Embed Size (px)
Citation preview

404Health Care Reform
January 2013
The Patient Protection and Affordable Care Act pp 13-21
Accountable Care Organizations pp 22-27
Incentives for Reform: Pay for Performance pp 28-32
The Family Physician and Health Care Reform pp 33-38

FP Essentials™
FP Essentials™ Subscription Information:
American Academy of Family Physicians 11400 Tomahawk Creek Parkway, Leawood, KS 66211-2680
For reference citations, use the following format: Waits JB, Smith L, Miller BF. Health Care Reform. FP Essentials™, Edition No. 404. Leawood, KS: American Academy of Family Physicians; January 2013.
Faculty
Barry D. Weiss, MDFP Essentials™ Medical Editor
Mindy A. Smith, MDJennifer E. Frank, MD
Associate Medical Editors
Editorial BoardBarry D. Weiss, MD, Chair
Heidi Chumley, MDS. Lindsey Clarke, MD
Joel J. Heidelbaugh, MDJanell Jones, MD
Barbara A. Majeroni, MD
Staff
Elaine Kierl GangelManaging Editor
Manager, CME Subscriptions & Bulletins Department
Andrea HardenSenior Associate Editor
Penelope L. LaRocqueKaren Montemayor
S. Jane ThomasContent Specialists
Sam CarlsonEditorial Assistant
Stacey HerrmannProduction Graphics Manager
Douglas E. Henley, MDExecutive Vice President
Perry A. Pugno, MD, MPHVice President for Education
Mindi McKenna, PhD, MBADirector,
Division of Continuing Medical Education
Ann M. Karty, MD, FAAFPMedical Director,
Division of Continuing Medical Education
Cover illustration byMark Miller
ISSN# 2159-3000
The FP Essentials faculty and staff thank the physicians listed below, each of whom
reviewed at least 1 manuscript between January 1, 2012, and December 31, 2012.
David S.H. Bell
Fred Corley
William Gregory Feero
Scott Fields
Mark Friedman
Angela Gialamas
Lawrence Tim Goodnough
Norah Lynn Henry
Aimee L. Lucas
Wayne J. Morgan
Adam B. Murphy
Stephen Paul
Matthew A. Rank
Karl T. Rew
Donald W. Shenenberger
Ganga L. Srinivas
Danielle Kim Turgeon
Fred Volkmar
Mike Weisgerber

FP Essentials™ 404
Health Care Reform
AUTHORS
John B. Waits, MDLacy Smith, MDBenjamin F. Miller, PsyD
John B. Waits, MD, -
Lacy Smith, MD, -
Benjamin F. Miller, PsyD, -
Acknowledgment-
-
FP Essentials.
Disclosure: According to AAFP policy, authors must disclose all associations with proprietary entities that may have a direct relationship to the subject matter of their manuscript. The authors and staff have returned disclosure forms indicating that they have no such affiliation or financial interest to disclose. The AAFP uses an anonymous peer review process to evaluate the content of this activity. This process ensures a clear resolution of any potential conflicts of interest, and guarantees the fairness and balance of the content.
Copyright © 2013 American Academy of Family Physicians. All rights reserved.Written permission from the American Academy of Family Physicians is required for reproduction of this material in whole or in part in any form or medium.

2
ForewordI am a family physician, not a legal scholar. As such,
I have little interest in pouring through pages of leg-islation to figure out what the Patient Protection and Affordable Care Act (PPACA) really means. However, I recognize, particularly with the recent decision by the Supreme Court of the United States, that under-standing this lengthy and complex piece of legislation is necessary because it will affect my future practice as well as my own family’s health care coverage.
Understanding this legislation requires learning new lingo, such as medical loss ratio and actuarial value. In Section One, Dr Waits and his colleagues do a remarkable job of distilling the important facets of PPACA into an explanation that is directed at the family physician. I now better understand the letter I recently received from my own health insurance company that assured me that its medical loss ratio was greater than 80%.
In Sections Two and Three, the authors tackle two relatively new, increasingly important, and controver-sial aspects of health care reform—accountable care organizations (ACOs) and pay for performance. The health care system in which I am employed is partici-pating in the Pioneer ACO Program, and I now have
a much better idea of what that may mean both prac-tically and financially for the organization. Part of my salary is already determined by how well my partners and I perform on certain quality indicators. Each year, the percentage of my salary determined by quality performance increases. After reading this edition of FP Essentials™, I recognize that pay-for-performance programs are the trend nationwide.
Section Four is personalized to those of us in family medicine, describing how the American Academy of Family Physicians (AAFP) views, articulates, advo-cates, and engages in the health care reform debate. In addition to discussing how the PPACA addresses some of the AAFP’s advocacy points pertaining to health care reform, this section also explores additional components of health care reform for which AAFP is currently advocating.
I hope you enjoy this FP Essentials and find its description of and perspective on health care reform relevant, succinct, understandable, and informative.
Jennifer E. Frank, MD, FAAFP, Associate Medical Editor Family Physician
Theda Care Physicians, Neenah, Wisconsin
Learning Objectives 1. Describe the key provisions in the Patient Protection and Affordable Care Act
(PPACA). 2. Identify changes brought about by health insurance reform that are most likely
to affect patients. 3. Describe the primary purpose of an accountable care organization (ACO). 4. Define the different types of ACO programs being offered by the Centers
for Medicare & Medicaid Services. 5. Describe the Hospital Value-Based Purchasing Program and what types
of outcomes will be measured. 6. Identify differences in how various pay-for-performance programs are structured. 7. Cite the American Academy of Family Physicians (AAFP) 7 principles for pay-for-
performance programs. 8. Describe the components of health care reform advocated for by the AAFP. 9. Discuss how the PPACA addresses the components advocated for by the AAFP.

3
ContentsPage
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Learning Objectives . . . . . . . . . . . . . . . . . . . . . . . .2Tables and Figures . . . . . . . . . . . . . . . . . . . . . . . . .4Information for Readers . . . . . . . . . . . . . . . . . . . .Pretest Questions . . . . . . . . . . . . . . . . . . . . . . . . . 6Pretest Answers. . . . . . . . . . . . . . . . . . . . . . . . . . . .7Key Practice Recommendations. . . . . . . . . . . . . .Preface. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
SECTION ONE The Patient Protection and Affordable Care Act . . 13
Background . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Goals of the PPACA . . . . . . . . . . . . . . . . . . . . . 13Reorganization and Reform
of the Insurance Industry . . . . . . . . . . . . . . 13Health Insurance ExchangesEssential Health BenefitsBenefit TiersPremium Credits and Cost-Sharing SubsidiesPatient/Consumer ProtectionReform in the Public Sector
Expansion of Coverage and Access to Care . . .17Expansion of Public Programs: Medicaid
and Children’s Health Insurance ProgramIndividual Mandates and SubsidiesEmployer Requirements
Quality and Reform of the Health Care Delivery System . . . . . . . . . . . . . . . . . . . . . .
Cost Containment and Taxes . . . . . . . . . . . . .
SECTION TWO Accountable Care Organizations . . . . . . . . . . . . .22
Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22ACOs Compared With Managed Care . . . . . . 22Payment Models . . . . . . . . . . . . . . . . . . . . . . . 22Quality Performance Standards . . . . . . . . . . . 23Concerns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Examples of Success . . . . . . . . . . . . . . . . . . . 26Early Challenges in Implementation . . . . . . . . 27Joint Principles for ACOs . . . . . . . . . . . . . . . . 27
Page
SECTION THREEIncentives for Reform: Pay for Performance. . . . .28
Pay for Performance . . . . . . . . . . . . . . . . . . . . 28Centers for Medicare & Medicaid Services
Pilot ProgramsHospital Value-Based Purchasing Program . . 28Other Pay-for-Performance Programs . . . . . . 28Concerns Amid Potential. . . . . . . . . . . . . . . . .
American Academy of Family PhysiciansOther OrganizationsPhysician PerspectivesPatient PerspectivesOther Perspectives
Evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Outpatient ProgramsHospital Programs
SECTION FOURThe Family Physician and Health Care Reform . 33
The American Academy of Family Physicians and Health Care Reform . . . . . . 33
Patient-Centered Medical Home . . . . . . . . . . .Medicare Physician Payment . . . . . . . . . . . . . 36
The American Medical Association/ Specialty Society Relative Value Scale Update Committee
Health Care Coverage for All . . . . . . . . . . . . . . 37Health Information Technology . . . . . . . . . . . . 37Health Care Research and Quality . . . . . . . . . 37Medical Liability and Reform . . . . . . . . . . . . . 37Health Insurance Consolidation . . . . . . . . . . . 38Changes to Graduate Medical Education . . . 38Translating Health Care Reform for Patients . . 38
References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Online Resources . . . . . . . . . . . . . . . . . . . . . . . .Suggested Reading . . . . . . . . . . . . . . . . . . . . . . . 46Posttest Questions . . . . . . . . . . . . . . . . . . . . . . . . 47Posttest Answers . . . . . . . . . . . . . . . . . . . . . . . . .
* Web sites accessed December 2012

4
PageTables
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 . . . . . . . 16
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Tables and Figures

Information for ReadersFP Essentials™
AAFP FP Essentials™-
FP EssentialsFP Essentials
-
-
FP Essentials --
How to Use FP EssentialsFP Essentials has a Pretest
-
-
How to Obtain CME CreditFP Essen-
tials -
-
--
--
-
-
from the FP Essentials
How to Comment on FP Essentials
FP Essentials
-

6
1.
❏
❏
❏❏ fix to the
❏
2. mandate within the Patient Protection and
❏
❏
❏
❏
3.
❏
❏
❏
❏
4.
❏
❏
❏
❏
5.
❏
❏
❏
❏ of health care systems.
❏
6.
❏
❏
❏
❏
❏
Pretest Questions

7
7.
❏ rate fix
❏
❏medical home as the model of care that
❏
health care.❏
8.
❏
❏
❏
❏
model of care.
Pretest AnswersQuestion 1: The correct answer is E.
-
See page 15.
Question 2: The correct answer is A.
shared responsibility payment. See page 18.
Question 3: The answer is D.
-
See page 22.
Question 4: The correct answer is B.
See page 22.
Question 5: The correct answer is A.
-
See page 29.
Question 6: The correct answer is A.-
See page 32.
Question 7: The correct answer is E.The American Academy of Family Physicians has stated

8
Notice to Subscribers
FP Essentials™
FP Essentials
-FP Essentials materials does not
the AAFP. FP Essentials
-
FP Essentials -
-
FP Essentials™
-
the American Academy of Family Physicians, 11400 Tomahawk Creek Parkway, Leawood, KS 66211-
-
-
-
See page 35.
Question 8: The correct answer is A.-
See page 35.
Pretest Answers

Strength of Recommendation Taxonomy (SORT)
Strength of Recommendation Definition
A a
a
Ca
aPatient-oriented evidence measures outcomes that matter to patients: morbidity, mortality, symptom improvement, cost reduc-tion, and quality of life. Disease-oriented evidence measures intermediate, physiologic, or surrogate end points that may or may not reflect improvement in patient outcomes (eg, blood pressure, blood chemistry, physiologic function, pathologic findings).
(From Ebell MH, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy [SORT]: a patient-centered approach to grading evidence in the medical literature. Am Fam Physician. 2004;69:548-556.)
1. -
2.
3. -
4.
Resources 1. Strength of evidence: SORT C
Source: N Engl J Med. N Engl J Med. Web site:
2. Strength of evidence: SORT CSource: Physician Group Practice (PGP) Demonstration Design Report.
Health Affairs. N Engl J Med.
Web site:
3. Strength of evidence: SORT ASource:
Cochrane Database Syst Rev. Web site:
4. Strength of evidence: SORT CSource: Benefits of Implementing the Primary Care Patient-Centered Medical Home: A Review of Cost and Quality Results, 2012. Web site:
Key Practice Recommendations

Health Care Reform
10
AAFP FP Essentials™ Approved as CME Clinical Content
FP Essentials™ 2013,
-
™

11
PrefaceOn March 23, 2010, President Barack Obama signed the Patient Protection and
Affordable Care Act (PPACA) into law.1 According to most health care policy experts, this was the most comprehensive overhaul of the US health care system since Medi-care and Medicaid were enacted by President Lyndon Johnson on July 30, 1965, as part of the Social Security Act Amendments of 1965.
In July 2012, the PPACA—including some of its more controversial components, such as the individual mandate and the expansion of Medicaid—was upheld in a 5 to 4 Supreme Court ruling. In this decision, Chief Justice John Roberts joined the major-ity in favor of upholding the law. Although there has been ongoing opposition to the PPACA, before and after the Supreme Court decision, individuals and states continue to prepare for the changes that it has enacted and will enact in the near future.
Health care reform is a controversial topic that engenders deeply held opinions in many individuals. This edition of FP Essentials™ attempts to steer clear of politi-cally charged debates, focusing instead on explaining the components of the PPACA, and discussing its implementation and its effect on family physicians, their patients, and their practices. Section One briefly discusses the legislation itself, focusing on the provisions that are most relevant to family physicians. Sections Two and Three discuss accountable care organizations and pay for performance, respectively. Section Four provides an overview of the American Academy of Family Physicians’ official positions on reform of the health care system; it also considers next steps for advocacy efforts. Suggested Reading and Online Resources for updated information are included.
FP Essentials™ 404
Health Care Reform

Health Care Reform
12

13
SECTION ONE
The Patient Protection and Affordable Care Act
Case 1. Theresa, a 38-year-old woman, presents to your office for a routine physical examination. She is a single mother with 2 children and is employed as a cashier at a local delicatessen. Her employer does not offer health insurance, and she cannot afford to purchase it on her own. Her children are covered under the state’s Medicaid program. She tells you that today’s visit will be self-pay. You decide to forego screening lipids and blood glucose because she is at low risk of cardiovascular conditions and diabetes. You counsel her about health maintenance and encourage her to update her vaccinations at the public health department, where it will be less expensive to do so. You also refer her to a local community health center that will provide cervical cancer screening at no cost. After she leaves, you feel frustrated that the fragmented US health care system makes it difficult for an employed single mother to access basic health care.
BackgroundAlthough the majority of Americans recognize the
need for health care reform, there is disagreement about how to accomplish it. Among countries in the Organisation for Economic Co-operation and Development, only the United States, Mexico, and Turkey fail to provide universal health coverage.2 The United States is the only industrialized nation without universal comprehensive health coverage for its citizens.3 In 2011, there were 48.6 million unin-sured individuals in the United States.4 Having such a large population of uninsured individuals leads to poor health outcomes5,6 and puts a burden on the nation’s economy.7 Rapidly increasing health care costs directly affect American employers and families. From 2002 until 2012, the employer contribution to health insurance increased by 97% from an average of $5,866 to $11,429, and the cost for an employee increased by 102% from an average of $2,137 to $4,316.8 It is estimated that by 2030, more than half of the cost of Medicare will be added directly to the federal budget deficit.8 Many health care policy experts, as well as some legislators, have begun to recognize that the provision of universal health care coverage for all citizens may help control costs. The
United States has been ranked 37th in health care system quality, despite spending the highest percent-age of gross domestic product on health care of all industrialized countries.9,10,11
Goals of the PPACAThe goals of the Patient Protection and Affordable
Care Act (PPACA) include12:
insurance industry;
system; and
pay for PPACA initiatives.
Reorganization and Reform of the Insurance Industry
The PPACA initiates new programs, sets new insur-ance requirements, and reforms the existing health care infrastructure. Although some reforms will be implemented over the next few years, several regula-tory initiatives call for immediate reform to existing private benefit plans. In addition, the PPACA insti-tutes health insurance exchanges to change the way in which individuals purchase health insurance.
Health Insurance ExchangesThe primary goals of health insurance exchanges
are 1) to allow individuals and employers to find affordable health insurance plans; 2) to compare premiums and benefits among different plans; and 3) to decrease administrative complexity. Exchanges accomplish these goals by defining what a basic policy includes and reforming the fine print regarding ben-efits and coverage.
Each state is required to offer an exchange for individuals and small businesses; states may opt to combine the 2. Each exchange will be administered by a nonprofit organization or a governmental agency. States may have more than 1 exchange operating within the state or work with other states to form a regional exchange, provided that each exchange serves a distinct geographic area. If a state does not offer a functional exchange by January 1, 2014, the secretary

