-
8/21/2019 8th Expert Comm 2012
1/72
WHO Expert Committeeon Leprosy
Eighth report
W H O T e c h n i c a l R e p o r t S e r i e s
This report contains the collective views of an international
group of experts and
does not necessarily represent the decisions or the stated
policy of the World Health Organization
-
8/21/2019 8th Expert Comm 2012
2/72
World Health Organization 2012
All rights reserved. Publications of the World Health
Organization are available on the WHO
web site (www.who.int) or can be purchased from WHO Press, World
Health Organization,
20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791
3264; fax: +41 22 791 4857;
e-mail: [email protected]).
Requests for permission to reproduce or translate WHO
publications whether for sale or for
noncommercial distribution should be addressed to WHO Press
through the WHO web site
(http://www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material
in this publication do not
imply the expression of any opinion whatsoever on the part of
the World Health Organization
concerning the legal status of any country, territory, city or
area or of its authorities, or concerning
the delimitation of its frontiers or boundaries. Dotted lines on
maps represent approximate border
lines for which there may not yet be full agreement.The mention
of specific companies or of certain manufacturers products does not
imply that they
are endorsed or recommended by the World Health Organization in
preference to others of a similar
nature that are not mentioned. Errors and omissions excepted,
the names of proprietary products
are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health
Organization to verify the
information contained in this publication. However, the
published material is being distributed
without warranty of any kind, either expressed or implied. The
responsibility for the interpretation
and use of the material lies with the reader. In no event shall
the World Health Organization be liable
for damages arising from its use.
This publication contains the collective views of an
international group of experts and does not
necessarily represent the decisions or the policies of the World
Health Organization.
Printed in Italy
WHO Library Cataloguing-in-Publication Data
WHO Expert Committee on leprosy: eighth report.
(WHO technical report series ; no. 968)
1. Leprosy - epidemiology. 2. Leprosy - prevention and control.
3. Leprosy - therapy.
I.World Health Organization. II.WHO Expert Committee on Leprosy
(2010: Geneva, Switzerland).
III.Series.
ISBN 978 92 4 120968 7 (NLM classification: WC 335)
ISSN 0512-3054
-
8/21/2019 8th Expert Comm 2012
3/72
iii
ContentsWHO Expert Committee on Leprosy v
Declarations of interest vii
1. Introduction 1
2. Leprosy in the world 3
2.1 Assessment of global data 42.2 Global leprosy situation in
2010 42.3 New case detection 42.4 Trends in case detection 42.5
Profiles of new cases 8
3. Epidemiology 11
3.1 Definition of a leprosy case 113.2 Classification 123.3
Transmission, infection and incubation period 123.4 Infectiousness
of leprosy 133.5 Risk factors 133.6 Interaction between HIV
infection and leprosy 133.7 Geographical variations 14
4. Chemotherapy and management 174.1 Chemotherapy 17
4.1.1 Standard MDT regimens 174.1.2 Existing second-line
antileprosy drugs 184.1.3 Promising new antileprosy drugs 194.1.4
Study on the uniform multidrug therapy regimen 214.1.5 Combined
therapy with four weeks of daily ofloxacin and rifampicin 214.1.6
Treatment regimens for special situations 224.1.7 Relapses after
multidrug therapy 22
4.2 Management of leprosy reactions and neuritis 234.2.1
Neuritis and nerve function impairment 234.2.2 Leprosy reactions
234.2.3 Treatment of leprosy reactions 24
4.3 Disability and rehabilitation 264.3.1 Magnitude of the
problem 264.3.2 Disability grading for leprosy 264.3.3 Prevention,
limitation and management of disabilities 264.3.4 Self-care 274.3.5
Community-based rehabilitation 27
5. Social issues 29
5.1 Equity, social justice and human rights 295.2 Gender 29
5.3 Enhancing the involvement of affected persons 305.4 Stigma
and stigmatization 30
-
8/21/2019 8th Expert Comm 2012
4/72
iv
5.5 Counselling 31
5.6 Residential care 31
6. Leprosy control and prevention 33
6.1 Improving the quality of leprosy services 336.2 Integrating
leprosy control into general health services 346.3 Referral system
346.4 Building and maintaining national capacity 366.5 Community
awareness and education 36
6.5.1 Community awareness 366.5.2 Information, education and
communication 37
6.6 Improving case detection 38
6.6.1 Case-finding and case-holding 386.6.2 Delay in diagnosis
386.7 Special areas and populations 38
6.7.1 Areas with a high disease burden 386.7.2 Areas with a low
disease burden 396.7.3 Underserved population groups 396.7.4 Urban
areas 40
6.8 Contact surveillance 416.9 Treatment adherence 42
6.9.1 Flexible treatment 426.10 Supply management for multidrug
therapy 42
6.11 Disease prevention 436.11.1 Primary BCG immunization
436.11.2 Immunoprophylaxis of contacts 446.11.3 Chemoprophylaxis of
contacts 446.11.4 Next steps prophylaxis strategy 45
6.12 Surveillance for drug resistance 456.13 Monitoring and
evaluation 46
6.13.1 Indicators for monitoring 466.13.2 Independent evaluation
of leprosy programmes 48
7. Strategy for further reducing the disease burden due
to leprosy setting targets 49
7.1 Elimination of leprosy as a public health problem 497.2 New
targets based on case detection and disability prevention 49
8. Research priorities 51
9. Conclusions and recommendations 53
Acknowledgements 55
References 57
-
8/21/2019 8th Expert Comm 2012
5/72
v
WHO Expert Committee on LeprosyGeneva, 1219 October 2010
Members
Dr Y.A. Al-Qubati, Taiz University School of Medicine, Taiz,
Yemen (Rapporteur)
Dr M.L.W. de Oliveira, Medical Professor, Rio de Janeiro Federal
University, Rio de Janeiro,
Brazil
Dr M. De Palma Caldas, Director, National Program for Control of
Tuberculosis and
Leprosy, Ministry of Health, Luanda, Angola
Professor P.E.M. Fine, Communicable Disease Epidemiology,
Infectious and TropicalDisease Department, London School of Hygiene
and Tropical Medicine, London,
England
Dr M.D. Gupte, Retired Director, National Institute of
Epidemiology, Indian Council of
Medical Research, Chennai, India1
Dr H.J.S. Kawuma, Medical Advisor, German Leprosy Relief
Association, Kampala,
Uganda
Dr T. Mori, Director Emeritus, Research Institute of
Tuberculosis, Japan Anti-Tuberculosis
Association, Kiyose, Tokyo, JapanDr H. Sansarricq, Former Head,
Leprosy Programme, WHO, Geneva, Switzerland
Professor W.C.S. Smith, Head, Department of Public Health,
Medical School, University
of Aberdeen, Aberdeen, Scotland (Chairman)
Professor G. Zhang, Deputy Director, Institute of Dermatology
and National Center for
Leprosy Control, Nanjing, China
Temporary advisers
Professor P.J. Brennan, Department of Microbiology, Immunology
and Pathology,
Colorado State University, Fort Collins, CO, USA
Professor S. Cole, Global Health Institute, Department of
Immunology, Ecole
Polytechnique Fdrale de Lausanne, Lausanne, Switzerland
Professor J.H. Grosset, Center for Tuberculosis Research, Johns
Hopkins University School
of Medicine, Baltimore, MD, USA
Dr S.K. Noordeen, Former Director, Action Programme for
Elimination of Leprosy, WHO,
Geneva, Switzerland
1 Unable to attend.
-
8/21/2019 8th Expert Comm 2012
6/72
vi
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
Mr J. Ramirez Jr., USA Coordinator and Board Member of
International Association for
Integration, Dignity and Economic Advancement (IDEA) and
American Leprosy
Missions, Houston, TX, USA
Representatives of other organizations
International Federation of Anti-Leprosy Associations (ILEP)
Mr D. Soutar, General Secretary, International Federation of
Anti-Leprosy Associations,
London, England
International Leprosy Association (ILA)
Dr M. Virmond, President, International Leprosy Association,
Bauru, BrazilRepresentative of Mr Y. Sasakawa, WHO Goodwill
Ambassador for Leprosy Elimination
Professor K. Kiikuni, Chair, Sasakawa Memorial Health
Foundation, Tokyo, Japan
Secretariat
Dr M.T. Htoon, Team Leader, WHO Global Leprosy Programme, WHO
Regional Office for
South-East Asia, New Delhi, India (Secretary)
Dr V. Pannikar, Temporary International Professional, WHO Global
Leprosy Programme,
WHO Regional Office for South-East Asia, New Delhi, India
-
8/21/2019 8th Expert Comm 2012
7/72
vii
Declarations of interestMembers of the WHO Expert Committee on
Leprosy reported the following:
Dr Y.A. Al-Qubati reported that he provides supervision to the
Leprosy Control
Programme of Yemen. For these services, he receives an
honorarium from the German
Leprosy and TB Relief Association (GLRA), which is a
nongovernmental organization.
Professor S. Cole reported that, through his previous employment
at Institut Pasteur, he
is a named inventor on a patent for antimycobacterial compounds
that have antileprosy
activity in a murine model. The patent in question has been
licensed to the company
Alere Technologies GmbH, for whom Professor Cole acts as a
consultant, with anannual income of approximately 20 000. He
currently teaches leprosy-related subjects
at the Ecole Polytechnique Fdrale de Lausanne.
