Embed Size (px)
Citation preview

A case study to investigate the feasibility of supporting radiotherapy workflows through
the use of mobile devices
Author: Ying-Ying Yang Öhlin
Master's Programme in Health Informatics Spring Semester 2016 Degree thesis, 30 Credits
Author: Ying-Ying Yang Öhlin Main supervisor: M.Sc./Ph.D., Stefano Bonacina, Health Informatics Centre, Department of learning, informatics, management and ethics, Karolinska Institutet Examiner: Ph.D., Sabine Koch, Department of learning, informatics, management and ethics, Karolinska Institutet

Master's Programme in Health Informatics Spring Semester 2016 Degree thesis, 30 Credits
Affirmation I hereby affirm that this Master thesis was composed by myself, that the work contained herein is my own except where explicitly stated otherwise in the text. This work has not been submitted for any other degree or professional qualification except as specified; nor has it been published. Arlöv, May 18, 2016
Ying-Ying Yang Öhlin

Master's Programme in Health Informatics Spring Semester 2016 Degree thesis, 30 Credits A case study to investigate the feasibility of supporting radiotherapy workflows through the use of mobile devices Abstract Background - ICT has evolved worldwide and been implemented in the field of radiation oncology over the last decades. Large amounts of information can be stored and sent digitally, which is time saving and radically reduces the risk of missed, lost or inaccurate information. Nevertheless, the two of the largest hospitals, SUS and KS, still use paper protocols. That is indefensible from a time, cost perspective and in term of patient safety. Objectives - To develop a mockup of user interfaces for envisaging their workflows, as well as to test the mockup on tablet and interview voluntary users. Methods - Template proposals to represent an electronic treatment plan (user interfaces) on a tablet were designed with a prototyping tool based upon an explicit understanding of the target end users. Simulations of how the processes would change to the end users were performed at Radiotherapy Departments at Skånes University Hospital in Lund and Radium Home at Karolinska University Hospital in Stockholm. Entirely ten volunteers participated the testing. Results - The feedback highlighted how the healthcare personnel were willing to change their current work methods. The participated healthcare personnel felt the suggestion of using electronic patient protocols instead of paper form was a good idea to support their workflows. They were impressed on the design. Conclusions - Upon the results, the use of this kind of innovations in radiation oncology practice may introduce an important tool to support workflows and improve cancer care. Nevertheless, the designed elements and IT technical solutions need to be ameliorated in order to facilitate the proposed system to become true. Keywords: Radiotherapy, paper treatment card, paper verification protocol, mobile technology, healthcare workflow, oncology information system.
Table of Contents
Glossary/List of abbreviations....................................………………….......... 7
List of figures…………………………………………………….……........... 8
List of tables……………………………………………………......……….... 8
1. Introduction……………………………………………….....………........ 9
1.1 Cancer and Radiotherapy ..................................................................... 9
1.2 Radiation Oncology Information System.............................................. 9
1.2.1 ARIA® Oncology Information System....................................... 10
1.2.2 MOSAIQ® Radiation Oncology.................................................. 10
1.3 External Radiotherapy......................................................................... 10
1.3.1 Patient Pathway of External Beam Radiation Treatment............ 10
1.3.2 Setup and Planning for External Beam Radiation Treatment......11
1.3.3 External Beam Radiation Treatment Delivery............................ 14
1.4 The Case of Skåne University Hospital in Lund................................. 15
1.4.1 Organization................................................................................ 15
1.4.2 Radiation Therapists.................................................................... 16
1.4.3 Oncologists.................................................................................. 16
1.4.4 Medical Physicists....................................................................... 17
1.4.5 Patient Pathway........................................................................... 17
1.4.6 Patient Paper Treatment Card (Skåne)........................................ 17
1.4.6.1 Paper Treatment Card Part 1............................................... 17
1.4.6.2 Paper Treatment Card Part 2............................................... 18
1.4.6.3 Paper Treatment Card Part 3............................................... 19
1.4.6.4 Verification protocol sheet for nurses to document............ 19
1.5 The Case of Radium Home at Karolinska University Hospital
in Solna, Stockholm........................................................................ 21
1.5.1 Organization................................................................................ 21
1.5.2 Healthcare Personnel................................................................... 21
1.5.3 Patient Paper Radiation Treatment Card at Radium Home........ 22
1.5.3.1 Patient Treatment Information Sheet.................................. 22
1.5.3.2 Verification (Setup) Protocol Form.................................... 23
1.5.3.3 Images................................................................................. 24
1.5.4 Patient Pathway........................................................................... 25
1.6 User-Centered Design……………………………………….……… 26
1.7 Think Aloud………………………………………………...………. 27
1.8 Problem Description............................................................................ 27
1.9 Previous Research…………………………………………..………. 28
2. Aim and Objectives................................................................................... 30
2.1 Aim...................................................................................................... 30
2.2 Objectives............................................................................................ 30
2.3 Research Questions............................................................................. 30
3. Methods………………………………………………...……......……… 31
3.1 Design………………………………………………………….…… 31
3.1.1 The Elements for Design…….…………………………...……. 31
3.1.2 The Users ……………………………………………….…….. 31
3.1.3 Scenarios………………………………………………………. 32
3.1.3.1 User Scenario of Nurse and Medical Physicist……...…….. 32
3.1.3.2 User Scenario of Physician………...………………...……. 32
3.1.4 Indigo Studio…………………………………………...……… 32
3.1.5 Interfaces…………………………………….………...………. 33
3.1.5.1 Log On Interface................................................................ 33
3.1.5.2 Appointment Scheduling Interface.................................... 33
3.1.5.3 Diagnosis and Setup Parameters Interface......................... 33
3.1.5.4 Treatment Beam (Dose) Planning Interface....................... 33
3.1.5.5 Verification Protocol Form Interface.................................. 33
3.1.5.6 Categories Interface........................................................... 34
3.1.5.7 Breast Patients Interface..................................................... 34
3.1.5.8 Workflows.......................................................................... 34
3.2 Settings and Participants..................................................................... 37
3.3 Data Collection for The Study............................................................ 38
3.3.1 Data Collection Strategy............................................................. 38

3.3.2 Prerequisites for The Study Activities................................... 38
3.4 Data Collection Method for The Template Proposals………………. 38
3.4.1 Documents…………………………………………...………… 39
3.4.2 Observation………………………………………...……….…. 39
3.4.3 Focus Group………………………………………...…………. 39
3.5 Ethical Consideration.......................................................................... 40
4. Results....................................................................................................... 41
4.1 Think Aloud and Observations........................................................... 41
4.2 Informal Interviews and Feedback...................................................... 42
4.2.1 Positive Feedback........................................................................ 42
4.2.2 Doubt and Negative Feedback.................................................... 43
4.2.3 Suggestion Feedback................................................................... 44
5. Discussion................................................................................................. 46
5.1 Method Discussion.............................................................................. 46
5.1.1 What Were Good......................................................................... 46
5.1.2 Limitation.................................................................................... 47
5.2 Result Discussion................................................................................ 48
5.2.1 Strengths and Weaknesses……………………………….……. 49
5.3 Future Work........................................................................................ 50
6. Conclusions............................................................................................... 51
Acknowledgments........................................................................................... 51
References…………………………………………………………..........…. 52
Appendices.……………………………….........................………………… 59
Appendix I - Consent/Questionnaire (Previous Research)..……… 59
Appendix II - Feedback Data (Previous Research)......................... 61
Appendix III - Theme Coding (Previous Research)........................ 63
Appendix IV - Diagrams (Previous Research)................................ 64
Appendix V - Consent form for this research................................. 65
Appendix VI - Figure17.................................................................. 66
Appendix VII – Time Frame........................................................... 67
7
ABBREVIATIONS 4G The fourth generation of mobile telecommunications technology 5G 5th generation mobile networks (5th generation wireless systems) BART Breathing Adapted Radiotherapy CBCT Cone Beam Computed Tomography CT Computerized (Computed)Tomography CTV Clinical Target Volume DSV Department of Computer and Systems Sciences EBRT External Beam Radiation Treatment EHR Electronic Health Record GTV Gross Tumor Volume GY Gray ICT Information and Communication Technology ICRU International Commission on Radiation Units & Measurements KS Karolinska University Hospital in Solna in Stockholm LAT Lateral LINAC Linear Accelerator LNG Long MED Mobile Electronic Devices MRI (MR) Magnetic Resonance (Imaging) MU Monitor Unit OAR Organs At Risk PET-CT Positron Emission Tomography-Computed Tomography PTV Planning Target Volume RH Radium Home RT Radiotherapy (Radiation Therapy or Radiation Treatment) SOK Skånes Onkologiska Klinik SSD Source to Skin (Surface) Distance SUS Skånes University Hospital TA Think Aloud UCD User-Centered Design VRT Vertical WBRT Whole Brain Radiotherapy WHO World Health Organizaiton Wi-Fi Wireless Fidelity

8
LIST OF FIGURES Figure 1 A Linear Accelerator.............................................................................................. 11 Figure 2 Patient Pathway...................................................................................................... 12 Figure 3 Thermoplastic Mask............................................................................................... 12 Figure 4 A treatment volume................................................................................................ 13 Figure 5 Adjustment of patient's position............................................................................. 14 Figure 6 Mapping.................................................................................................................. 15 Figure 7 Radiotherapy Department, Lund………………………………………………… 16 Figure 8 Simplified Patient Pathway.................................................................................... 17 Figure 9 Paper Treatment Card Part 1 (SUS)....................................................................... 18 Figure 10 Paper Treatment Card Part 2 (SUS)....................................................................... 20 Figure 11 Paper Treatment Card Part 3 (SUS)....................................................................... 20 Figure 12 Verification Protocol Sheet (SUS)......................................................................... 21 Figure 13 External origin and Internal origin......................................................................... 22 Figure 14 Patient treatment information sheet (RH).............................................................. 23 Figure 15 Verification Protocol Form (RH)........................................................................... 24 Figure 16 Images of External beam planning......................................................................... 25 Figure 17 Patient Pathway in swim lane diagram................................................................... 26 Figure 18 A User-Centered Design life-cycle......................................................................... 27 Figure 19 A UCD cycle…...................................................................................................... 27 Figure 20 Log On……………………………………………………..…………………….. 34 Figure 21 Appointment Scheduling…………………………………...……………………. 35 Figure 22 Diagnosis & Setup.................................................................................................. 35 Figure 23 Images..................................................................................................................... 35 Figure 24 Verification Protocol.............................................................................................. 35 Figure 25 Categories............................................................................................................... 36 Figure 26 Breast Patients........................................................................................................ 36 Figure 27 Workflows.............................................................................................................. 36 Figure 28 Data collection methods……………………………………………...………….. 39 Figure 29 Feedback 1.............................................................................................................. 42 Figure 30 Feedback 2.............................................................................................................. 43 Figure 31 Design with defect.................................................................................................. 47 Figure 32 Tablet with holder................................................................................................... 49 Figure 33 Tablet with holder and holster................................................................................ 49 LIST OF TABLES Table 1 Participants................................................................................................................ 37 Table 2 Results of mockup testing.................................................................................... 44-45

9
1. INTRODUCTION 1.1 Cancer and Radiotherapy The number of cancer cases is approximately 15 million cases worldwide by the year 2015 [1]. Furthermore, according to WHO, approximately 8.2 million people die each year from cancer which is one of the leading cause of death in the World. Cancer is also called malignant tumors which can grow uncontrolled beyond their usual boundaries and spread to other organs that leads to so called metastasizing. WHO stated "Metastases are the major cause of death from cancer" [2]. Early detection, accurate diagnosis and effective treatment can help to reduce suffering and increase survival rates. Thanks to the researches, various cancer treatment methods have been developed and advanced in the last decades [3] and have improved the 5-year survival rate to between 50 to 60 % in high-income counties [4]. In Sweden, the 5-year survival rate is slightly over 70 % and about 65 % for the 10-year survival rate according to a report from 2013 [5]. Radiotherapy (RT) is one of the effective methods to help cancer patients. RT is to kill [6] tumor cells and/or to control [7] cancer diseases by using high energy beams to destroy tumor DNA. In general, the RT processes encompass planning, administration of external or internal radiation therapy (brachytherapy), attention to side effects, and follow up after treatment [8]. Nevertheless, this research is going to surround external RT and the health personnel's workflows at Radiotherapy Departments at Skånes University Hospital (SUS) and Radium Home at Karolinska University Hospital.
1.2 Radiation Oncology Information System Computerized technologies have been used in medicine since 1950s [3]. Particularly in the field of Radiation Oncology, the relationship between healthcare and technology is deeply influenced and interconnected [9]. The first used computer technology in radiotherapy area was dose calculation in the early 1960s. Thereupon treatment planning systems in two-dimensional were put into practice in the middle of the 1960s [3]. Thereafter, a number of innovative solutions have over the years been implemented in the field of radiotherapy, such as graphics, imaging, display technologies, three-dimensional treatment planning systems, and so forth. The innovation solutions supply "better view of the anatomical relationships and dose distributions" [3]. Connecting with the images in the field of radiation oncology, there are another advanced technologies which allow the physicians and other health care personnel to make diagnosis, therapy decision, evaluation, prescription, to settle setup parameters, to plan target volume, to deliver RT treatments, to follow up, to document, and so forth [3].
In currently, all the aforementioned tasks are actually computerized performed and stored electronically in oncologic care management software for oncologic nurses to safely retrieve the right treatment to the right patient, to deliver the exact prescribed doses and provide qualified treatments to the patients. A radiation oncology information system consists of information and image management solutions with the mentioned different tasks for

