-
Deaths, and counting deaths, is a crucialpublic health indicator
for many reasons.Death is the final and most definitive
healthoutcome of many important public healthproblems. And most
important causes ofpoor health in a population, when commonand
severe enough, produce an elevation inthe mortality rate. Death is
easily defined,making it a health outcome for which astandardized
case definition is easilyapplied. Because death results from somany
health problems - from chronic dis-eases, infectious diseases and
injuries - themortality rate can provide an overall indica-tor of
general health status of a population.Mortality rates can also
provide informationon nutritional status because
widespreadmalnutrition among children or adultsalmost always
results in an elevation of themortality rate, especially if the
level of com-municable diseases is high. Nonetheless,the mortality
rate is a relatively insensitivemeasure of population health
statusbecause conditions often must be quitepoor before it is
markedly elevated. Themortality rate is also relatively
non-specific;there are many causes of elevated mortali-ty, any one
of which might lead to an
increase in the mortality rate. As a result, anelevated
mortality rate can indicate thatthere is indeed a health problem in
a popu-lation, but it cannot indicate the cause.
Mortality rates have been measured in manycountries for hundreds
of years. Deaths areoften counted by various authorities,
includ-ing religious leaders, civil authorities andpublic health
professionals. In stable popula-tions, mortality rates are usually
monitoredby registering deaths using a vital statisticssystem, and
reporting deaths is mandatoryin most countries. However, in many
coun-tries in the developing world, vital statisticssystems are far
from complete. Even if func-tioning, such systems usually are
disruptedearly in situations of civil conflict or displace-ment. As
a result, cross-sectional surveys areoften necessary to determine
accurate mor-tality rates.
Often, especially in emergency situations,initial surveys will
combine the assessmentof many different health and nutrition
out-comes. Recently, nutrition assessmentsurveys have begun
routinely includingmortality measurement. When combin-
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY 33
Defining and Measuring Mortality
2CHAPTER
Key messages Description of the different types of mortality
rates, with formulas used Crude mortality rate/crude death rate
(CMR) Age-specific mortality rate (ASMR) Age-specific mortality
rate for children under 5 years (ASMR-U5) Under-5 mortality rate
(U5MR) Cause-specific mortality rate Infant mortality rate (IMR)
Maternal mortality rate (MMR) Retrospective cross-sectional
mortality surveys The use of a recall period in mortality surveys
Determining the causes of mortality
-
ing nutrition and mortality assessment inthe same survey, it is
important to con-sider the sampling strategy so as not tochoose a
sample which is biased foreither outcome (See Chapter 3 for more
details). Forexample, you cannot include only house-holds with
children 6-59 months in thesurvey sample; the mortality rate in
suchhouseholds may not reflect the mortalityrate in all households
in the population.
COUNTING DEATHSJust counting the number of deaths in apopulation
is not sufficient. For example,if you hear that there have been
139deaths in a certain population, this tellsyou nothing about the
rate of death ifneither the size of the population fromwhich these
deaths were reported nor thetime period during which these
deathsoccurred were known. If you subse-quently learn that the
deaths came froma population of 5,000 persons, you stillhave
insufficient information: If thesedeaths occurred over 10 years,
the rate ofdeath in this population is quite low; onthe other hand,
if these deaths occurredin the same month, the rate of death
isextremely high. This example illustratesthat every mortality rate
must have:
The number of deaths (the numeratorof the mortality rate);
The size of the population from whichthe deaths came (the
populationdenominator of the mortality rate);and
The time period during which thedeaths occurred.
If 127 deaths occurred in a population of19,546 over 9 months
time, the deathrate would be 127 deaths per 19,546 peo-ple per 9
months. However, this rate can-not be compared to the mortality
rate in
other populations of different sizes or tonumbers of deaths
counted over differenttime periods. To determine if the deathrate
is high, low or normal as comparedwith rates in the same population
in pre-vious time periods or compared to ratesin other populations,
the mortality rate ina given population must be converted toa rate
using a standard populationdenominator and time period.
The first step in such a conversion is todecide how the final
rate should beexpressed. There are three differentways to express
the same mortality rate. a) # deaths/1,000/year: For many vital
statistics systems, which recorddeaths for longer time periods
for anentire nation or province, mortalityrates are often expressed
as the num-ber of deaths per 1,000 populationper year.
b) # deaths/1,000/month: In some dis-placed populations, when
the acuteemergency is over and the health sit-uation stabilized
somewhat, mortalityrates are sometimes expressed as thenumber of
deaths per 1,000 popula-tion per month.
c) # deaths/10,000/day: During acutehumanitarian emergencies,
when thenumber of deaths is totalled each dayor every few days, the
mortality rateis often expressed as the number ofdeaths per 10,000
population per day.
These are three different ways to expressthe same mortality
rate; the conversionamong them is merely an exercise inmathematics.
For example, to convertfrom 34 deaths per 1,000 per year todeaths
per 1,000 per month, just dividethe numerator by 12 (1/12th the
numberof deaths will occur in one month as inone year): 34 / 12 =
2.8 deaths per 1,000per month.
