Embed Size (px)
Citation preview

ENDOCRINE
DISORDERS
GERARD GABRIEL P. REOTUTAR, RM, RN, MAN

ANATOMIC AND PHYSIOLOGIC OVERVIEW
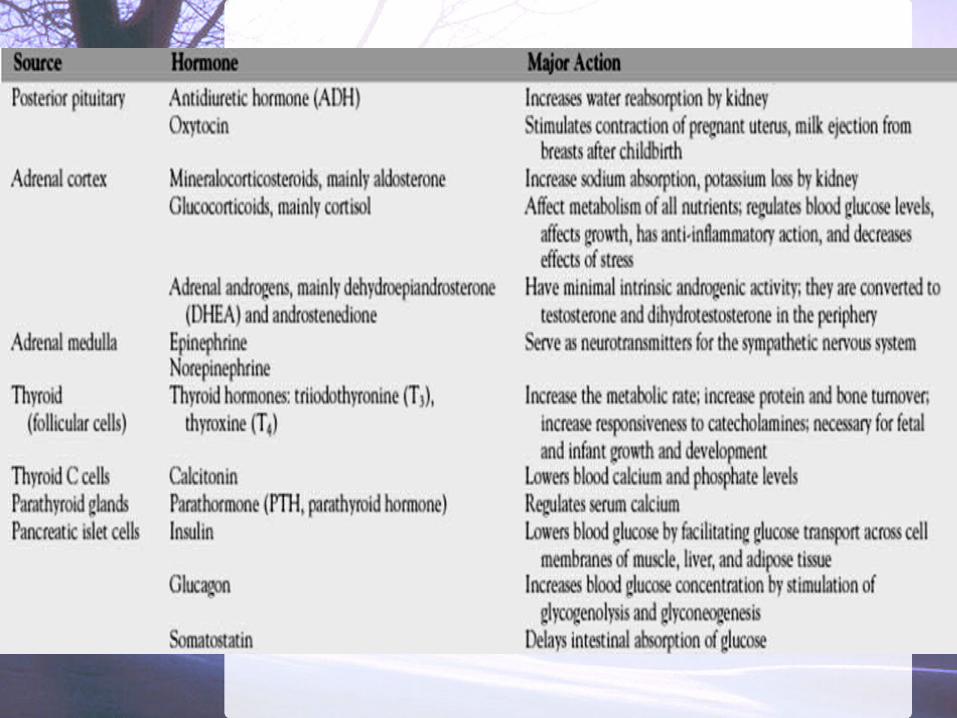
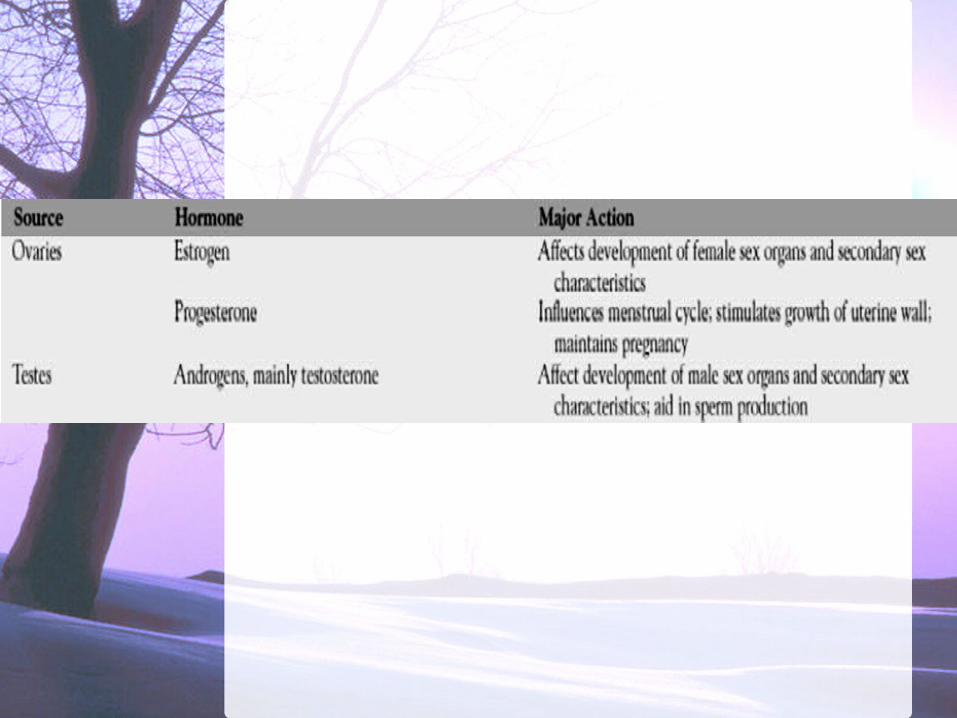
The endocrine system involves the release of chemical substances
known as hormones to regulate and integrate
body functions. Generally, these
hormones are produced by the endocrine
glands, but some are also produced by other
tissues.