Health Care Reform
14
of the Department of Health and Human Services will appoint a federal exchange.13
Essential Health BenefitsThe PPACA sets forth 10 categories of comprehen-
sive services, or essential health benefits (EHBs), that must be provided by any insurance plan (Table 1).14,15 According to the law, a state may require its exchange to offer more than these EHBs, but the state is then required to defray the cost of the additional benefits.16,17
On December 16, 2011, Department of Health and Human Services Secretary Kathleen Sebelius announced that the federal government would not define a standardized set of benefits within each of the 10 EHB comprehensive categories required by the PPACA; rather, state exchanges, although required to address all 10 categories, will be given latitude to choose the specific benefits and services that comprise the actual EHBs for their state or region.15 This made what was initially envisioned to be a definitive national benefit package for insurance plans into a national framework, or benchmark, by which the federal gov-ernment can judge the appropriateness of state (and/or regional) decisions regarding the exact services chosen
to define the benefit in each of the 10 categories. The Department of Health and Human Services outlines the mechanism by which states will determine benefits coverage. Critics of this approach are concerned that allowing states to define the scope of specific benefits and set their own quantitative limits might result in inequities in the quality and quantity of health care available to individuals from state to state.18
Benefit TiersTo participate in an exchange, insurance companies
need to design plans that offer the EHBs and conform to certain cost-sharing levels. The PPACA identifies 4 benefit tiers: bronze, silver, gold, and platinum. Insur-ance companies must design a silver and gold plan; designing a bronze or platinum plan is optional.
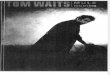
Typically, different levels of health plan coverage are specified in terms of copays and deductibles; how-ever, the PPACA defines levels of coverage using the concept of an actuarial value. The actuarial value is the percentage of total average costs for covered benefits that a plan will cover. This percentage increases as the plan tier progresses from bronze to silver to gold to platinum (Figure 1).19 If a health insurance company’s actuarial value on its gold plan is 80%, then the plan will pay 80% of the costs incurred for a standard pop-ulation covered by that plan. Enrollees would pay the remaining 20% through some combination of copays, deductible, or additional insurance coverage. How-ever, an individual may end up paying more or less than this 20%, depending on the quantity and type of health services used. The PPACA also places an annual limit on an enrollee’s out-of-pocket expenses that matches the limits for health savings accounts and high-deductible health insurance plans. The current limits are $5,950 for an individual and $11,900 for a family; the limits will be adjusted over time after 2014 based on increases in premiums.
Premium Credits and Cost-Sharing SubsidiesIn addition to annual limits on cost sharing, the
PPACA makes provisions for premium credits and subsidies to individuals or families whose income does not allow them to qualify for Medicaid but for whom obtaining insurance is still a significant burden. These premium credits can be thought of as a gift card, redeemable at the time of purchase, that results in a lower-cost insurance policy. Cost-sharing sub-sidies reduce an individual or family’s out-of-pocket
Table 1Essential Benefit Package: The 10 Comprehensive Services
Information from The Patient Protection and Affordable Care Act, §1302(b), 42 USC §18001 (2010).

Section One
expenses; these expenses would instead be covered by the insurance plan.
Using data from 2 Kaiser Family Foundation resources,19,20 Table 2 uses examples to compare plans available across all 4 benefit tiers, with a detailed view of silver plan options. Table 3 provides a more detailed description of what enrolling in a silver plan might entail for a 40-year-old single man and for a family of 4.
Patient/Consumer Protection The PPACA compels the health insurance indus-
try to submit to several patient/consumer protection measures.
Preexisting Conditions. One concern about the current insurance industry is the denial of coverage to individuals with preexisting conditions. Under the PPACA, denying benefits to children with a preexist-ing condition was prohibited as of September 23, 2010. The law prohibits denial of benefits for preex-isting conditions by all insurers for all populations, beginning January 1, 2014. In the meantime, $5 bil-lion has been allocated to fund a high-risk pool to pro-vide insurance for adults with preexisting conditions.21
Rescission. Another routine insurance industry practice with the potential to affect the sickest patients adversely is rescinding coverage. This practice ranges from placing annual and/or lifetime limits on cover-age to rescinding coverage from the highest users. The PPACA prohibits rescission, except in cases of fraud. In addition, lifetime limits on coverage were prohib-
ited as of September 23, 2010. Beginning on January 1, 2014, annual limits are also prohibited.
Medical Loss Ratio. In industry lingo, paying for the health care of an insured patient is called a medical loss. As of 2010, health plans are required to report their medical loss (ie, the percentage of the insurance com-pany’s income from enrollees’ premiums that is spent on clinical services [versus the percentage spent on other expenses, such as marketing or executive pay]).13 As of 2011, health plans in the large group market that do not spend at least 85% of premiums on clinical services are required to provide rebates to their enrollees; plans in individual or small group markets must spend at least 80% of premiums on clinical services.22 Similarly, premium increases will be reviewed by state or federal experts, and unjustified increases will disqualify a health plan from participating in the exchanges.
Reform in the Public SectorCoverage of Preventive Services. Improved cover-
age of preventive services is included in the reform of Medicare and Medicaid under the PPACA. Improve-ments include eliminating out-of-pocket costs (or cost sharing) for Medicare- and Medicaid-covered preven-tive services recommended (by a rating of A or B) by the US Preventive Services Task Force. Clinicians will be reimbursed 100% of the physician fee schedule for providing recommended services.
Medicaid Pays Medicare Rates. Before the PPACA was passed, state Medicaid programs, in efforts to cut
Figure 1. Four Tiers of Health Care Coverage
Information from Henry J. Kaiser Family Foundation. Focus on Health Reform. What the Actuarial Values in the Affordable Care Act Mean. Menlo Park, CA: KFF; 2011. Available at http://www.kff.org/healthreform/upload/8177.pdf.
Illustration courtesy of the University of Alabama Faculty Resource Center.
Bronze Plan
60% covered
Silver Plan
70% covered
Gold Plan
80% covered
Platinum Plan
90% covered

Health Care Reform
16
costs, frequently reduced payment to physicians. In each of the 5 fiscal years from 2003 to 2007, more than 90% of states reduced or froze physician pay-ments for services.23 In almost every state, this led to a situation in which Medicaid pays physicians approxi-mately 72% of Medicare rates.24,25,26 The PPACA attempts to rectify this by requiring state Medicaid agencies to pay 100% of the Medicare rates to primary care physicians by 2013. States will receive federal funding for this payment rate increase. Increasing physician payment is expected to improve access to care for those who are insured by Medicaid, which will ultimately improve health outcomes.27
Sustainable Growth Rate Fix. Currently, Medi-care physician payment rates are set based on the sustainable growth rate (SGR) formula. The formula
is complex and has undergone multiple modifica-tions. Essentially, lawmakers set targets for physician spending, and, when this threshold is exceeded, phy-sician reimbursement is cut across the board. From 1998 to 2001, physicians received payment increases in the range of 2.3% to 5.5%.28 Then, in 2002, the Centers for Medicare & Medicaid Services reduced physician reimbursement by 4.8%, based on the SGR formula. Since that cut and before the passage of the PPACA, Congress has intervened a number of times to temporarily avoid SGR-required payment cuts to physicians.29,30,31,32
Unfortunately, because the formula-based reduc-tions in physician payments are cumulative, perma-nently fixing the SGR would now cost more than $300 billion over the next 10 years.33,34 For this
Table 2Example Comparisons of Plans Across All 4 Benefit Tiers, With a Detailed View of Silver Plan Optionsa
Annual Premium
Monthly Cost
Annual Deductible
Maximum Out-of-Pocket Cost Physician Visit
Prevention Visitb Generic Rx
Emergency Department Hospital Stay
$321$4,000 family
c
$2,000 family
Plan $4,000 family
Plan $2,000 family
Plan
$8,000 family
$4,000 family
$488
aThese numbers are estimates provided for illustration purposes only.bIncluded in large, new menu of health plan benefits for which the insurance company pays 100% of the cost by law.cCBO estimates that a silver plan for a 40-year-old adult would have an annual premium of $4,500.
CBO = Congressional Budget Office; Rx = prescription.
Information from Henry J. Kaiser Family Foundation. . Menlo Park, CA: KFF; 2010. Available at http://healthreform.kff.org/SubsidyCalculator.aspx; Henry J. Kaiser Family Foundation.
. Menlo Park, CA: KFF; 2011. Available at http://www.kff.org/healthreform/upload/8177.pdf.

Section One
17
reason, legislators did not address the SGR in the PPACA. At the time of publication of this FP Essen-tials, the most recent intervention, or doc fix, averted a 27.4% reduction in Medicare physician payment and froze rates through the end of 2012.35
Medicare Bonus Payments for Primary Care. Primary care physicians will receive a 10% bonus payment paid quarterly from 2011 through 2015.13,30 Physicians qualify for this bonus if they are in primary care (ie, family medicine, geriatrics, internal medi-cine, pediatrics) and 60% or more of their Medicare Part B-allowed charges are office-based, nursing home-based, or home visit-based evaluation and management codes; the latter requirement is contro-versial.36,37,38 The Robert Graham Center for Policy Studies in Family Medicine and Primary Care and the
National Rural Health Asso-ciation have expressed concern that this threshold definition penalizes rural and other com-prehensivist family physicians who perform a higher percent-age of inpatient medicine, emergency department cover-age, and office-based proce-dures.39 In addition, the bonus is administered by Medicare Part B, so physicians in rural health centers and federally qualified health centers do not qualify. Basing this desirable incentive on fee-for-service cri-teria also could exacerbate the worst aspects of the volume-driven business existing in the current system.
Expansion of Coverage and Access to Care
The primary ways in which the PPACA expands insur-ance coverage are expansion of public programs, individual mandates and subsidies, and employer requirements.
Estimates from the Congres-sional Budget Office (CBO) indicate that the expansion of public programs will add 16
million enrollees, and the individual mandates and health care exchanges will provide another 16 mil-lion individuals with health insurance, for a total of approximately 32 million newly insured Americans.40 Family physicians must be prepared for an increased demand for primary care services.
Expansion of Public Programs: Medicaid and Children’s Health Insurance Program
Medicaid is a state-based program that provides health insurance for low-income families with state and federal funding. The Children’s Health Insur-ance Program (CHIP) is a program administered by the states to provide health insurance coverage to children without insurance whose family’s income is too high to qualify for Medicaid, but who are unable
Table 2Example Comparisons of Plans Across All 4 Benefit Tiers, With a Detailed View of Silver Plan Optionsa
Annual Premium
Monthly Cost
Annual Deductible
Maximum Out-of-Pocket Cost Physician Visit
Prevention Visitb Generic Rx
Emergency Department Hospital Stay
$321$4,000 family
c
$2,000 family
Plan $4,000 family
Plan $2,000 family
Plan
$8,000 family
$4,000 family
$488
aThese numbers are estimates provided for illustration purposes only.bIncluded in large, new menu of health plan benefits for which the insurance company pays 100% of the cost by law.cCBO estimates that a silver plan for a 40-year-old adult would have an annual premium of $4,500.
CBO = Congressional Budget Office; Rx = prescription.
Information from Henry J. Kaiser Family Foundation. . Menlo Park, CA: KFF; 2010. Available at http://healthreform.kff.org/SubsidyCalculator.aspx; Henry J. Kaiser Family Foundation.
. Menlo Park, CA: KFF; 2011. Available at http://www.kff.org/healthreform/upload/8177.pdf.

Health Care Reform
18
to purchase private insurance.41,42 However, states have broad discretion in setting up their own income eligibility standards.
Under the PPACA, a major gap in coverage will be closed with 2 government-based solutions.21 Medicaid will be expanded, and CHIP, which is set to expire in 2013, will be extended through a requirement that the states must extend its funding through 2015 and maintain current eligibility criteria through 2019.43,44 This could result in approximately 16 million new Medicaid and CHIP enrollees by 2019, according to CBO estimates. A recent study conducted by the Har-vard School of Public Health showed that as many as 22.4 million individuals could be added to Medicaid by 2019.45 If this study is correct, by 2019, Medicaid
and CHIP will surpass Medicare as the largest insur-ance payers in the country.46 Beginning in 2015, any child eligible to enroll in CHIP who is unable to do so because of enrollment caps will be eligible to receive tax credits in the exchanges.13,47
One of the most hotly debated—and sometimes misunderstood—aspects of the Medicaid expansion provisions is the status of undocumented immigrants. The PPACA does not change existing law; undocu-mented immigrants remain ineligible for Medicaid.
One aspect of the Medicaid expansion was at the center of the Supreme Court’s decision on June 28, 2012.48 Although the Court upheld the expansion of Medicaid, it ruled that it is unconstitutional for the federal government to penalize states for not com-
plying with this expansion of Medicaid eligibility and services. Because states are no longer at risk of losing existing Medicaid funding for state programs, they have more flexibility in choos-ing whether to expand Medicaid services. States that comply are given increased funding by the federal government with addi-tional conditions and restric-tions in place. States that choose not to expand will forego any additional monies from the federal government.49
Individual Mandates and Subsidies
Many individuals do not have an employer-covered health insurance plan or qualify to enroll in Medicaid or CHIP. Under the PPACA, these indi-viduals are required either to purchase a qualifying insurance policy in the exchange or to pay a shared responsibility payment.
It is important to understand the choices made by legislators and the president’s administra-tion in context. Without an individual mandate, there are limited options for achieving universal coverage in the exist-
Table 3Case Examples of Benefit Tiersa
Case 1.
(Table 2). His
Case 2.
(Table 2).
aCase examples are based on 2014 dollars, when the subsidies/tax credits take effect, and calculated with the Kaiser Family Foundation calculator (http://healthreform.kff.org/SubsidyCalculator.aspx).
CBO = Congressional Budget Office; EHB = essential health benefits; PPACA = Patient Protection and Affordable Care Act.

