Embed Size (px)
DESCRIPTION
fssgdsswdswd
Citation preview

1
HIPERTENSI

2

3

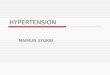
Angiotensin II (Ang II) generated in the afferent arteriole interacts with AT1 receptors on cellular components of the nephron
Angiotensinogen Ang I
Renin
ACEAng II
AT1R
= AT1 Receptor
Slide SourceHypertension Online
www.hypertensiononline.org4

5

Discussion Classification
Why BP should be controlled?
Hypertension Assessment
Target Blood Pressure
Non-pharmacologic Treatment
Pharmacologic Treatment based on Algorhythm
6

≥100or> 160 Stage 2
90-99or140-159 Stage 1
Hypertension
80-89or120-139Prehypertension
<80and< 120Normal
Diastolic(mm Hg)
Systolic(mm Hg)Category
Classification of Hypertension (JNC VII)
7

Category Systolic Diastolic
< 120 and < 80
120-129 and/or 80-84
High Normal 130-139 and/or 85-89
Grade 1 Hypertension 140-159 and/or 90-99
Grade 2 Hypertension 160-179 and/or 100-109
Grade 3 Hypertension ≥ 180 and/or ≥110
Isolated Systolic Hypertension
≥ 140 and < 90
ESH/ESC Classification of BP
Mancia G, et al. J Hypertens 2007;25:1105-1187
OptimalNormal
Slide Source Hypertension Online www.hypertensiononline.org
8

Category Systolic Diastolic
< 120 and < 80
Pre Hipertensi 120-139 and/or 80-89
Grade 1 Hypertension 140-159 and/or 90-99
Grade 2 Hypertension ≥ 160-179 and/or ≥ 100
Isolated Systolic Hypertension
≥ 140 and < 90
Indonesian Classification of BP
Sumber, Sani,2008
Normal
Slide Source Hypertension Online www.hypertensiononline.org
9

Discussion Classification
Why BP should be controlled?
Hypertension Assessment
Target Blood Pressure
Non-pharmacologic Treatment
Pharmacologic Treatment based on Algorhythm
10

Complications of Hypertension:End-Organ Damage
Chobanian AV, et al. JAMA. 2003;289:2560-2572.
Peripheral Vascular Disease Renal
Failure,Proteinuria
LVH, CHD, CHFHemorrhage,Stroke
Retinopathy
CHD = coronary heart diseaseCHF = congestive heart failureLVH = left ventricular hypertrophy
Hypertension
Slide SourceHypertension Online
www.hypertensiononline.org 11

Discussion Classification
Why BP should be controlled?
Hypertension Assessment
Target Blood Pressure
Non-pharmacologic Treatment
Pharmacologic Treatment based on Algorhythm
12

Assessment of Hypertensive Patients
Contributing factors
Complications of hypertension
Causes of secondary hypertension
Target of blood pressure
13

2009 Canadian Hypertension Education Program Recommendations
Assess and manage contributive factor in hypertensive patients i.e.
• Dislipidemia
• Disglycemia (e.g. impaired fasting glucose, diabetes)
• Obesity
• Unhealthy eating
• Physical inactivity
Assessment of Hypertension
Slide SourceHypertension Online
www.hypertensiononline.org
14

2009 Canadian Hypertension Education Program Recommendations
Search for exogenous potentially modifiable factors that can induce/aggravate hypertension
Prescription Drugs:• NSAIDs, including COXIBS (e.g. celecoxib)
• Corticosteroids and anabolic steroids
• Oral contraceptive and sex hormones
• Vasoconstricting/sympathomimetic decongestants
• Calcineurin inhibitors (cyclosporin, tacrolimus)
• Erythropoietin and analogues
• Monoamine oxidase inhibitors (MAOIs)
• Other sympathomemetics e.g. Midodrine
Other:• Licorice root
• Stimulants including cocaine
• Salt
• Excessive alcohol use
• Sleep apnea
Assessment of Hypertension
15