34
-
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
35
2CHAPTER
Because the actual number calculatedvaries depending on the
populationconstant and the time period, a mortal-ity rate should
never be stated withoutthese parameters. For example, you can-not
say that the mortality rate is 1.86;you must say that the mortality
rate is1.86 per 10,000 per day. The number1.86 would mean very
different things ifthe population constant and time periodwere
10,000 per day, 1,000 per year or1,000 per month.
SOURCES OF DATA TO CALCULATE MORTALITY RATESIn stable
populations, it is better to col-lect information of death
prospectivelywhere, as each death occurs, it is report-ed to public
health or governmentauthorities. Such systems allow the
cal-culation of recent death rates as fre-quently as is required,
and this data canbe collected easily. In vital statisticssystems,
death reporting is oftenmandatory for persons charged withburying
bodies. If deaths occur pre-dominantly in clinics or hospitals,
med-ical personnel may be responsible fordeath reporting. In many
societies, reli-
gious leaders record deaths. In humani-tarian emergencies,
someone may behired to count deaths and monitor thearea designated
as the graveyard or cre-mation site.
All of these systems of counting deathsrequire separate
information on the sizeof the population from which the
deathsoccurred in order to calculate mortalityrates. Such
information for the popula-tion denominator may come from
censuscounts; census projections; populationregistration; or the
monitoring of births,deaths, immigration and emigration..
Inhumanitarian emergencies and other sit-uations in which data on
population sizeis poor, techniques have been developedto estimate
population size.
But which population size is used as thedenominator if deaths
are counted for atime period during which the popula-tion size
fluctuates? One approachwould be to calculate the average
popu-lation during the time period (add thepopulation at the
beginning of the timeperiod to the population at the end ofthe time
period and divide by 2, produc-ing the arithmetic mean
population).
Example 2.1 Expression of mortality ratesEven though they may
appear to be very different, mortality rates expressed using
different population constants or time periods indicate the same
rate of death in apopulation. For example:
Take a mortality rate of 9.6/1,000 population/year. This could
be expressed as 0.8/1,000 population/month. This could also be
expressed as 0.26/10,000 population/day.
The equivalency of these rates can be seen if we calculate from
one rate to the other. For example, if the rate of 0.26 deaths per
10,000 per day remained constant for an enti-re year, we would
expect that about 95 people would die (0.26 x 365 days in a year)
outof each 10,000 people in the population.
-
A second approach would be to deter-mine the population at the
mid-point ofthe time period and use that (this iscalled the
mid-interval populationand is the method used most commonlyin vital
statistics systems). However, in many situations, the popu-lation
denominator for a mortality rateitself is only a rough population
esti-mate and no accounting can be madefor changes in the
population during thetime period of interest. This is often truein
humanitarian emergencies whichhave the additional complication of
highrates of in-migration and out-migration.
TYPES OF MORTALITY RATESMany different rates are used to
measuremortality: Crude mortality rate/crude death rate
(CMR) Age-specific mortality rate (ASMR) Age-specific mortality
rate for children
under 5 years (ASMR-U5) Under-5 mortality rate (U5MR)
Cause-specific mortality rate Infant mortality rate (IMR) Maternal
mortality rate (MMR)
Crude Mortality Rate (CMR)The crude mortality rate (CMR),
alsocalled the crude death rate or CDR, is
defined as the number of people of allages and both sexes who
die in a giventime interval divided by the total pop-ulation at the
mid-point of that timeinterval. The CMR always includesthe length
of the time interval and astandard population size, called
thepopulation constant. For example, aCMR may be 8.5 deaths per
1,000 per-sons per year.
It is calculated by the following formulawhere: the numerator of
the fraction in
parentheses is the number of deathswhich occurred in a specific
popula-tion during a certain time period.Only deaths which occurred
duringthis time period should be included inthe numerator of the
mortality rate.
the denominator of the fraction is thenumber of people in the
population inwhich these deaths occurred. Thispopulation should be
well defined,and only persons fitting this definitionshould be
included in the denomina-tor. For example, if you are calculat-ing
the mortality rate for a certainprovince, only people who lived
inthat province during the time periodof interest should be
included in thepopulation denominator.
36
-
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
37
2CHAPTER
This means that each person has an average likelihood of
0.006393 (or 0.6393% chance)of dying during the 8-month period.
Stating that the CMR is 377 deaths per 58,975 per 8 months has
little meaning; it can-not be directly and meaningfully compared to
other CMRs from previous periods orfrom other populations. However,
if this rate is converted to deaths per 1,000 per year,as follows,
it can be compared to other rates expressed in the same way:
1. To convert this likelihood to a likelihood for a standard
population size, we multiplythis rate by 1,000 to obtain 6.4. This
means that during the period of 8 months, 6.4 peo-ple died for each
1,000 people in the population.
2. To convert this likelihood to a likelihood for 1 year: 6.4 is
divided by 8/12ths (8 monthsdivided by the 12 months in 1 year) =
9.6 deaths per 1,000 population per year. This ratemeans that, if
the death rate for the 8-month period continued for an entire year,
forevery 1,000 people in the population, there would be 9.6
deaths.
Using the formula above, the rate of deaths per 1,000 per year
would be calculated asfollows:
Example 2.2 Calculation of CMR with standard time unitIn a
specific population, 377 deaths occurred during a period of 8
months in a popula-tion with a mid-interval size of 58,975.
