Embed Size (px)
Citation preview
Colors Used In IllustrationCentrals: Purple Bicuspid: RedCuspids: Yellow Molars: Green
Vol. 2007, Issue 1 www.holisticdental.org
The articles and opinions in this publication are for general information only and are not intended to provide specific advice or recommendations for any individual. We suggest that you consult your health care practitioner with regard to your specific situation. The opinions expressed are those of the authors and do not necessarily reflect the position of the Holistic Dental Association or the HDA Board of Directors.
Cover Artwork by Gina Fiore
President’s Message by Tim Gallagher .................................... 3
HDA Founding Member Honored ............................................ 3
Creating an Ideal Space for Dental Health .............................. 4 Interview with John Laughlin, DDS
Member Profile ..................................................................... 7Jim Kennedy, DDS
PTS/PTSD Primer for Dental Professionals .............................. 8By Joan Rothchild Hardin, Ph.D.
SPECIAL FEATURE: THE FUNCTIONAL MATRIXRemembering Melvin Moss, DDS, Ph.D. .................................12
Vitamin D – The Antibiotic? ..................................................15
Fluoride: Friend or Foe? ........................................................16
A History of Fluoride .............................................................17
Recommended reading ........................................................18
Upcoming teleconferences & events .....................................18
Clinical pearls .......................................................................19By Dr. Harold Ravins
The Holistic Dental Association
COMMUNICATOR
CONTeNTs
Holistic Dental AssociationBoard of Directors
Gerald H. Smith, DDSChairman303 Corporate Drive EastLanghorne, PA 19047215/968-4781Ronald King, DDSPast President6100 Excelsior Blvd., #ESt. Louis Park, MN 55416952/929-4545Tim Gallagher, DDSPresident990 W. Fremont Ave. #LSunnyvale, CA 94087408/739-9050James Bronson, DDSPresident-Elect6845 Elm Street, #507McLean, VA 22101703/506-9805Stanley Organ, DDSSecretary1317 Southwind CircleWestlake Village, CA 91361805/373-9089Fen-Hui Chen, DDS1030 Pearl St. #6La Jolla, CA 92037858/459-5445William Megill, DDSP. O. Box 185Rocky Hill, NJ 08553609/924-9411
Pentti J. Nupponen, DMD, MAGD, FIND, AIAOMT207 Market StreetHalifax, PA 17032 717/896-3911
Holistic Dental Association staffCraig Zunka, DDSBoard Advisor107 West 4th StreetFront Royal, VA 22630Sandra OrionExecutive DirectorPO Box 151444San Diego, CA 92175619/795-3292Rhona Gissen Stanley, DDS, MPHEditor460 West 24th St.NY, NY 10011212/912-1212

The Journal of the Holistic Dental Association 3
President’s MessageBy Tim Gallagher
At the next convention, the diagnos-tic summit, we will be giving you many pearls but one I find very interesting is the relationship between well done meats and periodontal status. Advanced glyca-
tion end products (AGEs) promote inflammation. While AGEs are formed in our bodies, especially when blood sugar is frequently elevated, they can also be absorbed from the diet. A diet high in preformed AGEs can serious-ly elevate blood levels of various inflammatory mediators, including C-reactive protein, tumor necrosis factor-alpha, and vascular cell adhesion molecules. A low-AGE diet can lower these inflammatory biochemicals.
What promotes the formation of AGEs in food? High heat/prolonged cooking does. Deep-fried foods, such as French fries, fried fish and shrimp, fried chicken, etc. are great sources of AGEs. Well done meats (including typical fast food burgers), overly crisp bacon, burnt toast, indeed anything cooked with high heat or for prolonged periods, provides an AGE-rich diet. Sugar, on baked goods, that has been browned, is a double whammy.
Dr. Steve Green, who will be presenting at the conven-tion, says that puffy, hypertrophic gingival papillae con-note increased inflammation and diminished apoptosis of cells (metabolic syndrome X or prediabetes). This identi-fies increased risk to depression, gall bladder disease, heart disease, stroke and cancer. AGEs increase this risk.
Steve also advises us to be proactive about health. The American Dental Association teaches brushing and flossing to control ever-present disease. Instead, we teach brushing and flossing to check effectiveness of cellular im-munity. ‘When you floss, is the floss clean?’ Is there just a light ‘moss’ on tongue? When our white blood cells do not keep our mouth clean, cellular immunity is disabled and inflammatory humoral immunity rises to attempt compen-sation.
A diet rich in rapidly digested sugars/starches (high glycemic), especially when consumed by those over-weight and/or insulin resistant, promotes inflammation. The typical American diet is rich in carbohydrates, with roughly two-thirds of the average American’s diet coming from inflammation-promoting high glycemic foods, such as bread, soft drinks/sodas, cakes, cookies, quick breads, doughnuts, sugar/syrups/jams, potatoes, cereal and pasta. If the inflammation response takes on a life of its own, be-coming self-perpetuating, chronic inflammation develops.
One of the many ways you can reduce inflammation is with fish oil. But there is a difference between health-food-grade fish oil and pharmaceutical grade fish oil. We will be addressing this controversy, but a simple test to determine the effectiveness of your fish oil is to see if your oil freezes in the refrigerator freezer. If it does freeze, it is ineffective. You can also place oil over water in a small cup and add a small piece of Styrofoam from a fast food container onto the oil. If the oil is effective, it will dissolve the styrofoam within 5 minutes.
HDA Founding Member HonoredCraig Zunka, DDS, a founding member of HDA, was the 2006 recipient of the Fellow of the Cranial Academy award presented to an outstanding leader in the field of cranial osteopathy.
An excerpt from the qualifications for the award:Section 12.2 - Fellow of The Cranial Academy AwardThe Fellow of The Cranial Academy Award was established
in 1995 to recognize the true leaders of The Cranial Academy. It is an honorary award intended to recognize outstanding physi-cians and to honor members of The Cranial Academy who have distinguished themselves by providing exemplary leadership, dedication in teaching, advocating and advancing osteopathy, specifically Cranial Osteopathy. Consideration in nominating fellowship candidates include:
A. Currently licensed and in good standing or retired with previous license void of disciplinary action
B. Active membership in The Cranial Academy for a mini-mum of ten years
C. Cranial Academy competency certificate or equivalentD. Compliance with The Cranial Academy’s code of
ethicsE. Meritorious service to The Cranial Academy and osteo-
pathic profession in all three areas:1. Minimum of three years of teaching Cranial Osteopathy
to students, physicians and dentists2. Advocating Cranial Osteopathy in business and profes-
sional life to the public, patients, students, physicians, dentists government and other business organizations.
3. Minimum of three years of advancing Cranial Osteopa-thy through published article(s) or research and/or leadership service to The Cranial Academy.
We congratulate Zunk on his outstanding achievements.
4 The Communicator
Creating An Ideal space for Dental Health:
As holistic dentists, we have certain standards that we follow in practicing dentistry. First, we want to be nourishing and caring of our patients and provide an atmosphere where the patient feels safe. This is not easy as even the thought of going to the dentist can bring up past traumas for many patients.
Second, we need to use dental materials that are biocompatible with each patient.
Third, we must make the connection between dental health and whole health, and acknowledge how an individual’s psychic and spiritual health contributes to physical health.
Fourth, we must be knowledgeable about complementary al-ternative medical practices to support each patient’s treatment.
Many of the dentists in HDA follow these criteria in their
practice. In this issue, one of HDA’s past-presidents, John Laughlin, DDS, shares how he built a new office for his practice to incorporate the principles of holistic dentistry.
HDA Interviews John Laughlin, DDsQ: You spent 1.2 million dollars on new building construc-
tion and equipment. How long will it take you to get back the money you invested?
A: I don’t think about it that way. I wanted a nicer place for my team, my patients, and lastly for myself. I have been in the practice of dentistry 34 years, first as an Air Force dentist for 2 years and then in private practice. It is wonderful, at last, to have a beautiful place, built according to my specifications. Even if I go to part-time work, I will have a gift to pass on to an-other dentist. The changes I made that follow holistic tenets will be perpetuated, and the philosophy of holistic dentistry will endure.
Q: How were you able to maintain full time practice and build your new of-fice at the same time?
A: I surrounded myself with my son, John, and my wife, Judy. Judy helped with the design, the interior decorating, the landscaping, and also painted the Chinese Brush Paintings that hang on the interior walls. Judy is a renowned artist, who has exhibited at the Lincoln Center Art Gal-lery in NYC. Designing the building was challenging and we ended up using the services of 3 architects, which resulted in my son designing a good portion of the building. John oversaw construction on a daily basis, as well as serving as adminis-trator of the existing practice, and at the same time finished college.