Discussion Classification
Background: Why BP should be controlled?
Hypertension Assessment
Target Blood Pressure
Non-pharmacologic Treatment
Pharmacologic Treatment based on Algorhythm 16

17

Discussion Classification
Background: Why BP should be controlled?
Hypertension Assessment
Target Blood Pressure
Non-pharmacologic Treatment
Pharmacologic Treatment based on Algorhythm 18

Lifestyle Modification
Modification RecommendationDecrease of
Sistolic Blood Pressure
Body weight Maintain normal body weight (BMI 18.5-24.9)
5-20 mm Hg every decrease of 10 kg BW
DASH dietConsumption of fruits, vegetables, low fat milk and low fat cheese
8-14 mm Hg
Reducing salt/sodium intake
Reducing sodium to not more than 2.4 g/ day or NaCl 6 g/day
2-8 mm Hg
Increasing physical activity
Aerobic exercise ie. Walking (30 min/day 4-5 days in a week)
4-9 mm Hg
Reducing alcohol consumption
Limiting alcohol consumption to not more than 2 oz/day for man and 1 oz / day for women.
2-4 mm Hg
Source: The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure JNCVII. JAMA. 2003;289:2560-2572.
19

Food Group Daily Serving Examples and Notes
Grains 7 – 8 Whole wheat bread, oatmeal, popcorn
Vegetables 4 – 5 Tomatoes, potatoes, carrots, beans, peas, squash, spinach
Fruits 4 – 5 Apricots, bananas, grapes, oranges, grapefruit, melons
Low-fat or fat-free dairy foods 2 – 3
Fat-free (skim)/low-fat (1%)milk, fat-free,/low fat yogurt, fat free/low fat cheese
Meats, poultry, fish ≤ 2Select only lean meats, trim away fats; broil, roast, or boil, no frying and remove skin from poultry
Nuts, seeds, dry beans 4 – 5 / week Almonds, peanuts, walnuts, sunflower seeds, soybeans, lentils
Fats and oils 2 – 3Soft margarines, low fat mayonaise, vegetables oil (oil, corn, canola, or safflower)
Sweets 5 / weeks Maple syrup, sugar, jelly, jam, hard candy, sorbet
DASH DIET
DASH eating plan available at: http://www.nhibi.nih.gov/health/public/heart/hpb/dash/new_dash.pdf20

Discussion Classification
Background: Why BP should be controlled?
Hypertension Assessment
Target Blood Pressure
Non-pharmacologic Treatment
Pharmacologic Treatment based on Algorhythm 21

History of antihypertensive drugs
Directvasodilators
Alpha-blockers
Peripheralsympatholytics
Ganglion blockers
Veratrumalkaloids
Central α2 agonists
Calciumantagonists-non-DHPs
Beta-blockers
Thiazidediuretics
Calciumantagonists-
DHPs
ARBs
1940’s 1950 1957 1960’s 1970’s 1980’s 1990’s 2000 2007
ACEinhibitors
DHP, dihydropyridine; ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker
Effectiveness and general tolerability
DRI
22

First line classes of antihypertensive drugs
Diuretics− Inhibit the reabsorption of salts and water from kidney tubules
into the bloodstream Calcium-channel antagonists
− Inhibit influx of calcium into cardiac and smooth muscle Beta-blockers
− Inhibit stimulation of beta-adrenergic receptors Angiotensin-converting enzyme (ACE) inhibitors
− Inhibit formation of angiotensin II Angiotensin II receptor blockers (ARBs)
− Inhibit binding of angiotensin II to type 1 angiotensin II − Receptors
23

Thiazide Diuretics
Thiazides
Veins • Mechanism: inhibit Na/K pumps in the distal tubule
• Examples:
•Hydrocholorthiazide 12.5-25 mg daily
•Chlorthalidone 12.5-50 mg daily
• Effective first line agent
• As single agent more effective if CrCl >30 ml/min
• Compelling indications: HF, High CAD risk, DM, Stroke, ISH
24

