Embed Size (px)
Citation preview

Accepted Manuscript
A clinical test of lumbopelvic control: Development and reliability of a clinical test ofdissociation of lumbopelvic and thoracolumbar motion
Edith Elgueta-Cancino, PT Siobhan Schabrun, BPhysio(Hons), PhD Lieven Danneels,PhD Paul Hodges, BPhty(Hons), PhD
PII: S1356-689X(14)00043-5
DOI: 10.1016/j.math.2014.03.009
Reference: YMATH 1545
To appear in: Manual Therapy
Received Date: 17 December 2013
Revised Date: 19 March 2014
Accepted Date: 21 March 2014
Please cite this article as: Elgueta-Cancino E, Schabrun S, Danneels L, Hodges P, A clinical test oflumbopelvic control: Development and reliability of a clinical test of dissociation of lumbopelvic andthoracolumbar motion, Manual Therapy (2014), doi: 10.1016/j.math.2014.03.009.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
A clinical test of lumbopelvic control: Development and reliability of a
clinical test of dissociation of lumbopelvic and thoracolumbar motion
1Edith Elgueta-Cancino (PT), 1Siobhan Schabrun, (BPhysio(Hons), PhD), 2Lieven
Danneels, (PT, PhD), 1Paul Hodges (BPhty(Hons), PhD)
1. The University of Queensland, Centre of Clinical Research Excellence in Spinal Pain,
Injury and Health, Brisbane, Queensland, Australia.
2. Ghent University, Department of Rehabilitation Sciences and Physiotherapy, Ghent,
Belgium.
Ethical review:
Approved by the Medical Research Ethics Committee of the University of Queensland.
Corresponding author:
Dr Paul Hodges
School of Health & Rehabilitation Sciences,
The University of Queensland, QLD 4072, Australia
phone: +61 7 3365 2008
e-mail: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
A clinical test of lumbopelvic control: Development and reliability of a clinical test
of dissociation of lumbopelvic and thoracolumbar motion

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Abstract 1
LBP is often associated with changes in motor control. Some subgroups of LBP have been 2
argued to have a compromised ability to dissociate lumbopelvic movement from that of the 3
thoracolumbar junction. Clinical methods to evaluate this task may aid identification of this LBP 4
subgroup and determine the utility of this information to guide clinical interventions. The study aimed 5
to develop a clinical test to assess the ability to dissociate lumbopelvic movement from that of the 6
thoracolumbar junction, and to evaluate the inter-rater reliability of the test in individuals with and 7
without low back pain (LBP) when performed by experienced and novice therapists. A clinical scale 8
was developed to characterise quality of performance of lumbopelvic motion with limited motion at the 9
thoracolumbar junction. Inter-tester repeatability was measured in three experiments. Test outcomes for 10
pain-free controls were compared between three assessors with different amounts of clinical 11
experience. Test scores for LBP participants were compared between two assessors, and between 12
assessments undertaken from video recordings. Agreement between assessors was tested with weighted 13
Kappa Coefficient. The test had acceptable reliability in pain-free and LBP participants, but was better 14
when undertaken by experienced therapists. Kappa index ranged from 0.81-0.66 for live assessments, 15
and 0.62 for video assessments. The results showed that the test is reliable when performed by 16
experienced assessors. The test can assess thoracolumbar movements in different groups of individuals. 17

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Introduction 18
Individuals with persistent low back pain (LBP) exhibit changes in motor behaviour. These 19
include changes in posture (Claus et al., 2009; Consmuller et al., 2012; Dankaerts et al., 2006b; Roussouly et 20
al., 2005), muscle activation (Dankaerts et al., 2006a; van Dieën et al., 2003), and movement (MacDonald et 21
al., 2009; Mok et al., 2011; Scholtes et al., 2009; Wong & Lee, 2004). Such changes have been used as a 22
basis to identify homogeneous subgroups within the heterogeneous LBP population (Dankaerts & 23
O'Sullivan, 2011; Dankaerts et al., 2007; Dankaerts et al., 2009; Fersum et al., 2009; Harris-Hayes & Van 24
Dillen, 2009). However, examination of motor behaviour often requires sophisticated laboratory tests 25
that have limited utility in clinical practice. A critical step forward is the development of clinically 26
viable methods to identify changes in motor behaviour in LBP. 27
Altered motor coordination of thoracic, lumbar, and pelvic segments is a feature of motor 28
behaviour discussed in the clinical literature and studied using laboratory-based investigations. Specific 29
subgroups of individuals with LBP have been identified to have: poor ability to dissociate movement of 30
the lumbopelvic region spine from that of the thorax (poor intersegmental coordination) (Wallwork et al., 31
2009); poor capacity to voluntarily maintain a lumbar lordosis (Danneels et al., 2002); compromised 32
control of the multifidus muscle (Freeman et al., 2010; MacDonald et al., 2009; Nelson-Wong & Callaghan, 33
2010); and “smudging” of the separate regions of the motor cortex involved in the activation of 34
short/deep and long/superficial muscles of the back which are responsible for coordinated motion of 35
these segments (Tsao et al., 2011). Although related, it has not been confirmed that all of these features 36
are present in the same individuals. Altered control of this aspect of motor behaviour may be relevant 37
for spine loading and characterise a specific LBP subgroup, but no clinical tools are available to 38
reliably measure dissociation of lumbopelvic from thoracic motion. Clinical methods are necessary to 39