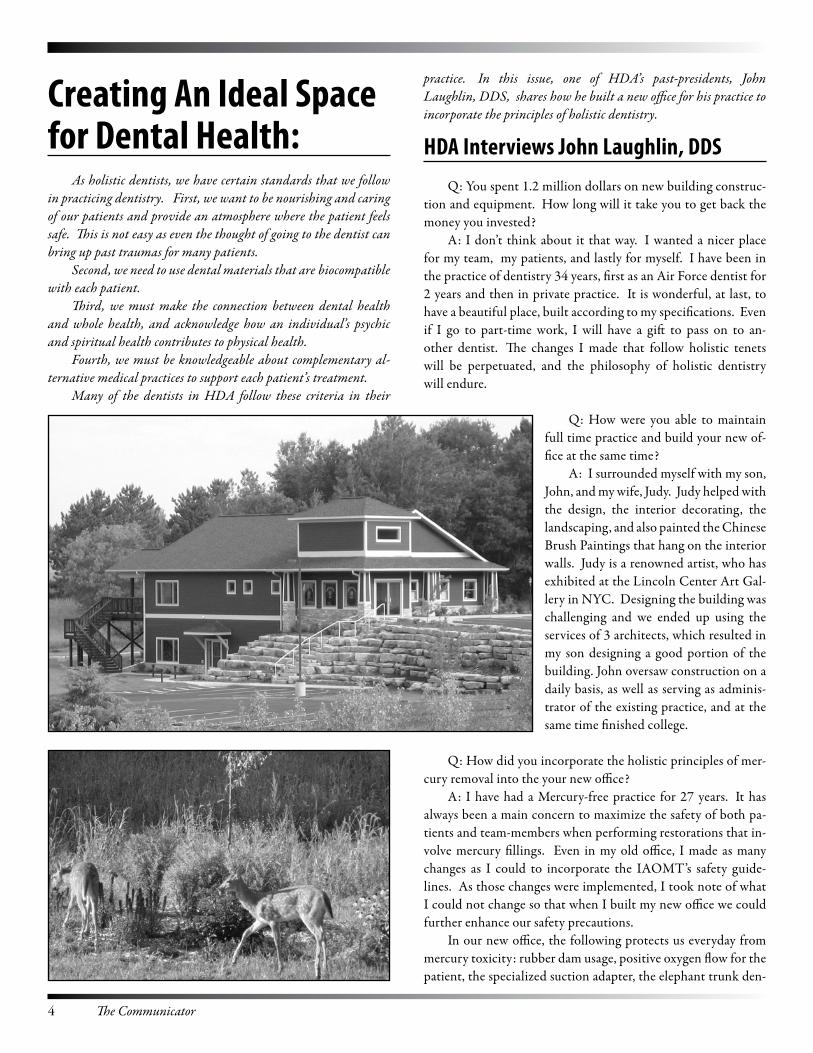
Q: How did you incorporate the holistic principles of mer-cury removal into the your new office?
A: I have had a Mercury-free practice for 27 years. It has always been a main concern to maximize the safety of both pa-tients and team-members when performing restorations that in-volve mercury fillings. Even in my old office, I made as many changes as I could to incorporate the IAOMT’s safety guide-lines. As those changes were implemented, I took note of what I could not change so that when I built my new office we could further enhance our safety precautions.
In our new office, the following protects us everyday from mercury toxicity: rubber dam usage, positive oxygen flow for the patient, the specialized suction adapter, the elephant trunk den-

The Journal of the Holistic Dental Association 5
tal air vacuum system, mercury vapor ionizer, masks for doctor & assistant, an air-exchanger in the HVAC system that replaces all the air in the building 1 1/2 times per hour, and a mercury separator to remove mercury from the waste water.
Q: How did you transfer the concepts of holistic practice into the design of your new office?
A: I originally looked into a geodesic dome for the design of the building, but I was advised against it because of its eccentric-ity and low resale possibilities. Other innovations I wanted to incorporate but did not were a green roof and solar electricity.
I decided on a more conventional design for the building, but did incorporate insulated panels (exterior wall construction), in-floor heating for both levels, rounded corners and curves as the interior design, and SolaTubes™ for lighting. SolaTubes™ gather the light of the sun and through a system of mirrors bring the light down from the roof and into the room. This decreases electrical demand and provides additional natural lighting.
After the carpeting was installed in the office, we ran the air-exchanger constantly for 60 days. I also used baking soda and an ozone machine to detoxify the carpet, as the glue in the carpet releases formaldehyde.
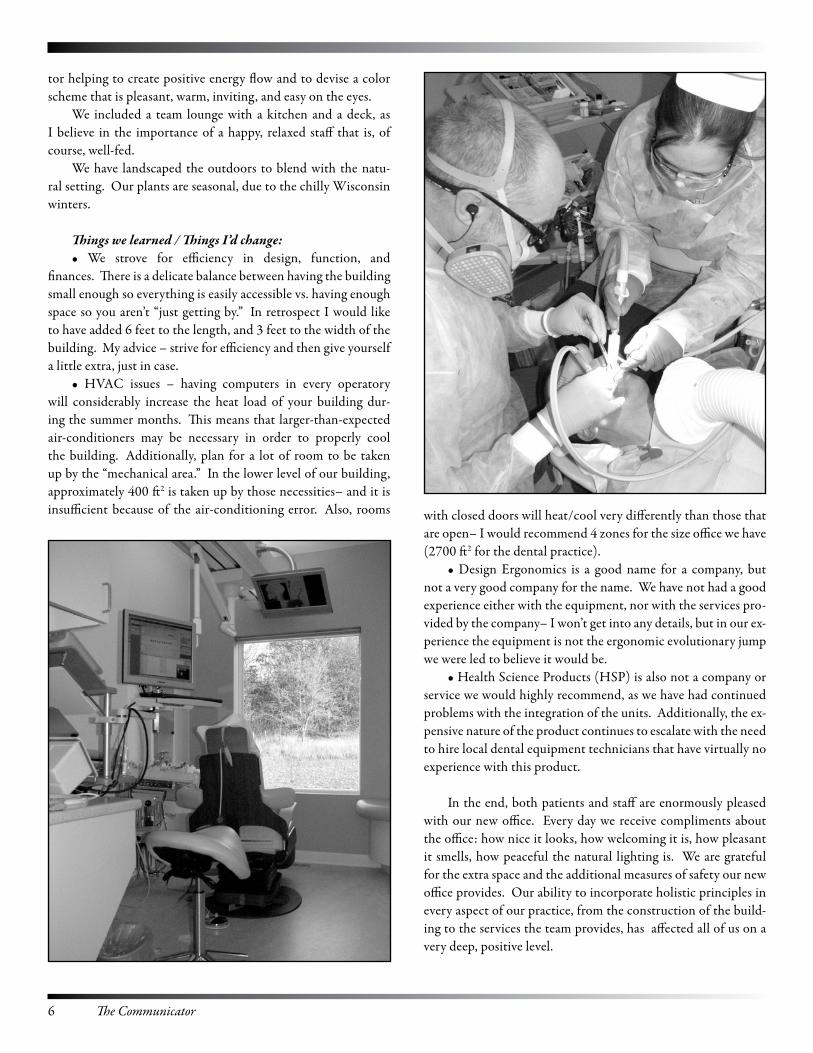
Our office uses only digital radiography. We have incor-porated a single Dexis™ x-ray sensor, a portable digital x-ray tube (Nomad™), and a digital panoramic/cephalometric x-ray machine (Planmeca – ProMax™). These units are expensive but as they substantially reduce radiation exposure, they are an im-portant service to both my patients and our dental team. My patients also appreciate the better diagnosis they receive with digital radiography, and I must tell you the combination of higher resolution and the ability to manipulate the images are invaluable.
The linoleum flooring in the operatories is a linseed oil product that is natural and durable. We have a separate room for dental cranial work and for ozone therapy. The central sound
system is carried to all the rooms and each room has its own vol-ume control that the team can adjust. Each room has two video monitors, one for the doctor or team-member, and the other for the patient. At this time the patients’ monitors show a random-ized slideshow of over three hundred photos, ranging from un-derwater photography to beautiful natural and man-made land-scape scenes.
I have a central-air based aromatherapy system that increases the “at-ease” and welcoming feeling of the office, and I use only the most natural essential oils so there are no problems with al-lergies.
I also had a Feng Shui consultant and interior decora-
“I wanted a nicer place for my team, my patients, and lastly for myself. I have been in the practice of dentistry 34 years, first as an Air Force dentist for 2 years and then in private practice. It is wonderful, at last, to have a beautiful place, built according to my specifications. Even if I go to part-time work, I will have a gift to pass on to another dentist. The changes I made that follow holistic tenets will be perpetuated, and the philosophy of holistic dentistry will endure.” –John Laughlin, DDS
6 The Communicator
tor helping to create positive energy flow and to devise a color scheme that is pleasant, warm, inviting, and easy on the eyes.
We included a team lounge with a kitchen and a deck, as I believe in the importance of a happy, relaxed staff that is, of course, well-fed.
We have landscaped the outdoors to blend with the natu-ral setting. Our plants are seasonal, due to the chilly Wisconsin winters.
Things we learned / Things I’d change: • We strove for efficiency in design, function, and
finances. There is a delicate balance between having the building small enough so everything is easily accessible vs. having enough space so you aren’t “just getting by.” In retrospect I would like to have added 6 feet to the length, and 3 feet to the width of the building. My advice – strive for efficiency and then give yourself a little extra, just in case.