Loop Diuretics
ThiazidesLoops
Veins• Mechanism: Inhibit Na/K/Cl ATPase in ascending loop of henle
• Examples:
•Furosemide 20 mg BID
• Typically only beneficial in patients with resistant HTN and evidence of fluid overload;
effective if CrCl <30 ml/min
• MUST be dosed at least twice daily (Lasix = Lasts six hours)
• Administer morning and lunch time to avoid nocturia
25

Aldosterone Receptor Antagonists
ThiazidesLoopsAldosterone Ant.
Veins • Mechanism: inhibit receptor aldosterone reducing Na & water retention
• Examples:
•Spironolactone 25 mg daily
• Can provide as much as 25 mmHg BP reduction on top of 4 drug regimen in resistant hypertension
• Monitor SCr and K
• Compelling indications: HF
Am J Hypertension. 2003; 16:925-930.26

Beta Blockers
Beta Blockers
Heart• Mechanism: Competitively inhibit the binding of catecholamines to beta-adrenergic receptors
• Examples:
•Atenolol 25-100 mg QD, Metoprolol 25 -100 mg BID, Bisoprolol 2.5 – 10 mg QD
•Carvedilol 6.25-50 mg (alfa+Beta) BID
• Monitor: HR, Blood Glucose in DM
• Not contraindicated in asthma or COPD but use caution
• Compelling indications: HF, post-MI, High CAD risk, DM
27

CCB Non-Dihydropyridine: Diltiazem and Verapamil
DiltiazemVerapamil
Heart• Mechanism: Decrease calcium influx into cells of vascular smooth muscle and myocardium
• Examples:
•Diltiazem Long acting; CD 100 -400 mg
•Verapamil 60-480 mg, long acting SR
• Monitor: HR
• Verapamil causes constipation
• Relatively contraindicated in HF
• Compelling indications: DM, High CAD risk
Arteries
28

CCB: Dihydropyridine
Dihydropyridine CCBs
Arteries• Mechanism: Decrease calcium influx into cells of vascular smooth muscle
• Examples:
•Amlodipine 2.5-10 mg PO daily
•Felodipine 2.5-10 mg PO daily
• OROS/GITS. Do not use immediate release nifedipine
• Monitor: Peripheral edema, HR (can cause tachycardia)
• Good add on agent if cost is not an issue
29

ACE Inhibitors
ACEI
• Mechanism: inhibiting synthesis of angiotensin II inhibit vasoconstriction
• Examples:
•ACEI: Captopril 12.5 -50 BID, Enalapril 2.5-40 mg daily –BID, Lisinopril 5 – 40 mg daily, Imidapril 5-10 QD, Perindopril 4-8 mg QD, Ramipril 2.5-20 mg
• Monitor: S Cr, K
• Compelling indications: HF, post-MI, High CAD risk, DM, CKD, Stroke
Arteries
Veins
30

ARB’s
ARB
• Mechanism: blocking action of angiotensin II inhibit vasoconstriction
• Examples:
•ARB: Irbesartan 150-300 mg QD, Losartan 25-100 mg BID, Olmesartan 20-40 mg, Telmisartan 20-80 mg, Valsartan 90-160 mgQD
• Monitor: S Cr, K
• Compelling indications: HF, post-MI, High CAD risk, DM, CKD, Stroke
Arteries
Veins
31

Alpha1 Blockers
Alpha1 Blockers
Arteries• Mechanism: Inhibit peripheral post-synaptic alpha1 receptors vasodilation
• Examples:
•Terazosin 1 – 20 mg daily
•Doxazosin 1 – 16 mg daily
• Cause marked orthostatic hypotension, give dose at bedtime
• Consider only as add on therapy
• Can be beneficial in patients with BPH
32

