Embed Size (px)
Citation preview

Dr. Rajesh GajbhiyeConsultant Gynecologist & directorMauli Women’s Hospital,Nagpur.

Hysterectomy can be performed in different ways
most of the indications are DUB,Fibroids,adenomyosis .
The best way to tackles is vaginal hysterectomy which is safer ,do not require gadgets and can be mastered by everybody.
We should not fall prey to the Gimmicks,gadgetsand glamour and subject our patients to such surgeries which may be associated with higher rates of complications ,which may be iatrogenic also

We should promote and propagate vaginal hysterectomy which is a indigenous surgery, natural surgery. In accordance with our PM Modi’s Misssion make in India.
we should upgrade our skills to do vaginal hysterectomy which is like a Aam Admi Surgery.

Intial in our residency only indication of vaginal hysterectomy was prolapse.The concept of Non Descent was not there. slowly second degree then NDVH
Then most of the contraindications and relative contraindications were challenged like Previous LSCS,Big fibroids nulliparity, even mild to mod endometriosis,even bening adenexal masses all have been conqured,and the scope goes on increasing till date.

Previously 80% of Hysterectomies were Abdominal A:V 80:20Now 70 % are Vaginal Hysterectomies V:A 70:30It differs from center to center

Now if cervix is accessible and mobility is there then vaginal hysterectomy should be thought of and now we say Trial of vaginal if not then you can always convert to other route.


In this era of evidence based medicine clear scientific evidence exists to determine the superiority for selection between all three methods available, that is vaginal hysterectomy (VH), total laparoscopic hysterectomy –laparoscopic or laparoscopic assisted vaginal hysterectomy (TLH or LAVH), and abdominal hysterectomy (AH).

2009 Cochrane Database Systemic Review
TLH- Increased operation time ,operation theater
occupancy and higher complication rate.
VH should be performed in preference to AH where possible.
If VH is not possible, TLH may avoid the need for AH.

The EVALUATE hysterectomy study, a multicenter randomized trial showed TLH was associated with a significantly higher risk of major complications and took longer time than AH.
Several studies show a clear benefit of the vaginal route over the abdominal, and only when VH is not possible is TLH preferred, though it is associated with higher bladder and ureterictrauma.

Donnez presented a series of 3190 laparoscopic hysterectomies for benign diseases from 1990 to 2006, wherein complications of TLH/LAVH were compared with those of AH and VH .
If VH can be performed safely then LAVH does not come in consideration.
LAVH/TLH replace AH

1. Lysis of adhesions
2. Treatment of pelvic endometriosis
3. Difficult oophorectomy
4. Fibroid that complicates VH
5. Evaluation of abdominal/pelvic cavity.

Recent advances and innovation in surgery has changed the views of Gynecologists.
One of the most dramatic change in the route of removal of the uterus during the last few years is switching over from abdominal to vaginal irrespective of its
Descent Volume (fibroids, Adenomyosis) Previous surgeries on it.

Natural Entrance
Direct approach to cervix and Uterus
Indications are increasing
More Gynec are adopting
Public Awareness is increasing
More demand for Stitch-less Surgery
NDVH

No need of costly equipments
Regional /local anaesthesia
Less Anaestheticcomplications
No Iatrogenic complications
Rapid recovery
Short hospital stay
Learning curve short

Nonavailability or nonaccessibility of laparoscope or laparoscopists in 80% of world population makes VH a popular choice.
In resource constraint country like India,wecannot rely on costly gazette based surgeries.
Vaginal route is the least invasive, most safe, and economical form amongst the available routes and techniques of hysterectomy.

Laparoscopic surgeons are striving to reduce the scar on abdomen from
multiport ------ minilaparoscopy
------single port
THEN WHY NOT VAGINAL WHICH IS TOTALLY SCARLESS

Anaesthesia related
Trocar related
Procedure related
Instrument related
Patient related

PREVIOUS LSCS
ENLARGED UTERUS
OPPHORECTOMY/BENIGN ADENEXALMASS

Cervicofundal sign by Dr Shirish Sheth to see for dimpling implying that there were dense adhesion with the anterior abdominal wall. Such case do LAVH.
Put speculum in post vaginal wall and see if the cervix is high up and behind pubic symphysis.

Scarred vesico-vaginal space can make the dissection more difficult ,whether the approach is Abdominal or Vaginal.
Vaginal approach is less difficult because one can enter in to the plane through 'surgical window' -least scarred area.
Scarred area


Try to Push finger laterally on the cervix.There is a loose covering tissue leads to broad ligament.
This is called Surgical Window.As a rule Bladder is non adherent
and free in its lateral one fifth.Use this window to enter over the
ant.surface of BL.
Once you enter the broad ligament,come medially by hooking the index finger .Thenwe will see VC ligament .cut thetissues by Sharp dissection withscissor under finger protectionand you will be in right space tos see VC peritoneal fold.

