Embed Size (px)
Citation preview
Urol. Radiol. 2, 58-60 (1980) Urologic Radiology
Clinical Pathologic Conference
63-Year-Old Man with a Right Flank Mass
Joan G o o d m a n and Yin Shih Department of Radiology, State University of New York, Downstate Medical Center, Brooklyn, New York, USA
Case Report
A 63-year-old male presented with symptoms of inter- mittent right flank pain of 2 years ' duration. Fourteen years prior to the present admission, a " r igh t renal cys t" had been diagnosed, Two years pr ior he had
Address reprint requests to." J. Goodman, M.D., Department of Radiology, State University of New York, Downstate Medical Center, 450 Clarkson Avenue, Brooklyn, NY 11203, USA
undergone a t ransurethral prostat ic resection, and at that time an intravenous u rogram revealed a right lower pole mass. Al though further evaluation was recommended, the pat ient refused.
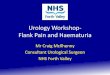
At the present admission there was no history of dysuria, frequency, hematur ia , or weight loss. Physical examinat ion revealed a palpable right f lank mass. No costovertebral angle tenderness was present. Routine labora tory studies were normal . Urography demonstra ted the right-sided mass (Fig. 1).
2
0171-1091/80/0002-0058 $01.00 © 1980 Springer-Verlag New York Inc.
J. Goodman and Y. Shih: Uroradiologic CPC 59
3
Fig. 1. A 15 minute film from an IVU demonstrates a right sided mass
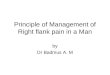
Fig. 2. Longitudenal scan 3.5 cm to the right of midline demonstrates a retroperitoneal mass, posterior to and separate from the right kidney, containing both cystic and solid components. This was confirmed on real time examination
