivepsychotherapy) and (2) a ‘low contact’ intervention. Treatment outcomewas evaluated six and twelve months after the initial assessment. Both thefamily therapy and minimal intervention groups had a significantly highernumber of drug-free days at six and twelve months, compared to the stan-dard treatment, despite receiving fewer treatment sessions. Across alltreatments there was evidence for a gender difference in response to ther-apy in users who were in a couple relationship. In couples where bothpartners were using drugs women did significantly better than men. Menliving with a non-drug-abusing partner fared better than men living witha drug-using partner. Across the treatment groups diminution in drug usewas accompanied by improvements in psychosocial functioning.Unemployment, sharing needles and injecting drugs were predictive ofpoor outcome.
Introduction
It is often assumed that drug users lead a chaotic, transientlifestyle isolated from their families, and many clinicians are there-fore sceptical about the possibility of involving the family activelyin treatment. Although it is true that engaging families of drugusers is often difficult (Szapocznik et al., 1988), the perception
2002 The Association for Family Therapy and Systemic Practice
The Association for Family Therapy 2002. Published by Blackwell Publishers, 108 CowleyRoad, Oxford, OX4 1JF, UK and 350 Main Street, Malden, MA 02148, USA.Journal of Family Therapy (2002) 24: 402–4220163–4445
a Senior Family Therapist/Manager, Institute of Psychiatry, London, UK.b Senior Lecturer in Clinical Psychology, Institute of Psychiatry, London, UK.c Clinical Nurse Specialist – Family Therapy, Institute of Psychiatry, London, UK.d Clinical Psychologist, Institute of Psychiatry, London, UK.e Reader in Psychotherapy, Institute of Psychiatry, London, UK.
Address for correspondence: Ivan Eisler, Psychotherapy Section, Institute ofPsychiatry, De Crespigny Park, London SE5 8AF, UK.
that this is due to the family being uninvolved does not accordwith the empirical evidence, as drug addicts are often quite closelyconnected (some would argue too closely connected) to theirfamilies. For instance, Vaillant (1966) found in a sample of drugusers in New York that 72 per cent were living with their familiesat age 22, and 47 per cent by age 30. Stanton et al. (1982) foundthat 66 per cent of eighty-five male heroin users either residedwith their parents or saw their mothers daily. In Britain, Bean(1971) in a study of 100 drug offenders, with an average age of 20,two-thirds of whom were using heroin, reported that 33 per centlived with their parents. Also in Britain, Crawley (1971) examined134 opiate users (mean age 21 years) admitted to a treatmentservice, and found that 62 per cent lived at home with theirparents. Similar findings have been found in many other studies(cf. Stanton and Shadish, 1997). Stanton et al. (1982) have alsosuggested that where the drug user is in a couple relationship thisis often unstable, compared with the misuser’s relationship withhis family of origin. The stress of treatment, particularly if the rela-tionship was established during active drug use, frequently drovethe couple apart, with the drug user returning to his family oforigin. To what extent these patterns pre-exist the drug misuserather than being a consequence is unclear.
In the family therapy literature, aspects of family functioning,which seem to encourage or maintain drug use by denying otherareas of conflict within the family system, have been described byclinicians (Madanes et al., 1980; Stanton et al., 1982; Kaufman,1985). Haley (1980) described the functional value heroin usecan attain in families, and there are indications from clinical stud-ies that the family system plays an important role in maintainingdrug use (Harbin and Maziar, 1975). Del Orto (1974) empha-sized the importance of family participation to minimize the riskof relapse, and suggested that attempting to treat drug users with-out seeing the family was futile. Commonly, the user is describedas remaining enmeshed in his family of origin, forgoing his needto separate normally. The goal of family-based treatment is there-fore generally seen as being to focus attention on these patternsof behaviour in order to bring about change in the drug user’sstatus regarding his use of drugs, as well as his role within thefamily system.
The enthusiasm of family therapists for their therapeuticapproach is not always matched by systematic evaluation of such
Family therapy in the treatment of opiate users 403
2002 The Association for Family Therapy and Systemic Practice

treatments. However, in the field of drug addiction there is agrowing number of studies providing support for the efficacy offamily therapy. Stanton and colleagues (Stanton et al., 1982)devised a short-term structural-strategic family therapy approachwhich, in combination with a methadone regime, they found tobe more effective in reducing drug use than either individualcounselling or taking part in a neutral family task. Szapocznikand colleagues demonstrated the efficacy of family-oriented treat-ments with young drug-abusing subjects from a Hispanic ethnicminority (Szapocznik et al., 1983, 1986). More recent studies haveshown family therapy to be more effective than individual coun-selling by probation officers (Hengeller et al., 1991; Borduin etal., 1995), group therapy (Joanning et al., 1992) or familypsychoeducation (Lewis et al., 1990; Joanning et al., 1992). On thebasis of a meta-analysis of over 1500 cases Stanton and Shaddish(1997) concluded that family/couples therapy is more effectivethan individual counselling/therapy, group therapy or familypsychoeducation. Reviews by Liddle (1995), Carr (2000a, 2000b)and Cormack and Carr (2000) have also concluded that familytherapy for substance abuse is gaining growing support fromempirical studies of treatment efficacy. The study cited in thispaper reports the results of a randomized treatment trial offamily therapy and two control treatments for adult opiate userswhich provides further evidence for the effectiveness of familytherapy.
Methodology
Participants
Opiate users presenting to an inner-city drug dependency clinicwere selected for the following criteria: absence of a history ofpsychiatric treatment; age over 18; not currently dependenton alcohol; opiate usage of more than six months’ duration. Tobe included in the study, patients also had to agree to be seenwith their partner or family, if required, during treatment. Afterinformed consent to participation in the study was obtained,a urine sample was taken. Once three consecutive daily urinespecimens were positive for opiates, a full assessment interviewwas arranged and the methadone reduction programme wasstarted.
