Embed Size (px)
Citation preview

Oncology ServiceWills Eye Institute
Carol Shields MD
Oncology ServiceWills Eye Hospital
Philadelphia PA USA
The Game of Uveal Melanoma
www.fighteyecancer.com
points•causes•features•therapy•collaborative ocular melanoma study•prognosis
Causes of uveal melanomahost factors•nevus•melanocytosis•light eye color•fair skin color•inability to tanenvironmental factors•arc welding•chronic sunlight exposure
Choroid Nevusfew reportswhite population 7%features
•pigmented 90%
•thickness <2mm
•drusen
•RPE atrophy
Choroid Nevus
questions
•do the features change over time
•can nevus affect vision
•can nevus enlarge
•rate of transformation into melanoma
answers
•yes
•yes
•yes
•1/8000
Choroid Nevus
Clinical�Spectrum�of�Choroidal�Nevi�Based�onAge�at�Presentation�in�3422�Consecutive�Eyes
Carol�L.�Shields,�MD,�Minoru�Furuta,�MD,�Arman�Mashayekhi,�MD,�Edwina�L.�Berman,�MBBS,Jonathan�D.�Zahler,�DO,�Daniel�M.�Hoberman,�BS,�Diep�H.�Dinh,�BS,�Jerry�A.�Shields,�MD
Purpose:� To�evaluate� the�clinical� features�of�choroidal�nevi�based�on�patient�age�at�presentation�and� toinvestigate�features�of�the�nevi�that�are�predictive�of�patient�symptoms.
Design:� Observational�case�series.Participants:� Three�thousand�four�hundred�twenty-two�consecutive�eyes�of�3187�patients.Methods:� Retrospective�clinic-based�study�of�clinical�features�at�referral.�Cox�proportional�hazards�regres-
sions�were�used�for�evaluation�of�factors�predictive�of�patient�symptoms.Main�Outcome�Measures:� Nevus�features�as�related�to�patient�age�group�at�diagnosis�(young�[!20�years],
mid-adult�[21–50�years],�older�adult�[!50�years])�and�factors�predictive�of�patient�symptoms�secondary�to�thenevus.
Results:� Of�the�3422�eyes�with�choroidal�nevus,�63�(2%)�were�in�young�patients,�795�(23%)�in�mid-adults,and� 2564� (75%)� in� older� adults.� The� following� factors� showed� no� substantial� increase� or� decrease� by� agecategory�(young,�mid-adult,�older�adult)�at�presentation:�symptoms�(14%,�12%,�13%),�mean�nevus�base�(5.6,�4.7,5.2�mm),�intrinsic�nevus�pigmentation�(89%,�74%,�77%),�related�subretinal�fluid�(SRF)�(11%,�15%,�9%),�overlyingorange� pigment� (6%,� 10%,� 6%),� retinal� pigment� epithelial� hyperplasia� (0%,� 9%,� 7%),� and� retinal� pigmentepithelial�atrophy�(2%,�13%,�10%).�The�following�factors�statistically�increased�with�age�category:�multiple�neviper�eye�(2%,�8%,�10%)�(P�"�0.0001),�mean�nevus�thickness�(1.2,�1.5,�1.6�mm)�(P#0.0001),�and�overlying�drusen(11%,�40%,�58%)�(P#0.0001).�Using�multivariate�analysis�of�the�entire�group,�factors�predictive�of�any�symptomincluded�nonpigmented�nevus�(P#0.001),�location�!�3�mm�to�foveola�(P�"�0.001),�subfoveolar�fluid�(P�"�0.002),any�SRF�(P�"�0.02),�and�subfoveolar�nevus�(P�"�0.027).
Conclusions:� Choroidal� nevi� show� similar� clinical� features� regardless� of� age� of� presentation,� with� theexception�of� increasing�number�of�nevi�per�eye,�slightly� increasing�thickness,�and�increasing�drusen�in�adultsversus�younger�patients.�Symptomatic�nevi�are�more�likely�to�be�nonpigmented,�beneath�the�foveola,�and�withsubfoveolar�fluid.� Ophthalmology�2008;115:546�–552�©�2008�by�the�American�Academy�of�Ophthalmology.
In� clinic-based� studies,� the� prevalence� of� choroidal� nevushas�varied�from�an�estimated�0.2%�to�30%�of�patients.1–8�Inpopulation-based� studies,� choroidal� nevus� prevalence� hasranged�from�1.9%�of�persons�older�than�13�years�to�6.5%�ofpersons�over�49.9,10�These�and�other�studies�have�suggestedthat�choroidal�nevus�is�a�fairly�common�tumor,�particularlyin� Caucasian� patients,� and� carries� a� small� potential� forgrowth�into�melanoma.3,10–23
Most� previous� investigations� on� choroidal� nevi� havefocused�on�a�select�adult�population�over�age�18�years,12,13
over� 30,3,5� and�over� 49.4,10� Some� studies� have�been�moreexclusive,�evaluating�middle-aged�surgical� trauma�patientsfrom� 18� to� 38� years2� and� middle-aged� pilots� and� recruitsfrom�18�to�41�years.6�Data�collection�has�varied�from�directophthalmoscopic� evaluation� to� indirect� funduscopy� to� ret-rospective� examination� of� fundus� photographs� to� obtaininformation�on�clinical�features�of�the�nevus�and�surround-ing�tissue.1,2,6,8,10� Review�of�color�fundus�photography,�asperformed�in�the�Blue�Mountains�Eye�Study�(BMES),10�canprovide�valuable�unbiased�information�on�gross�features�of
Originally�received:�March�8,�2007.Final�revision:�July�3,�2007.Accepted:�July�6,�2007.Available�online:�December�6,�2007.� Manuscript�no.�2007-325.
