Embed Size (px)
Citation preview
• 32 year old man• 2 months history of growing left supraclavicular lymph nodes• Antibiotic treatment was not successful• Thoraco-abdominal staging (at first CT, than PET-CT)
Prof. Dr. med. Beata BODE-LESNIEWSKAInstitute of Pathology and Molecular PathologyUniversity Hospital; Zurich
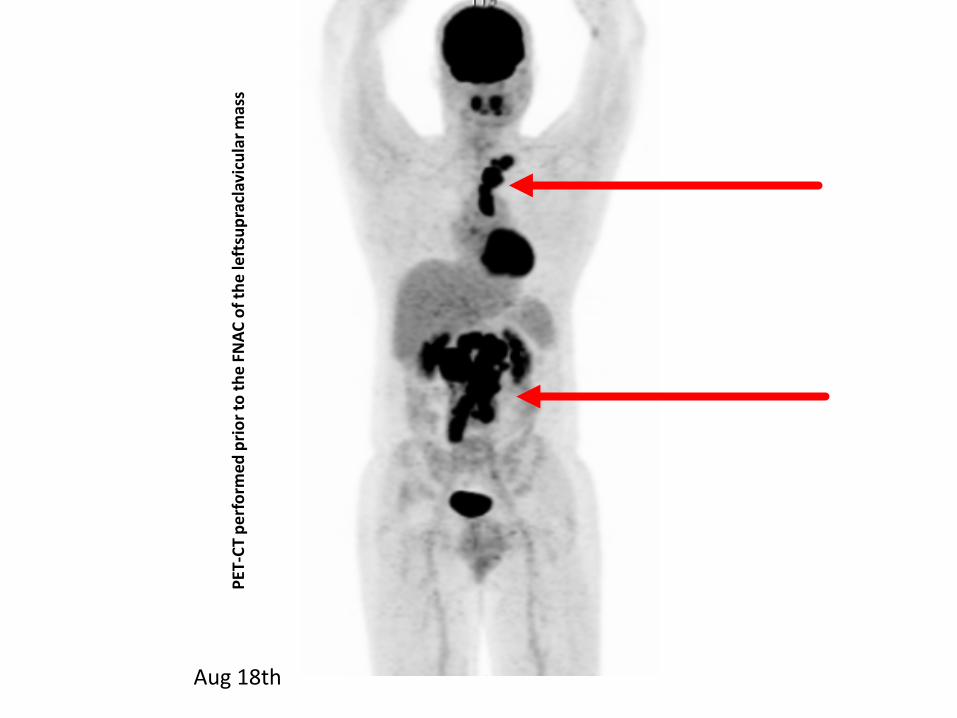
PET-
CT p
erfo
rmed
prio
rto
the
FNAC
of t
hele
ftsu
prac