Section One
ing US health care system without resistance from the health insurance industry. The industry position is that a mandate is needed to balance the lower profit margins that result from the enhanced regulations in the PPACA (eg, ending rescission and denial for pre-existing conditions, limiting the medical loss ratio).
New regulations make providing health insurance coverage a more expensive and less profitable endeavor, and, without the mandate, there would be nothing pre-venting individuals from waiting until they become ill to buy insurance.50,51,52 Effectively, the individual man-date and other requirements of the PPACA provide 16 million new customers to help defray the increased expense of complying with new regulations.
The individual mandate was one of the most con-troversial parts of the health care reform debate. The constitutionality of this portion of the legislation was at the center of the debate in National Federation of Independent Business v. Sebelius.53 In his opinion, Chief Justice John Roberts stated that the individual mandate exceeded congressional authority under the Commerce Clause, noting, “Congress has never attempted to rely on [this] power to compel individuals not engaged in commerce to purchase an unwanted product.”49 Although the PPACA characterizes the shared respon-sibility payment required of individuals who do not comply with the individual mandate as a penalty, not a tax, the Supreme Court found the individual mandate constitutional on the grounds that it is a valid exercise of the federal government’s power to tax.
Employer RequirementsAlthough no law required businesses to provide
health insurance to their employees before the PPACA, since 1999, 97% to 99% of businesses with 200 or more employees have provided some form of health benefits.54 As far back as the 1960s, three-fourths of the US population was covered by some sort of private, employer-based insurance.55 Premi-ums for family coverage continue to increase, as do employer and employee contributions to the health care plans, which is financially challenging for families and corporations alike.54,56,57,58
Just as the PPACA requires individuals to purchase a health plan or pay a penalty, employers with 50 or more full-time employees are assessed penalties if they do not offer an affordable health plan to their employ-ees; businesses with fewer than 50 full-time employees are exempt from the new requirements and penalties.
This law has the potential to have a major effect on the employer-based coverage market; its effect on an individual employer depends primarily on the size of the business and what coverage the employer currently provides to employees (Figure 2 and Table 4).
Quality and Reform of the Health Care Delivery System
The effort to reform and reorganize the exist-ing health insurance industry, while also expanding coverage and access to care, will have a major effect on the US health care system. The PPACA also aims to reform the way that health care is delivered, with a focus on improving quality through such measures as accountable care organizations (see Section Two), pay for performance (see Section Three), and the National Strategy for Quality Improvement in Health Care, which establishes goals, including improving overall quality of care, improving the health of the US popu-lation, and reducing the overall cost of health care.59
The Center for Medicare and Medicaid Innovation established the Partnership for Patients: Better Care, Lower Costs, a program aimed primarily at coopera-tive efforts to reduce hospital-acquired conditions and to improve the transition from inpatient care to out-patient care. In addition, under the Comprehensive Primary Care Initiative, the Centers for Medicare & Medicaid Services will pay participating primary care physicians and practices a monthly care management fee for providing comprehensive care management (eg, personalized preventive care plans, shared deci-sion making in chronic disease management, 24-hour access to care and information) to Medicare fee-for-service beneficiaries.60
Funding for innovation and effort in care coordi-nation for dual eligibles (ie, patients who qualify for Medicare and Medicaid), which can be complicated, also is planned.
Cost Containment and TaxesThe CBO, which is a nonpartisan entity charged
with estimating the cost of, or scoring, each piece of legislation before Congress, estimates that the cover-age components of the PPACA will have a gross cost of $934 billion from 2012 through 2019.61 However, because of predicted Medicare and Medicaid savings, as well as new taxes and fees, the CBO estimates that the law will reduce the total budget deficit by $119 billion from 2012 to 2019. Because the enactment of

Health Care Reform
20
Figure 2. Flowsheet for Businesses Navigating the MandatesReprinted from Henry J. Kaiser Family Foundation.
Menlo Park, CA: KFF; 2012. Available at http://healthreform.kff.org/the-basics/employer-penalty-flowchart.aspx.
If the employer has 25 or fewer employees and average wage up to $50,000, it may be eligible for a health insurance tax credit.
The penalty is $2,000 annually times the number of full-time employees minus 30. The penalty is increased each year by the growth in insurance premiums.
The penalty is $3,000 annually for each full-time employee receiving a tax credit, up to a maximum of $2,000 times the number of full-time employees minus 30. The penalty is increased each year by the growth in insurance premiums.
Start here.
Those employees can choose to
buy coverage in an exchange and
receive a premium tax credit.
Do any employees have to pay more
than 9.5% of family income
for the employer coverage?
The employer must pay a penalty for not offering
affordable coverage.
The employer must pay a penalty for not offering
coverage.
Employees can choose to buy coverage in an exchange and
receive a premium tax credit.
Does the insurance pay for at least 60% of covered health
care expenses for a typical population?
Did at least 1 employee receive a premium tax credit
or cost-sharing subsidy in an exchange?
Does the employer offer coverage to
its workers?
There is no penalty payment required of the employer since it offers
affordable coverage.
Penalties do not apply to small
employers.
Does the employer have at least 50
full-time equivalent employees?
No
Yes
YesNo
No
Yes
Yes
No
Yes

Section One
21
various provisions of the law is staggered, the CBO also evaluated the effect of the PPACA from 2012 to 2021; it estimates a $210 billion decrease in the deficit over this time period.
To cover the remaining costs of the PPACA, addi-tional revenue will be generated by tax changes related to providing health insurance and financing health care reform, changes in flexible spending accounts, changes to tax rates for deducted medical expenses, and new annual fees imposed on the pharmaceutical and health insurance industries.
Case 1, cont’d. Theresa returns to your clinic in June 2014 for a routine physical examination. She is still employed at the delicatessen, where she has been promoted to an assistant manager. She is now insured through a health care exchange, and her benefits include all of the recommended preventive health care services. She is able to receive all services, including cancer screen-ing, laboratory testing, and vaccinations, through your practice because they are all part of her plan’s essential health benefits.
Table 4Effects of the Mandate on Small Businesses of Different Sizes
Rural Hospital
Real Estate Firm
Local Lumber Mill
Accounting Firm
160 160
60 140 30
$180,000 $420,000
$260,000 $260,000
If businesses with more than 50 full-time employees are currently providing health insurance, but the plan does not cover, on aver-age, at least 60% of health care expenses (ie, equivalent to a bronze plan), or the employee’s portion of the premiums is more than 9.5% of household income, then the employee can opt out of the employer plan and participate in the exchanges (see ). In this scenario, if 1 or more full-time employees receive a premium tax credit or cost-sharing subsidy, the employer is required to pay the lesser of the following annually: $3,000 for each full-time employee receiving a premium tax credit $2,000 for each full-time employee, minus the first 30 employees
FPL = federal poverty level.
Information from Henry J. Kaiser Family Foundation. . Menlo Park, CA: KFF; 2011. Available at http://www.kff.org/healthreform/upload/8061.pdf.

22
SECTION TWO
Accountable Care OrganizationsCase 2. The medical director of your multispecialty
primary care practice has asked all physicians to attend an informational meeting about accountable care organiza-tions (ACOs). There has been discussion about whether your practice will try to qualify as an ACO. You anticipate that input will be solicited at this meeting, and you want to have a better understanding of ACOs before the meeting.
OverviewHealth care in the United States, for all its achieve-
ments and innovations, is often fragmented and uncoordinated, overemphasizing intervention and underemphasizing—and underfunding—prevention and the management of chronic disease.62,63 Inefficien-cies, wasteful duplication of services, and disparate goals and incentives have led many experts to refer to the US health care system as a nonsystem.64,65
The concept of an accountable care organization (ACO) was introduced in the course of discussions regarding unsuccessful attempts to coordinate the health care system as a whole and manage its many component parts.66,67 According to the Centers for Medicare & Medicaid Services (CMS), ACOs are groups of physicians, hospitals, and other clinicians who voluntarily partner to coordinate high-quality health care for Medicare patients.68,69 The goal of these partnerships is to provide patient-centered, coordinated, evidence-based, quality care to the right patients—especially the chronically ill—at the right time, while avoiding errors and duplication of services.
The goals of an ACO are consistent with what is often called the triple aim of improving health care: improving the experience of care, improving the health of populations, and reducing per capita costs of health care.70 When an ACO is successful in providing high-quality care, enhancing patient safety, and spend-ing health care dollars more wisely, it is rewarded with a share of the Medicare savings.68
Although the idea of broader medical partner-ships being accountable for coordinating health care delivery for quality enhancement and cost savings66 was initially proposed in 2006, ACOs primarily began to receive attention after the passage of the Patient Protection and Affordable Care Act (PPACA).
ACOs Compared With Managed Care
Previous initiatives in managed care, such as independent practice associations, physician-hospital organizations, and health maintenance organizations, may sound similar to ACOs. However, although there are some similarities between ACOs and the managed care organizations of the 1980s and 1990s, the differences are striking enough to offer the pos-sibility that ACOs can achieve a different outcome than previous efforts.
In ACOs, instead of insurance companies being held accountable for outcomes and cost, the accountability lies with the clinicians. Physician participation in the ACO is voluntary and does not require the physician to contract with any other health plan or intermedi-ary. Arguably, one of the biggest differences between ACOs and other managed care organizations is that ACOs have financial flexibility in how participating clinicians are compensated.
In addition, in an ACO, the Medicare beneficiary does not enroll in the ACO. If the patient’s primary care physician joins an ACO, then the patient is con-sidered a member of the ACO for the purposes of data collection for quality measurements and cost report-ing. Each beneficiary can opt out of the ACO, which essentially means finding another physician who is not in the ACO.
Unlike the managed care organizations of the 1980s and 1990s, ACOs are able to take advantage of emerging technologies to monitor the quality of the care delivered. Information technology (ie, electronic health record systems) offers improved efficiency for tracking payment and outcomes.
Payment ModelsIn the traditional fee-for-service arrangement
between hospitals, practices, or physicians and Medicare (or any fee-for-service insurer), the driv-ing financial incentive is volume. The more services rendered, the more money the hospital, group, or phy-sician makes. The way the health care system is set up, volume is often rewarded more tangibly than quality or outcomes.
Consider the typical metrics used in hospital and practice settings. Hospitals track their average daily cen-

23
Section Two
sus and propose various courses of action to fill inpa-tient, rehabilitation, and nursing home beds. Family medicine practices typically know how many patients are seen per day, per clinician, and, in some cases, per insurer, and practices are sometimes judged by quality metrics, such as the percentage of patients receiving influenza vaccines. Hospitals and family medicine prac-tices experience the effects of variables that can affect their metrics, such as a winter with a bad influenza sea-son (eg, markedly increased visit counts and inpatient admissions), or a winter relatively devoid of influenza when acute care appointment slots go unfilled.
In the era before the recent quality reporting initia-tives, it was rare for most hospitals and practices to have readily available information on the percentage of patients who received the influenza vaccination. This is 1 example of the health care system’s empha-sis on focusing on and paying for disease manage-ment rather than focusing on and paying for disease prevention. Although the value of preventive care is espoused readily by clinicians and institutions, with the historical focus on volume instead of outcomes or other quality metrics, this type of data was not tracked as closely.
There is a continuum of measures and incentives in the financial redesign of health care delivery, rang-ing from traditional fee-for-service models to full capitation plans. These plans also include bonuses for achieving quality measures (eg, pay for performance)
or financial measures (eg, shared savings), as well as penalties for not meeting quality or financial thresh-olds (Figure 3).
The Pioneer ACO Model was developed by CMS to test different payment models in organizations that already operate like an ACO and are experienced in providing coordinated patient care.71 Currently, 32 organizations have been chosen to participate. The Medicare Shared Savings Program requires participa-tion in an ACO and seeks to promote care coordina-tion, lower costs, and higher quality.72 The Advance Payment ACO Model, also established by CMS, is focused on providing up-front money to help smaller organizations participate in the shared savings pro-gram (Table 5).73
Quality Performance StandardsQuality benchmarking for ACOs will be derived
from claims data for an ACO’s Medicare beneficia-ries. Quality measures used to assess ACOs will align with existing quality initiatives (Table 6). The Physi-cian Quality Reporting Initiative has been extended and systematized as the Physician Quality Reporting System, which is a form of pay for performance that financially rewards physicians for reporting on certain quality measures. Physicians will be able to report data through electronic health records, as well as through registry options, such as those available on the Ameri-can Board of Family Medicine Web site (https://www.
theabfm.org/moc/pqrs.aspx).This payment reform can
be good news for physicians and organizations that already are measuring cost and quality issues. To receive shared savings, a Medicare ACO must meet 33 quality standards through report-ing the measure or meeting a performance standard, according to CMS.1 In year 1, reporting on the quality measures is the only requirement; however, in years 2 and 3, there are increased expec-tations for meeting standards. Twenty-five of the 33 measures are incentivized in the 2nd year, and 32 of 33 are incentivized in the 3rd year (Table 7). To receive bonus payments throughout the
Figure 3. Continuum of Measures and IncentivesIllustration courtesy of the University of Alabama Faculty Resource Center.

Health Care Reform
24
3-year phase-in, physicians or hospitals must reach a minimum attainment level of 30% of the standard benchmarks. Maxi-mum points (and payments) are attained at the 90% threshold.
Commercial ACOs organized outside of CMS may have separate requirements, differ-ent timeframes, and a different shared savings model than the Medicare ACOs, but all ACOs have the same underlying theme of coordinating services to provide higher quality care at a lower cost.1
ConcernsIn response to the initial pro-
posed rule for ACOs released by CMS in March 2011, multiple organizations—including the American Academy of Fam-ily Physicians, the American Medical Association, and the American Medical Group Association—expressed con-cerns about implementation. The American Medical Group Association—which represents organizations that were assumed to be likely early adopters, such as the Mayo Clinic—reported that 93% of its members would not enroll in an ACO unless the rules changed.74
The primary concerns were that ACOs forced physicians to bear too much perfor-mance risk for the cost of their patients and that they had the potential for placing too many demands on practices that were already struggling or had less experi-ence coordinating care. Under the proposed rule, if practices were unable to manage costs of consultations, imaging, laboratory tests, and other patient services adequately, they would then owe Medicare the amount of money spent that exceeded the ACO’s benchmark.1
In response, in October 2011, the final rule for ACOs addressed these concerns by stating clearly that Medicare, not the ACO, assumes all the insurance risk
(ie, the responsibility for paying claims for services furnished to Medicare beneficiaries). In addition, the Pioneer ACO Model was created to allow larger inte-grated health delivery systems to participate in a more streamlined way.75
The final rule for ACOs also provided time and additional resources to help small to medium prac-tices convert their administrative and health records processes so they comply with CMS regulations. To remove the performance risk that ultimately will be involved in enrolling in an ACO, the final rule allowed ACOs to choose between a shared savings-
Table 5Initial ACO Options From CMS
Program Description
a
aDesigned and refined by CMS in response to comments on the proposed rule on the Medicare Shared Savings Program. Two types of ACOs are eligible to participate: 1) an ACO that does not include any inpatient facilities AND has less than $50 million in total annual revenue; and 2) an ACO with less than $80 million in total annual revenue in which the only inpatient facilities are critical access hospitals and/or Medicare low-volume rural hospitals.
ACO = accountable care organization; CMS = Centers for Medicare & Medicaid Services.
Information from Advance Payment ACO Model. Centers for Medicare & Medicaid Ser-vices Web site. Available at http://innovations.cms.gov/initiatives/aco/advance-payment/index.html; Pioneer ACO Model. Centers for Medicare & Medicaid Services Web site. Available at http://innovations.cms.gov/initiatives/aco/pioneer; Medicare Shared Savings Program. Centers for Medicare & Medicaid Services Web site. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/index.html.

Section Two
only model and a 2-sided model for the first 3-year enrollment period.76
Many organizations were concerned about running afoul of Stark regulations or federal antitrust laws related to large mergers in smaller markets. For exam-ple, a successful ACO in a rural area might involve most physicians and hospitals in that region, thereby inhibiting competition for services. In response to this concern, the Center for Medicare and Medicaid Inno-vation, which oversees the implementation of ACOs, has worked extensively with the Department of Justice, Federal Trade Commission, Internal Revenue Service, and Department of Health and Human Services Office of the Inspector General, all of which released policy statements that provide guidance for ACOs.77
According to the Department of Justice/Federal Trade Commission final statement on antitrust enforcement regarding ACOs, a shared savings pro-gram ACO is given leeway to serve patients of private insurers and Medicare as long as the ACO is com-pliant with CMS legal, administrative, and clinical
processes.78 CMS, in turn, has relaxed many of the regulations that have prevented some physicians and hospitals from collaborating to the extent required by the shared savings program and other ACO proposals.
For example, a new ACO that accounts for less than 30% of a particular market would be free from antitrust suspicion unless it engages in deliberately anticompetitive behavior.79 For a larger ACO (ie, accounting for more than 30% of a market), the Department of Justice/Federal Trade Commission and CMS combined rules potentially would allow collabo-ration, to be determined on a case-by-case basis after a 90-day period to evaluate whether the ACO violates antitrust laws. Even in rural areas, where there is more risk of truly limiting competition by forming partner-ships and networks, ACOs will be given additional exemptions from antitrust prosecution, as long as certain regulations are followed.
Initially excluded from participation in the PPACA’s version of the ACO program, rural health clinics were included in the final rule. Rural physicians may need
to collaborate with larger, more urban health care systems to form a robust ACO.80 Beyond antitrust considerations, rural physicians and hospitals face unique challenges to participa-tion in an ACO, primarily in terms of having the resources to meet all of the requirements. Ongoing advocacy efforts call for policy makers to develop performance measures that are relevant to rural practices and provide these practices with the necessary technical assistance.
One of the challenges of ACO implementation is the complex-ity inherent in changing any ele-ment of the health care system. With major health care initia-tives, change is often slow and requires additional assistance. For example, many new pay-ment methods are being intro-duced (eg, bundled payments) as a means of paying ACO participants for their services. Implementing these new meth-
Table 6Quality Initiatives and Definitions
Quality Initiative Definition
PQRS
CMS = Centers for Medicare & Medicaid Services; HEDIS = Healthcare Effectiveness Data and Information Set; NCQA = National Committee for Quality Assurance; PQRI = Physician Quality Reporting Initiative; PQRS = Physician Quality Reporting System.
Information from various sources.

