Embed Size (px)
Citation preview
Ischemic Stroke and TIA: Mimics and Management
Ethan Cumbler MD, FACP Associate Professor of Medicine University of Colorado Hospital
UCH Stroke Council 2011
Disclosures and Relationships
No Conflicts
American Stroke Association Quality Speakers Bureau Western/Pacific Region
National Stroke Association Course Director
Improving In-hospital Stroke Through QI Interventions
Colorado Stroke Alliance Research Collaboration
Objectives
1. Recognize common conditions which can mimic acute stroke
2. Understand consequences of treating a stroke mimic with tPA
3. Identify appropriate means to manage co-morbid illness in the stroke patient -Hyperglycemia
-Hyperlipidemia -Hypertension
Thaumoctopus mimicus
Case ! A 55 year old female with HTN and DM II arrives at the Emergency room
20 minutes after onset of trouble speaking and loss of sight in the left visual field
! Symptoms started with a bright light in the left peripheral vision – Progression to vision loss on left side – 5 minutes later she began having slurred speech and difficulty finding words – Now starting to develop a left sided headache and nausea – Similar but less severe symptoms 4 times over last 20 years
! No other significant medical history or medications
! Exam confirms left visual field cut and dysarthria. – No motor or sensory deficits
! NIH Stroke Scale Score of 2
! Should the ED call a Stroke Alert?
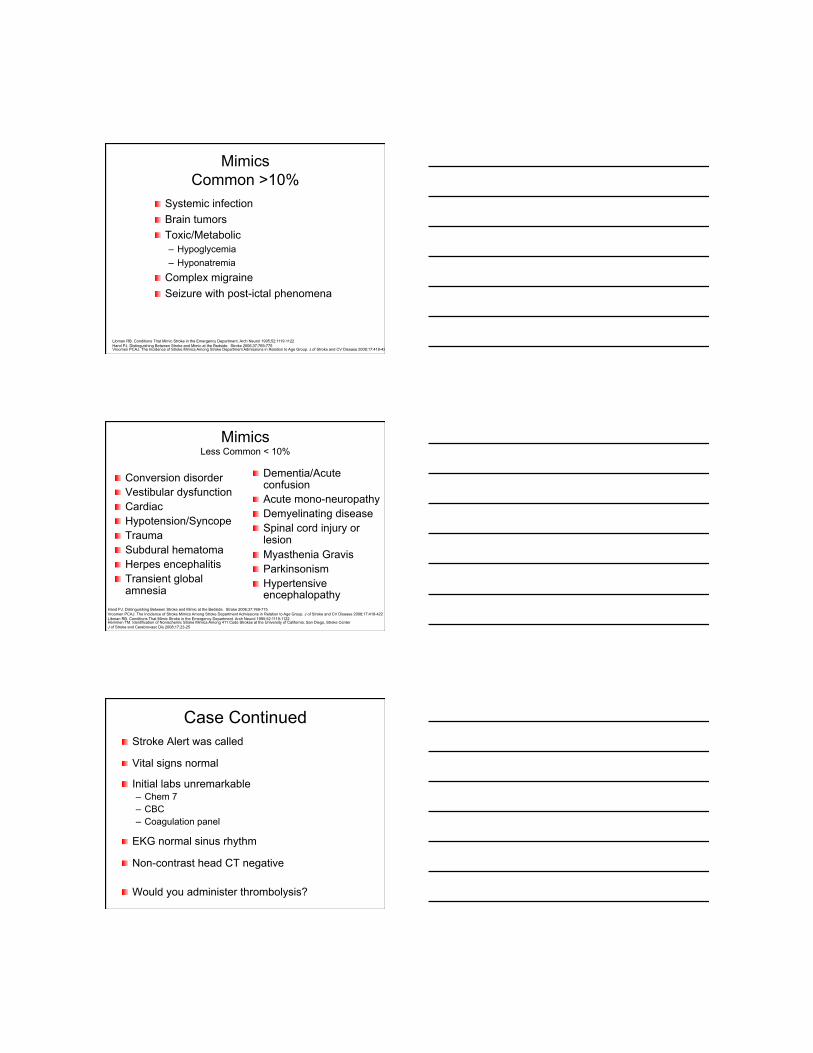
Neurologic Chief Complaint in 911 call
90% will not be strokes
ED Stroke Alerts For Suspected Stroke
20% will not be strokes
ED Physician Final Diagnosis of Stroke
9% will not be strokes
Libman RB. Conditions That Mimic Stroke in the Emergency Department. Arch Neurol 1995;52:1119-1122 Hand PJ. Distinguishing Between Stroke and Mimic at the Bedside. Stroke 2006;37:769-775 Ferro JM. Diagnosis of Stroke by the Non-neurologist. Stroke 1998:29:1106-9
Patient Treated With Thrombolysis ???