lavi
cula
rmas
s
Aug 18th
• 32 year old man• 2 months history of growing left supraclavicular
lymph nodes• Antibiotic treatment was not successful• Thoraco-abdominal staging (at first CT, than PET-
CT) showed large retroperitoneal, mediastinal and left supraclavicular tumor masses – based on imaging the strong clinical suspicion of a lymphoma has been rendered.
• Sonographically guided FNAC of the leftsupraclavicular lymph node
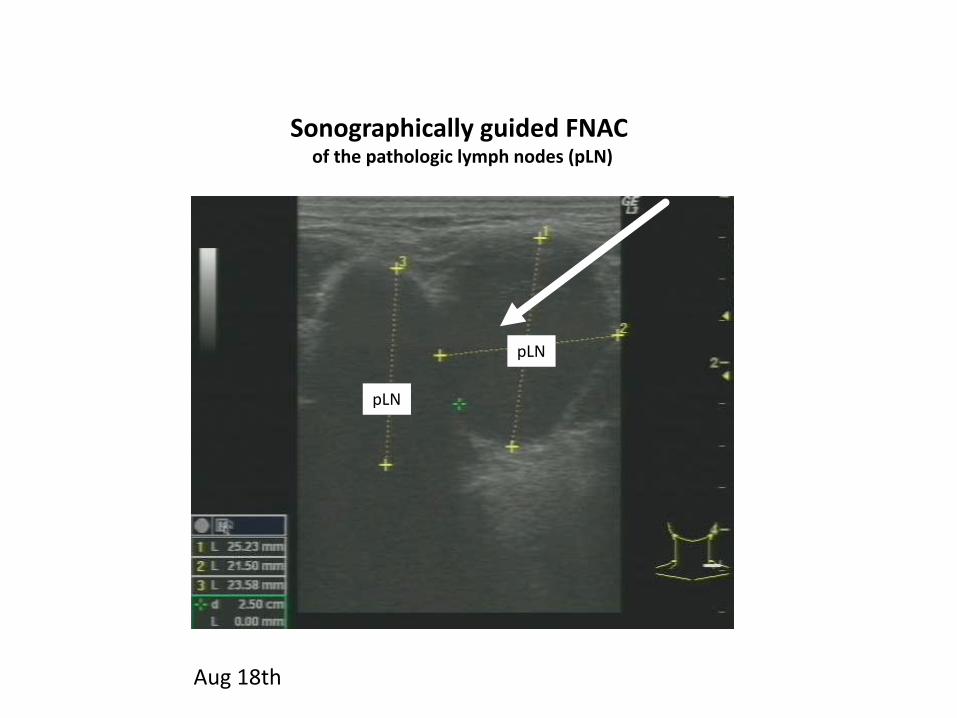
pLN
pLN
Sonographically guided FNAC of the pathologic lymph nodes (pLN)
Aug 18th
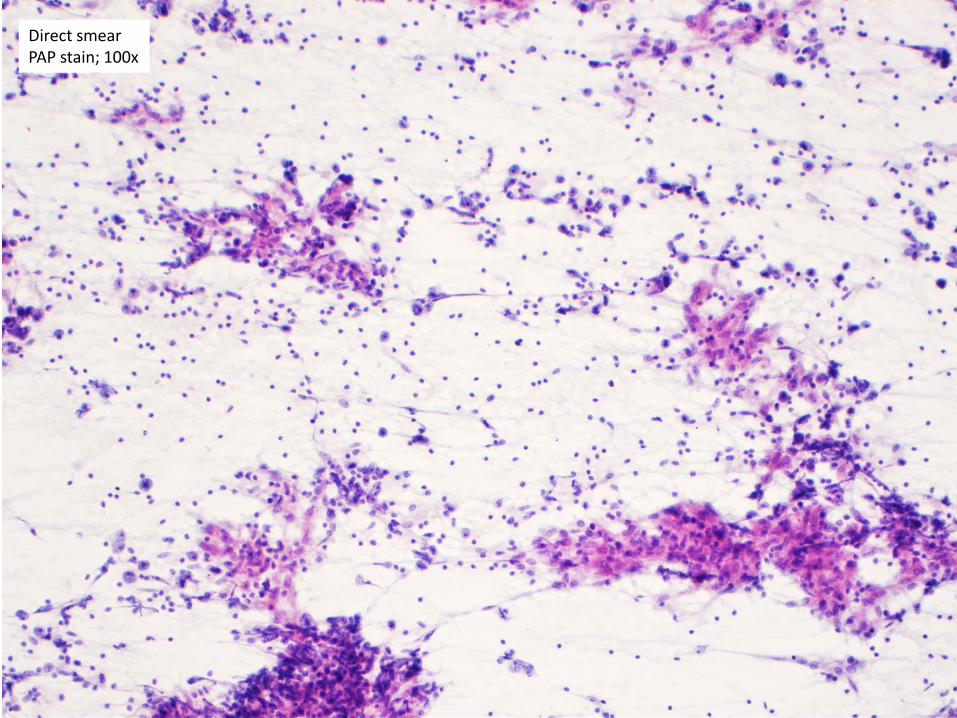
Direct smearPAP stain; 100x
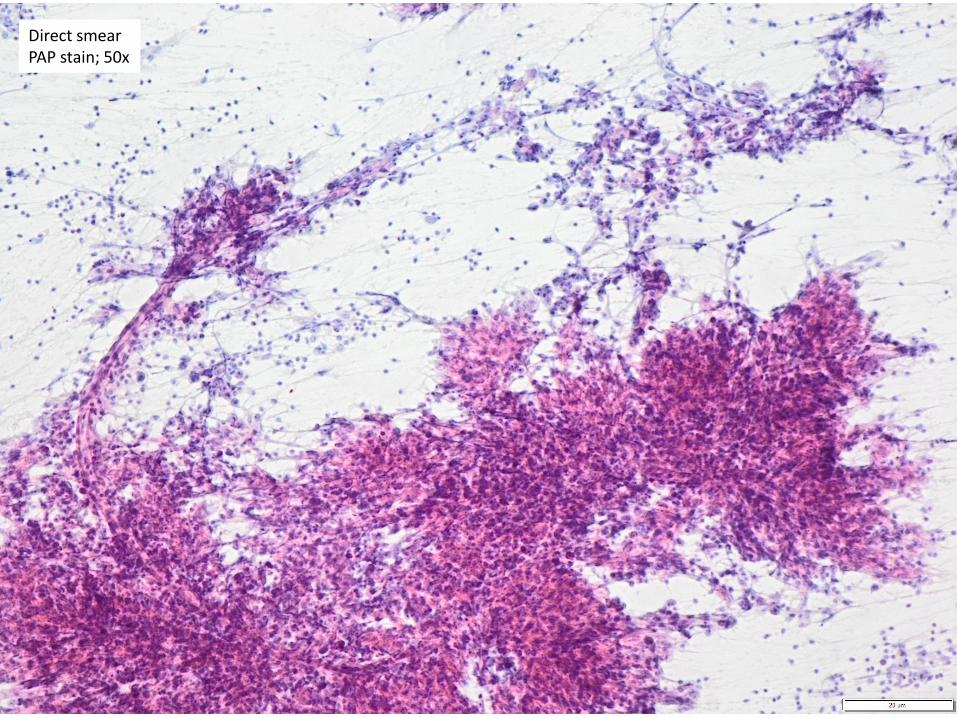
Direct smearPAP stain; 50x
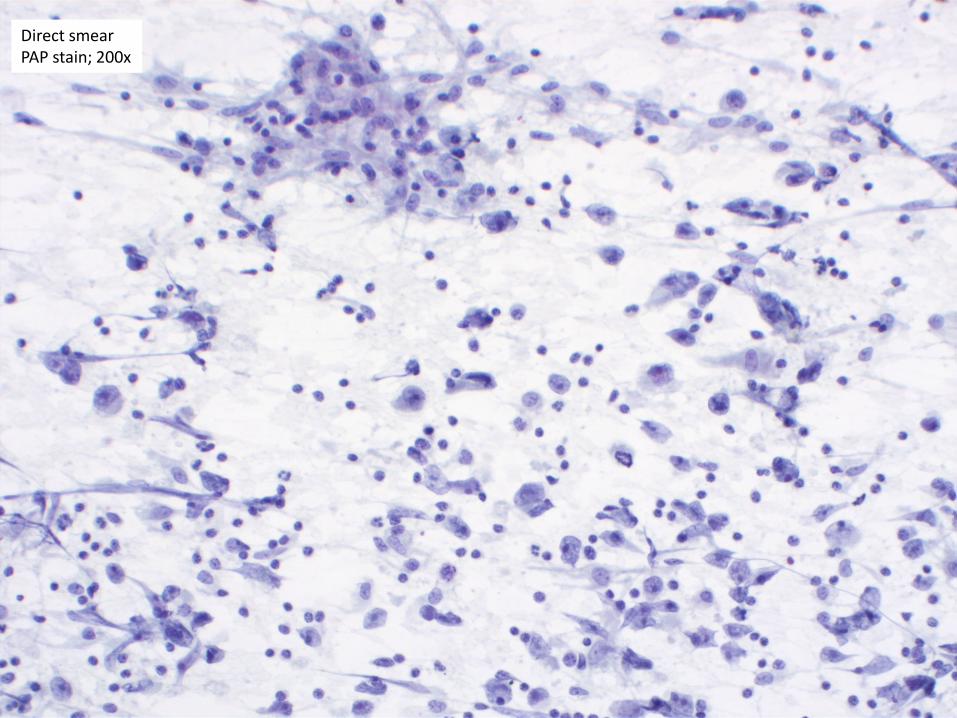
Direct smearPAP stain; 200x
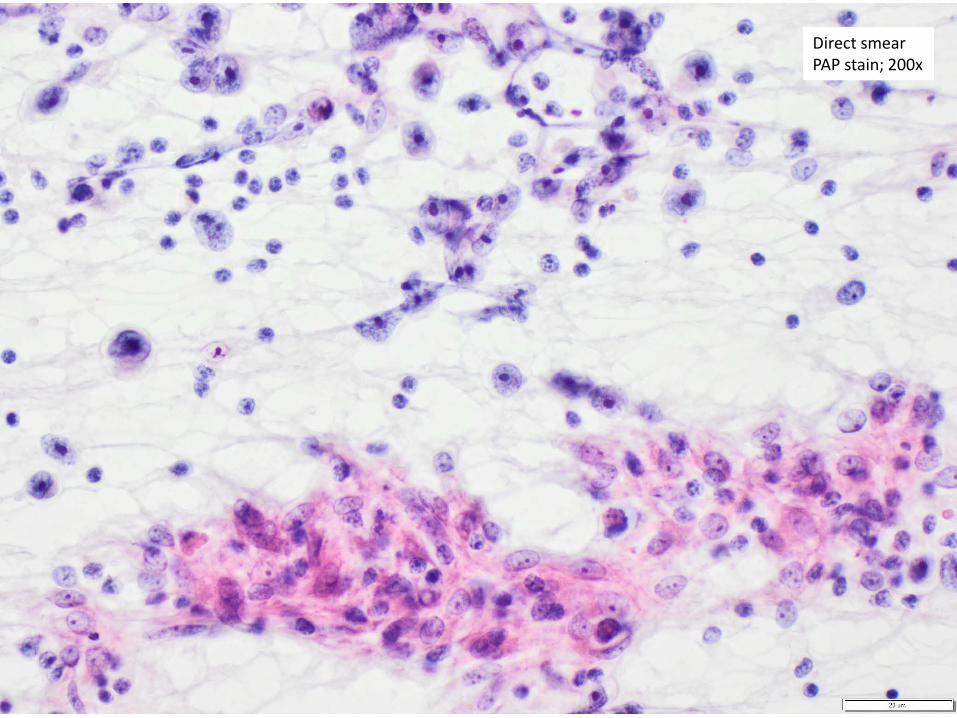
Direct smearPAP stain; 200x