THE PITUITARY GLAND
The pituitary gland, or hypophysis, is commonly referred to as the master
gland because of the influence it has on
secretion of hormones by other endocrine glands.
The round structure, about 1.27 cm (1/2 inch) in
diameter, is located on the inferior aspect of the brain.
The pituitary gland is divided into anterior and
posterior lobes. It is controlled by the
hypothalamus, an adjacent area of the brain that is
connected to the pituitary by the pituitary stalk.


Anterior PituitaryThe major hormones of the anterior pituitary gland are:
follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin, adrenocorticotropic hormone (ACTH),thyroid-stimulating hormone (TSH) growth hormone (GH) (somatotropin). melanocyte-stimulating hormone
POSTERIOR PITUITARY
The important hormones secreted by the posterior lobe of the pituitary gland are:
vasopressin, (antidiuretic hormone (ADH) oxytocin

Anterior PituitaryOversecretion of the anterior pituitarygland most commonly involves ACTH or GH and results in Cushing’s syndrome or acromegaly, respectively.
Acromegaly, an excess of GH in adults, results in bone and soft tissue deformities and enlargement of the viscera without an increase in height.
Oversecretion of GH results in gigantism in children; a person may be 7 or even 8 feet tall.

Insufficient secretion of GH during childhood results in generalized limited growth and dwarfism.
Under secretion (hyposecretion) commonly involves all of the anterior pituitary hormones and is termed panhypopituitarism. In this condition, the thyroid gland, the adrenal cortex, and the gonads atrophy (shrink) because of loss of the trophic-stimulating hormones.

Hypopituitarism may result from destruction of the anterior lobe of the pituitary gland.
Postpartum pituitary
necrosis (Sheehan’s syndrome) is another uncommon cause of failure of the anterior pituitary. It is more likely to occur in women with severe blood loss, hypovolemia, and
hypotension at the time of delivery.

POSTERIOR PITUITARY
The most common disorder related to posterior lobe dysfunction are:
diabetes insipidus, a condition in which abnormally large volumes of dilute urine are excreted as a resultof deficient production of vasopressine,
SIADH or Syndrome of Inappropriate Anti-Diuretic Hormone

DIABETES INSIPIDUS
Diabetes insipidus (DI) is a disorder of the posterior lobe of
the pituitary gland that is characterized
by a deficiency ofADH (vasopressin).
Excessive thirst (polydipsia) and large
volumes of dilute urine characterize the
disorder.
Causes:secondary to head trauma, brain tumor (eg, metastatic disease, lymphoma of the breast or lung).surgical ablation or irradiation of the pituitary gland. infections of the central nervous system (meningitis, encephalitis, tuberculosis)failure of the renal tubules to respond to ADH; nephrogenic form may be related to hypokalemia, hypercalcemia, and a variety of medications (eg, lithium, demeclocycline)

Clinical Manifestationsenormous daily output of very dilute, waterlike urine with a specific gravity of 1.001 to 1.005 occurs. The urine contains no abnormal substances such as glucose or albumin. intense thirst, causing the patient to drink 2 to 20 L of fluid daily and craves cold water. attempts to restrict fluids cause the patient to experience an insatiable craving for fluid and to develop hypernatremia and severe dehydration.

