-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
1/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
www.medscape.c
Case Presentation
The patient is a 44-year-old man from India with a 2-month
history of low-grade fever, headache, and neck pain.
Recent Medical History
During the 2 months before admission, the patient experienced
gradual progression of his symptoms to include retro-
orbital pain. He also developed confusion and memory lapses,
dysarthria, unsteady gait, fatigue, and anorexia. The ons
of these symptoms was subacute and worsened gradually. He was
evaluated extensively in India before being transferr
to our hospital for further evaluation and management.
Past Medical History
The patient's past medical history is remarkable for uveitis for
approximately 2 years before presentation. He had been
treated with intraocular steroids and oral prednisolone (which
he was taking continuously until 1-2 months prior to
admission, but at varying doses, ranging from 5 to 20 mg a day);
he had also received azathioprine and mycophenolate
mofetil, but these had been discontinued when the most recent
symptoms began because of concern that there might b
an underlying opportunistic infection. He also has a history of
thalassemia minor and had been diagnosed with hepatitis
as a child.
He resided in Calcutta but had traveled all over the world
related to his work as an entrepreneur. He had no history of
tobacco, alcohol, or illicit drug use. His family history was
negative for rheumatologic disease other than osteoarthritis in
his mother.
At the time of admission to Johns Hopkins Hospital, he was
taking no medications and had no history of drug allergies.
Physical Examination
General: well-appearing Indian man, agitated at timesVital
Signs: normal blood pressure and pulse, afebrile
HEENT: mild meningismus, small scar present on inner lower lip
(possible trauma vs ulceration)
Lungs: clear to auscultation bilaterally
Heart: regular, S1 and S2 normal
Abdomen: soft, not tender or distended with normoactive bowel
sounds
Extremities: good peripheral pulses, no clubbing/edema
Genitals: questionable ulceration on scrotum
Skin: folliculitis, otherwise no rash
Neurologic Examination
Mental status. The patient was uncooperative, with limited
attention. He was awake and oriented to self and occasiona
to the name of the hospital, but not to date, city, or state.
Formerly fluent in English, he followed simple commands only
intermittently and had difficulty communicating in English
throughout his hospitalization. He could name objects only
occasionally and could not cooperate with testing for repetition
or more complex commands.
Cranial nerves. His pupils were equal, round, and reactive to
light, and the funduscopic exam was normal, albeit limited
No afferent pupillary defect was observed. Extraocular movements
were intact and visual fields were full, although testin
was, again, limited. No facial droop was apparent but the family
reported noticing that the patient was mildly dysarthric;
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
2/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
facial sensation was grossly intact. His tongue was midline and
shoulder shrug was symmetric.
Motor. Formal testing could not be performed because of lack of
cooperation, but the patient had normal tone and at lea
antigravity strength in all 4 extremities. In spontaneous
movements he used both sides symmetrically.
Sensory. His sensation was grossly intact to noxious stimulation
of all extremities.
Reflexes. Reflexes were 2+ throughout and symmetric, with flexor
plantar responses.
Coordination. The patient was unable to cooperate with
finger-nose-finger and heel-knee-shin testing but had been not
to be dysmetric on the right at the hospital in India. He also
had some truncal instability.
Gait. The patient's gait was quite unsteady and he was unable to
take any steps. He had some retropulsion as well.
Work-up in India
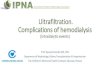
An MRI, performed approximately 1 month after the onset of his
symptoms, is shown in Figures 1 and 2. The MRI revea
abnormal T2-weighted signal, with asymmetric midbrain
enhancement as well as a faint enhancement in the basal gang
bilaterally.
Figures 1 and 2. FLAIR and T1-weighted postgadolinium images
reveal asymmetric midbrain and basal ganglia
enhancement.
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
3/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
Figures 1 and 2. FLAIR and T1-weighted postgadolinium images
reveal asymmetric midbrain and basal ganglia
enhancement.