• HVAC issues – having computers in every operatory will considerably increase the heat load of your building dur-ing the summer months. This means that larger-than-expected air-conditioners may be necessary in order to properly cool the building. Additionally, plan for a lot of room to be taken up by the “mechanical area.” In the lower level of our building, approximately 400 ft2 is taken up by those necessities– and it is insufficient because of the air-conditioning error. Also, rooms with closed doors will heat/cool very differently than those that
are open– I would recommend 4 zones for the size office we have (2700 ft2 for the dental practice).
• Design Ergonomics is a good name for a company, but not a very good company for the name. We have not had a good experience either with the equipment, nor with the services pro-vided by the company– I won’t get into any details, but in our ex-perience the equipment is not the ergonomic evolutionary jump we were led to believe it would be.
• Health Science Products (HSP) is also not a company or service we would highly recommend, as we have had continued problems with the integration of the units. Additionally, the ex-pensive nature of the product continues to escalate with the need to hire local dental equipment technicians that have virtually no experience with this product.
In the end, both patients and staff are enormously pleased with our new office. Every day we receive compliments about the office: how nice it looks, how welcoming it is, how pleasant it smells, how peaceful the natural lighting is. We are grateful for the extra space and the additional measures of safety our new office provides. Our ability to incorporate holistic principles in every aspect of our practice, from the construction of the build-ing to the services the team provides, has affected all of us on a very deep, positive level.
The Journal of the Holistic Dental Association 7
Member Profile: HDA Interviews Jim Kennedy, DDs
The Holistic Dental Association represents members who support diverse modalities of complementary alternative dentistry. Dr. Jim Kennedy focuses on the treatment of TMJ dysfunction, facial pain, sleep apnea, and orthodontics. When I mentioned his name to a well-established dental laboratory head technician, he said of Jim, “He’s a genius!”
Q: How long have you been in practice?A:30 years–20 years in Detroit; 6 years in Denver, and now in
Grand Junction, Colorado.I was motivated to relocate from Denver to Grand Junction
and bought a condo space for $210,000. I developed it into the office I wanted. Now I live less than 20 minutes from my practice in a small town. In Denver I was driving approximately one hour to work every day.
Q: How long will it take to recoup your money?A: We already have return on the space we bought. I spent
another $350,000 for equipment. My loan payment schedule is 20 years, but it will probably take 12 years to pay it off, working approximately 30 hours per week.
Q: How did you make the transition?A: I continued to work in Denver while my practice in Grand
Junction was building. It was difficult to decide when to make the full move. It has taken about 3 years to recover to the same income level. I started over. I had to meet all the dentists in the area and educate them about my specialty practice. I am a specialist, not by degree, but by education and skill.
Q: How did you transfer your concepts of holistic dentistry into the design of your new office?
A: We described the feeling we wanted in our new office to an interior decorator. We wanted a place where people would feel comfortable, a safe place, because we treat patients with a lot of problems and pain. We used the principles of feng sui. We used earth tones and southwestern accents. We have jute back carpets instead of rub-ber carpets. We rounded all the cor-ners and incorporated a water feature. We made sure there was flow and that it was quiet. We have a music system
throughout the office and satellite radio and play light classical music and soft jazz.
There are three operatories, a consultation room, a laboratory, and a staff lounge. There are computer monitors throughout the office. All charting is done in the computer and everything else is scanned into the computer. I do not leave the office until I enter all records into the computer.
I bought a digital tomogram which was my biggest equip-ment expense, about $60,000. I also have a Nikon digital camera in the consultation room for photographic diagnostics.
I have a state of the art sterilization area and new lab equip-ment, including model grinders and other lab equipment for mak-ing and repairing splints and orthodontic appliances.
Q: What would you do differently?A: I am happy with the office. There is not much I would
change. Little things need tweaking, for example, positioning of staff. In one room, I have rear delivery, access to standing or sit-ting, and this gives me more ergonomic options when I deliver patient care.
Q: What advice can you give to other dentists who want to build a new office?
A: The first and most important step in conceptualizing an office is the floor plan. How many rooms do you want? What are their purposes? What are you going to do in the room and how are you going to practice? And you must plan for future growth. For example, from the get-go, put in the plumbing for an extra op-eratory. Set up the present to allow expansion for future growth.
Then you need to look at the office design from a patient’s perspective. Ask yourself, “What will the patient think?” It is cru-cial how the patients view the office.
Our patients like the new office. They say it is comfortable and peaceful. To me, this is most important. I think we have ac-complished our goals.
Dr. Kennedy consults with a patient.
A water feature in the office soothes patients.
8 The Communicator
PTs/PTsD PRIMeR FOR DeNTAL PROFessIONALs: A Guide for Working with sexually Abused Patients
By Joan Rothchild Hardin, Ph.D.
INTRODuCTIONI hope that this information will assist dentists, orthodon-
tists, and other dental professionals to recognize the symptoms of Post Traumatic Stress or Post Traumatic Stress Disorder and avoid re-traumatization of the patient as a result of the dental experience. The dental staff that allies with the patient will increase compliance, improve the patient/dental relationship, and create an atmosphere of working together to achieve an optimal result in the dental treatment.
INCIDeNCe OF SexuAl ABuSe IN THe uSThe sexual abuse of children in our country is more com-
mon than many people realize. Surveys say that at least 1 in 5 women and 1 in 10 men recall childhood sexual abuse (ERIC, 1990). Repression of traumatic events occurring at a very young age is fairly common, and psychotherapists who work with anxious, depressed, substance abusing, eating disordered, and suicidal people know that many have repressed their mem-ories of sexual abuse and therefore do not have conscious recall of their experiences.
The 2004 National Crime Victimization Survey found that every two-and-half minutes someone is sexually assaulted somewhere in America, that one in six American women has been the victim of an attempted or completed rape, that 10% of sexual assault victims are men, and that 44% of rape victims are under age 18 with 80% being under age 30. Because of the methodology of this survey, these figures are only for people 13 and older (RAINN).
This means that chances are a significant percentage of the people who come to sit in your chair are victims of childhood or adult sexual abuse.
DeFINITIONS OF CHIlDHOOD SexuAl ABuSeChildhood sexual abuse is any sexual act performed by
an adult or older child with a child by force or cooperation. This includes fondling the child’s genitals, getting the child to fondle the adult’s genitals, rubbing the abuser’s genitals on the child, penetrating the child’s vagina or anus, mouth to genital contact, and using the child for pornographic purposes. Even
sexualized, seductive behavior towards a child where no sexual act takes place is abusive.
THe ABuSeRSChildren are most often abused by adults who are known
to them. The offender is usually a caregiver, an authority figure whom the child loves or trusts –a parent, another family mem-ber, a friend of the family, baby sitter, teacher, clergy, coach, doctor or dentist.
The Child Welfare Information Gateway of the U.S. De-partment of Health and Human Services (formerly the Nation-al Clearinghouse on Child Abuse & Neglect Information and the National Adoption Information Clearinghouse) reports these US statistics for 2004:
Of the 872,000 victims of child maltreatment, 62.4% suf-fered neglect, 17.5% were physically abused, 9.7% were sexually abused, 7.0% were emotionally or psychologically maltreated, and 2.1% were medically neglected.In addition, 14.5% experienced other types of maltreat-ment such as abandonment, threats of harm, and congeni-tal drug addiction.Nearly 80% of perpetrators were parents; about 90% were biological parents.For all types of child maltreatment combined, about 60% of perpetrators were women; about 40% were men.15.5% of all perpetrators were associated with more than one type of maltreatment. (Child Welfare Information Gateway).
These figures are for substantiated reports. The numbers of children experiencing unreported or unsubstantiated in-stances of child abuse each year are even higher.
POST TRAuMATIC STReSS AND POST TRAuMATIC STReSS DISORDeRPost Traumatic Stress (PTS) is traumatic stress that per-
sists following a traumatic incident (Rothschild, 1995). When Post Traumatic Stress is not resolved through some form of healing and accumulates to the point of causing recurrent, in-trusive thoughts about, images, feelings, and body sensations from the event(s), it is called Post Traumatic Stress Disorder (PTSD) (American Psychological Association, 2000). Trau-matic events stress our bodies and our minds, even when no direct bodily harm has been done, because traumatic stress can produce persistent arousal in the autonomic nervous system.
We encode our memories first as somatic sensation: sight, smell, sound, touch, taste, movement, position, behavioral sequence, visceral reaction. Later on, a sensory stimulus can evoke an old memory the way the smell of madeleines recalled a memory for Proust – except that when encoded memories are of traumas, recalling them is highly disturbing rather than pleasant.
•
•
•
•
•

The Journal of the Holistic Dental Association 9
One of the hallmarks of PTSD is flashbacks. These are re-plays of sensory memories of traumatic events, often intense and frequently accompanied by great, inexplicable fear. Instead of understanding that a memory of an event has been triggered, it feels like it is happening right now in the present.
As Babette Rothschild puts it in The Body Remembers, “Typically … individuals with PTS and PTSD are missing
the explicit information necessary to make sense of their dis-tressing somatic symptoms ….