From�the�Ocular�Oncology�Service,�Wills�Eye�Institute,�Thomas�JeffersonUniversity,�Philadelphia,�Pennsylvania.
Presented�at:�International�Congress�of�Ocular�Oncology,�June�2007,�Siena,Italy� (CLS),� and� American� Academy� of� Ophthalmology� meeting� (as� aposter),�November�2007,�New�Orleans,�Louisiana�(CLS).
Support�provided�by�the�Retina�Research�Foundation,�Retina�Society,�CapeTown,�South�Africa�(CLS);�Paul�Kayser�International�Award�of�Merit�in
Retina�Research,�Houston,�Texas�(JAS);�Michael,�Bruce,�and�Ellen�Ratner,New York, New York (JAS, CLS); Mellon Charitable Giving from theMartha W. Rogers Charitable Trust, Philadelphia, Pennsylvania (CLS);LuEsther Mertz Retina Research Foundation, New York, New York(CLS); and Eye Tumor Research Foundation, Philadelphia, Pennsylvania(CLS, JAS). The sponsors or funding organizations have had no role in thedesign or conduct of the research.
No conflicting relationship exists for any author.
Correspondence to Carol L. Shields, MD, Ocular Oncology Service, Suite1440, Wills Eye Institute, 840 Walnut Street, Philadelphia, PA 19107.E-mail:�[email protected].
546 © 2008 by the American Academy of Ophthalmology ISSN 0161-6420/08/$–see front matterPublished by Elsevier Inc. doi:10.1016/j.ophtha.2007.07.009
Choroid Nevus
groups
•young 0-20 yrs
•mid adult 20-50 yrs
•older adult >50 yrs
thick >1per eye drusen1.2 2% 11%1.5 8% 40%1.8 10% 58%
p<0.0001
Choroid Nevus Young Choroid Nevus Mid Adult

Choroid Nevus Older Adult Choroid Nevus
questions
•do the features change over time
•can nevus affect vision
•can nevus enlarge
•rate of transformation into melanoma
answers
•yes
•yes
•yes
•1/8000
Choroid NevusCLINICAL SCIENCES
Visual Acuity in 3422 Consecutive EyesWith Choroidal NevusCarol L. Shields, MD; Minoru Furuta, MD; Arman Mashayekhi, MD; Edwina L. Berman, MBBS;Jonathan D. Zahler, DO; Daniel M. Hoberman, BS; Diep H. Dinh, BS; Jerry A. Shields, MD
Objective: To evaluate visual acuity in eyes with cho-roidal nevus.
Design: This was an observational case series. Of 3422consecutive eyes with choroidal nevus, vision loss at 15years occurred in 2% of eyes with extrafoveolar nevusand in 26% of eyes with subfoveolar nevus, particularlythose with overlying retinal pigment epithelial detach-ment and foveal edema. A retrospective medical recordreview was conducted, with evaluation of visual acuityat presentation and at final examination. The main out-come measure was visual acuity.
Results: The median visual acuity at presentation was20/20 for eyes with either extrafoveolar or subfoveolarchoroidal nevus. Using Kaplan-Meier estimates, visionloss of 3 or more logarithm of the minimum angle of reso-lution (logMAR) lines at 5, 10, and 15 years occurred inless than 1%, 1%, and 2% of eyes with extrafoveolar ne-vus compared with 15%, 20%, and 26% of eyes with sub-
foveolar choroidal nevus, respectively. By multivariateanalysis, factors predictive of visual loss of 3 or more log-MAR lines included subfoveolar nevus location (rela-tive risk [RR], 15.52), juxtapapillary nevus location (RR,4.52), initial visual acuity of 20/50 or worse (RR, 15.40),overlying retinal pigment epithelial detachment (RR,22.16), and foveal edema (RR, 9.02). Factors predictiveof poor final visual acuity of 20/200 or worse includedsubfoveolar nevus location (RR, 11.32), overlying or-ange pigment (RR, 3.68), overlying retinal pigmentepithelial detachment (RR, 12.80), and foveal edema (RR,18.72).
Conclusion: Mild vision loss over many years should beanticipated in patients with subfoveolar choroidal ne-vus, particularly those with overlying retinal pigment epi-thelial detachment, orange pigment, and foveal edema.
Arch Ophthalmol. 2007;125(11):1501-1507
C HOROIDAL NEVUS IS THEmost common clinicallydetected intraocular tu-mor.1,2 In the Blue Moun-tains Eye Study,3 choroi-
dal nevi were found in 7% of the whitepopulation. This benign tumor manifests asa pigmented or nonpigmented mass deepto the retina, often with overlying drusenand retinal pigment epithelial (RPE) alter-ations.1-7 Choroidal nevus can produce cen-tral vision loss and peripheral visual fieldloss.4,8-11 Rarely, choroidal nevus can evolveinto malignant melanoma.7,12-18
Visual field defects were documented in38% of 42 eyes with choroidal nevus evalu-ated by Tamler and Maumenee4 and in 85%of 21 eyes analyzed by Flindall and Drance10
using static and kinetic techniques. In 1971,Naumann and associates6 found central vi-sual acuity loss in 13 of 124 eyes (10%) withchoroidal nevus. Gonder and coworkers8
later described 206 patients with choroi-dal nevi posterior to the equator of the eye
and found 22 (11%) with visual acuity loss.The vision loss was because of subfovealfluid (50%), presumed photoreceptor de-generation (42%), and choroidal neovas-cularization (8%).8 In 2005, Shields and as-sociates11 evaluated optical coherencetomography (OCT) of the retina overlying120 consecutive patients with choroidal ne-vus to better ascertain the reasons for vi-sual loss and found overlying retinal edema(15%), photoreceptor attenuation (51%),retinal thinning (22%), subretinal fluid(26%), and RPE detachment (12%). In thisreport, we analyze a large cohort of 3422eyes with stable choroidal nevus to ascer-tain initial and final visual acuity, loss of vi-sual acuity over time, and factors related tovisual acuity outcomes.