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
enable wider evaluation of this movement behaviour in a broad LBP population, and to determine the 40
utility of this information to guide clinical interventions. 41
This study aimed to: (i) develop a clinical test to assess the ability to dissociate lumbopelvic 42
motion from that of the thoracolumbar junction; and (ii) evaluate the reliability of the test in individuals 43
with and without LBP when performed by experienced and novice therapists. 44
45
Methods 46
Study design 47
The study was divided into a test-development phase and three experiments. The test-48
development phase involved development and refinement of criteria to quantify movement 49
performance, and design of a standardised video to instruct participants for the movement task. The 50
first experiment investigated the inter-rater reliability of the clinical test when applied to healthy 51
participants and compared the ratings of three assessors; two with at least 1-year of clinical 52
physiotherapy experience and one novice physiotherapist (a new graduate with limited clinical 53
experience). The second experiment assessed the inter-rater reliability (two experienced assessors) in 54
patients with persistent LBP. A third experiment studied the inter-rater reliability (two experienced 55
assessors) of the test when assessments were undertaken from video recordings in the same group of 56
patients. 57
Test-Development 58
The development of the test involved a combination of judgmental and consensus opinion 59
methodology. The initial judgmental approach involved development of the criteria by the investigators on 60
the basis of an extensive literature review of the topic and through observation of patients with back pain. 61

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
This test was then refined using a consensus opinion method in which a panel of expert clinicians was 62
involved in testing and commenting on the appropriateness of the criteria and scoring descriptions. The 63
expert clinicians (n=3) involved in this phase were all experienced with rehabilitation of patients with back 64
pain. 65
Rating Scale 66
The “Clinical test of thoracolumbar dissociation” was devised to assess a patient’s ability to 67
perform anterior/posterior pelvic tilt in sitting while attempting to maintain a constant position of the 68
thorax/thoracolumbar junction. The rating scale of the test was structured with five criteria with a 69
maximum score of 10. Each criterion represented descriptive characteristics of a specific movement 70
feature. Assessors provided a numeric value, based on a criterion referenced assessment, as a measure 71
of the quality of movement performance using characteristics such as; muscle activity, timing and 72
coordination (Table1, Fig. 1). Criteria were arranged such that the assessor first focused attention to 73
lumbopelvic movement. The second focus was motion and muscle activity of adjacent regions, 74
including consideration of the ability of the participant to move the lumbopelvic region relatively 75
independently from the thoracolumbar junction. A final focus included more global features of 76
movement performance including; (i) consideration of whether the task could be performed with equal 77
quality between movement directions (anterior and posterior pelvic tilt), (ii) the ability to maintain 78
movement quality with repetition, and (iii) the ability to maintain breathing. 79
Process for test refinement 80
During the consensus opinion phase the panel of expert clinicians piloted the test and provided 81
feedback. This resulted in refinement of the wording of the criteria and the assessment sequence. 82
Factors considered in refinement of the test were that: (i) criteria should create a fluid and logical order 83

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
of assessment; (ii) discrimination of the quality of the movement during the test should be expressed as 84
a positive concept with different levels of performance, and (iii) language should be intuitive and non-85
ambiguous. This process resulted in modification of descriptions that were considered to be ambiguous, 86
addition of words to add clarity. 87
Test performance 88
Performance of the test was evaluated in two steps. The first evaluation was undertaken after 89
viewing standardised instruction video, and the second after a two minute individualised training session 90
with specific feedback of features that required correction to improve the performance of the task.. 91
Standardised video instructions: Instructions for each participant were standardised using a 92
video that contained; (i) written and verbal instructions of the task “tilt the pelvis forwards and 93
backwards in the sitting position”, (ii) demonstration of the movement by a model, and (iii) instruction 94
to perform 10 repetitions. After this training the assessor rated the performance. 95
Individualised training: Participants received a two-minute session of standardised feedback 96
or training to improve performance by a single trained experimenter (physiotherapist). To standardize 97
and optimise the learning process a list of “training strategies” was created. This guide indicated 98
training methods that could be used to improve task performance based on errors identified in the initial 99
assessment. Techniques included training of postural alignment in sitting, standing or four point 100
kneeling, manual guidance of pelvic tilt, guidance to correct alignment of the pelvis, and feedback to 101
avoid excessive muscle activity. Performance was reassessed after the completion of the two minutes of 102
training. 103