Health Care Reform
26
ods might involve unanticipated challenges that require additional assistance or reworking. A 2011 study of the initial road test of a bundled payment pilot project showed that after 3 years of implementing systems and processes to support this payment model, none of the pilot participants had made a bundled payment.81 The authors concluded that changing health care is difficult and can take longer than anticipated.
Examples of SuccessBecause ACOs are held accountable for the cost
and quality of the full continuum of care delivered to a group of patients, industry observers are interested in how this model will be implemented within the Medicare program. This model already operates in the private sector; commonly cited examples include Kai-ser Permanente, Mayo Clinic, and Cleveland Clinic.
Table 7Quality Measures for ACOs
Better Care for Individuals
(only reporting in years 1-3)
(only reporting in years 1 and 2; P4P by year 3)
Better Health for Populations
ACE = angiotensin-converting enzyme; ACO = accountable care organization; ARB = angiotensin receptor blocker; CAD = coronary artery disease; EHR = electronic health record; GPRO = group practice reporting option; Hb = hemoglobin; LDL = low-density lipo-protein; LVSD = left ventricular systolic dysfunction; P4P = pay for performance.
Adapted from Quality Measurement & Health Assessment Group. . Baltimore, MD: Centers for Medicare & Medicaid Services; 2011. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Pay-ment/sharedsavingsprogram/Downloads/ACO_QualityMeasures.pdf.
Better Health for Populations (continued)
(only reporting in years 1 and 2; P4P by year 3)
(only reporting in years 1 and 2; P4P by year 3)
(only reporting in years 1 and 2; P4P by year 3)
(only reporting in years 1 and 2; P4P by year 3)
(only reporting in years 1 and 2; P4P by year 3)
(only reporting in years 1 and 2; P4P by year 3)

27
Section Two
These organizations allow physicians to work together to improve quality and efficiency (eg, through devel-opment of and adherence to practice guidelines). In these systems, salaried pay has helped to remove incentives to drive up volume, as seen in fee-for-ser-vice models. Organizations that meet agreed-on per-formance goals are rewarded financially to encourage further steps to improve care management, thereby encouraging a steady evolution into fully coordinated care systems.82
As of 2011, at least 8 private health insurance plans had entered ACO agreements with physicians using a shared risk payment model in which physicians are eligible for bonuses when costs are kept below a certain threshold, but are at risk of financial penalties for exceeding spending targets.82 An estimated 27 private health insurance plans had entered into shared savings contracts that make physicians eligible for bonuses but do not put them at financial risk. Other private ACO arrangements use partial capitation, a payment model in which physicians receive preset payments per patient, as well as payments based on actual services provided.
Early Challenges in ImplementationImplementing an ACO may uncover unforeseen
challenges and barriers, such as inadequate risk management capacity within the organization, lack of organizational structure to support care coordination, or inability to balance interests and engage stakehold-ers (eg, hospitals, primary care physicians, subspe-cialists) in creating governance and management processes. Other challenges include choosing among the many different types of payment models (some of which include financial risks), using the electronic health record to maximal advantage, reporting perfor-mance measures, and implementing standardized care management protocols. Although strategies exist for addressing each of these challenges, because each ACO is unique, general strategies may not be implemented easily. ACOs are in relative infancy in their develop-ment and implementation.82,83
The results of the Physician Group Practice Dem-onstration, a 5-year CMS project that created a partnership between numerous physician practices to better coordinate care across different health care set-
tings, showed that ACOs can improve the quality of care they deliver, but might have difficulty generating savings.84 Only half of the practices in the demonstra-tion were able to exceed a 2% savings threshold after 3 years, leading to concern that it will be challenging for ACOs to reduce spending growth meaningfully. How-ever, this result is not necessarily surprising given the fact that the current fee-for-service payment system penalizes physicians for doing what this demonstration required (ie, reducing the volume of services through better care coordination).82
Although Medicare Shared Savings Program con-tracts initially will extend only 3 years, ACOs that meet performance standards will be able to renew these contracts. With the ACO program operational, organizations will be motivated to change their under-lying business model because these changes might result in greater cost savings in the future.
According to CMS estimates, the Medicare Shared Savings Program will generate up to $940 million in net federal savings in its first 4 years if 270 ACOs sign up to participate.85 As the program progresses, more data will become available to evaluate the success of this program and its ability to attract provider inter-est in the ACO model. Once the program has been in place for a few years, data and experience will inform best practices for using ACO-type payment arrange-ments to improve quality and reduce costs.
Joint Principles for ACOsOn November 19, 2010, the American Academy
of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, and the American Osteopathic Association, represent-ing approximately 350,000 physicians, agreed on 21 joint principles for accountable care organizations as prerequisites for their support of ACOs.86 The joint principles are available on the American Col-lege of Physicians Web site (http://www.acponline.org/advocacy/where_we_stand/other_issues/aco-principles-2010.pdf). These joint principles include the administrative structure and payment system of ACOs. They are based on the assertion that primary care and the patient-centered medical home must serve as the foundation of any accountable care effort.

28
SECTION THREE
Incentives for Reform: Pay for Performance
Case 3. The first item on today’s agenda at your hospi-tal’s medical staff meeting is standardized care of hospital-ized patients with pneumonia. The first attachment is a standard order set, and the second is a protocol for pneumo-nia management that is several pages long. As you review the material in the packet, you find an estimate of the financial penalties the hospital could face if Medicare stan-dards are not met. It is a large amount, which highlights the importance of implementing a standardized approach.
Pay for Performance Pay for performance (P4P) is a reimbursement
model designed to tie payments and incentives to the quality of care provided rather than to the quantity of care provided, as with the current fee-for-service model. Various financial incentives reward physicians or practices for achieving a range of objectives, includ-ing improved clinical outcomes, enhanced health care delivery efficiencies, improved quality, and improved overall patient safety.87 The concept of P4P predates the passage of the Patient Protection and Affordable Care Act (PPACA), although the law does provide for some specific P4P programs (eg, the Hospital Value-Based Purchasing Program).
Centers for Medicare & Medicaid Services Pilot Programs
The Centers for Medicare & Medicaid Services (CMS) launched 2 P4P pilot projects. One was the Premier Hospital Quality Incentive Demonstration, in which 216 hospitals completed a 6-year program focused on meeting quality indicators in several areas of acute care, including medical (eg, pneumonia) and surgical (eg, hip replacement) care.88 Incentive pay-ments were provided under several different categories, including demonstrated improvement, attainment of quality standards, and top performance. The average composite quality score for all process and outcome measures improved over the 6-year project.
The second pilot was the Physician Group Practice Demonstration, a 5-year project that approximated how an accountable care organization (ACO) might function.89 The demonstration involved 10 physi-
cian practices and focused on performance measures in 4 clinical areas: diabetes, congestive heart failure, coronary artery disease, and preventive services. The financial incentives were up to 80% of shared savings, in addition to traditional Medicare fee-for-service payment. Performance incentives were determined on the basis of cost savings and performance on quality measures, which were phased in over the course of the project. As quality measures were added, the portion of the incentive based on quality increased; ultimately, 50% of the performance payment was for cost effi-ciency and 50% was for meeting quality benchmarks. Starting in year 1 and continuing through year 5, all practices met some or all of the performance stan-dards. By year 5, only 4 of the 10 practices earned incentive payments from shared savings.
Hospital Value-Based Purchasing Program The purpose of the Hospital Value-Based Purchasing
Program is to support Medicare payments to hospitals that meet or exceed performance standards on quality measures.90 This P4P-style program is implemented by CMS and is designed to improve quality and efficiency at hospitals across the country. Data on select qual-ity measures and outcomes, beginning with patients discharged on or after October 1, 2012, are being collected to serve as the basis for providing incentive payments to hospitals that meet or exceed goals. CMS selected quality measures from the 45 measures that were part of the Hospital Inpatient Quality Reporting Program for fiscal year 2011 (Table 8).
Skilled nursing facilities, home health agencies, and ambulatory surgical centers are also included in this program. Ineligible hospitals include rehabilitation, psy-chiatric, or children’s hospitals, certain cancer research and treatment facilities, and long-term care hospitals.
Other Pay-for-Performance Programs Case 4. You represent your practice on your health care
organization’s compensation committee. Starting next year, a portion of physician salary will be based on how well the practice is performing on certain quality indica-tors. You feel confident that you provide quality care to your patients, but you wonder how factors, such as patient nonadherence to diabetes management or vaccine refusal,

Section Three
will hurt you financially. You also have to explain this new incentive program to your practice partners.
Pay-for-performance programs have been imple-mented widely throughout the United States, as well as internationally, and include federal, public, private, and payer-funded programs.91 As of 2010, more than 150 programs have been implemented in the United States.92,93 The National Committee for Quality Assurance developed the most widely used measures of health care quality, the Healthcare Effectiveness Data and Information Set.94 As of 2009, 90% of managed care plans in the United States use these measures.90 The largest health care system in the United States has modified these measures to
assess 7 areas within its system: preventive clinical health, chronic clinical health, acute clinical health, patient experience/satisfaction, information systems (systemness), coordinated diabetes care, and effi-ciency.91,95,96 These areas include specific biomarkers for diabetes and cardiovascular care (eg, hemoglobin A1c [HbA1c] and blood pressure levels ), as well as delivery of care via electronic methods to improve communication and patient adherence.
There is great variety among the targeted health care goals and incentives, depending on a physician’s area of practice (eg, primary care, hospital-based care, subspecialty care). Most commonly, P4P programs include increased or decreased payments for physicians
based on performance, or individual physician versus group incentives; they also typically include incentives for achieving a specified goal within a category. Most of the largest health care systems in the United States use some form of P4P measures.97,98,99
Concerns Amid Potential
American Academy of Family Physicians
The American Academy of Family Physicians (AAFP) has long advo-cated multiple reforms in physician payment, including P4P. The AAFP advocates programs that adhere to 7 principles87:
-ity of care;
patient relationship;
that are based on evidence-based clinical guidelines;
physicians in the design of the program;
and scientifically valid;-
tives; and
Many organizational and technical challenges, as well as legal and ethi-
Table 8Hospital Value-Based Purchasing Program Quality Measures
ordered
CAP = community-acquired pneumonia; PCI = percutaneous coronary intervention.
Information from Centers for Medicare & Medicaid Services. Fact sheet: CMS pro-posals to improve quality of care during hospital inpatient stays. Appendix D. April 24, 2012. Available at http://www.cms.gov/apps/media/press/factsheet.asp?Counter=4346&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=false&cboOrder=date; Hospital value-based pur-chasing: measure explanations. Healthcare.gov Web site. Available at http://www.healthcare.gov/news/factsheets/2011/04/valuebasedpurchasing04292011b.html.

Health Care Reform
30
cal dilemmas, exist in the design and implementation of P4P programs.
Other OrganizationsOther organizations have weighed in on P4P (or
pay for outcomes), including The Joint Commission, which articulates essential elements for successful pay-ment reform (Table 9).100
In various position papers, the American Medical Association, the American Academy of Pediatrics, and the American College of Physicians have expressed support for P4P programs that follow principles similar to those outlined by the AAFP, including improvement in quality of care, use of performance measures based on evidence-based guidelines, support for the physician-patient relationship, and voluntary
physician participation.101,102 Other guidelines include access as a performance measure.103 The American College of Physicians specifically cautions against focusing on individual aspects of disease for perfor-mance measures, recommending an approach that considers the whole patient. Finally, the AAFP and the American Medical Association have discussed the ethical implications of systems that reward selection of only the healthiest patients.87,101
Physician PerspectivesA recent systematic review analyzed physician per-
spectives on P4P programs and identified 4 primary attitudes among supporters of P4P104:1) when the P4P measures are accurate, physicians should be given financial incentives for quality; 2) financial incentives are an effective way to improve health care quality; 3) the benefits of P4P outweigh potential risks; and 4) financial rewards are more effective than nonfinancial rewards (eg, peer recognition). Physicians critical of P4P programs primarily focused on 4 themes: 1) P4P is not an effective way to improve quality; 2) P4P measures might not accurately capture the quality of care; 3) P4P is imposed and managed externally, which potentially infringes on physician autonomy; and 4) P4P might be used to exert increased govern-mental control over the practice of medicine.
Patient PerspectivesIn 2004, England introduced a voluntary, national
P4P program for primary care physicians called the Quality and Outcomes Framework. In 2012, patients from 15 practices across England were queried about their perspective on this P4P program.105 The major-ity of patients were not aware that such a program existed, and many had not observed any specific effect on care. Some patients had noticed changes to care (eg, increased use of computers, preventive health reminders), and these changes were viewed positively. Many patients did not understand why physicians were receiving a bonus for doing what the patients considered to be simple things; some were concerned that the program would cause physicians to neglect areas that were not incentivized.
Other PerspectivesOne discussion of the unintended consequences of
the P4P model106 uses the framework of the 10 profes-sional responsibilities of a physician articulated in the
Table 9 Essential Design Principles for a Successful P4O Payment Reform
P4O = pay for outcomes.
Reprinted from Averill RF, Hughes JS, Goldfield NI. Paying for outcomes, not performance: lessons from the Medicare Inpatient Prospective Payment System. Patient Saf. 2011;37(4):185.

31
Section Three
American College of Physician’s charter on medical professionalism.107 From this, 4 ethics themes emerge.
First, quality measures should be based on consen-sus guidelines rigorously developed from unbiased and valid scientific evidence. Failure to do this undermines the impetus for P4P: improved quality. Second, in the physician-patient relationship, there must be hon-esty and transparency about the financial incentives involved in P4P models. Full disclosure is recom-mended, as are assurances of confidentiality in the transmission of patient data.
Third, P4P programs should not engender competi-tiveness or secrecy among physicians. Models that are developed in isolation rather than through collabora-tion or that reward only top tier performers run coun-ter to principles of medical ethics, professionalism, shared scientific knowledge, and camaraderie. Finally, and perhaps most critically, physicians should strive for equity and social justice for all patients. If patient populations that are medically or sociodemographi-cally complex are less likely to meet quality targets, P4P programs might affect physician willingness to provide care for these populations. A physician’s per-formance might not be scored accurately if individual physician data are reported without accounting for variability in clinical and socioeconomic case mix.106
It remains unclear how P4P programs affect physi-cian behavior and motivation, particularly consider-ing their heterogeneity.106,107,108 Some contend that the financial incentives of P4P might undermine a physician’s traditional motivation to provide qual-ity care, role as the leader of the health care team, or commitment to patients. It also has been argued that because a physician’s work is complex and multidi-mensional (ie, not just a single set of tasks), P4P may undermine the very results it is intended to achieve. Another approach has been recommended in which physicians are paid fairly, have the ability to influence patient outcomes, and receive recognition and a sense of accomplishment for the work they do.
In a 2007 study, claims data for Medicare benefi-ciaries were examined to determine who provided fee-for-service care, the proportion of care provided to a patient by the assigned primary care physician or practice, and the stability of assignments to a physician or practice over time.109 This study showed that care for Medicare beneficiaries is dispersed among multiple physicians, which limits the ability of any 1 physician to affect quality measures for assigned patients.
Administrative or accounting errors might unfairly influence P4P. A study in the United Kingdom that evaluated the Classification of Diabetes project showed that miscoding accounted for errors in out-come measures used to determine the quality of diabe-tes care.110 Patients misdiagnosed with type 2 diabetes because of a coding error were shown to have excellent control, with a mean HbA1c of 5.3%, compared with 7.2% for patients who were correctly diagnosed with type 2 diabetes. In addition, patients who were mis-coded and left off of the P4P register tended to have worse control overall, with a mean HbA1c of 8.1%. These findings, although limited to a specific popula-tion, highlight the challenge of ensuring that data are accurate and valid.
EvidenceEvaluation of the available data on the success or
effect of P4P programs is limited by heterogeneity of programs, which precludes systematic comparison. Some of the key differences include:
measured;
change, a process improvement, or an outcome measure;
global patient outcome or a proxy measurement (eg, low-density lipoprotein, HbA1c);
physicians or based on objective outcome measures;
or a percentage;
assessed; and
Although the primary literature on P4P typically reports financial incentives and/or changes in pay-ment, it rarely includes information necessary for rigorous scientific analysis, such as the precise baseline method of determining physician remuneration in the participating medical groups, the method by which incentives were distributed, or the percentage of total take-home pay the incentives represented.111
Recent research examining P4P programs shows results ranging from negligible effects to markedly positive effects on quality and cost across health care settings, populations, disease types, and countries.112