404 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice
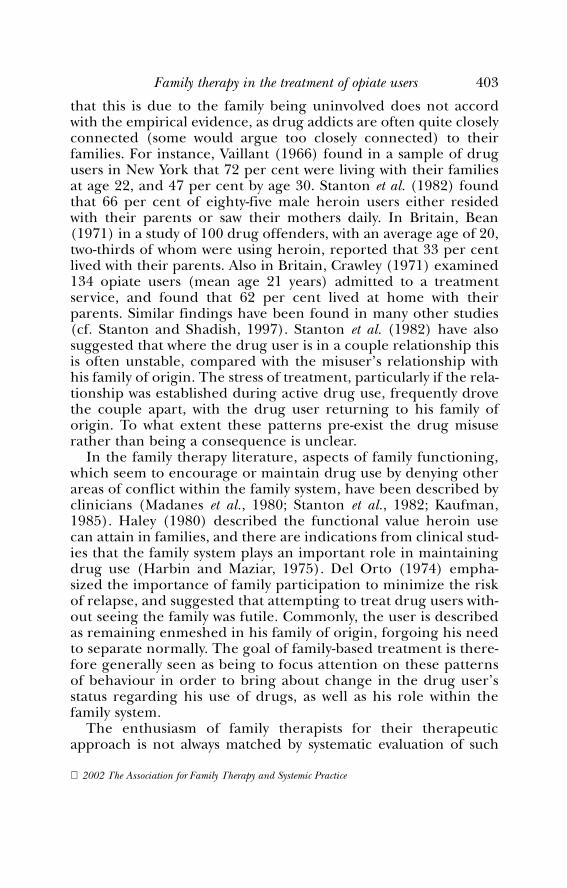
Over a fourteen-month period 423 drug users presented to theclinic seeking treatment. Of these, 119 subjects met the criteria forinclusion in the study and agreed to involve one or more familymembers, if required. Eighty-two per cent were self-referred, and allwere using opiate drugs, either illicit or prescribed, on a daily basis.
The characteristics of the subjects at presentation are shown inTable 1. Two-thirds of the subjects were male and their mean agewas 28.2 years. Over 80 per cent were either married or cohabiting.Nearly two-thirds of the partners were also drug users. Of thefemale drug users in the study, 71 per cent were in a partnershipwith another drug user, compared with 43 per cent of the male drugusers. Half of those living with a sexual partner also had a child inthe household. Only a small proportion were living with their familyof origin (14 per cent) or were living alone (6 per cent). A quarterof the subjects were in regular full-time employment, and half wereunemployed. Seven per cent gave their occupation as executive ormanagerial, 23 per cent as administrative, personnel, clerical andsales, 49 per cent as skilled manual and 19 per cent as unskilled.
Characteristics of drug use at presentation
The subjects were typically injecting drugs (70 per cent), asmaller number smoking, inhaling or taking the drug orally. All
Family therapy in the treatment of opiate users 405
2002 The Association for Family Therapy and Systemic Practice
TABLE 1 Characteristics of subjects at presentation
Sex Male 63%Female 37%
Age (years) x = 28.2; s.d. = 5.1Living arrangement Drug-using partner 53%
Non-drug-using partner 28%Family of origin 14%Living alone 6%
Employment Full-time work 27%Part-time work 20%Unemployed 53%
Occupation Executive or managerial 7%Administration,
clerical or sales 23%Manual 50%Unskilled 20%
of them were using opiates daily, although only just over one-third (35 per cent) described heroin as their drug of choice.Nevertheless, 86 per cent reported that heroin was their majorproblem drug, while the remaining subjects saw their main diffi-culty as being with either methadone (6 per cent), a combinationof various drugs (5 per cent) and occasionally barbiturates orother drugs. The majority of the subjects were heavy (58 percent) or moderate (36 per cent) drug users using Gossop et al.’s(1987) criteria.1 The heavy drug use is reflected in the amount ofmoney that subjects reported to spend on drugs in a thirty-dayperiod (x = £883). There was a high level of criminal convictions(33 per cent with one to five convictions, 9 per cent with six to tenconvictions and 17 per cent with eleven to thirty convictions; 18per cent refused to give details about their criminal records, and23 per cent said they had not been charged with a criminaloffence). The most frequent offences were shoplifting, drugcharges and deception. Some of the subjects had been chargedwith burglary, assault and robbery, and one with homicide.
The assessment and allocation to treatment
Three members of staff, a psychiatrist, another member of theclinic team and a member of the research team, carried out eachassessment. All the subjects were assessed using a standard semi-structured interview covering demographic information, currentpsychosocial functioning and drug use. The Addiction SeverityIndex (ASI) (McLellan et al., 1980) was scored from this inter-view. Standard psychometric tests, the Tyrer Brief Anxiety Scale(TBAS) (Tyrer et al., 1984) and the Montgomery and AsbergDepression Rating Scale (MADRS) (Montgomery and Asberg,1979) were also administered. Subjects were then randomly allo-cated either to family therapy (forty-one subjects) or to one oftwo control treatments: standard clinic treatment (thirty-eightsubjects) or ‘low’ contact (forty subjects). When a subject wascohabiting with another drug user both partners were placed inthe same treatment group. In the non-family therapy modalities,
406 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice
1 Heavy use = Heroin > 0.5g/day; Moderate use = Heroin 0.125g to 0.5g/day;Low use = Heroin <0.125g/day (or equivalent: e.g. 60mg of methadone = 0.5gstreet heroin) (Gossop et al., 1987).

each of the drug-using members of a couple was treated by adifferent therapist.
The random allocation resulted in relatively well-matchedgroups. There were no significant differences between the threegroups on any of the social, demographic or drug-use variables withthe exception of the age of onset. The low-contact group had amean age of onset of 21.6 years (s.d. 4.1), whereas in the family ther-apy group the mean age was 24.2 (s.d. 5.6) and in standard treat-ment 24.7 (s.d. 5.5) (F=4.14; p < 0.02).
The treatments
1 Family therapy (FT). The family therapy was a combined struc-tural and strategic approach following the model of Stanton et al.(1982), which placed particular emphasis on developing appro-priate boundaries and limits before introducing a strategic inter-vention. Patients in this group were allocated to one of theresearch therapists, a social worker and a nurse both of whomwere trained in family therapy. The therapist made arrangementson the day of assessment for the involvement of the patient’sfamily or partner in future sessions. They were seen for one hourfor up to sixteen sessions, initially every two weeks and thenmonthly or less often. Where the patient was in a couple rela-tionship the therapist worked primarily with the couple.Nevertheless, other significant relationships were always includedin the discussions during sessions, and other family members(parents and/or children or other family members)2 were alsoinvited to attend some sessions. Occasionally, if the family or part-ner did not attend a session, the individual was seen but the inter-view always focused on discussion of family relationships as well asmethadone reduction. Methadone was prescribed in a strictreduction regime, reducing the daily dose by 5mg every twoweeks. The non-negotiable methadone reduction regime wasopenly discussed, thereby modelling the achievement of thesegoals with the subject and other family members.
