Embed Size (px)
Citation preview

A 23 Year Old Woman who A 23 Year Old Woman who Presents with New Onset SEPresents with New Onset SE
Brandon Wills, DO, MSFellow, Clinical Toxicology
Toxikon Consortium of Cook County
Clinical Instructor in Emergency Medicine
University of Illinois at Chicago

Brandon Wills, DO, MS
Case PresentationCase Presentation
• 23 year-old female presents to the ED with generalized seizures x 3
• Pt. found by family member initially somnolent

Brandon Wills, DO, MS
Past Medical History & Social HistoryPast Medical History & Social History
• No details available (initially)

Brandon Wills, DO, MS
Physical ExamPhysical Exam
• VS: AF; 90/50; 116; 24; 97% on NRM
• Pt. having repeated brief generalized seizures with intermittent recovery
• HEENT- pupils 5mm, reactive
• CV- Tachy, no M/G/R
• Lungs- CTAB
• Skin- Warm, pink, dry
Your Differential Diagnosis?Your Differential Diagnosis?

Brandon Wills, DO, MS
Differential DiagnosisDifferential Diagnosis
• Neurologic• Infectious etiologies• Metabolic• Endocrine• Toxicologic
Brandon Wills, DO, MS
ED CourseED Course
• What would be your initial management?

Brandon Wills, DO, MS
ED CourseED Course
• What would be your initial management?• IV, O2, Monitor• IV ativan• Bedside glucose• Send laboratory studies• CT head?
Brandon Wills, DO, MS
ED CourseED Course
• Pt. given several doses of IV ativan without improvement
• Pt. was then intubated, sedated with propofol
Brandon Wills, DO, MS
Lab ResultsLab Results
• EKG: Sinus tach, narrow complex• HCO3- 10• Anion gap- 25• ABG- 6.99/28/172/7• WBC- 25.4• Chemistry = wnl• Utox- nl• ASA/APAP- negative• LFT’s- nl

Brandon Wills, DO, MS
ED CourseED CourseWe Want More HistoryWe Want More History
• No history of seizure disorder
• No history of trauma
• Family members arrive with an empty bottle of INH
Brandon Wills, DO, MS
• What would be your next step in this patient’s management?
ED CourseED Course

Brandon Wills, DO, MS
Isonicontinic Acid Hydrazide INHIsonicontinic Acid Hydrazide INH
Structurally similar to
• Pyridoxine (B6)
• NAD
• Nicotinic acid (Niacin)

Brandon Wills, DO, MS
Isonicontinic Acid Hydrazide INHIsonicontinic Acid Hydrazide INH
Pyridoxine(Vitamin B6)
INH
Nicotinic Acid(Niacin)

Brandon Wills, DO, MS
Isonicontinic Acid Hydrazide INHIsonicontinic Acid Hydrazide INH
Gyromitra species Rocket fuel
Structurally Similar Toxins
Monomethylhydrazine

Brandon Wills, DO, MS
Hydrazine EpidemiologyHydrazine Epidemiology11
INH
426- Exposures
58- Minor
70- Moderate
80- Major
1- Deaths
Gyromitra Species
44- Exposures
13- Minor
10- Moderate
0- Major
0- Deaths
1. AAPCC 2001 TESS Data
Brandon Wills, DO, MS
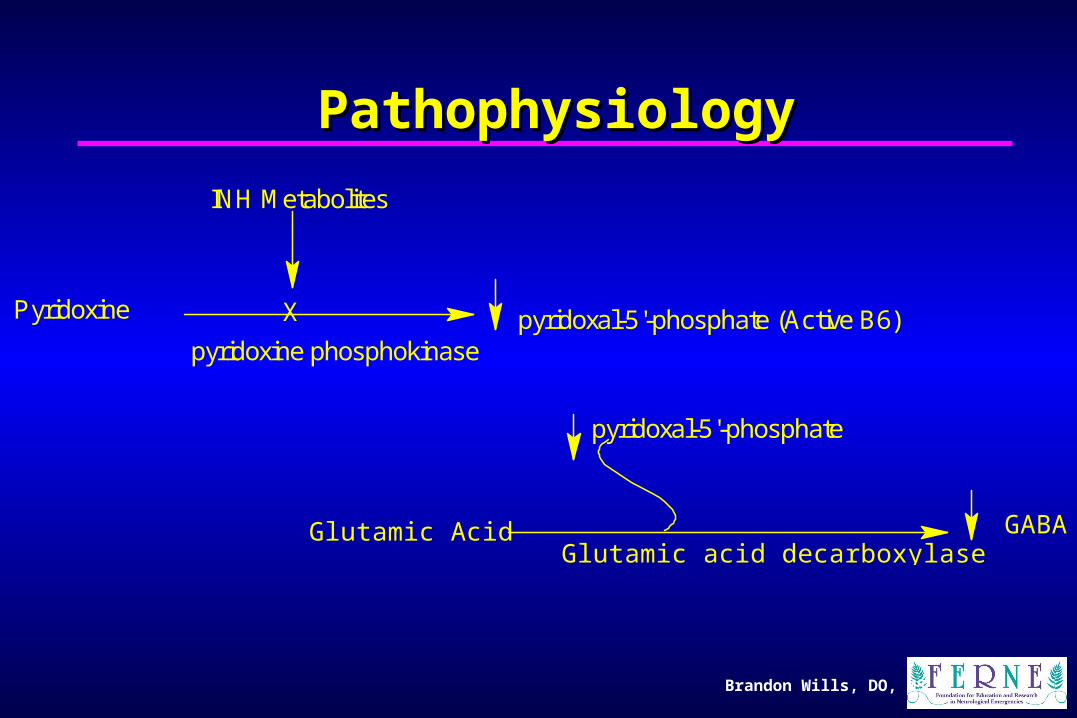
PathophysiologyPathophysiology
Glutamic Acid GABAGlutamic acid decarboxylase
pyridoxal-5'-phosphate
Pyridoxine pyridoxal-5'-phosphate (Active B6)X
pyridoxine phosphokinase
INH Metabolites