The remainder of his work-up in India is as follows:
Vascular: Transesophageal echocardiogram normal, anticardiolipin
and lupus anticoagulant normal, hemoglobin
electrophoresis normal.
Inflammatory: Antinuclear antibody (ANA)- and
anti-dsDNA-negative; rheumatoid factor (RF)-negative; ESR 5;
collagen
replated peptide (CRP) 0.23; negative cryoglobulins. A partially
completed gallium scan was negative; bone marrow
biopsy was negative for sarcoid; HLA-B27 was negative.
Demyelinating: Somatosensory evoked potentials, visual evoked
potentials, and brainstem auditory evoked response
were normal.
Infection: Urine tuberculosis (TB) PCR and TB skin test
negative, Ag test forPlasmodium falciparum, RPR, HIV-1,2, an
HCV all negative.Neoplastic: CT chest/abdomen normal.
Neurologic testing: Neuropsychological testing revealed
difficulty with word retrieval and word generation, and impaire
ideational fluency.
Slit-lamp exam revealed active vitreitis in both eyes.
EEG: 9-10 Hz, unremarkable
A lumbar puncture performed in India showed 22 WBCs (80%
lymphocytes, 20% polys), 0 RBC, protein 55, glucose 60.
Spinal fluid was negative for all of the following: Gram stain,
acid-fast bacilli, CSF IgG index, oligoclonal bands,
Cryptococcus antigen, CSF cytology, and ACE, and PCR-negative
for TB, herpes simplex virus (HSV), human
herpesvirus-6, Epstein-Barr virus (EBV), cytomegalovirus (CMV),
varicella zoster virus, enterovirus, Japanese encephal
virus.
Treatment Before Transfer
The patient received a brief course of empiric anti-TB therapy
(details of which medications were used were not availabl
this treatment was stopped because of significant
gastrointestinal side effects. He also received a daily pulse of
IV
solumedrol 1g for 5 days, with "worsening of symptoms" according
to the family. Two days before he was transferred, th
patient's MRI (Figures 3 and 4) and lumbar puncture were
repeated.
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
4/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
Figures 3 and 4. Repeat MRI scans reveal multiple new areas of
enhancement.
Figures 3 and 4. Repeat MRI scans reveal multiple new areas of
enhancement.
Lumbar puncture results now revealed 25 WBCs (differential not
available), a protein of 100, and CSF glucose of 41. HS
CMV, and TB PCR remained negative, as did the Gram stain.
In summary, this is a 44-year-old from India with a history of
uveitis and subsequent confusion, ataxia, headache, history
of low-grade fevers, with gradual progression over 2 months, and
possible scrotal ulceration. MRI imaging reveals multip
areas of enhancing, T2-bright signal in the brainstem as well as
in the periventricular white matter. His CSF demonstrate
a primarily lymphocytic pleocytosis with low CSF glucose and
elevated CSF protein.
What's the most likely diagnosis?
Tuberculosis
Sarcoidosis
Neuro-Behet's disease
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
5/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
Other systemic vasculitis
Progressive multifocal leukoencephalopathy
Multiple sclerosis/demyelinating disease
Primary CNS lymphoma
Astrocytoma
CNS Whipple's disease
Hospital Course
The patient underwent a repeat MRI and lumbar puncture at the
time of transfer (Figures 5 and 6).
Figures 5 and 6. FLAIR and T1-weighted postgadolinium scans 1
week after previous scans show larger areas of
enhancement.
Figures 5 and 6. FLAIR and T1-weighted postgadolinium scans 1
week after previous scans show larger areas of
enhancement.
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
6/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
The repeat lumbar puncture revealed 35 WBCs, CSF glucose, 37
mg/dL and protein, 81 mg/dL. The white cell count
differential showed 17% "other cells," and CSF cytopathology was
positive for high-grade lymphoma, monoclonal B-cell
population. CT scans and body PET were negative for any systemic
disease elsewhere, and ophthalmologic slit-lamp
exam revealed likely lymphomatous cells in the vitreous.