Assessment and Diagnostic Findings
The fluid deprivation test is carried out by withholding fluids for 8 to 12 hours or until 3% to 5% of the body weight is lost. The patient is weighed frequently during the test.

Plasma and urine osmolality studies – the inability to increase the specific gravity and osmolality of the urine is characteristic of DI. The patient continues to excrete large volumes of
urine with low specific gravity and experiences weight loss, increasing serum osmolality, and elevated serum sodium
levels. The patient’s condition needs to be monitored frequently
during the test, and the test is terminated if tachycardia, excessive weight loss, or hypotension develops.
Concurrent measurements of plasma levels of ADH and plasma and urine osmolality as well as a trial of desmopressin (synthetic vasopressin) therapy and intravenous (IV) infusion of hypertonic saline solution. If the diagnosis is confirmed and the cause (eg, head injury) is not obvious, the patient is carefully assessed for tumors that may be causing the disorder.

MEDICAL MANAGEMENT
The objectives of therapy are :
(1) to replace ADH (which is usually a long-term therapeutic program), (2) to ensure adequate
fluid replacement, (3) to identify and correct the underlying intracranial pathology. Nephrogenic causes require different management approaches.

PHARMACOLOGIC THERAPY
Desmopressin (DDAVP), a synthetic vasopressin without the vascular effects of natural ADH. It is administered intranasally; the patient sprays the solution into the nose through a flexible calibrated plastic tube. One or two administrations daily (ie, every 12 to 24 hours) usually control the symptoms. Vasopressin causes vasoconstriction;
thus, it must be used cautiously in patients with coronary artery disease.
Intramuscular administration of ADH, vasopressin tannate in oil, is used if the intranasal route is not possible. The medication is administered every 24 to 96 hours. The vial of medication should be warmed or shaken vigorously before administration. The injection is administered in the evening so that maximum results are obtained duringsleep. Abdominal cramps are a side effect of this medication. Rotation of injection sites is necessary to prevent lipodystrophy.

Clofibrate (Atromid-S), a hypolipidemic agent, has been found to have an antidiuretic effect on patients with DIwho have some residual hypothalamic vasopressin. Chlorpropamide (Diabinese) is also used in mild forms of the disease because they potentiate the action of vasopressin. Thiazide diuretics, mild salt depletion,and prostaglandin inhibitors (ibuprofen [Advil, Motrin], indomethacin [Indocin], and aspirin) are used to treat the nephrogenic form of DI.

ANTIDIURETIC HORMONE SECRETION
The syndrome of inappropriate
antidiuretic hormone
(SIADH) secretion includes excessive ADH secretion from the pituitary gland even in the face of subnormal serum
osmolality.

SIADH is often of nonendocrine origin:
occur in patients with bronchogenic carcinoma in which malignant lung cells synthesize and release ADH. occurr in patients with severe pneumonia, pneumothorax, and otherdisorders of the lungs, as well as malignant tumors that affect other organs.

Disorders of the central nervous system, such as head injury, brain surgery or tumor, and infection, are thought to produce SIADH by direct stimulation of the pituitary gland.
Some medications (eg, vincristine [Oncovin], phenothiazines, tricyclic antidepressants, thiazide diuretics) and nicotine have been implicated in SIADH; they either directly stimulate the pituitary gland or increase the sensitivity of renal tubules to circulating ADH.

Interventions include:
elimination of the underlying causerestricting fluid intake Diuretics such as furosemide (Lasix)
If severe hyponatremia is present.
Close monitoring of fluid intake and output, Daily weighingurine and blood chemistries, neurologic status is indicated for the patient at risk for SIADH.
Supportive measures and explanations of procedures and treatments assist the patient in managing this disorder.
























![Endocr Disr PDF Website Review 3-6-2013[1]](https://img.pdfslide.us/doc/110x75/577cdbe81a28ab9e78a96781/endocr-disr-pdf-website-review-3-6-20131.jpg)