Brandon Wills, DO, MS
INH ToxicokineticsINH Toxicokinetics
Therapeutic dose: 5-15 mg/kg
Toxic dose: >20 mg/kgsignificant toxicity >40 mg/kg
Peak [ ]: 2 hours
Elimination T1/2: 70-180 minutes
Brandon Wills, DO, MS
Clinical ManifestationsClinical Manifestations
Triad:
1. Refractory seizures
2. Severe metabolic acidosis
3. Coma

Brandon Wills, DO, MS
Clinical ManifestationsClinical Manifestations
Early: May mimic anticholinergic toxidrome
(N/V, tachycardia, ataxia, mydriasis, CNS dep.)
Late: Seizures, acidosis
Chronic: Hepatotoxicity

Brandon Wills, DO, MS
Lab StudiesLab Studies
• Chemistries
• Lactate
• EKG
• Hepatic enzymes
• +/- INH levels

Brandon Wills, DO, MS
Treatment of ToxicityTreatment of Toxicity
1. A,B,C’s2. Initial resuscitation and supportive care3. Decontamination
- Lavage?- Whole bowel irrigation?
- Activated charcoal?
4. Enhanced elimination5. Antidotes
Brandon Wills, DO, MS
Treatment of ToxicityTreatment of Toxicity
1. A,B,C’s
Brandon Wills, DO, MS
Treatment of ToxicityTreatment of Toxicity
2. Initial resuscitation and supportive care
IV Fluids
Benzodiazepines
+/- Sodium bicarb
Brandon Wills, DO, MS
Treatment of ToxicityTreatment of Toxicity
3. Decontamination- Lavage?
- Whole bowel irrigation?
- Activated charcoal?
Brandon Wills, DO, MS
Treatment of ToxicityTreatment of Toxicity
4. Enhanced elimination
Hemodialysis?

Brandon Wills, DO, MS
Treatment of ToxicityTreatment of Toxicity
5. Antidotes
Pyridoxine (B6)
Brandon Wills, DO, MS
Case CourseCase Course
Toxikon is a Medical Toxicology Consortium Including Cook County Hospital, The University of Illinois Hospital, and Rush Presbyterian St.
Luke's Medical Center
The Toxikon Consortium
Brandon Wills, DO, MS
Case CourseCase Course
• Recommended IV pyridoxine
• Pharmacy unable to mobilize B6
• Contacted Rush antidote depot for courier
• Pt. given 5g IV

Brandon Wills, DO, MS
Case CourseCase Course
• Seizure activity terminated• Repeat ABG: 7.31/34/503/17• Pt. extubated the following day• Transferred to psych facility on hospital
day 3

Brandon Wills, DO, MS
Teaching PointsTeaching Points
• Consider INH toxicity with patients presenting with refractory seizures

Brandon Wills, DO, MS
Teaching PointsTeaching Points
• Remember to treat the patient, not the poison (A,B,C’s)
Brandon Wills, DO, MS
Teaching PointsTeaching Points
• Gyromitra species are another source of hydrazine
Brandon Wills, DO, MS
Teaching PointsTeaching Points
• What is the antidote for INH-induced seizures?
•Pyridoxine (B6)•Dosing- gram (INH ingested):gram (B6)•Unknown ingestions, start with 5 grams IV•IV pyridoxine supplies are often limited•PO B6 may be crushed and given NG
Questions???Questions???