Using the information in the formula you get:377 58,975 =
0.006393 or 0.6393%
Vital statistics systems which calculate mor-tality on an annual
basis use the size of thepopulation on July 1 to indicate the
averagepopulation between January 1 and December31. Such systems
count the number of deathsduring a year's time, divide it by the
mid-interval population, then multiply by 1,000(the population
constant) to get the numberof deaths per 1,000 population per
year.
Since the CMR reflects the overall risk ofdeath in the
population among all ages andboth sexes, it is the least specific
indicator ofmortality. Mortality reflected in the CMRmay result
from causes as varied as thosefrom violent deaths from massacres to
thosefrom neonatal tetanus. If only one indicator
of mortality can be calculated, CMR is usu-ally the one chosen.
Ideally, a newly calcu-lated CMR should be compared with a
pre-vious CMR from the same population todetermine whether the
mortality rate is ris-ing or falling. Such trend information can
beused as an overall evaluation of health,nutrition and other
interventions. However,when prior mortality data are unavailable,
arough rule-of-thumb can be used: a CMR of less than 1 death
per
10,000/day indicates a reasonable healthsituation;
a CMR of more than 1 death per10,000/day reflects elevated
mortality; and
a CMR of more than 2 deaths per10,000/day indicates a health
emergency.
-
Calculating CMR using person-time unitsThe denominator of a
mortality rate is thenumber of people in the population; howev-er,
the denominator can also be seen asbeing based on person-time
instead of thenumber of persons. That is, a rate of 10deaths per
10,000 per day may be seen asthe risk of death in 10,000 people
during aperiod of one day, or the risk in 5,000 peo-ple during 2
days, or the risk in 1,000 peo-ple during 10 days. In all three
examples, thedenominator is 10,000 person-days (thenumber of people
in the population multi-plied by the number of days in the time
peri-od). This will be important later when dis-cussing the
measurement of mortality incross-sectional surveys. The sample
sizerequired to achieve a certain precisionaround the estimate of
the CMR is the num-ber of person-time units required in
thedenominator of the rate.
In general, if births and deaths are distribu-ted evenly
throughout the time period, theneach person who was born or who
diedduring the time period contributes, on ave-rage, _ a
person-time period to the denomi-nator. For example, vital
statistics systems
assume that births and deaths occur evenlythroughout the year.
Therefore, each personwho was born or who died during the
yearcontributed about _ a year to the denomina-tor. Use of the
mid-interval population, asdescribed above, captures half of deaths
andhalf of births and is one way of adjusting thepopulation
denominator for the incompletecontribution of births and
deaths.
Age-Specific Mortality Rates (ASMR)Age-specific mortality rates
(ASMR) restrictboth the numerator and denominator to per-sons of a
certain age. For example, a morta-lity rate for persons 15-49 years
of age is thenumber of deaths of persons 15-49 years ofage divided
by the mid-interval population ofpersons 15-49 years of age
(adjusted for thelength of the time period).
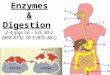
ASMR is often used to determine if the rate ofdeath is
substantially different from thatexpected in any specific age
group. Forexample, in a survey in Kosovo, the deathrate among young
men was much higherthan expected, indicating that some
factordisproportionately increased the risk of deathin this age
group.
38
Figure 2.1 Age-specific mortality rates, Badghis Province, March
2001 - April 2002.
3.5
3
2.5
2
1.5
1
0.5
0
-
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
39
2CHAPTERAge-Specific Mortality Rate for children under 5
(ASMR-U5)The age-specific mortality rate for childrenunder five
(ASMR-U5) is calculated bydividing the number of deaths of
childrenunder age 5 during a specific time periodby the number of
children under age 5.This is often called the under-5
mortalityrate; however, as described below, thisterm is also used
for a completely differentmeasure of mortality in children under
5years of age. For this reason, the termASMR-U5 is used here to
maintain adistinction between these two differentmeasures.
The ASMR-U5 often is used as a more sen-sitive indicator of the
affect of emergencyconditions on mortality. When health
andnutritional status in a population deteriora-tes, the ASMR-U5
often changes earlierand to a greater extent in a crisis
situationthan the crude mortality rate becauseyoung children are
more susceptible tohealth and nutrition insults than olderchildren
and adults.
Cause-specific mortality rateThe cause-specific mortality rate
mea-sures the rate of death due to a specificcause (i.e.,
malnutrition-related deaths,violence related deaths, etc.), and
itincludes only those deaths attributed tothe cause of interest in
the numerator.The population denominator may inclu-de the entire
population, or if the causeof death occurs predominantly in a
sub-group of the population, it may includeonly that subgroup. For
example, if 28people in a population of 78,904 diefrom tuberculosis
during the course of ayear, the cause-specific death rate
fortuberculosis during this time period
would be 35.5 deaths from tuberculosisper 100,000 population per
year.If data on the causes of deaths in apopulation are available,
cause-specificmortality rates provide informationabout the most
important causes ofdeath. Such information can be used todesign
intervention programs addres-sing these causes. However, in
manypopulations, such information is lackingand the causes of death
must be obtai-ned from other sources (see below).
