-
7/23/2019 4-hypovolemic-shock.ppt
1/21
HYPOVOLEMIC SHOCK
University of Medicine and Pharmacy, Iasi
School of Medicine
ANESTHESIA and INTENSIVE CARE
Conf. Dr. Ioana Grigoras
MEDICINE
4th year
English Program
Suport de curs
-
7/23/2019 4-hypovolemic-shock.ppt
2/21
HYPOVOLEMIC SHOCK
DEFINITION syndrom characterized by decreased circulating
blood
volume (hypovolemia), which results in reduction ofeffective
tissue perfusion pressure and generalizedcellular dysfunctions.
Forms:
Hemorrhagic shock
Non-hemorrhagic hypovolemic shock
-
7/23/2019 4-hypovolemic-shock.ppt
3/21
HYPOVOLEMIC SHOCKCAUSES:
Hemorrhagic:External blood loss (wounds)
Exteriorization of internal bleeding (hematemesis, melena,
epistaxis,
hemoptysis,etc.)
Internal bleeding (hemothorax, hemoperitoneum,etc. )
Traumatic shock
Non-hemorrahagic:Digestive losses (vomiting, diarrhea,
nasogastric suction, billiary, digestive
fistula, etc )
Renal losses (diabetes mellitus, polyuria caused by diuretics
overdose,
osmotic substances, polyuric phase of acute renal failure,
etc.)
Skin losses (intense physical effort, overheated enviroment,
burns, etc.)
Third space losses (peritonites, intestinal oclussion,
pancreatits, ascitispleural effusions, etc.)
-
7/23/2019 4-hypovolemic-shock.ppt
4/21
PATHOPHYSIOLOGY
Primary pathophysiological event(reduction of ventr icular f i l
l ing volumes and pressures)
compensatory phenomena macrocirculatory reaction
time
decompensatory phenomena microcirculatory reaction
-
7/23/2019 4-hypovolemic-shock.ppt
5/21
PATHOPHYSIOLOGYHypodynamic shock:
Macrocirculatory reaction: sympatho-adrenergic + humoral
reaction (ADH, cortizol, SRAA)
o EFFECTS: centralisation of the circulation (compensatory
effect)
worsening of tisular hypoperfusion (decompensatory effect)
Microcirculatory reaction: Alterations of capillary
exchanges
o EFFECTS: transcapilary filling (compensatory effect)
capilary leak (decompensatory effect) Maldistribution of blood
flow
o EFFECTS: preferential renal blood flow towards medular region
(corticalvasoconstriction)
Abnormal peripheral oxygen extractiono EFFECTS: early -
increased (compensatory effect)
late - decreased (decompensatory effect)
Rheologic changeso EFFECTS: blood viscosity, blood flow, CID
Endhotelial modificationso EFFECTS: morpho-functional
modifications
proinflamatory and procoagulatory status,
altered permeability
-
7/23/2019 4-hypovolemic-shock.ppt
6/21
HYPOVOLEMIC SHOCK
CLINICAL SIGNS: Intense thirst
Tachycardia
Tachypnea
Positive orthostatic test
Small pulse wave
hTA (blood hypotension)
Agitation, anxiety , confusion, coma
Oliguria
Cold extremities Profuse sweating
Collapsed peripheral veins
Delayed return of color to the nail bed
+ H istory of hemorrhagic or non-hemorrhagic losses
-
7/23/2019 4-hypovolemic-shock.ppt
7/21
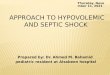
CLASSIFICATION OF HYPOVOLEMIC
SHOCKClass I Class II Class III Class IV
Blood loss- ml < 750ml 750-1500ml 1500-2000ml >2000ml
Blood loss-% 40%
Pulse rate 140/min
BP N N
Pulse wave
amplitude
N
Capillary refill N + + +
Respiratory rate 14-20/min 20-30/min 30-40/min >40/min
Urinary output >30ml/or Oliguria Oligoanuria Anuria
Mental status Mild anxiety Anxiety Confused Lethargy
-
7/23/2019 4-hypovolemic-shock.ppt
8/21
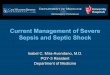
HR BP CO CVP PAOP SVR Da-vO2 SvO2
Hypovolemic
shock
Cardiogenic
shock
Septic shock N N N
DIFFERENTIAL DIAGNOSIS
WITH OTHER FORMS OF SHOCK
-
7/23/2019 4-hypovolemic-shock.ppt
9/21
ABBREVIATIONS: HR heart rate
BP arterial blood pressure CO cardiac output
CVP central venous pressure
PAOP pulmonary artery occlusion pressure
SVR systemic vascular resistance
Da-v O2 oxygen arterial-venous difference
SvO2 mixed venous blood oxygen saturation
-
7/23/2019 4-hypovolemic-shock.ppt
10/21
HYPOVOLEMIC SHOCK
TREATMENT PRINCIPLES
Initial treatment of shock states
Causative treatment STOP losses
Volume repletion
Inotropic therapy Vasomotor therapy
-
7/23/2019 4-hypovolemic-shock.ppt
11/21
TREATMENT OF HYPOVOLEMIC SHOCK
Causative treatmentSTOP losses
essential role
surgical treatment (when appropriate)
emergency surgery for ongoing hemorrhage
-
7/23/2019 4-hypovolemic-shock.ppt
12/21
TREATMENT OF HYPOVOLEMIC SHOCK
volume replacement
Vascular access site Solutions for volume replacement
Rhythm of administration
-
7/23/2019 4-hypovolemic-shock.ppt
13/21
TREATMENT OF HYPOVOLEMIC SHOCK Volume replacementSITE ofVASCULAR
ACCESS
Peripheral vascular access
Multiple access (2-4 veins) Large peripheral catheters
External jugular vein
Advantages: Short time of instalation
Requires basic knowledge and simple matherials
Minor complications (hematomas, cutaneous seroma, etc.)