10
oncologic healthcare personnel to work with. This kind of systems are such as ARIA® Oncology Information System [10] and MOSAIQ® Radiation Oncology [11].
1.2.1 ARIA® Oncology Information System
ARIA® Oncology Information System, supports of Varian Medical Systems, Inc., "combines radiation, medical and surgical oncology information into a complete, oncology-specific EMR that allows to manage the patient's entire journey—from initial diagnosis through post-treatment follow-up" [10]. With ARIA, the oncologic healthcare personnel can:
• Evaluate diagnosis-specific data to compare acute responses to treatment and long-term clinical outcomes [10]
• Develop disease-specific clinical protocols to facilitate a standard, consistent quality of care [10]
• Monitor radiation dose and review treatment images to determine if plan changes are required [10]
• Make confident decisions with the aid of embedded rule-based decision support [10] • Create structured, oncology-specific care plans for the post-treatment care and
support of cancer survivors [10]
1.2.2 MOSAIQ® Radiation Oncology
MOSAIQ Radiation Oncology supplies of Elekta AB, provides the entire picture of all collected and accessible patient information, personalized treatment from diagnosis through treatment and follow-up. Through a common interface, it provides "techniques with automated and customizable workflows" [11] with connected treatment planning and reduced errors to deliver the best healthcare for every patient [11].
RT department at Radium Home (Radiumhemmet) at Karolinska University Hospital in Solna in Stockholm has only used ARIA Oncology Information System to perform different tasks to delivery radiotherapy treatments to cancer patients. But RT department at Skånes University Hospital in Lund has used both ARIA Oncology Information System and MOSAIQ Radiation Oncology for the respectively implementations.
1.3 External Radiotherapy External Radiotherapy customarily calls External Beam Radiation Treatment (EBRT) because a radiation treatment usually deliveries highly focused "non-invasive" [12] beams of high-energy X-rays to the region of a patient’s tumor from outside of patient’s body by a radiotherapy machine called a Linear Accelerator - LINAC [13] (Figure 1). The method is to “destroy cancer cells while sparing the surrounding normal tissue” [13].
1.3.1 Patient Pathway of External Beam Radiation Treatment
It’s a complex process to deliver an effective radiotherapy to cure or relief from the disease to a cancer patient. The process requires accurate and careful preparation before treatment can
11
begin. Consequently many categories of healthcare personnel work together and engage in each stage of preparation and delivery of radiotherapy. A journey of patient pathway [14, 15] with the phases can look like the diagram below (Figure 2).
More details about the pathway are described in the following sections:
• 1.3.2 Setup and Planning for External Beam Radiation Treatment
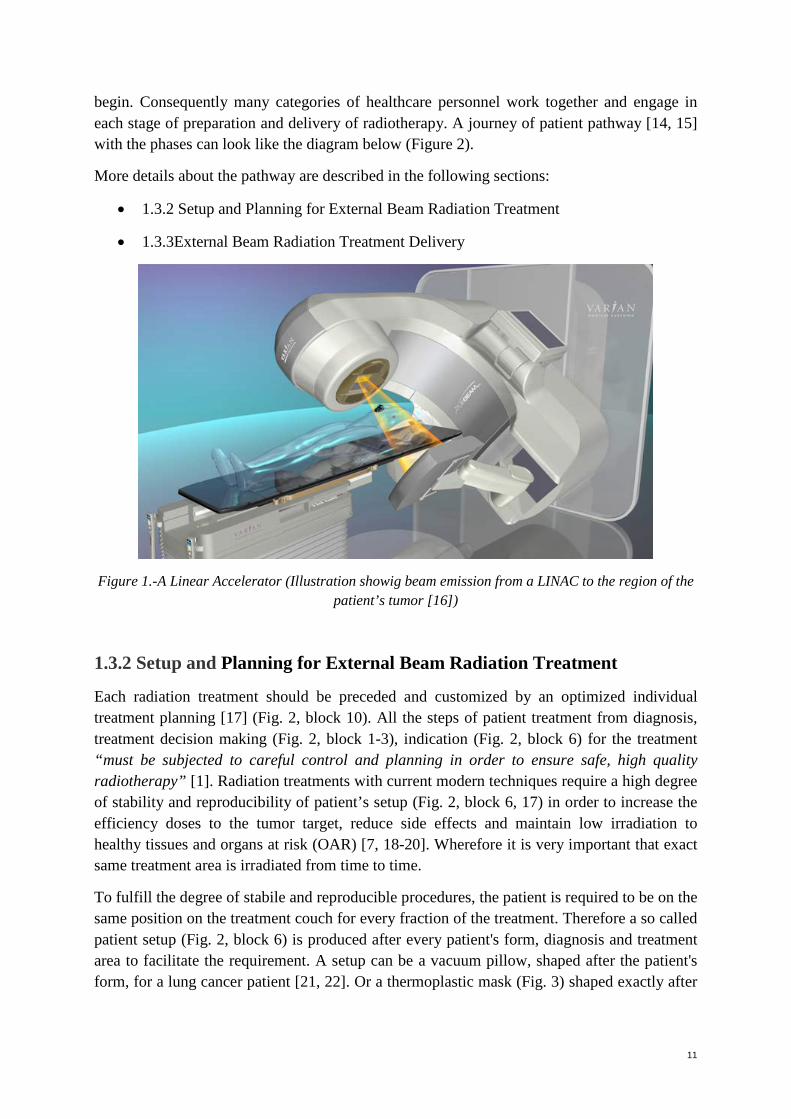
• 1.3.3External Beam Radiation Treatment Delivery
Figure 1.-A Linear Accelerator (Illustration showig beam emission from a LINAC to the region of the patient’s tumor [16])
1.3.2 Setup and Planning for External Beam Radiation Treatment
Each radiation treatment should be preceded and customized by an optimized individual treatment planning [17] (Fig. 2, block 10). All the steps of patient treatment from diagnosis, treatment decision making (Fig. 2, block 1-3), indication (Fig. 2, block 6) for the treatment “must be subjected to careful control and planning in order to ensure safe, high quality radiotherapy” [1]. Radiation treatments with current modern techniques require a high degree of stability and reproducibility of patient’s setup (Fig. 2, block 6, 17) in order to increase the efficiency doses to the tumor target, reduce side effects and maintain low irradiation to healthy tissues and organs at risk (OAR) [7, 18-20]. Wherefore it is very important that exact same treatment area is irradiated from time to time.
To fulfill the degree of stabile and reproducible procedures, the patient is required to be on the same position on the treatment couch for every fraction of the treatment. Therefore a so called patient setup (Fig. 2, block 6) is produced after every patient's form, diagnosis and treatment area to facilitate the requirement. A setup can be a vacuum pillow, shaped after the patient's form, for a lung cancer patient [21, 22]. Or a thermoplastic mask (Fig. 3) shaped exactly after

12
the patient's face, head and/or neck to keep the head stable on the treatment couch during radiation for a head and neck cancer patient or a whole brain radiotherapy [21, 23].
Figure 2.-Patient Pathway (Illustration showing pathway for external radiotherapy patients)
Figure 3.-Thermoplastic Mask (Illustration showig gantry of a LINAC for delivering beam emission to the region of the patient on the treatment table with setup of a thermoplastic mask [12])

13
After setup procedure, every patient needs to be scanned by computerized tomography (CT) (Fig. 2, block 6) and/or Magnetic Resonance Imaging (MRI) or Positron emission tomography-computed tomography (PET-CT) for the purpose of treatment planning [24] (Fig. 2, block 10). Simultaneously, the patient can get small tattoo dots and/or markings of waterproof pen on the skin of the chest and the flanks (Fig. 2, block 6) for cancer diagnosis in the upper body. The tattoo dots and the markings on skin are patient reference for the purpose of stable and reproducible setup procedures before each treatment during delivery (Fig. 2, block 17) of the RT period in order to secure the radiation comes to the treatment target [21].
According to ICRU Report 50 [20], the treatment volume (Fig.4), i.e., the Planning Target Volume (PTV) should include the Gross Tumor Volume (GTV, i.e., visible and/or palpable tumor), the Clinical Target Volume (CTV, i.e., margins added to the GTV to avoid uncertainties and reach the target of radiotherapy) [6] and consideration of OAR. E.g. treatment volume for a whole brain radiotherapy (WBRT) must cover the whole brain and include the cerebrum and cerebellum. The treatment field must cover within the skull by a margin of 1-2 cm, but the anterior caudal border needs to be shaped to prevent and avoid too much radiation dose come to the eyes (an OAR) [25].
Figure 4.-A treatment volume according to ICRU Report 50
Therefore before the treatment delivery (Fig. 2, block 16-20), the patient needs to meet a radiologist/oncologist [15, 26] (Fig. 2, block 1-2) in order to get a prescription (Fig. 2, block 3) to define a treatment, treatment set-up and area for CT scanning (Fig. 2, block 6) as verification film [1, 21, 25]. After CT scan, a radiologist needs to draw the outline of the GTV and define the CTV according to the verification film (Fig. 2, block 9). Afterwards, a dosimetrist [26] (a nurse or a medical physicist [15, 26]) needs to plan the PTV (Fig. 2, block 10). Afterwards, a radiologist and a medical physicist need to approve the PTV together [17] (Fig. 2, block 11-13). Each step of these processes should be documented [17]: "Sites must submit copies of the case history, treatment prescription, treatment administration sheet, dosimetry plans and portal verification films" [25].

14
1.3.3 External Beam Radiation Treatment Delivery
All treatments have side effects [27-29]. To reduce the unwanted side effects from radiation, a whole set treatment is often divided into a number of occasions until the patient get the planned radiation dose, so called fractionation. Normally a set of treatment is given once a day and five days a week for a few weeks [7, 21, 30] (Fig. 2, block 19). E.g., a left-sided breast cancer patient can have prescription of breathing adapted radiotherapy (BART) with a total radiation dose on 50 Gray (Gy) in 25 fractions (2 Gy per fraction) [31-33], i.e., the patient will need to go to the radiotherapy department for treatment in 5 weeks to complete the whole set treatment [32]. The first day (Fig. 2, block 15-16) of the whole set treatment before treatment delivery, the nurses will adjust the patient's position on the treatment couch (Fig. 5) according to the markings on the skin of the patient from the setup and the laser lights in the treatment room in order to obtain the precision of the dose delivery [30] (Fig. 2, block 17). Thereon the treatment fields must be accurately set, monitored, documented, mapped (Fig. 6) and assessed by nurses, medical physicists and/or radiologists [1, 17, 21] (Fig. 2, block 18, 20). Before each fractionation, the nurses need to reproduce the mentioned procedures to adjust patient's setup [30] (Fig. 2, block 17). And after treatment delivery of each fractionation, the nurses who were on responsibility of giving the treatment need to sign their initials in the paper patient treatment card for documentation.
Figure 5.-Adjustment of patient's position (Illustration showig the therapists adjust the patient's position on the treatment couch according to the markings on the skin of the patient and the laser
lights in the treatment room [14])

15
Figure 6.-Mapping: Setup Control (Illustration showig method of mapping (acquisition of verification to verify the patient’s setup and position)[16]
1.4 The Case of Skånes University Hospital in Lund
1.4.1 Organization
A modern building (Fig.7) was built directly adjacent to the existing Radiotherapy Department in Lund with common entrance [34]. The purpose to the new building was to merge RT departments in Lund and Malmö in May 2013 and to concentratedly deliver RT in Lund. The determination of an integration was induced based on the potential benefits of reaching better and more consistent use of processing capacity, more efficient patient flows, better opportunities for skills, better conditions for research and development as well as reduced investment and operating costs [35]. The reorganized RT department called Skånes Onkologiska Klinik (SOK). In current time, the RT department is a part of the Fields of Operation Hematology, Oncology and Radiation Physics (Verksamhetsområde: hematologi, onkologi och strålningsfysid).
Normally the new department delivers RT treatment to cancer patients in Skåne and Halmstad, but patients from other place of Sweden and sometimes from Nordic countries are welcome. From the consolidation, the RT treatments increased about 30% with 12 linear accelerator (LINAC) [35]. The 12 LINAC are seven (6 TrueBeam® and 1 Clinac®) from Varian Medical Systems, Inc. [10], four from Elekta AB [11] and one TomoTherapy® [36] for delivering radiation treatments. For setup, there are three computed tomography (CT) and one magnetic resonance image (MRI) scanner. With help of oncologic care management software in order to deliver the exact prescribed doses and provide qualified treatments, the department had used ARIA® Oncology Information System [10] and MOSAIQ® Radiation Oncology [11] for managing patient's personal details, diagnosis, therapy decision, evaluation,

16
prescription, setup parameters, graphics, images, displays, three-dimensional treatment planning, appointment scheduling, RT treatment delivery, clinical documentation, follow up and so forth. In current time, they only use ARIA® Oncology Information System.
Figure 7.-Radiotherapy Department, Lund [37]
1.4.2 Radiation Therapists
A radiation therapist [14, 26] can be a nurse or a radiographer, every new employed needs to take a special nursing education about RT to get the permission for delivering RT treatments to patients. Therapists check folders of treatment information and parameters, operate RT equipment to deliver radiation treatments to the patients. They also give RT information to the new patients at start of their treatment series. Moreover act as consultants at any occasion of reaction symptom from radiation [26], as coordinators to arrange transports, to contact physicians, dentists, dieticians, physiotherapists and so on for the patients. Each treatment room has one LINAC, about 5 oncology nurses and about 30 - 40 cancer patients daily. Generally every treatment takes about 10 - 20 minutes, but it sometimes takes 30 minutes or longer due to bad health condition of patient. With the purpose of taking turns for working and breaks, each treatment room is not allowed to have less than 3 therapists since every treatment needs 2 therapists to setup the patient. But it happened that there's only 2 therapists in one treatment room on some occasions due to sick leave, part time duty, vacations and meetings. So the amount of oncology nurses is about 60 for the 12 LINAC (5 nurses time 12 LINAC equals 60 nurses).
1.4.3 Oncologists
Oncologists [26] take overall responsibility for the patient’s treatment. They are involved in diagnosing and determining the staging of the cancer, deciding on a course of treatment and