Health Care Reform
32
Reviews consistently state that there is insufficient evidence to draw conclusions about the effectiveness of these programs.97,111,112,113
In almost all circumstances, the financial incentives and change in payment offered by a P4P program are not the only variables under consideration. Most P4P programs that have been studied have potential con-founding concurrent interventions, such as a shift to greater team-based care management, the addition of patient registries, and the greater availability of point-of-care resources and physician reminders, all of which potentially might affect physician performance as well.97
Outpatient ProgramsFindings in individual studies show that P4P
programs may increase the probability of quality improvement, whether it is measured in terms of process change (eg, obtaining biomarker tests such as for HbA1c and low-density lipoprotein at appropri-ate intervals, making appropriate referrals to tobacco quit-lines)114,115 or in terms of improved outcomes for certain measures (eg, achieving an HbA1c level less than 7%).116 A 5-year study of a P4P model that focused on 4 chronic disease and preventive screen-ing measures showed modest improvement on these measures after implementation of the program.98 The study also showed that removal of these incentives for 2 of the measures was associated with a subsequent decline in screening adherence.
Other valid studies show a lack of clinically sig-nificant effects of P4P programs117; however, many of these studies are small. In 1 study, physicians in 6 clinics were given financial incentives to achieve group targets for 3 preventive care measures. Partici-pants were also surveyed about their perception of the incentive program. After 6 years, there was no statisti-cal difference between the incentivized and nonincen-tivized clinics in performance indicators. In addition, survey results showed that most physicians did not think financial incentives were effective in improving quality of care.118
The available data lead to many additional questions. For example, how are successful P4P programs achiev-ing success? Does the mere presence of a financial incentive change physician behavior, or does the finan-cial incentive add needed capital to a practice, allowing it to invest in initiatives that can improve processes and outcomes (eg, developing a patient registry)?
One concern about P4P programs is that they may
exacerbate health care disparities by causing hospitals and clinics that are performing poorly on quality met-rics because of patient population or participation in safety-net clinics to think it impossible to achieve goals or to improve on low measures and give up on try-ing to achieve targets.119,120,121 This could increase the resource inequality affecting practices and hospitals that treat the socioeconomically disadvantaged,100,122 causing a net effect of stealing from the poor to give to the rich.123,124 However, there are no definitive conclu-sions on these issues.93,100,117,125,126
Hospital ProgramsThe Hospital Value-Based Purchasing Program
is based on the Premier Hospital Quality Incentive Demonstration. One study recently examined mortal-ity outcomes for hospitals participating in the demon-stration compared with hospitals who solely reported data publicly.127 Analysis of 6 years’ worth of mortality data for hospitals participating in the demonstration and control hospitals showed no significant difference in 30-day mortality for patients with acute myocardial infarction, congestive heart failure, or pneumonia, or patients who underwent coronary artery bypass graft-ing. All hospitals improved over baseline.
An earlier study compared 2 years’ worth of data on quality measures from hospitals participating in the demonstration with data from hospitals that only participated in public reporting.128 Compared to the control group, the demonstration hospitals achieved greater improvement in outcomes (eg, vaccination rates) and process measures. Both groups demonstrated an overall improvement from baseline performance.
The exact effect of hospital P4P programs on outcomes and the sustainability of any improvements achieved by such programs are still unclear. Currently, there is neither an existing model of a successful hos-pital P4P program, nor a blueprint on which to base a successful program.129
Cases 3 and 4, cont’d. After attending the hospital medical staff meeting and the organization’s compensa-tion committee meeting, you decide to read more about what outpatient and hospital pay-for-performance measures mean for you and your hospital/practice. Based on the available information, you conclude that pay for performance is here to stay for at least the next several years. However, how to do it well (ie, ensure that finan-cial incentives bring about the intended quality improve-ment) is uncertain.

33
SECTION FOUR
The Family Physician and Health Care Reform
Case 5. You are at a meeting of your state’s medical society. Many of the sessions are about issues related to health care reform. During the meeting, you receive information regarding the American Medi-cal Association/Specialty Society Relative Value Scale Update Committee and graduate medi-cal education expansion that you think might be harmful for family medicine. You are inter-ested in learning more about the American Academy of Family Physicians’ position on important health care reform issues.
The American Academy of Family Physicians and Health Care Reform
Multiple organizations, including the American Acad-emy of Family Physicians (AAFP), the American Medical Association (AMA), the Ameri-can College of Physicians, and the American Osteopathic Asso-ciation, developed principles for health care reform, which were presented to Congress (Table 10). Based on the assertion that improved individual and population health should be the end point of health care reform, these principles include univer-sal coverage, improved quality and safety, payment reform, and administrative and medical liability reform.
The AAFP has long advo-cated for health care reform that would make comprehensive, high-quality health care avail-able to all individuals, regardless
of age or medical condition.62 Policy and advocacy statements that pertain to health care reform are avail-able on the AAFP Web site (http://www.aafp.org/online/en/home/policy/federal/issues/reform.html).
Table 10Principles for Reform of the US Health Care Systema
system.
health care.
aPrinciples established by the American Academy of Family Physicians, American Acad-emy of Orthopaedic Surgeons, American College of Cardiology, American College of Emergency Physicians, American College of Obstetricians and Gynecologists, American College of Osteopathic Family Physicians, American College of Physicians, American Col-lege of Surgeons, American Medical Association, and American Osteopathic Association.
Reprinted from Principles for reform of the U.S. health care system. American Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/member-ship/initiatives/hrsprinciples.html.

Health Care Reform
34
Table 11AAFP Advocacy Positions and the PPACA
Advocacy Positions Addressed How
Health Care for All Yes
Health Care Research Yes
Yes
Patient-Centered Yes
Pay for Performance Yes
Family Physician Partial
Partial
ConsolidationPartial
Physician Payment Reform
Partial
Partial
continued

The AAFP identifies 7 major issues that should be addressed in health care reform, comprising the patient-centered medical home (PCMH), universal coverage, health information technology, Medicare physician payment, research and quality, medical liability reform, and health insurance consolida-tion (Table 11). Another component of health care reform involves addressing the shortage of primary care physicians, especially in light of the increas-ingly central role primary care will play under many Patient Protection and Affordable Care Act (PPACA) provisions.
The PPACA addresses many of these areas, and the AAFP has stated that this law is consistent with the advocacy principles adopted by its Congress of Del-egates in 2009.130 Specifically, the PPACA supports the PCMH, supports primary care residency training, and accomplishes health insurance reform. It also provides expanded access to care, as well as increasing reimbursement for primary care services from Medi-care and Medicaid, thereby increasing the willingness of physicians to care for patients insured by these programs and enhancing the role of primary care in health care delivery.
As previously discussed, the PPACA allows for expanded insurance coverage through the creation of the health insurance exchanges. It also includes mandates requiring businesses and individuals to purchase insurance. These provisions are in keeping with the AAFP’s principles for increased access to care and insurance coverage. The AAFP did not specifically
advocate for the controversial individual mandate; however, the AAFP and the AMA supported the man-date on the basis of the precedent set in Massachusetts and the core principle of individual responsibility for health care.
Patient-Centered Medical HomeThe AAFP has drawn attention to evidence indicat-
ing that the care provided by family physicians in a PCMH should be the foundation of any reform to the US health care system.131,132,133 For family physi-cians, the PCMH is a means of improving quality of care, improving care coordination, enhancing focus on patients, and highlighting the essential role of primary care. The AAFP provides information to help physi-cians implement elements of the PCMH on its Web site (http://www.aafp.org/online/en/home/member-ship/initiatives/pcmh.html).
The PCMH is 1 means of delivering the type of patient-centered care that is a feature of multiple provisions within the PPACA. Specific ways that the PPACA supports the PCMH model of care include piloting this model through the newly established Center for Medicare and Medicaid Innovation, providing a state Medicaid health home option, sup-porting and incentivizing the medical home concept within private health plans, providing support and education for the delivery of medical home services in primary care practices, and providing grants for teach-ing programs that educate medical students about the PCMH model of care.133
Table 11 (continued)
AAFP Advocacy Positions and the PPACA
Advocacy Positions Addressed How
Reform
AAFP = American Academy of Family Physicians; ACO = accountable care organization; CHIP = Children’s Health Insurance Program; CMS = Centers for Medicare & Medicaid Services; EHR = electronic health record; FQHC = federally qualified health center; GME = graduate medical education; NHSC = National Health Service Corps; P4P = pay for performance; PPACA = Patient Protection and Affordable Care Act; PQRS = Physician Quality Reporting System; SGR = sustainable growth rate; VBP = value-based purchasing.
Information from various sources.

Health Care Reform
36
Medicare Physician PaymentA central component of the AAFP’s focus on Medi-
care physician payment reform is fixing the sustainable growth rate (SGR) formula, which was not addressed by the PPACA. The AAFP specifically advocates for a multiyear SGR fix while data are gathered on pay-ment models, such as accountable care organizations (ACOs) and the PCMH; the resulting data would be used to develop a new physician fee structure.134
The final rule on ACOs from the Centers for Medicare & Medicaid Services (CMS) was supported by the AAFP as a way to address Medicare physician payment reform. The CMS incorporated in the final rule several AAFP proposals,135 including:
more than 1 ACO;-
ciaries, identified quarterly;-
sures used to determine shared savings benefits;
second and third year of participation; and
clinics, and federally qualified health centers to participate in ACOs.
The American Medical Association/Specialty Society Relative Value Scale Update Committee
The AMA formed the AMA/Specialty Society Rela-tive Value Scale Update Committee (RUC) in the early 1990s as an expert panel to develop and make recommendations to CMS regarding the relative value of new or revised CPT codes using the resource-based relative value scale that was mandated by Congress in the Omnibus Budget Reconciliation Act of 1989.136 The purpose of the RUC is to ensure that physician services across all subspecialties are well represented in the valuation of services with the resource-based rela-tive value scale.137
Of the RUC’s 31 committee members, 21 are appointed by national medical societies, with 1 posi-tion reserved specifically for primary care.136 The AAFP has stated that this is underrepresentation and expressed concern that the current composition biases the RUC in favor of procedures and subspecialty care rather than preventive care and chronic disease man-agement.138 Because many insurance plans base their payment on the Medicare fee schedule, the potential effect of this perceived bias reaches well beyond CMS
and Medicare.139 Some have argued that the RUC’s bias toward procedures and subspecialty care has led, in part, to the income disparity between primary care and subspecialties, which might discourage medical stu-dents from pursuing a career in primary care.140,141,142
On June 10, 2011, then-AAFP President Lori Heim, MD, asked the RUC to increase the number of physicians from primary care, including 1 each from the AAFP, the American Academy of Pediatrics, American College of Physicians, and the American Osteopathic Association; include a seat for geriat-rics; and eliminate 3 of the current seats allotted for subspecialty physicians.138 Dr Heim also requested that 3 new seats be added for nonphysicians represent-ing outside entities (eg, health systems). Finally, she requested a change to the RUC’s voting procedures to emphasize transparency.
In March 2012, the RUC responded to the AAFP’s call for reform, stating that, in general, it was already properly structured and was acting appropriately as an expert panel; it also denied having any formal advi-sory relationship with CMS. The RUC did agree to add a seat specifically for primary care and a seat for geriatrics. The RUC also agreed to move a step closer to voting transparency. However, the RUC declined to add as many primary care seats as requested by the AAFP and also declined to add any seats for such enti-ties as payers and health systems.140,143,144
Although acknowledging that the RUC’s response was inadequate and that the RUC has devastated primary care for 2 decades, the AAFP Board of Direc-tors decided to remain in the RUC because with-drawal—after making headlines—would have isolated the AAFP, weakened its long-term strategic objectives, and impaired its ability to advocate in the future for changes that benefit family medicine.145
In August 2011, 6 physicians filed a lawsuit against Department of Health and Human Services Secretary Kathleen Sebelius and CMS Administrator Donald Berwick, alleging that physicians have been harmed by the Medicare payment structure developed by the RUC.146,147 The plaintiffs also argued that, although the RUC is treated as a de facto federal advisory committee, it has not been required to adhere to the same federal management and reporting rules as other advisory committees. In May 2012, the lawsuit was dismissed. The presiding judge stated that because physicians know how much they will be paid for their services before they decide to participate in the

37
Section Four
Medicare program, their due process rights were not violated.148 The plaintiffs have since appealed.
Health Care Coverage for AllThe AAFP advocates for universal health care cover-
age that includes catastrophic protection; provides each individual with a PCMH; and reflects a shared respon-sibility for health care among individuals, employ-ers, government, and the private sector.62 The AAFP supports implementation of the PCMH as a means of centralizing the role of primary care, which is the foun-dation for universal coverage. In addition, the AAFP supports payment reform for primary care services. This includes elimination of any financial barriers (eg, copays) to services, such as primary care services pro-vided in a medical home, chronic disease management, evidence-based preventive services, and hospice care. The AAFP recommends a blended payment model that includes fee-for-service payments, care manage-ment fees, and pay-for-performance payment.
The PPACA advances many of the principles of universal health coverage articulated by the AAFP, including support for the PCMH, blended payment models, expansion of health insurance coverage (ie, through government programs and the individual and employer mandates), and increased emphasis on primary care.130
Health Information TechnologyThe AAFP believes that the health care industry,
including physicians, practices, and hospitals, needs to continue moving toward use of electronic health records149,150,151 and improved reporting on physician quality measures. There has been some disagree-ment on the timeline for these changes, as well as the amount of regulation and reporting required by the Physician Quality Reporting System and the PPACA.
For many years, the AAFP has stated that every fam-ily physician should be computer literate, able to use information technology effectively, and should obtain and use an electronic health record.149,151 Under the PPACA, the incentive for encouraging physicians to achieve these goals has changed from bonus payments for meeting criteria to a 1.5% reduction in Medicare reimbursement for physicians who are not using a cer-tified electronic health record or meeting meaningful use criteria by 2015.152 It is proposed that physicians not meeting the Physician Quality Reporting System requirements would be penalized in a similar manner.
The AAFP has advocated for greater flexibility in the meaningful use criteria and for more time for imple-mentation, requesting that penalties be delayed until 2017. In March 2012, the AAFP asked the Depart-ment of Health and Human Services to modify the timing of upcoming penalties for primary care physi-cians who are not able to meet the stringent require-ments of several new quality reporting initiatives.153
Health Care Research and QualityThe AAFP supports ongoing funding for the
Agency for Healthcare Research and Quality and the National Institutes of Health.154 A March 14, 2012, letter from the AAFP to the Patient-Centered Outcomes Research Institute (PCORI) outlined key research priorities that are largely in line with the institute’s proposed national priorities and research agenda.155 The priorities outlined in the proposed agenda—which is supported by the AAFP and other family medicine organizations—include: 1) assess-ing prevention, diagnosis, and treatment options; 2) improving health care delivery systems; 3) dis-seminating information about treatment options; 4) addressing health disparities; and 5) accelerating patient-centered and methodologic research.
Medical Liability and ReformThe PPACA does not address medical liability
reform, although this is a key component of the AAFP’s health care reform advocacy efforts. The AAFP endorses provisions of California’s medical liability law, which include modifying attorney fees, imposing a hard cap on noneconomic damages, informing juries of compensation the plaintiff has already received from other sources, implementing proportionate liability, providing alternative systems to resolve disputes, and requiring expert witnesses to have knowledge of and
The PPACA advances many of the principles of universal health cover-age articulated by the AAFP, includ-ing support for the PCMH, blended payment models, expansion of health insurance coverage, and increased emphasis on primary care.