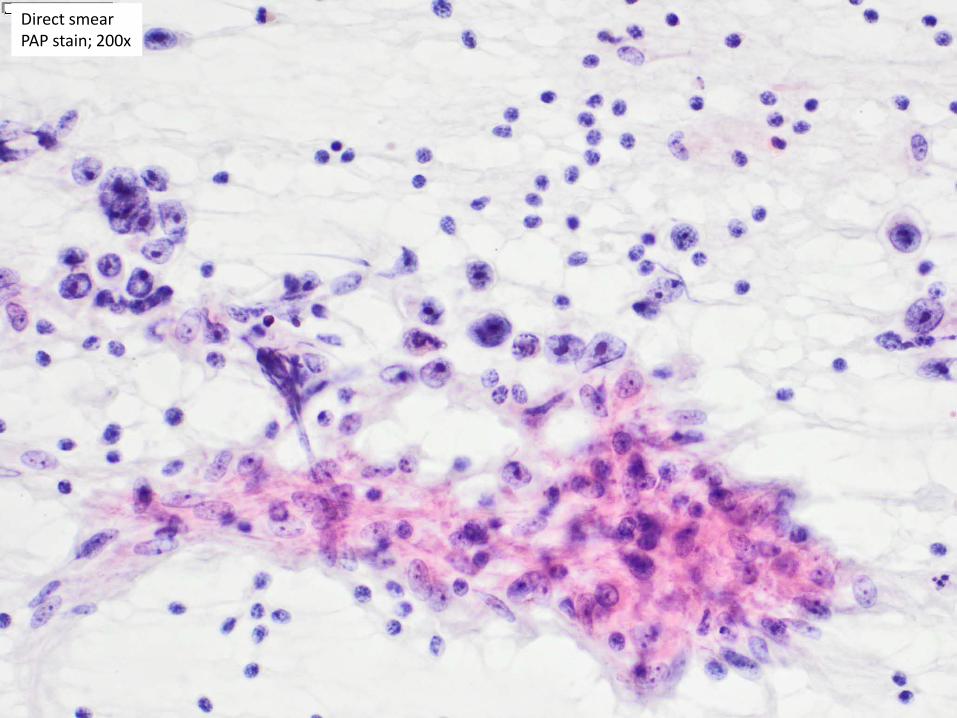
Direct smearPAP stain; 200x
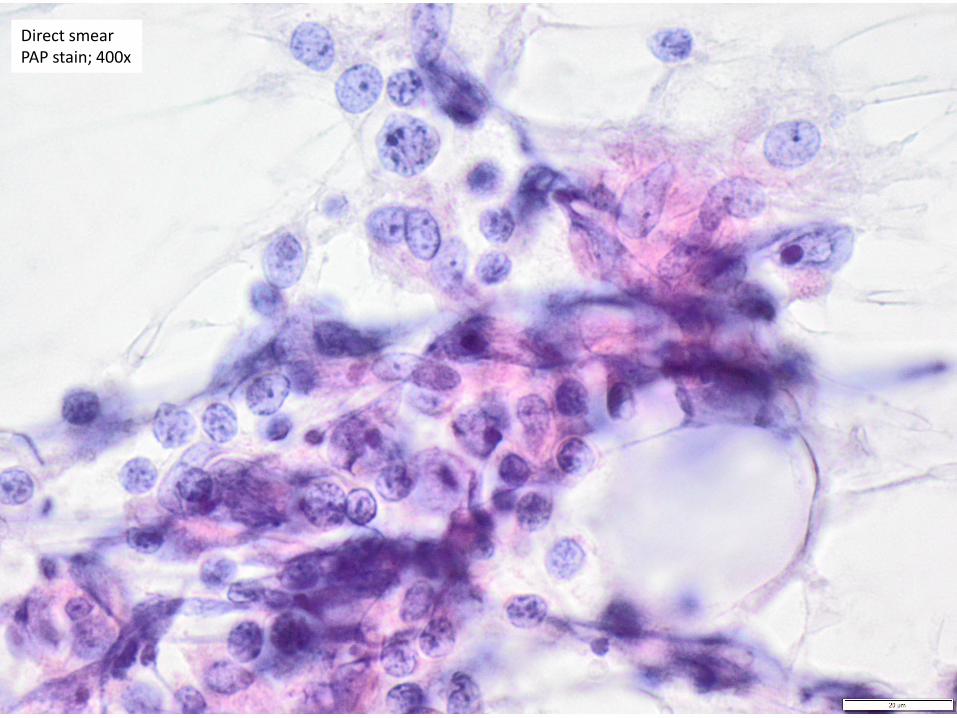
Direct smearPAP stain; 400x
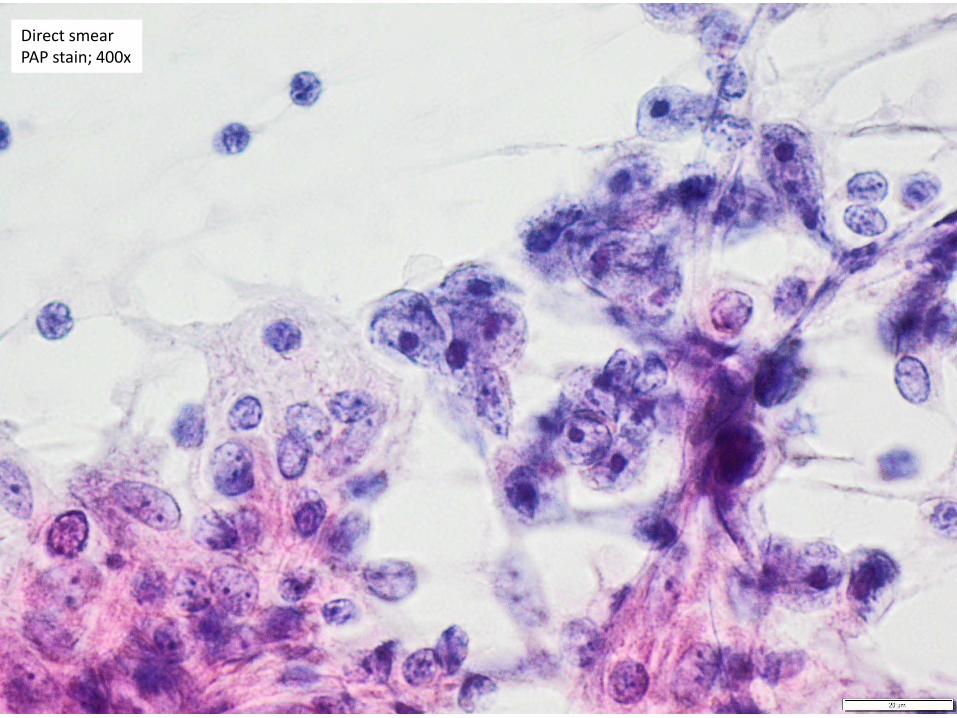
Direct smearPAP stain; 400x
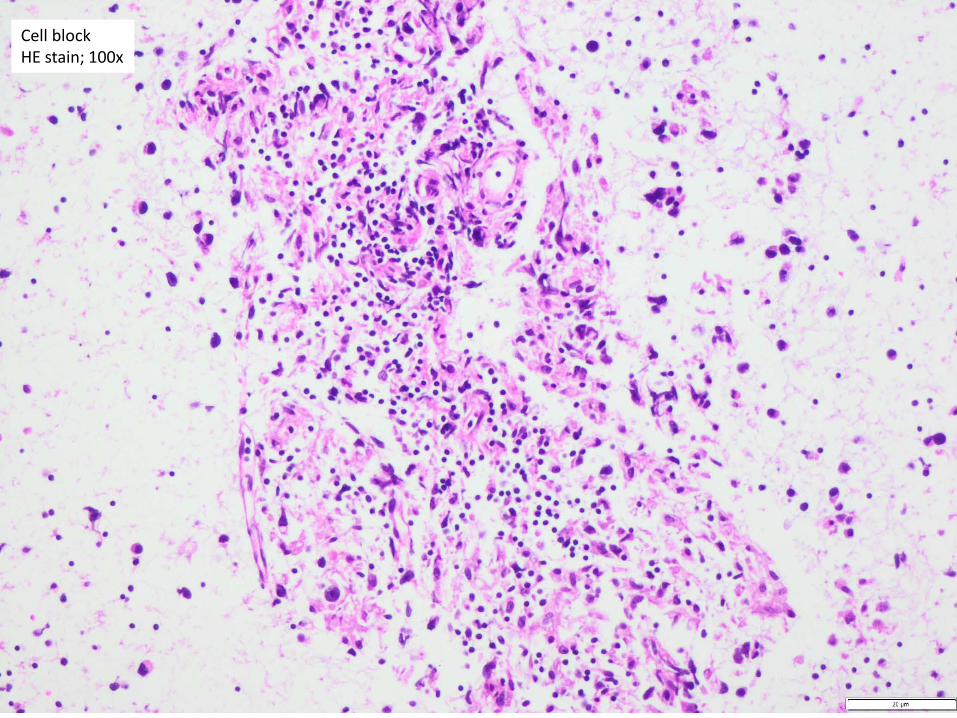
Cell block HE stain; 100x
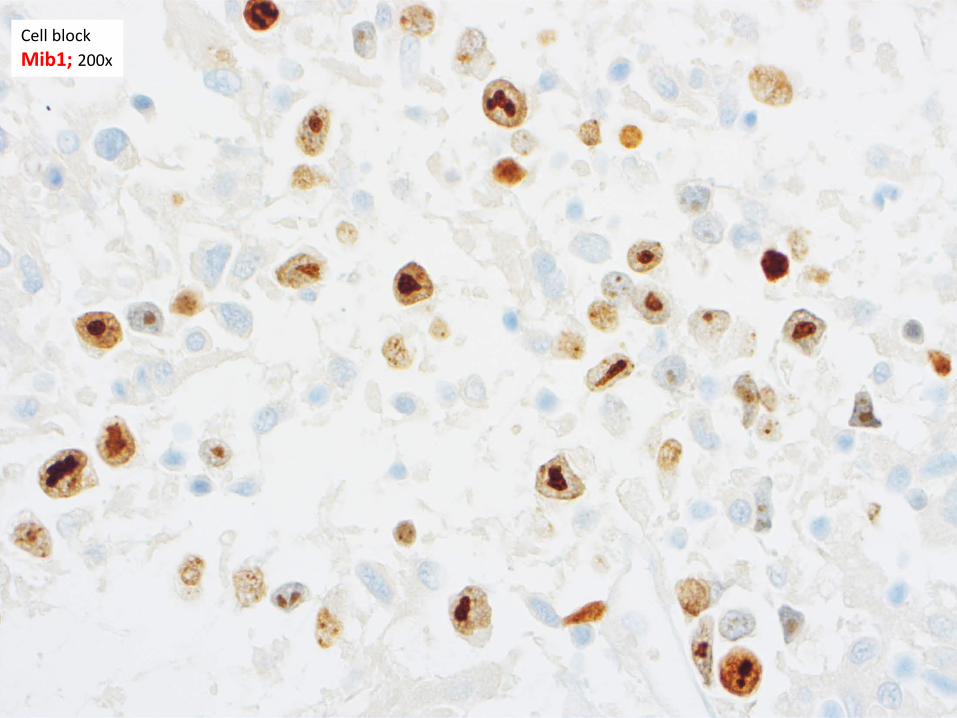
Cell block Mib1; 200x
Differential diagnosis
• Carcinoma• Melanoma• Lymphoma
– Hodgkin– Non-Hodgkin (anaplastic)