Mimics Common >10%
! Systemic infection ! Brain tumors ! Toxic/Metabolic
– Hypoglycemia – Hyponatremia
! Complex migraine ! Seizure with post-ictal phenomena
Libman RB. Conditions That Mimic Stroke in the Emergency Department. Arch Neurol 1995;52:1119-1122 Hand PJ. Distinguishing Between Stroke and Mimic at the Bedside. Stroke 2006;37:769-775 Vroomen PCAJ. The Incidence of Stroke Mimics Among Stroke Department Admissions in Relation to Age Group. J of Stroke and CV Disease 2008;17:418-422
Mimics Less Common < 10%
! Conversion disorder ! Vestibular dysfunction ! Cardiac ! Hypotension/Syncope ! Trauma ! Subdural hematoma ! Herpes encephalitis ! Transient global
amnesia
! Dementia/Acute confusion
! Acute mono-neuropathy ! Demyelinating disease ! Spinal cord injury or
lesion ! Myasthenia Gravis ! Parkinsonism ! Hypertensive
encephalopathy Hand PJ. Distinguishing Between Stroke and Mimic at the Bedside. Stroke 2006;37:769-775 Vroomen PCAJ. The Incidence of Stroke Mimics Among Stroke Department Admissions in Relation to Age Group. J of Stroke and CV Disease 2008;17:418-422 Libman RB. Conditions That Mimic Stroke in the Emergency Department. Arch Neurol 1995;52:1119-1122 Hemmen TM. Identification of Nonischemic Stroke Mimics Among 411 Code Strokes at the University of California, San Diego, Stroke Center J of Stroke and Cerebrovasc Dis 2008;17:23-25
Case Continued ! Stroke Alert was called
! Vital signs normal
! Initial labs unremarkable – Chem 7 – CBC – Coagulation panel
! EKG normal sinus rhythm
! Non-contrast head CT negative
! Would you administer thrombolysis?
Stroke Mimics Treated With Thrombolysis?
! 3-14% of pts treated with tPA are actually stroke mimics
! Three diagnoses: 1. Complex Migraine 2. Seizure 3. Conversion disorder
! Global aphasia most common symptom of mimics
Winkler DT. Thrombolysis in Stroke Mimics: Frequency, Clinical Characteristics, and Outcome. Stroke 2009:40:1522-25 Chernyshev OY. Safety of tPA in stroke mimics and neuroimaging-negative cerebral ischemia. Neurology 2010; 74: 1340 - 1345. Scott PA. Misdiagnosis of Stroke in Tissue Plasminogen Activator-Treated Patients. Characteristics and Outcomes. Ann Emerg Med 2003;42:611-618
Get to Know a Mimic #1 Complex Migraine
! Transient neurologic phenomena “aura” – Occur in a quarter of migraineurs
! Visual changes “fortifications” ! Scintillations, Scotoma, loss of vision ! Numbness ! Weakness (Hemiplegic migraine) ! Aphasia or mutism
Jean Marie Charcot, Illustration of scintillating scotoma, 1888.