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Experiment 1: Inter-tester reliability – Healthy controls 104
Participants: Eleven healthy individuals with no history of low back or pelvic pain (27[3] 105
years (mean [standard deviation]); 6 males, 5 females) were recruited. Participants were excluded if 106
they had suspected or confirmed spinal pathology, pregnancy, nerve root compromise, and previous 107
spinal surgery, or major surgery scheduled. The institutional Medical Research Ethics Committee 108
approved the study and all participants provided written, informed consent. 109
Assessors: Three independent assessors, one with postgraduate training in manual therapy (R1), 110
one working in clinical practice (R2, >1-year of clinical experience), and a novice new graduate 111
physiotherapist with limited clinical experience (R3) were trained to perform the assessment. Training 112
involved: (i) explanation and discussion of the criteria; (ii) familiarization with key concepts and 113
definitions, (iii) guided assessment of the test in pilot subjects, and (iv) review and discussion of the 114
rating of several individuals. 115
Procedure: The assessment was performed in one session for each participant. Each session 116
was divided into three phases: (i) pre-training assessment – basic training of the movement task 117
provided using the video and performance simultaneously assessed by 3 assessors; (ii) training - 2-118
minutes of standardised training provided by the experimenter based on the standardised training 119
strategies; and (iii) post-training assessment – same procedure as the pre-training assessment. 120
Participants sat on a chair adjusted to 110% of the height of fibula head with the hands relaxed 121
on the thighs, eyes open and looking forward to a screen. The back was exposed and the participant 122
wore shorts that did not restrict hip motion. 123
The test was performed once (ten repetitions of the test movement) with all assessors able to 124
evaluate the same participant at the same time. Assessors rated the participant’s best performance, 125
without interaction. The best performance was defined as the highest score that could be awarded based 126

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
on the assessed repetitions. Assessors were allowed and encouraged to palpate the participant to clarify 127
observations (muscle activation). It was considered necessary for all assessors to evaluate the same 128
performance so that inter-rater reliability could be determined without confounding by differences in 129
performance by the participant. 130
Assessors left the room after pre-training assessment and the experimenter provided 2-minutes 131
of training. All assessors then returned and scored the post-training performance concurrently. 132
Experiment 2: Inter-tester reliability – LBP participants 133
Participants: Twenty individuals with non-specific persistent LBP were recruited (31[9] years, 6 134
males, 14 females). Participants were excluded if they had suspected or confirmed spinal pathology of 135
non-musculoskeletal origin (e.g., tumor, infection, fracture, inflammatory disease), pregnancy, nerve 136
root compromise, or previous spinal surgery. 137
Assessors and Procedure: The experienced assessors from Experiment 1 (R1, R2) assessed the 138
participants as for Experiment 1. 139
Experiment 3: Inter-tester reliability - LBP participants by video assessment 140
Participants: Sixteen individuals with non-specific persistent LBP selected randomly from the 141
sample used in Experiment 2 were videoed from the front, side and back during the task, pre- and post-142
training. A research assistant edited the videos in a blinded manner. Participants were excluded if the 143
movement could not be observed clearly in all three views. Video recordings of ten individuals (28[9] 144
years, 2 males, 8 females) could be included. 145
Assessors and procedure: An experienced assessor (R1) from Experiment 1 and an additional 146
experienced assessor (R4) with postgraduate training in manual therapy participated. Assessors were 147

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
instructed to rate the performance after watching the video only once. They rated the pre-training video, 148
waited 2 minutes, and then rate the post-training performance to mimic the clinical situation. 149
Intra-tester reliability 150
Intra-tester reliability was assessed using the data for assessor R1. It was considered that 151
assessment of intra-tester reliability would be confounded by improvement in performance of the 152
participant after training. For this reason intra-tester reliability was assessed by comparison of the scores 153
provided by a single assessor on separate days, but with one assessment performed as a live assessment, 154
and the second assessment as a video assessment of the exact same performance by the participant. This 155
was achieved by using the data from assessor R1 in Experiments 2 and 3. 156
Statistical Analyses 157
Inter-rater reliability was assessed in two ways: general analysis of the total score, and detailed 158
analysis of each criterion separately. For both analysis the scores (total and each criterion) of the test 159
pre-training and post-training were compared between each combination of assessor pairs (R1 vs. R2; 160
R1 vs. R3; R2 vs. R3) using the weighted Cohen's Kappa Coefficient. This method measures the 161
agreement between assessors for categorical/ordinal data. Values of this index (k) range from 0 (no 162
agreement) to 1 (100% agreement) or -1 (100% disagreement) and the strength of agreement has been 163
defined by Landis and Koch (Landis & Koch) and Sim and Wright (Sim & Wright, 2005) (see Table 2). 164
Analyses were performed with a confidence interval (CI) of 95%. 165
166