“A flashback can be triggered through … something seen, heard, tasted, or smelled that serves as the reminder and sets the flashback in motion. It can just as easily be a sensation aris-ing from inside the body. Sensory messages from muscles and connective tissue that remember a particular position, action, or intention can be the source of a trigger…. Even an internal state aroused during a traumatic event, for example, accelerated heart rate, can be a trigger… The accelerated heart rate and in-creased respiration can be implicit reminders of the accelerated heart rate and increased respiration that accompanied the ter-ror or their trauma (Rothschild, 2000, 44-45).
When a person gets triggered, flashbacks tend to come in-stantaneously with no time to realize what is happening. The experience is often compared to falling down a rabbit hole: one minute you’re in the here and now, the next thing you know you’re in a state of fear - or nonexistent, nowhere.
WHAT THIS MeANS FOR YOu PROFeSSIONAllYThe problem for you as a professional trying to work in
the mouth of someone who experiences PTS or PTSD is that your work in the mouth may trigger memories, sensations, and emotions from old sexual abuses - and consequently fear and possibly a strong need not to cooperate with you, even get away from you. It is very important to understand that your patient is a person who has become intensely afraid - not someone who is trying to make your job harder by being difficult.
THe MOuTH AS AN eROGeNOuS ZONeThe mouth, lips, and tongue are very sensitive to touch and
taste and are a highly erogenous zone. Adults using children for their own sexual gratification often choose this site for abuse. The strong sucking response of infants is even taken advantage of by adult and teenage males who seek sexual gratification from someone they think will not tell or even remember.
Sexual abuse in or involving the mouth can produce a con-fusing combination of pleasurable and painful feelings. For people who have been sexually abused, the mouth can become charged with fear and negative energy. Since being touched around and in the mouth can feel very good, children who have been abused often experience a conflicted set of feelings for these events: pleasure, guilt and shame at having been aroused,
as well as anger, feeling out of control, and betrayed.
ORAl-MOTOR ISSueS AND DeFICITSChildren, who have been sexually abused orally, may
develop an intolerance to touch around the face, neck, and mouth. That intolerance may cause or exacerbate oral-motor issues, and the person may develop involuntary muscle move-ment and facial weakness which manifests as difficulties with chewing, swallowing, and speech.. For these children - and these children grown into adults - dental visits can be emotionally agonizing (Yehuda, 2006).
Carmen Santos, a psychologist who has studied the con-nection between adult female survivors of sexual abuse and dental anxiety, describes the psychic overlap between experi-encing sexual abuse and dental anxiety:
“Varying forms of abuse, such as those that inflict pain or cause lack of control and powerlessness, may have a dramatic impact on the individual’s ability to manage routine activities involving physical discomfort, and may cause dental phobia.
The symptoms that result consist of fear, anxiety, nausea, dissociation, flashbacks and feelings of shame. The shame can be about being anxious, about poor oral health, or about hav-ing someone find out about the abuse.
Many aspects of dental treatment symbolically represent sexual abuse for many survivors. The following conditions may trigger a repetition of earlier trauma: being alone with a per-son more powerful than oneself, being placed in a horizontal position, having someone nearby and touching you, having ob-jects placed in one’s mouth, being unable to talk or swallow, and experiencing or anticipating pain. Many dental experiences may remind the patient of their abuse experience in that they restrain movement, produce gagging sensations (impressions), and the feeling of suffocation(rubber dams).”
BODY MeMORIeSIn the more than 100 years during which responses to
overwhelming experiences have been systematically explored, it has been noted that the psychological effects of trauma are expressed as changes in the biological stress response. Excessive stimulation of the central nervous system during the trauma produces enduring neuronal changes. The abnormal startle re-sponse characteristic of PTSD is an example of such neuronal change (van der Kolk, Ch 12).
Apparently the cells retain a ‘memory’ of how a traumatic experience felt physically and emotionally.
Psychotherapists and body workers, such as massage thera-pists and acupuncturists, have long known that the body re-tains traumatic memories that can be released and healed through mind-body work, unblocking of energy, and physical manipulation. And, with the increasing popularity of yoga in this country, many people are now experiencing the tremen-

10 The Communicator
dous release of emotion from practicing poses that address body areas where traumatic memories are stored. Many people have related to me times when they started to cry deeply while doing hip-opening poses.
The most salient difference between explicit and implicit memories, and what makes implicit memories so readily trig-gered into body memories, is this: Explicit memories include such things as facts, events, people, and objects and are recalled consciously. Implicit memories include conditioned responses as well as motor and perceptual skills, and are accessed and per-formed unconsciously.
Studies are demonstrating that explicit memories are stored biochemically in the hippocampus in a spatial context (Kandel, 2006). That is, we typically remember people and events in relation to other memories – more or less in a story that makes sense to us. Implicit memories which have been acquired traumatically, in a state of hyperarousal, seem to be stored separately - perhaps in the amygdala (Rothschild, 2000, 71) - as isolated sensations and feelings that pop up when trig-gered by a stimulus later on (van der Kolk, 1996, Ch 12).
PATHOlOGICAl DISSOCIATIONGarden variety, everyday dissociation is useful and feels
very pleasant –getting lost in music or a daydream, imagining ourselves at a beach instead of in the dental chair. Dissociating seems to be something we’re born knowing how to do. When a person is repeatedly put into a state of hyperarousal and fear during childhood and needs to use this coping skill over and over again, dissociation develops into an involuntary way to deal with stress of any kind.
Dissociating lets the person ‘leave’ so as not to have to feel physical or emotional pain. However, if dissociation contin-ues to be used when the original danger no longer exists, it be-comes maladaptive.
Pathological dissociation is an ongoing process in which certain information (feelings, memories, physical sensations) is kept apart from other information with which it would nor-mally be logically associated (the story of what happened).
A pathologically dissociative person automatically discon-nects from situations perceived as dangerous or threatening, without being able to take time to determine whether there is in fact any real danger, leaving the person inappropriately - and often inconveniently - spaced out.
Involuntary, pathological dissociation, as in PTSD and Dissociative Identity Disorder (formerly called Multiple Per-sonality Disorder), occurs when a person suddenly becomes triggered by something that feels in some way like the long-ago trauma. The experience is never pleasant and makes the person it is happening to feel re-victimized, powerless, and out of con-trol. When someone gets triggered while in your office, a very old event gets recreated in which you suddenly become seen
as the abuser and the patient is the powerless child who has to protect her or himself from big powerful you.
Flashbacks, body memories, and dissociation can be trig-gered by anything that is reminiscent of the trauma: a physical sensation, a smell, a taste, an emotion, a verbal instruction, a particular movement like one that happened just before or dur-ing the old trauma.
SIGNS YOuR PATIeNT IS exPeRIeNCING PTS OR PTSDThe following behaviors may occur if what is happening to
your patient in the dental chair is causing trauma.1. Holding the breath, breathing very shallowly, irregu-
lar breathing - breathing this way is the hallmark of a person in a fearful, anxious state;
2. Appearing spacey, disoriented, age-regressed, or unresponsive;
3. Having trouble concentrating on what you are say-ing ;
4. Flinching or jumping at your touch or a noise;5. Crying or tearfulness while unable to explain why;6. Acting outright uncooperatively.
THINGS YOu CAN DO TO FACIlITATe WORKING WITH THeSe PATIeNTS 1. Explain what you are going to do, step by step, in an age
appropriate way. Do not treat a traumatized teen or adult sit-ting in your chair like a child by talking down to her or him.
2. Do not try to reassure the patient by saying “This won’t hurt.” It is more the psychic pain of reliving the past trauma than the present experience of the dental treatment that your patient is feeling. You are viewed as the abuser and your reas-surances will not help.
3. Provide frequent opportunities to rinse. This helps break up the exam or treatment into more manageable steps, lets the patient regain control between steps, and helps the pa-tient start breathing again.
4. Arrange a signal with your patient to indicate ‘stop’. This gives her more control of the situation. Remember always to respect such a ‘stop.’
5. When you notice the patient is holding her breath or breathing very shallowly, ask if she would be willing to take some deep breaths –ask the patient to breathe deeply, in and especially out five to ten times: “Like this, with me …” You may need to do this frequently since people in an anxious state breathe only enough to stay alive. Breathing along with the pa-tient will probably help you stay calm and focused too. Also, if you notice your patient pressing an arm or hand into the chest or belly, gently suggest she move it away so she can breathe bet-ter, remain more in the present, and feel less scared.
6. Give your patient a pad of paper and pen so she can relay
The Journal of the Holistic Dental Association 11
information to you and ask questions even if she is unable to speak because her mouth is numb or full of dental equipment.
7. Do not take the stance that this patient is just being dif-ficult or trying to do something to you. What you are engaged in with a previously traumatized patient is a struggle to stay in the present and not see you as another abuser.
8. If the patient is uncomfortable and trying to change po-sition, allow it. Never push the patient back into the chair or force her or his face into a particular position for your own purposes. It will work much better if you explain what position you need for the work you are doing and ask for cooperation.