The Migraine Aura Foundation http://www.migraine-aura.org Alice in Wonderland
I was playing in the garden when a brilliant, shimmering light appeared to my left — dazzlingly bright, almost as bright as the sun. It expanded, becoming an enormous shimmering semicircle stretching from the ground to the sky, with sharp zigzagging borders and brilliant blue and
orange colors. Then, behind the brightness, came a blindness, an emptiness in my field of vision, and soon I
could see almost nothing on my left side.
Oliver Sacks M.D.
Distinguishing Migraine from CVA ! History of Migraine
! Migraine neurologic deficits have a slow migratory or spreading pattern – CVA symptoms tend to be abrupt
! Neurologic aura deficits occur sequentially
! Biphasic pattern – Positive symptoms first followed by negative symptoms
! Symptoms tend to resolve over 20-60 min
Hemiplegic Migraine Unfortunately Does not Follow These Rules Foroozan R. Transient Neurologic Dysfunction in Migraine. Neurology Clinics 2009. 27:
Get to Know a Mimic #2 Seizure with Post-ictal Paresis
! Described by Todd in 1849
! Transient post-seizure neurologic deficits reported in 6-40% of seizure patients
! Median duration of post-ictal paresis only 3 minutes and vast majority have resolved within an hour
! Prior theory of “Neuronal Exhaustion”
! Modern theory of “Active Inhibition” Gallmetzer P. Postictal Paresis in Focal Epilepsies. Neurology 2004;62:2160-2164
Distinguishing Post-ictal Paresis from Stroke
! Pre-existing epilepsy should raise suspicion of post-ictal paresis
! Distinction made difficult by shared risk factors – Prior stroke can be a seizure focus – Most common cause of epilepsy in the elderly is stroke
! Early seizure can also complicate acute stroke – 2-5% of stroke pts have a seizure at onset of ischemia
! Seizure prior to onset of symptoms suggests post-ictal paresis – Used as an exclusion criteria in original thrombolytic NINDS trial
Feleppa M. Early Poststroke Seizures. Clinical and Experimental HTN 2006;28:265-270

Get to Know a Mimic #3 Conversion Disorder
! Psychiatric condition manifesting with transient motor or sensory deficits
! Hemiplegia ! Paralysis ! Blindness ! Diplopia ! Aphonia ! Others
! Manifestation of major emotional stress – Not the same as factitious disorder or malingering
! Can look VERY convincingly like stroke Phoebe SC. A Case of Conversion Disorder Presenting as a Severe Acute Stroke. J Emerg Med 2006;30:283-286 Chou JY. Conversion Disorder In Stroke: A Case Report. Kaohsiung J Med Sci 2006;22:586-589
Distinguishing Conversion Disorder from Stroke
! Give-way weakness – May be unreliable as this is “seen” in 30% of organic neurologic disease
! ‘La belle indifference’ – Unreliable in differentiating conversion from organic disease
! “Hoover sign” – involuntary extension of a pseudo-paralyzed leg when the ‘good leg’ is
flexing against resistance
! Neurologic deficits which do not match vascular distribution – Can mislead with multiple infarcts or entities such as dural venous sinus
thrombosis
! Inconsistency in exam
! “Teddy Bear Sign”?? The Neuropsychiatry of Conversion Disorder: The Neurological Diagnosis. Medscape Today. http://www.medscape.com/viewarticle/572542_3
What Happens if Mimic is Treated with Thrombolysis?
! Stroke patients receiving tPA had some complication in 19% of cases – 5% symptomatic ICH – 12% asymptomatic ICH – 1% angioedema
! None of the stroke mimics had symptomatic ICH – Overall prognosis much better for stroke mimics
Winkler DT. Thrombolysis in Stroke Mimics: Frequency, Clinical Characteristics, and Outcome. Stroke 2009:40:1522-25 Chernyshev OY. Safety of tPA in stroke mimics and neuroimaging-negative cerebral ischemia. Neurology 2010; 74: 1340 - 1345. Scott PA. Misdiagnosis of Stroke in Tissue Plasminogen Activator-Treated Patients. Characteristics and Outcomes. Ann Emerg Med 2003;42:611-618
CASE CONTINUES ! 10 years later your patient, now 65 years old re-
presents with – Sudden onset right sided weakness – Numbness of the right arm, leg, and face – Difficulty forming sentences
! Unfortunately she waits 5 hours before coming in to the hospital – BP 195/110 – Blood glucose 240 – LDL 102
! How do we manage her co-morbidities?