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Results 167
Inter-tester reliability – Healthy controls 168
The repeatability of the total scores revealed good agreement between assessors but differences 169
in the level of agreement between pairs of assessors based on experience and between measures made 170
before- and after-training. For pre-training measures the inter-rater agreement between R1 and R2 was 171
“almost perfect/very good”, but was less (“substantial/good”) for comparison between experienced 172
assessors (R1 and R2) and the less experienced assessor (R3) (Table 3). Agreement between assessors 173
was less after 2 minutes training. Agreement between R1 and R2, and R1 and R3 was “substantial” but 174
only “moderate” between R2 and R3 (Table 3). 175
Analysis of inter-rater reliability for each criterion revealed higher variability, but with the same 176
tendency for less reliable post-training measures and lower agreement with the less experienced 177
assessor. “Breathing”, was scored identically by all assessors at both measurement times. In the pre-178
training measures, all criteria showed at least a “moderate” level of agreement for the assessor with 179
postgraduate training (R1) and the other two assessors (R2 and R3) (Table 4). For the post-training 180
measures “moderate” agreement was only achieved for the experienced assessors (R1 and R2). 181
Inter-rater reliability – LBP participants 182
Analysis of total scores for LBP participants demonstrated “substantial/good” inter-rater 183
reliability in the pre-training phase and “moderate” agreement in the post-training phase (Table 3). 184
Analysis of individual criteria showed lower agreement for pre- and post-training assessments. 185
Three criteria had “moderate” to “very good” agreement in the pre-training phase, but higher variability 186
in the post-training phase (Table 4). “Breathing” was scored with perfectly agreement between 187
assessors. 188

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Inter-rater reliability – LBP participants by video assessment 189
Inter-rater reliability of the total scores from video analysis revealed that assessment remains 190
reliable with a “substantial” agreement in pre-training and “moderate” agreement post-training (Table 191
3). Analysis of each criterion demonstrated at least a “moderate” agreement in four of five criteria. 192
Again “breathing” was perfectly scored. This was also apparent for Criterion 2 (control of adjacent 193
regions) in the pre-training phase and Criterion 5 (repetition) in the post-training phase. One criterion 194
(Criterion 3 (performance in opposite directions)) was less reliable, with “slight” and “poor” levels of 195
agreement pre- and post-training, respectively (Table 4). 196
Intra-tester reliability 197
The intra-tester reliability of the total scores of R1 from LBP participants in vivo and video 198
analysis revealed a “substantial” and “moderate” agreement between scores provided pre-training and 199
post-training, respectively (Table 5). 200
201
Discussion 202
The results demonstrate that the “Clinical test of thoracolumbar dissociation” has acceptable 203
inter-rater reliability when used by trained physiotherapists. Although the agreement between assessors 204
was acceptable, it depended on the assessor’s experience and the degree of task training. Agreement 205
between assessors was better when participants’ performance was judged after minimal instruction than 206
after the training period. The reliability was also acceptable, although with marginally less agreement, 207
for participants with LBP, even when the test was undertaken using video recordings of movement. 208
These data confirm the potential utility of this test in clinical evaluation of patients with LBP. 209

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Intra and inter-rater reliability of the “Clinical test of thoracolumbar dissociation” 210
The total test score had good reliability between sessions for a single trained assessor, and 211
between assessors, but with some variation between criteria. This latter observation could be explained 212
by differences in the components evaluated in each criterion. For instance, Criterion 4, which assesses 213
breathing, had a perfect agreement. This criterion is rated as a dichotomous “yes” or “no” pertaining to 214
the ability to breathe during the movement, which is relatively straightforward to assess. High 215
agreement was also identified for Criteria 1 and 2, which describe key movement components of the 216
test and are defined by detailed criteria that are assessed from the “best” performance of the task. In 217
contrast, agreement between assessors was lower for Criteria 3 and 5 (healthy control – “moderate”; 218
LBP – “slight” – “poor”), which assess differences in the performance of the task between directions of 219
movement (i.e. anterior and posterior pelvic tile) and consistency of the ability to perform the task with 220
repetition. Greater difficulty with assessment of these criteria might reflect subjectivity of assessment 221
of features that rely on relative quality between directions/repetitions. In addition, the determination of 222
quality of performance in these criteria involves consideration of multiple components including 223
movement features and muscle activation that are separately assessed in Criteria 1 and 2. 224
Greater reliability for experienced assessors 225
Our data show a “high” level of agreement (Landis et al.; Sim et al., 2005) between assessors who 226
have several years of clinical experience and less agreement between assessors when one is a novice 227
clinician. This concurs with data from other studies (Alqarni, 2011; Dankaerts et al., 2011; Dankaerts et al., 228
2006b; Dankaerts et al., 2006c; Luomajoki et al., 2007; 2008; Tidstrand & Horneij, 2009; Van Dillen et al., 229
1998) and the conclusion of a recent systematic review that identified assessor experience as a key 230
factor in determination of reliability and minimization of the risk of bias for clinical assessments of 231