Final Diagnosis
Primary CNS lymphoma.
Discussion
Primary CNS lymphoma is a subtype of non-Hodgkin's lymphoma that
is confined to the central nervous system, includi
the brain, eyes, meninges, and spinal cord. These lymphomas
comprise 1% to 6% of malignant brain tumors in
immunocompetent patients, with a peak incidence in the sixth
decade of life, more often in men than in women.[1,2] In
immunocompetent patients the incidence is 0.3 per 100,000
person-years.[3] Among the population with AIDS and in
primary immunocompromised patients in whom this diagnosis is
seen, the incidence is 4-5 per 1000 person-years.[4]
Thus, 2% to 6% of persons with AIDS develop primary CNS lymphoma
at some point in their disease and, at autopsy, u
to 12% of these patients are found to have it.[2,4]
This discussion will be limited to primary CNS lymphoma in the
immunocompetent patient, rather than primary CNS
lymphoma in AIDS patients, which is typically an EBV-associated
malignancy (the association with Epstein-Barr virus is
not seen in the subtype of immunocompetent patients as it is in
AIDS patients).[4,5]
Diagnosis of Primary CNS Lymphoma
Cognitive changes are often the first symptoms of primary CNS
lymphoma, and may be followed by psychomotor slowin
personality changes, disorientation, or changes from elevated
intracranial pressure.[2] Two percent to 33% of patients
have seizures at some point; because primary CNS lymphoma is
typically a disease of white matter, seizures are not as
prevalent as they would be in a patient with a primary gray
matter lesion.[2] Approximately 10% to 20% of patients have
apparent uveitis at the time of diagnosis and this is a
well-known "mimicker" of lymphoma.[3,5]
Neuroimaging most frequently reveals solitary lesions, but up to
30% of patients may have multiple lesions.[5] The lesion
are typically periventricular, homogeneously enhancing, and with
no central necrosis.[6] The typical locations include the
corpus callosum, the thalamus, and the basal ganglia. The
predilection for the corpus callosum is almost always limited
patients with primary CNS lymphoma. Involvement of the spinal
cord is rare (approximately 1% of patients),[6] and
although leptomeningeal involvement may only be seen on
neuroimaging in 7% of patients by 1 report,[3] there is
involvement of the leptomeninges in up to 40% of patients at
diagnosis.[3,5] The last MRI performed on our patient
revealed these clearly demarcated enhancing periventricular
lesions. Earlier findings may not be so clear-cut.
Furthermore, lesions on MRI may disappear quickly when steroids
are given but can return at a later time.[2,3]
Other conditions that can appear similar radiographically
include gliomas, metastatic cancers, or inflammatory
conditions[7]; in an immunosuppressed patient, toxoplasmosis can
have a very similar appearance radiographically. The
differential is often much broader based on early imaging
findings that may not yet show distinct mass lesions. To make
definitive diagnosis, consideration of biopsy, either
stereotactic or open, should be made; ideally this should not be
done
after a patient has completed a course of steroids because this
may interfere with pathological diagnosis.[3,7]
A recent autopsy study[8] demonstrated extensive lymphomatosis
despite fewer lesions revealed by MRI; many of these
patients had undergone MRIs within 2 weeks of death, suggesting
that the MRI does truly underestimate tumor burden.
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
7/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
Prognosis and Treatment
If untreated, the median survival of this disease is 4.6
months.[9] Treatment options include steroids, whole brain
radiatio
and chemotherapy, or some combination of these. Treatment with
steroids alone may lead to rapid disappearance of
lesions, but this is only a transient effect and lesions will
inevitably return. Use of whole brain radiation alone leads to
a
response rate of greater than 90%, but many of these patients
relapse as well, within 10-14 months.[3,5,9]
In the past, radiation to ocular compartments was considered
necessary for patients with eye involvement, as was spine
radiation for patients with positive CSF cytopathology. However,
new results from chemotherapeutic trials[10] indicate th
extensive radiation may no longer be necessary. Preirradiation
chemotherapy plus radiotherapy is another combination
that has been tried using a variety of chemotherapeutic agents.