Because the number of deaths from a sin-gle cause is usually far
lower than thenumber of deaths from all causes (mea-sured by the
crude mortality rate), thedenominator of cause-specific death
ratesis often expressed as per 100,000 popula-tion. This allows the
actual rate to be anumber greater than one. In the exampleabove,
the cause-specific death rate fortuberculosis could also be
expressed as0.355 deaths from tuberculosis per 1,000per year, but
that rate is less easily under-stood than the larger number of
35.5deaths per 100,000 per year.
As mentioned above, the denominator ofmortality rates for causes
of death whichoccur predominantly or only in a certainpopulation
group may include only thosemost susceptible to death from
thatcause. For example, death rates for uteri-ne or ovarian cancer
are almost alwaysexpressed as the number of deaths per100,000 adult
women because deathsfrom these causes are confined towomen.
Similarly, death rates for prosta-te cancer are calculated using a
denomi-nator consisting of the number of adultmen in the
population.
-
40
MORTALITY RATIOSSome mortality rates are not truly rates,even
though they may be called a morta-lity "rate." These include rates
whichuse live births as a denominator, such asthe UNICEF under-five
mortality rate, theinfant mortality rate and the maternalmortality
rate.
The under-five mortality rate, or U5MRas the term is most
commonly used, isthe probability of dying before the age offive,
usually expressed per 1,000 livebirths. The U5MR cannot be
calculated
directly from data on births and deathsby age in a single year
because thedeaths, for example, of four-year-oldsoccur to children
born four to five yearsbefore the occurrence. U5MR can be
cal-culated using life table methods, frombirth history data (the
recording of thedate of each birth and the age of deathfor those
that have died), or using indi-rect methods that are beyond the
scope ofthis manual. This measure of childhoodmortality is used
most frequently by UNICEFand others who conduct large
healthassessment surveys.
Comparison of the two measures of under-5 mortality rates
Both U5MR and ASMR-U5 measure the mortality risk for children
under 5 years of age,but the two indicators express the risk
differently. In the case of U5MR, the risk is expressed as the
cumulative probability of dying
before age 5 years in a hypothetical group of 1,000 births. In
the case of ASMR-U5, the risk is expressed relative to the
mid-interval
population as with the crude and other age-specific mortality
rates.
Because U5MR expresses risk over 5 years, whereas ASMR-U5
expresses risk peryear, U5MR is often almost five times as large as
ASMR-U5.
As each measure (U5MR and ASMR-U5) has its uses and its
advocates, there is nooverwhelming reason to recommend one over the
other; they are two different waysof expressing much the same data.
Since relief agencies tend to be more familiar withage-specific
mortality rates, which are derived in the same way as the CMR
(countingdeaths during a period of time and dividing by a
population denominator), that methodwill usually be the one used in
emergency assessments. Moreover, the usual nutritionand mortality
assessment survey done in emergency situations does not gather
thedata necessary to calculate the U5MR; only the ASMR-U5 can be
calculated.
On the other hand, U5MR is used by UNICEF and others when
measuring child morta-lity in stable populations. It is presented
as the measure of child mortality in manysummary publications, such
as the State of the World's Children. To avoid confusion,any
reporting on under-five mortality should specifically note whether
it is calculatedas an age-specific mortality rate or as the
probability of dying by the age of 5 years.For WFP purposes, the
ASMR-U5 should be used.
-
Infant Mortality Rate (IMR)*The infant mortality rate (IMR) is
the num-ber of deaths in children under 1 year ofage in a given
period divided by the num-ber of live births in the same time
period.The infant mortality rate allows assess-ment of the rate of
death in the most vul-nerable age group - children less than 1year
of age. It often rises earlier and fasterin the face of poor health
and nutritionthan other mortality rates.
The infant mortality rate also is describedas a ratio since many
of the children whodie and are recorded in the numeratorwere born
before the beginning of the timeperiod, and thus their birth is not
recordedin the denominator. If the time period is1996, for example,
then a six-month-oldchild dying in March 1996 would havebeen born
in 1995; her death would add tothe numerator but her birth would
not beadded to the denominator. Likewise, achild born late in the
year would still be atrisk of dying under the age of one formuch of
the following year.
The difference between a ratio such asthe infant mortality rate
and the usualmortality rate can also be seen anotherway. The infant
mortality rate calculatesthe chances that a live-born infant
willdie before his first birthday - it is a cumu-lative incidence.
The denominator is thepopulation at the beginning of the
timeinterval of interest. A normal mortality
rate gives the average risk of dying dur-ing the time interval
for a person in apopulation and represents a true rate. Ituses as
the denominator the averagepopulation during the time interval,
ormid-interval population.
Maternal Mortality Rate (MMR) **The maternal mortality rate
(MMR) usesas the numerator all deaths of pregnantwomen or
pregnancy-related deaths with-in 42 days of the end of pregnancy.
Thedenominator is live births. Maternaldeaths are often a
relatively rare cause ofdeath and, as such, the rates should
becalculated only for relatively large popula-tions (more than
1,000,000). Randomvariation in the maternal death rate calcu-lated
in small populations with few birthsmay be misinterpreted as
significanttrends, when they are not actually so.