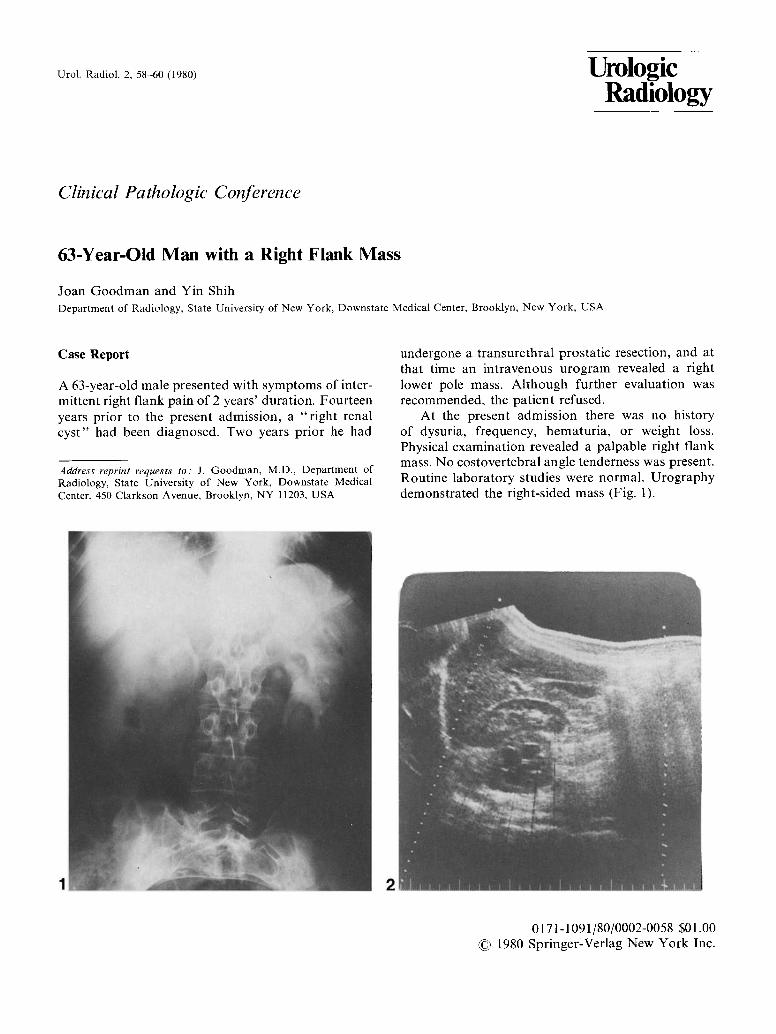
Fig. 3. Abdominal CT scan demonstrates the mass and shows it to be displacing the kidney anteriorly
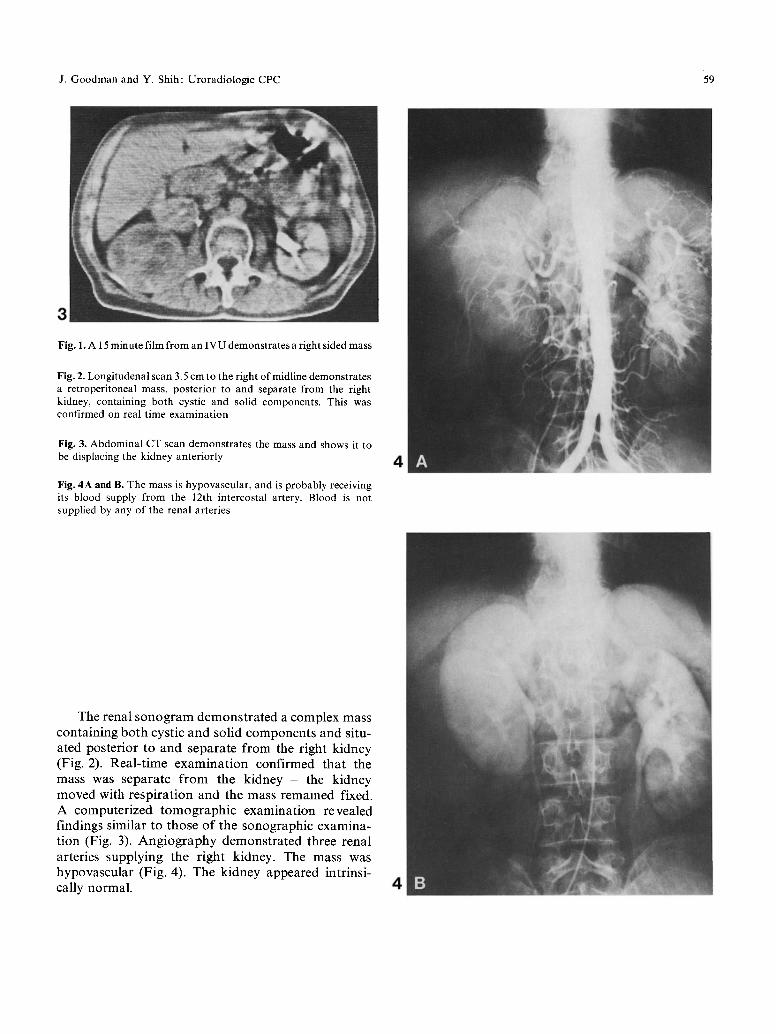
Fig. 4A and B. The mass is hypovascular, and is probably receiving its blood supply from the 12th intercostal artery. Blood is not supplied by any of the renal arteries
4
The renal s o n o g r a m d e m o n s t r a t e d a complex mass con t a in ing bo th cystic a n d solid c o m p o n e n t s and situ- ated poster ior to and separa te f rom the r ight k idney (Fig. 2). Rea l - t ime e x a m i n a t i o n conf i rmed that the mass was separa te f rom the k idney - the k idney moved with r e sp i ra t ion and the mass remained fixed. A computer ized t o m o g r a p h i c examina t i on revealed f indings s imilar to those of the sonographic examina- t ion (Fig. 3). A n g i o g r a p h y demons t r a t ed three renal arteries supp ly ing the r ight kidney. The mass was hypovascu la r (Fig. 4). The k idney appeared in t r ins i - cally normal . 4

60 J. G o o d m a n and Y. Shih: Uroradiologie CPC
Diagnosis: Benign Schwannoma
Surgical explorat ion of the re t roper i toneum was per- formed. A solid mass just below the left dorsal fascia was identified. The mass was easily enucleated f rom the surrounding tissue. A large intercostal vessel was seen draped over the mass. The kidney was unin- volved and was anter ior to the mass within an intact Gero ta ' s fascia. The histologic diagnosis was a benign schwannoma [1-5].