• Sarcoma (e.g. epithelioid sarcoma, angiosarcoma, etc…)
• Germ cell tumor
• (Mesothelioma)
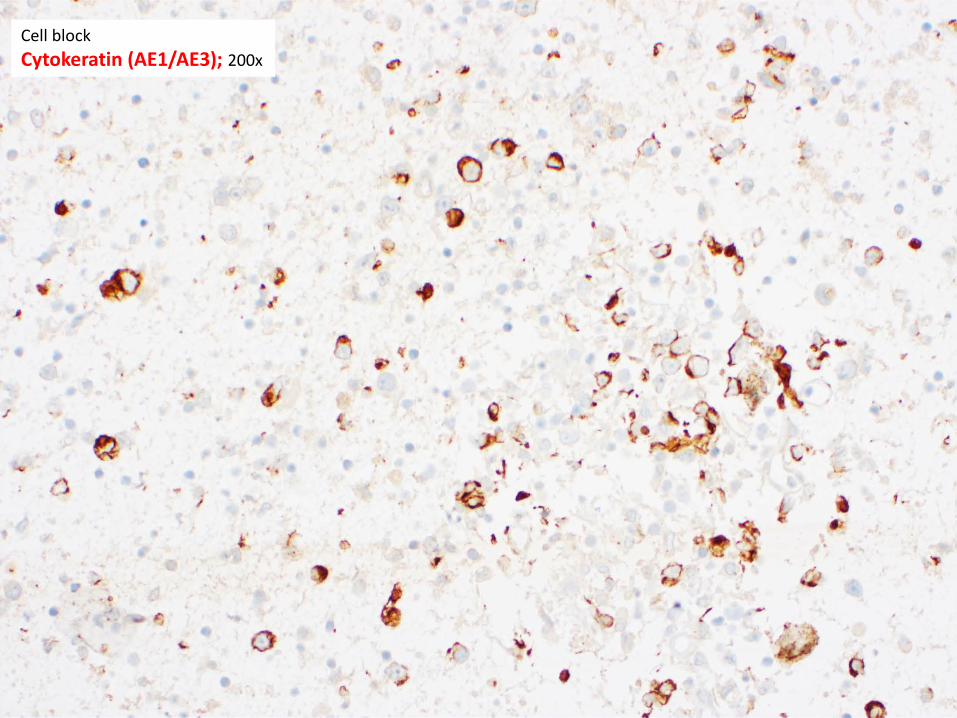
Cell block Cytokeratin (AE1/AE3); 200x
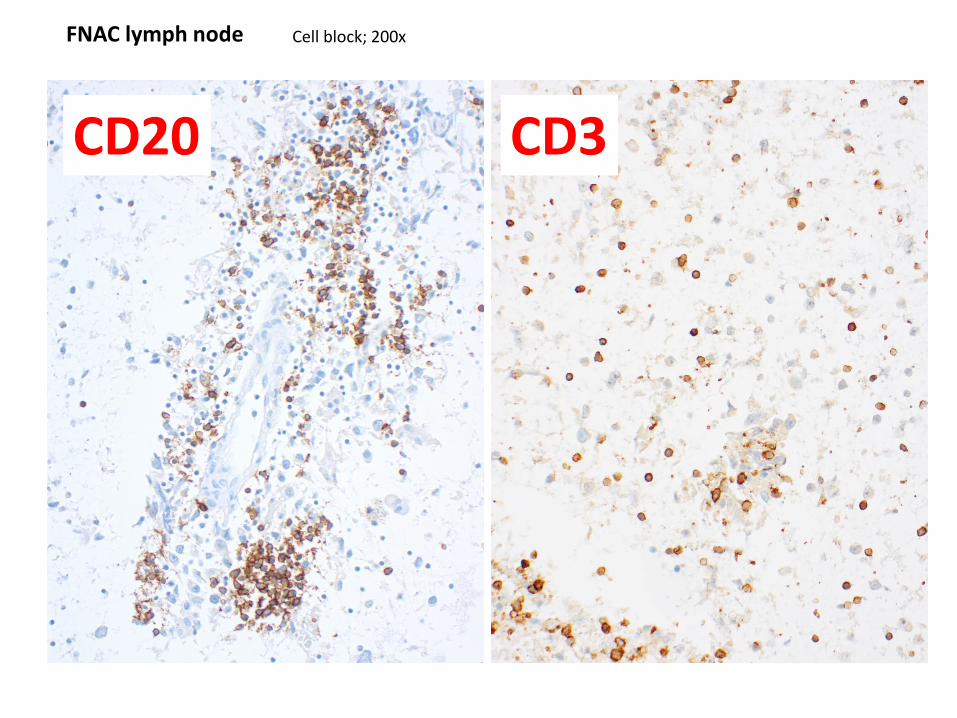
CD3CD20
Cell block; 200xFNAC lymph node
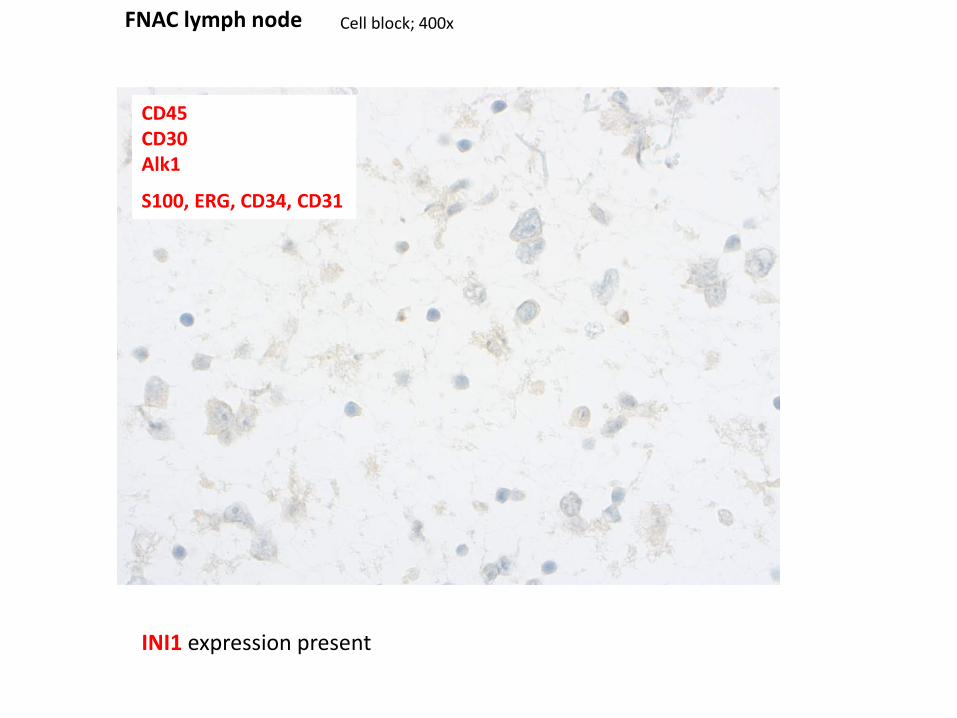
Cell block; 400xFNAC lymph node
CD45CD30Alk1
S100, ERG, CD34, CD31
INI1 expression present
Differential diagnosis