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
movement control in LBP (Alqarni, 2011; Carlsson & Rasmussen-Barr, 2013). Our study supports this 232
observation and indicates that the reliability of the “Clinical test of thoracolumbar dissociation” 233
depends on the experience/skill of the assessors. Although some studies suggest experience is not 234
important, this is generally identified for tests that rely on simple criteria that involve limited clinical 235
judgment such as examination forms and videoed assessments (Fritz et al., 2000) 236
Assessment can be biased by training of the task 237
The two minutes of standardized training appears to have differentially biased the observations 238
of the assessors. This is evidenced by greater agreement between assessors for assessment conducted 239
after the video training than for the second assessment after training by the therapist. This cannot be 240
explained by differences in task performance as the assessors examined patients concurrently. The 241
difference in rating after training indicates additional factors influenced the assessor’s judgment. There 242
are several possibilities. First, assessors may have been influenced by an expectation of improved 243
performance after training. Some assessors may have rated performance poorer if they expected greater 244
improvement from training. Second, recollection of the pre-training assessment and subsequent 245
comparison with the post-training performance may have affected the rating. The 2-minute period 246
between assessments is unlikely to prevent assessors being influenced by their initial assessment. Other 247
studies have included a 15 minute “washout” period and reported this time period to be sufficient to 248
reduce the influence on the assessment (Dankaerts et al., 2011). 249
Reduced agreement (change of Kappa value to a lower category of strength of agreement or 250
lower Kappa value with in a strength of agreement category) after training was limited to Criterion 3 251
(ability to perform the task in opposite directions) for healthy controls. For LBP participants, agreement 252
between assessors and between sessions for a single assessor declined for both Criteria 3 and 5 after 253

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
training. As indicated above, these scores involve assignment of a score on the basis of comparison of 254
performance between movement directions, and the maintenance of quality of performance between 255
repetitions. Different assessors not only score individuals differently on these items, but agreement on 256
these items declined after training. As these features require reflection of performance over a number of 257
repetitions and require some qualitative judgement, they may be influenced to a greater degree by the 258
expectation of the assessor, and this may differ between assessors and between patients. Alternatively, 259
it is possible that although training improved performance, variation between repetitions increased as 260
participants trialled various methods they had been taught to optimize task performance. This may have 261
been expressed as an initial deterioration of performance. As people with LBP have less precise control 262
of movement (Willigenburg et al., 2013) the attempt to voluntarily correct or improve movement based 263
on learning of a new task could have led to disorganization of the movement as they attempted to 264
modify their established pattern. Previous studies have shown that specific training of voluntary actions 265
and skills change motor patterns (Adkins et al., 2005; Laird et al., 2012; Perez et al., 2004) of muscle 266
coordination (Jensen, 2005; van Dieën et al., 2003) even after a short period of training time (Tsao et al., 267
2010). However, the short duration of practice is unlikely to be sufficient to change behaviour and the 268
mode of training might have interfered with the initial performance, as has been shown for some 269
training paradigms (Shea & Morgan, 1979). Reliability could be improved in future by; (i) use of only 270
the pre-training measure, (ii) provision of a longer period between assessments, (iii) greater period of 271
training longer to allow performance to stabilise, or (iv) tighter definition of Criteria 3 and 5. 272
Inter-rater reliability for LBP vs. healthy control participants 273
Although inter-rater reliability for both healthy and LBP groups was acceptable, agreement was 274
better for the healthy group. It is possible that worse agreement for the LBP group was the result of 275

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
greater variability in task performance by the participants, leading to different scores by the assessors 276
despite both scoring the performance at the same time. However, other possible explanations require 277
consideration. In this study the assessors knew that the participants had LBP and this may have biased 278
assessment in a differential manner. Perhaps some therapists rated LBP participants differently if they 279
“expected” the performance to be better or worse rather than attributing a rating purely based on 280
observation. In some ways this concurs with the observation that agreement was worse after the 2-281
minutes training for the pain-free participants. This implies some potential for differential bias of 282
therapists based on expectation. Despite this possibility, the ratings maintained acceptable reliability, 283
but future use of the test should highlight that this may be possible and assessors should be encouraged 284
to faithfully report the performance without bias. 285
Reliability of video assessments 286
Reliability of many clinical tests has been evaluated using video analysis (Henry, 2013, 287
Luomajoki, 2007). Videoed assessment has advantages as it allows the test to be viewed by multiple 288
assessors, at any time, under identical conditions with a single performance by the participant. A 289
disadvantage is that it may reduce the quality of clinical judgment, as the assessor is not able to interact 290
with the participant. This is important for the clinical test under investigation as one component of the 291
criteria involved the qualification of muscle activity and palpation of muscle could provide useful 292
information. Despite this limitation, agreement between assessors was acceptable. The small reduction 293
in reliability is explained by either the absence of interaction with the participant or because assessors 294
were unable to see the features of the task performance with sufficient detail as a result of the video 295
recording. 296

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Intra-tester reliability 297
Intra-rater reliability is a complex measure for clinical test that incorporate training in their format, 298
as the patient's performance is likely to improve with the training component. So to more purely evaluate 299
the contribution of measurement on different days but without the variation in patient performance we did 300
it by comparison of the measures of the exact same trials but first live and second by video. Even though we 301
expect that there will be some loss of accuracy by the different modes we found good intra-rater reliability, 302
which indicate that test has consistency even when it is used by different approaches. 303
Clinical issues/implications 304
The test described here is the first to assess the ability to dissociate movement of the 305
lumbopelvic region from that of the thoracolumbar region. The reliability of the test confirms it may be 306
used clinically to aid identification of subgroups within the LBP population. Further work is required to 307
determine whether subgrouping based on this test, and subsequent directed treatment, influences 308
clinical outcomes; whether the measure can be changed with treatment; whether the movement pattern 309
relates to other motor control parameters such as muscle activation; and whether the test can 310
discriminate individuals in this subgroup from the healthy population. 311
312
313

