Embed Size (px)
Citation preview

clinical case
LEFT ADRENALECTOMY FOR ADRENAL CARCINOMA
Wilmar Azal Neto, Fernandes Denardi Division of Urology, UNICAMP
CLINICAL BACKGROUND Forty four year-old female patient was referred to our clinic with a left adrenal mass in CT abdominal scan. Patient presented with hirsutism, dysmenorrhea and severe fascial redness.
Comorbidities: Systemic hypertension.
Background: Acute pancreatitis in 2006 which developed a symptomatic pancrreatic pseudocyst and underwent caudal pancreatectomy with splenectomy in 2007.
Physical exam: Good performance status, fascial redness, obese. Hirsutism. Distended abdomen, hairy skin, subcostal incision on left side, no palpable abdominal mass.
LABS: 1)Creatinine = 1,0 mg/dl (VR<1,2 mg/dl). Cortisol: 31 mg/dl (VR: 3-18 mg/dl). 2) Abdominal CT scan (Figure 1)
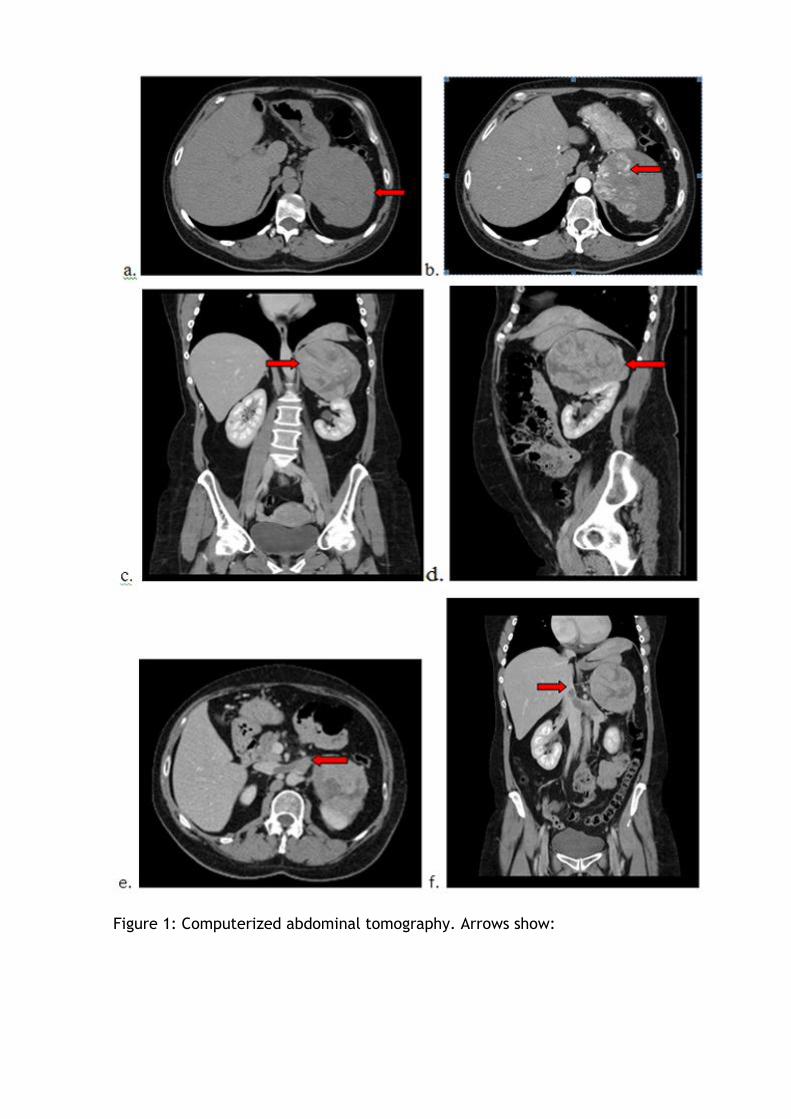
Figure 1: Computerized abdominal tomography. Arrows show:
a. Axial cut: non-contrast enhanced CT, arrow shows large adrenal lesion
b. Axial cut: Arterial phase, arros shows intense contrast enhancement
c. Coronal cut: arrow shows large adrenal lesion dislodging left kidney
d. Sagital cut: arrow shows large adrenal lesion
e. Axial cut: arrow shows left adrenal vein thrombi extending into left renal vein and inferior vena cava
f. Coronal cut: Arrow shows vena cava thrombi
DIAGNOSIS: Cushing syndrome secondary to functioning left adrenal carcinoma
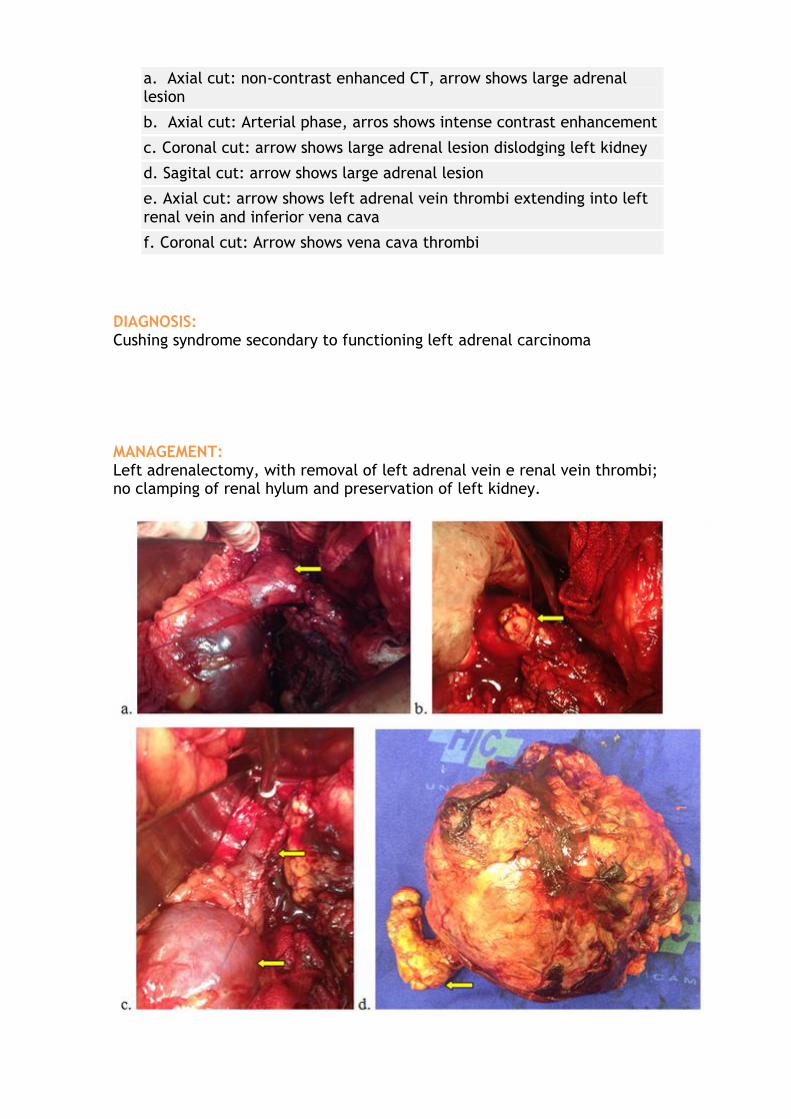
MANAGEMENT: Left adrenalectomy, with removal of left adrenal vein e renal vein thrombi; no clamping of renal hylum and preservation of left kidney.
a. Arrow shows renal vein thrombi
b. Arrow shows thrombi removal from left renal vein after venotomy
c. Arrows show left renal vein suture and maintenance of adequate renal perfusion
d. Specimen: left adrenal tumor and arrow shows venous thrombi
PATHOLOGY: Adrenal cortical carcinoma
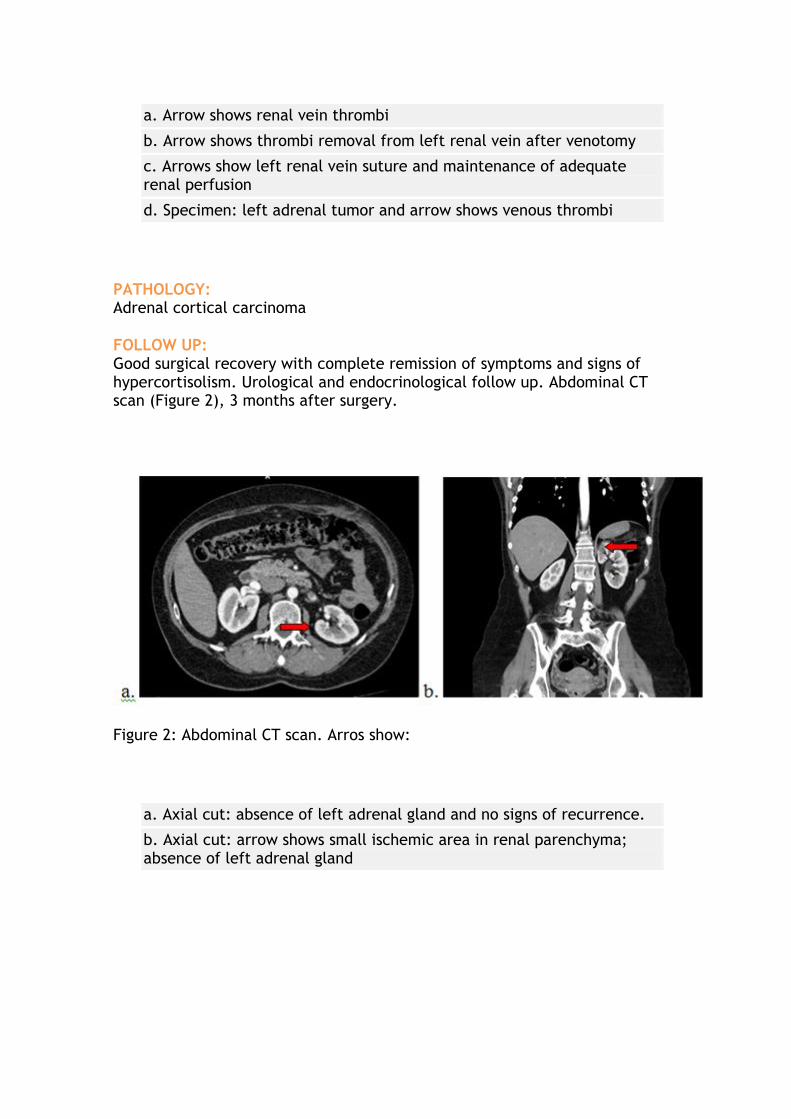
FOLLOW UP: Good surgical recovery with complete remission of symptoms and signs of hypercortisolism. Urological and endocrinological follow up. Abdominal CT scan (Figure 2), 3 months after surgery.
Figure 2: Abdominal CT scan. Arros show:
a. Axial cut: absence of left adrenal gland and no signs of recurrence.
b. Axial cut: arrow shows small ischemic area in renal parenchyma; absence of left adrenal gland
EDITORIAL COMMENT: Andre Moraes Oncologista do Centro de Oncologia de Campinas
Adrenal cortical carcinoma is a rare entity and presents with an agressive behaviour with high metastatic potential (50% of cases at the initial diagnosis) (1). Clinical factors related with poor prognosis include advanced age, high staging and augmented cortisol secretion (2). In the present case, history, physical exam and metabolic evaluation corroborate to the diagnosis of Cushing's Syndrome, with hypertension and hirsutism.
In cases where clinical diagnosis is not as obvious, a diagnostic imaging-oriented puncture biopsy would be reasonable since tumoral mass seems unlikely to be surgically removed, as long as pheochromocytoma was not suspected, as puncture might trigger a cathecolamine discharge with risk of fatal hypertension.
Around 70 to 85% of patients who undergo complete ressection develop local recurrence or metastatic lesions during follow up with a 5-year survival rate between 16 and 35% and less than 1-year survival rate for those with incomplete tumoral ressection (3).
In this clinical scenario with high recurrence rate and low survival rate the use of systemic therapy is critical.
Acute side effects of DDT (4,4'-(2,2,2-tricloroetane-1,1-diil)bis(clorobenzene)), a potent pesticide no longer commercially available, included adrenocortical necrosis in subjects with acute intoxication, which led to the development of Mitotane, op'DDD (1,1,Dicloro-2-p-clorofenil-2-o-clorofeniletano), initially applied to patients with advanced disease with clinical benefits varying from 20-50% of patients, reducing symptoms and improving progression free survival, used either as single therapy or in combination with other agents (4,5,6). In advanced cases, combination of Mitotane and EDP regimen (etoposide, doxorrubicine and cysplatine), in a recent publication (7), recommends its use due to evidence of longer progression free survival observed in the group treated with this combination.
Another important recent finding was the overexpression of IGF-2 (Insulin Growth Factor 2) influencing IGF-1R/mTOR pathway which is present in these tumors. Experimental treatment with cixutumumabe, a novel monoclonal antibody that acts against IGF-1R, in combination with tensirolimus, have shown efficacy in disease control close to 42% in preliminary results (8).

Whenever complete ressection is feasible, as in the present case, and when poor prognostic factors are found such as high volume disease, early age at diagnosis, hypercortisolism (2), adjuvant therapy with Mitotane is advised. A retrospective multicentric study showed that Mitotane at low daily dose (2 to 3 g/day) for 3 to 162 months resulted in a significant improvement in disease free survival and was well tolerated when compared with 2 historical studies (9).
Mitotane use in clinics must be monitored with adequate cortisol reposition and thyroid function assessment as this may be affected by the drug. Dose should be titrated aiming for adequate balance between therapeutic efficacy and side effects tolerance. Literature still lacks strong data to determine how long the drug should be used for. Caution should be taken to deliver clinical benefit.
References:
1. Nader N. Hanna, MD, and Daniel E. Kenady, MD. Curr Opin Oncol 12:49, 2000
2. Gwenaelle Abiven, Joel Coste, Lionel Groussin, Philippe Anract et col. J Clin Endocrinol Metab 91:2650, 2006
3. Irina Veytsman, Lynnette Nieman and Tito Fojo. J Clin Oncol 27:4619, 2009
4. Jame Abraham M.D.,Susan Bakke R.N.,Ann Rutt R.N.,Beverly Meadows R.N. Cancer 94:2333, 2002
5. Alfredo Berruti M.D., Massimo Terzolo M.D., Anna Pia M.D., Alberto Angeli Ph.D. and Luigi Dogliotti Ph.D. Cancer 83:2194, 1998
6. Alfredo Berruti, Massimo Terzolo, Paola Sperone, Anna Pia, Silvia Della Casa, et col. Endocr Relat Cancer 12:657, 2005
7. Martin Fassnacht, M.D., Massimo Terzolo, M.D., Bruno Allolio, M.D.,Eric Baudin, M.D.et col. N Engl J Med 366:2189, 2012
8. A Naing, P LoRusso, S Fu, D Hong, H X Chen, L A Doyle, A T Phan, M A Habra and R Kurzrock. Br J Cancer 108:826, 2013
9. Massimo Terzolo, M.D., Alberto Angeli, M.D., Martin Fassnacht, M.D., Fulvia Daffara, M.D.et col. N Engl J Med 356:2372, 2007

EDITORIAL COMMENT: Heraldo Mendes Garmes
Division of Endocrinology, FCM - UNICAMP
This case demonstrates the importance of early diagnostic in patients starting with hirsutism and menstrual irregularity during reproductive life.
The diagnosis of adrenal carcinoma is hardly established in the primary care of these patients, because it is a rare disease with an annual incidence of 0.5 to 2 cases per million and floating between clinical symptoms of Cushing's syndrome, hyperandrogenism and hypertension. As proposed by the European network studies in tumors of adrenal protocol, early assessment of excessive production of cortisol, androgens and mineralocorticoids, dosage of metanephrines to rule out pheochromocytoma, is essential for diagnosis, both clinical suspicion, as an incidental finding in adrenal tumor on imaging (1,2).
After diagnosis, the patient should perform follow a multidisciplinary specialist center for correct surgical treatment, tumor staging and follow-up according to current protocols (3,4).
References:
1- Allolio B, Fassnacht M. Clinical review: Adrenocortical carcinoma: clinical update. J Clin Endocrinol Metab. 2006 Jun;91(6):2027-37
2- Libè R, Fratticci A, Bertherat J. Adrenocortical cancer: pathophysiology and clinical management. Endocr Relat Cancer. 2007 Mar;14(1):13-28
3- Fassnacht M1, Kroiss M, Allolio B. Update in adrenocortical carcinoma. J Clin Endocrinol Metab. 2013 Dec;98(12):4551-64.
4-Terzolo M, Daffara F, Ardito A, Zaggia B, Basile V, Ferrari L, Berruti A. Management of adrenal cancer: a 2013 update. J Endocrinol Invest. 2014 Mar; 37(3): 207-17.

learning by image
ALTERNATIVE SURGICAL TREATMENT OF BENIGN PROSTATIC HYPERPLASIA: PROSTATE PLASMA VAPORIZATION
Juliano Moro, Daniel Moser da Silva, Carlos D’Ancona Division of Urology, UNICAMP
HISTORY
Weak stream for the past 3 years.
Patient refers LUTS (Lower Urinary Tract Symptoms) for the past 3 years. IPSS (International Prostatic Symptoms Score) is 28. Patient refers continuous worsening symptoms. He has no additional complaints.
PERSONAL BACKGROUND
Controlled hypertension (captopril).
No other comorbidities or previous surgical intervention.
PHYSICAL EXAM: Fibroelastic 40g prostate.
LABS: Total PSA: 0,6ng/mL Creat: 1,1mg/dL Urine I: normal. Culture: negative
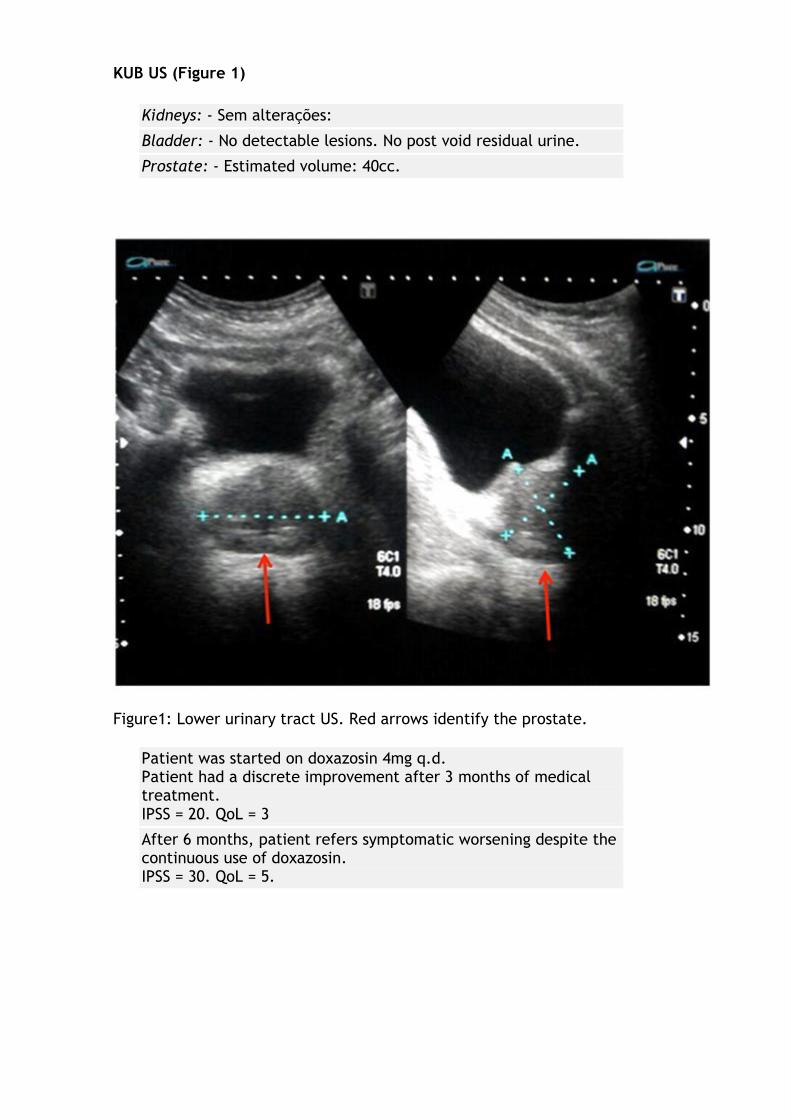
KUB US (Figure 1)
Kidneys: - Sem alterações:
Bladder: - No detectable lesions. No post void residual urine.
Prostate: - Estimated volume: 40cc.
Figure1: Lower urinary tract US. Red arrows identify the prostate.
Patient was started on doxazosin 4mg q.d. Patient had a discrete improvement after 3 months of medical treatment. IPSS = 20. QoL = 3
After 6 months, patient refers symptomatic worsening despite the continuous use of doxazosin. IPSS = 30. QoL = 5.
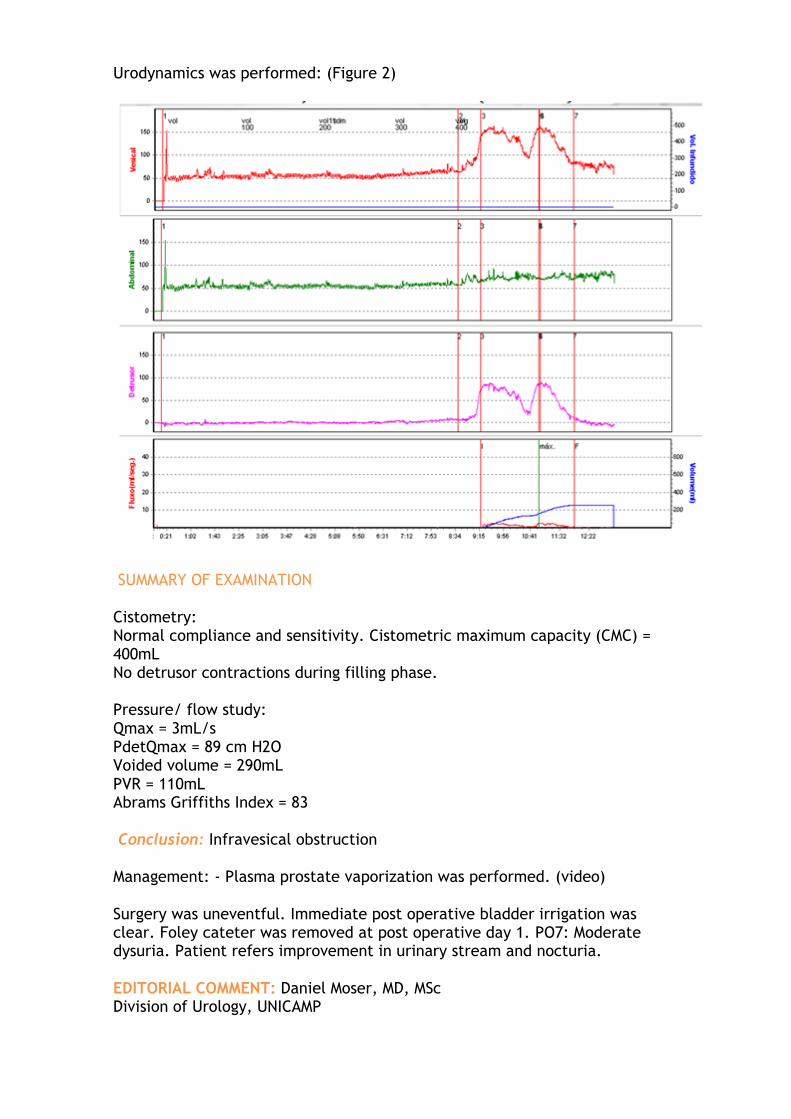
Urodynamics was performed: (Figure 2)
SUMMARY OF EXAMINATION
Cistometry: Normal compliance and sensitivity. Cistometric maximum capacity (CMC) = 400mL No detrusor contractions during filling phase.
Pressure/ flow study: Qmax = 3mL/s PdetQmax = 89 cm H2O Voided volume = 290mL PVR = 110mL Abrams Griffiths Index = 83
Conclusion: Infravesical obstruction
Management: - Plasma prostate vaporization was performed. (video)
Surgery was uneventful. Immediate post operative bladder irrigation was clear. Foley cateter was removed at post operative day 1. PO7: Moderate dysuria. Patient refers improvement in urinary stream and nocturia.
EDITORIAL COMMENT: Daniel Moser, MD, MSc Division of Urology, UNICAMP
Does the monopolar transurethral resection of the prostate (TURP) still remain the "gold standard" for treatment of increased prostate volume? For many authors, yes. However, some aspects of the technique are still in question by defensors of new technologies. The intraoperative and postoperative bleeding and intravascular fluid absorption during irrigation are the most questioned points of the traditional and established method. Bipolar plasma vaporization is an extra alternative to the defenders of the idea that improvements in the technology used in the TURP should be incorporated in urological armamentarium. By allowing vaporization with bipolar resection loop and use saline solution, many studies leave us with the sensation that the method can reach (or may have already achieved for many), the rank of "gold standard" of the conventional TURP. When the two methods are compared, several studies addressed to this topic show advantages, quite persuasive in favor of prostatic bipolar plasma vaporization. Geavelet et al, in a prospective and randomized study, with follow-up of 18months, compared the two methods.1 The rates of perforation and intra-operative bleeding, as well as the drop in hemoglobin rates are significantly lower in plasma vaporization. Other parameters such as postoperatively hematuria, blood transfusion and clots retaining are also significantly better in vaparization plasma. The operative time is shorter in vaporization, especially in cases that the bipolar resection loop is not used concomitantly. Rates of irritative symptoms and urethral stricture were similar.
We performed this technique in a group of patients study in our department, at Campinas University. The vaporization technique leaves us completely safe regarding bleeding. The learning curve for our residents involved few patients and it was easy to guide them in the technique (especially due to almost nonexistent intraoperative bleeding and low risk of absorption of the saline solution, allowing increased surgical time). The first two or three procedures took longer time, but after them we felt more confortable and begun to perform faster surgeries. There are no limits of prostate volume for vaporization. Huge prostate (more than 100g) can well be vaporized, if necessary using two surgical sections. If the concern is material for histological examination, the bipolar loop can be interleaved providing specimen for evaluation. The method is available since 2008 in North American market and for about five years in Brazil. There is no doubt that this technique is a potential candidate in the competitive market of endoscopic treatments for increasing prostate volume to replace the "gold standard" monopolar TURP.

References:
1. Geavlete B., Georgescu D., Multescu R., Stanescu F., Jecu M., Geavlete P. Bipolar Plasma Vaporization vs Monopolar and Bipolar TURP–A Prospective, Randomized, Long-term Comparison. Urology 78: 930–936, 2011.
new technologies
RANDOMIZED CONTROLLED TRIAL COMPARING RETROPERITONEAL LAPAROSCOPIC PYELOLITHOTOMY VERSUS PERCUTANEOUS NEPHROLITHOTOMY FOR THE TREATMENT OF LARGE RENAL PELVIC CALCULI: A PILOT STUDY
Li Sheng, Liu Tong-Zu, Wang Xing-Huan, Zeng Xian-Tao, Zeng Guang, Yang Zhong-Hua, Weng Hong, Meng Zhe, and Huang Jing-Yu. Journal of Endourology. August 2014, 28(8): 946-950. doi:10.1089/end.2014.0064 Journal of Endourology
ABSTRACT This study aimed to evaluate the eficacy and safety of laproscopic retroperitoneal pyelolitotomy (LRP) versus percutaneous nephrolithotomy (PNL) in the treatment of large pelvic calculi. According to 2013 european guideline, PNL is the recommended first treatment to treat renal calculi larger than 2cm. However, thsi procedure may not be the most suitable depending on the calculi complexity and renal anatomy of the patient. Design: Single institution randomized prospective study involving 178 patients divided into 2 groups of 89 subjects each to undergo either technique. Mean stone size: 2,9 + 1,0 vs. 3.0 + 0,9 cm in LRP and PNL , respectively. Follow up was 3 months long.
No difference in lenght of hospital stay, blood transfusion rate, conversion rate and post operative complications (fistulae, bleeding) was noted.
Significant differences between LRP and PNL were seen in stone free rates (98% vs. 90%, p = 0,03), operative time (90,87 + 33,4 vs. 116,8 + 44,4 minutos, p < 0,001), hemoglobin decrease (0,9 + 0,5 vs. 1,7 + 1,3 g/dL, p < 0,001) and post operative fever (3,4% vs. 13,5%, p = 0,02), respectively.
LRP has the advantage of avoiding traumatizing renal parenchyma as opposed to PNL. As such, there is a presumed lower risk of intra operative bleeding. Another aspect to be highlighted is that in cases of pyonephorsis, PNL group must postpone the procedure after placing a drain into the collecting system. While in laparoscopic group, treatment of infection, drainage of infected collection and retrieval of urinary stone can all be performed in the same procedure.
Results miust be interpreted with caution, however, as many confunding factors such as surgeon's proficiency, available disposable materials, patient's anatomy and calculi configuration may all impact stone free rates and complication rate. Conclusion: Both procedures show to be safe and effective for treating large pelvic renal calculi with minor advantages favouring LRP. These resuts must be validated by future studies.

On August 29, Danilo Souza Lima da Costa Cruz presented Master of Science with the following subject: Parameters of two-dimensional perineal ultrasonography for evaluation of urinary incontinence after Radical Prostatectomy
Mentor: Prof. Carlos D'Ancona
Members : Professors Fabricio Carrerette, Carlos D’Ancona (Orientador), Danilo Souza da Costa Cruz, Neson Caserta e José Tadeu Tamanini
SUMMARY:
Purpose: To compare sonographic patterns through perineal ultrasonography in men without prostate surgery, with continent and incontinent men after radical prostatectomy.
Methods: This cross-sectional clinical study investigated the differences of a dynamic evaluation of the urethra and pelvic floor contraction using perineal ultrasound in men without prostate surgery and in men submitted to radical prostatectomy with and without stress urinary incontinence. Ninety two male patients were included, which 70% of them underwent radical prostatectomy (RP) for more than one year. Thirty one men with clinically post prostatectomy incontinence were compared by two-dimensional (2D) perineal ultrasound to 34 patients without post prostatectomy incontinence and to 27 men without surgery in two centers in Brazil.
All patients had negative urine culture. The incontinent group also presented 24h pad test and urodynamic evaluation. The examination was performed with the patient in supine position, with legs slightly abducted, similar to lithotomy. The transducer was placed in the perineal area (between the scrotum and anus), with sagittal orientation, to obtain images of the pubic symphysis, bladder, bladder neck and urethra.
During examination, hypermobility of the proximal urethra, urethral angle, bladder neck funnelling and voluntary contraction of the pelvic floor were assessed. These parameters were evaluated during Valsalva maneuver, perineal contraction and rest.
Results: Our results showed that the continent group presented the urethral angle at rest significantly lower than the prostate group (p = 0.0002). We also observed that the incontinent group showed the displacement of the anterior bladder neck during contraction significantly lower than the continent group (p = 0.008). This condition was more evident when compared the severe incontinent group with the continent group. (p=0,022)
Conclusion: We observed a significant difference between the continent group and the group without prostate surgery when urethral angle was compared. We also observed a significant difference in anterior displacement of the bladder neck during contraction when comparing continent and incontinent groups.
On August 5, Dr. Ricardo Miyaoka presented PhD thesis with the following subject:

Relaxing effect of BAY 41-2272, a soluble guanylate cyclase stimulator, in isolated human ureter segments in A standardized in vitro model
Mentor: Prof. Carlos D'Ancona
Members : From the left to the right: Professors Forato Anhê, Carlos D¹Ancona (Mentor), Ricardo Miyaoka (applicant), Cassio Riccetto, Eduardo Mazzuchi e Fabio Vicentini.
SUMMARY:
Introduction: Medical expulsive therapy in the treatment of ureteral calculi aims to reduce the timeframe for spontaneous stone expulsion avoiding an unwanted surgical intervention. Current clinical therapy is essentially based upon the use of calcium channel blockers and alpha-adrenergic antagonists which have been recently shown to offer questionable efficacy according to well-designed recent clinical trials with a high level of evidence. As such, it is necessary to continue the pursuit for new agents that could abbreviate the time for ureteral stone expulsion.
Objectives: To report on a standardized ureteral contractility in vitro model with isolated human ureter segments in order to characterize the relaxation induced by soluble guanylate cyclase stimulator BAY 41-2272; to assess the involvement of NO-cGMP-PDE5 pathway and potassium channels in ureteral relaxation; to assess the immunohystochemical expression of endothelial (eNOS) and neuronal NO synthase (nNOS), soluble guanylate cyclase (sGC) and type 5 phosphodiesterase (IPDE5) in human ureter.
Materials and Methods: Distal ureteral segments harvested from 17 multiple organs deceased donors (age 24-65; mean 40 ± 3.2; men/women ratio 2:1) were used. Ureteral contractility was assessed with segments immersed into Kreb’s solution after being pre contracted with 80mM KCl. BAY 41-2272 induced ureteral relaxation in KCl pre contracted isolated segments with pEC50 and Emax of 5,82 ± 0,12 (n=8) and 84 ± 5%, respectively. Addition of a NOS inhibitor (L-NAME, 100 μM, n=6) or soluble guanylate cyclase (ODQ, 10 μM, n=6) led to a reduction of 21% and 44% in Emax values (P<0,05), respectively. pEC50 values remained unaltered. PDE5 inhibitor sildenafil (100 n M) enhanced (pEC50: 6,39 ± 0,10, n=8, P<0,05) the relaxing effect provoked by BAY 41-2272 compared with control curve.
Neither unspecific potassium channel blockers glibenclamide nor ATP-dependent potassium channel blocker tetraethylammonium (TEA) nor ureteral urothelium removal influenced the relaxation response by BAY 41-2272. Immunochemistry markers showed eNOS expression in ureteral vascular endothelium, nNOS in urothelium, nerve structures and with less intensity in smooth muscle. Soluble guanylate cyclase was present in urothelium and smooth muscle; and PDE5 was only expressed in ureteral smooth muscle.
Conclusions: BAY 41-2272 relaxes human isolated ureter segments in a concentration-dependent manner, mainly by activating the sGC enzyme in smooth muscle cells rather than in the urothelium, although a cyclic guanosine monophosphate-independent mechanism may exist. This pharmacological class may have a role in treating ureteral obstructive calculi..
JULY 15, MRS. MARCY PEREIRA LANCIA PRESENT THESIS IN THE DIVISION OF UROLOGY UNICAMP WITH THE FOLLOWING STUDY:
The effects of chronic inhibition of nitric oxide synthesis on bladder function in partial outlet obstructed mice.
Mentor: Prof. Carlos D'Ancona and Co Mentor: Prof. Edson Antunes
Members : Professors Cassio Riccetto, Rogerio Simonetti, Marcy Lancia Pereira (Candidate) Carlos D’Ancona (Mentor), Julio Alejandro Rojas Moscoso and Fernanda Bruschi Marinho Priviero
SUMMARY:
Benign prostatic hyperplasia (BPH) or Benign prostatic enlargement (BPE) leads to urinary tract dysfunction, which can be seen in experimental models, like rodents, by causing bladder outlet obstruction (BOO). Nitric oxide (NO), synthetized from L-arginine by three isoforms (iNOS, eNOS and nNOS) has been studied because it can be responsible for the urinary morphofunctional alterations.
This study aims to evaluate chronic bladder function in mice with BOO and treated chronically with L-NAME (non-selective NOS inhibitor) and aminoguanidine (iNOS selective inhibitor). Animals were divided into 6 experimental groups: Sham, Sham + L-NAME, Sham + aminoguanidine, BOO, BOO + L-NAME e BOO + aminoguanidine. BOO induction was made by laparotomy and partial ligature of bladder neck with a catheter as external guide. After 5 weeks of surgical procedure, animals were evaluated and filling cystometry, tissue bath contractile studies and bladder weight. BOO animals showed increase of non voiding contractions (NVC) and bladder capacity, and also less contractile response to Carbachol and Electric Field Stimulation.
Inhibition of NOS isoforms diminished bladder capacity in BOO animals. L-NAME caused more NVC, prevented bladder weight gain and leaded to augmented contractile responses at muscarinic and electric stimulation. Aminoguanidine diminished NVC, but did not avoid bladder weight gain in BOO animals and did not cause increase in contractile responses. These results suggest that constitutive NOS (eNOS and nNOS) seem to be more important in chronic BOO pathophysiology than iNOS.
Held on 14 and 15 October - 1st International Congress of ABAPP
The Urology congratulates Prof. Dr. Paulo Cesar Rodrigues Palma for organizing and conducting the event.
MAKE EARLY REGISTRATION AND HAVE 25% DISCOUNT!!
ICS 2014, Rio de Janeiro - 20th - 24th October 2014
__
Weekly meeting of Unicamp Urology Online!
The last weekly meeting of each month will be broadcast live from the 26th of February. This project aims to share knowledge and experiences with urologists from all over Brazil and the world. Do not miss this opportunity to discuss clinical cases, without leaving your home or office. Simply access the Urology Without Borders link and enter login (urologia) and password
(semfronteiras).

























![Endocr Disr PDF Website Review 3-6-2013[1]](https://img.pdfslide.us/doc/110x75/577cdbe81a28ab9e78a96781/endocr-disr-pdf-website-review-3-6-20131.jpg)