The maternal mortality rate is critical todetermine the need for
antenatal andobstetric services. Although the actualproportion of
all deaths in a populationresulting from pregnancy-related causesis
often small, the effects of a woman ofchildbearing age dying are
often muchgreater for her family and the society thanthe deaths of
others in the population.Therefore, in a certain country, if
therewere 34,459 births in 2004 and 78 mater-nal deaths, the
maternal mortality ratewould be 226.4 deaths per 100,000
livebirths.
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
41
2CHAPTER
*
**
-
CROSS-SECTIONAL SURVEYS FORRETROSPECTIVE MORTALITY RATESAs
mentioned above, it is better tocount deaths prospectively so that
themortality rates calculated representrecent events. However,
sometimes thesystem to count deaths does not exist ordid not exist
during an earlier timeperiod in which you want to measuremortality.
In such cases, mortality canbe measured using surveys. Just as
withnutritional status or other health outco-mes, mortality
information can be col-lected from the randomly selected
hou-seholds. The people living in these hou-seholds report the
number of deathswhich have occurred in that householdduring a
specified time period. Duringdata analysis, the information
ondeaths for all the households includedin the survey sample is put
together.The total number of deaths in all thehouseholds is counted
and becomes thenumerator of the mortality rate. Thedenominator of
the mortality rate is thetotal number of people in the all
thehouseholds included in the survey sam-ple. The time period is
the period in therecent past during which deaths areasked about.
Hence, you do not need toknow the size of the entire
populationsurveyed or a count of the total numberof deaths in that
population in order tomeasure the mortality rate.
Determining the recall periodIn order to calculate a mortality
ratefrom data obtained by a survey, onlydeaths which occurred in a
definedperiod in the past, called the recallperiod, should be
included. To improvethe accuracy of mortality estimates
incross-sectional surveys, the beginningof the recall period should
be a memo-rable date known to everyone in thepopulation. For
example, the start of the
recall period may be a major holiday orfestival (Christmas,
beginning ofRamadan, etc.), an election, an episodeof catastrophic
weather or other remar-kable event. The end of the recallperiod is
usually the date the interviewtakes place. You can then calculate
thelength of the recall period by countingthe days between the
holiday or otherevent marking the start of the recallperiod and the
date of data collection.Of course, this is rarely a nice
roundnumber of days, like 90 or 180 days.
To detect such deaths, survey workersask respondents living in
randomlyselected households to tell them aboutdeaths which occurred
during thisrecall period. The denominator of themortality rate,
being the total numberof people living in selected households,can
also be seen as the number of per-son-time units (i.e., the number
of per-sons in the selected households timesthe number of time
units in the recallperiod). For example, if a survey selec-ted 569
households in which 3,243 peo-ple lived and the recall period was
7.3months, the denominator would be23,674 person-months. The same
num-ber of person-time units could be obtai-ned from a recall
period of 3.65 monthsand a survey sample of 6,846 people.The
denominator of the mortality ratecan therefore be increased either
byincreasing the number of persons in thesurvey sample or by
increasing thenumber of time units (that is, the lengthof the
recall period).
42
-
Lengthening the recall period is one wayto minimize the sample
size. However,as you lengthen the recall period, you areasking
survey respondents to reportdeaths which occurred in the
moredistant past; naturally,an individual'smemory may become less
reliable overtime. This is especially true if, along withrecalling
the death, you also ask respon-dents about the circumstances or
causesof the death. Moreover, by lengtheningthe recall period, you
will produce anestimate of the mortality rate for a longerperiod in
the past, which may be lessrelevant to current needs than a
morerecent mortality rate.
Thus the sample size for a mortality rateis the number of
person-time units nee-ded to obtain the desired precisionaround the
estimate of the mortality rate.In acute emergencies, the
person-timeunit is usually person-days to express themortality rate
in terms of the number ofdeaths per 10,000 population per day.
Instable populations, the mortality ratemay be expressed as the
number ofdeaths per 1,000 population per monthor per year. The
procedure for calculatingthe minimum sample size to achieve a
certain precision for the mortality rate isdescribed in the
chapter on surveys.
If the mortality rate calculated from sur-vey data includes all
reported deathsduring the recall period, that rate is anaverage for
the entire recall period. Italso may also be possible to
recorddeaths as having occurred in specificparts of the recall
period. For example, ifthe recall period is 9.5 months, one
couldrecord the death as occurring in one ofthree intervals: 1-3
months, 4-6 months,or 7-9.5 months prior to the interviewdate.
Because this increases the comple-xity of the mortality survey, it
shouldonly be included if the additional infor-mation is useful and
if the persons inter-viewed can reliably place deaths intothese
shorter intervals. Most people tendto recall important or traumatic
events ashaving occurred more recently thanactual fact, so care
must be taken to besure responses are accurate. In practice,in
populations where calendar time isnot closely followed and dates
are notwell remembered, recalling exactly whendeaths occurred can
be very difficult.Nonetheless, if a traumatic or importantdate can
be identified within the recall
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
43
2CHAPTERAdvantages of a longer recall period
A smaller sample size (i.e., number ofhouseholds) is needed for
the sameprecision, potentially saving resour-ces and time.
If deaths are recorded for specificparts of the recall period,
it is possibleto look at sub-intervals of time (e.g.,before and
after displacement) or toexamine monthly trends (dependingon sample
size).
Disadvantages of a longer recall period
Mortality rate may be less relevant tocurrent needs than a
mortality ratecalculated for a more recent timeperiod.