• Carcinoma• Melanoma• Lymphoma
– Hodgkin– Non-Hodgkin
• Sarcoma• Germ cell tumor
• Mesothelioma
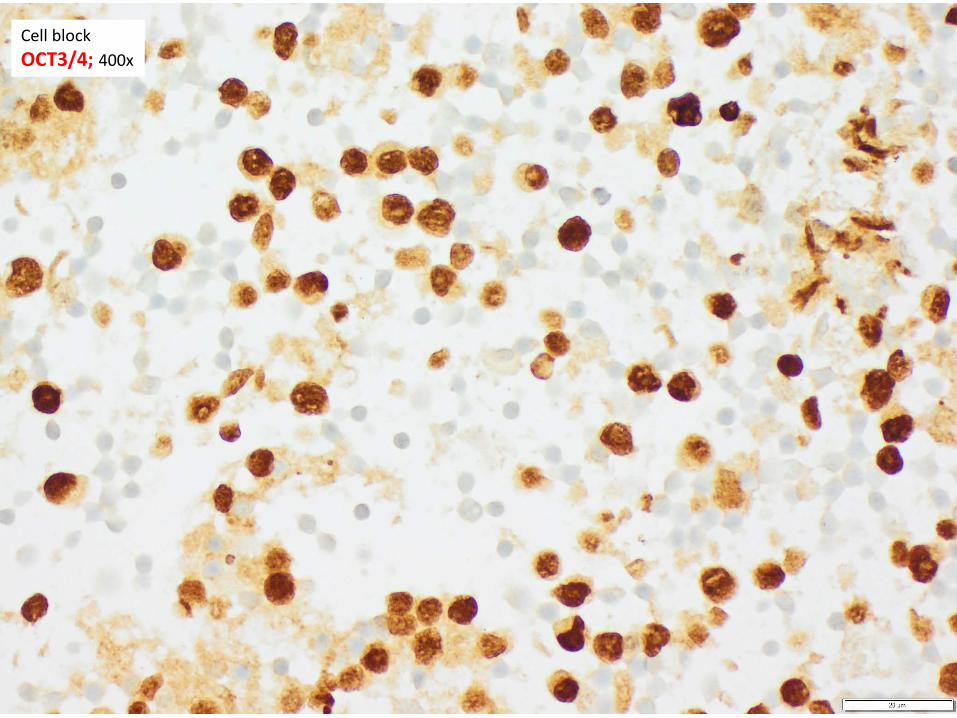
Cell block OCT3/4; 400x
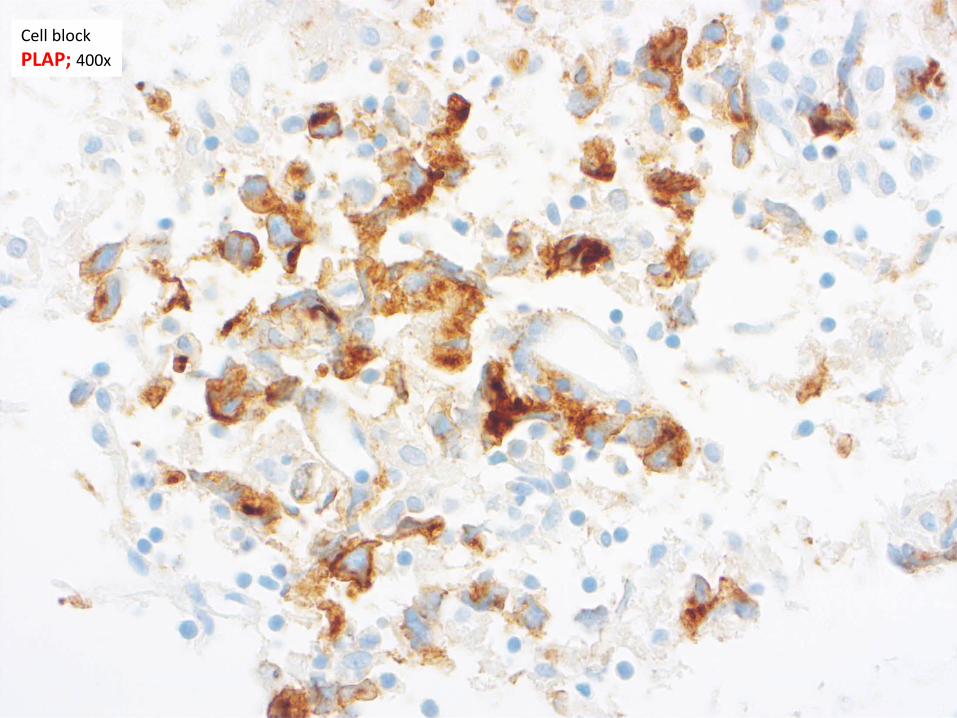
Cell block PLAP; 400x
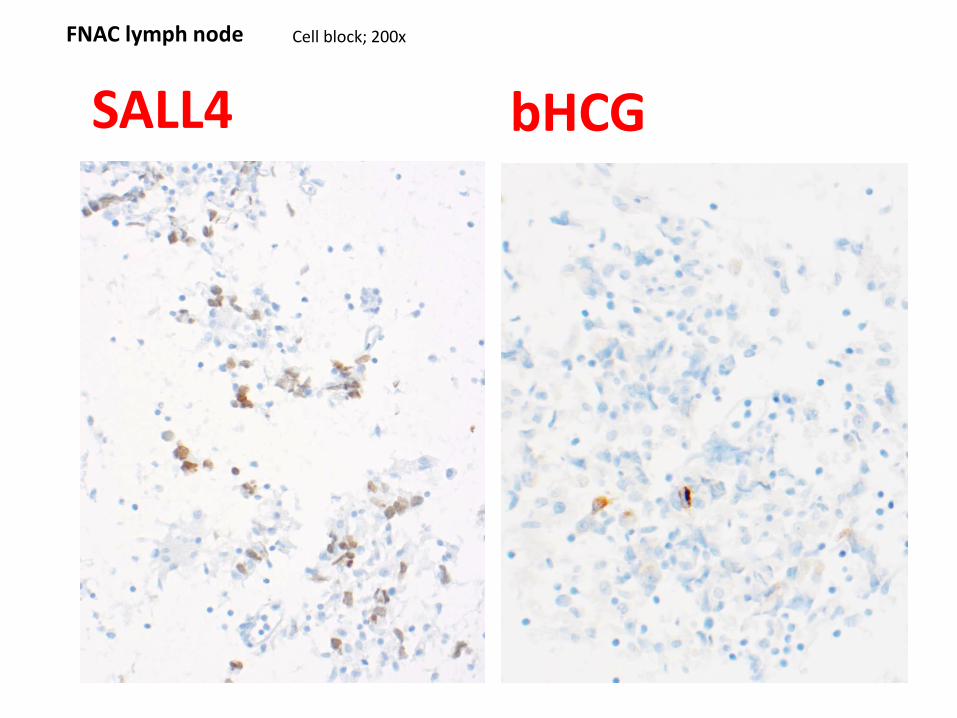
SALL4 bHCGCell block; 200xFNAC lymph node
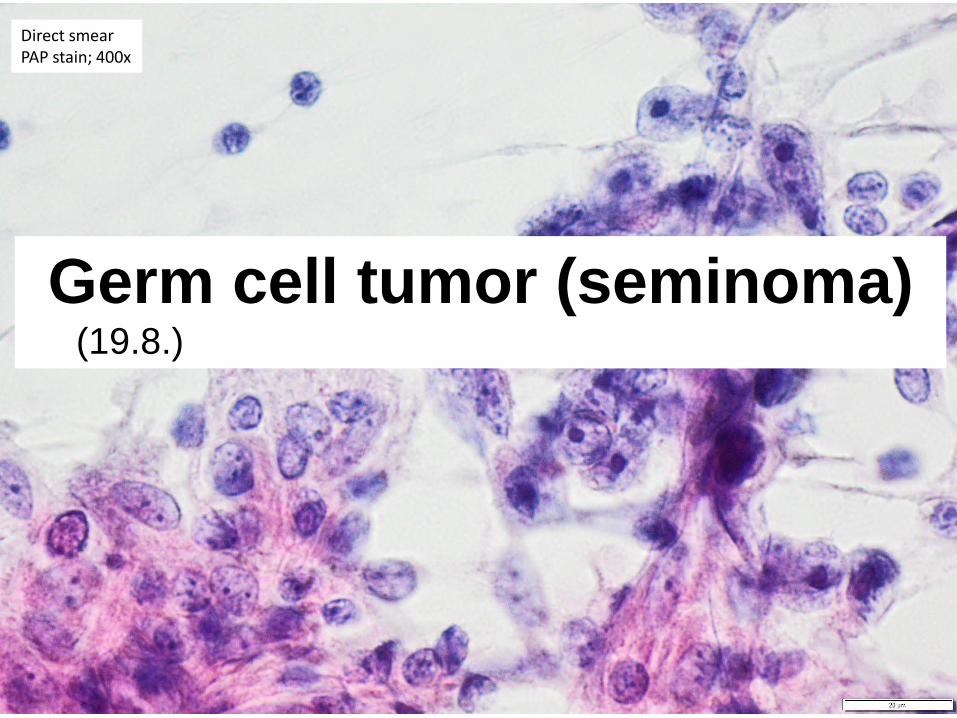
Direct smearPAP stain; 400x
Germ cell tumor (seminoma)(19.8.)