METHODS
A retrospective medical record review wasperformed on all patients with the clinical
Author Affiliations: OcularOncology Service, Wills EyeInstitute, Thomas JeffersonUniversity, Philadelphia,Pennsylvania.
(REPRINTED) ARCH OPHTHALMOL / VOL 125 (NO. 11), NOV 2007 WWW.ARCHOPHTHALMOL.COM1501
©2007 American Medical Association. All rights reserved. by CarolShields, on November 13, 2007 www.archophthalmol.comDownloaded from
Choroid Nevus
groups
•subfoveal
•extrafoveal
initial final20/20 20/3020/20 20/25
vision loss 3 lines
@5 @10 @20 yrs 15% 20% 26%<1% 1% 2%
why does subfoveal nevus have vision loss?
Choroid Nevus
questions
•do the features change over time
•can nevus affect vision
•can nevus enlarge
•rate of transformation into melanoma
answers
•yes
•yes
•yes
•1/8000
growth is a presumed indicator of malignant potential
growth is not an unequivocal indicator of malignancy
Slow Enlargement of Choroidal Nevi:A Long-Term Follow-Up Study
Arman Mashayekhi, MD, Sophia Siu, BS, Carol L. Shields, MD, Jerry A. Shields, MD
Purpose: Choroidal nevi are generally considered to be stable lesions, and growth of a choroidal nevus isusually believed to be a sign of malignant transformation. We performed this study to determine whetherchoroidal nevi enlarge over a long period of follow-up without undergoing malignant transformation.
Design: Retrospective observational case series.Participants: A total of 278 patients with 284 nevi who had at least 7 years of photographic follow-up
without clinical signs of transformation into melanoma were included in the study.Methods: Data on demographic and clinical information were extracted from patients’ charts. Detailed
fundus drawings and color fundus photographs were reviewed and compared for evidence of enlargement.Main Outcome Measures: Nevus enlargement without clinical evidence of transformation into melanoma.Results: Of the 278 patients, 69% were female and more than 99% were White with a median age at
presentation of 57 years (range, 4–87 years). The largest nevus basal diameter was a median of 5 mm (range,0.5–14 mm), and the median thickness was 1.5 mm (range, 0.1–3.6 mm). Only 14 nevi (5%) had subretinal fluidoutside the nevus, and 6% showed overlying orange pigment. Overlying retinal pigment epithelial alterationsincluded drusen (61%), atrophy (6%), hyperplasia (10%), and fibrous metaplasia (6%). Of 284 nevi, 31% showedslight enlargement over a mean follow-up of 15 years. The median increase in diameter was 1 mm (mean, 0.9mm; range, 0.2–3.0 mm), and the median rate of enlargement was 0.06 mm/yr (mean, 0.06 mm/yr; range,0.01–0.36 mm/yr). None of the lesions that enlarged developed new risk factors that are generally associatedwith malignant transformation. Frequency of enlargement was 54% in patients aged less than 40 years and 19%in patients aged more than 60 years. On multivariate analysis, younger patient age was the only factor predictiveof nevus enlargement (P!0.001).
Conclusions: With long-term follow up, 31% of choroidal nevi showed slight enlargement without clinicalevidence of transformation into melanoma. The frequency of enlargement was inversely related to patient age.
Financial Disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussedin this article. Ophthalmology 2011;118:382–388 © 2011 by the American Academy of Ophthalmology.
Choroidal nevi are common benign melanocytic tumors ofthe ocular fundus reported in 6.5% of the general whitepopulation on clinical examination.1 Despite their benignnature and their low potential for causing visual symptoms,2
choroidal nevi have been the subject of interest amongophthalmologists mainly because of their clinical resem-blance and potential malignant transformation to choroidalmelanoma. Although the true malignant potential of choroi-dal nevi is not known, these lesions have long been sus-pected of being precursors of choroidal melanoma.3–7 How-ever, most of the interest in choroidal nevi lies in thedifficulties associated with differentiating them from smallchoroidal melanomas leading to delayed or unnecessarytreatment with potentially life-threatening consequences orvisually damaging complications, respectively.8,9
Most ophthalmologists will face the important and some-times challenging task of differentiating between a choroi-dal nevus and a small choroidal melanoma. The traditionalapproach to management of small choroidal melanocyticlesions has been one of careful observation for detection ofgrowth. On the basis of this approach, lesions that remain
stable are considered to be benign choroidal nevi, whereaslesions that show enlargement are diagnosed as melanomasand treated accordingly.4,7,8,10–17 Because of the difficultiesassociated with repeated follow-up examinations and con-cerns regarding possible deleterious consequences of fol-lowing untreated small melanomas, in the 1970s ocularoncologists started identifying14,15,18 and later substitutingcertain tumor features predictive of future growth, so-calledrisk factors, for actual tumor growth.7,19–24 On the basis ofthis approach, the absence of risk factors (or the presence ofonly 1 risk factor) favors diagnosis of a choroidal nevuswhereas the presence of several risk factors (generally !2)signifies a choroidal melanoma.7,9,21,25–27 Despite their dif-ferences, both of these approaches rely on growth (or ab-sence of growth) for differentiating choroidal nevi fromsmall choroidal melanomas. This emphasis on growth byclinicians is based on the widely held belief that choroidalnevi, in contrast with choroidal melanomas, are stablelesions.
