Embed Size (px)
Citation preview
647 Neonatal morbidity and mortality of operativevaginal delivery: a 10-year study of 82,000 infantsColin Walsh1, Michael Robson2, Fionnuala McAuliffe3
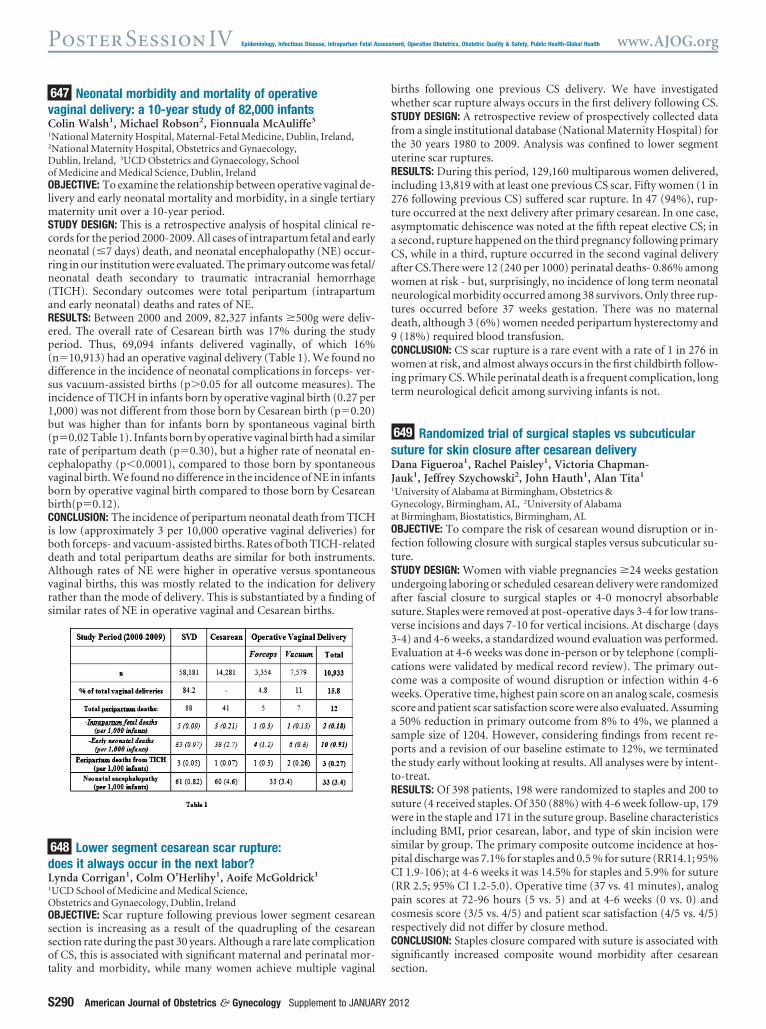
1National Maternity Hospital, Maternal-Fetal Medicine, Dublin, Ireland,2National Maternity Hospital, Obstetrics and Gynaecology,Dublin, Ireland, 3UCD Obstetrics and Gynaecology, Schoolof Medicine and Medical Science, Dublin, IrelandOBJECTIVE: To examine the relationship between operative vaginal de-livery and early neonatal mortality and morbidity, in a single tertiarymaternity unit over a 10-year period.STUDY DESIGN: This is a retrospective analysis of hospital clinical re-cords for the period 2000-2009. All cases of intrapartum fetal and earlyneonatal (�7 days) death, and neonatal encephalopathy (NE) occur-ring in our institution were evaluated. The primary outcome was fetal/neonatal death secondary to traumatic intracranial hemorrhage(TICH). Secondary outcomes were total peripartum (intrapartumand early neonatal) deaths and rates of NE.RESULTS: Between 2000 and 2009, 82,327 infants �500g were deliv-ered. The overall rate of Cesarean birth was 17% during the studyperiod. Thus, 69,094 infants delivered vaginally, of which 16%(n�10,913) had an operative vaginal delivery (Table 1). We found nodifference in the incidence of neonatal complications in forceps- ver-sus vacuum-assisted births (p�0.05 for all outcome measures). Theincidence of TICH in infants born by operative vaginal birth (0.27 per1,000) was not different from those born by Cesarean birth (p�0.20)but was higher than for infants born by spontaneous vaginal birth(p�0.02 Table 1). Infants born by operative vaginal birth had a similarrate of peripartum death (p�0.30), but a higher rate of neonatal en-cephalopathy (p�0.0001), compared to those born by spontaneousvaginal birth. We found no difference in the incidence of NE in infantsborn by operative vaginal birth compared to those born by Cesareanbirth(p�0.12).CONCLUSION: The incidence of peripartum neonatal death from TICHis low (approximately 3 per 10,000 operative vaginal deliveries) forboth forceps- and vacuum-assisted births. Rates of both TICH-relateddeath and total peripartum deaths are similar for both instruments.Although rates of NE were higher in operative versus spontaneousvaginal births, this was mostly related to the indication for deliveryrather than the mode of delivery. This is substantiated by a finding ofsimilar rates of NE in operative vaginal and Cesarean births.