Professor P.E.M. Fine reported that he is on the Editorial Board
of the journal Leprosy
Review. He also reviews grants related to leprosy research for
the Order of Malta, for
which he has received an honorarium payment for the past four
years.
Professor J.H. Grosset reported that he is a member of the
Scientific and Medical
Commission of Association Raoul Follereau of France as well of
the United States
of America/Japan Panel for Leprosy and Tuberculosis Research. He
receives no
remuneration for either position.
Dr H.J.S. Kawuma reported that he works as a Medical Adviser in
Uganda for the
German Leprosy and TB Relief Association (GLRA), which is a
nongovernmental
organization.
Dr S.K. Noordeen reported that he was involved in the
preparation of the background
documents for this meeting under an Agreement for the
Performance of Work (APW)
with WHO; this APW expired on 10 October 2010.
Mr J. Ramirez Jr reported that he serves as Managing Editor of
The Star, an international
magazine put together by persons affected by leprosy. He also
serves as the UnitedStates of America Coordinator for the
International Association for Integration, Dignity
and Economic Advancement (IDEA), an organization comprising
primarily persons
affected by leprosy. He receives no remuneration for either
position.
Professor W.C.S. Smith reported that he is President of the
Leprosy Mission International
and Chair of the Technical Commission of the International
Federation of Anti-Leprosy
Associations. He receives no remuneration for either
position.
-
8/21/2019 8th Expert Comm 2012
8/72
-
8/21/2019 8th Expert Comm 2012
9/72
1
1. IntroductionTe WHO Expert Committee on Leprosy held its
eighth meeting in Geneva,Switzerland, rom 12 to 19 October 2010.
Opening the meeting on behal oDr Margaret Chan, WHO
Director-General, and Dr Samlee Plianbangchang,Regional Director,
WHO South-East Asia Region, which hosts the GlobalLeprosy Programme
(GLP), Dr Hiroki Nakatani, Assistant Director-General,conveyed the
appreciation o Dr Chan and Dr Samlee or the gracious supportbeing
provided or GLP by WHO partners and experts.
Dr Nakatani noted the progress made towards elimination o
leprosy
since the Committees previous (seventh) meeting in 1997. He
recounted thecatalytic role played by World Health Assembly
resolution WHA44.9 (1991)(1) in pushing orward the leprosy agenda.
Te commitment to eliminateleprosy was reiterated by the World
Health Assembly in 1998 throughresolution WHA51.15 (2), and the
elimination target was reached globally atthe end o 2000 (3). Since
the introduction o multidrug therapy (MD) in1981, an estimated 15
million patients have been cured and disabilities havebeen
prevented in some 23 million individuals (4). Such an
achievement,Dr Nakatani stated, had been made possible by the
unique partnership betweengovernments, communities, WHO, academia,
industry and nongovernmental
organizations (NGOs). Progress in the elimination o leprosy had
been achievedthrough the synergistic efforts o all the supporting
organizations.
It was acknowledged that, despite significant progress in
controllingthe disease and reducing the disease burden, much still
remained to be done tosustain the gains and urther reduce the
impact o leprosy, especially in terms oits physical, mental and
socioeconomic consequences or those affected and ortheir
amilies.
Five-year initiatives or the elimination o leprosy were set out
in WHOpublications o 2000 (5) and 2005 (6); the most recent
initiative Globalstrategy for further reducing the disease burden
due to leprosy 20112016 waspublished in 2009 (7). Te emphasis in
these strategies has shifed to reducingthe occurrence o impairments
and disabilities due to leprosy and to ways oensuring the
sustainability and quality o leprosy services. Te strategies
haveincluded such specific issues as gender equity and human rights
and initiativesto reduce the stigma and discrimination aced by
people affected by leprosy andtheir amilies.
Te purpose o this eighth meeting o the Expert Committee was:
to analyse the global leprosy situation;
to review the current status o developments in areas such as
thetreatment o leprosy and its various complications;
-
8/21/2019 8th Expert Comm 2012
10/72
2
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
to consider the results o research and experience in leprosy
control
since the previous meeting and to review existing indicators
oprogress in order to determine whether better indicators could
beintroduced;
to advise on technical and operational issues relating to
efforts aimedat urther reducing the burden due to leprosy.
-
8/21/2019 8th Expert Comm 2012
11/72
3
2. Leprosy in the worldData on leprosy are reported to WHO
routinely by most countries,
except those o the European Region, and published annually in
the WeeklyEpidemiological Record (WER) (8). While such data are
useul in providinga broad picture o leprosy patterns and trends,
their interpretation is madedifficult by operational differences
between different national programmes andthe act that the data
cover different time periods.
In the past, the emphasis has been on prevalence data that is,
dataon the numbers o cases registered or treatment at the beginning
o the year.Because o the long duration o treatment, prevalence was
considered anappropriate measure, as it reflected the burden on
health services. Starting inthe early 1980s, prevalence declined
dramatically throughout the world as aconsequence o the shortened
treatment regimens that ollowed introduction oMD (9). Differences
in treatment duration between countries, as a result eithero
different programme policies or o different proportions o
multibacillary(MB) cases (which require longer treatment than
paucibacillary (PB) cases), havecomplicated the comparison o
prevalence data between countries.
More recently, the emphasis has shifed to case detection, as
this providesa more appropriate measure o recent transmission and
current epidemiological
circumstances. Case-detection statistics are useul or measuring
trends overtime provided that detection and registration policies
remain constant. However,recent aggressive case-finding in many
countries with higher leprosy burdenshas complicated the
interpretation o trends. Te act that data rom somelow incidence
countries may be influenced by an appreciable proportion ocases
occurring in immigrants provides a urther challenge: these cases do
notreflect autochthonous (local) transmission and may or may not be
included innational statistics.
Nevertheless, several patterns are clear. Te disease remains
endemicin all countries o the Arican and South-East Asia regions
and in most
countries o the Eastern Mediterranean Region. In the Region o
the Americas,autochthonous leprosy is ound in all countries with
the exceptions o Canada,Chile and several island countries o the
Caribbean. In the European Region,although data are not transmitted
to WHO, autochthonous leprosy is knownto persist at low levels in
several southern and eastern European countriesbut seems to have
disappeared rom much o the northern and western parto the
continent. In the Western Pacific Region, the disease persists in
mostlarge countries apart rom New Zealand and with the exception o
some smallisland nations. Tere is some evidence that transmission
may have stopped inJapan, although small numbers o autochthonous
cases still appear in older
individuals (8). Heterogeneity in leprosy requency and clinical
maniestationsbetween populations is a prominent eature o the
disease.
-
8/21/2019 8th Expert Comm 2012
12/72
4
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
2.1 Assessment of global dataSeveral broad trends over the past
30 years are evident. Te first is the
tremendous decline in registered prevalence since 1980, in all
countries,which reflects the shif rom long-term dapsone monotherapy
to shorter MD
regimens. Tis change was initiated by the WHO Study Group
recommendationin 1981 (9) and was achieved through aggressive
implementation o MD in all
countries during the 1990s. It has resulted in a major decline
in the burden o
leprosy on health services in endemic communities. Te second
broad trendrelates to incidence. Case-detection numbers and rates
have allen in almostall countries, reflecting both improvements in
socioeconomic conditions and
the effects o leprosy programmes. It is important to identiy and
enhancethose measures that have been most successul in bringing
about these alls.Te third trend is more difficult to demonstrate on
the basis o available databut relates to the decline in numbers and
proportions o cases with disabilitiesamong newly diagnosed
patients. Tere are only rough estimates o the totalnumber o
individuals with leprosy-attributable disabilities alive today
(4).
2.2 Global leprosy situation in 2010A total o 141 Member States
submitted reports to WHO at the beginning o
2010: 38 countries rom the Arican Region, 36 rom the Region o
the Americas,10 rom the South-East Asia Region, 22 rom the Eastern
MediterraneanRegion and 35 rom the Western Pacific Region (8). Tese
data are shown,by WHO region, in able 1, which reveals considerable
heterogeneity at theregional level, with highest numbers and rates
in the South-East Asia Region. Atthe beginning o 2010, the global
registered and reported point prevalence was211 903 cases; during
2009, 244 796 new cases were detected.
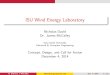
2.3 New case detection
Te reported trends in new case detection rom 2000 to 2009 are
shown inable 2, by WHO region. Decline was evident in all regions,
in particular inthe Arican and South-East Asia regions. Tese trends
were influenced bychanges in case-detection policies and aggressive
case-detection efforts insome large countries in the early years o
this century. Figure 1 shows the case-detection rates reported or
2009 or all countries that provided data to WHO:geographical
variation is clear.