Discussion
The schwannoma is a pr imary nerve sheath tumor, arising f rom a schwann cell of neural crest origin. It is mos t common l y found as an acoustic neuroma but can also involve a peripheral nerve in the neck, medias t inum, and extremities, and is often associated with neurof ibromatos is [6, 7]. It is rarely found in the re t roper i toneum with a perinephric location mos t unusual [2]. Of the 162 cases of retroperi toneal tumors reviewed by Melicow [8], 18 cases of neural tumors were found; of these, 3 were schwannomas. Stout [9] reviewed 137 cases of mal ignant schwannomas and found 6 to be in the retroperi toneal space.
Schwannomas may be benign or malignant. Most re troperi toneal schwannomas are mal ignant and re- currence is c o m m o n following local excision, prob- ably due to intraneural spread of t umor [7]. Schwan- nomas are usually slow-growing tumors, rarely reach- ing 2 cm in size ; however, retroperi toneal schwanno- mas may grow to be large. The tumor is solid in nature; cystic degenerat ion occurs as the tumor en- larges [4, 8].
mass to the adjacent kidney may be evaluated by real-time ultrasound.
Pathologic Findings
On gross examinat ion, the tumor mass is generally well encapsulated, extending along the course of the nerve. Lesions f rom the extremities, lumbar regions, and medias t inum frequently involve nerve trunks. Re- troperitoneal s chwannomas are usually large, and it is difficult to evaluate nerve involvement. The tumors are white-gray in color with areas of hemor rhage and cystic degenerat ion. They are frequently avascu- lar, even though there m a y be hemorrhagic areas [1]. Microscopically, spindle cells are seen arranged in tight, wavy, interlocking bundles. Nuclei are plump, ovoid with one mitosis per high-power field. More bizzare tumors have p lumper nuclei and more mi- toses. Regions of osteoid or chondroid metaplasia may be seen.
Therapy
The t reatment of choice for mal ignant schwannoma is radical excision of the t u m o r [2, 10]. Neura l tumors are generally not sensitive to radiation therapy, but if inadequate no rma l tissue margin is resected, radio- therapy is p robab ly indicated.
References
Clinical Findings
Patients classically present with back pain, fever, mal- aise, and weight loss [2, 10], a l though it is not unusual for them to be asymptomat ic . Physical examinat ion usually reveals an abdomina l or flank mass.
Imaging
Radiologically, retroperi toneal tumors may be seen as a soft tissue mass on the plain film or be demon- strated on IVU. Retroper i toneal schwannomas are usually large and are likely to affect the kidney by mass effect. Recent advances in ul t rasound and CT scanning make them the obvious choice in examining the re t roper i toneum. The relationship of the tumor
1. Johenning PW, D 'Ange lo J: Neur i l emoma and the urologist. J Urol 109.'377, 1973
2. Bair ED, Woods ide JR, Wil l iams WL, Bordon TA: Perirenal mal ignant s chwannoma present ing as renal cell carcinoma. Urology 11:510, 1978
3. Carpenter WB, K e r n o h a m JW: Retroperi toneal gangl ioneuro- mas and neurof ibromas . A clinicopathological study. Cancer •6.'788, 1963
4. Deming CL, N e w m a n H R : Schwannomas . J Urol 72.'316, 1954 5. Melassonos JC, Smith EB: Pr imary retroperitoneal t um o r -
mal ignant neur i l emoma. Arch Surg 80.705, 1960 6. Ghosh BC, Ghosh A, H u v o s J, For tner : Mal ignant schwanno-
ma : a cl inicopathological study. Cancer 31:184, 197 3 7. White H: Survival in ma l ignan t schwannoma. Cancer 27:720,
1971 8. Melicow M N : Pr imary tumors o f the re t roperi toneum : a clini-
copathological analysis of 162 cases. Review of literature and table of classification. J Int Coil Surgeons 19:401, 1953
9. Stout AP: The mal ignan t t umor of the peripheral nerves. Am J Cancer 25:1, 1935
10. Richards JL, Matolo N M : Mal ignan t s chwannoma: report of a case mimicking l umba r disc disease. Am Surg 45.'49, 1979