Family therapy in the treatment of opiate users 407
2002 The Association for Family Therapy and Systemic Practice
2 We have used the term ‘family therapy’ (rather than couple therapy)throughout the paper to emphasize that even when the work was mainly with thecouple, conceptually, the family as a whole was always part of the therapists’consideration.

2 Standard clinic treatment (ST). The therapists for this group weremembers of the drug dependency clinic staff, which included sixnurses, a social worker, a consultant psychiatrist and two otherpsychiatrists. The treatment was provided by members of the multi-disciplinary team, most of whom came from a nursing background,and the majority did not have extensive training in psychotherapy.The treatment did not follow a clearly defined theoretical model andis best described as pragmatic, supportive counselling combinedwith information and advice on managing the drug problem andrelated issues. The subjects had their methadone reduced slowly asadvised by the case manager or the clinic staff, who met regularly todiscuss the treatment of all their patients. Methadone was prescribedin a flexible reduction regime, which sometimes included continu-ing on a stable dose or occasionally increasing the dose temporarily.The pace of methadone reduction and frequency of appointmentswere determined to a large extent by the expressed needs of theclients. The course of treatment was open-ended.
3 Low contact treatment (LC). Subjects in this group were seen by oneof the two research therapists. It was a more structured, limitedapproach than the standard treatment and discouraged dependencyon the therapist. On the day of assessment the therapist gave subjectsa package of information about local services, which might assist themin remaining drug-free (i.e. housing, social services, self-help groupsand information about drugs and the treatment programme). Theywere seen monthly for a standardized thirty-minute interview for up totwelve months. Methadone was prescribed using the non-negotiablemethadone reduction regime used in the family therapy treatmentgroup, reducing the daily dose by 5mg every two weeks.
Assessment of outcome and data analysis
Outcome was assessed at six months and one year after the start oftreatment when all the initial screening measures were repeated.Whenever possible, the assessment included those subjects who hadterminated treatment early. Subjects were contacted at their lastknown address or through a contact person established at assess-ment. Frequency of opiate usage was seen as the main outcomemeasure rather than the composite score from the AddictionSeverity Index, as opiate usage gives a clinically more meaningful
408 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice

picture than the ASI score. For the main outcome comparisonssubjects were categorized into three groups:
1 opiate-free (i.e. those using neither street drugs nor prescribedmethadone)
2 occasional users (those using less than twenty-five days per month)3 regular users (those using twenty-five days or more per month).
We also report outcome data based on heroin usage alone (i.e. nottaking into account the usage of prescribed methadone).
The data were analysed using the STATISTICA for Windowsprogram version 5.5 (Statsoft Inc, 1999). For continuous data theMANOVA test was performed. Categorical data were tested usingthe chi-square and Fisher Exact Probability Test as appropriate. Themain comparisons between treatments were done on an intention-to-treat basis. For these analyses baseline data were used for subjectswho were in prison (one subject at the six-month assessment andseven at the twelve-month assessment) or who were not available forfollow-up. To ensure that differential retention rates for the threetreatments did not bias the results, the analyses were repeated usingonly those subjects for whom complete data were available at thesix- and twelve-month assessment dates.
Results
Of the 119 subjects originally assessed, 101 (85 per cent) werefollowed up at six months. At six months the proportion of casesfollowed up from each treatment group was similar (88 per cent inFT, 84 per cent in ST and 83 per cent in LC). At twelve months onlyeighty-four subjects (70 per cent) were seen, with the reduction innumbers most noticeable in the standard treatment group of whomonly twenty-four (63 per cent) were available and willing to be seencompared to twenty-eight (70 per cent) for the low-contact groupand thirty-two (78 per cent) for the family therapy group.
The mean number of sessions attended differed by treatmentgroup. Those in the family therapy group attended an average of 13.7(s.d. = 6.5) sessions,3 those in the low-contact group 8.9 (s.d. = 4.1)
Family therapy in the treatment of opiate users 409
2002 The Association for Family Therapy and Systemic Practice
3 The average amount of therapist time needed per user in FT is in fact lower ifone takes into account that in some families both partners were using drugs. Theaverage number of sessions per user (10.1, s.d. 8.6) is not significantly differentfrom the LC group.
sessions and those who received the standard clinic treatment a meanof 18.1 (s.d. = 10.2) sessions (F = 3.6; p < 0.0001).
Overall changes in drug use and self-rating
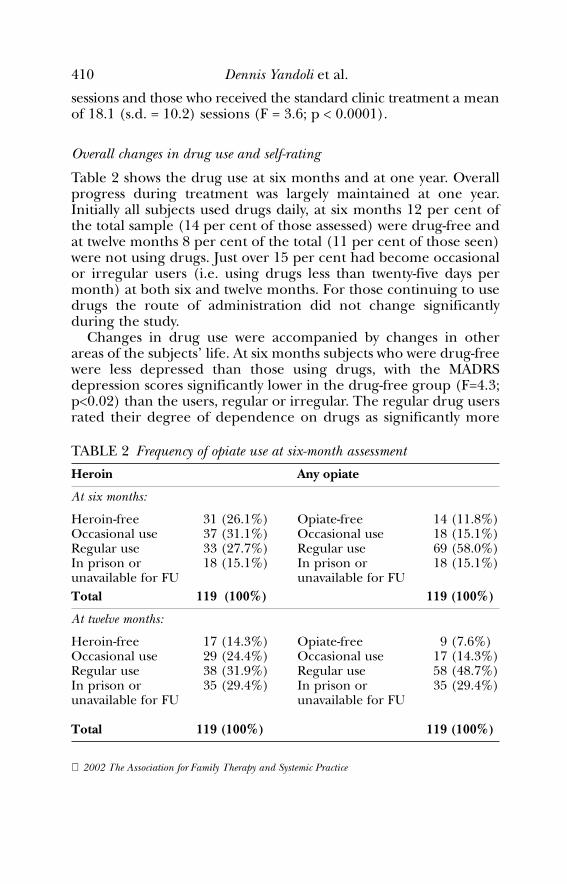
Table 2 shows the drug use at six months and at one year. Overallprogress during treatment was largely maintained at one year.Initially all subjects used drugs daily, at six months 12 per cent ofthe total sample (14 per cent of those assessed) were drug-free andat twelve months 8 per cent of the total (11 per cent of those seen)were not using drugs. Just over 15 per cent had become occasionalor irregular users (i.e. using drugs less than twenty-five days permonth) at both six and twelve months. For those continuing to usedrugs the route of administration did not change significantlyduring the study.