2.4 Trends in case detection
able 2 shows that the global decline in case detection was
dramatic (about58%) during the period 20002005 and much more
limited (about 18%)
-
8/21/2019 8th Expert Comm 2012
13/72
Leprosy in the world
5
Table 1
Registered prevalence of leprosy and number of new cases
detected, as reported byWHO region (excluding the European Region),
2010
WHO region Registered
prevalencea
(beginning
of 2010)
New cases
detectedb
during 2009
Grade 2 disabilities
during 2009c
Among
new cases
Rate per
1 000 000
populationNumber %
African 30 497 (0.40) 28 935 (3.75) 3 146 10 4.1
Americas 43 370 (0.49) 40 474 (4.58) 2 645 6 3.0
South-East Asia 120 456 (0.68) 166 115 (9.39) 7 286 4 4.1
Eastern
Mediterranean
8 495 (0.17) 4 029 (0.70) 608 15 0.11
Western Pacific 8 635 (0.05) 5 243 (0.29) 635 12 0.4
Total 211 903 (0.37) 244 796 (4.27) 14 320 6.7 2.5
a Prevalence rate is shown in parentheses as the number of cases
per 10 000 population.b Case-detection rate is shown in parentheses
as the number of cases per 100 000 population.c New-case grade 2
disability rate per 1 000 000 population.
during the period 20062009. It shows also that the dramatic
decline observedduring 20002005 was largely the result o the 67%
reduction in detected
cases in the South-East Asia Region over that period; during
20062009 thereduction as in other WHO regions was 18%. Because o
the numerous
operational changes that have occurred at country and regional
levels duringthe past 10 years, it is impossible to determine which
actors were responsible
or the observed dramatic decline in case-detection rate or to
assess the
epidemiological significance o the decline.Te steady all in case
detection has not been uniorm, either among
countries or over the years, and fluctuations have occurred as a
result ooperational actors, particularly during special
case-detection campaignsorganized in certain countries (8).
Comparison o peak case-detection igures reached between 1992
and2009 with the igures or 2009 in the top 16 countries (i.e. those
accountingor 93% o the global disease burden) reveals two very
dierent trends.Detailed analysis identiies two groups o countries
one group o eight
showing considerable decline, and another group o eight showing
a verymodest decline.
-
8/21/2019 8th Expert Comm 2012
14/72
6
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
Table
2
Num
berofleprosycasesdetecteda
nnually,
byWHOregion(excludingtheEuropeanRegion),20002009
WHOregion
Annualcasedetection
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
African
54602
39612
48248
47006
46918
45179
34480
34468
29814
28935
Am
ericas
44786
42830
39939
52435
52662
41952
47612
42135
41891
40474
South-EastAsia
606703
668658
520632
405147
298603
201635
174118
171576
167505
166115
Eastern
Me
diterranean
5565
4758
4665
3940
3392
3133
3261
4091
3938
4029
We
sternPacific
7563
7404
7154
6190
6216
7137
6190
5863
5859
5243
Total
719219
763262
620638
514718
407791
299036
265661
258133
249007
244796
-
8/21/2019 8th Expert Comm 2012
15/72
Leprosy in the world
7
Figu
re
1
Case-detectionratesreportedfor2009
-
8/21/2019 8th Expert Comm 2012
16/72
8
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
In the 16 top countries there was a decline (rom peak
case-detection rate
to case detection in 2009) o 71.7% over a mean period o 9.2
years, indicatingan annual geometric decline o 12.9%.
In 8 o those 16 top countries, accounting or 64% o the global
burdeno cases, the decline over a mean period o 9.2 years was 78%
an annualgeometric decline o 15.2%. In the other 8 countries, with
29% o the globalburden o cases, the decline over a mean period o
9.9 years was only 27.7% anannual geometric decline o 3.2%.
2.5 Profiles of new cases
Statistics on age, sex, classification, disability status and
relapse are collectedroutinely by many countries and reported to
WHO. Tough potentially oconsiderable interest or monitoring trends,
these statistics vary considerablybetween countries or reasons that
include operational actors such as coverageand case-finding
methods, which makes comparisons difficult.
Age is traditionally broken down in terms o child (under age
15)versus adult cases; the proportion o cases among children would
be expectedto decrease as transmission declines. In the past, age
patterns have beeninfluenced by BCG (bacille CalmetteGurin)
vaccination, which shouldreduce cases among children, and by school
surveys, which selectively increase
case detection among children. Te proportion o child cases in
2009 variedbetween 0.6% in Argentina and 32% in the Comoros
Islands.
Data reported by sex should give some evidence o gender equity
inpopulations, but are complicated by the act that males have a
greater tendencyto MB disease and the proportion o MB disease
varies between populations.Te reported proportion or emales in 2009
varied rom 6.5% in Ethiopiato 60% in the Central Arican Republic.
Classification statistics have beeninfluenced by repeated changes
in criteria or classification over the past 20years; new cases
reported in 2009 ranged rom 32% MB in the Comoros to 95%MB in the
Philippines.
Statistics on grade 2 disability (G2D) are o particular interest
as theyprovide a potential indicator both o programme quality (a
programme withearly case detection should be associated with a low
proportion o G2D) and othe morbidity burden attributable to leprosy
(8). Te act that the proportion onew cases with G2D ranged rom 1.5%
(Liberia) to 23% (China) indicates thatcountries may differ
considerably in terms o how disabilities are detected andreported
as well as in the predominant clinical maniestations o the
disease.
Tese differences in patient profiles between countries highlight
ethnicand cultural differences between populations and differences
in national leprosycontrol programmes. Tey could be valuable
indicators o practices and trends
within countries and are thus important to national programme
managers (seesection 6.13 on monitoring and evaluation).
-
8/21/2019 8th Expert Comm 2012
17/72
Leprosy in the world
9
Table
3
Detectiontrendofleprosyin16cou
ntriesreporting1000newcasesduring19922000
Co
untry
N
umberofnewcasesdetected
19
92
1993
1994
1995
1996
1997
1998
1999
2000
Bangladesh
7307
6943
7983
8782
11225
11320
12351
14336
12135
Brazil
30094
34235
32515
3
2724
39792
43933
42055
43175
Ch
ina
3755
3755
2096
2109
1845
1854
2051
2051
1595
De
mocraticRep.o
fCongo
3247
3927
4195
4344
5526
3781
4221
3103
Eth
iopia
1936
4090
4790
5160
4747
4444
4457
4457
4931
Ind
ia
517000
456000
414894
39
1760
415302
519952
634901
537956
474286
Ind
onesia
13219
12638
17255
1
3492
15071
15337
18367
17477
13539
Ma
dagascar
2050
740
4701
4676
3921
11555
8957
8704
7689
Mo
zambique
1732
1930
2583
3430
4225
4195
3764
5488
6617
My
anmar
9816
12018
8303
6577
6935
9086
14357
30479
10262
Ne
pal
5953
6152
6169
4783
6602
7446
6570
18693
6661
Nigeria
4381
4381
7827
7147
6871
7176
7230
7918
7918
Philippines
7169
3442
4450
3988
4051
4942
3490
3390
2596
Sri
Lanka
944
1059
1897
1528
776
1376
1757
1700
Sudan
1980
1489
3100
1765
2126
2633
2077
2426
2045
Un
itedRep.o
fTanzania
2731
2596
2596
2747
2798
3535
5081
4640
Total
6096
39
555415
524516
49
5230
532514
651288
723483
706489
602892
-
8/21/2019 8th Expert Comm 2012
18/72
10
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
Table
3
(continued)
Detectiontrendofleprosyin16cou
ntriesreporting1000newcasesduring20012009
Co
untry
N
umberofnewcasesdetected
20
01
2002
2003
2004
2005
2006
2007
2008
2009
Bangladesh
10
740
9844
8712
8242
7882
6280
5357
5249
5239
Brazil
41
070
38365
49206
4
9384
38410
44436
39125
38914
37610
Ch
ina
1
726
1646
1404
1499
1658
1506
1526
1614
1597
De
mocraticRep.o
fCongo
4
980
5037
7165
1
1781
10737
8257
8820
6114
5062
Eth
iopia
4
523
4632
5193
4787
4698
4092
4187
4170
4417
Ind
ia
617
993
473658
367143
26
0063
169709
139252
137685
134184
133717
Ind
onesia
13
286
12377
14641
1
6549
19695
17682
17723
17441
17260
Ma
dagascar
8
599
5482
5104
3710
2709
1536
1521
1763
1572
Mo
zambique
5
713
5830
5907
4266
5371
3637
2510
1313
1191
My
anmar
9
684
7386
3808
3748
3571
3721
3637
3365
3147
Ne
pal
13
830
13830
8046
6958
6150
4235
4436
4708
4394
Nigeria
5
981
5078
4799
5276
5024
3544
4665
4899
4219
Philippines
2
669
2479
2397
2254
3130
2517
2514
2373
1795
Sri
Lanka
2
309
2214
1925
1995
1924
1993
2024
1979
1875
Sudan
1
299
1361
906
722
782
884
1706
1901
2100
Un
itedRep.o
fTanzania
4
656
6497
5279
5190
4237
3450
3105
3276
2654
Total
749
058
595716
491635
38
6424
285687
247022
240541
233263
227849
-
8/21/2019 8th Expert Comm 2012
19/72
11
3. Epidemiology3.1 Definition of a leprosy caseTe presence o
classical clinical signs plays a major role in the diagnosis
oleprosy, although demonstration o the causative organism by
slit-skin smears,histopathology or polymerase chain reaction (PCR)
is sometimes used tosupport the diagnosis. Since the availability o
laboratory acilities or slit-skin smear or histopathology is
restricted in many endemic countries, and thecurrent PCR technology
is still not adequately reliable, diagnosis o most caseso leprosy
in the field will continue to be based on clinical evidence, at
least or
the time being. However, this situation may not be ideal when
disease incidenceis declining and where more sensitive diagnostic
tools and procedures may beneeded to ensure that all cases that
need treatment are diagnosed and cured (10).
Leprosy should be suspected in people with any o the
ollowingsymptoms or signs:
pale or reddish patches on the skin;
loss, or decrease, o eeling in the skin patches;
numbness or tingling o the hands or eet;
weakness o the hands, eet or eyelids;
painul or tender nerves; swelling o or lumps in the ace or
earlobes;
painless wounds or burns on the hands or eet.