17
prescribing the radiation dose. They also have responsibilities to draw outlines of treatment area, approve a treatment plan, to check and give comments on verification images. They help the therapists at any emergency occasion. At examination room, there are one to five physicians to examine and approve the verification images depends on their working schedules, vacations, meetings, and/or sick leaves.
1.4.4 Medical Physicists
"They are responsible for ensuring the proper commissioning and calibration of radiation-producing equipment and the safe use of radiation, protecting the patients, staff and members of the public in compliance with the relevant legislation" [26]. They have responsibilities to check and approve a treatment plan, to help the nurses to check and approve a setup, a CT scanning, a patient's position on treatment couch, dose counters, verification images and so on. They also have another duties (such as researches, test of new method or system) [35, 38] at RT department, they work according to their schedule. Normally, there are about 3 medical physicists work for treatment planning and 3 to 4 work for LINAC, setup and CT/MR daily.
1.4.5 Patient Pathway
The cancer patient pathway in Lund is as Figure 2 generally. There is sometimes emergency treatment that the patient can skip step 4-5 (Fig.2, block 4-5) and have only one treatment with 8 Gy radiation in one day [39]. For example, if a patient has diagnosis of multiple myeloma or skeletal metastases, and the patient's condition has risk of getting spinal cord compression or fracture [39]. A simplified patient pathway is presented as Figure 8.
Figure 8.-Simplified Patient Pathway
1.4.6 Patient Paper Treatment Card (Skåne)
As checklist, viewing patient treatment parameter information, clinical documentation, follow-up and communication within healthcare personnel, the department has used paper treatment cards (Fig. 9-12) to support their healthcare work to deliver RT treatment to patients.
1.4.6.1 Paper Treatment Card Part 1
In Figure 9, the part 1 of a paper treatment card is represented. Single sections of the card are labeled with a letter and/or with a figure. The explanation is as follows:
A. Place for patient personal details: name, person identification number, address and telephone number.
B. Area for physicians to describe the patient’s diagnosis and prescribe radiation treatment
18
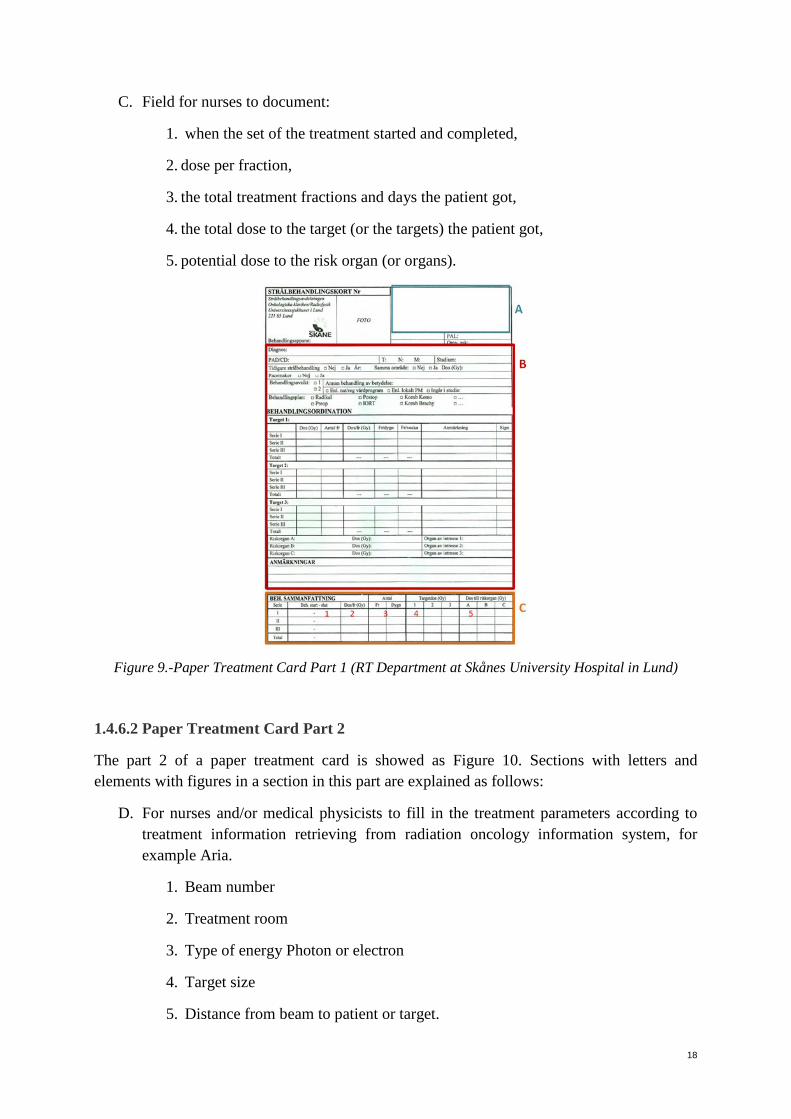
C. Field for nurses to document:
1. when the set of the treatment started and completed,
2. dose per fraction,
3. the total treatment fractions and days the patient got,
4. the total dose to the target (or the targets) the patient got,
5. potential dose to the risk organ (or organs).
Figure 9.-Paper Treatment Card Part 1 (RT Department at Skånes University Hospital in Lund)
1.4.6.2 Paper Treatment Card Part 2
The part 2 of a paper treatment card is showed as Figure 10. Sections with letters and elements with figures in a section in this part are explained as follows:
D. For nurses and/or medical physicists to fill in the treatment parameters according to treatment information retrieving from radiation oncology information system, for example Aria.
1. Beam number
2. Treatment room
3. Type of energy Photon or electron
4. Target size
5. Distance from beam to patient or target.

19
6. Angle of beam (treatment head)
7. Collimator angle: to shape the radiation beams with multi-leaf collimators in order to deliver the radiation as treatment planning. [26]
8. Couch angle
9. Bolus: setting up shell, is a tissue-equivalent material to be placed between the radiation beams and the skin to increase the surface dose and/or to compensate for missing tissue in order to get precisely determined radiation doses in the treatment area.
10. Type of wedge: an attenuator to reduce the radiation in order to protect OAR or to obtain coequal dose on the whole treatment area
11. Number of blocks: type of block to stop radiation.
12. Type of wedge
13. Dose of beam
E. 14. For nurses to document the doses came to the targets from each treatment beam (LINAC angle).
1.4.6.3 Paper Treatment Card Part 3
The part 3 of a paper treatment card is represented as Figure 11. Single sections of the card are labeled with letters. The explanation is as follows:
F. For nurses at fixation/CT section to document the patient’s setup parameters. For example, setup of vacuum pillow or thermoplastic mask
G. For dosimetrists [26] to document the treatment planning
H. For every personnel (physician, medical physicist and/or nurse) who involved to settle the radiation therapy to sign under.
1.4.6.4 Verification protocol sheet for nurses to document
In Figure 12, a verification protocol sheet is represented. Single elements of the sheet are marked with figures. The explanation for the elements is as follows:
1. Datum = date: which date the nurses took picture on the patient to secure the patient’s position.
2. Avvikelse = deviation: how much the difference between the marks on the patient’s skin and the mapping (acquisition of verification to verify the patient’s setup and position).
3. Vrt. = vertical: how high the couch position should be.

20
4. Lng = Long: how long the couch position should be.
5. Lat = lateral: how much to the right or to the left the couch position should be.
6. Brits-höjd = high of the couch: how high the couch should be.
7. Kommentar = comments: for example, do we need a correction?!
Figure 10.-Paper Treatment Card Part 2 (RT Department at Skånes University Hospital in Lund)
Figure 11.-Paper Treatment Card Part 3 (RT Department at Skånes University Hospital in Lund)

21
Figure 12.-Verification Protocol Sheet (RT Department at Skånes University Hospital in Lund)
1.5. The Case of Radium Home at Karolinska University Hospital in Solna, Stockholm
1.5.1 Organization
Radium Home (Radiumhemmet) [40] was the first oncology clinic in Sweden and founded in 1910. The clinic moved to Karolinska Hospital in 1937 but has kept the name "Radiumhemmet" until now. The clinic had an extensive improving during the 1950s and 1960s. The older equipments were replaced with innovation like LINAC. In current this RT department has 8 LINAC (1 TrueBeam and 7 Clinac) from Varian Medical Systems, Inc. [10], 1 CT and 1MR. But one LINAC is on rest condition due to shortage of therapists. The treatment capacity is about 30 patients per LINAC per day. The main cancer patients are from Stockholm area and Gotland.
1.5.2 Healthcare Personnel
Healthcare personnel at Radium Home have similar duties as the ones in Skåne. In the category of therapist, it's a women dominated profession, there are only 2 male nurses among totally about 40 nurses at this department. The nurses at this department are 45-year old in

22
average according to the previous research (Appendix I). The nurses are required to have at least 2-year work experiences of variety of medical backgrounds and special oncology education to obtain qualified ability of operating RT treatments to cancer patients. This is attributable to "ionizing radiation is a complex process involving highly trained personnel" [1]. Since cancer patients are increased significantly in Sweden [21], the department has a strategy of delivering treatments more than eight hours at one or two treatment rooms a day. For operating the strategy, the department has employed new nurses.
1.5.3 Patient Paper Radiation Treatment Card at Radium Home
1.5.3.1 Patient Treatment Information Sheet
Patient treatment information sheet (Fig.14) is containing patient information retrieved from Radiation Oncology Information System and printed out on a piece of paper for nurses to check treatment parameters and to deliver treatments accordingly. Explanation for the elements what the healthcare personnel use for is in Figure 14.
Additional explanation for specific terminology, such as "Yttre origo", "Inre origo" and "Iso", is as follows. "Origo" (Fig.14, no.18) is origin, is defined during treatment planning, it's a zero point on patient's skin or inside of patient's body as patient reference for nurses to set up the patient before each treatment. "Yttre origo" (Fig.13 & Fig.14, no.18) is external origin, it is a zero point on patient's tattoo on skin on the chest, it's usually a patient reference for breast and/or lung cancer patients. "Inre origo" (Fig.13 & Fig.14, no.18) is internal origin, it is a zero point inside the patient's body according to anatomic structures (for example, the upper edge of the symphysis pubis or the leading edge of a vertebra) or the markings on the patient's skin, i.e., an intersection point of the three tattoos on patient's skin. "Iso" (Fig.14, no.18) is a determined meet point inside the patient's body where the radiation should reach. The determined meet point for x, y and z axes in a Cartesian coordinate system is set to (0, 0, 0). The Iso, external origin and internal origin are determined by dosimetrists [26] together with physicians and medical physicists during treatment (dose) planning.
Figure 13.-External origin and Internal origin

23
Figure 14.-Patient treatment information sheet (Radium Home)
1.5.3.2 Verification (Setup) Protocol Form
Verification protocol form (Fig.15) is used as a manner to control the patient's position. The form is printed out in a piece of paper for nurses to document the method and the result of taking images on patient's position on treatment couch (setup). The documented form should be sent to the physicians for examination and approval after different fractions depending on different diagnosis according to the determined regulations. Sometimes the physicians need to check the verifications with help of medical physicists. After approval, the physicians and/or with medical physicists will define how often the nurses should have verification control on the patient, for example, every day, once a week or no more control or reset iso point.

24
Figure 15.-Verification (Setup) Protocol Form (Radium Home)
1.5.3.3 Images
External beam planning: Both departments in Lund and Solna retrieve these images from Radiation Oncology Information System, Aria, and print out with colors by a printer for checking the PTV & CTV area, the origin point and the dose distribution over the treatment target. (Fig.16)

25
Figure 16.-Images of External beam planning
1.5.4 Patient Pathway It is important that a RT patient is in the same position on the treatment couch each time the patient receive treatment. It is ascribable to the relatively high radiation and attenuation potential side effects. A setup for a patient is produced according to physician's prescription and patient's form to make it easier to be in the same position after meeting with physician. Afterwards a CT scanning should be done for dose planning. On that occasion a treatment can be delivered when the folder of treatment information and parameters is completed. The RT patient pathway (Fig.2) at Radium home is similar to the RT department at SUS generally. In a swim lane diagram as Figure 17 shows how different categories of healthcare personnel engage in the radiation treatment preparation and delivery in patient pathway. Nurses assistants employ appointment scheduling (block 4 & 5). Physicians have responsibilities for radiation treatment of consultation, prescription, target outlines, plan approving and having consents for the radiation treatment from the patient (block 1-3, 9 & 11). The radiation treatment planning team (block 7) is including dosimetrists [26], physicians and medical physicists. A dosimetrist can be a nurse or a medical physicist. Blocks 7, 10 & 20 are collaboration between nurses and medical physicists. Furthermore physics checks of a radiation treatment plan should be performed by a medical physicist (block 12). The rest steps in the patient pathway are engaged by nurses (block 6, 8, 13-19 & 21).
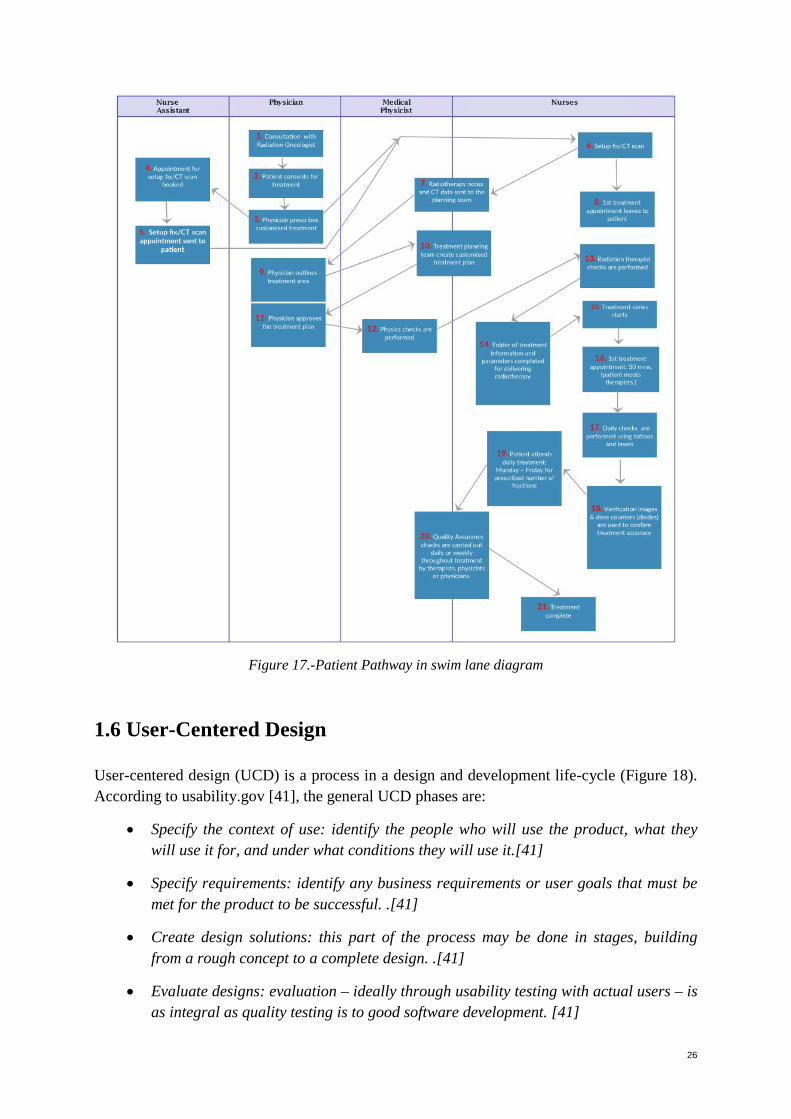
26
Figure 17.-Patient Pathway in swim lane diagram
1.6 User-Centered Design User-centered design (UCD) is a process in a design and development life-cycle (Figure 18). According to usability.gov [41], the general UCD phases are:
• Specify the context of use: identify the people who will use the product, what they will use it for, and under what conditions they will use it.[41]
• Specify requirements: identify any business requirements or user goals that must be met for the product to be successful. .[41]
• Create design solutions: this part of the process may be done in stages, building from a rough concept to a complete design. .[41]
• Evaluate designs: evaluation – ideally through usability testing with actual users – is as integral as quality testing is to good software development. [41]

27
Katsulis et al. also divided the UCD cycle into four phases (Fig.19): Study (workflow observations), Design (gathering user requirements), Build (prototype comparison interviews) and Evaluate (usability testing) [42]. UCD is depending on the influences from the active involvement of the end-users who will use the product. UCD helps the researcher to gain deep understanding of the end-users’ needs, to obtain a suitable and user-friendly user interface. [41-44] “With the development of any application or tool, the design process should be user-centered.” [42]
Figure 18.-A User-Centered Design life-cycle [41] Figure 19.-A UCD cycle upon Katsulis et al. 1.7 Think Aloud Think-aloud is a method for user interactions with prototype interface design. The participants are asked to follow the instructions and to say or to repeat everything out loud for each task during interactions with interface design. The researcher sits beside the participants, so the researcher can give instructions, observe and help the participants when needed. The method provides immediate feedback. The method helps the researcher to understand the strategies that participants use to do a task. It assists the researcher to capture the respondents’ thoughts, to detect potential causes of response errors and/or biases within the tasks. [45-47]
1.8 Problem Description Science, innovation and information technology has affected peoples' livelihood over the last decades greatly. The new information technologies have been changing peoples' way of thinking and how they do things. For instance, a transition from the paper record to the electronic record made it possible to allow larger possibilities of communication, to manage and to provide healthcare more successfully with higher effectiveness [48]. Particularly the information and communication technology (ICT) has influenced the field of clinical oncology tremendously [9].