CO-MORBIDITIES
! Hyperglycemia
! Hypertension
! Hyperlipidemia
Sugar
Loco Moco Burger
Salt
Hyperglycemia ! Common on presentation with stroke
– Seen in 1/3 of admissions
! Associated with bad outcome – Larger infarctions – More disability – Increased mortality
! Is this causation or correlation – Stress response cortisol/catecholamines high blood sugar – Pre-existing Diabetes (recognized or unrecognized) – Hyperglycemia harms ischemic brain tissue
Hyperglycemia in Acute Ischemic Stroke: Pathophysiology and Clinical Management. Nature Reviews Neurology 2010;6:145-155
Potential Mechanisms Of Harm From Hyperglycemia
! May reduce recanalization – Increased thrombin and tissue factor – Decreased activity of tPA
! May decrease reperfusion – Impaired vasodilation via impact on nitric oxide
! May increase re-perfusion injury – High glucose can increase oxidative stress
Harm of Intensive Insulin Regimens
! Hypoglycemia – Reported in average of 31% of patients in 7
trials of IV insulin in stroke patients
! Effect of hypoglycemia may be more significant in stroke patient than in the general medicine patient
Hyperglycemia in Acute Ischemic Stroke: Pathophysiology and Clinical Management. Nature Reviews Neurology 2010;6:145-155
Glycemic Control Recommendations
! Recommendation is to control to <200 – Goal of 80-140
! How to achieve this goal and whether intensive insulin drip therapy will end up proving beneficial is not clear
! Large trials in stroke patients using clinical outcomes are needed
The Pendulum Swings
Intensive Insulin Therapy
Moderate Insulin Therapy
The NICE-SUGAR Study Investigators. N Engl J Med 2009;360:1283-1297
Management of Co-morbidities Glycemic Control
PEARLS ! Rarely a need for dextrose in IVF in the first 24 hrs