Although most leprosy patients have skin lesions that are
visible,experienced field workers are aware that a great variety o
skin lesions aremaniest in cases o the disease. Some are very
diffused and difficult todistinguish rom the normal skin. In these
cases, the other symptoms and signsbecome important or
diagnosis.
Leprosy is diagnosed when at least one o the ollowing cardinal
signs
is maniested:
definite loss o sensation in a pale (hypopigmented) or reddish
skinpatch;
a thickened or enlarged peripheral nerve, with loss o sensation
and/or weakness o the muscles supplied by that nerve;
the presence o acid-ast bacilli in a slit-skin smear.
Te quality o diagnosis should be monitored as part o regular
technicalsupervision. I there are indications o substantial
over-diagnosis, a validation
exercise on a representative sample o cases can be conducted to
determine themagnitude o the problem.
-
8/21/2019 8th Expert Comm 2012
20/72
12
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
3.2 ClassificationLeprosy is a classic spectral disease, being
maniest in a variety o clinicalorms related to the type and
strength o the immune response. A strong cellularimmune response is
effective in curtailing the multiplication o M. leprae andis thus
associated with PB disease. A weak cellular response allows bacilli
toreplicate reely in the body, leading to MB disease orms.
In 1981, the WHO Study Group on Chemotherapy o Leprosy orControl
Programmes classified leprosy as MB and PB according to the degreeo
skin-smear positivity (9). Tis was an essentially operational
classification,intended to serve as the basis or chemotherapy.
Multibacillary leprosy included
polar lepromatous (LL), borderline lepromatous (BL), and
mid-borderline(BB) cases in the RidleyJopling classification, with
a bacteriological index o2+ or more at any site in the initial skin
smears. Paucibacillary leprosy includedindeterminate (I), polar
tuberculoid () and borderline tuberculoid (B)cases in the
RidleyJopling classification, with a bacteriological index o
-
8/21/2019 8th Expert Comm 2012
21/72
Epidemiology
13
and other armadillo species, and its precise contribution to
leprosy in the
Americas, is unknown and is a topic or research (13).Inection is
thought to occur primarily by the respiratory route but there
is also evidence that it may occur through injured skin (14). Te
mechanism odissemination rom the primary site to the final location
in the skin and nervesis unclear. Te incubation period rom inection
to clinical maniestations isvariable, but appears to be shorter or
PB disease (in the order o 25 years) thanor MB (in the order o 510
years and sometimes much longer) (15).
3.4 Infectiousness of leprosy
Te inectiousness o leprosy patients is related to the size o the
bacillarypopulation in the body. It has been shown that a single
dose o riampicinreduces the load o viable bacilli to such low
levels that it is no longer possibleto cultivate the organism in an
animal model. In public health terms, it isreasonable to conclude
that inectiousness becomes negligible afer the start oMD (16).
3.5 Risk factorsLeprosy cases occur at all ages in endemic
populations, although the diseaseis rare among the very young
because o the long incubation period beorethe appearance o clinical
maniestations. Cases are more commonly reportedin males than emales
in most populations. While this may be the result obiased case
ascertainment or selective hiding o the disease in emales in
somepopulations, the prevalence o MB disease is higher among males
than emalesin all populations, which may reflect a gender
difference in immune responseor exposure. Contact with a known
(especially MB) case is recognized as a riskactor in all
populations, as is the absence o a history o BCG vaccination.
Lowsocioeconomic status is likewise associated with leprosy in all
populations, orreasons that remain unclear. Although there is
evidence that certain geneticactors may be associated with leprosy,
the population-attributable risk is smalland leprosy should
thereore not be considered a genetic disease. Familyclustering is
determined predominantly by contact, not by shared genes. Itis
useul to recollect that leprosy extended north o the Arctic Circle
in thenineteenth century and is thus compatible with cold as well
as warm climates.Te gradual disappearance o the disease rom high
latitudes over the pastcentury is thought to be attributable
largely to socioeconomic actors.
3.6 Interaction between HIV infection and leprosyIn the 1980s it
was eared that the HIV pandemic might have the same effect on
leprosy as it has on tuberculosis. It was predicted that
patients with leprosy andHIV coinection would be at increased risk
o lepromatous disease and aster
-
8/21/2019 8th Expert Comm 2012
22/72
14
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
clinical evolution, and that leprosy would be more difficult to
treat. None o these
ears has has been realized, and the interaction between HIV and
M. leprae isknown to be ar more subtle than that between HIV and M.
tuberculosis. Mosto the recent epidemiological, clinical and
pathological studies show neither anincreased HIV prevalence among
leprosy cases nor an alteration in the clinicalspectrum o leprosy
among coinected patients. On the other hand, there is someevidence
that immune-mediated reactions (particularly ype 1) occur moreofen
in coinected patients (17).
Tere are several reports o leprosy presenting as an
immunereconstitution disease among patients starting highly active
antiretroviral
treatment (HAAR), probably as a result o the unmasking o an
existingsubclinical inection or incubating disease (18).
Histopathological observationsreveal a normal spectrum o appearance
in biopsies o leprosy lesions romcoinected patients. Although no
data indicate whether HIV inectionexacerbates nerve damage in
leprosy, it may alter the immune response toM. leprae in nerves
because o its neuropathic effect. LeprosyHIV coinectedpatients
respond equally well to MD and experience similar
side-effectprofiles. Some studies showed that patients with
lepromatous disease andHIV coinection were at a higher risk o
reversal reactions and neuritis butresponded as expected to steroid
therapy.
In considering the relationship o HIV and leprosy it is also
importantto recognize that HIV coinection may influence
health-seeking behaviour andthis in turn may affect the chance o
leprosy being diagnosed (19).
3.7 Geographical variationsGeographical variations are a
striking eature o leprosy at every level. As shownin Figure 1,
there are considerable differences between countries: among the141
countries reporting, just 7 countries accounted or 85% o all new
casesdetected in 2009.
Geographical variations are also prominent within countries. In
India in2009, or example, 12 out o 35 states (with 79% o the
population) accountedor 94% o all new leprosy cases. In Brazil rom
2005 to 2007, 10 populationclusters with 17% o the population
contributed 53% o all cases in that country.In Indonesia, in 2007,
14 out o 33 provinces (with 60% o the population)accounted or 83% o
cases. In China, in 2009, 3 out o 31 provinces (with 12.4%o the
population) had 54.5% o cases. Tese regional patterns have long
beenrecognized, but their mechanism remains unclear.
Even at the local level, leprosy cases are ofen reported to be
ar morecommon in certain villages or valleys than in others. In
some circumstances
this may be the result o biased case ascertainment selective
searching and ahigh diagnostic suspicion in certain areas but the
observation is so common
-
8/21/2019 8th Expert Comm 2012
23/72
Epidemiology
15
in leprosy-endemic populations that it is more likely to reflect
important risk
actors that are not yet understood.Tese variations have two
important implications. First, they indicate
the importance o risk actors that remain to be elucidated and
whoserecognition could be useul in control o the disease. Second,
they allowtargeting o leprosy control activities, which improves
the costeffectivenesso control programmes. However, while targeting
may be good policy in somecircumstances, the very wide distribution
o the disease, ofen at very lowrequency, needs to be kept in mind i
appropriate services are to be provided toall cases.
-
8/21/2019 8th Expert Comm 2012
24/72
-
8/21/2019 8th Expert Comm 2012
25/72
17
4. Chemotherapy and management4.1 Chemotherapy4.1.1 Standard MDT
regimens
Tree standard first-line drugs riampicin, cloazimine and dapsone
areavailable or use in multidrug regimens o fixed duration, none o
which shouldbe used as monotherapy.
Multibacillary leprosy
Te standard adult treatment regimen or MB leprosy is:
riampicin: 600 mg once a month
cloazimine: 300 mg once a month, and 50 mg daily
dapsone: 100 mg daily
Duration: 12 months.
Te standard child treatment regimen or MB leprosy is:
riampicin: 450 mg once a month
cloazimine: 150 mg once a month, and 50 mg every other day
dapsone: 50 mg dailyDuration: 12 months.
Paucibacillary leprosy
Te standard adult treatment regimen or PB leprosy is:
riampicin: 600 mg once a month
dapsone: 100 mg daily
Duration: 6 months.
Te standard child treatment regimen or PB leprosy is:
riampicin: 450 mg once a month
dapsone: 50 mg daily
Duration: 6 months.
Note: Children under 10 years o age should receive
appropriatelyreduced doses o drugs, such as
riampicin: 10 mg/kg body weight once a month
dapsone: 2 mg/kg body weight per day
cloazimine: 1 mg/kg body weight to be given on alternate
days,depending on the dosage.
-
8/21/2019 8th Expert Comm 2012
26/72
18
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
Tere may be occasional cases o dapsone hypersensitivity although
the
drug is relatively non-toxic in the doses used. In the event o
hypersensitivity,dapsone must be stopped immediately and the
adverse reaction reported(dapsone syndrome).