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
References 314
Adkins, DL, Boychuk, J, Remple, MS, Kleim, JA. Motor training induces experience-315
specific patterns of plasticity across motor cortex and spinal cord. Journal of 316
Applied Physiology 2005; 101(6): 1776-1782. 317
Alqarni, AM. Clinical Tests to Diagnose Lumbar Segmental Instability: A Systematic 318
Review. Journal of Orthopaedic and Sports Physical Therapy 2011. 319
Carlsson, H, Rasmussen-Barr, E. Clinical screening tests for assessing movement 320
control in non-specific low-back pain. A systematic review of intra- and inter-321
observer reliability studies. Manual therapy 2013; 18(2): 103-110. 322
Claus, AP, Hides, JA, Moseley, GL, Hodges, PW. Is ‘ideal’ sitting posture real?: 323
Measurement of spinal curves in four sitting postures. Manual therapy 2009; 324
14(4): 404-408. 325
Consmuller, T, Rohlmann, A, Weinland, D, Druschel, C, Duda, G, Taylor, W. 326
Comparative evaluation of a novel measurement tool to assess lumbar spine 327
posture and range of motion. European Spine Journal 2012; 21(11): 2170-2180. 328
Dankaerts, W, O'Sullivan, P. The validity of O'Sullivan's classification system (CS) for a 329
sub-group of NS-CLBP with motor control impairment (MCI): Overview of a 330
series of studies and review of the literature. Manual therapy 2011; 16(1): 9-14. 331
Dankaerts, W, O'Sullivan, P, Burnett, A, Straker, L. Altered patterns of superficial trunk 332
muscle activation during sitting in nonspecific chronic low back pain patients: 333
importance of subclassification. Spine 2006a; 31(17): 2017-2023. 334
Dankaerts, W, O'Sullivan, P, Burnett, A, Straker, L. Differences in sitting postures are 335
associated with nonspecific chronic low back pain disorders when patients are 336
subclassified. Spine 2006b; 31(6): 698-704. 337

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
Dankaerts, W, O'Sullivan, P, Burnett, A, Straker, L. The use of a mechanism-based 338
classification system to evaluate and direct management of a patient with non-339
specific chronic low back pain and motor control impairment-a case report. Man 340
Ther 2007; 12: 181 - 191. 341
Dankaerts, W, O'Sullivan, P, Burnett, A, Straker, L, Davey, P, Gupta, R. Discriminating 342
Healthy Controls and Two Clinical Subgroups of Nonspecific Chronic Low 343
Back Pain Patients Using Trunk Muscle Activation and Lumbosacral Kinematics 344
of Postures and Movements A Statistical Classification Model. Spine 2009; 345
34(15): 1610-1618. 346
Dankaerts, W, O'Sullivan, PB, Straker, LM, Burnett, AF, Skouen, JS. The inter-examiner 347
reliability of a classification method for non-specific chronic low back pain 348
patients with motor control impairment. Manual therapy 2006c; 11(1): 28-39. 349
Danneels, LD, Coorevits, PC, Cools, AC, Vanderstraeten, GV, Cambier, DC, Witvrouw, 350
EW, De Cuyper, HDC. Differences in electromyographic activity in the 351
multifidus muscle and the iliocostalis lumborum between healthy subjects and 352
patients with sub-acute and chronic low back pain. European Spine Journal 353
2002; 11(1): 13-19. 354
Fersum, KV, Sullivan, PBO, Kvaringle, A, Skouen, JS. Inter-examiner reliability of a 355
classification system for patients with non-specific low back pain. Manual 356
therapy 2009; 14(5): 555-561. 357
Freeman, M, Woodham, M, Woodham, A. The role of the lumbar multifidus in chronic 358
low back pain: a review. Pm & R 2010; 2(2)): 142 - 146. 359
Fritz, JM, Delitto, A, Vignovic, M, Busse, RG. Interrater reliability of judgments of the 360
centralization phenomenon and status change during movement testing in 361

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
patients with low back pain. Archives of Physical Medicine and Rehabilitation 362
2000; 81(1): 57-61. 363
Harris-Hayes, M, Van Dillen, LR. The Inter-Tester Reliability of Physical Therapists 364
Classifying Low Back Pain Problems Based on the Movement System 365
Impairment Classification System. PM&R 2009; 1(2): 117-126. 366
Henry, SM, Van Dillen, LR, Trombley, AR, Dee, JM, Bunn, JY. Reliability of novice 367
raters in using the movement system impairment approach to classify people 368
with low back pain. Manual therapy 2013; 18(1): 35-40. 369
Jensen, JL. Motor skill training and strength training are associated with different plastic 370
changes in the central nervous system. Journal of Applied Physiology 2005; 371
99(4): 1558-1568. 372
Laird, R, Kent, P, Keating, J. Modifying patterns of movement in people with low back 373
pain -does it help? A systematic review. BMC Musculoskeletal Disorders 2012; 374
13(1): 169. 375
Landis, JR, Koch, GG. The Measurement of Observer Agreement for Categorical Data. 376
Biometrics 1977; 33(1): 159-174. 377
Luomajoki, H, Kool, J, de Bruin, ED, Airaksinen, O. Reliability of movement control 378
tests in the lumbar spine. BMC Musculoskeletal Disorders 2007; 8(1): 90. 379
Luomajoki, H, Kool, J, de Bruin, ED, Airaksinen, O. Movement control tests of the low 380
back; evaluation of the difference between patients with low back pain and 381
healthy controls. BMC Musculoskeletal Disorders 2008; 9(1): 170. 382
MacDonald, D, Moseley, GL, Hodges, PW. Why do some patients keep hurting their 383
back? Evidence of ongoing back muscle dysfunction during remission from 384
recurrent back pain. Pain 2009; 142(3): 183-188. 385