! Metformin problematic-contrast/lactic acidosis
! Sulfonylurea medications associated with hypoglycemia when oral intake interrupted
! Sliding scale insulin alone is a poor choice for more than 24 hours
Evidence-Based Suggestions For the Hyperglycemic
Stroke Patient
! For the critically ill stroke patient – IV insulin drip titrated to BG 140-180
! For the stroke patient on the general medical ward – Anticipatory short acting SQ insulin prior to meals – Correction factor based on blood glucose – Long acting SQ insulin as basal control – Adjust daily if not at goal BG
! Long term glycemic control to A1c <7 American Association of Clinical Endocrinologists and American Diabetes Association Consensus Statement on Inpatient Glycemic Control. Diabetes Care. 2009;32:1119-1131
Hyperlipidemia ! Population studies find a weak association between
cholesterol and risk of stroke
! Lesser evidence that some lipid lowering agents reduce risk of stroke alone or added to other agents – Fibrates – Niacin – Ezetimide
! Statins do reduce stroke – And reduce stroke severity when already treated
Statins and Clinical Outcome of Acute Ischemic Stroke: A Systematic Review. Int Arch Med 2010;3:22 Statintherapy in the Primary and Secondary Prevention of Ischaemic Cerebrovascular Diseases. Int J of Cardiology. 2010-in press Interventions in the Management of Serum lipids for Preventing Stroke Recurrence. Cochrane Database Sys Rev 2009;(3):CD002091
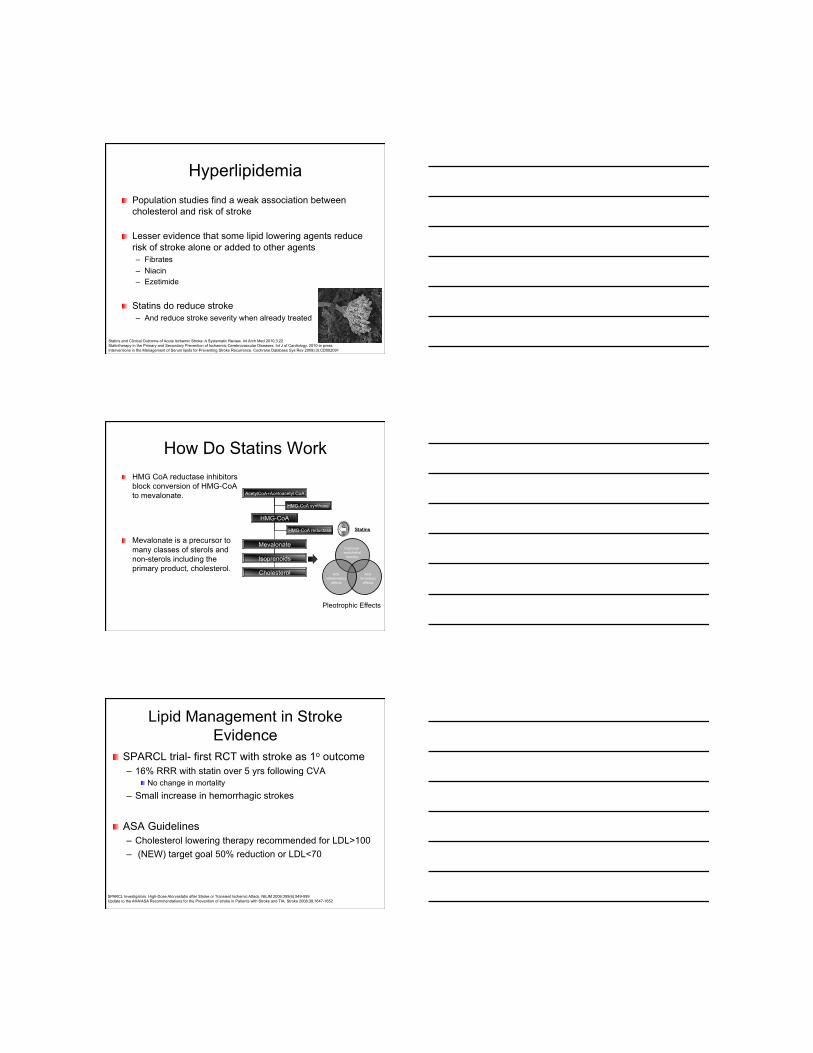
How Do Statins Work ! HMG CoA reductase inhibitors
block conversion of HMG-CoA to mevalonate.
! Mevalonate is a precursor to many classes of sterols and non-sterols including the primary product, cholesterol.
AcetylCoA+Acetoacetyl CoA
HMG-CoA
HMG-CoA synthase
Mevalonate
Isoprenoids
Cholesterol