Because of the central role of growth in the currentapproach to management of small choroidal melanocytic
382 © 2011 by the American Academy of Ophthalmology ISSN 0161-6420/11/$–see front matterPublished by Elsevier Inc. doi:10.1016/j.ophtha.2010.06.006
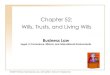
Choroid Nevus Enlargement
16 yowm enlargement over 10 years

Choroid Nevus Enlargement
enlargement over 10 years
Choroid Nevus Enlargement
3 mm growth in 2 years
MelanomaChoroid Nevus
questions
•do the features change over time
•can nevus affect vision
•can nevus enlarge
•rate of transformation into melanoma
answers
•yes
•yes
•yes
•1/8000
Nevus Growth to Melanoma Nevus Growth to Melanoma
Mathematical estimates
•Ganley 1/4500
•Singh et al 1/8845
•Kivela et al 1/100 .... if we live to 80 yrs
Population based study - Blue Mtn Eye Study
Clinic based study - Shields et al
annual rate
cumulative rate
Nevus Growth to MelanomaRisk factors
low risk high risk
Nevus Growth to Melanoma
most important paper from our practice
published 1995
published 2009
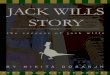
Nevus Growth to MelanomaTh > 2 mmFluidSymptomsOrange pigmentMargin at discUS HollowHalo absentDrusen absent
ToFindSmallOcularMelanomaUsing HelpfulHintsDaily
Nevus Growth to MelanomaTh > 2 mmFluidSymptomsOrange pigmentMargin at discUS HollowHalo absentDrusen absent
-+++++++
Each factor adds relative risk of ~ 32187 x greater risk

Tests
OCT
Autofluorescence
Ultrasound
Fluorescein Angiography
OCT EDI
pigmented lesion•no transmission •poor posterior border•compression of choroidal vessels
important difference is
shaggy photoreceptors
Nevus vs Melanoma
edi oct of choroidal nevus versus melanomashaggy photoreceptors - elongated
important difference is
shaggy photoreceptors
Nevus vs Melanoma thicker
subretinal fluidshaggy photoreceptors
p=0.001
Autofluorescence
nevus
melanoma
nevus
melanoma
Autofluorescence Causes of uveal melanomahost factors•nevus•melanocytosis•light eye color•fair skin color•inability to tanenvironmental factors•arc welding•chronic sunlight exposure

Causes for uveal melanoma
Melanocytosis!
1/400 risk
Causes for uveal melanoma
Melanocytosis!
1/400 risk
at risk for melanoma
at risk for melanoma
at risk for melanoma
points•causes•features•therapy•collaborative ocular melanoma study•prognosis
color melanotic 85% amelanotic 15%size base 11 mm thickness 5.5 mm

Quadrant uveal melanoma in 8033 eyes
Nasal 21%
Temporal 28%
Inferior 22%
Macula 4%
Diffuse 3%
Superior 22%
! ! 2.6 mm! ! 4.3 mm! ! 7.0 mm
points•causes•features•therapy•collaborative ocular melanoma study•prognosis
Treatment Uveal Melanoma
• Observation• Laser• Thermotherapy• Plaque radiotherapy• Charged particle radiotherapy• Resection• Enucleation• Exenteration• Systemic therapies
Depends• Tumor size• Tumor location• Status of opposite eye• Patient age• Patient health• Patient desires and fears
Treatment Uveal Melanoma
Basically• Small• Medium• Large
TTTRadiotherapy
RadiotherapyResection Enucleation
RadiotherapyEnucleation
Treatment Uveal Melanoma
0-3mm
3-8mm
>8mm
Plaque Radiotherapy Melanoma
Radiation parameters
• Apex 8000 cGy
• Base 30000 cGy
Plaque Radiotherapy Melanoma
standard
custom roundcustom notch
custom curvilinear

Radiation Team
• Radiation oncologist
• Radiation physicist
Radiation Lead Container
Plaque transportation
Prevent exposure
Ocular Oncologists
Surgical placement of radiation plaque
All personnel
Every person in the room wears radiation badge
Exposure measurement
Radiation Device
Dummy plaque
Radioactive plaque
Radioactive Plaque
Stored on hospital tray
Betadiene
Sterile metal container face down
Rinsed
Radioactive Plaque
Rinsed
Seed count
Sutures already in sclera
Tie down
Radioactive Plaque
Precisely localize intraocular tumor with transillumination or scleral depression
Rotate eye with muscle sutures
Long sutures to find plaque for removal

Radioactive Plaque
Conjunctival closure with 7-0 vicryl
Maxitrol and Atropine ointments
Tarsorrhaphy suture
Patch
Plaque Radiotherapy Choroid Melanoma
Plaque Radiotherapy Iris Melanoma
Plaque Radiotherapy Follow upEye
•Maxitrol tid 3-6 wks•Atropine qhs 3-6 wks•Recheck and measure 4 months•Eye exam q 4 months then q 6 months for life
SystemicTwice yearly•Physical examination (liver and lung)•Liver function testsOnce yearly•Chest xray•MRI abdomen
Plaque Small Melanoma Plaque + TTT small melanoma
before! ! after3.0 mm! ! 1.3 mm
Plaque Small Melanoma
thickness5 mm! ! ! ! ! 2 mm
Plaque Medium Melanoma
thickness9 mm! ! ! ! ! 2 mm
Plaque Large Melanoma
Oncology ServiceWills Eye Institute
thickness10 mm! ! ! ! ! 2 mm
Plaque Large Melanoma

Juxtapapillary choroidal melanoma
Magnitude of this problem
• of >10,000 uveal melanoma treated over 30 years
•n=650 juxtapapillary melanoma
• 7% of all uveal melanoma
Juxtapapillary choroidal melanoma
8 x 6 x 2.9 mmrequire • 12 mm radiation field• situate on 15 mm notched plaque post distribution• precision in placement
Requirements include knowledge and precision in•Tumor measurement•Plaque design•Plaque placement
• Juxtapapillary• Epipapillary!• Circumpapillary
Juxtapapillary choroidal melanomaPlaque radiotherapy
n=650
Plaque Radiotherapy for JuxtapapillaryChoroidal MelanomaTumor Control in 650 Consecutive Cases
Mandeep S. Sagoo, MB, PhD,1 Carol L. Shields, MD,1 Arman Mashayekhi, MD,1 Jorge Freire, MD,2
Jacqueline Emrich, PhD,2 Jay Reiff, PhD,2 Lydia Komarnicky, MD,2 Jerry A. Shields, MD1
Purpose: To evaluate treatment of juxtapapillary choroidal melanoma with plaque radiotherapy and toinvestigate the role of supplemental transpupillary thermotherapy (TTT).