Additional information, such as causeof death, becomes
increasingly unreliable as the recall period lengthens.
-
period, separate mortality rates can becalculated for both the
period before andthe period after such a date. For exam-ple, some
surveys done in displacedpopulations have asked if a specific
death in the household occurred beforeor after the household
left its home villa-ge. Separate mortality rates could thenbe
calculated for the pre-displacementand post-displacement
periods.
44
How long should the recall period be?
There is no absolutely correct length for a recall period for
surveys measuringmortality rates. The recall period should be based
on the objectives of the surveyand the following factors:
Accuracy: the recall period should be short enough to allow
accurate recall ofinformation about the death. For most purposes, a
recall period greater than oneyear probably will result in less
accuracy.
Statistical precision: the recall period should be sufficiently
long to provide enoughperson-time units to obtain the desired
precision around the estimate of the morta-lity rate. For sample
sizes used in many surveys, such as 1,000 households, a
recallperiod substantially less than 90 days produces relatively
poor precision.
Recent changes in mortality rates: if mortality rates are
changing rapidly, you maynot be interested in the average rate over
the last year, but rather the average rateover the prior few
months. The population should also have a relatively
constantmortality rate during the recall period. This may have to
be assumed if no informa-tion is available.
Seasonality in mortality: if you are trying to measure the
impacts on mortality of fac-tors not determined by season, the
recall period should be chosen to cover severalseasons so these
effects can be mitigated.
Logistic considerations: longer recall periods reduce the number
of householdswhich need to be included in the survey sample and
therefore the time needed tocomplete the survey.
During the acute phase of an emergency, it may be advisable to
use a short recallperiod, such as 1-3 months, because you may be
most interested in the mortalityrate for a very recent time period.
When measuring mortality in stable populationswith less fluctuation
in the mortality rate, much longer recall periods (such as oneor
more years) can be used.
-
Mortality interview To estimate a mortality rate from a sur-vey
we need to know (a) the number ofpeople at risk, and (b) the length
of timeover which they were at risk. However,the composition of
some of the house-holds will have changed during the recallperiod
(death, birth, migration into andout of the household). As a
result, thenumber of people within each of thehouseholds may not
have been constantduring the recall period.
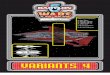
Figure 2.2 demonstrates this concept gra-phically. Time moves
from left to right,with the vertical line on the left being
thebeginning of the recall period and thevertical line on the right
being the end ofthe recall period - usually the date of
datacollection at each household. The asses-sment of mortality will
count only thosedeaths which occurred during the recallperiod
(those deaths occurring betweenthe vertical lines). Each horizontal
lineillustrates a household member. The topline shows a household
member wholived in the household at the beginningof the recall
period and still lived therewhen the survey team visited the
house-hold. The other horizontal lines repre-sent other household
members whoentered or left the household during the
recall period by various means, includingbirth and death. The
dotted horizontallines represent household members whodied during
the recall period; these per-sons would be counted in the
numeratorof the mortality rate. The householdshown in Figure 2.2
had three membersat the beginning of the recall period andalso had
three members at the end of therecall period; however, only one
personwas in the household during the entireinterval. At one time
in the middle of therecall period, the household had
sixmembers.
Two main methods have been used tocount the number of people in
a house-hold in order to calculate a denominatorfor mortality
rates: the past householdcensus method and the current
householdcensus method. For both methods, a hou-sehold census is
taken, whereby a list ismade of all the people living in the
house-hold. In the past household method, thecensus is done as of
the beginning of therecall period. Interviewers might pose
aquestion such as, At the time of {name ofholiday or event}, who
lived in this hou-sehold? In the current household censusmethod,
the census is done as of the timeof the interview; the question
often posedis, Who lives in this household now?
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
45
2CHAPTER
Beginning ofrecall period
Time End of recall period(Usually when survey data
collected)
HH member
Moved into HHduring recall period
Birth during recall period
Moved out of HHduring recall period
Death during recall period
Birth and death duringrecall period
Figure 2.2. Household members' experience during the recall
period
-
In this manual we recommend a modifica-tion of the current
household censusmethod. Essentially, a census is done atboth the
end and the beginning of therecall period. In order to calculate
thedenominator you need to: 1. Ask the household respondent to list
all
the household members at the time ofthe survey (the end of the
recall period).
2. Ask the household respondent if eachof these household
members werepresent at the start of the recall period.
3. Add to the household list all the mem-bers of the household
who were presentat the start of the recall period but arenot
currently present in the household.
4. Ask the household respondent the cur-rent status of each of
the members whowere in the household at the beginningof the recall
period but are no longer inthe household. Status may include
alivebut living elsewhere, dead or unknown.
5. Ask the household respondent if eachperson on the household
list is youngeror older than 5 years of age. Thisallows calculation
of an age-specificmortality rate for children under 5years of
age.
6. Ask the household respondent if anybabies were born during
the recall peri-od and where these newborns are now.
The interviewer also can ask for additionalinformation if other
indices of mortalityare to be calculated:1. The age of each member.
These data
confirm whether an individual is aboveor below 5 years of age
and allow ademographic pyramid of the popula-tion to be
constructed. In addition,other age-specific mortality rates couldbe
calculated, such as those shownabove for Badghis Province.