Central Acting Agents
Central Acting Mechanism:Clonidine
Heart • Mechanism: false neurotransmitters reduce sympathetic outflow reducing sympathetic tone
• Examples:
•Clonidine 0.75-0.6 mg bid, Methyldopa 250 mg-1000 mg BID (Pregnancy), Reserpin 0,1 -0,25 mg QD
• Monitor: HR (bradycardia)
• Side effects often limiting: Dry mouth, orthostatic, sedation
• Withdrawal/Rebound effect
33

Vasodilators
Dihydropyridine CCBsHydralazineMinoxidil
Arteries• Mechanism: Direct vasodilation of arterioles via increased intracellular cAMP
• Examples:
•Hydralazine 20-400 mg BID-QID
•Minoxidil 2.5-40 mg PO daily-BID
• Monitor: HR (can cause reflex tachycardia), Na/Water retention
• Hydralazine is an alternative in HF if ACEI contraindicated
• Consider minoxidil in refractory patients on multi-drug regimens
34

Direct Renin Inhibitor; ALISKIREN• Monotherapy effective in lowering SBP and DBP in hypertensive patients
• Effective also in combination with a thiazide diuretic, a CCB and an ACE inhibitor or an ARB
• Protect against subclinical organ damage when combined with an ARB=➔ the available evidence justifies its use in hypertension, in combination with other agents. Mancia et al.Reappraisal of ESC Hypertension Guidelines 2007
NEWER ANTIHYPERTENSIVE AGENTS
35

Hypertension treatment strategy: JNC VIILifestyle modifications
Not at goal blood pressure (<140/90 mmHg)(<130/80 mmHg for patients with diabetes or chronic kidney disease)
Initial drug choices
Without compelling indications
With compelling indications
Stage 1 hypertension(SBP 140-159 or DBP90-99 mmHg)Thiazide-type diuretics for most. May consider ACE-I, ARB, BB, CCBor combination
Stage 2 hypertension(SBP ≥160 or DBP ≥100 mmHg)Two-drug combination formost (usually thiazide-typediuretic and ACE-I or ARB, or BB, or CCB)
Drug(s) for the compelling indications
Other antihypertensiveDrugs (diuretics, ACE-I, ARB, BB, CCB) as needed
Not at blood pressure goal
Optimize dosages or add additional drugs until goal blood pressure is achieved.Consider consultation with hypertension specialist.
JNC VII. JAMA 2003;289:2560-2572
SBP, systolic blood pressure; DBP, diastolic blood pressure; ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BB, beta-blocker; CCB, calcium-channel blocker
36

Treatment initiation: JNC VII
Normal Pre-hypertensionStage 1 hypertensionStage 2 hypertension
Lifestyle modificationEncourage Yes Yes Yes
Initial drug therapy
Without compelling indicationNo antihypertensive drug indicatedThiazide-type diuretics for most; may consider ACE-I, ARB, BB, CCB, or combinationTwo-drug combination for most (usually thiazide-type diuretic and ACE-I or ARB or BB or CCB)
With compelling indicationsDrug(s) for compelling indicationsDrug(s) for compelling indications; other antihypertensive drugs (diuretics, ACE-I, ARB, BB, CCB) as needed
ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BB, beta-blocker; CCB, calcium-channel blocker
JNC VII. JAMA 2003;289:2560-257237

38

39

40

Follow-up
Hypertensive patients are recommended to be followed at least every month
Follow-up visits are used to:− Increase the intensity of lifestyle and drug
therapy,
− Monitor the response to therapy
− Assess adherence
41

Summary Hypertension is becoming a burden to the
community due to impact on target organs & premature death.
Treatment has proven to reduce morbidity & mortality, but majority of patients were not treated adequately.
Aggressive treatment shown benefit in achieving target blood pressure.
More frequent follow up will be necessary for patients with stage 2 hypertension or patients with comorbid conditions.
42



Thank you