Design: Retrospective, comparative case series.Participants: We included 650 consecutive eyes with juxtapapillary choroidal melanoma within 1 mm of the
optic disc.Methods: Eyes with juxtapapillary choroidal melanoma receiving plaque radiotherapy over a 31-year period
from October 1974 to November 2005 were included in the study. The TTT and no TTT groups were analyzedseparately and compared.
Main Outcome Measures: Local tumor control, metastasis, and tumor-related mortality.Results: The median basal tumor diameter was 10 mm (range, 1.5–21) and median thickness was 3.5 mm
(range, 0.5–14.8). In 481 eyes (74%), the tumor was directly adjacent to the optic disc and in 169 eyes (26%) theposterior tumor margin was between 0.1 and 1.0 mm from the optic disc. The circumpapillary extent of the tumorwas !4 clock-hours in 321 eyes (50%), 4–8 clock-hours in 250 eyes (38%), and "8 clock-hours in 79 eyes(12%). Plaque radiotherapy using iodine-125 in 616 eyes (95%), cobalt-60 in 19 eyes (3%), iridium-192 in 12 eyes(2%), and ruthenium-106 in 3 eyes (!1%) delivered a median radiation dose of 8000 cGy (range, 3600–15 500)to the tumor apex and adjunctive TTT was used in 307 eyes (56%). Kaplan-Meier estimates for tumor recurrence,metastasis, and death were 14%, 11%, and 4% at 5 years and 21%, 24%, and 9% at 10 years, respectively.Eyes treated with additional TTT showed slight (statistically nonsignificant) reduction in recurrence and metas-tasis. Using multivariable analysis, factors predictive of tumor recurrence included foveolar tumor requiring TTT(hazard ratio, 5.07; P!0.001) and greater tumor thickness (hazard ratio, 1.29 per mm increase; P!0.001). Factorspredictive of metastasis included greater tumor base (hazard ratio, 1.21 per mm increase; P!0.001) andincreasing intraocular pressure (hazard ratio, 1.11 per mmHg increase; P # 0.020).
Conclusions: Plaque radiotherapy for juxtapapillary melanoma provides local tumor control in approxi-mately 80% of eyes at 10 years. In subjects who received TTT, there was slight but nonsignificant improved localtumor control and lower metastatic rate.
Financial Disclosure(s): The authors have no proprietary or commercial interest in any of the materialsdiscussed in this article. Ophthalmology 2011;118:402–407 © 2011 by the American Academy of Ophthalmology.
The management of choroidal melanoma in close proximityto the optic disc (juxtapapillary melanoma) poses severalunique challenges, owing to the posterior location of thetumor adjacent to visually significant structures. These in-clude the choice of optimal treatment such as radioactiveplaque,1–3 proton beam irradiation,4 stereotactic radiosur-gery,5 transpupillary thermotherapy (TTT),6 or enucle-ation.7 If radiotherapy is chosen, there is the dilemma ofwhether adjunctive treatment to the tumor, such as TTT,6,8
should be used to ensure optimal tumor control.It has been "10 years since our group demonstrated equiv-
alent survival in patients with juxtapapillary melanoma treatedwith plaque radiotherapy versus enucleation.9 In prior reports,we established that plaque radiotherapy is effective for juxta-
papillary melanoma encircling the optic disc (circumpapillarymelanoma)10 and for juxtapapillary melanoma overhangingthe optic disc.11 In this study, we evaluate our overall experi-ence of plaque radiotherapy for juxtapapillary melanoma andspecifically explore the use of adjuvant TTT with regard totumor control, metastases, and mortality.
Patients and Methods
The electronic database of patients evaluated at the OncologyService of Wills Eye Hospital, Philadelphia, Pennsylvania, wassearched for juxtapapillary choroidal melanoma treated withplaque radiotherapy. Juxtapapillary choroidal melanoma was de-fined as a choroidal melanoma with posterior margin touching,
402 © 2011 by the American Academy of Ophthalmology ISSN 0161-6420/11/$–see front matterPublished by Elsevier Inc. doi:10.1016/j.ophtha.2010.06.007
points•causes•features•therapy•collaborative ocular melanoma study•prognosis
Collaborative Ocular Melanoma Study
Collaborative Ocular Melanoma Studywhat should you remember?