HMG-CoA reductase Statins
Improved endothelial
function
Anti-thromboic
effects
Anti-inflammatory
effects
Pleotrophic Effects
Lipid Management in Stroke Evidence
! SPARCL trial- first RCT with stroke as 1o outcome – 16% RRR with statin over 5 yrs following CVA
! No change in mortality
– Small increase in hemorrhagic strokes
! ASA Guidelines – Cholesterol lowering therapy recommended for LDL>100 – (NEW) target goal 50% reduction or LDL<70
SPARCL Investigators. High-Dose Atorvastatin after Stroke or Transient Ischemic Attack. NEJM 2006;355(6):549-559 Update to the AHA/ASA Recommendations for the Prevention of stroke in Patients with Stroke and TIA. Stroke 2008;39:1647-1652
Evidence-Based Suggestions ! Avoid interrupting prior statin use during
hospitalization for stroke
! High-dose high-potency statin therapy for stroke patients with LDL>100 – Statin rec to 50% reduction of LDL or <70
! Especially in very high risk patients – Unclear if statin of benefit if LDL already <70
– For low HDL consider niacin or gemfibrozil
! Start prior to hospital discharge
! Unclear if recommendations apply to hemorrhagic strokes Guidelines for the Prevention of Stroke in Patients with Stroke or Transient Ischemic Attack. Stroke 2011;42-in press
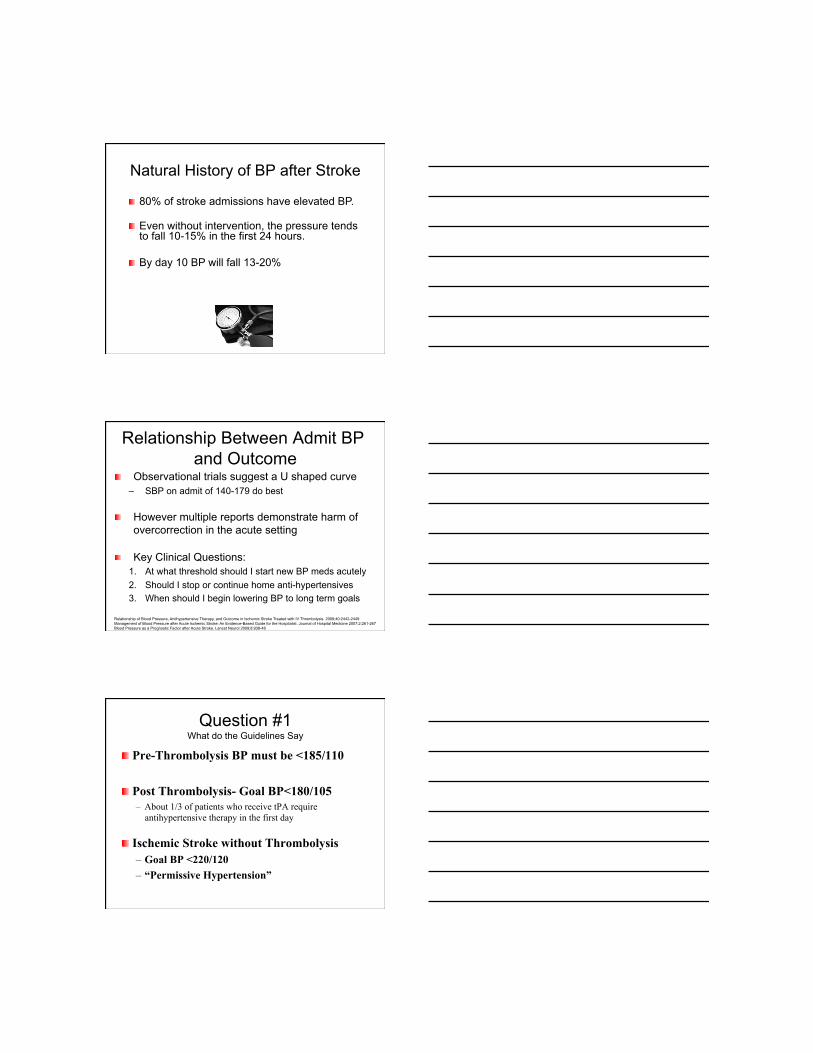
Management of Co-morbidities Hypertension Ischemic Penumbra
! Zone of at risk tissue susceptible to reduction below the threshold of viability in response to relatively small drops in MAP.
Objective of Blood Pressure Control
Maximize perfusion to the ischemic
penumbra
Minimize risk of hemorrhagic transformation
Natural History of BP after Stroke
! 80% of stroke admissions have elevated BP.
! Even without intervention, the pressure tends to fall 10-15% in the first 24 hours.