4.1.2 Existing second-line antileprosy drugs
Since the mid-1980s, the bactericidal activities o the new
fluoroquinolones
(pefloxacin and ofloxacin), a new macrolide (clarithromycin) and
a tetracycline(minocycline) have been demonstrated (2023). In the
limited experimental
tests carried out in mouse models, all these drugs were able to
render the
mouse inoculums non-inective afer only 1 month o treatment. Te
newdrugs showed greater bactericidal activity than dapsone and
cloazimine. In thenude mouse model o leprosy, a single dose o a
minocycline+clarithromycin
combination killed 96% o viableM. lepraeand a single dose o a
minocycline+clarithromycin+ofloxacin combination killed 98.4% a
bactericidal effect close
to the 99.5% killing effect o a single dose o riampicin
(24).
Tese drugs were also tested in humans with MB leprosy.
Ofloxacin,given at a daily dose o 400 mg, killed more than 99.99% o
the viable M. leprae
afer only 4 weeks o therapy (2527). Similar bactericidal
activities were
demonstrated with minocycline and clarithromycin (28). Te
bactericidalactivity o a single dose o
minocycline+clarithromycin+ofloxacin was testedin patients with MB
leprosy against a single dose o riampicin alone and
4 weeks o standard MD. Although the bactericidal effect o the
three-drugcombination was similar to that observed in the mouse
model, the severe
gastrointestinal side-effects related to the use o
clarithromycin were sufficientto preclude the routine use o this
drug in the field (29). A single dose o
ofloxacin 400 mg + minocycline 100 mg killed 6898% o viableM.
lepraeanda single dose o riampicin 600 mg + ofloxacin 400 mg +
minocycline 100 mg
killed more than 99%.
Ofloxacin
O the many fluoroquinolones that have been developed, ofloxacin
was the
first o interest or leprosy. Te results o clinical trials have
indicated that itsoptimal dosage or the treatment o leprosy is 400
mg daily. While a single
dose o ofloxacin displayed a modest bactericidal effect, 22
doses killed 99.99%o the viable M. leprae in lepromatous patients.
Side-effects include nausea,diarrhoea and other gastrointestinal
complaints, and a variety o central nervoussystem complaints
including insomnia, headaches, dizziness, nervousness and
hallucinations. Most side-effects do not require discontinuation
o ofloxacintreatment, and serious problems are rare (26).
-
8/21/2019 8th Expert Comm 2012
27/72
Chemotherapy and management
19
Minocycline
Minocycline, a member o the tetracycline group o antibiotics,
has significantbactericidal activity against M. leprae greater than
that o clarithromycinalthough much less than that o riampicin. Te
standard dose o 100 mg dailygives a peak serum level that exceeds
the minimum inhibitory concentration(MIC) o minocycline against M.
leprae by a actor o 1020 and has shownpromising bactericidal
activity in lepromatous patients. Te side-effects ominocycline
include discolouration o teeth during their period o ormation,and
the drug should thereore not be given during pregnancy or to inants
andchildren. Other side-effects include occasional pigmentation o
the skin and
mucous membranes, various gastrointestinal symptoms and central
nervoussystem complaints, including dizziness and unsteadiness.
Minocycline ismost commonly used or the long-term treatment o acne,
indicating that itis generally well tolerated; however, some rare
but serious side-effects suchas autoimmune hepatitis and lupus
erythematosus-like syndrome have beenreported recently (30).
Clarithromycin
Clarithromycin is a member o the macrolide group o antibiotics
and displayssignificant bactericidal effect againstM. lepraein mice
and in humans (27, 28).
In lepromatous patients, a daily dose o 500 mg o clarithromycin
kills 99% oviableM. lepraewithin 28 days and >99.9% in 56 days.
Te most common side-effect is gastrointestinal irritation
(including nausea, vomiting and diarrhoea),which is particularly
requent when clarithromycin is given at a dose o2000 mg.
4.1.3 Promising new antileprosy drugs
In recent years moxifloxacin (a fluoroquinolone) and riapentine
(a long-acting riamycin derivative) have been identified as having
highly promisingantimycobacterial activities.
Moxifloxacin
Moxifloxacin is a ourth-generation synthetic fluoroquinolone
with broad-spectrum antibiotic activity against both Gram-positive
and Gram-negativebacteria. Like other fluoroquinolones it unctions
by inhibiting bacterialtopoisomerase II (DNA gyrase) and
topoisomerase IV enzymes that arerequired or bacterial DNA
replication, transcription and repair and thusinhibits cell
replication.
Moxifloxacin has shown potent bactericidal activity against M.
leprae
in mice and humans. Given at 150 mg/kg in mice (equivalent to
400 mg inhumans), it is as active as riampicin. A single dose o
moxifloxacin 150 mg/kg
-
8/21/2019 8th Expert Comm 2012
28/72
20
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
killed five times more M. leprae than a single dose o ofloxacin
150 mg/kg.
In humans, given at a dose o 400 mg daily, it killed more than
99% M. lepraewithin 7 days, and no viable bacilli were demonstrated
rom day 28 onwards. Itis more potent than ofloxacin, minocycline
and clarithromycin (31, 32).
Rifapentine
Riapentine is a semi-synthetic riamycin derivative with a
prolonged action(serum hal-lie 15 hours) compared with riamycin
(hal-lie 3 hours).Because o its long hal-lie, riapentine was
investigated in the 1980s and1990s in combination with other
medications or the once-weekly treatment
o tuberculosis.Like all riamycin derivatives, riapentine targets
DNA-dependent RNA
polymerase, which is necessary or RNA synthesis and thus or
production oproteins. Tis process is different in human
(eukaryotic) cells and bacteria,and all riamycin derivatives,
including riapentine, affect the process only inbacteria.
Resistance to riapentine can develop during tuberculosis treatment
byselection o pre-existing riamycin-resistant mutants within large
populations otubercle bacilli. I resistance develops to one
riamycin-type drug, the bacteriabecome resistant to all riamycin
derivativess.
Riapentine can cause some body fluids such as saliva, urine,
breast milk,
tears and sweat to become orangered in colour. Te skin, teeth
and tongue mayalso change colour and dentures and contact lenses
can be permanently stained.Riapentine may reduce the effectiveness
o contraceptive pills, and other ormso contraception should
thereore be used during treatment with this drug.
In leprosy treatment, riapentine exhibited more potent
bactericidalactivity than riampicin in both in mice and humans. In
the mouse oot-padmodel, a single riapentine dose o 10 mg/kg killed
20 times more M. lepraethana single riampicin dose o 10 mg/kg. A
single dose o a riapentine+moxifloxacin+minocycline combination
killed 50 times moreM. lepraethan a single dose
oriampicin+ofloxacin+minocycline (32).
Diarylquinoline (R207910)
Diarylquinoline offers a new mechanism o antituberculosis action
byinhibiting mycobacterial adenosine triphosphate (AP) synthase. Te
drugpotently inhibits drug-sensitive and drug-resistant M.
tuberculosisin vitro andshows bactericidal activity both in
patients with drug-susceptible pulmonarytuberculosis and in those
with multidrug-resistant (MDR) pulmonarytuberculosis (3336).
AgainstM. lepraein mice, a single dose o 25 mg/kg is
bactericidal. Te
drug is as active as riampicin, riapentine and moxifloxacin and
more activethan minocycline. In mice, multiple doses o 1 mg/kg five
times a week were as
-
8/21/2019 8th Expert Comm 2012
29/72
Chemotherapy and management
21
active as a single dose o 25 mg/kg. Similarly, a dose o 25 mg/kg
once a month
was as active as the same dose given five times a week.
Diarylquinoline has along hal-lie (1 week in humans). Te drug may
be used to replace minocyclinein the new combined regimens or
once-a-month treatment or leprosy.
Other new drugs active against Mycobacterium tuberculosis
complex
Te activities o PA-824 (a nitroimidazopyran) and linezolid (an
oxazolidinone)against M. leprae are rather modest (37). A single
100 mg/kg dose o PA-824showed no significant bactericidal activity;
afer five consecutive days otreatment the bactericidal effect was
significantly weaker than that o a single
dose o diarylquinoline or o moxifloxacin. Tus, PA-824 has a
narrow spectrumo activity, limited primarily to theM.
tuberculosiscomplex (37). Neither PA-824nor linezolid which yielded
similar results is a promising drug or thetreatment o leprosy.
4.1.4 Study on the uniform multidrug therapy regimen
In order to shorten the duration o treatment and simpliy drug
supplylogistics, a multicentre study has been launched to assess
the efficacy o theWHO-recommended 6-month MD regimen or MB leprosy
in new cases oall types o o leprosy, both MB and PB. Patients are
to be actively ollowed
or a minimum period o 8 years afer completion o treatment to
monitorreactions and relapses. Tis study aims to recruit a total o
5000 newlydetected, previously untreated patients (2500 PB and 2500
MB). It is designed asa multicentre, open field study; some 3400
patients have been recruited so arand about 2000 patients have
completed their treatment. Te preliminary reportis avourable (38),
but no conclusions can yet be drawn.
4.1.5 Combined therapy with four weeks of daily ofloxacin and
rifampicin
Te possibility o urther shortening the duration o MD was
evaluated in ariampicinofloxacin field trial. Tis was a
multicentre, double-blind trialorganized by the Steering Committee
on Chemotherapy o MycobacterialDiseases (HEMYC), a component o the
UNDP/World Bank/WHO SpecialProgramme or Research and raining in
ropical Diseases (DR). Multibacillaryleprosy patients were
randomized into our groups and treated with:
24 months o standard WHO-MD or MB leprosy (as
positivecontrol);
12 months o WHO-MD or MB leprosy;
12 months o WHO-MD or MB leprosy with riampicin 600 mg
plus ofloxacin 400 mg daily during the initial 4 weeks; and
riampicin 600 mg plus ofloxacin 400 mg daily or 4 weeks.