Changes in drug use were accompanied by changes in otherareas of the subjects’ life. At six months subjects who were drug-freewere less depressed than those using drugs, with the MADRSdepression scores significantly lower in the drug-free group (F=4.3;p<0.02) than the users, regular or irregular. The regular drug usersrated their degree of dependence on drugs as significantly more
410 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice
TABLE 2 Frequency of opiate use at six-month assessment
Heroin Any opiate
At six months:
Heroin-free 31 (26.1%) Opiate-free 14 (11.8%)Occasional use 37 (31.1%) Occasional use 18 (15.1%)Regular use 33 (27.7%) Regular use 69 (58.0%)In prison or 18 (15.1%) In prison or 18 (15.1%)unavailable for FU unavailable for FUTotal 119 (100%) 119 (100%)
At twelve months:
Heroin-free 17 (14.3%) Opiate-free 9 (7.6%)Occasional use 29 (24.4%) Occasional use 17 (14.3%)Regular use 38 (31.9%) Regular use 58 (48.7%)In prison or 35 (29.4%) In prison or 35 (29.4%)unavailable for FU unavailable for FU
Total 119 (100%) 119 (100%)
serious than those who were occasional users or drug-free (ASIDegree of Drug Dependency – F=5.8; p<0.005). There were nodifferences overall in the subjects’ view of their ability to cope withlife, family relationships and leisure activities, but those who werenot using drugs rated themselves as significantly more confidentthan those using occasionally or regularly (ASI Confidence – F=5.3;p<0.01). At six months, the drug-free group had lower Tyrer anxi-ety scores but the difference did not reach statistical significance.
At twelve months, there was again no significant difference inanxiety scores. Depression scores (F=6.8; p<0.002), plus a numberof measures on the Addiction Severity Index (Degree of DrugDependency – F=18.0; p<0.001, Coping with Life Generally – F=1.2;p<0.005, Relationships with the Family – F=5.2; p<0.01, LeisureActivities – F=3.3; p<0.05 and Confidence – F=6.43; p<0.005) wereall better in those who were drug-free compared with the regularusers. The occasional drug users had intermediate scores. At twelvemonths the mean amount of money that subjects estimated theyhad spent on drugs was £332 (s.d. 568) compared with £883 (s.d.1150) at presentation.
Predictors of outcome
Of those who were unemployed at assessment, 72.5 per cent wereusing drugs daily and only 2.5 per cent were opiate-free at twelvemonths, whereas of those who had been in a job at the outset, 20per cent were drug-free and another 20 per cent had significantlyreduced their usage (X2=6.1; p<0.05). Initially, half of the subjectsreported that they shared their needles. They were significantlymore likely to be using drugs regularly at one year than those whodid not (p=0.01, Fisher test).
Gender, family configuration and outcome
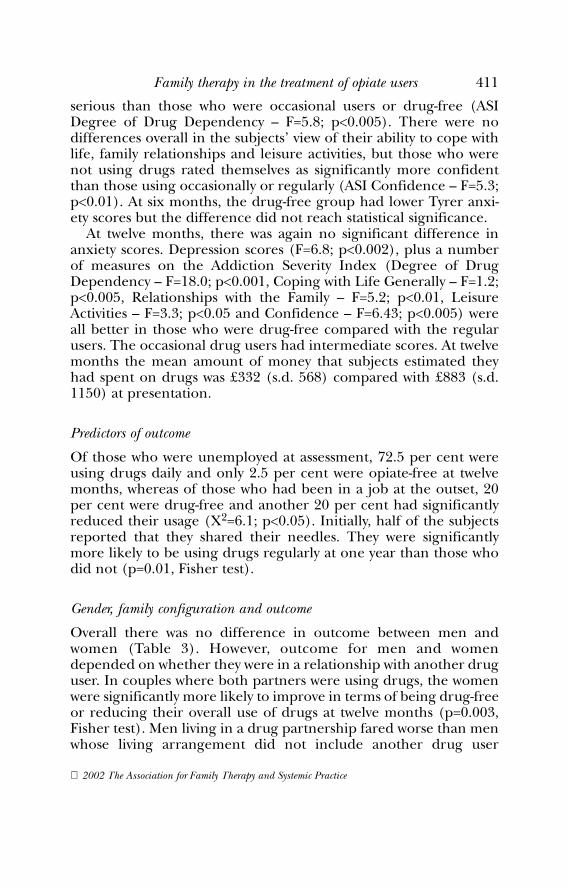
Overall there was no difference in outcome between men andwomen (Table 3). However, outcome for men and womendepended on whether they were in a relationship with another druguser. In couples where both partners were using drugs, the womenwere significantly more likely to improve in terms of being drug-freeor reducing their overall use of drugs at twelve months (p=0.003,Fisher test). Men living in a drug partnership fared worse than menwhose living arrangement did not include another drug user
Family therapy in the treatment of opiate users 411
2002 The Association for Family Therapy and Systemic Practice
(p=0.03, Fisher test). There were relatively few drug-using womenwho were not in a relationship with another user and their outcomeat one year was generally poor (85 per cent using drugs dailycompared with 74 per cent of males in a non-drug partnership and63 per cent of women whose partners were also using). There wereno differences in outcome between individuals living alone or withtheir family of origin and those living as a couple.
Differences in outcome for the three treatment groups
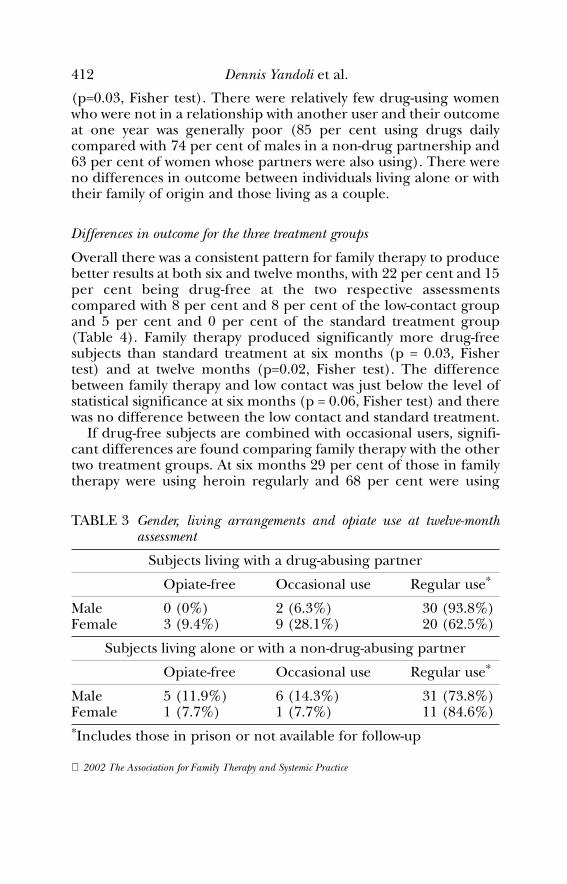
Overall there was a consistent pattern for family therapy to producebetter results at both six and twelve months, with 22 per cent and 15per cent being drug-free at the two respective assessmentscompared with 8 per cent and 8 per cent of the low-contact groupand 5 per cent and 0 per cent of the standard treatment group(Table 4). Family therapy produced significantly more drug-freesubjects than standard treatment at six months (p = 0.03, Fishertest) and at twelve months (p=0.02, Fisher test). The differencebetween family therapy and low contact was just below the level ofstatistical significance at six months (p = 0.06, Fisher test) and therewas no difference between the low contact and standard treatment.