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
Mok, NW, Brauer, SG, Hodges, PW. Changes in Lumbar Movement in People With 386
Low Back Pain Are Related to Compromised Balance. Spine 2011; 36(1): E45-387
E52. 388
Nelson-Wong, E, Callaghan, JP. Is muscle co-activation a predisposing factor for low 389
back pain development during standing? A multifactorial approach for early 390
identification of at-risk individuals. Journal of Electromyography and 391
Kinesiology 2010; 20(2): 256-263. 392
Perez, MA, Lungholt, BKS, Nyborg, K, Nielsen, JB. Motor skill training induces 393
changes in the excitability of the leg cortical area in healthy humans. 394
Experimental Brain Research 2004; 159(2): 197-205. 395
Roussouly, P, Gollogly, S, Berthonnaud, E, Dimnet, J. Classification of the normal 396
variation in the sagittal alignment of the human lumbar spine and pelvis in the 397
standing position. Spine 2005; 30(3): 346-353. 398
Scholtes, SA, Gombatto, SP, Van Dillen, LR. Differences in lumbopelvic motion 399
between people with and people without low back pain during two lower limb 400
movement tests. Clinical Biomechanics 2009; 24(1): 7-12. 401
Shea, JB, Morgan, RL. Contextual Interference Effects on the Acquisition, Retention, 402
and Transfer of a Motor Skill. Journal of Experimental Psychology: Human 403
Learning and Memory 1979; 5(2): 179-87. 404
Sim, J, Wright, CC. The Kappa Statistic in Reliability Studies: Use, Interpretation, and 405
Sample Size Requirements. Physical Therapy 2005; 85(3): 257-268. 406
Tidstrand, J, Horneij, E. Inter-rater reliability of three standardized functional tests in 407
patients with low back pain. BMC Musculoskeletal Disorders 2009; 10(1): 58. 408
Tsao, H, Danneels, LA, Hodges, PW. ISSLS prize winner: smudging the motor brain in 409
young adults with recurrent low back pain. Spine 2011; 36(21): 1721-1727. 410

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
Tsao, H, Druitt, TR, Schollum, TM, Hodges, PW. Motor Training of the Lumbar 411
Paraspinal Muscles Induces Immediate Changes in Motor Coordination in 412
Patients With Recurrent Low Back Pain. The Journal of Pain 2010; 11(11): 413
1120-1128. 414
van Dieën, JH, Selen, LPJ, Cholewicki, J. Trunk muscle activation in low-back pain 415
patients, an analysis of the literature. Journal of Electromyography and 416
Kinesiology 2003; 13(4): 333-351. 417
Van Dillen, LR, Sahrmann, SA, Norton, BJ, Caldwell, CA, Fleming, DA, McDonnell, 418
MK, Woolsey, NB. Reliability of Physical Examination Items Used for 419
Classification of Patients With Low Back Pain. Physical Therapy 1998; 78(9): 420
979-988. 421
Wallwork, T, Stanton, W, Freke, M, Hides, J. The effect of chronic low back pain on 422
size and contraction of the lumbar multifidus muscle. Man Ther 2009; 14(5): 423
496 - 500. 424
Willigenburg, NW, Kingma, I, Hoozemans, MJM, van Dieën, JH. Precision control of 425
trunk movement in low back pain patients. Human Movement Science 2013. 426
Wong, TKT, Lee, RYW. Effects of low back pain on the relationship between the 427
movements of the lumbar spine and hip. Human Movement Science 2004; 428
23(1): 21-34. 429
430

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Acknowledgements
The authors thank Annina Schmidt, David Klyne and Michael Bergin for their
assistance with data collection and Asad Khan for his assistance with statistical
analysis.
Funding:
This project was supported by funds from the National Health and Medical
Research Council of Australia (Fellowships [PH: APP1002190, SS: ID631612],
Program Grant [ID631717]).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Table1. Rating scale for the “Clinical test of thoracolumbar dissociation”
Criteria Initial performance Initial performance
1. Quality of pelvic motion
– direction with best
quality
Moves the pelvis in to
anterior/posterior tilt in
manner that is smooth,
controlled and to the end
3 3
Moves the pelvis but not
ideal in terms of
smoothness, range or with
too much muscle activity
2 2
Jerky, uncoordinated,
limited motion of the
pelvis +/- excessive
muscle activity
1 1
Inability to move the
pelvis into anterior or
posterior tilt
0 0