The most promising results have been seen with
methotrexate as the agent of choice.[2,11,12] The "DeAngelis
protocol" consists of IV methotrexate at a dose of 1g/m2,
followed by whole brain radiation and finally ara-C,
dexamethasone, and intrathecal methotrexate. Survival has been
fai
good, even up to a greater than 20% 5-year survival, but
significant neurotoxicity has been reported during this
survival
period.[11]
Various other regimens of preirradiation methotrexate-based
chemotherapy have been used with varying results and
some persistent neurotoxicity.[3,13-15] Neurotoxicity is
probably a consequence of the whole brain radiation, and sympto
consist primarily of dementia, ataxia, urinary incontinence, and
leukoencephalopathy.[3,13] This is seen more frequently
patients older than 60 years[3,13,14]; in one report, some
degree of neurotoxicity was seen in up to 32% of patients.[13]
Other treatment possibilities have included intra-arterial
administration of mannitol to help disrupt the blood-brain
barrier
for subsequent chemotherapy delivery. Mannitol works by
loosening the tight junctions of the blood-brain barrier by
shrinking the endothelial cells osmotically, thus allowing
better diffusion of chemotherapeutic agents (with the best
resul
when using methotrexate as part of the regimen). Intra-arterial
administration of mannitol is complicated and the mannito
administration has significant toxicities, including sepsis and
stroke. However, the patients who tolerated this therapy
experienced a median survival of greater than 40 months and less
neurotoxicity because there was no associated
radiation.[16]
The final therapeutic approach has involved using
chemotherapeutic agents alone, with the goal of lowering
neurotoxicit
from radiation. Combination therapy with agents such as
cyclophosphamide/hydroxydoxorubicin/Oncovin
(vincristine)/prednisone (CHOP), as is typically used for
systemic non-Hodgkin's lymphoma, hasn't produced very
promising results, although adding an alkalizing agent such as
thiotepa has provided some benefit because it rapidly
diffuses to the brain.[3] However, recent data have indicated
excellent results in patients who receive high-dose IV
methotrexate, at a dose of 8 g/m2, which is sufficient to
penetrate the blood-brain barrier, thus eliminating the need
for
intrathecal methotrexate.[10,14] This dose is given every 2
weeks to a maximum of 8 cycles or until a complete response
achieved (MRI is performed with every other cycle), then 2 more
cycles are given every 2 weeks, followed by monthly
maintenance for 11 months. This regimen has much less toxicity,
although creatinine clearance must be carefully follow
before initiating this high-dose treatment and before oral
leucovorin rescue is included; patients are hospitalized for
each
cycle. In a preliminary study,[10] 52% of patients experienced a
complete response (defined as complete resolution of th
tumor radiographically), 22% had a partial response, and 22%
experienced progression of disease at 22.8 months.Median survival
was not yet reached at the time that this study was completed.
Our Patient's Follow-up
Our patient received the high-dose IV methotrexate protocol, and
after a few cycles his gait and cognition were already
improving. He has not required either intrathecal chemotherapy
or ocular radiation for his documented ocular lymphoma
His first follow-up MRI reveals some improvement in abnormal
signal (Figures 7 and 8), and a follow-up ophthalmologic
exam after 3 cycles showed normal vitreous with no tumor
cells.
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
8/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
Figures 7 and 8. MRIs after 2 cycles of high-dose methotrexate
show some resolution of enhancing lesions.
Figures 7 and 8. MRIs after 2 cycles of high-dose methotrexate
show some resolution of enhancing lesions.