-
8/21/2019 8th Expert Comm 2012
30/72
22
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
Te published results (39) showed that the trial regimen o
daily
riampicin and ofloxacin or 4 weeks resulted in an unacceptable
relapse rate o13%. Tus, daily treatment with riampicin and
ofloxacin or 4 weeks is not aviable option.
4.1.6 Treatment regimens for special situations
Patients who cannot take rifampicin
Special treatment regimens are required or individual patients
who cannottake riampicin because o side-effects or intercurrent
diseases, such as chronichepatitis, or who have been inected with
riampicin-resistant M. leprae. Te
ollowing 24-month regimen is recommended: Daily administration o
50 mg cloazimine, together with two o the
ollowing drugs 400 mg ofloxacin, 100 mg minocycline or 500
mgclarithromycin or 6 months, ollowed by daily administration o50
mg cloazimine, together with 100 mg minocycline or 400 mgofloxacin
or an additional 18 months (40). I available, ofloxacin maybe
replaced by moxifloxacin 400 mg, which has stronger
bactericidalactivity againstM. leprae.
Patients who cannot take rifampicin
Multibacillary leprosy patients who reuse to take cloazimine
because o skindiscolouration also need a sae and effective
alternative treatment. In suchpatients, cloazimine in the normal
12-month MD may be replaced by ofloxacin,400 mg daily, or by
minocycline, 100 mg daily, or 12 months. Similarly, ofloxacinmay be
replaced by moxifloxacin, 400 mg.
In 1997, the WHO Expert Committee on Leprosy (41)
alsorecommended the ollowing alternative 24-month regimen or adult
MBleprosy patients who reuse to take cloazimine: riampicin, 600 mg
oncea month, ofloxacin, 400 mg once a month, and minocycline, 100
mg once amonth, or 24 months.
Patients who cannot take dapsone
I dapsone produces severe toxic effects in any PB or MB leprosy
patient, it mustbe stopped immediately. No urther modification o
the regimen is required orpatients with MB leprosy. For PB leprosy,
however, cloazimine in the dosageused in the standard MD or MB
leprosy should be substituted or dapsonein the 6-month treatment
regimen.
4.1.7 Relapses after multidrug therapy
Relapse afer MD remains low, even afer almost 30 years o
widespread use.Some reports suggest that the risk o relapse is
higher in a subset o patients
-
8/21/2019 8th Expert Comm 2012
31/72
Chemotherapy and management
23
with a pre-MD average bacterial index (BI) o 4 or more. Recently
published
WHO operational guidelines recommend that it may be advisable to
treat anMB patient with high BI or more than 12 months, taking
careul considerationo the clinical and bacteriological evidence. A
number o studies have reportedthat retreatment o relapses ollowing
dapsone monotherapy or MD withanother course o standard MD regimens
is highly successul (4143).
Although demonstration o organisms resistant to dapsone is
relativelycommon, probably because o pre-existing dapsone-resistant
strains, there arereports on organisms resistant to riampicin,
cloazimine or quinolones afercompletion o treatment with MD. Most
investigators consider that a relapseafer MD is most likely to be
due to persisters and only rarely to resistance.
Tis is borne out by the results o molecular tests on biopsies
rom a smallnumber o relapsed cases.
Several risk actors or relapses in leprosy have been suggested,
includingpersisters, re-inection, drug resistance,
inadequate/irregular therapy, use omonotherapy, high initial BI,
number o skin lesions and lepromin negativity.Te risk o relapse in
patients coinected with HIV is a possibility and needsurther
investigation. Currently, diagnosis o relapse is based mainly on
clinicaleatures such as appearance o a new lesion and a
significantly increased BI.Some studies have demonstrated the
utility o histopathological changesand simple serological tests in
confirming the diagnosis o relapse. Tere is a
possibility o developing molecular tests based on PCR or early
identificationo relapses (44).
4.2 Management of leprosy reactions and neuritis4.2.1 Neuritis
and nerve function impairment
Nerve unction impairment (NFI) results rom a variety o
pathological andimmunological processes taking place in the
peripheral nerves. Te presence olongstanding NFI at the time o
registration and MB classification are the mainrisk actors or
subsequent development o serious nerve damage in leprosy.
Te proportion o new cases with NFI at diagnosis may be as high
as 20%.Leprosy reactions, particularly ype 1 or reversal reactions,
are regardedas the leading cause o NFI. Most patients, particularly
those with MB disease,develop NFI events and reactions during the
first 6 months afer startingtreatment: these events diminish over
time (including time afer MD) and veryew patients develop such
events afer the second year ollowing completiono MD. However,
nerves can be unctionally impaired in the absence o anyobvious
signs or symptoms o reactions (silent neuropathy) (45, 46).
4.2.2 Leprosy reactions
ogether, the two major clinical types o leprosy reactions ype 1
or reversalreaction, and ype 2 or erythema nodosum leprosum (ENL)
reaction may
-
8/21/2019 8th Expert Comm 2012
32/72
24
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
affect 3050% o all MB leprosy patients (47). Because M. leprae
inects
peripheral nerves, the inflammation associated with reactions is
a medicalemergency: severe nerve injury may develop rapidly, with
subsequent losso sensation, paralysis and deormity (48). No
clinical or laboratory tests areavailable that can accurately
predict either which patients are the most likely todevelop a
reaction or when such a reaction might occur.
ype 1 reactions are recognized by swelling and redness o skin
patchesand are regarded as severe when associated with loss o nerve
unction (losso sensation or muscle weakness), pain or tenderness in
one or more nerves,when the red swollen skin patches are on the ace
or overlying another major
nerve trunk, when skin lesion anywhere becomes ulcerated and
when there ismarked oedema o the hands, eet or ace. ype 1 reactions
occur across thewhole leprosy spectrum.
ype 2 or ENL reactions are characterized by the appearance o
tender,erythematous nodules in MB patients. Tey are regarded as
severe whennumerous ENL nodules occur in association with high ever
and neuritis orbecome ulcerated and when other organs (e.g. eyes,
testes, lymph nodes andjoints) are involved. A severe ENL reaction
can be recurrent and chronic andmay vary in its presentation.
Promising new markers to identiy patients at high risk o
developing
reactions have been demonstrated but additional studies are
needed todetermine their sensitivity and specificity (49).
4.2.3 Treatment of leprosy reactions
Te mainstay o treatment o both types o reaction is
corticosteroids becauseo their anti-inflammatory effects. Some
studies have demonstrated betterresults when steroids are
administered or longer than 12 weeks, particularlyin the treatment
o neuritis. o ensure that due attention is given to the risk
oserious side-effects o long-term use o steroids, such as weight
gain, pepticulcer, diabetes, hypertension, reactivation o
tuberculosis, osteoporosis andpsychiatric disorders, these drugs
should be prescribed only by someoneproperly trained in their use.
rials o prophylactic steroids have demonstratedonly a shortterm
effect on prevention o NFI. Several studies have indicatedthat NFI
improves to some extent without steroid therapy, which may
beattributable to MD (45).
Cyclosporine has been used to treat ype 2, or ENL, reactions
with mixedresults (50). Azathioprine and methotrexate have been
used in combinationwith prednisolone or treatment o ype 2 reactions
and may offer a steroid-sparing regimen or treatment (51).
Pentoxyylline, a NF-alpha inhibitor, has
shown no significant benefit. Inhibition o lymphocyte
prolieration by severalpotent antimetabolites has had little or no
consistent effect in the treatment o
-
8/21/2019 8th Expert Comm 2012
33/72
Chemotherapy and management
25
either type o leprosy reaction. Similarly, clinical inhibitors o
NF-alpha, IL-2,
and other cytokines have had minimal effects on reactions (52,
53).Although several studies have demonstrated the useulness o
thalidomide in the treatment o acute ENL reactions, its use is
restrictedbecause o its teratogenic effects and o ethical and legal
considerations. Inaddition, thalidomide availability is limited by
restrictions on its import andsupply in many endemic countries. WHO
thereore recommends its use onlyunder strict medical supervision in
specialized reerral acilities.
It is important to educate all patients about the signs and
symptoms oreactions and NFI and to encourage them to return to
health centres immediatelyin case o such events even those that
occur afer completion o MD.
National leprosy programmes should continue to ensure that an
efficientreerral system exists within the general health services
to allow timely nerveunction assessment and diagnosis and treatment
o patients experiencingreactions, neuritis and related
complications such as iritis. Regular availability oantireaction
drugs should be ensured.
Guidelines for the management of severe reactions
Severe ype 1 or reversal reaction
Severe reversal (ype1) reactions should be treated with a
courseo steroids usually lasting 36 months. Patients still on
antileprosytreatment should continue the standard course o MD.
Severe ype 2 or ENL reaction
Severe ENL reaction should be treated with a standard course
oprednisolone (daily dosage not exceeding 1 mg/kg body weight)or 12
weeks. Patients who experience reactions while still onMD should
continue the standard treatment with MD. I MDhas been completed,
the management o ENL should not includerestarting o MD. Adequate
doses o analgesics to control everand pain should be
prescribed.