If drug-free subjects are combined with occasional users, signifi-cant differences are found comparing family therapy with the othertwo treatment groups. At six months 29 per cent of those in familytherapy were using heroin regularly and 68 per cent were using
412 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice
TABLE 3 Gender, living arrangements and opiate use at twelve-monthassessment
Subjects living with a drug-abusing partner
Opiate-free Occasional use Regular use*
Male 0 (0%) 2 (6.3%) 30 (93.8%)Female 3 (9.4%) 9 (28.1%) 20 (62.5%)
Subjects living alone or with a non-drug-abusing partner
Opiate-free Occasional use Regular use*
Male 5 (11.9%) 6 (14.3%) 31 (73.8%)Female 1 (7.7%) 1 (7.7%) 11 (84.6%)*Includes those in prison or not available for follow-up
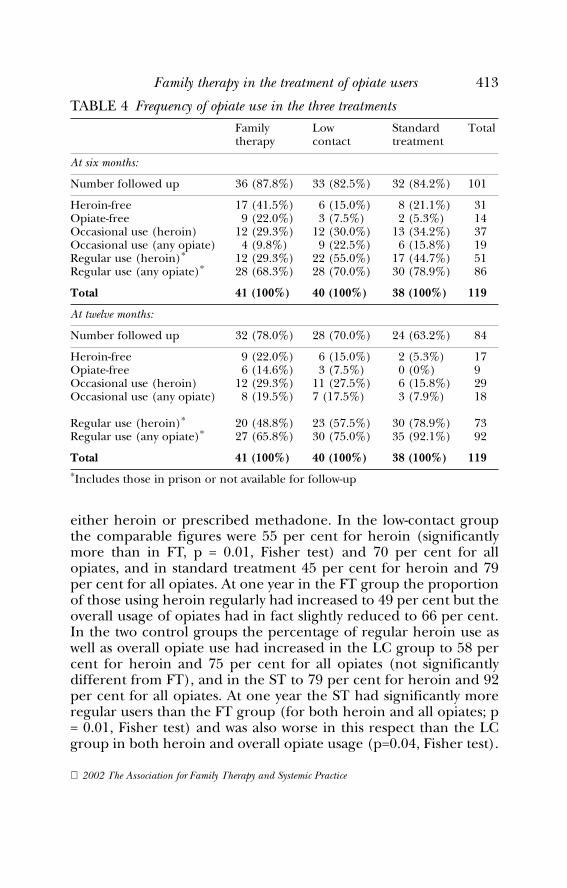
either heroin or prescribed methadone. In the low-contact groupthe comparable figures were 55 per cent for heroin (significantlymore than in FT, p = 0.01, Fisher test) and 70 per cent for allopiates, and in standard treatment 45 per cent for heroin and 79per cent for all opiates. At one year in the FT group the proportionof those using heroin regularly had increased to 49 per cent but theoverall usage of opiates had in fact slightly reduced to 66 per cent.In the two control groups the percentage of regular heroin use aswell as overall opiate use had increased in the LC group to 58 percent for heroin and 75 per cent for all opiates (not significantlydifferent from FT), and in the ST to 79 per cent for heroin and 92per cent for all opiates. At one year the ST had significantly moreregular users than the FT group (for both heroin and all opiates; p= 0.01, Fisher test) and was also worse in this respect than the LCgroup in both heroin and overall opiate usage (p=0.04, Fisher test).
Family therapy in the treatment of opiate users 413
2002 The Association for Family Therapy and Systemic Practice
TABLE 4 Frequency of opiate use in the three treatmentsFamily Low Standard Totaltherapy contact treatment
At six months:
Number followed up 36 (87.8%) 33 (82.5%) 32 (84.2%) 101
Heroin-free 17 (41.5%) 6 (15.0%) 8 (21.1%) 31Opiate-free 9 (22.0%) 3 (7.5%) 2 (5.3%) 14Occasional use (heroin) 12 (29.3%) 12 (30.0%) 13 (34.2%) 37Occasional use (any opiate) 4 (9.8%) 9 (22.5%) 6 (15.8%) 19Regular use (heroin)* 12 (29.3%) 22 (55.0%) 17 (44.7%) 51Regular use (any opiate)* 28 (68.3%) 28 (70.0%) 30 (78.9%) 86
Total 41 (100%) 40 (100%) 38 (100%) 119
At twelve months:
Number followed up 32 (78.0%) 28 (70.0%) 24 (63.2%) 84
Heroin-free 9 (22.0%) 6 (15.0%) 2 (5.3%) 17Opiate-free 6 (14.6%) 3 (7.5%) 0 (0%) 9Occasional use (heroin) 12 (29.3%) 11 (27.5%) 6 (15.8%) 29Occasional use (any opiate) 8 (19.5%) 7 (17.5%) 3 (7.9%) 18
Regular use (heroin)* 20 (48.8%) 23 (57.5%) 30 (78.9%) 73Regular use (any opiate)* 27 (65.8%) 30 (75.0%) 35 (92.1%) 92
Total 41 (100%) 40 (100%) 38 (100%) 119*Includes those in prison or not available for follow-up

Further analyses were performed to evaluate whether those whowere in a couple relationship responded differently to treatmentfrom those who were still living with their family of origin or ontheir own. The findings were clearest for those living with a part-ner (some of whom were also users); nine out of thirty-threesubjects treated with couple/family therapy were drug-free at sixmonths (two were occasional users), compared with one out ofthirty-two subjects in the low-contact group (six occasional users)and one out of thirty-one in the standard treatment (six occa-sional users) (X2 = 13.84, p< 0.01). The differences between thetreatments were less clear at one year. The number who weredrug-free or only occasional users was still significantly higher inthe FT group (four opiate-free, six occasional) compared with theST group with no drug-free subjects and only three occasionalusers (p = 0.04, Fisher test), but the LC group showed similarresults (three opiate-free, five occasional) to family therapy. Theresults for individuals living without a partner showed no clearpattern at six months, but at one year again appeared to favourfamily therapy, with four out of eight being drug-free or occa-sional users whereas all seven in the standard treatment wereusing drugs daily (p = 0.05, Fisher test).