28
The author is a radiographer and oncology nurse (radiation therapist [26]) at radiotherapy [15] department at Skånes University Hospital (SUS) in Lund and at Radium home at Karolinska University Hospital (KS) in Solna, Stockholm. At both departments the healthcare personnel still deliver treatments to cancer patients according to protocols [49] of paper treatment cards (a sort of patient health record) [50], nevertheless there are already EHR [51] and Radiation Oncology Information System [10, 11] for clinical documentation. The physicians (radiologists, oncologists) [26], medical physicists [26] and nurses use the paper treatment cards to document different information about patients. The physicians use the treatment cards to document diagnosis, prescriptions of treatments and other information by hand writing which are not always readable and leads to increased risk of patient safety [52]. The nurses/therapists use the treatment cards as checklists [53], to note and/or to sign for each treatment. The medical physicists use the cards to fill up the specifications of the prescribed treatments. The treatment cards are preserved in order of patients' last names in a drawer in each treatment control room. Sometimes a patient card could be forgot to put back in the drawer, sometimes a treatment card could get stuck somewhere due to a physician or a medical physicist or a nurse forgot to fix things on it for many different reasons. At that instant it would take longer time and more energy to search the forgotten treatment card which couldn't be found at once when it's time to give treatment to a patient. Or the card might still be at another treatment room where the patient got a treatment the day before. Even when the healthcare personnel remembered that the patient's treatment card forgot in another treatment room, time was still needed for the healthcare personnel to make a call to check and rush to the room and pick up the card. Occurrences have always affected the day's treatment schedule and wasted patients' time. Many oncology nurses have experienced these kinds of unexpected situations which falling out from the framework were very harmful for patients since radiation could also harm people [52]. 1.9 Previous Research In consideration of aforementioned predicament at radiotherapy departments that the forgotten paper treatment cards and protocols could jeopardize patient’s safety and influence the healthcare personnel workflows. The author had a suggestion to puzzle out a secure method to retrieve and preserve patient information with mobile digital solution. Everything started with the author's study, Scientific Communication and Research Methodology HT2015 – Period C, D, at DSV at Stockholm University. The author made an investigation (Appendix I - IV) at the mentioned radiotherapy departments. The investigation was built on the healthcare personnel’s opinions which were carried out with a questionnaire (Appendix I). The aim of the investigation was focused on imagine of using mobile technology to support daily healthcare work.
The participants’ thoughts and motivations to the suggestion were very positive. Most of the participants, 76 % (Appendix IV, Diagram 3), were positive to the suggestion of using patient

29
treatment protocols with mobile technology in tablet form when giving radiotherapy treatment to patient. The motivations (Appendix II & III) were, inter alia:
• "increase security",
• "interesting with new ways of working",
• "patients can enter their own person data to confirm that we have the right patient in the treatment room",
• "it's more flexible and faster to get information and change things",
• "more reliable for the benefit of the patients"
• and "provided technology is reliable and minimum of interruptions".
There is lack of knowledge why healthcare personnel at radiotherapy departments in Sweden still use paper treatment cards during giving radiotherapy treatments to patients. There is also lack of knowledge about using mobile technology during giving radiotherapy treatments to patients in Sweden. But according to Braun et al. [54], the outcome of their study “suggests mobile technology presents promising opportunities to improve the range and quality of services provided by community health workers”. As well as Pryss et al [55] suggested mobile task management towards supporting healthcare personnel during a ward round and improving “IT support of knowledge-intensive process in general”. Moreover, 65% of physicians from different countries in Europe “declared to use a smartphone and/or tablet during their clinical activity” in the study of De Bari et al. [9] In addition, majority of the participants from the previous research as aforementioned accepted to the suggestion of envisaging of using mobile technology to support daily healthcare work. Lack of knowledge, scientific researches and the positive results from the previous research excited the motivation to investigate a suggestion, the feasibility of supporting radiotherapy workflows through the use of mobile devices.

30
2. AIM and OBJECTIVES
2.1 Aim This research was a case study to investigate the feasibility of supporting radiotherapy workflows through the use of mobile devices.
2.2 Objectives The study was to survey the opportunity of using the proposed method to support the healthcare personnel's workflows at radiotherapy departments. The objectives of the study are:
• To develop a mockup of user interfaces for envisaging their workflows. • To test the mockup on tablet and interview voluntary users.
2.3 Research Questions The purpose for this study was to determine the feasibility of healthcare personnel at radiotherapy departments in Sweden using electronic treatment cards on mobile technology – i.e. tablets - during patient radiotherapy treatment, rather than the current paper treatment cards. The main question to be answered is:
• How do the healthcare personnel feel about managing electronic treatment cards on mobile devices?
The sub-questions to be answered are:
• How should a mobile workflow support for radiotherapy be designed? • What could be the advantages and disadvantages of using electronic treatment cards
while giving radiotherapy treatments to patients?

31
3. METHODS This research was a qualitative case study with think aloud, observation and informal interviews to explore a challenge and gather qualitative feedback from the participants of the healthcare personnel at two radiotherapy departments regarding a new working method on a proposed system with mobile technology. A mockup was performed to present the proposed system and tested by the target end users with a tablet. With UCD as substrate, methods of observation, focus group and the gathered documents were used to create the proposed system. The proposed system was designed with a prototyping tool and carried out based on the same paper forms from the gathered documents that the users are familiar with. Before the testing, every participant received from the author verbal information about the study and consent rules, as well as verbal instruction about how to do the test. During the testing, every participant did every task with think aloud method according to the author's instruction. Informal interviews were conducted in the meanwhile. The author observed, interviewed the responders and noted the answers. Thematic analysis [56, 57] was used to analyze the collected feedback.
3.1 Design The first and second phases before design phase in UCD process is to identify and to meet the users' goals in order to let the mockup to be successful: who would start or use the proposed system, who would use, supply or remove patient information, what will the user use the proposed system for and which elements should be included in the proposed system to support the healthcare personnel's workflows. [41] 3.1.1 The Elements for Design Which elements should be included in the proposed system to support the healthcare personnel's workflows? The elements for design were collected from the paper forms from both radiotherapy departments at SUS and Radium Home. The paper forms are the paper radiation treatment cards and verification protocol (section 1.4.6 & 1.5.3) for documentation, as check list and as support material during delivering radiotherapy to patients. The forms were examined and studied for exploration and selection of important elements for being in the mockup design. The designs were based on the same paper cards that the users are familiar with in order to have user-friendly approaching. 3.1.2 The Users The users are “the set of people who will use the system, playing the roles defined by the actors” [58]. The relationships between the users and the proposed system were considered: Who would start or use the proposed system? Who would use, supply or remove patient information? What will the user use the proposed system for? The followed user scenarios are the blue prints to the design for the proposed system.

32
3.1.3 Scenarios Scenario is “a description of what could possibly happen” [59]. It’s a part of the design process, it’s a vehicle to communicate between the designer and the users. It helps the designer to create new ideas, to understand the users’ reflection and action in iterative user-centered design process. It’s a media of thinking and communication that takes place in design. [60] 3.1.3.1 User Scenario of Nurse and Medical Physicist Breast cancer patient A has a radiotherapy start at treatment room 2 at 10.20. Nurse B gets information from the appointment scheduling in oncology information system, Aria (section 1.2.1), that the patient is waiting outside the treatment room. Nurse B picks out the folder (Fig.2, block 14) of treatment information for the patient from a drawer in the treatment control room. Afterwards, she goes out with the folder to meet and show the patient into the treatment room. Nurse B checks the patient’s id number, diagnosis, treatment area and introduces the radiotherapy process (Fig.2, block 15 & 16) for the patient according to the patient information in her hand. Nurse C comes into the room to help nurse B to setup the patient on the treatment couch (Fig.5). Both nurses check patient id, treatment and setup parameters according to information in the paper treatment sheets (Fig. 14 & 15), they also check the treatment area and dose distribution according to the image sheet (Fig.16). Medical physicist D is also in the room for a start to check all treatment parameters, treatment area, dose distribution and the patient’s position according to the information sheets (Fig.2, block 20). He needs to give the approval for the quality assurance checks before the first treatment. Thereupon the first treatment can be delivered. 3.1.3.2 User Scenario of Physician Physician E comes into the images checking room. There’re many setup (verification) protocols (Fig.12 & 15) needed to be checked. The protocols are put in two different trays, one tray is for breast cancer patients and the other one is for the other kinds of cancer patients such as prostate cancer, lung cancer and so on. Physician E chooses one sheet from breast cancer tray. Subsequently she goes into the oncology information system (section 1.2.1) to check the images from CT (Fig.2, block 6) and the mapping from the treatment room (Fig.6) according to the patient information in the setup protocol sheet. She needs to see if there’s a big difference between the images. Fortunately the deviation between the images is within tolerance. So she writes comment in the setup protocol sheet: “nice picture, well done!”. She thereon signs and ticks in the box (Fig.15, p.3): no more picture before each treatment. 3.1.4 Indigo Studio An ideal mockup tool for the proposed system should include interaction functions of writing, touching, changing information, checking off, scrolling, links, covering different colors for different categories or area and so on. Furthermore the proposed design should be presented for the participants with a mobile device, i.e., a tablet to make it like real in the future. Hence

33
the mockup should be simulated by the participants via Wi-Fi. Indigo Studio of Infragistics [61] was chosen for interaction prototyping. Indigo Studio mockup tool had many different icons, forms and functions to choose, it was quite easy to use, to design, to click to create new screen state and so on. The designed interfaces are described in the followed section, 3.4.4 Interfaces. 3.1.5 Interfaces This initial prototype was designed based on the paper treatment cards, setup protocols, images sheet and the user scenarios. 3.1.5.1 Log On Interface The proposed system was an idea to support healthcare work of nurses, physicians and medical physicists in relating to RT treatments. Hence the log on interface was designed with three different personnel categories for logging on. The end user should fill in her/his own employ id-code and password. (Fig.20) 3.1.5.2 Appointment Scheduling Interface This interface described lists with patients' appoitments for treatments in different room for a day. The interface was only created with 2 treatment rooms for choosing to motivate 12 LINAC at SUS and 8 LINAC at Radium home respectively.(Fig.21) The idea was all information of a patient would be retrieved and followed to the chosed patient when a patient in the lists was chosen and screentouched. 3.1.5.3 Diagnosis and Setup Parameters Interface From this interface, the healthcare personnel could view the patient's personal information and study different information about the patient's treatment, such as diagnosis, target, treatment dose, setup, radiation energy and so on. (Fig.22) 3.1.5.4 Treatment Beam (Dose) Planning Interface A screenshot symbolized even an advanced connection between the proposed system and the existing treatment planning system for retrieving dose distribution over the treatment target (Fig.23). 3.1.5.5 Verification Protocol Form Interface Verification protocol form is used as a manner to control the patient's position. This interface provided places for nurses, physicians and medical physicists to retrieve, write, choose, supply, give comments, remove, correct and document any information around patient's setup and sign for the comments/instructions (Fig.24).

34
3.1.5.6 Categories Interface Categories of type of cancer patients including breast patients and others was for the use of the physicians and/or medical physicists to choose a category of patient for going further to a patient list (Fig.25). 3.1.5.7 Breast Patients Interface Patient list showed up after fingertouching on a patient category. This was also for the use of the physicians and/or medical physicists. After fingertouching on a patient in the list, a verification protocol form with saved information belonging to the chosen patient would show up. Thereupon the physicians and/or medical physicists can retrieve, write, choose, supply, give comments, remove, correct and document any information around patient's setup and sign for the comments/instructions (Fig.26). 3.1.5.8. Workflows Workflows of the proposed system for the healthcare personnel are as Figure 27. The purple workflow is designed for nurses and medical physicists. After they log into the system, they can choose a patient and thereon an interface which is belonging to the patient will be pop-up accordingly. They can switch to Appointment Scheduling interface again and choose another patient. They can also log out in any interface. The blue workflow is suitable for physicians and medical physicists. After they log into the system, they can choose a category, thereupon a patient. Afterwards, they can switch to any interface which is belonging to the patient accordingly. They can switch to Breast Patients interface and choose another patient, or switch to Categories interface and choose another category. They should be able to log out in any interface, but the author forgot the log out element in interfaces of Categories (Fig.25) and Breast Patients (Fig.26).
Figure 20.-Log On

35
Fig.21-Appointment Scheduling Fig.22.-Diagnosis & Setup
Fig.23.-Images Fig.24.-Verification Protocol

36
Fig.25.-Categories Fig.26.-Breast Patients
Figure 27.-Workflows

37
3.2 Settings and Participants The study sites were at RT Departments at SUS in Lund and Radium home at KS in Solna, Stockholm. In order to get general opinions on the mockup testing for the proposed system, the researcher recruited volunteers at both radiotherapy departments. Time and place for representing the template proposals were determined and settled between the researcher and the participants a few weeks before performances. Every participant simulated the proposed system with a tablet.
In order to avoid function disorder on the tablet and Wi-Fi during any testing, a simulation on the proposed system was double checked by the researcher before each testing. The testings were performed at varied places, such as treatment control room or staff room, where the Wi-Fi was working since the mockup presentation should work like a real system as much as possible.
The RT Department at SUS has 12 LINAC, about 60 nurses and about 30 to 40 patients per treatment room a day. The nurse-to-patient ratio per day ranges from 1:6 to 1:8. Or 1:10 to 1:13 when it's only three nurses at one treatment room. The daily ratio of physician-to-treatment room and medical physicists-to-treatment room ranges from 1:12 or 1:6. Though, there are also backup physicians and medical physicists who can help the nurses and the patients.
The RT Department at Radium home has 8 LINAC (7 in operating and 1 as backup), about 40 nurses and about 30 patients per treatment room a day. The nurse-to-patient ratio is about 1:6 or 1:10 when it's only 3 nurses at a treatment room. The ratio of physician-to-treatment room and medical physicists-to-treatment room is as same as the department at SUS, it ranges from 1:12 or 1:6. There are also backup physicians and medical physicists who can help the nurses and the patients.
Ascribable to the aforementioned heavy workload of the healthcare personnel, it was a challenge to recruit volunteers to the testing. In order to fulfil the tests, the author needed to adapt with the volunteers schedule. Varied roles (nurse, physician and medical physicist) at the radiotherapy departments were purposefully selected to participate this study. There were total ten volunteers took part in the testing, five of them were nurses, three were medical physicists and two were physicians. (Table 1)
Table 1.-Participants Nurse Medical Physicist Physician Group demonstration SUS 3 1 0 -- -- Radiuhemmet 2 2 2 Group 1 Group 2 Remarks: Group 1: 1 physician, 1 medical physicist, 1 nurse, 2 engineers and 2 purchasers Group 2: 3 nurses