Disadvantages: The diameter of peripheral catheter must be
adapted for peripheral veins dimensions
Vascular access can be lost (restless patient, during
transportation); must be changed at 24-48hours;
no catecholamines administration (except in emergency for a
short time period,until a centralvenous access is available)
Central venous access
After peripheral vascular access is established and volume
replacement is initiatedAdvantages:
Reliable and long lasting venous access (7-10 days)
Allows CVP measuring and guiding of treatment
Allows the administration of catecholamines and hypertonic
substances
Disadvantages: Risk of complication (at instalationpneumothorax,
cervical or mediastinal hematoma, cardiac
dysrhytmias; during utilizationinfection, gas embolism)
-
7/23/2019 4-hypovolemic-shock.ppt
14/21
TREATMENT OF HYPOVOLEMIC SHOCK
Volume replacement - Solutions for volume
replacement
Isotonic crystalloid solutions
Hypertonic crystalloid solutions Colloid solutions
Whole blood and red blood cells Fresh-frozen plasma
Platelets
-
7/23/2019 4-hypovolemic-shock.ppt
15/21
TREATMENT OF HYPOVOLEMIC SHOCK
Solutions for volume replacement
-I sotonic crystalloid solutions Normal saline (NaCl 0,9 %),
Ringer solution, lactated Ringer solutions
Advantages:
easy available
cheap
reduced risks
Disadvantages: Small volume effect (out of 1000ml infused
solution 250-300ml remains
intravascullarly, the rest is distributed to the interstitial
space)
short duration of volume effect
risk of interstitial edema, metabolic hyperchloremic
acidosis
-Hypertoniccrystall oid solutions
hypertonic saline (NaCl 7,4%)
Advantages:
Ef f icient blood volume resuscitation with small solu tion
volume (water i s atractedfrom intersti tial space )
Avoidance of f luid over load and per ipheral edema
Disadvantages:
may resul t in acute pulmonary edema
-
7/23/2019 4-hypovolemic-shock.ppt
16/21
TREATMENT OF HYPOVOLEMIC SHOCK
Solutions for volume replacementColloid sollutions
Dextrans: Dextran 70, Dextran 40
Gelatines: Gelofusin, Haemacel, Eufusin
Hetastarch: Haes, Voluven, Refortan Human albumin 5%, 20%
Advantages: Good volume effect
Long duration of volume effect
Disadvantages: expensive
r isk for anaphylactic reactions
inter fere with blood groups determination
can induce/ aggravate coagulation disorders
-
7/23/2019 4-hypovolemic-shock.ppt
17/21
TREATMENT OF HYPOVOLEMIC SHOCK
Solution for volume replacementBlood and blood productsare not
volume solutions
Only isogroup isoRh blood
Only after restauration of intravascular volume with cristalloid
/colloid
solutions;
For correction of oxygen transport
In case of posthemorragic anemia (after volume replacement)
orongoing hemorrhage
In case of massive blood transfusionadd fresh-frozen plasma
and
platelet concentrate
-
7/23/2019 4-hypovolemic-shock.ppt
18/21
TREATMENT OF HYPOVOLEMIC SHOCK
Volume replacement
RHYTHM OF ADMINISTRATION
Rhytm of administration depends on: Ongoing losses / stopped
losses
Rhytm of lossesrapid (minutes, hours) or slow (days)
instalation
For the patient with hypotensionnormal saline (2000 ml
in the first 15-30 minutes)
after the first 15-30 minutes - volume replacement
continues depending on the clinical and hymodinamic
parameters (BP, HR, etc..)
-
7/23/2019 4-hypovolemic-shock.ppt
19/21
TREATMENT OF HYPOVOLEMIC SHOCK
Volume replacement
MONITORING THE TREATMENT EFFICIENCY
Clinical parameters normalisation of BP, HR, pulse amplitude,
skin colour and
temperature, mental status, urinary output
Hemodynamic parameters
Normalization of CVP, PCPB, DC, RVS, so
Laboratory parameters
Normalization of acid-base balance, liver, renal tests, Hb i Ht,
so
-
7/23/2019 4-hypovolemic-shock.ppt
20/21
TREATMENT OF HYPOVOLEMIC SHOCK
Inotropic support
Only after volume replacement
Used to improve cardiac output
Dobutamine
inotropic positive support
peripheral arterial vasodilatation
-
7/23/2019 4-hypovolemic-shock.ppt
21/21
TREATMENT OF HYPOVOLEMIC SHOCK
Vasopressor therapy NOT RECOMMENDED (may aggravate
peripheral
hypoperfusion and metabolic acidosis)
EXCEPTIONS
Only temporary
In case of ongoing hemorrhage, which outruns thepossibilities of
volume replacement
Only until surgical procedure stops the hemorrhage(emergency
surgical treatment)
Noradrenaline, dopamine, adrenaline