For a uterus upto 12 weeks' size or 250–300 cm3 volume, it is in the best interest of patients to perform VH.
For greater sizes or volumes, after ligatinguterines various debulking procedure like bisection,morcellation,coring.


Anterior-Posterior bulge is easier to tackle than Transverse Bulge
Appropriate insertion of Myoma Screw is of real help in enucleating the fibroid and for pulling force to drag out.
While Clamping remain nearer to Uterine border


If hysterectomy can be performed vaginally, neither route for the hysterectomy should be changed to other than vaginal nor ovaries be preserved, when they need to be removed, simply because hysterectomy is to be performed vaginally.
Difficult and it is mandatory to remove ovaries, one could add laparoscopic assistance.
benign mobile adnexa for salpingo-oophorectomy at vaginal hysterectomy.
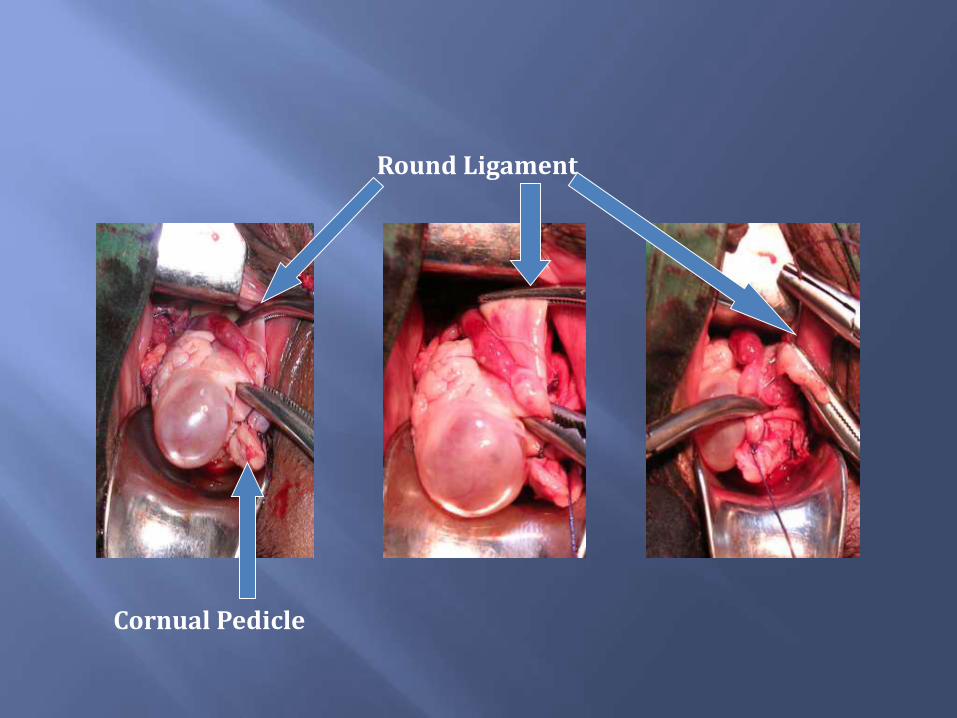
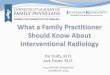
Round Ligament
Cornual Pedicle

After ligating the round ligament …clamps are applied overinfundibulo pelvic ligament..cut it to remove tube and ovary ….then ligate the pedicle
Infundibulo pelvic Ligament
Tube andOvary
Tube and Ovary removed




Removal of large simple ovarian cyst after removal of Uterus




While cutting the pedicle do not fashion or else the intervening area may bleed.
Always transfix the pedicle. Take a bite from the tip of the pedicle.
While tightening the knot put one thumb near the knot on one thread and pull the other thread till the knot is tight. Always take double throw.

Haemostasis is the most important step. After the hysterectomy is over checking of hemostatis by putting a surgical pad inside. I keep one of the thread of TO pedicle long as this pedicle goes out of vision so by pulling the thread you can visualise the pedicle.

Anchor the uterosacral to the vault of vagiina.thisgives vault support.

Our doubts are traitors and make us lose the good, we oft might win by fearing to attempt” by Shakespeare is so true and applicable for all those who do not perform VH in the absence of contraindication and have doubt about succeeding.

In choosing a hysterectomy technique in women with benign gynecological conditions without prolapse, there is no doubt that the vaginal route is safest, least invasive, economical, cosmetic, and natural route
This has the best scientific evidence in its favorand is the route of choice for most women. Unfortunately, however, the vaginal route (though backed by strong evidence) is used in less than 40% of cases instead of the desirable and possible 70–90%.


Thank you