All the data analyses were also conducted including only thosesubjects for whom complete assessment data were available at eitherassessment point. The results were essentially the same for each ofthe above comparisons.
Mortality rates
At one year, two patients had died (both from the FT group). At fiveyears, according to the Central Register of Births, Marriages andDeaths, there were three further deaths (one from the FT groupand two from the ST group).4 There were no deaths in the low-contact group. Thus the overall death rate at five years was 4.2 percent. The differences in death rates between treatment groups arenot statistically significant.
414 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice
4 In the family therapy group one subject committed suicide and two died as aresult of an accidental drug overdose. In the standard treatment group one subjectdied in a car accident and one of an accidental overdose.

Discussion
Before discussing the findings, it is necessary to examine factorsthat may have biased the results. The first question is about the reli-ability of the data. The most reliable information was obtainedabout the number of deaths. Over five years the overall death rateof 4.2 per cent may be compared with Oppenheimer and Stimson’s(1982) death rate of 12 per cent over seven years and Vaillant’s of23 per cent over twenty years (Vaillant, 1973).
The assessment of drug use, on the other hand, depended largelyon self-report. An attempt was made to validate drug usage by urineresults, but incomplete data were obtained because of difficultiesarising when the interviews were conducted in the clients’ homes orin prisons, rather than in the clinic setting. Where urine sampleswere available, these were generally consistent with the subjects’self-report. In any case, attempts to compare self-reports of drugusers and analysis of urine at the time of assessment may be oflimited value, since a single urine screen only provides informationabout drug use in the previous twenty-four hours. A positive urinesample in someone claiming to be drug-free would show that thesubject was lying, but in others would be of little use. The only reli-able assessment of frequency of drug use would be a continuousdaily urine screen over an extended period of time, which wasimpractical in the context of this study. Given the nature of thepopulation under study, the self-report of the frequency of drug useis bound to contain inaccuracies. The question is whether distor-tions arising out of self-reports of drug use are likely to vary betweenthe treatment groups. While we have no evidence for this, the possi-bility cannot be discounted.
The overall significance of the results also has to be viewed withsome caution due to the relatively high attrition rate from the study,with 85 per cent of subjects seen at six months but only 70 per centat twelve months. The number of subjects traced was similar for allgroups at six months but at twelve months there were differencesbetween the three treatment groups. The highest number ofsubjects was traced in the family therapy group and the fewest in thestandard treatment group. These differences make comparisonsbetween the treatment groups and changes within each group moredifficult to evaluate. The assumption that those who were not tracedor were imprisoned were using as frequently as at the start of thestudy may be erring on the conservative side (but, given the nature
Family therapy in the treatment of opiate users 415
2002 The Association for Family Therapy and Systemic Practice
of the subject population, it is likely to give a more accurate picturethan excluding them from the analysis) and on the face of it couldhave marginally favoured the family therapy group. The data analy-ses using only subjects with complete assessment data support theconclusion that the differences between treatments were notunduly affected by this assumption. It is therefore probably safe toconclude that the more favourable result for the group that hadreceived family therapy is a reliable one.
Finally, a word of caution is needed concerning the overall size ofthe sample. While the main comparisons between the three treat-ments are fairly robust, when the results are broken down further(e.g. when considering interactions between type of treatment andfamily configuration or the comparisons of outcome broken down bygender and drug use in the couple) the numbers are small, and anyconclusions drawn from these findings can be only very tentative.
Overall the study showed that 12 per cent of clients stopped usingdrugs at six months and tended to maintain their progress at twelvemonths. This is similar to other studies with the exception ofGossop’s (1987) study, in which an unusually successful outcomefollowed inpatient treatment. The 8 per cent drug-free at twelvemonths in the study is similar to the 10 per cent drug-free subjectsat one year reported by Vaillant (1973), and approximately 7 percent in Oppenheimer and Stimson (1982) at one year (rising tomore than 30 per cent over seven years). Oppenheimer andStimson (1982) excluded subjects who had died, were imprisonedor whose drug use was uncertain, so the analysis of outcome atseven years involved 79 per cent of the original sample, although 97per cent had been traced. The likely effect of excluding this groupof subjects is to make the results appear more favourable than wasin fact the case.
At each of the assessments the subjects who were opiate-freeshowed consistent improvement in depression scores and, to a lesserextent, in anxiety scores, in association with overall improvement insocial functioning. The study shows that employment at the initialassessment was a predictor of good outcome. It was unclear whetherthe other positive prognostic indicators (not sharing needles andnot injecting) were secondary to the employment status or indepen-dent factors, as those who share needles may also be moreentrenched in a drug-using subculture. These findings may haveimplications for treatment in that employed drug users are perhapsmore likely to benefit from short-term outpatient treatment,
416 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice

whereas unemployed drug users may require more intensive orlonger term treatment including inpatient detoxification.
Despite the clinically based predictions, different family configu-rations appeared to have little effect on outcome, though there maybe a differential effect depending on the type of treatment. Thefindings with respect to the gender of the subjects were interestingand have not been reported elsewhere. Females in a two-usercouple relationship had a relatively good outcome, in contrast withfemales who were not involved in such a relationship. Females werevery rarely the sole drug user in a relationship. A possible explana-tion for this may be that women were more likely to become secon-darily involved with drugs, having formed a relationship with a druguser. Anecdotally in this population, it also seemed that drug-usingwomen were more likely to be ejected from their family of origin, incontrast with male subjects who remained involved with and depen-dent on their families of origin despite their drug use.
There is one further important aspect of the study that has to beconsidered when evaluating the overall results. Recent research hasshown that methadone withdrawal, a core treatment used for allthree groups in our study, may be less effective than methadonemaintenance in reducing illicit drug use and improving psychoso-cial functioning (Gerstein, 1992; Gossop et al., 2001). The length oftreatment, between six and twelve months for the low-contact andfamily therapy groups and twelve months for most of the standardclinic treatment, was short. The initial dose of methadone (mean =40mg) was also low. In Gerstein’s review (1992), good outcome wasassociated with long-term treatment and higher doses ofmethadone (a minimum of 60mg). It could be argued that a morepowerful methadone treatment (i.e. a higher dosage and/or longerterm treatment) would have provided a stronger baseline outcomefor all three groups against which the additional benefits of thespecific treatments could be compared.