! By day 10 BP will fall 13-20%
Relationship Between Admit BP and Outcome
! Observational trials suggest a U shaped curve – SBP on admit of 140-179 do best
! However multiple reports demonstrate harm of overcorrection in the acute setting
! Key Clinical Questions: 1. At what threshold should I start new BP meds acutely 2. Should I stop or continue home anti-hypertensives 3. When should I begin lowering BP to long term goals
Relationship of Blood Pressure, Antihypertensive Therapy, and Outcome in Ischemic Stroke Treated with IV Thrombolysis. 2009;40:2442-2449 Management of Blood Pressure after Acute Ischemic Stroke: An Evidence-Based Guide for the Hospitalist. Journal of Hospital Medicine 2007;2:261-267 Blood Pressure as a Prognostic Factor after Acute Stroke. Lancet Neurol 2009;8:938-48
Question #1 What do the Guidelines Say
! Pre-Thrombolysis BP must be <185/110
! Post Thrombolysis- Goal BP<180/105 – About 1/3 of patients who receive tPA require
antihypertensive therapy in the first day
! Ischemic Stroke without Thrombolysis – Goal BP <220/120 – “Permissive Hypertension”
150 125 100 75
50
25 Cerebral Perfusion Pressure (mm Hg))
Cer
ebra
l Blo
od F
low
(ml/1
00 g
/min
)
175
25
50
75
NORMAL
ISCHEMIA
Chronic HTN
• In the setting of acute stroke auto-regulation is lost, • Cerebral blood flow becomes linear relationship with MAP
Question #2 Continue or Stop Home Meds? ! COSSACS Trial
– Randomized 763 patients to continue or hold home antihypertensives for 2 weeks
– No change in disability or death – No benefit or harm demonstrated
Effects of Antihypertensive treatment after acute stroke in the Continue or Stop Post-Stroke Antihypertensives Collaborative Study. Lancet Neurol 2010:9:767-75
Question #3 When Should I Start New Meds?
! CHIPPS trial – Lisinopril or Labetolol vs placebo – BP on entry averaged SBP 181 mm Hg – SBP fell 21 points with tx vs 11 in placebo group
! No difference in outcome at 2 wks ! Longer term the group with lowered bp did better
– 60% reduction in mortality at 3 months
! Caveat- Underpowered study of only 179 pts Controlling Hypertension and Hypotension Immediately Post-Stroke. Lancet Neurol 2009;8:48-56
Evidence-Based Suggestions ! Reasonable to continue home antihypertensives
– Thiazides may be held acutely given risk of hyponatremia after CVA
! Avoid overcorrection of BP in hyperacute period – Permissive HTN still permitted in first 24 hours
! Modest bp reduction (10-15%) likely safe but no clear evidence it is of acute benefit – Timing of initiation may vary based on size of penumbra
! Long term benefit of lowering bp is well established – Diuretic or Diuretic+ACE-I have best evidence – Goal NORMAL blood pressure
Chronic Blood Pressure Control
! UK TIA study demonstrated a 28% decrease in long term stroke risk for every 10mm drop in systolic BP.
! By comparison- How much risk reduction do you get with aspirin?
! 15%
The Treatment Imperative Does Not End At Hospital Discharge
Hackam DG et al. Stroke. 2007;38:1881-1885.
! Outpatient use of secondary prevention measures suboptimal – 43% not regularly exercising – 36% not getting dietary counseling – 23% not regularly using anti-platelet agent – 19% not having cholesterol monitoring – 9% not on antihypertensive
Use of Stroke Secondary Prevention Services. Stroke. 2009;40:1811-1819
With Aggressive Treatment Impact can be Huge
! Mathematical Model of Risk Reduction – 5 year intensive control of 5 risk factors
! Diet, and exercise ! High potency anti-platelet agent ! High-dose statin ! Aggressive BP control
! Relative Risk Reduction: 90% – NNT = 5
Hackam DG et al. Stroke. 2007;38:1881-1885.
Conclusions ! Many Stroke Mimics
– Focus on migraine, seizure, and conversion to avoid being fooled in the decision to give lytics
! Permissive HTN still appropriate after CVA – But long term-- Normotensive is the goal
! Statins indicated after ischemic stroke – Target LDL <70 or 50% reduction
! Targeting normoglycemia after stroke can not be recommended based on current evidence – Moderate control is reasonable to BP<200