A combination o cloazimine and corticosteroids is indicated
ormanagement o patients with severe ENL who are not
respondingsatisactorily to treatment with corticosteroids alone or
or whomthe risk o corticosteroid toxicity is high. Prednisolone
should begiven in daily dosage not exceeding 1 mg/kg body weight.
reatmentwith cloazimine should start with 100 mg three times a day
or amaximum o 12 weeks, with the dose then tapering to 100 mg twice
aday or 12 weeks and to 100 mg once a day or 1224 weeks.
Management o ENL reaction with cloazimine alone is indicatedin
cases o severe ENL when the use o corticosteroids is
-
8/21/2019 8th Expert Comm 2012
34/72
26
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
contraindicated. reatment with cloazimine should ollow the
same
guidelines as when it is used in combination with
prednisolone.However, the total duration o treatment with high-dose
cloazimineshould not exceed 12 months.
It should be noted that it takes about 46 weeks or cloazimineto
take ull effect in controlling ENL. Management o severe ENLreaction
is complex and should be undertaken only by physiciansat reerral
acilities, who will adjust the dose and duration o anti-reaction
drugs according to patients individual needs.
4.3 Disability and rehabilitationDisability in new patients as
well as in people who have completed treatment remains a challenge.
Addressing the problem o disability alls within thebroad scope o
public health but requires support rom social services,
thecommunity and the voluntary sector.
4.3.1 Magnitude of the problem
Currently there is no robust inormation on the numbers o people
affected bydisability due to leprosy at either global or national
level. While inormation
on G2D among new cases is regularly collected, only limited
inormation isavailable on disability among people who have
completed MD.For planning and implementation o rehabilitation
measures or people
with leprosy-related disabilities, it is important to estimate
the total prevalenceo G2D in the population. It would thereore be
useul to include, in all nationalprogrammes, a new measure o total
prevalence o G2D in the population asone o the main indicators or
monitoring urther reduction in disease burden.As well as inormation
on total prevalence o G2D, more detailed inormationwill be needed
at the local level on the specific rehabilitation needs,
includingphysical, social and economic needs, o leprosy-affected
communities.
4.3.2 Disability grading for leprosy
Te three-grade WHO disability grading system (0, 1, 2) has been
in use orseveral years and has proved to be a good basis or
measuring the magnitude othe problem and organizing physical
rehabilitation activities at both individualand community
levels.
4.3.3 Prevention, limitation and management of disabilities
Prevention o disabilities begins with early diagnosis o leprosy,
recognition
and treatment o complications such as neuritis and reactions,
identificationo patients at risk o developing secondary disability,
and timely intervention.
-
8/21/2019 8th Expert Comm 2012
35/72
Chemotherapy and management
27
Although or programme purposes statistics are compiled only or
G2D, it is
important that inormation on grade 1 disability is also made
available at theclinic level so that such patients are supported by
preventive measures suchas provision o ootwear and protective
devices and advice on sel-care. Tesepreventive measures are equally
relevant or individuals who are cured and donot normally present
themselves at clinics except as part o an active ollow-up.
Management o disabilities should be an integral part o routine
treatmentservices at the clinic level and should also cover people
who have been cured.Available services should include the provision
o aids and appliances, specialistmedical care, and surgical
reconstruction and rehabilitation acilities.
4.3.4 Self-care
Sustaining the prevention and management o disabilities requires
greateremphasis on sel-care and sel-help through counselling o
those in need, aswell as o their amilies and community members.
Sel-care measures shouldinclude care o dry, denervated skin o palms
and soles in order to preventwounds, ulcers and skin cracks.
Prevention o occupational injuries, such asburns caused by handling
hot objects, should be an important aspect o thecounselling o
individuals with sensory loss in the limbs, as should care o
theeyes where indicated.
4.3.5 Community-based rehabilitation
Following the Declaration o Alma-Ata (1978), stating that health
is aundamental human right, and in consideration o the constraints
o scope,expertise and resources imposed on specialized medical
rehabilitation services,WHO introduced the strategy o
community-based rehabilitation (CBR). Tiswas intended to enhance
the quality o lie or people with disabilities throughcommunity
initiatives, promoting the concept o the inclusive communityand
using local resources to support the rehabilitation o people with
disabilities
within their own communities. However, stigma and lack o
knowledge meantthat specialized rehabilitation services and many
CBR programmes ailed torecognize people with leprosy-related
disabilities as equal members o thecommunity requiring
rehabilitation.
In recent years there has been a change in attitude towards
leprosy.Stigma has lessened in many countries and people affected
by leprosy nowmore ofen remain within their amilies and
communities. As a result,involvement o amily and community members
is now seen as critical orempowering people affected by leprosy,
encouraging them to play an activerole in their rehabilitation and
urther reducing the stigma o the disease. Te
central strategy o CBR is to acilitate community action to
ensure that peoplewith disabilities including those disabled by
leprosy have the same rights
-
8/21/2019 8th Expert Comm 2012
36/72
28
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
and opportunities as all other community members, including, or
example,
equal access to health care, education, skills training,
employment, amily lie,social mobility and political empowerment.
Tus CBR has become a legitimatestrategy or meeting the needs o
people affected by leprosy and enhancingtheir quality o lie.
Community-based rehabilitation calls or a comprehensive,
rights-basedapproach, involving sectors other than health. Te
recently published WHO/ILEP Technical guide on community-based
rehabilitation and leprosy: meetingthe rehabilitation needs of
people affected by leprosy and promoting quality of life(54)
highlights the importance o the CBR approach, and the
WHO/UNESCO/ILO/IDDC Communitybased rehabilitation: CBR guidelines
(55) includes asupplementary section on leprosy and CBR that urther
promotes the inclusiono leprosy-affected persons in broader CBR and
development programmes.
-
8/21/2019 8th Expert Comm 2012
37/72
29
5. Social issuesTe Seventh Meeting o the Expert Committee on
Leprosy did not addresssocial issues except in reerence to the
meeting held in 1952 (40), whichrecommended that the issue o human
rights be acknowledged, especially withregard to the particularly
negative impact o leprosy on women.
In June 2010, WHO hosted a meeting o regional managers,
individualsaffected by leprosy and various experts with the aim o
developing guidelinesor increasing the participation o
leprosy-affected persons in leprosy controlactivities (56). Te
meeting identified several areas, with correspondingstrategies, or
enhancing the empowerment o those affected. Te empowerment
strategies aim to increase the inclusion o persons affected by
leprosy indifferent aspects o community lie, including health,
housing, social welare,education and decision-making, as well as in
socioeconomic activities. Teresult o this enhanced participation
and empowerment is threeold: greaterwillingness o individuals
affected by leprosy to seek diagnosis; completion othe prescribed
treatment plans; and improved quality o lie.
5.1 Equity, social justice and human rightsTe principle o equity
is based on the premise that disparities or inequalities in
the levels o health enjoyed by different populations are
unnecessary, avoidableand unjust. It is the right o individuals
enshrined in the Universal Declarationo Human Rights (57). In 2008,
the United Nations Convention on the Rightso People with
Disabilities came into orce. Tis Convention represents a majornew
international legal instrument and, with its greater ocus on
inclusivity indevelopment, is o critical importance in protecting
the rights o all personswith disabilities, including those affected
by leprosy.
Further potential or improving the condition o persons affected
byleprosy and promote their rights to quality o lie was enshrined
in the UnitedNations Human Rights Council resolution on the
Elimination o discriminationagainst persons affected by leprosy and
their amily members, which receivedunanimous approval in June 2008
(58). Tis has been urther strengthenedwith the adoption by the
Human Rights Council in September 2010 o a set oprinciples and
guidelines on the elimination o discrimination against
personsaffected by leprosy and their amilies (59).
Equity, social justice and human rights in the world o leprosy
aredifficult to attain without continually challenging those who
label this populationin pejorative terms; consistent respect or
those affected is essential.
5.2 Gender
Te sociocultural norms in many societies discriminate against
girls andwomen, ofen consigning them to a lower status and value
and placing them at
-
8/21/2019 8th Expert Comm 2012
38/72
30
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
considerable disadvantage in terms o access to resources and
goods, decision-
making power, and choices and opportunities in all spheres o
lie. Since womenappear to suffer more negative health consequences
o leprosy than men (60),the topic o women in the world o leprosy is
a cross-cutting issue.
Health systems need to give greater emphasis to gender in the
trainingo health proessionals and health-care workers in order to
improve awareness oand sensitivity to gender concerns and
disparities (61).
Programmes need to identiy patterns o service use, levels
oparticipation in decision-making and perceptions o quality o care.
Whendefining priorities in leprosy control services, it is critical
to increase womensinvolvement in health action at all levels. Tere
is evidence that integration oleprosy services into general health
services, coupled with decentralization, hasimproved the
accessibility o services or all population groups in general andor
the emale population in particular (62).
5.3 Enhancing the involvement of affected personsPersons
affected by leprosy have a major role to play in leprosy
services,especially in the areas o advocacy, awareness,
rehabilitation and case-finding.Organized efforts by these
individuals are vital to promoting a positive publicperception o
and attitude to the disease; to effecting change in any legal
measures that are discriminatory in nature; and to ensuring that
leprosycontrol continues to occupy an important place in the health
policy rameworko the country.
Persons affected by leprosy also have a clear role and
responsibility inthe area o community involvement or social action.
Teir involvement canlead to country-specific definitions o the
quality o service to be provided, aswell as help the programme in
setting the standard or quality. Tey can provideregular inormation
to programme managers, supervisors or sponsors onthe quality o
services. Teir participation in research and evaluation can
assistin identiying needs, particularly with respect to the
accessibility and quality o
services being provided. Tey can contribute to reorming leprosy
services andprovide a ocus on issues o discrimination and stigma.