The main focus of the study was the comparison of family ther-apy with two control treatments. While the differences in outcomebetween the three treatments were modest, there was neverthelessa consistent pattern favouring those who were treated with familytherapy. This was particularly true for those subjects who were livingwith a partner, whether this partner was a drug user or a non-user.The advantage of involving the family in treatment was less clear forthose subjects who were still living with their families of origin butthe numbers in this subsample were the smallest, and this finding
Family therapy in the treatment of opiate users 417
2002 The Association for Family Therapy and Systemic Practice

has to be treated with caution. Surprisingly, of the two control treat-ments, the standard clinic treatment achieved the worst outcome,with the low-contact group showing intermediate results.
Other differences were also found between the treatment groupsin terms of utilization of treatment facilities. The majority of thefamily therapy group and of the low-contact group completed treat-ment within six months and both groups required significantlyfewer sessions than with the standard treatment. The improvementsfound at six months in these two treatment groups were generallymaintained at one year without further treatment. The standardclinic treatment group, which underwent a longer period of treat-ment and attended for a higher number of appointments, showeda lower abstinence rate and more subjects were lost to subsequentassessments. It is possible that the subjects continuing in this treat-ment longer than the interim assessment period of one year mightdo better in the long term (Gerstein, 1992). Because of the shortinterim assessment period it is not possible, at this stage, toconclude that length of treatment is not a major factor in deter-mining the eventual outcome. The low-contact group provides aninteresting comparison, being intermediate in its outcome resultsand in the degree of co-operation with both six- and twelve-monthassessments. It was a more structured, limited approach than thestandard treatment and did not encourage dependency on the ther-apist and, similar to the family therapy treatment group, used anon-negotiable methadone reduction regime. The encouragementof the use of self-help groups in the low-contact group may also haveenhanced the results of what might otherwise be considered theweakest form of treatment.
The less structured, open-ended nature of the standard clinictreatment and the flexibility of the pace of methadone reductionmeant that the subjects in this group experienced a different rela-tionship with their therapist, could control the treatment more, andpossibly experienced less anxiety and pressure to alter drug usewithin a fixed time frame. The counsellors delivering the treatmentin this group had varied levels of therapeutic training (although allof them had considerable experience of working in the drug addic-tion field) and this may have also influenced the results.
If one accepts that the drug use reported at six- and twelve-month assessments reflected accurate patterns of behaviour, howsuccessful were the different treatments? Strang et al. (1987) havepointed out that total abstinence is not the only criterion for
418 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice

successful treatment and damage limitation is an important goal.Once an individual ceases to use drugs daily and/or can maintainemployment and a stable, non-criminal lifestyle, the problems ofdrug use are significantly reduced. Our study suggests that this wasmost likely to happen for subjects who received family therapy ofwhom just under half were either abstinent or at least not usingdaily. In the standard clinic treatment only 13 per cent of subjectsachieved this, although they were maintained in treatment longer.
Implications for clinical practice
Comparative treatment studies are often presented as if the princi-pal question that needs answering is ‘Which is the best treat-ment/best theoretical model/best aetiological explanation’? Afinding, that one treatment is more effective than others, is thenused as an argument that this is the treatment of choice and thatother treatments should be relegated to ‘second line’ or ‘adjunc-tive treatment’ status. The implication is that the treatment ofchoice should be the one that deals with the core dysfunction,while the role of the other treatments is to help resolve some of theassociated problems. While few people would openly argue forsuch a simplistic view, this is at least a subtext for many discussionsabout the value of different treatments. Indeed, we ourselves havepresented the results of our study as if the main implication wasthat family therapy should be the favoured treatment. Similarly,non-family therapists, while perhaps recognizing that family ther-apy has a useful role to play, are more likely to view it as an ‘adjunc-tive treatment’ aimed particularly at changing dysfunctional familypatterns.
In our clinical experience, however, the best treatment results areusually obtained from a combination of treatments which is notonly a way of addressing different aspects of the problem but canalso maximize the strength of each specific treatment. Viewed inthis way, family therapy is best understood not as the main treat-ment or as a treatment to be used alongside other treatments butrather as an approach that works best when it is integrated withother aspects of treatment. We have no evidence to propose that themain aim of the family interventions should be to change the struc-ture or the dynamics of the family (although this may also takeplace in some cases). It is probably more useful to think of familytherapy as a way of helping the family to examine how they may be
Family therapy in the treatment of opiate users 419
2002 The Association for Family Therapy and Systemic Practice

involved in finding ways of dealing with the different problems withwhich both the user and the family have to contend.
One of the difficulties in involving families in treatment (particu-larly with adult clients) is that they often feel that the reason theyare being asked to sessions is that they are seen as the cause of theproblem. It is important therefore to emphasize that the aim ofinvolving them in the therapy is to explore how they can help.This is likely to include discussions of how the whole family hasbecome affected by the drug addiction, which often becomes thecentral organizing factor around which much of family liferevolves. Helping family members to disentangle themselves fromthis can assist them in using their resources to fight the addictionthat has invaded their lives. Other aspects of the treatment (suchas methadone reduction or methadone maintenance) becomepart of this conversation but do not necessarily have a centralfocus.
The discussion with the family will aim to widen the choicesaround both the drug-taking behaviour and also the family’sresponse to it. The family will need to consider the implications ofthe different choices. ‘How will things change if your partner isgoing to be using methadone on a regular basis for a considerablelength of time?; ‘How are you going to make sure that normal every-day disagreements are not covered up by arguments about drugs?’;‘How will your relationship be affected (positively and negatively) asreliance on drug use diminishes?’; ‘What are the problems that youmight have to deal with when there are no drugs in your life?’;‘What will the drug user and other members of the family doinstead, now that drug use is not their central concern?’; ‘Is it theuser’s responsibility alone for stopping, and if he decides to stop (ornot to stop), how will you deal with this?’. In all these examples theprimary aim of the therapy is to help family members to gain a newperspective on how they address problems in their life in termswhich are wider than drug use alone.
Conclusions
This study adds to the evidence for the value of including the familyin the treatment of adult opiate users. Positive results were achievedwith a relatively small number of sessions with the couple or familyin comparison to the standard treatment. While family therapy onits own is unlikely to provide a way out of drug-taking for most
420 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice

opiate users there is now compelling evidence that it should be usedroutinely as a significant component of the overall treatment pack-age in drug addiction.