1. medium melanoma 3-8 mm thickness
plaque provides same prognosis as enucleation
2. large melanoma >8 mm thickness
no need to irradiate eye before enucleation
neither proved that therapy prevents metastasisearly detection may be the best way to
minimize metastasis
points•causes•features•therapy•collaborative ocular melanoma study•prognosis
Prognosis of Uveal Melanoma
melanoma is a deadly eye cancer

Prognosis of Uveal Melanoma
old literatureseveral reports on prognosisfactors related to prognosis
clinicalhistopathologycytologygenetic
2003Kujala, Makitie, KivelaMetastasis n=289 pts@ 5 yrs 31%@15 yrs 45%@25 yrs 49%@35 yrs 52%
Prognosis of Uveal Melanoma2003Kujala, Makitie, KivelaIf death from melanoma 62% by 5 yrs 90% by 10 yrs 98% by 25 yrs100% by 35 yrs
Prognosis of Uveal Melanoma
if metastasis, most picked up by 15 years following eye diagnosis
2009Shields CL, Furuta, Thangappan, et al.n=8033MetastasisPractical millimeter by millimeter basis
Prognosis of Uveal MelanomaCLINICAL SCIENCES
Metastasis of Uveal MelanomaMillimeter-by-Millimeter in 8033 Consecutive EyesCarol L. Shields, MD; Minoru Furuta, MD; Archana Thangappan, MD; Saya Nagori, MD;Arman Mashayekhi, MD; David R. Lally, MD; Cecilia C. Kelly, MD; Danielle S. Rudich, MD;Anand V. Nagori, MD; Oojwala A. Wakade, MD; Sonul Mehta, MD; Lauren Forte, BS;Andrew Long, BS; Elaina F. Dellacava, MD; Bonnie Kaplan, MD; Jerry A. Shields, MD
Objective: To determine the rate of metastasis of uvealmelanoma on the basis of tumor thickness in millimeters.
Methods: Retrospective medical record review.
Results: The mean (median) patient age was 58 (59)years. A total of 8033 eyes were examined. Of the 285eyes with iris melanoma, the mean tumor thickness was2.7 mm and metastasis occurred in 0.5%, 4%, and 7% at3, 5, and 10 years, respectively. Of the 492 eyes with cili-ary body melanoma, the mean tumor thickness was 6.6mm and metastasis occurred in 12%, 19%, and 33% at3, 5, and 10 years, respectively. Of the 7256 eyes withchoroidal melanoma, the mean tumor thickness was 5.5mm and metastasis occurred in 8%, 15%, and 25% at 3,5, and 10 years, respectively. For all uveal melanoma, me-tastasis at 5, 10, and 20 years was 6%, 12%, and 20% forsmall melanoma (0-3.0 mm thickness), 14%, 26%, and
37% for medium melanoma (3.1-8.0 mm), and 35%, 49%,and 67% for large melanoma (!8.0 mm). More specifi-cally, metastasis per millimeter increment at 10 years was6% (0-1.0 mm thickness), 12% (1.1-2.0 mm), 12% (2.1-3.0 mm), 16% (3.1-4.0 mm), 27% (4.1-5.0 mm), 28% (5.1-6.0 mm), 29% (6.1-7.0 mm), 41% (7.1-8.0 mm), 50% (8.1-9.0 mm), 44% (9.1-10.0 mm), and 51% (!10.0 mm).Clinical factors predictive of metastasis by multivariateanalysis included increasing patient age, ciliary body lo-cation, increasing tumor diameter, increasing tumor thick-ness, having a brown tumor, and the presence of sub-retinal fluid, intraocular hemorrhage, or extraocularextension.
Conclusion: Increasing millimeter thickness of uveal mela-noma is associated with increasing risk for metastasis.
Arch Ophthalmol. 2009;127(8):989-998
I N 1962, PAUL ET AL1 FROM THEArmed Forces Institute of Pathol-ogy reported the demographicdata and prognosis of 3852 pa-tients with uveal melanoma, the
largest collection of patients with intra-ocular melanoma then. Their data re-vealed the following information: mean ageat diagnosis of 55 years, approximately54% male, and less than 1% African Ameri-can. On the basis of the follow-up of 2652cases, mortality rate by actuarial methodwas 29% at 5 years, 40% at 10 years, and46% at 15 years, with a median survivalof 15" years. Ten-year mortality was lowerin younger patients (aged 20-39 years) at26% vs older patients (aged !70 years) at51%. In 1992, Diener-West et al2 pro-vided a meta-analysis of 8 published ar-ticles that further refined our understand-ing of uveal melanoma prognosis bygeneral tumor size. The combinedweighted estimate of 5-year mortality was16% for small tumors, 32% for medium tu-mors, and 53% for large tumors. Later, theCollaborative Ocular Melanoma Study dis-
closed melanoma-related mortality at 10years to be 17% to 18% for medium mela-noma and 40% to 45% for large mela-noma.3-6
Uveal melanoma prognosis has beenshown to be dependent on several clini-cal factors including tumor location in theciliary body, large tumor size, diffuse (flat)configuration, and extraocular extensionas well as histopathologic and cytoge-netic factors including epithelioid cell type,increased mitotic activity, infiltrating lym-phocytes, tumor vascular networks, andchromosomal mutations including mono-somy 3 and 8q addition.7,8 In several ar-ticles, tumor size has been identified as oneof the key clinical features predictive of me-tastasis.9,10 Furthermore, increasing tu-mor thickness, from small to medium tolarge, has been correlated with increas-ing risk for metastasis, but the exact rela-tionship per millimeter of tumor thick-ness has not been previously addressed,to our knowledge. In this analysis, weevaluate a large cohort of 8033 patients ob-served long-term for melanoma-related
Author Affiliations: OcularOncology Service, Wills EyeInstitute, Thomas JeffersonUniversity, Philadelphia,Pennsylvania.
(REPRINTED) ARCH OPHTHALMOL / VOL 127 (NO. 8), AUG 2009 WWW.ARCHOPHTHALMOL.COM989
©2009 American Medical Association. All rights reserved. at Thomas Jefferson University, on August 13, 2009 www.archophthalmol.comDownloaded from
Practical method for estimating metastatic risk
Melanoma Prognosis
• tumor thickness
• ajcc classification
• age
• melanocytosis
• configuration
• genetics - most powerful
Prognosis of Uveal Melanoma
doctor, what is my prognosis?
individualize prognosis based on data in office at first visit
CLINICAL SCIENCES
Metastasis of Uveal MelanomaMillimeter-by-Millimeter in 8033 Consecutive EyesCarol L. Shields, MD; Minoru Furuta, MD; Archana Thangappan, MD; Saya Nagori, MD;Arman Mashayekhi, MD; David R. Lally, MD; Cecilia C. Kelly, MD; Danielle S. Rudich, MD;Anand V. Nagori, MD; Oojwala A. Wakade, MD; Sonul Mehta, MD; Lauren Forte, BS;Andrew Long, BS; Elaina F. Dellacava, MD; Bonnie Kaplan, MD; Jerry A. Shields, MD
Objective: To determine the rate of metastasis of uvealmelanoma on the basis of tumor thickness in millimeters.