Health Care Reform
38
practice in the same medical specialty as the defen-dant.156 However, the PPACA does include grants to states to test alternative dispute resolution methods, for which the AAFP has advocated.
Health Insurance ConsolidationThe AAFP advocates for the health insurance indus-
try to be regulated like other industries to promote competition, which will bring about reform.157 In addition, the AAFP advocates for changes in regula-tion so that primary care physicians can negotiate contracts with third-party payers in a more equitable manner. The PPACA addresses this issue through the formation of health insurance exchanges and ACOs.
Changes to Graduate Medical EducationIn conjunction with the Association of Family Med-
icine Residency Directors and the Society of Teach-ers of Family Medicine, the AAFP has articulated a vision of how reforming graduate medical education to improve and expand primary care training can help address the workforce shortage.158,159
The AAFP’s proposed approach includes reforms, such as capturing lost residency positions from hospitals that close and expanding the residency cap (ie, the limit on the number of residents for which a hospital can receive funding, which has been frozen since 1997) for primary care and other subspecialties with demonstrated physician workforce shortages. The AAFP also supports the expansion of residency training at federally qualified health centers and other nonhospital community sites with sustainable funding, provided that certain conditions are met.160 In addition, the AAFP supports Section 5508(a) of the PPACA, which establishes funding for new or expanded teaching health centers (ie, community-based, ambulatory patient care centers that operate primary care residency programs).
The AAFP’s primary disagreement with the Asso-ciation of American Medical College’s position161 on medical education issues germane to health care reform pertains to the use of limited federal resources to address the primary care workforce shortage by investing in expanded graduate medical education. The AAFP’s policy supports preferential funding for
residency programs that have a track record of training primary care physicians, physicians located in and/or serving rural and inner-city populations, or physicians from underrepresented minorities.158,159
Translating Health Care Reform for PatientsAccording to numerous surveys, in the years before
the debates regarding health care reform in 2009 and 2010, there was dissatisfaction with the cur-rent health care system and support for health care reform among physicians and the general public in the United States.162,163,164,165 Stated public opinion now reflects that some Americans are dissatisfied with or oppose the PPACA.166,167,168 However, when individu-als are queried about the components of the PPACA, rather than about the law as a whole, there is support for individual measures.169 Public opinion about the PPACA might remain divided for some time.
The Kaiser Family Foundation conducted a survey of public opinion about the PPACA after the Supreme Court’s ruling.170 This poll showed that overall opin-ion of the PPACA was unchanged after the ruling, with 41% of those surveyed still having an unfavorable opinion of the law and 41% having a favorable opin-ion. A majority of Americans polled (56%) said they want to see the detractors of the law stop their opposi-tion campaign, assist with implementation, and move on to dealing with other national problems.
Patients likely have many questions about how the PPACA will affect them and their families. There are several good references to help families—and family physicians—understand more about the PPACA and how it will affect them now and in the future (see Sug-gested Readings).
Case 5, cont’d. After attending a number of presenta-tions on health care reform for the family physician, you realize that the Patient Protection and Affordable Care Act (PPACA) touches on many important aspects of health care reform, but not all. You discover that the American Academy of Family Physicians and other organizations have carefully considered approaches to health care reform that overlap with the PPACA in some instances but also include other aspects, such as an emphasis on the patient-centered medical home and recommendations for payment reform and primary care training.

1. Patient Protection and Affordable Care Act, 42 USC §18001 (2010).
2. Carey D, Herring B, Lenain P. Health Care Reform in the United States. Economics Department Working Paper No. 665. Paris: Organisation for Economic Co-operation and Development; 2009. Available at http://search.oecd.org/offi-cialdocuments/displaydocumentpdf/?doclanguage=en&cote=eco/wkp(2009)6. Accessed December 2012.
3. Henry J. Kaiser Family Foundation. Number of uninsured Americans drops by 1.3 million. Kaiser Health News. Sep-tember 2012. Available at http://www.kaiserhealthnews.org/daily-reports/2012/september/13/census-numbers.aspx. Accessed December 2012.
4. DeNavas-Walt C, Proctor BD, Smith JC. Income, Poverty, and Health Insurance Coverage in the United States: 2011. Current Population Reports, P60-243. Washington, DC: US Census Bureau; 2012. Available at http://www.census.gov/prod/2012pubs/p60-243.pdf. Accessed December 2012.
5. Hadley J. Sicker and poorer—the consequences of being uninsured: a review of the research on the relationship between health insurance, medical care use, health, work, and income. Med Care Res Rev. 2003;60(2 Suppl):3S-75S; discussion 76S-112S.
6. Frakt A, Carroll AE, Pollack HA, et al. Our flawed but benefi-cial Medicaid program. N Engl J Med. 2011;364(16):e31.
7. Board on Health Care Services, Institute of Medicine of the National Academies. America’s Uninsured Crisis: Con-sequences for Health and Health Care. Washington, DC: National Academies Press; 2009.
8. Mayne L, Girod C, Weltz S. 2011 Milliman Medical Index. Milliman Research Report. May 2011. Available at http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2011.pdf. Accessed December 2012.
9. World Health Organization. The World Health Report 2000—Health Systems: Improving Performance. Geneva: WHO; 2000.
10. Nolte E, McKee M. Measuring the health of nations: analysis of mortality amenable to health care. BMJ. 2003;327(7424):1129. Erratum in BMJ. 2004;328(7438):494.
11. Nolte E, McKee CM. Measuring the health of nations: updat-ing an earlier analysis. Health Aff (Millwood). 2008;27(1):58-71. Erratum in Health Aff (Millwood). 2008;27(2):593.
12. Doherty RB. The certitudes and uncertainties of health care reform. Ann Intern Med. 2010;152(10):679-682.
13. Henry J. Kaiser Family Foundation. Focus on Health Reform: Summary of New Health Reform Law. Menlo Park, CA: KFF; 2011. Available at http://www.kff.org/healthreform/upload/8061.pdf. Accessed December 2012.
14. Iglehart JK. Defining essential health benefits—the view from the IOM Committee. N Engl J Med. 2011;365(16):1461-1463.
15. Weil A. The value of federalism in defining essential health benefits. N Engl J Med. 2012;366(8):679-681.
16. Henry J. Kaiser Family Foundation. Explaining Health Care Reform: Questions About Health Insurance Exchanges. Menlo Park, CA: KFF; 2010. Available at http://www.kff.org/healthreform/7908.cfm. Accessed December 2012.
17. Henry J. Kaiser Family Foundation. Focus on Health Reform: Explaining Health Care Reform: Questions About Health Insurance Exchanges. Menlo Park, CA: KFF; 2010. Available at http://www.kff.org/healthreform/upload/7908-02.pdf. Accessed December 2012.
18. Ruger JP. Fair enough? Inviting inequities in state health benefits. N Engl J Med. 2012;366(8):681-683.
19. Henry J. Kaiser Family Foundation. Focus on Health Reform: What the Actuarial Values in the Affordable Care Act Mean. Menlo Park, CA: KFF; 2011. Available at http://www.kff.org/healthreform/upload/8177.pdf. Accessed December 2012.
20. Henry J. Kaiser Family Foundation. Health Reform Source. Health Reform Subsidy Calculator. Menlo Park, CA: KFF; 2010. Available at http://healthreform.kff.org/Subsidycalcula-tor.aspx. Accessed December 2012.
21. National Conference of State Legislators. Coverage of Unin-surable Pre-existing Conditions: State and Federal High-Risk Pools. Washington, DC: National Conference of State Legislatures; 2012. Available at http://www.ncsl.org/issues-research/health/high-risk-pools-for-health-coverage.aspx. Accessed December 2012.
22. Healthcare.gov. Medical loss ratio: getting your money’s worth on health insurance. 2010. Available at http://www.healthcare.gov/news/factsheets/2010/11/medical-loss-ratio.html. Accessed December 2012.
23. Smith V, Gifford K, Ellis E, et al. Kaiser Commission on Medicaid & the Uninsured. Low Medicaid Spending Growth Amid Rebounding State Revenues: Results From a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007. Menlo Park, CA: KFF; 2006. Available at http://www.kff.org/medicaid/upload/7569.pdf. Accessed December 2012.
24. Henry J. Kaiser Family Foundation. State Health Facts. Med-icaid-to-Medicare Fee Index, 2008. Menlo Park, CA: KFF; 2009. Available at http://www.statehealthfacts.org/compare table.jsp?ind=196&cat+4. Accessed December 2012.
25. Zuckerman S, Williams AF, Stockley KE. Trends in Med-icaid physician fees, 2003–2008. Health Aff (Millwood). 2009;28(3):w510-519.
26. Palfrey JS. How health care reform can benefit children and adolescents. N Engl J Med. 2009;361(17):e34.
27. Roberts M, Rhoades JA. The Uninsured in America, First Half of 2009: Estimates for the U.S. Civilian Noninstitutional-ized Population Under Age 65. Rockville, MD: Agency for Healthcare Research and Quality; August 2012. Statistical Brief No. 291. Available at http://meps.ahrq.gov/mepsweb/data_files/publications/st291/stat291.shtml. Accessed December 2012.
28. Fiegl C. Quest for SGR reform: avoiding the eleventh-hour drama. American Medical News. July 18, 2011. Available at http://www.ama-assn.org/amednews/2011/07/18/gvsa0718.htm. Accessed December 2012.
References

40
Healthcare Reform
29. Silva C. Medicare pay: SGR fatigue. American Medical News. May 3, 2010. Available at http://www.ama-assn.org/amed news/2010/05/03/gvsa0503.htm. Accessed December 2012.
30. Henry J. Kaiser Family Foundation. Congress approves tax package including temporary ‘doc fix’. Kaiser Health News. February 21, 2012. Available at http://www.kaiserhealthnews.org/Daily-Reports/2012/February/21/cap-hill-watch-doc-fix.aspx. Accessed December 2012.
31. Carey MA. FAQ: the ‘doc fix’ dilemma. Kaiser Health News. February 2012. Available at http://www.kaiserhealth-news.org/Stories/2011/December/15/FAQ-Doc-Fix.aspx. Accessed December 2012.
32. Merlis M. Medicare payments to physicians. Congress has enacted another short-term ‘doc fix.’ A permanent solution to this perennial problem remains elusive. Health Affairs. Feb-ruary 28, 2012. Available at http://healthaffairs.org/health-policybriefs/brief_pdfs/healthpolicybrief_64.pdf. Accessed December 2012.
33. Congressional Budget Office. The budget and economic outlook: fiscal years 2012 to 2022. January 31, 2012. Avail-able at http://www.cbo.gov/publication/42905. Accessed December 2012.
34. Congressional Budget Office. Cost estimate. H.R. 3961 Medicare Physician Payment Reform Act of 2009. November 4, 2009. Available at http://www.cbo.gov/sites/default/files/cbofiles/ftpdocs/107xx/doc10704/hr3961.pdf. Accessed December 2012.
35. Association of American Medical Colleges. Congress passes short-term SGR fix [press release]. January 6, 2012. Available at https://www.aamc.org/advocacy/washhigh/highlights2012/270436/congresspassesshort-termsgrfix.html. Accessed December 2012.
36. American Academy of Family Physicians. The secret to get-ting a 10 percent Medicare bonus in 2011. Getting Paid [blog post]. December 23, 2010. Available at http://blogs.aafp.org/fpm/gettingpaid/entry/are_you_banking_on_the. Accessed December 2012.
37. Porter S. Provision in health care reform law gives pri-mary care financial boost. AAFP News Now. September 9, 2010. Available at http://www.aafp.org/online/en/home/ publications/news/news-now/practice-management/ 20100903primcarebonus.html. Accessed December 2012.
38. Centers for Medicare & Medicaid Services. Incentive pay-ment program for primary care services, Section 5501(a) of the Affordable Care Act. MLN Matters. Updated August 8, 2012. Available at http://www.cms.gov/Outreach-and-Educa-tion/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM7060.pdf. Accessed December 2012.
39. Robert Graham Center. Effects of Proposed Primary Care Incentive Payments on Average Physician Medicare Revenue and Total Medicare Allowed Charges: A White Paper. Washing-ton, DC: RGC; 2009. Available at http://www.graham-center.org/online/etc/medialib/graham/documents/publications/mongraphs-books/2009/rgcwp-effects-proposed. Par.0001.File.tmp/medicare-simulations.pdf. Accessed December 2012.
40. Sommers BD, Epstein AM. Medicaid expansion—the soft underbelly of health care reform? N Engl J Med. 2010;363 (22):2085-2087.
41. Iglehart JK. Expanding coverage for children—the Demo-crats’ power and SCHIP reauthorization. N Engl J Med. 2009;360(9):855-857.
42. Medicaid.gov. CHIP eligibility standards. Available at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Childrens-Health-Insurance-Program-CHIP/CHIP-Eligibility-Standards-.html. Accessed December 2012.
43. Henry J. Kaiser Family Foundation. Focus on Health Reform: Summary of Coverage Provisions in the Patient Protection and Affordable Care Act. Menlo Park, CA: KFF; 2012. Avail-able at http://www.kff.org/healthreform/upload/8023-R.pdf. Accessed December 2012.
44. Henry J. Kaiser Family Foundation. Focus on Health Reform: Medicaid and Children’s Health Insurance Program Provi-sions in the New Health Reform Law. Menlo Park, CA: KFF; 2010. Available at http://www.kff.org/healthreform/upload/7952-03.pdf. Accessed December 2012.
45. Sommers B, Swartz K, Epstein A. Policy makers should pre-pare for major uncertainties in Medicaid enrollment, costs, and needs for physicians under health reform. Health Aff (Millwood). 20111;20(11):2186-2193.
46. Sisko AM, Truffer CJ, Keehan SP, et al. Exhibit 6. National health spending projections: the estimated impact of reform through 2019. Health Aff (Millwood). 2010;29(10):1933-1941. Erratum in Health Aff (Millwood). 2010;29(11):2128.
47. Bill summary & status. 111th Congress (2009–2010). H.R. 3590. The Library of Congress, Thomas Web site. Available at http://thomas.loc.gov/cgi-bin/bdquery/z?d111:H.R.3590:. Accessed December 2012.
48. National Federation of Independent Business v Sebelius, 567 US 2 (2012).
49. Landers RM. The dénouement of the Supreme Court’s ACA drama. N Engl J Med. 2012;367(3):198-199.
50. The Economist. Health insurance premium hikes: the insur-ance death spiral is here. Democracy in America [blog post]. February 19, 2010. Available at http://www.economist.com/blogs/democracyinamerica/2010/02/health_insurance_pre-mium_hikes. Accessed December 2012.
51. Klein E. The importance of the individual mandate. The Washington Post. Economic and Domestic Policy, and Lots of It [blog post]. December 16, 2009. Available at http://voices.washingtonpost.com/ezra-klein/2009/12/draft_1.html. Accessed December 2012.
52. Klein E. An interview with Mark Pauly, father of the individual mandate. The Washington Post. Economic and Domestic Policy, and Lots of It [blog post]. February 1, 2011. Available at http://voices.washingtonpost.com/ezra-klein/2011/02/an_ interview_with_mark_pauly_t.html. Accessed December 2012.
53. Hall MA. Health care reform—what went wrong on the way to the courthouse. N Engl J Med. 2011;364(4):295-297.