38
3.3 Data Collection for The Study 3.3.1 Data Collection Strategy
This research is a qualitative case study. Due to the limitation of amount of participants, this study was designed to use qualitative method to analyze the data. The case "the feasibility of supporting radiotherapy workflows through the use of mobile devices" should be determined under the study. According to Mason, qualitative method can collect different types of data, such as feelings, experiences, opinions, needs desires and so on [62]. Qualitative case study could be "a valuable method for health science research to develop theory, evaluate programs, and develop interventions" [63]. The method provides the novice research "an excellent opportunity to gain tremendous insight into a case" [63]. 3.3.2 Prerequisites for The Study Activities Since this study was constrained in a specific area and the workloads of the potential participants to test the designed system are overloaded, the author recruited volunteers to participate this study to avoid risk of failing or unexpected problems. The researcher believed that to recruit the volunteers to participate in the study at both radiotherapy departments, Skånes University Hospital in Lund and Radium home at Karolinska University Hospital in Solna in Stockholm, could give more general opinions. Hence participants should be recruited at both departments. Varied roles (nurse, physician and medical physicist) from the departments should be purposefully selected to participate in the study. Thereupon schedules and sites for testing the proposed design should be set up according to the agreements between the author and the volunteers. Wi-Fi should work for simulation at the sites. The testing sites should be at the respective places. As well as data for design elements should be also collected at both radiotherapy departments. User interfaces should be user-centered designed with a prototyping tool to visualize the proposed system according to the form of the paper treatment cards gathered from the departments and the potential users’ needs during their workflows. Think aloud testing, observation, informal interviews and feedback were used to test the proposed design to discuss flexibility of mobile technology (i.e. tablets) to support radiotherapy workflows. The research questions should be discussed during the testing. Thematic analysis should be used to analyze the collected data from the testing.
3.4 Data Collection Method for The Template Proposals According to usability.gov, there are no exact specified methods for each phase in UCD process (Fig.18) [41]. Based on the UCD life cycle from usability.gov, the author consequently carried out a UCD process with methods of observation, focus group and the gathered documents (paper protocol forms) to collect data for the template proposals for this study. In Figure 28, methods of data collection from paper forms and observation were used to meet the general principal for the phase of “Specify Context of Use” in UCD life cycle from usability.gov. Focus group was used to correspond to the phase of “Specify

39
Requirements”. Create prototype was used to stand for the phase of “Produce Design Solutions” and Mockup testing was used to meet the phase of “Evaluate Designs”.
Figure 28.-Data collection methods (data collection from paper forms, observation & focus group) for design were used in this study to meet the general UCD phases from usability.gov.
3.4.1 Documents
In order to exemplify the initial prototype as resembled as possible to the paper documents, the elements for design were collected from the paper forms from both radiotherapy departments at SUS and Radium Home. The paper forms are the paper radiation treatment cards and verification protocol (section 1.4.6.4 & 1.5.3.2) for documentation, as check list and as support material during delivering radiotherapy to patients. The forms were examined and studied for exploration and selection of important elements for being in the mockup design. The prototyping was designed based on these paper forms that the users are familiar with in order to have user-friendly approaching. 3.4.2 Observation With observation the researcher could understand how the users for the proposed system manage and work with the patient paper treatments cards and protocols. The author capitalized the context of users’ use by working with the therapists in February, 2016 in order to observe the users’ working attitudes and needs. Scenario descriptions from observations were delineated in Sections 3.1.3.1 and 3.1.3.2.
3.4.3 Focus Group
Focus group is a simple, quick and effective technique to discuss different perceptions and identify needs of staff. It is customarily a small group discussion and has advantages for a researcher in the field of health and medicine to generate data. [64] The author spontaneously discussed with four therapists at one treatment control room about the idea of using mobile

40
device to support their workflow and a simple picture in words about the template proposals. All of them did feel it was an interesting idea and support the author’s overture.
3.5 Ethical Consideration Ethics [65] is to respect and protect the rightness of an individual and/or the individual’s conduct. The author acted and worked with ethical consideration that she applied permission for doing the research at the RT departments. The author respected each participant’s time, condition and wish, that every participant was allowed to change time for simulating the mockup. All the participants received oral information about the study from the author according to the consent form (Appendix V). All the volunteers were allowed to request more information about the study or interrupt or cancel the participation. She protected and dealt with each answer, opinion, feedback and result in right, careful manner and confidentially. So that none of the participants’ identities was revealed and this study represented with real value from the outcome. The author also respected and protected any patient’s personal details so that no patient information was exposed on any collected data.

41
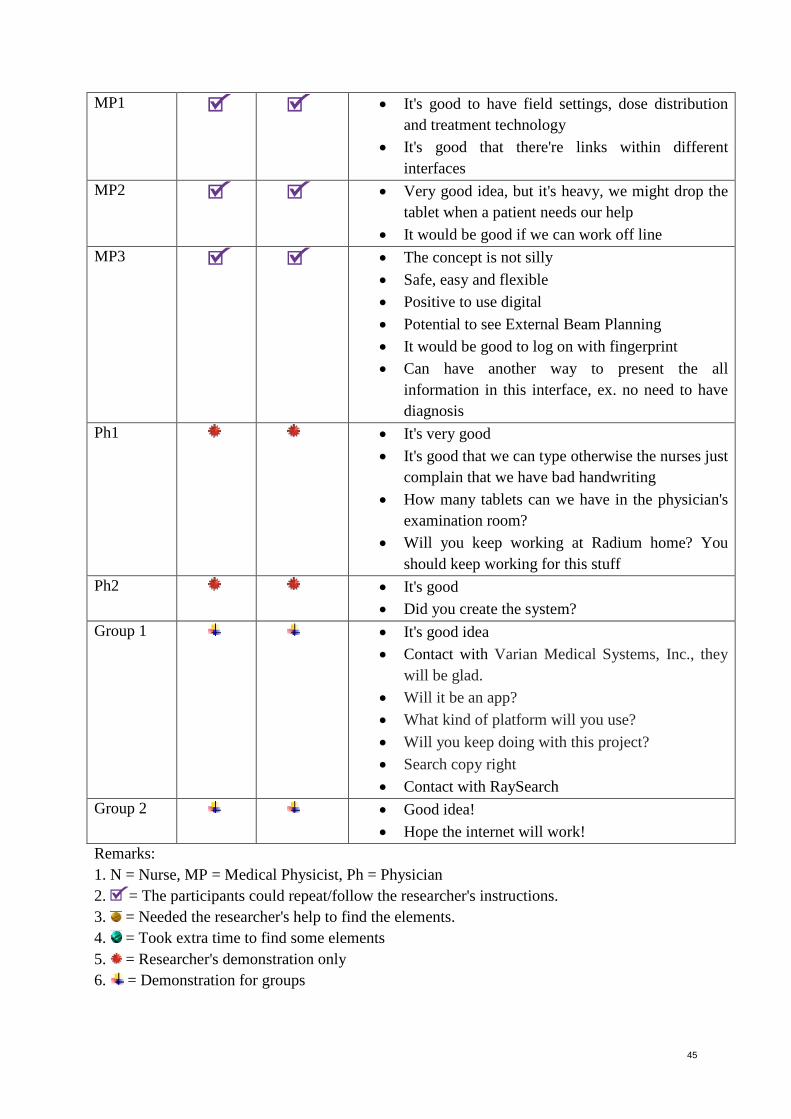
4. RESULTS This research was a qualitative case study. The motivation to this study was from a question of how to resolve the problem of patient paper treatment cards for RT departments after the author’s observations and experiences. The author had a suggestion to figure out a secure method to retrieve and preserve patient information. Everything started with the author's study, Scientific Communication and Research Methodology HT2015 – Period C, D, at DSV at Stockholm University. This study was a continue work from previous research (Section 1.9 & Appendix I-IV). In consideration of most of the participants, 76 %, from the previous research were positive to the suggestion of using patient treatment protocols with mobile technology in tablet form while deliver RT treatments to patients, the present research focused on presenting a proposed electronic patient treatment parameters on a tablet with a mockup and focused on investigating the feasibility of the suggestion. Based upon an explicit understanding of the target end users, the template proposals to represent an electronic treatment plan (user interfaces) on a tablet were carried out with a prototyping tool pursuant to the data collection from documents, observation and focus group. Furthermore the designs were based on the same paper cards that the users are familiar with in order to have user-friendly approaching. Simulations of how the processes would change to the end users were performed at Radiotherapy Departments at Skånes University Hospital in Lund and Radium Home at Karolinska University Hospital in Stockholm. The results of the present research were gathered from think aloud, observations, informal interviews and feedback from the participants during the testing of the proposed system with a mockup on a tablet. 10 volunteers participated the testing, 5 nurses, 3 medical physicists and 2 physicians took part in the mockup testing (Table 1). Subsequently, when it said the author had a good idea and good design for them to work without paper treatment protocols in the near future, they invited the author to demonstrate the workflow function on a tablet. Their feedback will be presented and considered here under but will not be included into the results. Nevertheless, the author can conclude that the interfaces design reached user-friendly approaching upon the feedback.
4.1 Think Aloud and Observations Most of the participants could follow and repeat the researcher's instructions and find the elements in different interfaces and do the tasks. Two participants had some problems and took an extra time to find some elements in the mockup. Only one participant needed the researcher's help to find the elements. Two participants needed the researcher to explain and demonstrate how the proposed system could work due to time constrains. (Table 2)

42
4.2 Informal Interviews and Feedback The feedback (Fig.29, 30 & Table2) from the unstructured interviews with the participants during the mockup testing will be divided into 3 parts: positive feedback, doubt and negative feedback, and suggestion feedback. 4.2.1 Positive Feedback The mockup design got significant positive feedback that every participant (10 of 10) felt it's a good idea to work with a tablet. The verbatim quotes from them were:
• Very good idea • Very nice design • The concept is not silly • Safe, easy and flexible • Positive to use digital • Potential to see External Beam Planning • It’s good with different colors for different things • It’s good to have beam settings, dose distribution and treatment technology • It’s good that there’re links within different interfaces • It's good that we can type otherwise the nurses just complain that we have bad
handwriting
Figure 29.-Feedback 1

43
Figure 30.-Feedback 2
4.2.2 Doubt and Negative Feedback The author got one negative feedback:
"It's heavy, we might drop the tablet when a patient needs our help." And one doubt feedback:
"Can internet work in the treatment rooms?" Notwithstanding every participant felt it was a good idea to have electronic patient treatment parameters in tablet form instead of paper form, the future system should take the small warnings in consideration.

44
4.2.3 Suggestion Feedback Nevertheless every participant felt it was a good idea to have electronic patient treatment parameters in tablet form instead of paper form, the author got diverse suggestion feedback on the designed elements in view of people has distinct perspectives on looking at objects. Those suggestions are as Figure 29, 30 and in Table 2. Table 2.-Results of mockup testing (including observation on participants' abilities on researcher's instructions and feedback) Participants Think
aloud Observation Feedback
N1 • Very good idea • Different colors for different situations • It would be better if there’s one more column with
symbols of different gantry angles N2 • Very good idea
• Should can show check off ( ) when the patient is completed her/his treatment for the day.
• Including how many days the patient has been treated.
• Place for signatures for treatment planning approved and plan created
N3 • Good idea • Need extra place for remarks/notes. • Can internet work in the treatment rooms?
N4 • Very good idea and very nice design • It's good with different colors for different things • No need to photo, address • Should put a title for the area • Should have different colors to show different
verification requirements with date. • It would be better with bold style for the figures. • Should show what type of bolus and the thickness
of bolus. If bolus is required, this column should turn to red for warning
• You can search copy right for the design N5 • It's good idea
• 1 CBCT/week • Need a place to note who has done the correction • You can contact with Innovation Dept. at KS for
further work.
45
MP1 • It's good to have field settings, dose distribution and treatment technology
• It's good that there're links within different interfaces
MP2 • Very good idea, but it's heavy, we might drop the tablet when a patient needs our help
• It would be good if we can work off line MP3 • The concept is not silly
• Safe, easy and flexible • Positive to use digital • Potential to see External Beam Planning • It would be good to log on with fingerprint • Can have another way to present the all
information in this interface, ex. no need to have diagnosis
Ph1 • It's very good • It's good that we can type otherwise the nurses just
complain that we have bad handwriting • How many tablets can we have in the physician's
examination room? • Will you keep working at Radium home? You
should keep working for this stuff Ph2 • It's good
• Did you create the system? Group 1 • It's good idea
• Contact with Varian Medical Systems, Inc., they will be glad.
• Will it be an app? • What kind of platform will you use? • Will you keep doing with this project? • Search copy right • Contact with RaySearch
Group 2 • Good idea! • Hope the internet will work!
Remarks: 1. N = Nurse, MP = Medical Physicist, Ph = Physician 2. = The participants could repeat/follow the researcher's instructions. 3. = Needed the researcher's help to find the elements. 4. = Took extra time to find some elements 5. = Researcher's demonstration only 6. = Demonstration for groups

46
5. DISCUSSION
5.1 Method Discussion This research was a qualitative case study to explore the feasibility of supporting radiotherapy workflows through the use of mobile devices. UCD process was used to collect data for the design and for the results of this study. Documents collection, observation and focus group were the methods to collect data for the design. Think aloud, observation and informal interviews were used to gather the participants' opinions on the designed mockup. The results showed positive responds on the proposal and the design.
5.1.1 What Were Good
Case study is “a situation in real life that can be looked at or studied to learn about something” [66]. Alike description of Baxter et al. that case study allowed the participants tell their stories and describe their views of reality, and the author to better understand the participants' actions [63]. The author did learn from the results that the participants were positive to the suggestion of working with mobile technology. From the different opinions, the author also learned how the interfaces of the proposed system should be improved to meet the users’ need in the future work.
User-centered design method was to identify and meet user goals to let the mockup to be successful. For instance, Steitz et al. stated that an outpatient whiteboard was successfully evolved and implemented in an oncology contest by following an iterative UCD process [67]. Nevertheless, there is no rigid method for each phase as stated in usability.gov. [41] Likewise Katsulis et al., they had Microsoft’s conventional UCD cycle as the underlying approach for their study. Moreover they stated users’ involvement in UCD process could vary based on the scenario. [42] Wherefore, for this study, documents collection, observation and focus group were conducted in UCD life cycle in order to identify users’ need. Focus group was also used in the study of Sundberg et al. considering the sample size and “group interaction could give a rich material” [27]. According to the feedback, “very nice design” and “Did you create the system?”, UCD methods were used in this study did help the author to make the mockup like a real system.
During the mockup testing, methods for data collection were think aloud, observation and informal interviews. With observation the researcher could understand how the participants follow the researcher's instruction and simulate the mockup. Think aloud method could be used to test a system at any stage, even at early stage of prototypes [68]. It's easy to use. The researcher could take notes while the participants doing their tasks and talks. The researcher could realize if a participant had a problem at a task according to her/his talk, on that occasion the researcher could help her/him to complete a task. In the same manner, Johnsen et al. used thinking strategies to identify actual and potential problems [69]. The researcher could get reasonable good findings on which design elements were user-friendly or not. It was also a good manner to compensate any missed observation period since the author was alone to present the mockup.