9. Do not try to negate the patient’s fear by ignoring it or trying to engage in small talk.
10. Provide good distractions like music, animal or nature videos, your spoken explanations of what you’re doing while you are doing it.
11. Be respectful of the person’s struggle. Even if you rec-ognize the abuse the patient has suffered, do not try to get her or him to talk about it – for many reasons, including that it is inappropriate to the situation, that you are not trained in how to do this, and that memories of and feelings about much childhood sexual abuse are often repressed. If the patient re-members being abused and trusts you enough to bring up the subject, listening respectfully, thanking her for telling you so
you can make her time in your chair easier for her, and staying within your comfort area with the material are probably going to be the most satisfying for both of you.
12. You have to prove your trustworthiness to the patient. Make reassuring eye contact, smile sincerely, be relaxed and confident, do not criticize the patient, who is doing the best she or he can manage at the time.
CONCluSIONSRecognizing when traumatic sexual experiences have made
patients fearful of dentists and dental procedures and becom-ing more adept in your approach to these patients will reward you with better compliance. Patients will come to value you as a safe person in their lives and stop dreading or postponing regular check ups and necessary dental work. You may even be able to assist in their healing by becoming perceived as a trust-worthy authority figure rather than another violator.
ReFeReNCeSFor references, please contact the author:Dr. Joan Rothchild Hardin393 West Broadway #4New York, NY 10012Tel (212) 966-9433 Fax (212) 431-9196
Reach Holistic Dental Professionals All Over The World–ADVeRTIse IN THe COMMUNICATOR!Want to contact health-oriented practitioners in the dental profession’s most forward-looking, enlightened international organization? Call today to get started!
Commercial Advertising Rates
size 1 Insertion 2-3 Insertions 4-6 Insertions1/4 Page(3 3/4” w x 4 3/4” h)
$85 $75 $65
1/2 Page(7 1/2” w x 4 3/4” h)
$105 $95 $85
3/4 Page(5 1/2”w x 9 1/2” h)
$120 $105 $95
Full Page(7 1/2”w x 9 1/2”h)
$135 $120 $105
Deadlines: In order to keep pace with the volatile health care industry at this time, our publication schedule changes frequently. Please contact the editor at (215) 968-4781 for deadline information.
specifications: All ads must be presented on CD or via email in high resolution PDF, TIFF, or EPS format. Image resolution should be 300 DPI. Please outline all fonts, and ensure all linked graphics are included. Other formats may require additional handling charges.
For more information or to place your order, contact:Sandra Orion, Executive Director • (619) 923-3120 • [email protected]
12 The Communicator
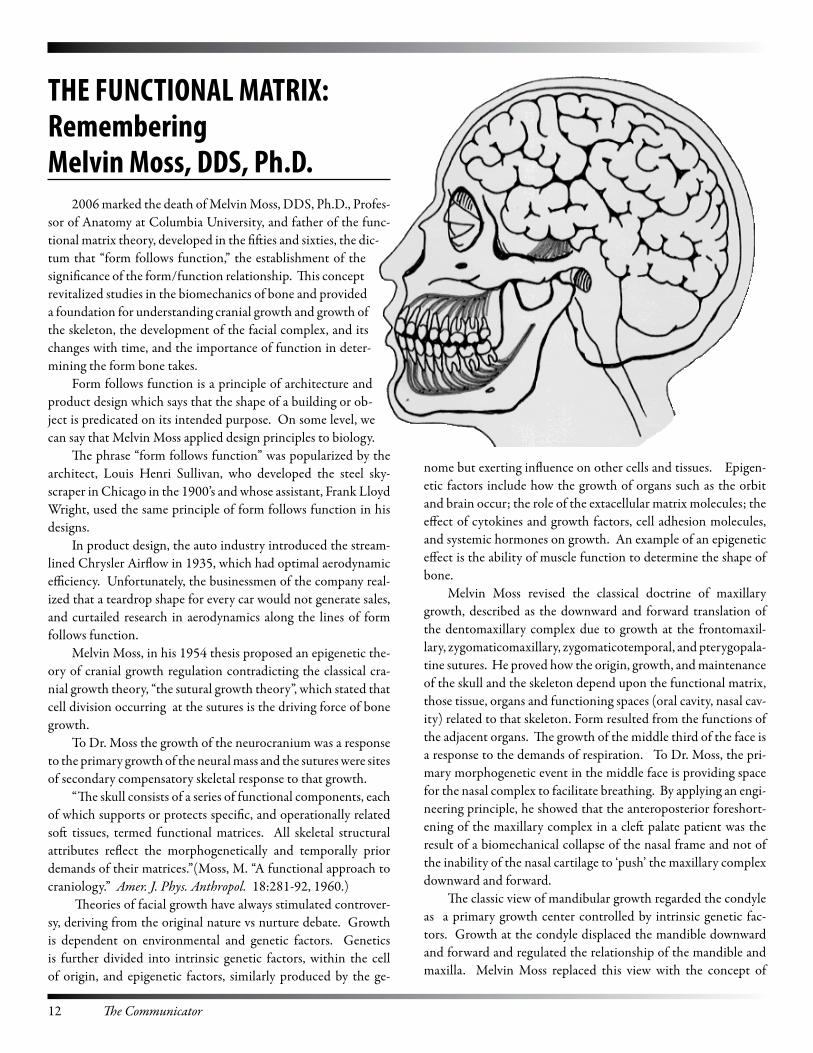
THe FUNCTIONAL MATRIX: Remembering Melvin Moss, DDs, Ph.D.
2006 marked the death of Melvin Moss, DDS, Ph.D., Profes-sor of Anatomy at Columbia University, and father of the func-tional matrix theory, developed in the fifties and sixties, the dic-tum that “form follows function,” the establishment of the significance of the form/function relationship. This concept revitalized studies in the biomechanics of bone and provided a foundation for understanding cranial growth and growth of the skeleton, the development of the facial complex, and its changes with time, and the importance of function in deter-mining the form bone takes.
Form follows function is a principle of architecture and product design which says that the shape of a building or ob-ject is predicated on its intended purpose. On some level, we can say that Melvin Moss applied design principles to biology.
The phrase “form follows function” was popularized by the architect, Louis Henri Sullivan, who developed the steel sky-scraper in Chicago in the 1900’s and whose assistant, Frank Lloyd Wright, used the same principle of form follows function in his designs.
In product design, the auto industry introduced the stream-lined Chrysler Airflow in 1935, which had optimal aerodynamic efficiency. Unfortunately, the businessmen of the company real-ized that a teardrop shape for every car would not generate sales, and curtailed research in aerodynamics along the lines of form follows function.
Melvin Moss, in his 1954 thesis proposed an epigenetic the-ory of cranial growth regulation contradicting the classical cra-nial growth theory, “the sutural growth theory”, which stated that cell division occurring at the sutures is the driving force of bone growth.
To Dr. Moss the growth of the neurocranium was a response to the primary growth of the neural mass and the sutures were sites of secondary compensatory skeletal response to that growth.
“The skull consists of a series of functional components, each of which supports or protects specific, and operationally related soft tissues, termed functional matrices. All skeletal structural attributes reflect the morphogenetically and temporally prior demands of their matrices.”(Moss, M. “A functional approach to craniology.” Amer. J. Phys. Anthropol. 18:281-92, 1960.)
Theories of facial growth have always stimulated controver-sy, deriving from the original nature vs nurture debate. Growth is dependent on environmental and genetic factors. Genetics is further divided into intrinsic genetic factors, within the cell of origin, and epigenetic factors, similarly produced by the ge-
nome but exerting influence on other cells and tissues. Epigen-etic factors include how the growth of organs such as the orbit and brain occur; the role of the extacellular matrix molecules; the effect of cytokines and growth factors, cell adhesion molecules, and systemic hormones on growth. An example of an epigenetic effect is the ability of muscle function to determine the shape of bone.
Melvin Moss revised the classical doctrine of maxillary growth, described as the downward and forward translation of the dentomaxillary complex due to growth at the frontomaxil-lary, zygomaticomaxillary, zygomaticotemporal, and pterygopala-tine sutures. He proved how the origin, growth, and maintenance of the skull and the skeleton depend upon the functional matrix, those tissue, organs and functioning spaces (oral cavity, nasal cav-ity) related to that skeleton. Form resulted from the functions of the adjacent organs. The growth of the middle third of the face is a response to the demands of respiration. To Dr. Moss, the pri-mary morphogenetic event in the middle face is providing space for the nasal complex to facilitate breathing. By applying an engi-neering principle, he showed that the anteroposterior foreshort-ening of the maxillary complex in a cleft palate patient was the result of a biomechanical collapse of the nasal frame and not of the inability of the nasal cartilage to ‘push’ the maxillary complex downward and forward.