41
References
54. Henry J. Kaiser Family Foundation, Health Research and Educational Trust. Employer Health Benefits 2011 Annual Survey. Menlo Park, CA: KFF; 2012. Available at http://ehbs.kff.org/. Accessed December 2012.
55. Lazarus D. Wal-Mart offers latest sign that employer-based health coverage is failing. Los Angeles Times. October 28, 2011. Available at http://articles.latimes.com/2011/oct/28/business/la-fi-lazarus-20111028. Accessed December 2012.
56. Johnson T. Backgrounder. Healthcare costs and U.S. com-petitiveness. Council on Foreign Relations. March 26, 2012. Available at http://www.cfr.org/health-science-and-technol-ogy/healthcare-costs-us-competitiveness/p13325. Accessed December 2012.
57. Sood N, Ghosh A, Escarce JJ. Employer-sponsored insur-ance, health care cost growth, and the economic performance of U.S. industries. Health Serv Res. 2009;44(5 Pt 1):1449-1464.
58. Mataconis D. Wage growth over past ten years worse than during Great Depression. Outside the Beltway. June 3, 2011. Available at http://www.outsidethebeltway.com/wage-growth-over-past-ten-years-worse-than-during-great-depres-sion/. Accessed December 2012.
59. Agency for Healthcare Quality and Research. 2012 Annual Progress Report to Congress on the National Strategy for Quality Improvement in Health Care. Rockville, MD: AHRQ; 2012. Available at http://www.ahrq.gov/workingforquality/. Accessed December 2012.
60. Comprehensive Primary Care Initiative. Centers for Medi-care & Medicaid Services Web site. Available at http://www.innovations.cms.gov/initiatives/Comprehensive-Primary-Care-Initiative/index.html. Accessed December 2012.
61. Elmendorf D. CBO’s Analysis of the Major Health Care Leg-islation Enacted in March 2010. Washington, DC: Congres-sional Budget Office; 2011. Available at http://cbo.gov/sites/default/files/cbofiles/ftpdocs/121xx/doc12119/03-30-health-carelegislation.pdf. Accessed December 2012.
62. Health care for all: a framework for moving to a primary care-based health care system in the United States. Ameri-can Academy of Family Medicine Web site. Available at http://www.aafp.org/online/en/home/policy/policies/h/healthcare.html. Accessed December 2012.
63. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: IOM; 2001. Available at http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Qual-ity%20Chasm%202001%20%20report%20brief. Accessed December 2012.
64. Introduction. In: Jonas S, Goldsteen RL, Goldsteen K, eds. An Introduction to the U.S. Health Care System. 6th ed. New York: Springer Publishing Co.; 2007:1.
65. The current US health care systems. In: Kovner AR, Knick-man JR, Jonas S. Jonas and Kovner’s Health Care Delivery in the United States. 10th ed. New York: Springer Publishing Co.; 2011:3-8.
66. Fisher ES, Staiger DO, Bynum JP, et al. Creating account-able care organizations: the extended hospital medical staff. Health Aff (Millwood). 2007;26(1):w44-57.
67. Welch SS. Accountable care organizations—overview. In: American Medical Association Practice Center Manage-ment, eds. ACOs, CO-OPs and Other Options: A “How-To” Manual for Physicians Navigating A Post-Health Reform World. 2nd ed. Chicago: AMA; 2012:20-42.
68. National Committee for Quality Assurance. Accountable Care Organizations. Draft 2011 Criteria: Overview. Washing-ton, DC: NCQA; October 2010. Available at http://www.ncqa.org/portals/0/publiccomment/ACO/ACO_%20Overview.pdf. Accessed December 2012.
69. Accountable care organizations. Centers for Medicare & Medicaid Services Web site. Available at http://www.cms.gov/aco. Accessed December 2012.
70. Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Aff (Millwood). 2008;27(3):759-769.
71. Pioneer ACO Model. Centers for Medicare & Medicaid Ser-vices Web site. Available at http://innovations.cms.gov/initia-tives/aco/pioneer/. Accessed December 2012.
72. Medicare Shared Savings Program. Centers for Medicare & Medicaid Services Web site. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/shared-savingsprogram/index.html?redirect=/sharedsavingspro-gram/. Accessed December 2012.
73. Advance Payment ACO Model. Centers for Medicare & Med-icaid Services Web site. Available at http://innovations.cms.gov/initiatives/aco/advance-payment/index.html. Accessed December 2012.
74. Fisher DW. re: Medicare Shared Savings Program: account-able care organizations [Letter to Donald Berwick, CMS administrator]. May 11, 2011. Available at http://www.amga.org/advocacy/MGAC/Letters/05112011.pdf. Accessed December 2012.
75. Bobbitt JD. What family physicians need to know about ACOs. Fam Pract Manag. 2011;18(5):17-22.
76. Bee G, Dunlay C. Risk-bearing under the MSSP ACO final rule. ABA Health eSource. 2012;8(5). Available at http://www.americanbar.org/newsletter/publications/aba_health_esource_home/aba_health_law_esource_0112_bee.html. Accessed December 2012.
77. Healthcare.Gov. Antitrust guidance for providers in ACOs. In: Accountable Care Organizations: Improving Care Coor-dination for People with Medicare. 2011. Available at http://www.healthcare.gov/news/factsheets/2011/03/accounta-blecare03312011a.html. Accessed December 2012.
78. Department of Justice/Federal Trade Commission Issues Final Statement of Antitrust Policy Enforcement Regarding Accountable Care Organizations [news release]. Wash-ington, DC: Department of Justice, Justice News. October 20, 2011. Available at http://www.justice.gov/opa/pr/2011/October/11-at-1384.html. Accessed December 2012.
79. Rau J, Galewitz P. New ACO rules outline gains and risks for doctors, hospitals. Kaiser Health News. March 31, 2011. Available at http://www.kaiserhealthnews.org/stories/2011/march/31/aco-rules.aspx?referrer=search. Accessed December 2012.

42
Healthcare Reform
80. Mackinney AC, Mueller KJ, McBride TD. The march to accountable care organizations—how will rural fare? J Rural Health. 2011;27(1):131-137.
81. Hussey PS, Ridgely MS, Rosenthal MB. The PROMETHEUS bundled payment experiment: slow start shows problems in implementing new payment models. Health Aff (Millwood). 2011;30(11):2116-2124.
82. Berenson R, Burton R. Next steps for ACOs. Health Affairs. January 31, 2012. Available at http://www.healthaffairs.org/healthpolicybriefs/brief.php?brief_id=61. Accessed Decem-ber 2012.
83. Trisolini M, Kautter J, Pope GC, et al. Physician group prac-tice (PGP) demonstration design report. Health Care Financ Rev. 2007;29(1):15-29.
84. Wilensky GR. Lessons from the Physicians Group Prac-tice Demonstration—a sobering reflection. N Engl J Med. 2011;365(18):1659-1661.
85. Berenson R, Burton R. Accountable care organizations in Medicare and the private sector: a status update. Urban Institute. November 2011. Available at http://www.urban.org/uploadedpdf/412438-Accountable-Care-Organizations-in-Medicare-and-the-Private-Sector.pdf. Accessed December 2012.
86. American Academy of Family Physicians; American Academy of Pediatrics; American College of Physicians; American Osteopathic Association. Joint Principles for Accountable Care Organizations. November 19, 2010. Available at http://www.acponline.org/advocacy/where_we_stand/other_issues/aco-principles-2010.pdf. Accessed December 2012.
87. Pay-for-performance. American Academy of Family Physi-cians Web site. 2010. Available at http://www.aafp.org/online/en/home/policy/policies/p/payforperformance.html. Accessed December 2012.
88. Premier Hospital Quality Incentive Demonstration fact sheet. Centers for Medicare & Medicaid Web site. Available at https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Downloads/HospitalPremierPressRelease-FactSheet.pdf. Accessed December 2012.
89. Medicare Physician Group Practice Demonstration fact sheet. Centers for Medicare & Medicaid Web site. Available at https://www.cms.gov/Medicare/Demonstration-Projects/DemoProjectsEvalRpts/downloads/PGP_Fact_Sheet.pdf. Accessed December 2012.
90. Centers for Medicare & Medicaid Services. Fact sheet: CMS proposals to improve quality of care during hospital inpatient stays. Appendix D. April 24, 2012. Available at http://www.cms.gov/apps/media/press/factsheet.asp?Counter=4346&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=false&cboOrder=date. Accessed December 2012.
91. Harbaugh NC Jr. Pay for performance: quality- and value-based reimbursement. Pediatr Clin North Am. 2009;56(4): 997-1007.
92. Agency for Healthcare Research and Quality. Health care costs and financing. Pay for performance does not improve care quality in the short term in safety-net settings. Avail-able at http://www.ahrq.gov/research/oct10/1010RA5.htm. Accessed December 2012.
93. Young G, Meterko M, White B, et al. Pay-for-performance in safety net settings: issues, opportunities, and challenges for the future. J Healthc Manag. 2010;55(2):132-141; discussion 141-142.
94. National Committee for Quality Assurance. The Value of Requiring Health Plans To Report NCQA’s HEDIS Quality Measures. Washington, DC: NCQA; 2012. Available at http://www.ncqa.org/portals/0/Public%20Policy/ValueinRequir-ingHEDIS_8.15.12.pdf. Accessed December 2012.
95. Integrated Healthcare Association. Advancing Quality Through Collaboration: The California Pay for Performance Program. Oakland, CA: IHA; February 2006. Available at http://www.iha.org/pdfs_documents/p4p_california/P4P WhitePaper1_February2009.pdf. Accessed December 2012.
96. Integrated Healthcare Association. The California Pay for Per-formance Program. The Second Chapter: Measurement Years 2006–2009. Oakland, CA: IHA; June 2009. Available at http://www.iha.org/pdfs_documents/home/FINAL%20White%20 Paper%20June%202009.pdf. Accessed December 2012.
97. de Bruin SR, Baan CA, Struijs JN. Pay-for-performance in disease management: a systematic review of the literature. BMC Health Serv Res. 2011;11:272.
98. Lester H, Schmittdiel J, Selby J, et al. The impact of remov-ing financial incentives from clinical quality indicators: longi-tudinal analysis of four Kaiser Permanente indicators. BMJ. 2010;340:c1898.
99. Werner RM, Kolstad JT, Stuart EA, et al. The effect of pay-for-performance in hospitals: lessons for quality improve-ment. Health Aff (Millwood). 2011;30(4):690-698.
100. Averill RF, Hughes JS, Goldfield NI. Paying for outcomes, not performance: lessons from the Medicare Inpatient Prospective Payment System. Jt Comm J Qual Patient Saf. 2011;37(4):184-192, 145.
101. American Medical Association. Principles for pay-for-performance programs. June 2005. Available at http://www.ama-assn.org/resources/doc/psa/principles4pay62705.pdf. Accessed December 2012.
102. Hodgson ES, Simpson L, Lannon CM. Principles for the development and use of quality measures. Pediatrics. 2008;121(2):411-418.
103. Snyder L, Neubauer RL. Pay for performance principles that ensure the promotion of patient centered care—an ethics manifesto. Philadelphia: American College of Physicians; 2007. Available at http://www.acponline.org/running_prac-tice/ethics/issues/policy/p4p_ba.pdf. Accessed December 2012.
104. Lee JY, Lee SI, Jo MW. Lessons from healthcare providers’ attitudes toward pay-for-performance: what should purchas-ers consider in designing and implementing a successful program? J Prev Med Public Health. 2012;45(3):137-147.

43
References
105. Hannon KL, Lester HE, Campbell SM. Patients’ views of pay for performance in primary care: a qualitative study. Br J Gen Pract. 2012;62(598):e322-328.
106. Qaseem A, Snow V, Gosfield A, et al. Pay for performance through the lens of medical professionalism. Ann Intern Med. 2010;152(6):366-369.
107. Medical professionalism in the new millennium: a physician charter. Ann Intern Med. 2002;136(3):243-246.
108. Cassel CK, Jain SH. Assessing individual physician perfor-mance: does measurement suppress motivation? JAMA. 2012;307(24):2595-2596.
109. Pham HH, Schrag D, O’Malley AS, et al. Care patterns in Medicare and their implications for pay for performance. N Engl J Med. 2007;356(11):1130-1139.
110. Hassan Sadek N, Sadek AR, Tahir A, et al. Evaluating tools to support a new practical classification of diabetes: excel-lent control may represent misdiagnosis and omission from disease registers is associated with worse control. Int J Clin Pract. 2012;66(9):874-882.
111. Scott A, Sivey P, Ait Ouakrim D, et al. The effect of finan-cial incentives on the quality of health care provided by primary care physicians. Cochrane Database Syst Rev. 2011;(9):CD008451.
112. Van Herck P, De Smedt D, Annemans L, et al. Systematic review: effects, design choices, and context of pay-for-per-formance in health care. BMC Health Serv Res. 2010;10:247.
113. Witter S, Fretheim A, Kessy FL, et al. Paying for performance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database Syst Rev. 2012;(2):CD007899.
114. An LC, Bluhm JH, Foldes SS, et al. A randomized trial of a pay-for-performance program targeting clinician referral to a state tobacco quitline. Arch Intern Med. 2008;168(18):1993-1999.
115. Chung S, Palaniappan LP, Trujillo LM, et al. Effect of phy-sician-specific pay-for-performance incentives in a large group practice. Am J Manag Care. 2010;16(2):e35-42.
116. Chen JY, Tian H, Juarez DT, et al. Does pay for performance improve cardiovascular care in a “real-world” setting? Am J Med Qual. 2011;26(5):340-348.
117. Gavagan TF, Du H, Saver BG, et al. Effect of financial incen-tives on improvement in medical quality indicators for pri-mary care. J Am Board Fam Med. 2010;23(5):622-631.
118. Fairman KA, Curtiss FR. Clinical quality indicators and provider financial incentives: does money matter? J Manag Care Pharm. 2010;16(5):360-366.
119. Dowd B, Feldman R, Nersesian W. Setting pay for perfor-mance targets: do poor performers give up? Health Econ. 2012. [Epub ahead of print]
120. Goldman LE, Vittinghoff E, Dudley RA. Quality of care in hospitals with a high percent of Medicaid patients. Med Care. 2007;45(6):579-583.
121. Werner RM, Goldman LE, Dudley RA. Comparison of change in quality of care between safety-net and non-safety-net hospitals. JAMA. 2008;299(18):2180-2187.
122. Chien AT, Wroblewski K, Damberg C, et al. Do physician organizations located in lower socioeconomic status areas score lower on pay-for-performance measures? J Gen Intern Med. 2012;27(5):548-554.
123. Casalino LP, Elster A, Eisenberg A, et al. Will pay-for-per-formance and quality reporting affect health care dispari-ties? Health Aff (Millwood). 2007;26(3):w405-414. Erratum in Health Aff (Millwood). 2007;26(6):1794.
124. Werner RM. Does pay-for-performance steal from the poor and give to the rich? Ann Intern Med. 2010;153(5):340-341.
125. Carrier ER, Schneider E, Pham HH, et al. Association between quality of care and the sociodemographic compo-sition of physicians’ patient panels: a repeat cross-sectional analysis. J Gen Intern Med. 2011;26(9):987-994.
126. Blustein J, Weissman JS, Ryan AM, et al. Analysis raises questions on whether pay-for-performance in Medicaid can efficiently reduce racial and ethnic disparities. Health Aff (Millwood). 2011;30(6):1165-1175.
127. Jha AK, Joynt KE, Orav EJ, et al. The long-term effect of premier pay for performance on patient outcomes. N Engl J Med. 2012;366(17):1606-1615.
128. Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007;356(5):486-496.
129. Ryan A, Blustein J. Making the best of hospital pay for per-formance. N Engl J Med. 2012;366(17):1557-1559.
130. The Patient Protection and Affordable Care Act. American Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/policy/federal/issues/reform/ppaca.html. Accessed December 2012.
131. Principles for reform of the U.S. health care system. Ameri-can Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/membership/initia-tives/hrsprinciples.html. Accessed December 2012.
132. The value of primary care and family physicians. American Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/aboutus/theaafp/business.html. Accessed December 2012.
133. PCMH definition and selected results by PCMH feature. In: Nielsen M, Langner B, Zema C, et al. Benefits of Implement-ing the Primary Care Patient-Centered Medical Home: A Review of Cost and Quality Results, 2012. Washington, DC: Patient-Centered Primary Care Collaborative; 2012:14-30. Available at http://www.pcpcc.net/files/benefits_of_imple-menting_the_primary_care_pcmh.pdf. Accessed December 2012.
134. Medicare physician payment. American Academy of Fam-ily Physicians Web site. Available at http://www.aafp.org/online/en/home/policy/federal/issues/reform/payment.html. Accessed December 2012.