As role models, theyare the major contributors to cultivating
positive attitudes.
5.4 Stigma and stigmatizationLeprosy has a strong social and
psychological impact on all individualsaffected by the disease
(including amily members) and the societies in whichthey live. Te
disease carries significant stigma: communities respond withear,
rejection, insensitivity, use o pejorative terms, and general
devaluation
o the status o affected persons who, in turn, eel threatened by
the rest osociety. Socioeconomic rehabilitation o affected people
can play a major role in
-
8/21/2019 8th Expert Comm 2012
39/72
Social issues
31
improving their quality o lie, increasing their social
integration and reducing
leprosy-related stigma. Some reports suggest that stigmatization
is in decline,particularly where integrated programmes are
unctioning. Although stigmamay change in nature rom overt rejection
o those affected by leprosy to theindividuals ear o what might
happen as a result o having leprosy (6365) it ofen persists long
afer the disease has ceased to be a public health problem.
Te response o the programme should be twoold. It is importantto
address the community, responding to unanswered questions,
dispellingmisunderstandings and myths, and helping people to
acknowledge andaccept those affected by leprosy without prejudice.
It is equally importantto empower persons affected by leprosy to
deal with the daily challenges omisunderstanding and
miscommunication.
Te treatment programme should also include counselling as
animportant management strategy, and should introduce guidelines
and protocolsor building the competence o health proessionals in
three important areas:transorming knowledge into inormation that is
easily understandable bypersons affected by leprosy; managing
people and tasks; and communicationskills. A well-trained health
person should be able to advise, support, guide,share inormation
and empower others.
5.5 CounsellingTe purpose o counselling is to provide support to
individuals in emotionaldistress in order to lessen their distress
and allow them to unction optimallyin their everyday lives.
Counselling by trained and experienced proessionalsis a critical
resource that should be available to all persons affected by
leprosyand that should ofen be extended to their amily members. It
should becommunity-based and initiated at the time o diagnosis.
When provided by individuals who are amiliar with the
community,knowledgeable about the emotional impact o leprosy and
proessionally trainedcan have a positive impact on the social
issues discussed in sections 4.14.4.
5.6 Residential carePersons newly diagnosed with leprosy should
not be admitted or long-term institutional care. Te consequence o
such institutionalization is ofensignificant difficulty in
returning to independent living and in the evento institutions
closing there is the problem o finding suitable
alternativeaccommodation or inpatients.
-
8/21/2019 8th Expert Comm 2012
40/72
-
8/21/2019 8th Expert Comm 2012
41/72
33
6. Leprosy control and preventionElimination o leprosy as a
public health problem defined, in terms oprevalence, as ewer than 1
leprosy case registered or treatment per 10 000population was
achieved at the global level at the end o 2000. Morerecent
approaches, however, have ocused on monitoring new case
detectionand working to reduce the burden o disease. Eradication o
leprosy is notconsidered to be easible since there is no test or
inection and the incubationis very long; moreover, many aspects o
the natural history o the disease(such as subclinical inection and
the role o carrier states) are unknown (or
example, there is at least one animal reservoir the armadillo o
M. leprae).Te current approach targets reduction in disability in
new cases based on earlycase detection, treatment with MD, and
good-quality services that includeprevention o disability to reduce
the burden o disease.
6.1 Improving the quality of leprosy servicesImproving the
quality o care not only enables all the needs o the patient to
bemet but also makes it possible to attract more people to come or
examination,which results in improved case detection. Te elements o
good-quality careinclude:
easy accessibility o health care;
availably o MD;
management o complications and side-effects;
disability care and prevention o disability (POD);
CBR;
respect or individual rights o patients; and
elimination o stigma and gender bias.
Tese elements can be ensured by improving:
the capacity o peripheral health services to deal with essential
tasks(diagnosis, classification, MD, need or reerral, etc.);
availability o appropriate tools/protocols, resources and the
necessarycompetence at reerral points;
the counselling o patients and their amilies; and
community awareness.
Patients should be reviewed at the end o MD treatment to
confirmthe completion o treatment and to assess any new nerve
unction impairments
-
8/21/2019 8th Expert Comm 2012
42/72
34
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
that may have developed during treatment. Patients should be
counselled at this
point on the risks o uture reactions and relapses and on
recommended actions.
Sel-care should be re-emphasized and advice given on prevention
o disability.
6.2 Integrating leprosy control into general health servicesTe
need to integrate leprosy control into general health services is
based
largely on the principles o equity and sustainability. In
addition, integration
allows issues o stigma and discrimination against persons
affected by leprosy
and their amilies (66, 67) to be more effectively addressed. In
an integrated
programme, leprosy control activities should be conducted in
multipurpose
settings by health workers within the general health services.
However,integration does not mean that specialized personnel no
longer have a role.
Tey mustbe a part o the integrated programme at the national
level; may also
be available at the intermediate (regional or provincial) or
even district level;
and are expected to play a vital part in coordination, planning
and technical
support and in monitoring o progress in leprosy control (68).
Almost all
endemic countries have already involved general health workers,
to a varying
extent, in antileprosy activities.
Te key issue is that o improving the perormance o the
integrated
programme, which may be achieved by:
raising community awareness o the main eatures o leprosy its
curability and the availability o ree treatment and
increasing
community participation in case-finding, case-holding, MD
delivery and POD;
building capacity within general health services;
ensuring regular supervision and technical support by
workers
rom higher levels o the general health system and by
specialized
leprosy workers;
ensuring adequate reerral services;
ensuring availability o the necessary quantities o MD drugs,
o
other medical supplies and o materials or handling
complications
and care at the peripheral level.
6.3 Referral systemAn ideal reerral system ensures that patients
can receive appropriate, high-
quality care or their condition in the closest possible acility
and at the lowest
cost given the resources available to the health system (69).
Improving theeffective unctioning o reerral systems requires
progress in three areas: reerral
-
8/21/2019 8th Expert Comm 2012
43/72
Leprosy control and prevention
35
system design, acilitation o the transer o both patients and
inormation
between levels, and effective reerral discipline.
Improving the design o the reerral system requires
identification o the
services that can appropriately be provided at each level o care
in both rural and
urban settings, including community- and home-based care and
primary health
care at district, secondary and tertiary levels and in
specialized hospitals (70).
Te development o effective transportation arrangements is
critical to
ensure that patients rom remote areas have a air chance o being
reerred
to specialists. When the patients treatment has finished at the
higher-level
acility, back-reerral to the original acility must include
inormation regarding
treatment, investigations already done and ollow-up expected at
the lower level.Te bypassing o lower-level services by patients is
a common problem
that leads to overcrowding o higher-level acilities. Effective
reerral discipline
demands improvements in the quality o care at lower levels and
in the
availability o resources in order to strengthen primary health
care services,
giving them greater credibility and making them more attractive
to patients.
A reerral system will unction effectively i all services
providers adhere to the
reerral discipline, reerring appropriately and ollowing the
agreed protocols o
care (71).
Te reerral system has a crucial role in defining the quality o
carethat a programme can provide to persons affected by leprosy; it
should include
identification o the primary-, secondary- and tertiary-level
services that are
available to meet a whole range o needs (72). An integrated
leprosy control
programme thus needs the support o an efficient reerral system
to be effective.
Currently, the reerral system in most programmes is either
non-existent or is
very weak as regards meeting programme needs. Strengthening
existing reerral
acilities and, where necessary, establishing an adequate number
o such acilities
to orm the national reerral network should be one o the key
priorities or
integrated leprosy control programmes.
Te reerral system should include a network o individuals
andinstitutions capable o providing services. Teir tasks and
responsibilities should
be clearly defined, along with procedures and protocols or good,
standardized
clinical practices, including protocols or the flow o patients
and inormation
to and rom different levels. Te system should build
partnerships, coordinating
the work o all care providers to maximize care and reduce cost.
An effective
reerral system requires good communication and coordination
between
levels o care: a range o options are available or effective
communication and
transer o inormation, including personal visits, telephone,
post, e-mail, and
telemedicine). It is also important to ensure that persons
affected by leprosy areprovided with support or travel rom remote
areas when needed.
-
8/21/2019 8th Expert Comm 2012
44/72
36
WHOTechnicalReportSeries,No.96
8,2
012
WHO Expert Committee on Leprosy Eighth report
Besides direct patient care, reerral hospitals has other roles
within the
health system, such as teaching and research, as well as
technical support andquality assurance to lower levels o health
services (70). Tey may also be closelyinvolved in other public
health interventions such as disease-specific healthpromotion and
education activities.
6.4 Building and maintaining national capacityCapacity building
assumes greater importance against the backdrop o adeclining
disease burden, shrinking resources, competing interests and
prioritiesand, most importantly, loss o clinical expertise in
leprosy. Te Enhanced Global
Strategy envisages a two-pronged approach,















![MINUTES OF STATE EXPERT APPRAISAL COMMITTEEmpseiaa.nic.in/pdfs/Minutes-146.pdf · MINUTES OF STATE EXPERT APPRAISAL COMMITTEE 146th MEETING 8th November 2013 [V.Subramanian, Chairperson]](https://img.pdfslide.us/doc/110x75/5aaea55e7f8b9aa8438c5448/minutes-of-state-expert-appraisal-of-state-expert-appraisal-committee-146th-meeting.jpg)