Methods: Retrospective medical record review.
Results: The mean (median) patient age was 58 (59)years. A total of 8033 eyes were examined. Of the 285eyes with iris melanoma, the mean tumor thickness was2.7 mm and metastasis occurred in 0.5%, 4%, and 7% at3, 5, and 10 years, respectively. Of the 492 eyes with cili-ary body melanoma, the mean tumor thickness was 6.6mm and metastasis occurred in 12%, 19%, and 33% at3, 5, and 10 years, respectively. Of the 7256 eyes withchoroidal melanoma, the mean tumor thickness was 5.5mm and metastasis occurred in 8%, 15%, and 25% at 3,5, and 10 years, respectively. For all uveal melanoma, me-tastasis at 5, 10, and 20 years was 6%, 12%, and 20% forsmall melanoma (0-3.0 mm thickness), 14%, 26%, and
37% for medium melanoma (3.1-8.0 mm), and 35%, 49%,and 67% for large melanoma (!8.0 mm). More specifi-cally, metastasis per millimeter increment at 10 years was6% (0-1.0 mm thickness), 12% (1.1-2.0 mm), 12% (2.1-3.0 mm), 16% (3.1-4.0 mm), 27% (4.1-5.0 mm), 28% (5.1-6.0 mm), 29% (6.1-7.0 mm), 41% (7.1-8.0 mm), 50% (8.1-9.0 mm), 44% (9.1-10.0 mm), and 51% (!10.0 mm).Clinical factors predictive of metastasis by multivariateanalysis included increasing patient age, ciliary body lo-cation, increasing tumor diameter, increasing tumor thick-ness, having a brown tumor, and the presence of sub-retinal fluid, intraocular hemorrhage, or extraocularextension.
Conclusion: Increasing millimeter thickness of uveal mela-noma is associated with increasing risk for metastasis.
Arch Ophthalmol. 2009;127(8):989-998
I N 1962, PAUL ET AL1 FROM THEArmed Forces Institute of Pathol-ogy reported the demographicdata and prognosis of 3852 pa-tients with uveal melanoma, the
largest collection of patients with intra-ocular melanoma then. Their data re-vealed the following information: mean ageat diagnosis of 55 years, approximately54% male, and less than 1% African Ameri-can. On the basis of the follow-up of 2652cases, mortality rate by actuarial methodwas 29% at 5 years, 40% at 10 years, and46% at 15 years, with a median survivalof 15" years. Ten-year mortality was lowerin younger patients (aged 20-39 years) at26% vs older patients (aged !70 years) at51%. In 1992, Diener-West et al2 pro-vided a meta-analysis of 8 published ar-ticles that further refined our understand-ing of uveal melanoma prognosis bygeneral tumor size. The combinedweighted estimate of 5-year mortality was16% for small tumors, 32% for medium tu-mors, and 53% for large tumors. Later, theCollaborative Ocular Melanoma Study dis-
closed melanoma-related mortality at 10years to be 17% to 18% for medium mela-noma and 40% to 45% for large mela-noma.3-6
Uveal melanoma prognosis has beenshown to be dependent on several clini-cal factors including tumor location in theciliary body, large tumor size, diffuse (flat)configuration, and extraocular extensionas well as histopathologic and cytoge-netic factors including epithelioid cell type,increased mitotic activity, infiltrating lym-phocytes, tumor vascular networks, andchromosomal mutations including mono-somy 3 and 8q addition.7,8 In several ar-ticles, tumor size has been identified as oneof the key clinical features predictive of me-tastasis.9,10 Furthermore, increasing tu-mor thickness, from small to medium tolarge, has been correlated with increas-ing risk for metastasis, but the exact rela-tionship per millimeter of tumor thick-ness has not been previously addressed,to our knowledge. In this analysis, weevaluate a large cohort of 8033 patients ob-served long-term for melanoma-related
Author Affiliations: OcularOncology Service, Wills EyeInstitute, Thomas JeffersonUniversity, Philadelphia,Pennsylvania.