The classic view of mandibular growth regarded the condyle as a primary growth center controlled by intrinsic genetic fac-tors. Growth at the condyle displaced the mandible downward and forward and regulated the relationship of the mandible and maxilla. Melvin Moss replaced this view with the concept of

The Journal of the Holistic Dental Association 13
bone growing as a functional unit, not just from the stimulus of the condyle, but including the body of the mandible, the condyle and the coronoid, angular and alveolar processes. Experimental support for the functional matrix theory of mandibular growth was provided by the results of condylectomy which showed that growth of the rest of the mandible was unaffected. Moss empha-sized that the condylar growth occurs as an adaptive response to the functional behavior of the oral cavity and orofacial muscula-ture and that some parts of the mandible only reach optimal size with the full development and functional activity of their associ-ated muscles (Craniofacial Development, Growth And Evolution, Murray C. Meikle).
Melvin Moss based his functional cranial hypothesis on his study and measuring of the craniological collections in the Amer-ican Museum of Natural History and on the anatomical literature of the time, namely. On Growth and Form by D’Arcy Wentworth Thompson and The Development Of The Vertebrae Skull by Gavin de Beer. He built on the theories that went before. In the lab, reports his wife and colleague, Dr. Letty Moss-Salentijn, he used the approach, “If you want to test whether a structure is respon-sible for a specific parameter of growth, remove the structure and see what happens to that parameter.” (Moss-Salentjn, L. Melvin Moss and the functional matrix. J Dent Res. 76.(12)1997). Other labs tested and verified Melvin Moss’ thesis, first with intramem-branous bone, the major classification of bone that forms the skull. Bone forms in 2 ways either by intramembranous ossifica-tion or endochondral ossification.
The first stage in the development of bone is the migration of mesenchymal cells (embryonic connective tissue cells) into the area of bone formation, at about the 6th or 7th week of embry-onic development. These cells increase in size and number and differentiate. Some cells become chondroblasts, which form car-tilage, and bone, and some cells become osteoblasts.
Whether bone or cartilage is the more primitive tissue is still undecided, but the distinction has long existed. Aristotle, who lived 384-322 BC, separated fish into chondrichthyes and osteicthyes. The skeleton of the most primitive living fish–the lampreys–is cartilaginous. But in extinct jawless craniates, the exoskeleton consists of a type of acellular bone with dentine tu-bercles.
Cartilage and bone form from the same mesenchymal stem cell and their differentiation may well be determined, as Melvin Moss taught, by their functional imperative.
Bones formed by intramembranous ossification are the flat bones of the skull, most parts of the mandible, and parts of the clavicle. Osteoblasts cluster in the fibrous membrane and become a center of ossification. The cells secrete a matrix composed of collagen, proteins, and glycoproteins, in which calcium salts and other minerals are deposited. A network of trabeculae or bony spicules with vascular spaces radiates outward from the initial site of ossification until it meets other trabeculae, which become
united by fibrous joints called sutures or fuse into the open lat-ticework of spongy bone. The spaces between the trabeculae fill with red marrow. The original connective tissue that surrounds the growing bone becomes periosteum.
Dr. Moss conjectured that the principle of the functional matrix would be applicable not only to sutures and intramem-branously formed bones but also to endochondrally formed bones–the vertebrae, the long bones, and most of the bones in the body.
Endochondral ossification is the replacement of cartilage by bone. Again the mesenchymal cells proliferate and differentiate and the chondroblasts lay down an extracellular matrix of colla-gen and chondroitin sulfate proteoglycans. Early in the embryo, a cartilage model or template of the future bone is laid down and covered by a membrane called the perichondrium. Blood vessels penetrate the perichondrium and stimulate cells in the internal layer to enlarge and become osteoblasts and form a periosteal bony collar. Cartilage cells hypertrophy and burst. This changes the pH, making it more alkaline and causing calcification and deposition of minerals. When the cartilage cells die, they leave large cavities and blood vessels migrate in and a marrow cavity is formed.
Dr. Moss viewed cartilage as just one of many connective tis-sues in the body whose differentiation was established because of site-specific biomechanical conditions.
For example, growth in the articular cartilage of the condyle represented evidence of a compensatory secondary growth re-sponse to the primary growth of the mandible down due to the function of mastication.
As far as the role of the cranial cartilage, in the basicranial synchondroses, Dr. Moss believed that they were similarly con-trolled by the functional matrix and not under genetic control. He devised an experiment, using a drug that would affect the functional matrix but not the skeletal tissue, and demonstrated that if the growth of the brainstem was reduced, the spheno-oc-cipetal synchondroses was affected and would not grow indepen-dently.
Bone is constantly remodeled. In the adult, there is a balance between the amount of bone resorbed and the amount formed. This maintains mineral homeostasis, acid/alkaline balance, adap-tation to mechanical loading, and the structural integrity of the organism. It has been estimated that there is a complete turnover of the human skeleton every 10 years.
Dr. Melvin Moss’ theory of the functional matrix revo-lutionized our view of bone and made us aware that bone is a dynamic and mobile tissue whose form is dependent on use and the influences of surrounding tissues and other loads. This new paradigm has changed the way we practice orthodontics and supports the principles of cranial osteopathy. The func-tional matrix theory is a holistic approach to the biomechanics of bone.
DENTAL MATERIALS SUMMIT2 0 0 6AVAILABLE
NOW!AVAILABLE
NOW!
HDA ConferenceNewark, New Jersey
This seminar will teach you:• Latest bleaching concepts and techniques• Newest generation dentin adhesive systems• New Universal Composite Resins• Latest role of glass ionomers in restorative dentistry• Newest concepts in posts and cores• Metal-free crown and bridge systems• Current concepts and techniques for treatment of cavity preparations• How to test and select biocompatible materials• Current concepts in nutritional treatment
Special Offer!Get The Whole SummitFor Just $325 Cassette /
$425 CD / $475 DVD
Tape CD DVD Amount Thursday Morning, March 23
Dr. Doug Cook – Dental Materials w/ 8-page handout $52 $65 $112Dr. Jim Kennedy – Nutrition w/ 37-page handout $52 $65 N/AThursday Afternoon, March 23
Jess Clifford – Dental Materials $52 $65 $112Dr. Jeff Moss – Nutrition w/ handout $52 $65 N/AFriday, March 24
Dr. Robert Marshall – Dental Materials w/ 48-page handout
$89 $115 $210
saturday, March 25
Dr. Karl Leinfelder – Dental Materials w/ 24-page handout
$89 $115 $210
sPeCIAL PRICe for entire set $325 $425 $475Shipping & Handling (all orders) $5.00
TOTAL ORDeR
ORDeR FORM Please Print
Date: _______________________________________
Form of Payment: q Check q Visa q MasterCard
Credit Card #: _________________________________
exp. Date: ____________________________________
Name: ______________________________________
Address: _____________________________________
___________________________________________
City: _______________ state: ________ ZIP: ______
signature ____________________________________
PLeAse FAX YOUR ORDeR TO (619) 615-2228 • Holistic Dental Association • PO Box 151444 • san Diego, CA 92115 • Phone: (619) 923-3120

The Journal of the Holistic Dental Association 15
Vitamin D – The Antibiotic? New discoveries shed light on the importance of the “sunshine vitamin”
Vitamin D is continuing to make headlines as an extremely im-portant nutrient. Not only is it essential for controlling osteoporosis, especially in the elderly, but also it may well be a factor in limiting MS.
Now Vitamin D is being called, “THE ANTIBIOTIC VI-TAMIN”, based on the work of Adrian F. Gombart who reported that Vitamin D boosts production in white blood cells of the anti-microbial, CATHELICIDIN, that defends the body against bac-teria, viruses, and fungi. Further contributions were made by John J. Cannell, a psychiatrist at Atascadero California State Hospital, who gave his patients Vitamin D, simply because they, like most of the population, were deficient. He noticed that when a flu epidemic hit the State Hospital, only his patients did not get the flu, and proposed that Vitamin D was the protective agent.
The hormone 1,25-D, the active form of Vitamin D, binds to short sequences of DNA and these sequences switch on the activ-ity of adjacent genes, one of which is the antimicrobial peptide, CALTHELICIDIN.
More studies are continuing, but the preliminary data shows that “d sunshine vitamin” and exposure to sunlight are protective against colds, flu, and other respiratory infections.
In some cases, taking vitamin D supplements to compensate for a shortage of sunlight may stop diseases before they start. A 2001 study found that giving Finnish children 2,000 IU of vitamin D each day starting at age 1 reduced the risk of Type 1 diabetes by 80%.
Generous amounts of D also seem to strengthen bones and pre-vent fractures. A 2005 study in the Journal of the American Medical Assn. found that an extra 700 to 800 IU of vitamin D, taken with or without calcium, reduced the risk of hip fractures in post-meno-pausal women by 26%.
The immune reaction known as inflammation, which can also be a leading player in gum disease and tooth loss (SN: 2/24/01, p. 116: Avail-able to subscribers at http://www.sciencenews.org/articles/20010224/fob2.asp), may be reversed by Vitamin D. Low blood concentrations of vitamin D were linked to gum disease in a study of 11,200 men and women who had taken part in the federally sponsored National Health and Nutrition Examination Survey, Thomas Dietrich of Boston Uni-versity’s dental school and his colleagues report.