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
2. Control of adjacent
regions – direction with
best quality
Moves pelvis with gentle
lordosis/kyphosis of the
lumbar spine but limited
movement at the
3 3
Moves pelvis mild
thoracolumbar extension
or activity of
thoracolumbar erector
2 2
Moves pelvis but with
excessive thoracolumbar
extension and activation
of thoracolumbar erector
1 1
Moves into thoracolumbar
extension/flexion with no
motion of pelvis
0 0
3. Directional preference

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
Moves with high quality a
into anterior and posterior
tilt
2 2
Moves with high quality
in one direction 1 1
Does not moves in high
quality in either direction 0 0
4. Breathing
Able to maintain quiet
breathing during the task 1 1
Unable to maintain quiet
breathing during the task 0 0

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
5. Repetition
Able to perform 10
repetitions with high
quality a
1 1
Able to perform some
(between 1-10) repetitions
with higha quality
0.5 0.5
Unable to perform any
repetitions with high
quality a
0 0
TOTAL SCORE /10 /10
a High quality pelvic control
- Moves into
anterior/posterior tilt in
manner that is initiated with

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
Table 2. Strength of agreement for the Kappa coefficients (Landis et al., 1977)
Strength of agreement Kappa
coefficients
Almost perfect/Very Good 0.81 - 1
Substantial/Good 0.61 – 0.80
Moderate 0.41 – 0.60
Fail 0.21 – 0.40
Slight 0.01- 0.20
Poor < 0

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
Table 3. Inter-rater agreements of total test scores in Control and LBP participants
Assessors Pre-training Post-training
k 95%CI k 95%CI
Control
R1/R2 0.81 (0.68 - 0.93) 0.75 (0.29 - 0.95)
R1/R3 0.70 (0.34 - 0.93) 0.71 (0.31 - 0.95)
R2/R3 0.63 (0.29 - 0.89) 0.48 (-0.05 - 0.92)
LBP
R1/R2 0.66 (0.33 - 0.84) 0.51 (-0.03 - 0.79)
LBP (Video)
R1/R4 0.62 (0.19-0.81) 0.60 (0.11-0.90)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
Table 4. Inter-rater agreement of each criteria score for control and LBP participants
Control Control Control LBP LBP
(Video)
Assessors R1/R2 R1/R3 R2/R3 R1/R2 R1t/R4
Criteria 1 Pre k 0.94 0.77 0.66 0.60 0.44
CI (0.77-1.00) (0.441-0.97) (0.37 - 0.87) (0.07 - 0.82) (0.00-1.00)
Criteria 1 Post k 0.65 0.76 0.49 0.63 0.67
CI (0.24 -0.89) (0.3 -1.00) (0.06 - 0.78) (0.11 - 0.87) (0.00-0.93)
Criteria 2 Pre
k 0.43 0.70 0.09 0.57 NaN
CI (0.0 - 1.0) (0.27 - 0.92) (-0.71 - 0.89)
(0.130 -
0.85) NaN
Criteria 2 Post k 0.61 0.18 0.35 0.34 0.68
CI (0.12 - 0.93) (-0.34 - 0.60) (-0.07 - 0.67) (0.12 - 0.54) (0.17-1.00)
Criteria 3 Pre k 0.57 0.58 0.44 0.15 0.29
CI (0.18- 0.87) (0.17 - 0.83) (-0.11 - 0.87) (-0.14 - 0.43) (-0.46-1.0)
Cirteria 3 Post
k 0.40 0.52 0.36 0.41 0.06
CI (0.05 - 0.86) (0.22 - 0.86) (0.00 - 0.75) (0.00 - 0.76)
(-0.23-
0.36)
Criteria 4 Pre k NaN NaN NaN NaN NaN
CI NaN NaN NaN NaN NaN
Criteria 4 Post k NaN NaN NaN NaN NaN
CI NaN NaN NaN NaN NaN
Criteria 5 Pre k 0.42 0.67 0.33 0.21 0.62
CI (-0.03 - 0.88) (0.21 - 1.00) (-0.13 - 0.80) (-0.15 - 0.56) (-0.05-1.0)
Criteria 5 Post k 0.51 0.49 0.35 -0.03 NaN
CI (0.00 - 0.89) (-0.08 - 0.92) (-0.83 - 1.00) NaN
*NaN= it is not possible to calculate k because there is a perfect match between
scores

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
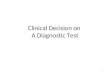
Figure 1. Demonstration of Clinical test of thoracolumbar dissociation. (A) Expected
performance anterior/posterior tilt of the pelvis in sitting while attempting to maintain a
constant position of the thorax and thoracolumbar junction. (B) Spine curvatures
described for each position. (C) Pattern of movement that combines lumbar and
thoracolumbar junction. (D) Spine curvatures described by the altered pattern.
Table 5. Rater 1 intra-rater agreement of total test scores in LBP participants live and
videoed assessments.
Assessors Pre-training Post-training
k 95%CI k 95%CI
Total Scores
R1/R1v 0.56 (0.17-0.86) 0.78 (0.58-0.93)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT