Embed Size (px)
Citation preview

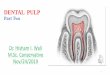
Disorders of the Dental Pulp
Dr. Rima SafadiFrom Dr. Huda Hammad lectures

Pulpitis
Inflammation of the pulpal tissue regardless of infective agent– Acute or chronic– Reversible or irreversible– With or without sypmtoms
We have to decide:– To restore the tooth– To remove the pulp– To remove the entire tooth
So: we have to decide if the process is reversible or irreversible

Causes of PulpitisBacterial: Caries Cracks Periodontal pockets Malformed teethTraumatic: Crown fractures Root fractures Partial avulsion Bruxism Abrasion
Iatrogenic: Heat generation Deep preperations Pulp exposure Filling materials Toxic disinfictants

Reversible pulpitis: Irritated pulp Mildest forms of inflammatory response
– Vasodilatation– Some transudation– Slight infiltrate of lymphocytes

Reversible pulpitis


Irreversible Wide spectrum of acute and chronic
inflammatory changes– Treatment removal of the pulp

Acute irreversible pulpitis

Pain Symptoms
Reversible: Elicited Sharp 10-15 minutes Unaffected by posture Easily localized
Irreversible: Spontaneous Dull >20 minutes Affected by body posture Difficult to localize

Pulp is contained within a solid champer Has limited blood supply through apical
foramen Inflammation mechanism gets destructive
– Inflammation: dilatation of blood vessels– Leakage of fluid from blood vessels– Migration of cells

Pulpal Necrosis: Untreated irreversible pulpitis (infected with bacteria):
– Lose acute and chronic symptoms– Degeneration of nerve fibers– Autolysis– Irritation to the periodontal membrane– Extensive pain (limited area), extrusion of tooth
Non infected pulpal necrosis:– No symptoms for months– Change in color of the tooth

Histopathology of Pulpal Disease
It is difficult to correlate clinical signs and symptoms with the degree of pulpal inflammation
Spectrum of histologic changes between normal and necrotic

Histopathology of Pulpal Disease
Overview:
Low caries level: mildest response:– Diffuse infiltration of lymphocytes and
macrophages– No exudate formation
Bacterial entrance: dilated and congested blood vessels– Exudate formation– Compression of blood vessels– Ischemia and necrosis---- pulp abscess

Acute Pulpitis May be confined to one horn of dental pulp (focal
acute pulpitis) or involve the whole pulp ( total acute pulpitis)
Cause: 1. Rapid bacterial invasion of dentinal tubules2. Overheating to the extent of ruptured blood
vessels Mainly in children and adolescents No possibility of drainage
– Build up of pressure


Acute Pulpitis
Pulp Abscess: Core: (exudate): PMN cells, fibrin, necrotic
cells, debris and RBC Zone of granulation tissue: newly formed
blood vessels, young fibroblasts plasma cells and lymphocytes
No outer surrounding capsule– Pus quickly spread reach PDL

Chronic Pulpitis When there is little or no penetration into the
pulp by large numbers of virulent types of bacteria.– Older teeth
• Scelrotic dentin• Reparative dentin formation

Chronic Pulpitis
Microscopically: Loose connective tissue, Dense Bundles of collagen Reduction in size and number of blood vessels and
nerves Diffuse infiltrate of lymphocytes and plasma cells
– Known as pulp fibrosis Focal and diffuse calcifications may occur
– Pulp stones: spherical calcifications– Dystrophic calcifications: linear calcifications


Pulp Calcification Pulp stones (denticles): organic core
– True pulp stones: contain tubules– False pulp stones: concentric layers of calcified
material– Free, adherent, interstitial
Dystrophic calcifications: granular material scattered along collagen fibers or in larger masses– Mainly in root canals

Chronic Hyperplastic Pulpitis
1. Opened occlusal cavity
2. Good blood supply through a widely opened apical foramen
3. Regenerative capacity of young pulpal tissue– Stimulation of pulp to proliferate– Excessive overgrowth– Fibrotic– Deficient in nerves– May be epithelialized


?????????????



![BDNF and NT3 Reprogram Human Ectomesenchymal Dental Pulp … · 2019-05-10 · dental pulp [1–7]. Dental pulp tissue has been under intense focus by the tissue-engineering field](https://img.pdfslide.us/doc/110x75/5f2d46f9106dfa58f83e3f64/bdnf-and-nt3-reprogram-human-ectomesenchymal-dental-pulp-2019-05-10-dental-pulp.jpg)