2. The sex of each member. These dataallow calculation of
separate mortalityrates for males and females.
3. The date of each death if mortalityrates are to be calculated
for sub-periods within the recall period.
4. The cause of death if cause-specificmortality rates or
proportional causesof death are to be calculated.
These data are collected on a form, usinga separate sheet for
each household.Figure 2.3 shows an example of the form.
46
-
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
47
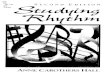
2CHAPTERFigure 2.3 Example of household mortality data
collection form
1ID
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
2Sex
F
M
M
F
F
F
M
M
F
M
M
F
M
M
M
3Current
age (in years)
23
26
54
48
18
12
8
2 mos
4
1
3
29
33
8
31
Survey district: Ambo Village: Limbo Cluster number: 4
HH number: 23 Date: 12- Aug - 04 Team number: 2
4Present
now
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
NO
NO
NO
NO
5Present at
beginning of recallperiod
Yes
Yes
Yes
Yes
NO
Yes
Yes
NO
Yes
Yes
NO
Yes
Yes
Yes
Yes
6Current status(1=Alive;2=Dead;
3=Unknown)
1
1
1
1
1
1
1
1
1
1
1
2
1
1
3
Tally (if data on household members will not entired into the
computer)
a. Number of HH members at end of recall period
b. Number of children < 5 years at end of recall period
c. Number of HH members at beginning of recall period
d. Number of children < 5 years at beginning of recall
period
e. Total number of deaths
Numberabove
11
4
12
2
1
Data comefrom:
Column 4
Columns 3 & 4
Column 5
Columns 3 & 5
Column 6
-
Sometimes survey managers may be tem-pted to ask each household
respondentonly the number of people in the house-hold rather than
listing each householdmember. Although this may be faster, it isfar
less accurate than asking the respon-dent to list all the household
members. Wetherefore strongly recommend that thehousehold members
are listed on a formsuch as that above.
The numerator of the crude mortality ratein the survey sample is
simply the totalnumber of all deaths counted in the surveysample
during the recall period - that is,the sum of all the numbers in
row e forall the households selected for the surveysample. The
population denominator ofthe mortality rate is the average of the
totalpopulation in selected households at thebeginning of the
recall period (the sum ofrow c for all households) and the
totalpopulation in selected households at theend of the recall
period (the sum of row
a for all households). This averagepopulation is then multiplied
by thenumber of time units in the recall periodto derive the
person-time denominatorfor the mortality rate. The time
andpopulation constants are then applied toconvert the mortality
rate to a standardform which can be compared to othermortality
rates.
For under-five mortality, a comparableprocess is followed. The
numerator of theunder-five mortality rate is the number ofdeaths in
children under 5 years of agewhich occurred in selected households,
orthe total of row f for all households. Thedenominator for this
mortality rate is theaverage of the number of children under 5years
of age at the beginning and end ofthe recall period - that is, the
average ofrows d and b. This mid-interval popu-lation of children
under 5 years of age ismultiplied by the number of time units inthe
recall period, as described above.
48
What to do with people whose status in the household is reported
as unknown?
If such persons represent relatively few people who are no
longer in the households,they can be excluded from both the
numerator and denominator.
If they represent a large proportion of household members who
are no longer in the hou-sehold, two mortality rates can be
calculated: one assuming that the unknown membersare alive and one
assuming that the unknown members are dead. Some probing with
mem-bers of the community may also give you an idea whether those
whose status is unknownare more likely to be dead or alive but
living elsewhere. For example, in a population wheremany young men
fled the household to join a fighting group which has not lost many
mem-bers in battle, heads of households may report their status as
unknown, but they may belikely to be alive. In other situations
where attackers take household members away andthere have been mass
executions, such household members may be more likely to be
dead.
In any situation where the number of persons with unknown status
is larger than 10 per-cent of the number of deaths, calculate two
mortality rates (one rate excluding unknownpersons from the
numerator, and therefore assuming that they are still alive, and
thesecond rate including unknown persons in the numerator and
therefore assuming thatthey are dead).
-
CAUSE OF MORTALITY One of the survey objectives may be
todetermine the major causes of death dur-ing the recall period.
During a cross-sec-tional survey, this is done by asking ques-tions
of a surviving household memberwho was present just before and
duringthe death of their relative. The questionsare meant to elicit
a description of thesigns and symptoms experienced by theperson who
died in order to determinewhat illness caused the death.
Thisprocess is notoriously difficult even withan extended interview
of a closely relatedperson very soon after death. Lists of
vali-dated questions exist; however, the inter-view is much too
long for most emergencyassessments and requires highly
skilledinterviewers. More abbreviated lists ofquestions have been
used in some sur-veys, but such lists have not been proper-ly
validated.
Nonetheless, some causes of death may bedistinct enough to
diagnose with fewerquestions. For example, malnutrition maybe
suspected as a cause of death if thepopulation being surveyed has
experi-enced famine and food insecurity, if thesurviving relative
reports lack of food inthe household and if the deceased personhad
rapid weight loss in the few weeksbefore death. In addition, some
diseasesare well known by mothers and others inthe society. Many
cultures and languageshave specific terms for measles,
neonataltetanus and other common illnesses withrelatively unique
appearances.