The rate of loss in tooth-gum attachment was 25 percent higher among those participants with the least vitamin D com-pared to those with the most vitamin. Since poor attachment cor-related with low vitamin D even when bone density was taken into account, the investigators believe that the observed effect reflected vitamin D’s positive impact on immunity. In the July, 2006, is-sue of American Journal of Clinical Nutrition, they conclude that Vitamin D “may be important for preventing tooth loss.”
David Feldman of Stanford University School of Medicine explains.
“What’s now clear is that Vitamin D is a potent force in regulat-ing cell growth, immunity, and energy metabolism.”
He is the editor of a 1300 page compilation of research findings from more than 100 labs working on Vitamin D.
“Not only is the vitamin gaining increasing respect as a governor of health but it’s also serving as a model for drugs that might tame a range of recalcitrant diseases.”
Calling Vitamin D a vitamin is a mistake as a vitamin is an es-sential food that the body can’t make, but we can make vitamin D in our skin, using cholesterol molecules as precursors and sunshine as an activator. Once vitamin D is available, the body converts it first into 25-hydroxy vitamin D and then into 1,25-dihydroxy vitamin D (1,25-D). This final form, which is actually a hormone, is the only active variety. Researchers loosely refer to all three substances in this biochemical cascade as “vitamin D.”
The American Journal of Clinical Nutrition, July 2006, contains a review article on optimal serum concentrations of 25-hydroxyD for multiple health outcomes. The abstract states “This review summarizes evidence from studies that evaluated thresholds for se-rum 25(OH)D concentrations in relation to bone mineral density (BMD), lower-extremity function, dental health, and risk of falls, fractures and colorectal cancer. For all endpoints, the most advanta-geous serum concentrations of 25(OH)D begin at 30 ng/mL and the best are between 36-40 ng/L.”
lATeST NeWS ON VITAMIN DIn children with epilepsy on anticonvulsant drugs, Vitamin D
metabolism is compromised and the children exhibit the symptoms of Vitamin D deficiency. The mechanism of action appears to be ac-celerated catabolism of Vitamin D. Drugs implicated are phenytoin, phenobarbital, carbamazapine, valproic acid. 25 OH D is recom-mended in patients taking anticonvulsants.
Adrian F. Gombart reported that Vitamin D boosts production in white blood cells of the antimicrobial, CATHELICIDIN, that defends the body against bacteria, viruses, and fungi.

16 The Communicator
CITATIONS “Steroid and xenobiotic receptor and Vitamin D receptor cross-
talk mediates CYP24 expression and drug-induced osteomalacia.” Zhou, C, etal. J Clin Invest.2006 Jun;116(6). Epub 2006 May 11
“Effect of carbamazapine and valproic acid on bone mineral density, IGF-1 and IGFBP-3.” Kumandas S. etal. J Pediatr Endocri-nol Metab. 2006 Apr;19(4):529-34
“Bone mineral density and serum levels of 25 OH vitamin D in chronic users of antiepileptic drugs.” Kulak CA, etal. Arq Neurop-siquiatr. 2004 Dec;62(4):940-8. Epub2004 Dec 15.
“Bone metabolism and vitamin D levels in carbamazapine-treated patients.” Verrotti A.etal. Epilepsia.2006 Sep;47(9):1586; author reply 1586-7.
“Effects of anticonvulsant therapy on vitamin D status in chil-dren: prospective monitoring study.” Nicolaidou P., etal. J Child Neurol 2006 Mar;21(3):205-9.
Fluoride: Friend or Foe?
Fluoridation of community water is one of the top 10 public health achievements of the 20th century. Yet, there is enormous con-troversy about fluoride. Do the benefits outweigh the risks? The major benefit is reduced caries. 1.6 fewer cavities is the most optimis-tic statistic, and this is provided by the ADA. Many people believe that the toxicity of fluoride is not worth the decrease in cavities.
Profluoride legislation has been defeated or tabled in Oregon, Arkansas, Nebraska, Hawaii, California, Colorado, Iowa, Missouri, NY, Ohio, Utah, Washington.
Other established organizations have issued warnings.The FDA placed a warning on toothpaste with fluoride: “if
more than used for brushing is accidentally swallowed, get medical help or contact a poison control center.”
The CDC issued guidelines stating that in communities with non-fluoridated water the only children who should get fluoride pills are those at high risk for decay, due to familial tendencies.
In March, 2006, a panel of dentists, toxicologists, and research-ers, assembled by the National Research Council, under the umbrel-la of the National Academy of Sciences, determined that the current level of fluoride, 4ppm, in community water, is too high, and that fluoride, rather than preventing decay, might initiate decay, as too much fluoride causes mottling and softening and more susceptibility to decay(fluorosis). Even more alarming, the committee reported that fluoride may have systemic effects-- such as lowering of IQ–as much as 8 points–and that over a lifetime the ingestion of fluoride could weaken bones and increase fractures.
Also in the spring of 2006, a Harvard doctoral study suggested an association between fluoride in water and osetosarcoma.
No one disputes the fact that fluoride, a natural element found in rocks and groundwater, protects tooth enamel. Since 1945, mu-nicipal systems serving 170 million Americans have added fluoride (mostly in the form of hydrofluorosilicic acid) to their water, and the prevalence of cavities in the U.S. has fallen dramatically. But good nutrition and healthy dental habits may protect from decay as well as fluoride.
What has changed since 1945 is how much toxicologists know about the harmful effects of fluoride compounds. Ingested in high doses, fluoride is indisputably toxic; it was once commonly used in rat poison. Hydrogen fluoride is regulated as a hazardous pollutant in emissions from chemical plants and has been linked to respira-tory illness.
The Australian and New Zealand Journal of Public Health reviewed the scientific literature on the effects of fluoride on bone structure and reported that 5 major epidemiological studies from the US, United Kingdom, and France, show a higher rate of hip fractures in fluoridated regions.
And more studies continue to link fluoride to bone disease, cancer, and mental problems.
Time Magazine and Prevention Magazine informed the public of the “danger in the water supply”, in summer 2006, and advised their read-ers to raise questions about the necessity of fluoride with their dentists.
The ADA continues to support fluoridation and provide point-ers to help dentists respond to patient inquiries and refute the dan-gers of fluoride. A quote from the ADA:
“MAGAZINe ARTICle MAY CONFuSe ReADeRS ABOuT WATeR FluORIDATION SAFeTY
A cover story in the August issue of Prevention magazine, ‘The Danger in Your Water,’ contains what we believe is misin-formation about the safety of community water fluoridation. The article appears to misconstrue the findings of the recent National Research Council report. It also highlights a research analysis by a then-Harvard doctoral student that suggests a possible association between fluoride in water and osteosarcoma (a rare form of bone cancer). The ‘association’ found in this one, limited study, falls far below any scientific standard needed to establish a cause-and-ef-fect relationship.”
ALTeRNATIVes TO FLUORIDe
Practitioners concerned about the possible risks associated with fluo-ride use may wish to try some of the following:
MI Paste: GC America Inc: www.gcamerica.com
Cavistat: arginine bicarbonate/calcium carbonate-containing denti-frice. Contact: Ortek Therapeutics Inc. [email protected]
Magnesium
Milk of Magnesia

The Journal of the Holistic Dental Association 17
A History of FluorideAs Presented in Prevention Magazine by Timothy GowerAs researched by Joel Griffiths in “Covert Action Quarterly” #42 and reported by Dylana Accolla, licAcup
1850: Fluoride emissions from iron and copper industries are poi-soning livestock, crops, and people.
1900: Lawsuits and heavy regulations threaten to put an end to these industries in Germany and England. The invention of the tall smokestack saves those industries by dispersing fluorides and other toxins into the upper air, so less of it directly effects living creatures below.
1909: Colorado Springs dentist Frederic K. McKay asks the US den-tal community to help him find an explanation for the “Colorado brown stain,” a discoloring of teeth common to the Pikes Peak area.
1927: A dentist in Bauxite, AR, reports extensive staining of resi-dents’ teeth. The town gets its water from a deep well near the site of an aluminum mine; fluoride is a waste by-product of aluminum mining.
1931: The Public Health Service, under the leadership of Andrew W. Mellon, US Treasury Secretary and a founder and major stock-holder of the Aluminum Company of America (Alcoa), sends a dentist named Trendley Dean to several remote Western towns where drinking water contains high concentrations of natural fluo-ride from deep in the earth’s crust to determine the effect of fluoride in the drinking water. He learns that fluoride discolors the teeth but the people in the towns have fewer cavities.
1933: The world’s first major air pollution disaster, in the Meuse Val-ley, Belgium, involves fluoride poisoning. Several thousand people become violently ill and die.
1937: Danish fluoride researcher Kaj E. Roholm, MD, Copenhagen’s deputy health commissioner, publishes a 364-page report titled Flu-orine Intoxication. In it, he details the bone disease, skin lesions, and mortality that result from long-term exposure to fluoride. He also questions its ability to protect teeth.