648 Lower segment cesarean scar rupture:does it always occur in the next labor?Lynda Corrigan1, Colm O’Herlihy1, Aoife McGoldrick1
1UCD School of Medicine and Medical Science,Obstetrics and Gynaecology, Dublin, IrelandOBJECTIVE: Scar rupture following previous lower segment cesareansection is increasing as a result of the quadrupling of the cesareansection rate during the past 30 years. Although a rare late complicationof CS, this is associated with significant maternal and perinatal mor-tality and morbidity, while many women achieve multiple vaginal
births following one previous CS delivery. We have investigatedwhether scar rupture always occurs in the first delivery following CS.STUDY DESIGN: A retrospective review of prospectively collected datafrom a single institutional database (National Maternity Hospital) forthe 30 years 1980 to 2009. Analysis was confined to lower segmentuterine scar ruptures.RESULTS: During this period, 129,160 multiparous women delivered,including 13,819 with at least one previous CS scar. Fifty women (1 in276 following previous CS) suffered scar rupture. In 47 (94%), rup-ture occurred at the next delivery after primary cesarean. In one case,asymptomatic dehiscence was noted at the fifth repeat elective CS; ina second, rupture happened on the third pregnancy following primaryCS, while in a third, rupture occurred in the second vaginal deliveryafter CS.There were 12 (240 per 1000) perinatal deaths- 0.86% amongwomen at risk - but, surprisingly, no incidence of long term neonatalneurological morbidity occurred among 38 survivors. Only three rup-tures occurred before 37 weeks gestation. There was no maternaldeath, although 3 (6%) women needed peripartum hysterectomy and9 (18%) required blood transfusion.CONCLUSION: CS scar rupture is a rare event with a rate of 1 in 276 inwomen at risk, and almost always occurs in the first childbirth follow-ing primary CS. While perinatal death is a frequent complication, longterm neurological deficit among surviving infants is not.
649 Randomized trial of surgical staples vs subcuticularsuture for skin closure after cesarean deliveryDana Figueroa1, Rachel Paisley1, Victoria Chapman-Jauk1, Jeffrey Szychowski2, John Hauth1, Alan Tita1
1University of Alabama at Birmingham, Obstetrics &Gynecology, Birmingham, AL, 2University of Alabamaat Birmingham, Biostatistics, Birmingham, ALOBJECTIVE: To compare the risk of cesarean wound disruption or in-fection following closure with surgical staples versus subcuticular su-ture.STUDY DESIGN: Women with viable pregnancies �24 weeks gestationundergoing laboring or scheduled cesarean delivery were randomizedafter fascial closure to surgical staples or 4-0 monocryl absorbablesuture. Staples were removed at post-operative days 3-4 for low trans-verse incisions and days 7-10 for vertical incisions. At discharge (days3-4) and 4-6 weeks, a standardized wound evaluation was performed.Evaluation at 4-6 weeks was done in-person or by telephone (compli-cations were validated by medical record review). The primary out-come was a composite of wound disruption or infection within 4-6weeks. Operative time, highest pain score on an analog scale, cosmesisscore and patient scar satisfaction score were also evaluated. Assuminga 50% reduction in primary outcome from 8% to 4%, we planned asample size of 1204. However, considering findings from recent re-ports and a revision of our baseline estimate to 12%, we terminatedthe study early without looking at results. All analyses were by intent-to-treat.RESULTS: Of 398 patients, 198 were randomized to staples and 200 tosuture (4 received staples. Of 350 (88%) with 4-6 week follow-up, 179were in the staple and 171 in the suture group. Baseline characteristicsincluding BMI, prior cesarean, labor, and type of skin incision weresimilar by group. The primary composite outcome incidence at hos-pital discharge was 7.1% for staples and 0.5 % for suture (RR14.1; 95%CI 1.9-106); at 4-6 weeks it was 14.5% for staples and 5.9% for suture(RR 2.5; 95% CI 1.2-5.0). Operative time (37 vs. 41 minutes), analogpain scores at 72-96 hours (5 vs. 5) and at 4-6 weeks (0 vs. 0) andcosmesis score (3/5 vs. 4/5) and patient scar satisfaction (4/5 vs. 4/5)respectively did not differ by closure method.CONCLUSION: Staples closure compared with suture is associated withsignificantly increased composite wound morbidity after cesareansection.
PosterSessionIV Epidemiology, Infectious Disease, Intrapartum Fetal Assessment, Operative Obstetrics, Obstetric Quality & Safety, Public Health-Global Health www.AJOG.org
S290 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2012





