ReferencesBean, P. (1971) Social aspects of drug abuse: a criminological study of a group of
London drug offenders. Journal of Criminal Law, Criminology and Police Science, 62:80–86.
Borduin, C., Mann, B., Cone, L. and Heggeler, S. (1995) Multisystemic treatmentof serious juvenile offenders: long-term prevention of criminality and violence.Journal of Consulting and Clinical Psychology, 63: 569–578.
Carr, A. (2000a) Evidence-based practice in family therapy and systemic consulta-tion. II Adult-focused problems. Journal of Family Therapy, 22: 273–295.
Carr, A. (2000b) Evidence-based practice in family therapy and systemic consulta-tion. I Child focused problems. Journal of Family Therapy, 22: 29–60.
Cormack, C. and Carr, A. (2000) Drug abuse. In A. Carr (ed.), What Works forChildren and Adolescents? A Critical Review of Psychological Interventions withChildren, Adolescents and their Families. London: Routledge.
Crawley, J.A. (1971) A case note study of 134 out-patient drug addicts over a 17-month period. British Journal of Addiction, 66: 209–218.
Del Orto, A. ( 1974) The role and resources of the family during the rehabilitationprocess. Journal of Psychedelic Drugs, 6: 435–445.
Gerstein, G.R. (1992) The effectiveness of drug treatment. In C.P. O’Brien andJ.H. Jaffe (eds), Addictive States. New York: Rave.
Gossop, M., Green, L., Phillips, G. and Bradley, B. (1987) What happens to opiumaddicts immediately after treatment: a prospective follow-up study. BritishMedical Journal, 294: 1377–1380.
Gossop, M., Marsden, J., Stewart, D. and Treacey, S. (2001) Outcomes aftermethadone maintenance and methadone reduction treatments: two-yearfollow-up results from the National Treatment Outcome Research Study. Drugand Alcohol Dependence, 62: 255–264.
Haley, J. (1980) Leaving Home: Therapy with Disturbed Young People. New York:McGraw-Hill.
Harbin, H.T. and Maziar, H.M. (1975) The families of drug abusers: a literaturereview. Family Process, 14: 411–431.
Hengeller, S.W., Borduin, C.M., Melton, G.B., Mann, B.J., Smith, L.A., Hall, J.A.,Cone, L. and Fucci, B.R. (1991) Effects of multi-systemic therapy on drug useand abuse in serious juvenile offenders: a progress report from two outcomestudies. Family Dynamics Addictions Quarterly, 1: 40–51.
Joanning, H., Thomas, F., Quin, W. and Mullen, R. (1992) Treating adolescentdrug abuse: a comparison of family systems therapy, group therapy and familyeducation. Journal of Marital and Family Therapy, 18: 345–356.
Kaufman, E. (1985) Family systems and family therapy for substance abuse: anoverview of two decades of research and clinical experience. The InternationalJournal of Addiction, 20: 897–916.
Lewis, R.A., Piercy, F.P., Sprenkle, D.H. and Trepper, T.S. (1990) Family based
Family therapy in the treatment of opiate users 421
2002 The Association for Family Therapy and Systemic Practice

interventions for helping drug abusing adolescents. Journal of Adolescent Research,5: 82–95.
Liddle, H.A. (1995) Efficacy of family therapy for drug abuse: promising but notdefinitive. Journal of Marital and Family Therapy, 4: 511–543.
McLellan, A.T., Luborsky, L., Woody, G.E. and O’Brien, C.P. (1980) An improveddiagnostic evaluation instrument for substance abuse patients: the AddictionSeverity Index. Journal of Nervous and Mental Disease, 168: 26–33.
Madanes, C., Dukes, J. and Harbin, H. (1980) Family ties of heroin addicts. Archivesof General Psychiatry, 37: 889–894.
Montgomery, S.A. and Asberg, M. (1979) A new depression scale designed to besensitive to change. British Journal of Psychiatry, 134: 382–389.
Oppenheimer, E. and Stimson, G.V. (1982) Seven year follow-up of heroin addicts:life histories summarised. Drug & Alcohol Dependence, 9: 153–159.
Stanton, M.D. and Shaddish, W.R. (1997) Outcome, attrition and family-coupletreatment for drug abuse: a meta-analysis and review of the controlled, compar-ative studies. Psychological Bulletin, 12: 170–191.
Stanton, M.D., Todd, T. and Associates (1982) The Family Therapy of Drug Abuse andAddiction. New York and London: Guilford Press.
StatSoft Inc (1999) STATISTICA for Windows. Tulsa, OK: StatSoft Inc WEB:<http://www.statsoft.com>.
Stimson, G.V. and Oppenheimer, E. (1982) Heroin Addiction, Treatment and Controlin Britain. London: Tavistock.
Strang, J., Heathcote, S. and Watson, P. (1987) Habit moderation in injecting drugaddicts. Health Trends, 19: 16–18.
Szapocznik, J., Kurtinez, W.M., Foote, F.H., Perez-Vidal, A. and Hervis, O. (1983)Conjoint versus one-person family therapy: some evidence for the effectivenessof conducting family therapy through one person. Journal of Consulting andClinical Psychology, 51: 889–899.
Szapocznik, J., Kurtinez, W.M., Foote, F.H., Perez-Vidal, A. and Hervis, O. (1986)Conjoint versus one-person family therapy: further evidence for the effective-ness of conducting family therapy through one person with drug-abusingadolescents. Journal of Consulting and Clinical Psychology, 54: 395–397.
Szapocznik, J., Perez-Vidal, A., Brickman, A.L., Foote, F.H., Santiesteban, D.,Hervis, O. and Kurtinez, W.M. (1988) Engaging adolescent drug abusers andtheir families in treatment: a strategic structural systems approach. Journal ofConsulting and Clinical Psychology, 56: 552–557.
Tyrer, P.J., Owen, R.T. and Cicchetti, D.V. (1984) The brief scale for anxiety: asubdivision of the comprehensive psychopathological rating scale. Journal ofNeurology, Neurosurgery & Psychiatry, 9: 970–975.
Vaillant, G.E. (1966) A 12 year follow-up of New York narcotic addicts. III. Somesocial and psychiatric characteristics. Archives of General Psychiatry, 15: 599–609.
Vaillant, G.E. (1973) A twenty-year follow-up of New York narcotic addicts. Archivesof General Psychiatry, 29: 237–241.
422 Dennis Yandoli et al.
2002 The Association for Family Therapy and Systemic Practice