Embed Size (px)
Citation preview

Surat Tanprawate, MD, FRCPTNorthern Neuroscience Center
Chiangmai University
Resident Tutorial Long case Board
Examination
www.neurologycoffeecup.com

www.neurologycoffeecup.com
“Fear factors in Long Case Neuro Examination”
and“How to approach to ataxia”
By
Dr. Surat
Present


Fear Factors
• Hard to get neurological history
• Hard to do the physical neurological exam
• Hard to conclude the results
• Hard to make neurological diagnosis

Fear Factors
• Hard to get neurological history
• Hard to do the physical neurological exam
• Hard to conclude the results
• Hard to make neurological diagnosis
Symptomatology
Practice the physical exam
Practice to list the problem
To know the common diseases


Key Concept
Symptoms approach
“Algorithm”

Key Concept
Symptoms&Signs
“Specific examination”

Key Concept
To diagnose
“Problem list and Conclusion”



Symptomatology
Syndrome

• Disorder of consciousness
• Level of consciousness
• Content of consciousness
• Mental disorder• Memory• Intelligence• Personality• Behavioral • Dementia
• Visual disorder• Visual loss
• Ocular motility disorder
• Diplopia
• Abnormal ocular ossilation
Symptomatology

Lower cranial nerve disorder
• Deafness/tinnitus
• Vertigo
• Balance/staggering
• Swallowing
• Voice change
Symptomatology
Multiple Cranial Nerve Disorders

• Sensory disorder• Pain disorder
• Headache and facial pain• Others pain disorder
• Numbness/tingling
• Motor disorder • Weakness• Movement disorder• Gait abnormality• Ataxic disorder
• Sphincter disorder
• Episodic disorder– Seizure/epilepsy– Syncope– TIA– Abnormal movement– Migraine
Symptomatology

Syndrome• Amnistic and Dementia syndrome
• Neuro-opthalmology syndrome
• Syndrome of Multiple cranial nerve disorder
• Stroke syndrome
• Cortical stroke syndrome
• Lacunar stroke syndrome
• Brain stem stroke syndrome
• Spinal cord syndrome

Ataxia

Algorithm
Specific examination
Conclusion and Diagnosis
Ataxia
Gait abnormality
Specific examination-confirm ataxic disorder-for categorized ataxia

GreekwordA=nega.ve
Taxi=order

Ataxic symptoms?-Nystagmus-Dysarthria-Trunkcal ataxia-Limb and gait -ataxia
Ataxic symptoms mimicker?
Ataxia: disease other than cerebellum
Cerebellar’s disease-Where’s the lesion (cerebellum, cerebellar peduncle, cerebellar tract) -What’s the lesion
True Ataxia• Mildweakness• Apraxia• Abnormalmovement• Gaitabnormality
AtaxiaAlgorithm

NeuroanatomyNeurophysiology

• Coordinating skill voluntary movement
• Muscle activity
• Control equilibrium
• Muscle tone
Function of cerebellum

• Lesion
• Incoordination (ataxia) of volitional movement
• Tremor (ataxic or intention tremor)
• Disorder of equilibrium and gait
• Diminish muscle tone
Function of cerebellum

Toa7ributedsensorimotornetwork:
• cerebralcortex
• basalmotornuclei
• thalamus
• re:cularforma:on
Cerebellar pathway



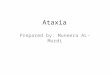
Func.onalZone

Functional divisions
Deep Nuclei Connections Functions
Vermis(face, proximal
body)
Fastigial Vestibular nucleusReticular formationMedial descending system
Axial and proximal muscle controlProgressive movement
Intermediate zone (spinal cord)
Interposed Red nucleusMotor cortexLateral descending system
Distal muscle controlProgressive movement
Lateral zone (cortex, pons)
Dentate Red nucleusThalamusMotor, premotor cortex
Motor planningInitiationTiming
Flocculonodular lobe
Vestibular nuclei, visual system
Vestibular nuclei Axial equilibriumEye movementsVestibular reflexes
Part of Cerebellum

Cerebellar peduncles
Tracts connect to brain stem
Major pathways Connections
Superior Brachium conjunctivuum
Afferent Efferent
Rubral, thalamic, Dentate, spinal cord
Middle Brachium pontis Afferent only
Pontine nuclei
Inferior Restiform body Afferent Efferent
Vestibular, olive, Spinal cordReceives from Flocculonodular lobe
BasicAnatomy–Cerebellarpeduncles

Blood Vessel

Ataxic symptoms?-Nystagmus-Dysarthria-Trunkcal ataxia-Limb and gait -ataxia
Ataxic symptoms mimicker?
Ataxia: disease other than cerebellum
Cerebellar’s disease-Where’s the lesion (cerebellum, cerebellar peduncle, cerebellar tract) -What’s the lesion
True Ataxia• Mildweakness• Apraxia• Abnormalmovement• Gaitabnormality
AtaxiaAlgorithm

What is the cerebellar syndrome?
What is the associated signs?