In many situations of conflict, it may be ofinterest to
determine if deaths have beencaused by war-related violence.
Becausesuch violence is easily identified by laypeople, a short
series of questions, such asthose below, can often accurately
identifydeaths due to this cause.
Questions to detect war-related violence:
1) Did (the person) die from some sort ofinjury such as being
assaulted, shot orstabbed, a car accident, a fall, drown-ing,
poisoning, burn, bite or sting?If YES, go to next question. If NO,
record death as not related toinjury or violence.
2) Was this injury caused by someonefighting the war such as
from a bullet,bomb, mine, machete or assault? If NO, record
non-war-related injury orviolence as cause of death. If YES, record
war-related injury or vio-lence as cause of death.
War-related violence normally affectsonly particular areas
within the wholesurvey area. As a result, if war-relatedviolence
was a major cause of death dur-ing the recall period, the sample
size mayhave to be substantially larger to meas-ure mortality rates
with any precision(see chapter on surveys for more
detailedexplanation). Nevertheless, determiningthe contribution of
war-related violenceto overall mortality may be important inmany
situations.
In general, because of the complexity ofdetermining the causes
of deaths in cross-sectional surveys through interviews,alternate
sources of data should be usedto determine the causes of death.
Suchsources could be disease surveillance,death registration,
clinic or hospital logbooks, or others. If other sources of dataon
causes of deaths do not exist, suchinformation could be collected
duringsurveys if the following conditions exist:
If local terms exist for causes of inter-est, and respondents
can reliably iden-tify them.
If the causes of interest consist only ofviolence.
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
49
2CHAPTER
-
50
Example 2.3 Calculation of mortality rates from a
cross-sectional survey
The data for a cluster sample survey were gathered between June
11 and 17. The sam-ple contained 387 households. At the end of
Ramadan, the November 14, before the sur-vey, 2,818 people lived in
the households selected for the survey sample, of which 535were
children under 5 years of age. At the end of the recall period
(i.e., at the time of sur-vey data collection), the population of
these selected households was 2,827, of whom 578were children under
5 years of age. During the recall period, 44 people died; 31 of
thesedeaths were children under 5 years of age. Seventeen adults
had left the householdduring the recall period and were living
elsewhere; 4 adults were no longer in the house-hold, and their
current status was unknown.
The first step in calculating any mortality rate is to determine
the length of the recallperiod. The mid-point of data collection
fell on June 14; this date can be used as the endof the recall
period. There are 213 days between November 14 and June 14. These
213days are equivalent to 7 months (November 14 - June 14).
Crude mortality rate (in deaths per 10,000 population per
day)
The denominator equals the average population size:
(2,818 + 2,827) = 2,822.52
multiplied by the length of the recall period:
2,822.5 persons x 213 days = 601,192.5 person-days
The numerator equals the 44 deaths reported in all ages during
the recall period. Therefore,the mortality rate equals:
44 deaths x 10,000 = 0.73 deaths per 10,000 population per
day601,192.5 person-days
Crude mortality rate (in deaths per 1,000 population per
month)
If the CMR is to be expressed as deaths per 1,000 per month, the
recall period would be 7months. Therefore, the denominator would
be:
2,822.5 persons x 7 months = 19,757.5 person-months
and the mortality rate would be:
44 deaths x 1,000 = 2.22 deaths per 1,000 population per
month19,757.5 person-months
-
MEASURING AND INTERPRETING MALNUTRITION AND MORTALITY
DEFINING AND MEASURING MORTALITY
51
2CHAPTERAge-specific mortality rate for children under 5 years
of age (in deaths per 10,000 population per day)
The denominator equals the average size of the population of
children under 5 years of age:
(535 + 578) = 556.52
multiplied by the length of the recall period:
556.5 persons x 213 days = 118,534.5 person-days
The numerator equals the 31 deaths reported in children under 5
years of age during therecall period. Therefore, the mortality rate
equals:
31 deaths x 10,000 = 2.62 deaths per 10,000 population per
day118.534.5 person-days
Age-specific mortality rate for children under 5 years of age
(in deaths per 1,000 population per month)
If the age-specific mortality rate for children under 5 years of
age is to be expressed as deaths per 1,000 per month, the recall
period would be 7 months. Therefore, the denominator would be:
556.5 persons x 7 months = 3895.5 person-months
and the mortality rate would be:
31 deaths x 1,000 = 7.96 deaths per 1,000 population per
month3895.5 person-months
-
REFERENCES
Measuring Mortality, Nutritional Status and Food Security in
Crisis Situations: SmartMethodology, Version 1, June 2005. UNICEF
and USAID, New York and Washington, D.C.2005. Available at:
http://www.smartindicators.org/.
Spiegel PB, Sheik M, Woodruff BA, Burnham G. The accuracy of
mortality reporting indisplaced persons camps during the
post-emergency phase. Disasters 2001;25:172-180.
Myatt M, Taylor A, Robinson WC. A method for measuring mortality
rates using pre-vious birth history. Field Exchange 2002;14:13-15.
Available at: http://www.ennonline.net/fex/17/index.html
Woodruff BA. A method for measuring mortality rates using
previous birth history:a commentary. Field Exchange 2002;14:16.
Available at: http://www.ennonline.net/fex/17/index.html
52