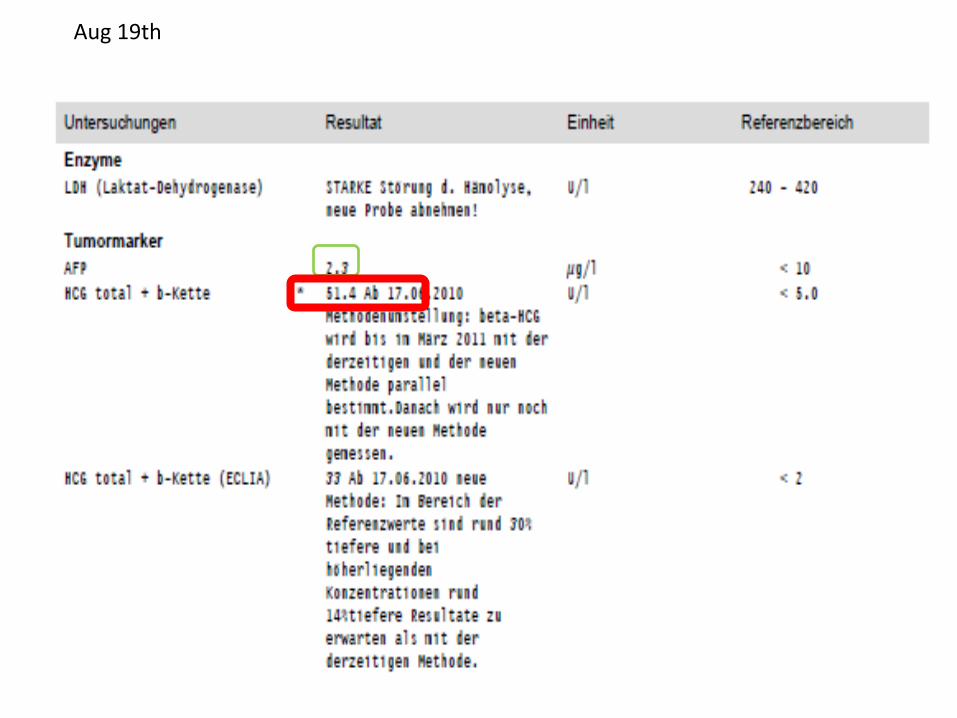
Aug 19th
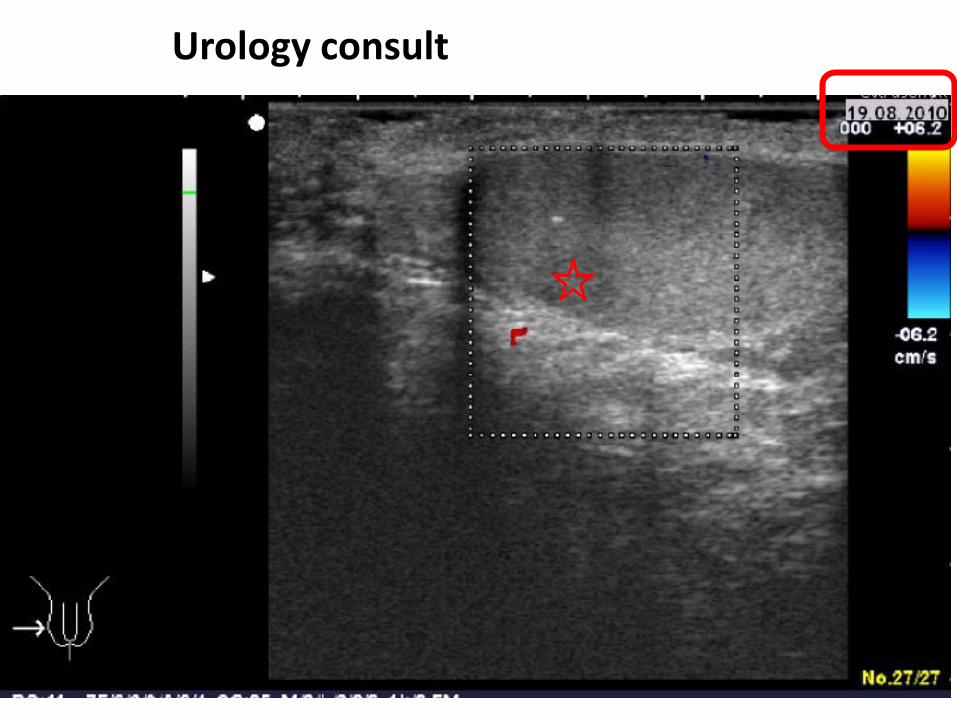
Urology consult
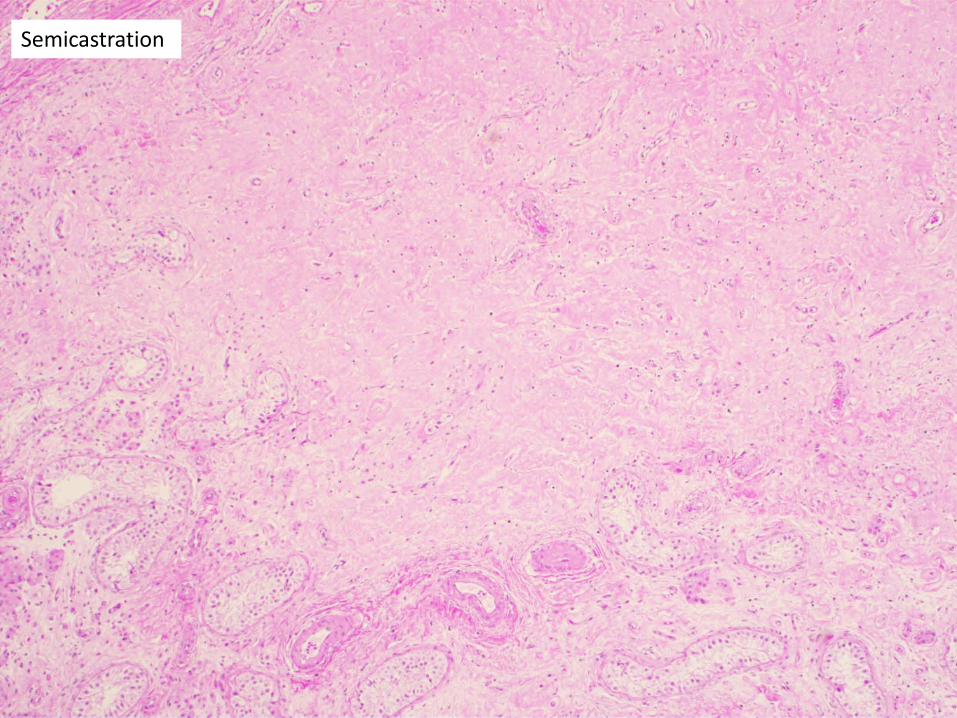
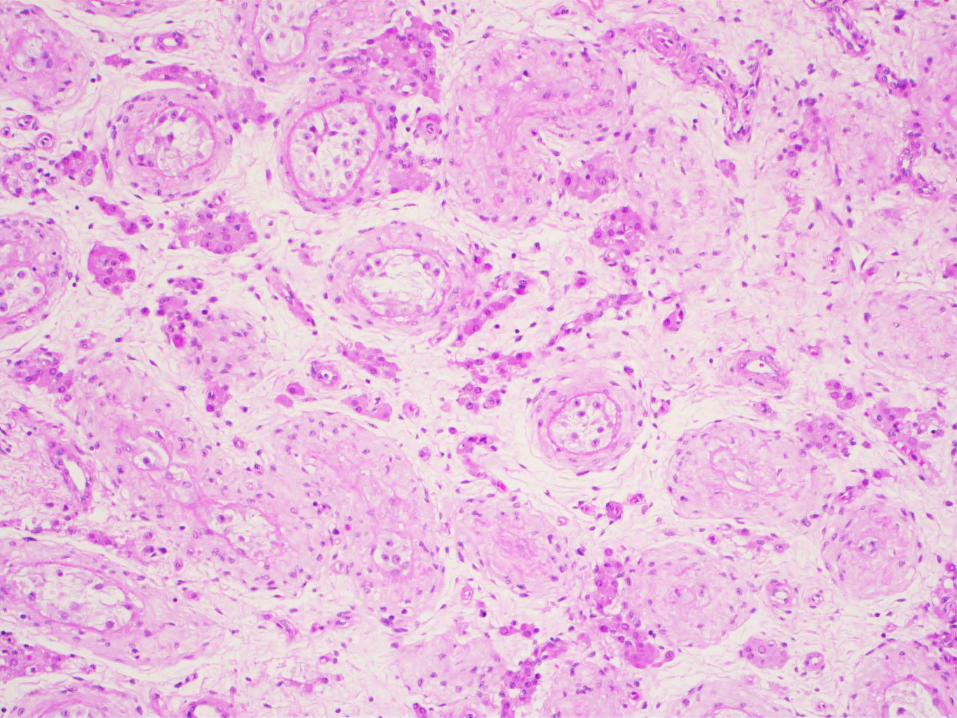
Semicastration
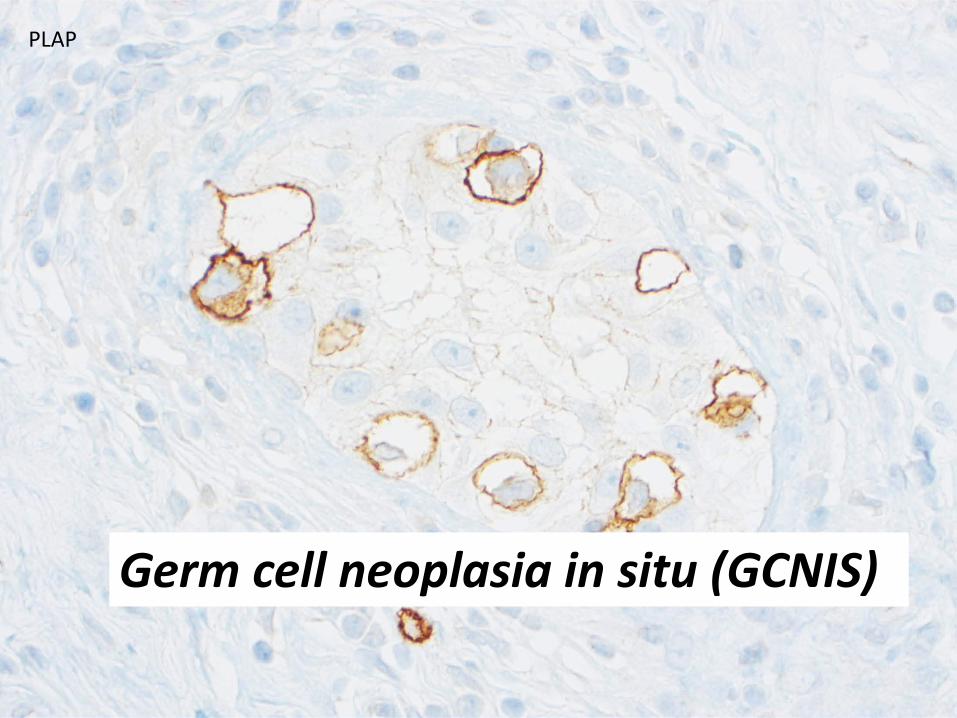
PLAP
Germ cell neoplasia in situ (GCNIS)
Final diagnosis• Metastatic (at presentation) seminoma
– Extensive metastases retroperitoneal and leftcervical
– Initial manifestation as supraclavicularlymphadenopathy
• «Burnt out» (regressed) germ cell tumor of the right testis– Semicastration with focal scaring– Advanced atrophy of the tubuli– Germ cell neoplasia in situ (GCNIS) present
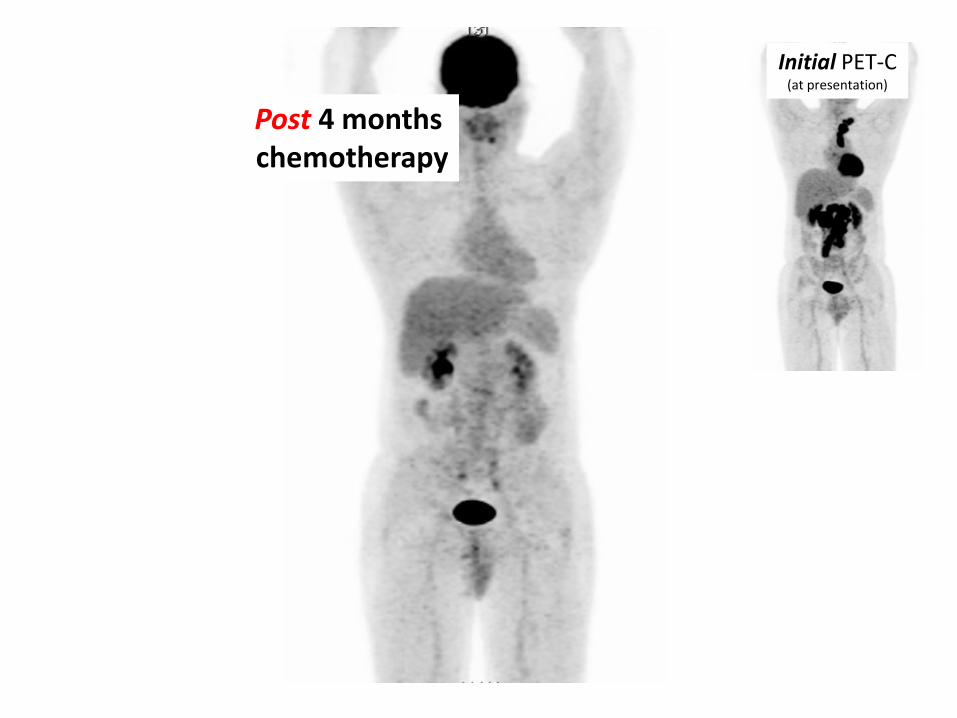
Post 4 monthschemotherapy
Initial PET-C(at presentation)
Follow up• Recurrent tumor 6 month after initial
presentation• High dose chemotherapy with autologous
bone marrow transplantation – successful• Local lumbal spine radiotherapy for residual
tumor
• 6 years after initial presentation no furthertumor manifestations – declared as cured
Germ cell Tumors (GCT)• Rare (1% of male malignancy)• Incidence 1.5 -12 / 100 000 (higher in industrialiezed
countries)– Ethnicity / genetic susceptibility– Enviromental factors
• … however - most common cancer among young male patients (puberty to 40-ies) in industrialized countries
• High metastatic potential• Accompanied by tumor markers in blood (AFP, bHCG)
• Curable with modern combined therapy regimens(most important chemotherapy)
• Usual presentation as a testicular mass• Some 3-10% of seminomas and embryonal
carcinomas present as a metastatic disease• Practically all choriocarcinomas are metastatic
at presentation