References
1. Schabet M. Epidemiology of primary CNS lymphoma. J
Neurolooncol. 1999;43:199-201.
2. Schlegel U, Schmidt-Wolf IG, Deckert M. Primary CNS lymphoma:
clinical presentation, pathological classificatio
molecular pathogenesis and treatment. J Neurol Sci.
2000;181:1-12.Abstract
3. Basso U, Brandes AA. Diagnostic advances and new trends for
the treatment of primary central nervous system
lymphoma. Eur J Cancer. 2002;38:1298-1312.Abstract
4. Goplen AK, Dunlop O, Liestol K, Lingjaerde OC, Bruun JN,
Maehlen J. The impact of primary central nervous
system lymphoma in AIDS patients: a population-based autopsy
study from Oslo. J Acquir Immune Defic Syndr
Hum Retrovirol. 1997;14:351-354.Abstract
5. Plasswilm L, Herrlinger U, Korfel A, et al. Primary central
nervous system (CNS) lymphoma in immunocompetent
patients. Ann Hematol. 2002;81: 415-423.Abstract
6. Buhring U, Herrlinger U, Krings T, Thiex R, Weller M, Kuker
W. MRI features of primary central nervous system
-
7/31/2019 44-Year-Old Man With Fever, Headache, Confusion, And
Ataxia
9/9
9/21/11 2:4-Year-Old Man With Fever, Headache, Confusion, and
Ataxia (printer-friendly)
Page ttp://www.medscape.com/viewarticle/460254_print
Medscape General Medicine. 2003;5(3) 2003 Medscape
lymphomas at presentation. Neurology.
2001;57:393-396.Abstract
7. Gliemroth J, Kehler U, Gaebel C, Arnold H, Missler U.
Neuroradiological findings in primary cerebral lymphomas
non-AIDS patients. Clin Neurol Neurosurg.
2003;105:78-86.Abstract
8. Lai R, Rosenblum MK, DeAngelis LM. Primary CNS lymphoma: a
whole-brain disease? Neurology. 2002;59:1557
1562.
9. Glass J, Gruber ML, Cher L, Hochberg FH. Preirradiation
methotrexate chemotherapy of primary central nervous
system lymphoma: long-term outcome. J Neurosurg.
1994;81:188-195.Abstract
10. Batchelor T, Carson K, O'Neill A, et al. Treatment of
primary CNS lymphoma with methotrexate and deferredradiotherapy: a
report of NABTT 96-07. J Clin Oncol. 2003;21:
1044-1049.Abstract
11. DeAngelis LM, Yahalom J, Thaler HT, Kher U. Combined
modality therapy for primary CNS lymphoma. J Clin
Oncol. 1992;10: 635-643.Abstract
12. DeAngelis LM, Seiferheld W, Schold SC, Fisher B, Schultz C.
Combination chemotherapy and radiotherapy for
primary central nervous system lymphoma: Radiation therapy
oncology group study 93-10. J Clin Oncol. 2002;20
4643-4648.Abstract
13. Abrey LE, Yahalom J, DeAngelis LM. Treatment for primary CNS
lymphoma: The next step. J Clin Oncol. 2000;1
3144-3150.Abstract
14. Watanabe T, Katayama Y, Yoshino A, Komine C, Yokoyama T,
Fukushima T. Long-term remission of primary
central nervous system lymphoma by intensified methotrexate
chemotherapy. J Neurooncol. 2003;63:87-95.
Abstract
15. O'Brien P, Roos D, Pratt G, et al. Phase II multicenter
study of brief single-agent methotrexate followed by
irradiation in primary CNS lymphoma. J Clin Oncol. 2000;18:
519-526.Abstract
16. Dahlborg SA, Henner WD, Crossen JR, et al. Non-AIDS primary
CNS lymphoma: First example of a durable
response in a primary brain tumor using enhanced chemotherapy
delivery without cognitive loss and without
radiotherapy. Cancer J Sci Am 1996;2: 166.