47
According to Johannesson et al. [70], interviews are the most common way to obtain "a large number of requirements in a short time", are good for a researcher to elaborate "a problem in an interactive and creative way". By Randolph's sight [71], interviews are good to gather "deep knowledge over a limited area". "Informal interviewing goes hand-in-hand with participant observation" [72].
Indigo Studio mockup tool had many different icons, forms and functions to choose, it was quite easy to use, to design, to click to create new screen state and so on. The ready work could be uploaded on a website for interactions with functions of writing, touching, changing information, checking off, scrolling, links, covering different colors for different categories or area and so on.
5.1.2. Limitation
There are many tools for interaction, wireframe and prototyping tools on the market. It was quite difficult and took time to choose a suitable one for the proposed system. In spite of Indigo Studio mockup tool had potential to act as a real system, there was one disadvantage that it did not have the function of changing information in table forms. The author needed to insert free text form into table form in order to have the function of writing or changing information for testing (Fig.31). Though, the disadvantage did not disturb the whole design and its presentation during testing since the author got feedback such as "very nice design" and "Did you create the system?". For the testing, time and the healthcare overloaded work were the biggest enemies to this research. Likewise the report from Yu et al., oncology nurses in China face heavy burdens of care for cancer patients [73]. One participant was forced to divide the testing into 2 parts, 4 persons changed their schedules a couple of times and 2 tested in quick ways. The author did not use audio or video, and she was alone to perform the testing. Hence few findings might be missed. Fortunately, the author also used informal interviews to recall the potential missing. Furthermore, the author had difficulty to find general themes to code the findings with thematic analysis method since every designed element was so important for the personnel's daily work and each participant has different views on the elements.
Figure 31.-Design with defect

48
5.2 Result Discussion This research was to survey the feasibility of supporting radiotherapy workflows through the use of mobile devices. Positive feedback was received. The results highlighted how the healthcare personnel were willing to change their current work methods with mobile electronic devices (MED). The results interpreted the impact of the use of MED and revealed a similarity to the study of De Bari et al. that their study rendered a picture of current perception on impact of MED during the physicians’ clinical activities [9]. The proposed system got significant positive responds from every participant (10 of 10). Coding for the main general collected data was "it's a good idea" to work with a tablet, which could be answered to the main question of this research: How do the healthcare personnel feel about managing electronic treatment cards on mobile devices? The author could also determine that this case was feasible to use electronic protocols for supporting workflows upon the phenomenon of the extra meetings and the special responds. Those special responds are such as:
• You can search copy right for the design. • You can contact with Innovation Dept. at KS for further work. • Will you keep working at Radium home? You should keep working for
this stuff. • Contact with Varian Medical Systems, Inc., they will be glad. • Will you keep doing with this project? • Contact with RaySearch [74]. • Did you create the system?
The advantages of using electronic treatment cards were:
• Positive to use digital • Safe, easy and flexible • It's good that we can type otherwise the nurses just complain that we
have bad handwriting The feedback revealed same approaches as De Bari et al. [9] and Sundberg et al. [27] that the use of this kind of innovations in clinical practice may introduce an important tool to support workflows to improve cancer care. Moreover the author got feedback on the prototype design that it was a nice design. Consequently the author can conclude that the interfaces design reached user-friendly approaching. The disadvantages of using electronic treatment cards were:
• Can internet work in the treatment rooms? • Hope the internet will work!

49
• But it's heavy, we might drop the tablet when a patient needs our help. Only 20% (2 of 10) participants were concerning the function of wireless computer network, the author construed the phenomenon as the majority people trusted current IT technology since it has tremendously exploded and improved in the last decades. Likewise the depiction of De Bari et al. that ICT has advanced so that tablets and smartphones are widely diffused worldwide. The 5th generation mobile networks (5G) might help to clear the doubt. 5G has a hundred times higher data rate than the 4G network, a thousand times more data sets, one-tenth response time, ten times longer battery life, a hundred times more connected gadgets, better reliability and 5G mobile devices can be connected with different base stations in the same time [75]. "1 gigabit per second to be offered simultaneously to many workers on the same office floor". "Signaling and spectral efficiency should be enhanced" Also "coverage and latency should be improved". [76] Regarding to the concern of tablet's weight could affect healthcare personnel's work, the author couldn't give the participant an appropriate reply. However, the author later on found one way might solve the problem as Figure 32 and 33. The method is to paste a holder with neoprene strap adjusts to fit any hand size in the back of a tablet and put in a holster to avoid dropping while helping a patient [77]. Then the researcher couldn't improve the designed mockup interfaces according to each suggested feedback by reason of time constrain of this research. Another reason was due to the researcher couldn't find the themes for coding with thematic analysis method since each participant had different views on the designed elements. Therefore the researcher leaves this discussion for Future Work.
Fig.32.-Tablet with holder [77] Fig.33.-Tablet with holder and holster [77]
5.2.1 Strengths and Weaknesses The author is studying in health informatics domain that she understands the workflows, processes and technical aspects, as well as knows how to interpret and transfer the collected data into design. Consequently the author did the best to ensure that there were no ambiguities on the methods to the design, the testing and the data collection to the results. On the contrary,

50
the expert aspects could be a weakness that the author might bias the collected data, might interpret the collected elements and/or the feedback in another way that the target end-users did not intend.
5.3 Future Work If the researcher follows the participants' suggestions to keep working with this project, first of all the researcher should contact with health informatics companies, such as Innovation Department at KS, Varian Medical Systems, Inc. and RaySearch, to discuss the possibility for the proposed system. The objects to be discussed are such as connections to oncology information system, registrations, platform and so forth. If it’s feasible to conduct the proposed system into tablets, this project should fulfill the entire UCD process. Subsequently, the second step would be “produce design solutions” [41] (Fig.18), i.e., a project leader and engineers should be employed to develop the proposed system. Thereupon the author’s designed elements could be reexamined, redesigned and improved. Afterwards, “evaluate designs” [41] (fig.18) should be performed. Thereafter, the system should be adjusted and evaluated until it’s satisfied by the end-users. The project could also hand over to any of the aforementioned companies for developing, evaluation and implementation. Another alternative is to authorize Cambio to develop this project in consideration of they had developed a comparable system like Nova Ward Tablet [78].

51
6. CONCLUSIONS ICT has evolved worldwide and been implemented in the field of radiation oncology over the last decades. Large amounts of information can be stored and sent digitally, which is time saving and radically reduces the risk of missed, lost or inaccurate information. Nevertheless, the two of the largest hospitals, SUS and KS, still use paper protocols. That is indefensible from a time, cost perspective and in term of patient safety. This research was to survey the feasibility of supporting radiotherapy workflows through the use of mobile devices. A mockup for the proposed system was presented for the healthcare personnel with a tablet through Wi-Fi. The testing was to suggest the healthcare personnel to use electronic treatment cards/protocols instead of paper form. Significant positive feedback on the template proposals was received from the 10 of 10 participated healthcare personnel who felt the suggestion of using electronic patient protocols instead of paper form was a good idea to support their workflows. Despite the disadvantage of a tablet might be heavy, they were impressed on the prototyping design. As well as the advantages of using electronic treatment cards were that it’s safe, easy and flexible to work with a tablet. The significant positive feedback highlighted how the healthcare personnel were willing to change their current work methods. Consequently the author could determine that this case was feasible. Nevertheless, in accordance with the suggestion feedback on the designed elements and IT technical solutions, there are manifold objects needed to redirect examination, to be verified and arrayed. There are such as connections to oncology information system, registrations, platform and so forth if the departments authentically desire to use electronic treatment cards/protocols instead of paper form. Aught the author believes that in the near future the time will be in and the dream will become true since mobile technology within healthcare system is going to be improved and moving toward standardized [79-80]. Such as Cambio has already developed COSMIC Nova Ward Tablet [78] and the Swedish telecommunication company, Ericsson, is working on 5G. The using of the proposed system will not blow up other mobile devices with 5G since 5G in the future will promise to offer many workers on the same office floor simultaneously.
ACKNOWLEDGMENTS The author thank much all the participants at Radiotherapy departments at SUS and Radium home with their valuable time to take part in this study and offer their opinions and suggestions on the design. Thank also their managers' supports to allow the author to do the research at the departments. As well as huge appreciation to the author's supervisor, Stefano Bonacina, who was so kind and had so much patience to guide and help the author to complete this research.

52
References:
1. IAEA, (2008), Setting Up a Radiotherapy Programme: clinical, Medical Physics, Radiation Protection and Safety Aspects, ISBN 92–0–101807–X, IAEA Library Cataloguing in Publication Data, International Atomic Energy Agency, Vienna.
2. WHO, (2016), Cancer, World Health Organization, Retrieved 2016-04-02 from http://www.who.int/cancer/en/
3. Jain, NL., and Kahn, MG., (1993), Clinical Decision-Support Systems in Radiation Therapy, Report Number: WUCS-93-14, All Computer Science and Engineering Research, DOI: 10.7936/K7GQ6W0V
4. WHO & uicc, (2005), Global Action Against Cancer - Updated version, ISBN 92 4 159314 8, World Health Organization and International Union Against Cancer,
5. Socialstyrelsen & Cancerfonden, (2013), Cancer in figures 2013 (Cancer i siffror 2013, ISBN: 978-91-89446-64-9.
6. Edvardsson, A., (2012). Evaluation of respiratory gating - dose sparing and set-up, the Department of Radiation Physics Malmö, Skåne University Hospital, Department of Medical Radiation Physics, Clinical Sciences, Lund University, Lund. Retrieved 2015-12-25 from https://lup.lub.lu.se/student-papers/search/publication/3327132
7. Mullins, K., (2015), Stereotactic Body Radiotherapy for Early-Stage Non-Small Cell Lung Cancer: When and Why Is It Appropriate Therapy?, University of Cincinnati College of Nursing and Oncology Hematology Care, Cincinnati, Ohio, J Adv Pract Oncol. 2015 Jul-Aug; 6(4): 351–354
8. Cancer Research UK, (2016), Let’s beat cancer sooner: Radiotherapy, What external beam radiotherapy is, Retrieved 2016-04-01 from http://www.cancerresearchuk.org/about-cancer/cancers-in-general/treatment/radiotherapy/
9. De Bari et al. (2016). The Pocketable Electronic Devices in Radiation Oncology (PEDRO) Project: How the Use of Tools in Medical Decision Making is Changing? Technology in Cancer Research & Treatment 2016, Vol.15(2) 365-376. DOI: 10.1177/1533034615572287.
10. Varian, (1999-2016), ARIA® Oncology Information System, Varian Medical Systems, Inc., Retrieved 2016-04-05 from https://www.varian.com/oncology/products/software/information-systems/aria-radiation-oncology
11. Elekta, (2015), MOSAIQ® Radiation Oncology, Elekta AB, Retrieved 2016-04-05 from https://www.elekta.com/software-solutions/care-management/mosaiq-radiation-oncology.html
12. Saint Luke’s Radiation Oncology Network, (2016), External Beam Radiotherapy (EBRT), Retrieved 2016-04-01 from http://stlukesnetwork.ie/treatments/treatment/radiotherapy.html

53
13. RadiologyInfo.org, (2016), Linear Accelerator (LINAC), Radiological Society of North America, Inc. (RSNA). Retrieved 2016-04-01 from http://www.radiologyinfo.org/en/info.cfm?pg=linac
14. Society of Radiographers, (2016), Radiotherapy staff, The Society and College of Radiographers. Retrieved 2016-04-01 from http://www.sor.org/about-radiography/patient-information/overview-radiotherapy
15. Hermitage Medical Clinic, (2014), Radiotherapy: What is radiotherapy?, Patient Pathway, Retrieved 2016-04-01 from http://www.hermitageclinic.ie/services-specialities/clinical-departments/radiotherapy-department/patient-pathway/
16. Genesys Hurley Cancer Institute, (2016), Radiation Oncology Services, Retrieved 2016-04-05 from http://www.ghci.org/?page_id=104
17. Strandman, J., (2009), Regulaitons on medical radiotherapy of Swedish Radiation Safety Authority (Strålsäkerhetsmyndighetens föreskrifter om medicinsk strålbehandling), Strålsäkerhetsmyndighetens författningssamling SSMFS 2008:33 13§, ISSN: 2000-0987, Strålsäkerhetsmyndigheten (Swedish Radiation Safety Authority), Stockholm.
18. Nadalin, W., (2010), Reproducibility of patient’s setup in radiotherapy, Radiol Bras. 2010 Jul/Ago;43(4):V–VI, Colégio Brasileiro de Radiologia e Diagnóstico por
19. Frøseth, TC., Strickert, T., Solli, KS., Salvesen, Ø., Frykholm, G., and Reidunsdatter, RJ., (2015), A randomized study of the effect of patient positioning on setup reproducibility and dose distribution to organs at risk in radiotherapy of rectal cancer patients, Radiation Oncology 2015 10:217, DOI: 10.1186/s13014-015-0524-3.
20. ICRU, (2015), Prescribing, Recording, and Reporting Photon Beam Therapy (Report 50), International Commission on Radiation Units & Measurements, Inc., MD 20841-3095 USA, Retrieved 2016-04-02 from http://icru.org/home/reports/prescribing-recording-and-reporting-photon-beam-therapy-report-50
21. Cancerfonden, (2015), Radiotherapy (Strålbehandling), Retrieved 2016-04-02 from https://www.cancerfonden.se/om-cancer/stralbehandling
22. Navarro-Martin, A., Cacicedo, J., Leaman, O., Sancho, I., Carcía, E., Navarro, V. and Guedea, F., (2015), Comparative analysis of thermoplastic masks versus vacuum cushions in stereotactic body radiotherapy, Radiation Oncology (2015) 10:176, DOI 10.1186/s13014-015-0484-7
23. van Beek, S., Mencarelli, A., Remeijer, P., Sonke, JJ., Rasch, CRN., Local interfractional setup reproducibility for 2 individual head and neck supports in head and neck cancer patients, Practical Radiation Oncology, Volume 4, Issue 6, November-December 2014, Pages 448-454. Elsevier B.V.
24. Johnston, MJ., (2006), Unintended overexposure of patient Lisa Norris during radiotherapy treatment at the Beatson Oncology Centre Glasgow in January 2006, Warranted Inspector appointed by the Scottish Ministers, ISBN 0-7559-6297-4, www.scotland.gov.uk