• «Burnt out» (regressed) testicular tumors– May cause bulky metastatic diesease– Should not be confused with (rare) extragonadal
primaries (retroperitoneum, mediastinum)
GCT - Subtypes
• Seminoma• Non-seminomatous GCT
– Embryonal carcinoma– Yolk sac tumor– Choriocarcinoma– Teratomas
• Mixed GCT
Cytologic diagnosis of GCT• Not on primary tumors• Possible in metastatic setting
– First diagnosis, if testicular primary not obvious– Recurrent tumor– Advantage: rapid turn over time
• final pathologic tissue diagnosis within 2 days• No excisional biopsy neccessary• Semicastration on the 4th day• Disease specific diagnosis chemotherapy prompty started
Facit
• Metastatic germ cell tumor (GCT) may causecervial lymphydenopathy (not onlyretroperitoneal / mediastinal)
• Cytologic diagnosis of GCT is well feasible
• GCT should be considered as a differential diagnosis especially in young male patientswith rapidly progressive lymphadenopathy

www.zytologie.usz.ch

![[PPT]TUMOR TRAKTUS UROGENITAL - FK UWKS 2012 C | … · Web viewTUMOR TRAKTUS UROGENITAL I. Tumor Ginjal A. Tumor Grawitz B. Tumor Wilms II. Tumor Urotel III. Tumor Testis IV. Karsinoma](https://img.pdfslide.us/doc/110x75/5ade93b87f8b9ad66b8bb718/ppttumor-traktus-urogenital-fk-uwks-2012-c-viewtumor-traktus-urogenital.jpg)




![CD8+ Tumor-Infiltrating T Cells Are Trapped in the Tumor … · 2016. 12. 19. · tumor cells induces immunogenic cross-presentation of dying tumor cells [4,5] or sensitizing tumor](https://img.pdfslide.us/doc/110x75/5fbd8f04c0953e25272e83ca/cd8-tumor-infiltrating-t-cells-are-trapped-in-the-tumor-2016-12-19-tumor-cells.jpg)






