44
Healthcare Reform
135. AAFP statement: AAFP commends CMS for improving Medicare ACO final rule, announcing the Advance Payment Model. American Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/media/releases/2011newsreleases-statements/aco-final-rule.html. Accessed December 2012.
136. The RVS Update Committee. American Medical Association Web site. Available at http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/the-resource-based-rela-tive-value-scale/the-rvs-update-committee.page. Accessed December 2012.
137. RBRVS: Resource-Based Relative Value Scale. American Medical Association Web site. Available at http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/the-resource-based-relative-value-scale.page. Accessed December 2012.
138. Porter S. Academy goes on record strongly urging changes in RUC structure, process. AAFP News Now. June 10, 2011. Available at http://www.aafp.org/online/en/home/publications/news/news-now/practice-professional-issues/20110610rucletter.html. Accessed December 2012.
139. Goertz R. Stating our case to the RUC. American Academy of Family Physicians Leader Voices [blog post]. September 26, 2011. Available at http://blogs.aafp.org/cfr/leadervoices/entry/stating_our_case_to_the. Accessed December 2012.
140. Klepper B, Kibbe DC. Quit the RUC. Kaiser Health News. January 20, 2011. Available at http://www.kaiserhealth-news.org/columns/2011/january/012111kepplerkibbe.aspx?referrer=search. Accessed December 2012.
141. Mathews AW, McGinty T. Physician panel prescribes the fees paid by Medicare. The Wall Street Journal. October 26, 2010. Available at http://online.wsj.com/article/SB10001424052748704657304575540440173772102.html. Accessed December 2012.
142. Reinhardt UE. The little-known decision-makers for Medicare physicians fees. The New York Times Economix [blog post]. December 10, 2010. Available at http://economix.blogs.nytimes.com/2010/12/10/the-little-known-decision-makers-for-medicare-physicans-fees/. Accessed December 2012.
143. Fischer PM. Why medical specialists should want to end the reign of the RUC. Replace the RUC [blog post]. August 16, 2011. Available at http://www.replacetheruc.org/2011/08/16/why-medical-specialists-should-want-to-end-the-reign-of-the-ruc/. Accessed December 2012.
144. Klepper B, Fischer P, Behan KA. Stifling primary care: why does CMS continue to support the RUC. The Health Care Blog [blog post]. May 25, 2011. Available at http://thehealth-careblog.com/blog/2011/05/25/stifling-primary-care/. Accessed December 2012.
145. Stream G. We’re changing our approach to the RUC. As We See It: Voices from the AAFP [blog post]. March 16, 2012. Available at http://www.aafp.org/online/en/home/publica-tions/news/news-now/opinion/20120316presmessonruc.html. Accessed December 2012.
146. Klepper B, Keppe D. A legal challenge to CMS’ reliance on the RUC. Health Affairs Blog [blog post]. August 9, 2011. Available at http://healthaffairs.org/blog/2011/08/09/a-legal-challenge-to-cms-reliance-on-the-ruc/. Accessed December 2012.
147. Arvantes J. Primary care physicians file lawsuit to bring more transparency to RUC process. AAFP News Now. August 12, 2011. Available at http://www.aafp.org/online/en/home/ publications/news/news-now/government-medicine/2011 0812ruclawsuit.html. Accessed December 2012.
148. Fischer v Berwick, (D Md 2012), F Supp.
149. Electronic health records. American Academy of Family Phy-sicians Web site. Available at http://www.aafp.org/online/en/home/policy/policies/e/electronichealth.html. Accessed December 2012.
150. Information technology used in health care. American Acad-emy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/policy/policies/i/infotechinhtlh-care.html. Accessed December 2012.
151. Medical informatics. American Academy of Family Physi-cians Web site. Available at http://www.aafp.org/online/en/home/policy/policies/m/medicalinformatics.html. Accessed December 2012.
152. Mather RC, Hettrich C, Nunley R. Penalties coming under PPACA, PQRI. AAOS Now. January 2011. Available at http://www.aaos.org/news/aaosnow/jan11/advocacy2.asp. Accessed December 2012.
153. Joint letter to CMS regarding upcoming penalties. AAFP News Now. March 28, 2012. Available at http://www.aafp.org/online/etc/medialib/aafp_org/documents/policy/fed/statements/cms032812.Par.0001.File.dat/PenaltiesLetter 032812.pdf. Accessed December 2012.
154. Health care research and quality. American Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/policy/federal/issues/reform/quality.html. Accessed December 2012.
155. Public comment on PCORI national priorities for research and research agenda. American Academy of Family Physi-cians Web site. Available at http://www.aafp.org/online/etc/medialib/aafp_org/documents/policy/fed/statements/pcori031412.Par.0001.File.tmp/PCORI031412.pdf. Accessed December 2012.
156. Medical liability reform. American Academy of Family Physi-cians Web site. Available at http://www.aafp.org/online/etc/medialib/aafp_org/documents/policy/fed/background/mlr120610.Par.0001.File.tmp/Medical-Liability-June-2011.pdf. Accessed December 2012.
157. Health insurance consolidation. American Academy of Fam-ily Physicians Web site. Available at http://www.aafp.org/online/en/home/policy/federal/issues/reform/insurance.html. Accessed December 2012.
158. Medical education and the shortage of primary care physi-cians. American Academy of Family Physicians Web site. Available at http://www.aafp.org/online/en/home/media/browse/advocacy/aafp-advocacy-focus/education-short-age.html. Accessed December 2012.

References
159. American Academy of Family Physicians. Family Physician Workforce Reform: Recommednations of the American Academy of Family Physicians. Leawood, KS: AAFP; Sep-tember 2009. Available at http://www.aafp.org/online/en/home/policy/policies/w/workforce.html. Accessed Decem-ber 2012.
160. Expansion of residency training programs at federally quali-fied community health centers (FQHCs). American Academy of Family Physicians Web site. July 2007. Available at http://www.aafp.org/online/en/home/policy/policies/e/exprestrng-programs.html. Accessed December 2012.
161. Policy priorities to improve the nation’s health: from Amer-ica’s medical schools and teaching hospitals. Association of American Medical Colleges Web site. December 2008. Available at https://www.aamc.org/download/48286/data/obamatransition.pdf. Accessed December 2012.
162. Ackermann RT, Carroll AE. Support for national health insur-ance among U.S. physicians: a national survey. Ann Intern Med. 2003;139(10):795-801.
163. Carroll AE, Ackerman RT. Support for national health insur-ance among U.S. physicians: 5 years later. Ann Intern Med. 2008;148(7):566-567.
164. Keyhani S, Federman A. Doctors on coverage—physicians’ views on a new public insurance option and Medicare expansion. N Engl J Med. 2009;361(14):e24.
165. Washington Post-ABC news poll: health care. The Washing-ton Post. October 20, 2003. Available at http://www.washing-tonpost.com/wp-srv/politics/polls/vault/stories/data102003.html. Accessed December 2012.
166. Henry J. Kaiser Family Foundation. Public opinion on health-care issues. Kaiser Health Tracking Poll. February 2010. Available at http://www.kff.org/kaiserpolls/upload/8051-F.pdf. Accessed December 2012.
167. Newport F. Obama approval on economy down, on foreign affairs up. Gallup Politics. February 8, 2010. Available at http://www.gallup.com/poll/125678/Obama-Approval-Econ-omy-Down-Foreign-Affairs-Up.aspx. Accessed December 2012.
168. Health care reform: it’s time to decide, and 54% of voters oppose the health care plan. Rasmussen Reports. March 2010. Available at http://www.rasmussenreports.com/public_content/politics/current_events/healthcare/septem-ber_2009/health_care_reform. Accessed December 2012.
169. August Kaiser health tracking poll: a look at the GOP as the Republican convention draws near. Health Reform Source. August 2012. Available at http://healthreform.kff.org/public-opinion.aspx. Accessed December 2012.
170. Henry J. Kaiser Family Foundation. Early reaction to Supreme Court decision on the ACA. Kaiser Health Track-ing Poll. July 2010. Available at http://www.kff.org/kaiser-polls/8329.cfm. Accessed December 2012.
Online ResourcesHealth Care Reform: The Patient Protection and Affordable Care Act & American Academy of Family Physicians and Health Care Reform
American Academy of Family Physicians AAFP News Now Web site: http://www.aafp.org/online/en/home/publications/news/news-now.html
Policy & Advocacy Web site: http://www.aafp.org/online/en/home/policy.html
Society of Teachers of Family Medicine Advocacy in Action Web site: http://www.stfm.org/advocacy/index.cfm
Health Affairs Blog Web site: http://healthaffairs.org/blog/
Kaiser Family Foundation Web site: http://www.kff.org/
Health Reform Source Web site: http://healthreform.kff.org/
Implementation Timeline Web site: http://healthreform.kff.org/timeline.aspx
Health Reform Subsidy Calculator Web site: http://healthreform.kff.org/SubsidyCalculator.aspx
Kaiser Health News Web site: http://www.kaiserhealthnews.org/
New England Journal of Medicine Health Policy and Reform Web site: http://healthpolicyandreform.nejm.org/
New York Times Health Section Web site: http://www.nytimes.com/pages/health/index.html
Washington Post Wonkblog, Ezra Klein Web site: http://www.washingtonpost.com/blogs/ezra-klein
Accountable Care Organizations
American Academy of Family Physicians Frequently asked questions Web site: http://www.aafp.org/online/en/home/practicemgt/ specialtopics/designs/practiceaffiliationoptions/faq.html
American Academy of Family Physicians, the American Acad-emy of Pediatrics, the American College of Physicians, and the American Osteopathic Association
Joint principles of ACOs Web site: http://www.acponline.org/advocacy/where_we_stand/other_issues/aco-principles-2010.pdf
Centers for Medicare & Medicaid Services Introductory video, synopsis, and links to frequently asked questions Web site: http://www.cms.gov/aco
Web sites accessed December 2012.

46
Healthcare Reform
Suggested ReadingHealth Care Reform: The Patient Protection and Affordable Care Act & American Academy of Family Physicians and Health Care Reform
Epperly T. Fractured. 1st ed. New York: Sterling & Ross Publish-ers; 2012.
Jonas S, Goldsteen R, Goldsteen K, eds. An Introduction to the U.S. Health Care System. 6th ed. New York: Springer Publishing Company; 2007.
Washington Post Staff. Landmark : The Inside Story of America’s New Health-Care Law and What it Means for Us All. 1st ed. New York: PublicAffairs; 2010.
Accountable Care Organizations
American Academy of Family Physicians; American Acad-emy of Pediatrics; American College of Physicians; American Osteopathic Association. Joint Principles for Accountable Care Organizations. November 19, 2010. Available at http://www.acponline.org/advocacy/where_we_stand/other_issues/aco-principles-2010.pdf. Accessed December 2012.
American Medical Association Practice Center Management. ACOs, CO-OPs and Other Options: A “How-To” Manual for Physi-cians Navigating A Post-Health Reform World. 3rd ed. Chicago: AMA; 2012.
Berenson R, Burton R. Next steps for ACOs. Health Affairs. Janu-ary 31, 2012. Available at http://www.healthaffairs.org/healthpoli-cybriefs/brief.php?brief_id=61. Accessed December 2012.
Bobbitt JD. What family physicians need to know about ACOs. Fam Pract Manag. 2011;18(5):17-22.
Fisher ES, Shortell SM. Accountable care organizations: account-able for what, to whom, and how. JAMA. 2010;304(15):1715-1716.
Hossain F. How different types of people will be affected by the health care overhaul. New York Times. March 24, 2010. Available at http://www.nytimes.com/interactive/2010/03/24/us/politics/20100319-health-care-effect.html?ref=business. Accessed December 2012.
Kocher R, Sahni NR. Physicians versus hospitals as lead-ers of accountable care organizations. N Engl J Med. 2010;363(27):2579-2582.
Mackinney AC, Mueller KJ, McBride TD. The march to account-able care organizations—how will rural fare? J Rural Health. 2011;27(1):131-137.
Porter S. AAFP and other primary care associations release joint principles for accountable care organizations. Ann Fam Med. 2011;9(1):87-88.
Pay for performance
Averill RF, Hughes JS, Goldfield NI. Paying for outcomes, not per-formance: lessons from the Medicare Inpatient Prospective Pay-ment System. Jt Comm J Qual Patient Saf. 2011;37(4):184-192, 145.
de Bruin SR, Baan CA, Struijs JN. Pay-for-performance in dis-ease management: a systematic review of the literature. BMC Health Serv Res. 2011;11:272.
Gavagan TF, Du H, Saver BG, et al. Effect of financial incentives on improvement in medical quality indicators for primary care. J Am Board Fam Med. 2010;23(5):622-631.
Pay for performance. American Academy of Family Physicians Web site. 2010. Available at http://www.aafp.org/online/en/home/policy/policies/p/payforperformance.html.
Qaseem A, Snow V, Gosfield A, et al. Pay for performance through the lens of medical professionalism. Ann Intern Med. 2010;152(6):366-369.
Scott A, Sivey P, Ait Ouakrim D, et al. The effect of financial incentives on the quality of health care provided by primary care physicians. Cochrane Database Syst Rev. 2011;(9):CD008451.
Van Herck P, De Smedt D, Annemans L, et al. Systematic review: effects, design choices, and context of pay-for-performance in health care. BMC Health Serv Res. 2010;10:247.
Werner RM. Does pay-for-performance steal from the poor and give to the rich? Ann Intern Med. 2010;153(5):340-341.
Witter S, Fretheim A, Kessy FL, et al. Paying for performance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database Syst Rev. 2012; (2):CD007899.

47
1.
❏
❏
❏
❏
2.
❏❏❏❏
3.
❏❏❏❏
4.
❏
❏
❏❏ fix to the
❏
5. mandate within the Patient Protection and
❏
❏
❏
❏
6.
❏
❏
❏
❏
7. of the triple aim
❏
❏
❏
❏
Posttest Questions
Complete the online quiz at http://www.aafp.org/fpequiz.

Health Care Reform
48
8.
❏
❏
❏
❏
9.
❏❏❏
❏
10.
❏❏❏❏
11.
❏
❏
❏
PPACA.❏
❏
12.
❏
❏
❏
❏ of health care systems.
❏
13.
❏❏
data.❏❏
14.
❏
❏
❏
❏
❏

Posttest Questions
15.
❏
❏
❏
❏
16.
❏ rate fix
❏
❏medical home as the model of care that
❏
health care.❏
17.
❏
❏
❏
❏
model of care.
18. The American Academy of Family Physicians
❏
❏
❏
❏
❏
19. The American Academy of Family Physicians is
❏❏❏❏
❏
20. American Academy of Family Physicians for medical
❏❏
❏❏

Question 1: The correct answer is B.
-
See page 13.
Question 2: The correct answer is A.
actuarial value
See page 14.
Question 3: The correct answer is D.
a medical loss
- See page 15.
Question 4: The correct answer is E.
-
See page 15.
Question 5: The correct answer is A.
shared responsibility payment. See page 18.
Question 6: The answer is D.
See page 22.
Question 7: The correct answer is C.
consistent with what is often called the triple aim of
See page 23.
Question 8: The correct answer is B.
See page 22.
Question 9: The correct answer is C.-
See page 23 and Table 5.
Question 10: The correct answer is C.A shared risk
See page 27.
Question 11: The correct answer is A.
See page 28.
Question 12: The correct answer is A.-
-
See page 29.
Question 13: The correct answer is B.
- See page 29.
Posttest Answers

Posttest Answers
Question 14: The correct answer is A.-
See page 32.
Question 15: The correct answer is B.
-
safety-net
. See page 32.
Question 16: The correct answer is E.The American Academy of Family Physicians has stated
-
-
-
See page 35.
Question 17: The correct answer is A.-
See page 35.
Question 18: The correct answer is A.-
See page 36.
Question 19: The correct answer is A.
See page 37.
Question 20: The correct answer is A.
See page 37.

Notes

The following topics appear in this month’s edition of the AAFP program:
Clinical Topic:
Clinical Topic: Journal Notes:
Editor’s Q&A:
The next edition of AAFP will be:
Common Fractures