54
25. Fogarty, G., Morton, RL., Vardy, J., Nowak, AK., Mandel, C., Forder, PM., Hong, A., Hruby, G., Burmeister, B., Shivalingam, B., Dhillon, H. and Thompson, JF., (2011), Whole brain radiotherapy after local treatment of brain metastases in melanoma patients - a randomised phase III trial, BMC Cancer 2011, 11:142, DOI: 10.1186/1471-11-142.
26. Department of Health, (2013), Health Building Note 02-01: Cancer treatment facilities, GOV.UK, Retrieved 2016-05-01from https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/147860/HBN_02-01_Final.pdf
27. Sundberg, K., Langius-Eklöf, A, Blomberg, K. & Isaksson, AK. (2015). Feasibility of an interactive ICT-platform for early assessment and management of patient-reported symptoms during radiotherapy for prostate cancer. European Journal of Oncology Nursing 19 (2015) 523-528. http://dx.doi.org/10.1016/j.ejon.2015.02.013.
28. Falchook, A.D. et al. (2016). Use of mobile device technology to continuously collect patient-reported symptoms during radiation therapy for head and neck cancer: A prospective feasibility study. Advances in Radiation Oncology (2016) xx, 1-7. http://dx.doi.org/10.1016/j.adro.2016.02.001.
29. Maguire, R. et al. (2015). Development of a Novel Remote patient Monitoring System: The Advanced Symptom Management System for Radiotherapy to Improve the Symptom Experience of Patients With Lung Cancer Receiving Radiotherapy. Cancer Nursing. Volume 38(2), March/April 2015, p E37-E47. DOI: 10.1097/NCC.0000000000000150
30. Le Verre, C., Troccaz, J., Artignan, X., Bolla, M., (2005), Intensity-based registration of portal images for patient positioning in radiotherapy, TIMC Laboratory, La Tronche cedex & Radiotherapy department, Grenoble cedex, France, ResearchGate, Retrieved 2016-03-30 from https://www.researchgate.net/publication/253095258_INTENSITY-BASED_REGISTRATION_OF_PORTAL_IMAGES_FOR_PATIENT_POSITIONING_IN_RADIOTHERAPY
31. Edvardsson, A., Nilsson, MP., Amptoulach, S., and Ceberg, S., (2015), Comparison of doses and NTCP to risk organs with enhanced inspiration gating and free breathing for left-sided breast cancer radiotherapy using the AAA algorithm, Radiation Oncology (2015) 10:84, DOI 10.1186/s13014-015-0375-y, BioMed Central
32. Hatschek, T., (2013), Breast camcer, primary treatment: Postoperative radiotherapy (Bröstcancer, primärbehandling: Postoperative strålbehandling), Radiumhemmet, Karolinska Sjukhuset, internetmedicin.se. Retrieved 2016-04-02 from http://www.internetmedicin.se/page.aspx?id=829
33. World Health Organization, (2016), What is Ionizing Radiation?, Retrieved 2016-04-05 from http://www.who.int/ionizing_radiation/about/what_is_ir/en/index2.html

55
34. Stålprofil AB, (2014), Project idea #8: Radiotherapy Department Lund (Projekttips #8: Strålbehandlingen Lund), Retrieved 2016-05-01 from http://www.stalprofil.se/projekttips/projekttips-8-stralbehandlingen-lund/
35. Skånes universitetssjukhus, (2012), Radiotherapy concentrated to Lund (Strålbehandlingen koncentreras till Lund), Retrieved 2016-05-01 from https://www.skane.se/sv/Webbplatser/Skanes-universitetssjukhus/Nyheter/Arkiv/Nyheter-2012/Stralbehandlingen-koncentreras-till-Lund-/
36. Brachytherapy.com, (2016), What is TomoTherapy?, Cancer Treatment Centers of America, Retrieved 2016-05-01 from http://www.brachytherapy.com/tomotherapy.aspx
37. NCC. Radiotherapy Department, Lund (Strålbehandlingsklinik, Lund). Retrieved 2016-06-01 from http://www.ncc.se/vara-projekt/stralbehandlingsklinik-lund/
38. Medicinska Fakulteten, (2012), New radiotherapy equipment was inaugurated (Ny strålbehandlingsapparat invigdes), Lunds universitet. Retrieved 2016-05-01 from http://www.med.lu.se/klinvetmalmo/nyhetsarkiv/120309straalbehandl
39. Hagberg, H. (2016). Skeletal metastases (Skelettmetastaser). internetmedicin.se. Retrieved 2016-05-01 from https://internetmedicin.se/page.aspx?id=1563
40. Nordisk familjebok (2015). Radiumhemmet, pp 891-892. Uggleupplagan. 22. Possession - Retzia. Retrieved 2016-05-01 from http://runeberg.org/nfcb/0466.html
41. usability.gov (2016). What & Why of Usability: User-Centered Design Basics. U.S. Department of Health & Human Services. Retrieved 2016-05-17 from http://www.usability.gov/what-and-why/user-centered-design.html
42. Katsulis, Z., Ergai, A., Leung, WY., Schenkel, L., Rai, A., Adelman, J. et al. (2016). Iterative user centered design for development of a patient-centered fall prevention toolkit, Applied Ergonomics 56 (2016) 117-126, Elsevier Ltd., http://dx.doi.org/10.1016/j.apergo.2016.03.011
43. Schnall, R., Rojas, M., Bakken, S., Brown III, W., Carballo-Dieguez, A., Carry, M. et al. (2016). A user-centered model for designing consumer mobile health (mHealth) applications (apps). Journal of Biomedical Informatics 60 (2016) 243-251, Elsevier Inc., http://dx.doi.org/10.1016/j.jbi.2016.02.002
44. Vredenburg, K., Mao, JY., Smith, PW., Carey, T. (2002). A survey of User-Centered Design Practice. CHI 2002, April 20-25, 2002, Minneapolis, Minnesota, USA, ACM 1-58113-453-3/02/0004
45. Joffer, J., Jerdén, L., Öhman, A., Flacking, R. (2016). Exploring self-rated health among adolescents: a think-aloud study. BMC Public health (2016) 16:156, DOI 10.1 186/s 12889-016-2837-z
46. Marley, S., Bekker, H.L. & Bewick, B.M. (2016). Responding to personalized social norms feedback from a web-based alcohol reduction intervention for students:
56
Analysis of think-aloud verbal protocols, Psychology & Health, DOI: 10.1080/08870446.2016.1161192
47. Pinnock, R., Fisher, TL., Astley, J. (2016). Think aloud to learn and assess clinical reasoning, Medical Education, Volume 50, Issue 5, Pages 585-586, DOI: 10.111/medu.13006
48. Tebold, I., (2004), Patient record's digital development (Patientjournalens Digitala Utveckling), Handelshögskolan, Göteborgs universitet, Retrieved 2016-02-01 from https://gupea.ub.gu.se/bitstream/2077/1186/1/Nr_7_IT.pdf
49. The Anglia Cancer Network (AngCn), (2016), Clinical protocols: Breast RT Protocol (AngCN-CCG-RT8_v2 BREAST protocol.pdf), Head & Neck Radiotherapy Protocol (AngCN-CCG-RT11_v0 2[4).pdf) and so on, Retrieved 2016-03-30 from http://www.angcn.nhs.uk/network-groups/ccgs/radiotherapy/documents/clinical-protocols.aspx
50. Gustafsson, T., Moller, TR. And Nordberg, UB., (1973), BEKO – A system for documentation of external beam treatment in radiotherapy, Departments of Radiation Therapy and of Radiation Physics, University Hospital, S-22185 Lund, Sweden, Computer Programs in Biomedicine 3 (1973) 135-144, North-Holland Publishing Company
51. HealthIT.gov, (2013), What is an electronic health record (HER)? Retrieved 2016-04-01 from https://www.healthit.gov/providers-professionals/faqs/what-electronic-health-record-ehr
52. Johnston, AM., (2006), Unintended overexposure of patient Lisa Norris during radiotherapy treatment at the Beatson Oncology Centre, Glasgow in January 2006, Warranted Inspector appointed by the Scottish Ministers, ISBN 0-7559-6297-4, Retrieved 2016-03-30 from http://www.gov.scot/Resource/Doc/153082/0041158.pdf
53. Fayers, PM., Hopwood, P., Harvey, A., Girling, DJ., Machin, D. and Stephens, R., (1997), Quality of Life Assessment in Clinical Trials-Guidelines and a Checklist for Protocol Writers: the U.K. Medical Research Council Experience, MRC Cancer Trials Office, European Journal of Cancer Vol.33, No.1, pp. 20-28, Elsevier Science Ltd.
54. Braun, R., Catalani, C., Wimbush, J., Israelski, D., (2013), Community health workers and mobile technology: a systematic review of the literature, PLoS One. 2013 Jun 12;8(6):e65772. doi: 10.1371/journal.pone.0065772. Print 2013.
55. Pryss, R., Mundbrod, N., Langer, D., Reichert, M. (2014), Supporting medical ward rounds through mobile task and process management, Inf Syst E-Bus Manage (2015) 13:107-146, DOI 10.1007/s10257-014-0244-5, Springer-Verlag Berlin Heidelberg 2014
56. Braun, V. and Clarke, V., (2006), Using thematic analysis in psychology, Qualitative Research in Psychology, 3 (2). pp. 77-101. ISSN 1478-0887, Retrieved 2015-12-02 from http://eprints.uwe.ac.uk/11735/2/thematic_analysis_revised

57
57. Wannheden, C., Westling, K., Savage, C., Sandahl, C. & Ellenius, J. (2013). HIV and tuberculosis coinfection: a qualitative study of treatment challenges faced by care providers, Int J Tuberc Lund dis 17 (8): 1029-1035, http://dx.doi.org/10.5588/ijtld.12.0446
58. Bittner, K. & Spence, I. (2008). Use Case Modeling (p.16). Addison-Wesley, ISBN: 0-201-70913-9
59. Scenario. (n.). Merriam-Webster's Learner's Dictionary, An Encyclopӕdia Britannica Company. Retrieved 2016-05-30 from http://www.merriam-webster.com/dictionary/scenario
60. Bødker, S. (2000). Scenarios in user-centred design – setting the stage for reflection and action. Department of Computer science, University of Aarhus, Denmark. Interacting with computers 13 (2000) 61-75, doi:10.1016/S0953-5438(00)00024-2
61. Infragistics. (2016). Indigo Studio Trial Version, Retrieved 2016-02-15 from http://www.infragistics.com/products/indigo-studio
62. Mason, M., (2010), Sample Size and Saturation in PhD Studies Using Qualitative Interviews, Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 11(3), Art. 8, http://nbn-resolving.de/urn:nbn:de:0114-fqs100387.
63. Baxter, P. & Jack, S. (2008). Qualitative Case Study Methodology: Study Design and Implementation for Novice Researchers. The Qualitative Report Volume 13 Number 4 December 2008 544-559, http://www.nova.edu/ssss/QR/QR13-4/baxter.pdf Kitzinger, J. (1995). Qualitative research. Introducing focus groups. BMJ 1995;311:299-302
64. Kitzinger, J. (1995). Qualitative research. Introducing focus groups. BMJ 1995;311:299-302
65. ethics. (n.d.). Dictionary.com Unabridged. Retrieved 2016-05-10 from Dictionary. com website http://www.dictionary.com/browse/ethics
66. Case study. (n.). Merriam-Webster. Retrieved 2016-06-10 from http://www.merriam-webster.com/dictionary/case%20study
67. Steitz, BD., Weinberg, ST., Danciu, I. & Unertl, KM. (2016). Managing and Communicating Operational Workflow: Designing and Implementing an Electronic Outpatient Whiteboard. Appl Clin Inform. 2016 Feb 3;7(1):59-68. doi: 10.4338/ACI-2015-07-CR-0082. eCollection 2016.
68. Nielsen, J. (2016). Thinking Aloud: The #1 Usability Tool. NN/g Nielsen Norman Group. Retrieved 2016-05-05 from https://www.nngroup.com/articles/thinking-aloud-the-1-usability-tool/
69. Johnsen, HM., Slettebø, Å. & Fossum, M. (2016). Registered nurses’ clinical reasoning in home healthcare clinical practice: A think-aloud study with protocol analysis. Nurse Education Today 40 (2016) 95-100. http://dx.doi.org/10.1016/j.nedt.2016.02.023

58
70. Johannesson, P. & Perjons, E. (2014). An Introduction to Design Science: Research strategies and methods, pp 39-73. Springer Link, DOI 10.1007/978-3-319-10632-8_3, ISBN 978-3-319-10632-8.
71. Randolph, J. (2008). Multidisciplinary Methods in Educational Technology Research and Development: Chapter 4 Data Collection in Educational Technology Research. HAMKin e-julkaisuja 1/2008. ISBN 978-951-784-456-7 (PDF)
72. Cohen, D. & Crabtree, B. (2006). "Qualitative Research Guidelines Project." July 2006. http://www.qualres.org/HomeInfo-3631.html
73. Yu, H., Jiang, A. & Shen, J. (2016). Prevalence and predictors of compassion fatigue, burnout and compassion satisfaction among oncology nurses: A cross-sectional survey. International Journal of Nursing Studies. Volume 57 (2016) 28-38. doi:10.1016/j.ijnurstu.2016.01.012
74. RaySearch Laboratories AB (2015). Advancing Cancer Treatment. Retrieved 2016-05-01 from http://www.raysearchlabs.com/about/About-RaySearch/
75. Ahlbom, H. (2016). The solution that makes 5g efficiently (Lösningen som gör 5g effektivare). NyTeknik. Retrieved 2016-05-10 from http://www.nyteknik.se/nyheter/losningen-som-gor-5g-effektivare-6336332
76. Wikipedia (2016). 5G. Retrieved 2016-05-10 from https://en.wikipedia.org/wiki/5G
77. handeholder.com (2011). Universal tablet - Holding solutions. Bums Computer Services & Handeholder Products Inc. Retrieved 2016-05-10 from http://www.handeholder.com/
78. cambio.se (2016). COSMIC Nova Ward Tablet. Cambio Healthcare Systems. Retrieved 2016-05-10 from http://www.cambio.se/index.php/cambio-cosmic/cosmic-nova-ward-tablet-2/
79. Cadenhead, C.D. (2016). What Will the ICU of the Future Look Like. Society of Critical Care medicine. Retrieved 2016-05-17 from http://www.sccm.org/Communications/Critical-Connections/Archives/Pages/What-Will-the-ICU-of-the-Future-Look-Like.aspx
80. McHugh, M., Van Dyke, K., McClelland, M. & Moss, D. (2011). Improving Patient flow and Reducing Emergency Department Crowding: A Guide for Hospitals. U.S. Department of Health and Human Services. Agency for Healthcare Research and Quality. AHRQ Pub. No. 11(12)-0094. www.ahrg.gov