(REPRINTED) ARCH OPHTHALMOL / VOL 127 (NO. 8), AUG 2009 WWW.ARCHOPHTHALMOL.COM989
©2009 American Medical Association. All rights reserved. at Thomas Jefferson University, on August 13, 2009 www.archophthalmol.comDownloaded from
8033 eyes each mm adds 5% risk for mets 2 mm (x5%) = 10% mets @10yrs 4 mm (x5%) = 20% 8 mm (x5%) = 40% 10mm (x5%) = 50%
emphasize early detection small melanoma reduce risk for mets
Choroid Melanoma
510
1520
2530
3540
4550
>50
510
1520
2530
3540
4550
>50

510
1520
2530
3540
4550
>50
Melanoma Prognosis
• tumor thickness
• ajcc classification
• age
• melanocytosis
• configuration
• genetics - most powerful
AJCC defined by base and thicknessMelanoma Prognosis
• tumor thickness
• ajcc classification
• age
• melanocytosis
• configuration
• genetics - most powerful
children have slightly better pronosis than adults
Melanoma Prognosis
• tumor thickness
• ajcc classification
• age
• melanocytosis
• configuration
• genetics - most powerful
Choroid melanoma in ocular melanocytosis
melanoma arising from ocular melanocytosis has 2x higher risk for metastasis than those without

Melanoma Prognosis
• tumor thickness
• ajcc classification
• age
• melanocytosis
• configuration
• genetics - most powerful
AJCC defined by base and thickness
diffuse melanoma
102
flat 18x18x2.0
Diffuse Melanoma
• special variant of flat melanoma <3 mm thickness• thin melanoma is better• thin (flat) melanoma could be worse
• diffuse melanoma carries 2x risk for metastasis compared to non-diffuse
if <3 mm:flat (diffuse) melanoma has 2x higher risk for metastasis than non-diffuse
Oncology ServiceWills Eye Hospital
Melanoma Prognosis
• tumor thickness
• ajcc classification
• age
• melanocytosis
• configuration
• genetics - most powerful
Prognosis of Uveal Melanoma in 500 CasesUsing Genetic Testing of Fine-NeedleAspiration Biopsy Specimens
Carol L. Shields, MD,1 Arupa Ganguly, PhD,2 Carlos G. Bianciotto, MD,1 Kiran Turaka, MD,1
Ali Tavallali, MD,1 Jerry A. Shields, MD1
Purpose: To determine the relationship between monosomy 3 and incidence of metastasis after genetictesting of uveal melanoma using fine-needle aspiration biopsy (FNAB).
Design: Noncomparative retrospective case series.Participants: Five hundred patients.Methods: Fine-needle aspiration biopsy was performed intraoperatively immediately before plaque radio-
therapy. The specimen underwent genetic analysis using DNA amplification and microsatellite assay. Systemicfollow-up was obtained regarding melanoma-related metastasis.
Main Outcome Measures: Presence of chromosome 3 monosomy (loss of heterozygosity) and occurrenceof melanoma metastasis.
Results: Disomy 3 was found in 241 melanomas (48%), partial monosomy 3 was found in 133 melanomas(27%), and complete monosomy 3 was found in 126 melanomas (25%). The cumulative probability for metastasisby 3 years was 2.6% for disomy 3, 5.3% for partial monosomy 3 (equivocal monosomy 3), and 24.0% forcomplete monosomy 3. At 3 years, for tumors with disomy 3, the cumulative probability of metastasis was 0%for small (0–3 mm thickness), 1.4% for medium (3.1–8 mm thickness), and 23.1% for large (!8 mm thickness)melanomas. At 3 years, for tumors with partial monosomy 3, the cumulative probability of metastasis was 4.5%for small, 6.9% for medium, and [insufficient numbers] for large melanomas. At 3 years, for tumors with completemonosomy 3, the cumulative probability of metastasis was 0% for small, 24.4% for medium, and 57.5% for largemelanomas. The most important factors predictive of partial or complete monosomy 3 included increasing tumorthickness (P " 0.001) and increasing distance to optic disc (P " 0.002).
Conclusions: According to FNAB results, patients with uveal melanoma demonstrating complete mono-somy 3 have substantially poorer prognosis at 3 years than those with partial monosomy 3 or disomy 3. Patientswith partial monosomy 3 do not significantly differ in outcome from those with disomy 3.
Financial Disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussedin this article. Ophthalmology 2011;118:396–401 © 2011 by the American Academy of Ophthalmology.
Several articles have been written on the relevance of ge-netic testing of uveal melanoma.1,2 In 1996, Prescher et al3
reported the landmark observation that uveal melanomawith chromosome 3 monosomy was an important predictorof worse patient prognosis. In that report, the authors ret-rospectively evaluated 54 enucleated eyes with uveal mel-anoma and correlated the copy number of chromosome 3 tothe known patient outcome. Several publications on genetictesting of melanoma from enucleated eyes have confirmedtheir observations.4–8
In 2002, Naus and associates9 reported that fine-needleaspiration biopsy (FNAB) could be reliably used to sampletumors for genetic testing of uveal melanoma and the resultscorrelated to those obtained by open biopsy after enucle-ation. In 2006, Midena and associates10 reported the firstclinical series of 8 eyes with uveal melanoma sampled byFNAB for genetic testing using fluorescent in situ hybrid-
ization. Later, Young et al11 used transscleral FNAB intothe tumor base for genetic testing in 18 eyes and found a50% yield. Shields et al12 added their experience with 140cases of FNAB for uveal melanoma and indicated that transpars plana FNAB into the tumor apex provided adequateDNA for microsatellite assay in 97% of cases with littlecomplication and no patient with tumor recurrence along theneedle tract. This report provides an analysis of patientprognosis in 500 cases based on results of genetic testingfrom FNAB for uveal melanoma.
Materials and Methods
We reviewed the clinical records of all patients on the OcularOncology Service at Wills Eye Institute, Philadelphia, Pennsylva-nia, with the diagnosis of uveal melanoma managed with FNAByielding DNA for genetic testing of chromosome 3 status at the
396 © 2011 by the American Academy of Ophthalmology ISSN 0161-6420/11/$–see front matterPublished by Elsevier Inc. doi:10.1016/j.ophtha.2010.05.023
questions how do we do it what are the results

after FNAB
plaque applied microarray analysis
monosomy 3 correlated with
• increasing thickness• peripheral location
monosomy 3 • small mm 25%• med mm 30%• large mm 50%
MLPA analysis
Mortality at 10 years disomy 3 0% monosomy 3 55% monosomy 3, 8q gain 71%
GEP gene expression profiling
2 classes correlate with survival at 8 years
• class 1 95% • class 2 31%
points•causes•features•therapy•collaborative ocular melanoma study•prognosis
Oncology ServiceWills Eye Institute
Carol Shields MD
Oncology ServiceWills Eye Hospital
Philadelphia PA USA
The Game of Uveal Melanoma
www.fighteyecancer.com