1939: Researcher Gerald J. Cox at the Mellon Institute in Pittsburgh releases results from a rat study (showing healthier teeth) to support his recommendation that water be fluoridated. Cox gets help from Edward L. Bernays, a nephew of Sigmund Freud who pioneered the application of Freud’s psychological theories to advertising and gov-ernment propaganda. “If you can influence the [group’s] leaders, ei-ther with or without their conscious cooperation,” wrote Bernays in his 1928 book Propaganda, “you automatically influence the group which they sway.” The main targets of Bernays advertising blitz are doctors and dentists. Under Bernays’ media tactics, a quick shift in peoples’ perception of fluoride begins to take place.
1942: A National Institutes of Health study of 7,000 children shows
that fluoride at 1 part per million (ppm) in water is enough to mini-mize tooth decay without causing discoloration–or dental fluorosis, as it’s now called.
1945: Federal scientists choose four pairs of cities for a 13- to 15-year study of fluoridation: Grand Rapids and Muskegon, MI; Newburgh and Kingston, NY; Evanston and Oak Park, IL; and Brantford and Sarnia, Ontario. Grand Rapids becomes the first city in the world to have fluoridated water.
1951: Muskegon, the comparison city for Grand Rapids, begins fluori-dating its own water supply. Communities across the country join in, well in advance of any published results of the four-cities studies.
1955: Procter & Gamble introduces Crest, the first fluoride tooth-paste endorsed by the American Dental Association.
1962: Results from the Grand Rapids study are published. The find-ings are called into question because the control was dropped 6 years into the study.
1964: The movie Dr. Strangelove or: How I Stopped Worrying and Learned to Love the Bomb is released. In it, an insane general, Jack D. Ripper, attributes fluoridation to a communist plot.
1977: A federal report finds evidence that Americans’ consumption of fluoride from food and water has increased significantly. At these levels, the report states, bone damage is a risk.
1990: As part of its “Healthy People 2000” plan, the CDC sets a goal of getting fluoridated water to 75% of Americans. Then, as now, roughly two-thirds have treated water.
1993: A government review board, the National Research Council, issues a report indicating that the variety of fluoride sources in the United States could make limiting fluoride exposure necessary, and “reduction of fluoride concentrations in drinking water would be easier to administer, monitor, and evaluate” than alternative cut-backs.
1997: The FDA requires toothpaste manufacturers to place a poi-son control label on tubes and boxes reading: If more than used for brushing is accidentally swallowed, get medical help or contact a Poison Control Center right away.
2001: The CDC issues new guidelines saying that fluoride supple-ments should only be given to children in nonfluoridated commu-nities who are also at high risk of cavities.
2006: The NRC releases a report suggesting that the current upper limit for fluoride in water could cause tooth damage, bone fractures, and neurological problems and may be connected to certain can-cers. It recommends the EPA lower the safe exposure limit.
Addenda: The US Public Health Services has endorsed silicofluo-ride, a chemical by-product of various industries, to be added to wa-ter as a cheaper substitute for naturally occurring sodium fluoride. Research since 1975 has shown that it is much more toxic than so-dium fluoride.
18 The Communicator
Join Our Teleconferences!These are FREE opportunities to learn without cost or travel, and enhance your practice! These confer-
ences are approximately one hour long, and take place about every other month. Simply call (888) 387-8686 at the appropriate time, enter the conference room number (2722323) followed by the # sign, then wait for the conference to begin. Many of these confer-ences will have handouts that you can download before the confer-ence on which to make notes.
Our next teleconferences are:Thursday, Feb. 22, 2007 and Tuesday, April 17, 2007 Both start at 8 pm (C.T.)The February conference will be on N.A.E.T. and how it can
help your dental patients overcome their allergies and multiple chemical sensitivities. The April conference will be on how to relax your anxious dental patients with storytelling and voice control.
In addition, you can listen 24/7 to previous educational con-ference calls (Building Biology, State Dental Boards 101, Reiki En-ergy Healing, Occlusal Cranial Balancing Technique, Oral Galva-nism). For playback information, go to our website, and click on “Member Services.”
www.holisticdental.org
Recommended ReadingNOTE: If anyone wants to recommend a
book or review a book, please contact the editor by writing to [email protected].
REIKI: A Comprehensive Guide by Pamela Miles (Tarcher/Pen-guin 2006) is the first mainstream book to address this increasingly common healing practice.
The author draws from 20 years of experience to present a rea-soned and researched overview of Reiki from its beginnings in 19th century Japan to the current widespread integration into conventional health care environments. She also reviews the state of research on the practice and the challenges involved.
Miles explains why Reiki is safe and articulates how Reiki can support well-being at all stages of life and be a resource for people ad-dressing a wide range of health challenges. Reiki’s increasingly docu-mented ability to quickly reduce anxiety and pain, and the flexibility of delivery makes it a good beginning for dentists wanting to expand into holistic care. But beware—there are no education or practice standards. You can learn to practice Reiki in a 10-12 hour training given by a Reiki master.
Miles includes guidance on how to find one and questions to help evaluate if a practitioner is credible.
Upcoming eventsIAOMT 2007 Spring MeetingInternational Academy Of Oral Medicine and ToxicologyMarch 15-17, Tuscon, AzContact: (863) 420-6373Topics:• Equipment for mercury-free practice• Fluoride and perio and political implications of fluoridation• Dental amalgam mercury release and effects• Practice management• Detox and nutrition• Biocompatible materials
Fordham Page Nutrition Study Club Presents:Balance the Chemistry; Balance the energyJames Braly, MD and Beth Gustafson, Medical IntuitiveMarch 23, 24, 2007Crown Plaza Washington, DCCourse Fee: $395Contact: (800) 832-9901 or (540) 635-3610
The Cranial Academy 60th Anniversary ConferenceJune 21-24, 2007, Tucson, ArizonaTucson Marriott University ParkContact: (317) 594-0411
upcoming Courses Offered at the International Center for Nutritional ResearchFor further information visit www.icnr.com
March 8, April 5 & April 19 (2007) • CEUs: 7 AGD CreditsIDI Seminar - Introductory Diagnostic Indicators: 1-Day Seminar. A prerequisite for all seminars : ALF, PAR, OCB and DBC,
March 9 & 10 (2007) • CEUs: 14 AGD CreditsAlF Seminar: Dynamics of Correcting Dental Orthopedic Distortions FIRST TIME OFFERED: March 30 & 31 (2007) • CEUs: 14 AGD Credits. QNC Seminar: Quantum Nutrition Concepts
April 6 & 7 (2007) • CEUs: 28 AGD Credits. OCB Seminar: Occlusal Cranial Balancing Technique.
April 20 & 21 (2007) • CEUs: 14 AGD Credits. PAR Seminar: Physiologic Adaptive Range Concept; diag-nose and resolve difficult cases
May 4 & 5 (2007) • CEUs: 14 AGD Credits. DBC Seminar: Dental / Whole Body Connection; learn to diagnose the dental origins of medical problems
2007
The Journal of the Holistic Dental Association 19
HOLISTIC DeNTAL ASSOCIATION DIAGNOsTIC sUMMIT 2007
October 17 -20Tuscany Hotel & Casino • Las Vegas, NV
• Participateinpeerdiscussions• Findoutaboutnewdevelopments• Learnfromourdistinguishedguestspeakers• Andmore!
DON’T MIss THIs sPeCIAL eVeNT!
For more information, visit www.holisticdental.org
Clinical PearlsJewels for safe Removal of Defective Amalgam RestorationsBy Dr. Harold Ravins
Before removal of amalgam:1. Check the levels of:
GlutathioneMagnesiumVitamin CSeleniumVitamin ELipoic acidAcetyl cysteine
(Note a deficiency or excess) 2. To determine if the blood/brain barrier is intact, check the
levels of the following neurotransmitters:Acetylcholine chlorideAdrenalineBeta Endorphin
•••••••
•••
DopamineGamma amino butyric acidHistamineL-TryptophanNorepinephrine
3. Evaluate the presence and load of Heavy Metals in the body by fecal testing, using Doctors Data Laboratories.
4. Have the patient give you a complete list of all supplements he/she presently takes.
5. Check biocompatibility of all materials used.
During removal of amalgam:1. Use rubber dam, high power suction, mercury ionizer, ster-
ile O2 mask on the nose2. Use a new carbide #1156 bur for all teeth3. Inform the patient that the basic removal will take under 35
seconds per amalgam.4. Remove corrosive debris with slow round bur5. Rinse cavity with antioxidant6. Replace the amalgam with Fuji 9, for the first phase of re-
storing tooth.7. Restore the tooth permanently with a tested nonreactive
material-- filling, inlay, onlay, or crown.
•••••
20 The Communicator
PO Box 151444San Diego, CA 92175
THe COMMUNICATORVisit us on the web: www.holisticdental.org
The Most Effective Truly Natural®
Anti-microbial and Anti-halitosis Products Ever Developed!1-800 -747-4372
DENTAL HERB COMPANY ®
PROFESSIONAL STRENGTH, TRULY NATURAL® ORAL HYGIENE PRODUCTS
Time tested botanicalremedies for modernPeriodontal and Halitosis Therapy.
Commumicator ad color 7.75x5.375 6/20/06 11:14 AM Page 1





