59
Appendix I-Consent/Questionnaire (Previous Research) Consent form and Questionnaire for previous research for a study for Scientific Communication and Research Methodology HT2015 – Period C, D at DSV at Stockholm University:
Dear participant,
I’m Ying-Ying Yang Öhlin, I’m now engaging in a study of researching the acceptance of using computerized tablet for documentation of patients’ radiotherapy treatments since it’s proved that mobile technology provided improved quality of health services. The idea of using mobile technology is to secure patients’ safety and facilitate healthcare work efficiently. For getting appropriate data, the idea participants are those who work and/or have worked at a radiotherapy department. Every single part of this participation in the study is complete confidentiality. Your name will not be presented in the study. You are voluntary to take part in this study and you are free to declare off from this study at any time without giving any reason. If you have any question about the project, you’re welcome to contact me.
Sincerely yours,
Ying-Ying Yang Öhlin, [email protected]
Questionnaire
1. Gender: ○ Male……… ○ Female……..
2. Age: …………….
3. What’s your position at radiotherapy department?
○ Nurse…………. ○ Nurse assistant ………….
○ Physician………….. ○ Medical physicist ……………
4. How many years have you worked at radiotherapy department? …………………
5. Does the radiotherapy department use paper patient treatment cards for giving treatments to patients? ○ Yes ………… ○ No …………
6. How many years have the kind of treatment cards been used? ...................
7. What’s the purpose to use paper patient treatment cards? …………………………………………………………………………………. ………………………………………………………………………………….
8. Are you satisfied with the paper patient treatment cards?
○ 1….. ○ 2…….. ○ 3…… ○ 4……. ○ 5…………
(1 = not satisfied at all, 5 = Very satisfied)
Comments (optional): …………………………………………………………… ………………………………………………………………………………….....

60
9. Do you experience any paper patient treatment card got disappeared or became forgotten somewhere? ○ Yes ……. ○ No …...
10. How often do you experience that? ………………….
11. Do you feel anxiety when a paper patient treatment card is disappeared or became forgotten somewhere? ○ Yes……….. ○ No…………
Comments (optional): ...............................................................................................
12. Do you feel it’s harmful for patients when a paper patient treatment card is disappeared or became forgotten somewhere? ○ Yes ………. ○ No ………….
Comments (optional): …………………………………………………………. …………………………………………………………………………………..
13. How often do you use mobile technology in your days? …………………...
14. Do you feel anxiety when you use mobile technology?
○ Yes …….. ○ No ……..
15. Can you imagine using mobile technology (tablet) at work?
○ Yes …….. ○ No ………..
Comments (optional): …………………………………………………………... ………………………………………………………………………………….....
16. It said mobile technology provided opportunities to improve the quality of healthcare services. How do you think? ………………………………………………………………………………….. …………………………………………………………………………………..
17. Will you accept to conduct paper patient treatment cards into mobile technology with tablets as substrate (som underlag) for giving radiotherapy treatments to patients?
○ Yes…….. ○ No ………..
Comments (optional): …………………………………………………………… ………………………………………………………………………………….....
18. Do you think it’s safe to use mobile technology (tablet) at a radiotherapy department?
○ Yes …… ○ No ……….
Comments (optional): .............................................................................................
.................................................................................................................................
19. Can you imagine the use of mobile technology (tablet) at a radiotherapy department will secure patients’ safety and facilitate healthcare work efficiently?
○ Yes.………. ○ No…………
Comments (optional): …………………………………………………………… .………………………………………………………………………………….....
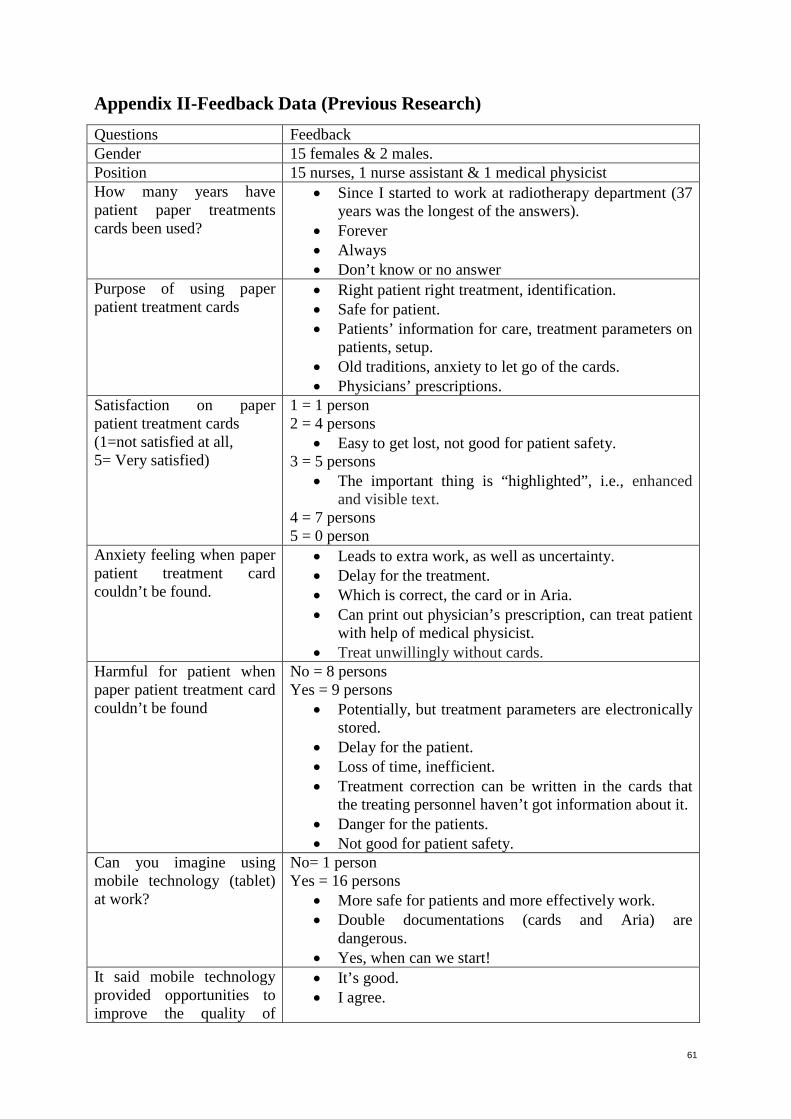
61
Appendix II-Feedback Data (Previous Research) Questions Feedback Gender 15 females & 2 males. Position 15 nurses, 1 nurse assistant & 1 medical physicist How many years have patient paper treatments cards been used?
• Since I started to work at radiotherapy department (37 years was the longest of the answers).
• Forever • Always • Don’t know or no answer
Purpose of using paper patient treatment cards
• Right patient right treatment, identification. • Safe for patient. • Patients’ information for care, treatment parameters on
patients, setup. • Old traditions, anxiety to let go of the cards. • Physicians’ prescriptions.
Satisfaction on paper patient treatment cards (1=not satisfied at all, 5= Very satisfied)
1 = 1 person 2 = 4 persons
• Easy to get lost, not good for patient safety. 3 = 5 persons
• The important thing is “highlighted”, i.e., enhanced and visible text.
4 = 7 persons 5 = 0 person
Anxiety feeling when paper patient treatment card couldn’t be found.
• Leads to extra work, as well as uncertainty. • Delay for the treatment. • Which is correct, the card or in Aria. • Can print out physician’s prescription, can treat patient
with help of medical physicist. • Treat unwillingly without cards.
Harmful for patient when paper patient treatment card couldn’t be found
No = 8 persons Yes = 9 persons
• Potentially, but treatment parameters are electronically stored.
• Delay for the patient. • Loss of time, inefficient. • Treatment correction can be written in the cards that
the treating personnel haven’t got information about it. • Danger for the patients. • Not good for patient safety.
Can you imagine using mobile technology (tablet) at work?
No= 1 person Yes = 16 persons
• More safe for patients and more effectively work. • Double documentations (cards and Aria) are
dangerous. • Yes, when can we start!
It said mobile technology provided opportunities to improve the quality of
• It’s good. • I agree.
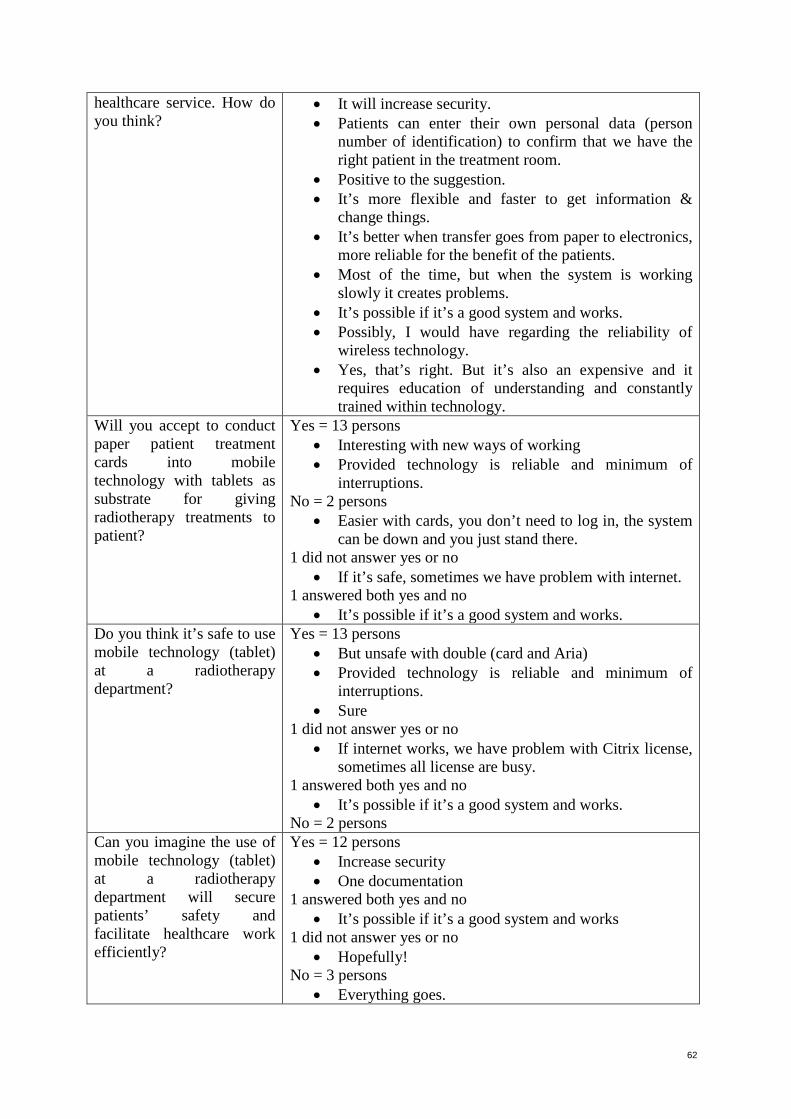
62
healthcare service. How do you think?
• It will increase security. • Patients can enter their own personal data (person
number of identification) to confirm that we have the right patient in the treatment room.
• Positive to the suggestion. • It’s more flexible and faster to get information &
change things. • It’s better when transfer goes from paper to electronics,
more reliable for the benefit of the patients. • Most of the time, but when the system is working
slowly it creates problems. • It’s possible if it’s a good system and works. • Possibly, I would have regarding the reliability of
wireless technology. • Yes, that’s right. But it’s also an expensive and it
requires education of understanding and constantly trained within technology.
Will you accept to conduct paper patient treatment cards into mobile technology with tablets as substrate for giving radiotherapy treatments to patient?
Yes = 13 persons • Interesting with new ways of working • Provided technology is reliable and minimum of
interruptions. No = 2 persons
• Easier with cards, you don’t need to log in, the system can be down and you just stand there.
1 did not answer yes or no • If it’s safe, sometimes we have problem with internet.
1 answered both yes and no • It’s possible if it’s a good system and works.
Do you think it’s safe to use mobile technology (tablet) at a radiotherapy department?
Yes = 13 persons • But unsafe with double (card and Aria) • Provided technology is reliable and minimum of
interruptions. • Sure
1 did not answer yes or no • If internet works, we have problem with Citrix license,
sometimes all license are busy. 1 answered both yes and no
• It’s possible if it’s a good system and works. No = 2 persons
Can you imagine the use of mobile technology (tablet) at a radiotherapy department will secure patients’ safety and facilitate healthcare work efficiently?
Yes = 12 persons • Increase security • One documentation
1 answered both yes and no • It’s possible if it’s a good system and works
1 did not answer yes or no • Hopefully!
No = 3 persons • Everything goes.

63
Appendix III-Theme Coding (Previous Research)
Theme coding 1 (purpose of using paper treatment cards and experiences of not finding paper
treatment cards)
Theme coding 2 (mobile technology using experiences and imagine of conducting paper treatment
cards into mobile technology for healthcare work)
(1= not satisfied at all, 5= Very satisfied)

64
Appendix IV-Diagrams (Previous Research)
Diagram 1-Satisfaction with paper cards
Diagram 2-Experiences on not finding paper cards
Diagram 3-Suggestion Acceptance: 76% participants accepted to the suggestion of conducting paper
protocols into mobile devices

65
Appendix V-Consent form for this research
Dear participant,
I’m Ying-Ying Yang Öhlin, I’m now engaging in a study of researching the feasibility of using computerized tablet for information/documentation/verification of patients’ radiotherapy treatments since it’s proved that mobile technology provided improved quality of health services. The idea of using mobile technology is to secure patients’ safety and facilitate healthcare work efficiently. For getting appropriate data, the idea participants are those who work and/or have worked at a radiotherapy department. Every single part of this participation in the study is complete confidentiality. Your name will not be presented in the study. You are voluntary to take part in this study and you are free to declare off from this study at any time without giving any reason. If you have any question about the project, you’re welcome to contact me.
Sincerely yours,
Ying-Ying Yang Öhlin ([email protected])

66
Appendix VI-Figure 17 Figure 17.-Patient Pathway in swim lane diagram (Page 26)

67
Appendix VII-Time Frame