Pure cerebellum
ClassifiedCerebellarsyndrome
WithBrainstem
signs
ClassifiedBrainstemSyndrome?
With mild hemiparesis
Involve fronto-Ponto-
CerebellarPathway“Ataxic
hemiparesis”
Associated signs

Cerebellar hemispheric syndrome
Rostral vermis
syndrome
Caudal vermis
syndrome
Pancerebellar syndrome
Unilateral intermediate, lateral zones
Ant, sup vermis
Flucculonodular,
post vermis
All regions
Classifiedcerebellarsyndrome

Cerebellarsyndromes
Regionsinvolved
Distribu.onsofdeficits
Commoncauses
Cerebellarhemispheresyndrome
Cerebellar hemisphere
Ipsilateralhead&body
Infarct,neoplasm,abscess,demyelina:on
Rostralvermissyndrome
Ant,supvermis Gait,trunk Alcoholism,thiaminedef
Caudalvermissyndrome
Flucculonodular,postvermis
Axialdiisequilibrium
Midlineneoplasm
Pancerebellarsyndrome
Allregions Bilateralsymmetricalsignsofcerebellardysfunc:on
Toxic,metabolic,infec:ous,paraneoplas:c,degenera:ve
Cerebellar syndrome and its disorders

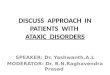
Posterior inferior cerebellar artery (PICA)Anterior inferior cerebellar artery (AICA)
Superior cerebellar artery (SCA)Posterior cerebral artery (PCA)
PICA = lateral medulla & inferior cerebellumAICA = lateral caudal pons & part of cerebellum
SCA = superior cerebellum & rostral laterodorsal ponsPCA = midbrain, thalamus, medial surface of occipital lobe, inferior and medial
surfaces of temporal lobe

Brainstem Vascular Territories

SYNDROME STRUCTURES DAMAGED CLINICAL SYMPTOM
Lateral medullary (PICA, Wallenberg’s)syndrome
Damage Level:
Lateral medullar
Corticospinal tract(pyramid)
Contralateral hemiplegia
Trigerminal spinal nucleus
Ipsilateral facial hemisensory loss
Ipsilateral palatal, pharyngeal, vocal cord paralysisDysarthria, dysphagia
Spinothalamic tract Contralateral hemisensory loss
Vascular supplyPICA
Nucleus ambiguous
Sympathetic fiber Ipsilateral Horner’s syndrome
Vertigo, N/VVestibular nuclei
Cerebellum Ipsilateral cerebellar sign

SYNDROME STRUCTURES DAMAGED CLINICAL SYMPTOM
Lateral inferior pontine syndrome
(AICA stroke syndrome)Damage Level:
Lateral inferior pons
Vestibular nucleus Ipsilateral vertigo, N/V, nystagmus
Contralateral hemisensory loss
Nuclear of CN7 Ipsilateral facial palsy
Ipsilateral deafnessCochlear nucleus
Cerebellum Ipsilateral ataxia
Spinothalamic tract
CN 5 Ipsilateral hemisensory loss of face

Neurological examination in
ataxia

Nystagmus
Patient Video

Intention tremor
Patient Video

Finger to Nose Test
Patient Video

Ataxic gait
Patient Video

Ataxic speech
Patient Video

What’s lesion?
Time, Caused, OnsetMedical History
Neurological Signs

• Sudden
• Vascular
• Acute
• Intoxication
• Viral, Post infectious
Time Caused Onset
• Subacute
• Intoxication
• Chronic
• Hereditary
• Paraneoplastic syndrome
• Hypothyroid
• Intoxication

• Acquired
• Wernicke’s encephalopathy
• Miller Fisher syndrome
• Hereditary
• SCA
• FA
Symmetrical ataxia plus syndrome

Imaging • to exclude identifiable
structural lesion• Atrophy of cerebellum or
spinal cord
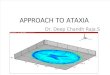
AD
Acquired causes-Alcohol/medication
-Hypothyroid-Vit.B12-Anti-HIV
-Paraneoplastic study-GAD Ab
Evaluate •Accurate family history• Phenotype
Singleton patient
AR
SCA1,2MJD
SCA6,7SCA10,12DRPLASCA17
FAAT
AVEDAbetalipoproteinemia
AOAMitochondrialdisorder
Pt.withprogressiveataxia

ENDwww.neurologycoffeecup.com
Next Episode: Neuro-opthalmology approachDiplopia, Visual loss, Ptosis