Embed Size (px)
Citation preview

When Is Diabetes DistressClinically Meaningful?Establishing cut points for the Diabetes Distress Scale
LAWRENCE FISHER, PHD, ABPP1
DANIELLE M. HESSLER, PHD1
WILLIAM H. POLONSKY, PHD, CDE2
JOSEPH MULLAN, PHD3
OBJECTIVEdTo identify the pattern of relationships between the 17-item Diabetes DistressScale (DDS17) and diabetes variables to establish scale cut points for high distress among patientswith type 2 diabetes.
RESEARCH DESIGN AND METHODSdRecruited were 506 study 1 and 392 study 2adults with type 2 diabetes from community medical groups. Multiple regression equationsassociated the DDS17, a 17-item scale that yields a mean-item score, with HbA1c, diabetesself-efficacy, diet, and physical activity. Associations also were undertaken for the two-itemDDS (DDS2) screener. Analyses included control variables, linear, and quadratic (curvilinear)DDS terms.
RESULTSdSignificant quadratic effects occurred between the DDS17 and each diabetes vari-able, with increases in distress associated with poorer outcomes: study 1 HbA1c (P, 0.02), self-efficacy (P , 0.001), diet (P , 0.001), physical activity (P , 0.04); study 2 HbA1c (P , 0.03),self-efficacy (P , 0.004), diet (P , 0.04), physical activity (P = NS). Substantive curvilinearassociations with all four variables in both studies began at unexpectedly low levels of DDS17: theslope increased linearly between scores 1 and 2, was more muted between 2 and 3, and reached amaximum between 3 and 4. This suggested three patient subgroups: little or no distress, ,2.0;moderate distress, 2.0–2.9; high distress, $3.0. Parallel findings occurred for the DDS2.
CONCLUSIONSdIn two samples of type 2 diabetic patients we found a consistent pattern ofcurvilinear relationships between the DDS and HbA1c, diabetes self-efficacy, diet, and physicalactivity. The shape of these relationships suggests cut points for three patient groups: little or no,moderate, and high distress.
Diabetes Care 35:259–264, 2012
D iabetes distress (DD) refers to theunique, often hidden emotional bur-dens and worries that are part of the
spectrum of patient experience when man-aging a severe, demanding chronic diseaselike diabetes (1). High levels of DD arecommon (prevalence, 18–35%; 18-monthincidence, 38–48%) and persistent overtime, and they are distinct from clinical de-pression in their linkages with glycemiccontrol and disease management (2–4).High levels of DD have been significantlyassociated with poor glycemic control,poor self-care, low diabetes self-efficacy,and poor quality-of-life, even after control-ling for clinical depression (5).
A critical concern is the establishmentof a reliable and valid cut point or crite-rion to define high DD so that furtherassessment and/or intervention might beinitiated. Use of a standard cut point alsoenhances consistency of findings acrossstudies and provides a uniform criterionfor identifying patients at risk. In thisstudy, we examined the relationship be-tween the 17-item Diabetes Distress Scale(DDS17) (6), a widely used factor-analyzed, theory-driven, self-report survey,and several diabetes biologic and manage-ment measures in two samples of patientswith type 2 diabetes. We also included acomparable analysis of the 2-item DDS
(DDS2) screener, based on the 17-itemscale (7). Our goal was to identify the de-gree and pattern of relationships betweenDDS scores and diabetes behavioral andbiologic variables to define cut points forhigh DD for use in clinical and researchsettings.
Although there is no universally ap-plicable method for determining a scalecut point, empiric approaches fall intotwo categories (8,9). A data-oriented ap-proach dichotomizes a scale at a prespe-cified point along the scale distributionand compares those above the cut pointwith those who reach criterion using agold standard measure. For example,scores from the Patient Health Question-naire 9 (10), a depression survey, werecompared with scores on a gold standard,structured psychiatric interview like theComprehensive International DiagnosticInterview (11). A second approach toestablishing a scale cut point is most oftenused when no gold standard measure isavailable or practical. It observes the cova-rying relationships between the score dis-tribution of the scale of interest with thesame respondents’ scores on other relevantvariables or outcomes. Using the DDS, forexample, we might observe the linear andquadratic (curvilinear) relationships be-tween DDS scores and scores on diabetesself-efficacy, disease-management, and/orHbA1c. This analysis would tell us notonly how substantive the relationshipswere but also where along the scale distri-butions these relationships occurred, whatform they took, and where a cut pointmight best be placed.
Because we found no logical, face-valid justification for selecting a specificDDS score for a cut point and becausethere currently is no gold standard mea-sure of high DD, we adopted the latterapproach: the optimal categorization ofDD in relation to key diabetes-specificbiologic (HbA1c) and behavioral (e.g., di-abetes self-efficacy, diet, physical activity)variables, after adjusting for demographicsand disease status. Linear and nonlineartermswere included to enhance comprehen-siveness. Because the shape and degree ofrelationship between score distributions can
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c
From the 1Department of Family & Community Medicine, University of California, San Francisco, SanFrancisco, California; the 2Behavioral Diabetes Institute, San Diego, California; and the 3School of Nursing,University of California, San Francisco, San Francisco, California.
Corresponding author: Lawrence Fisher, [email protected] 16 August 2011 and accepted 29 October 2011.DOI: 10.2337/dc11-1572© 2012 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and thework is not altered. See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
care.diabetesjournals.org DIABETES CARE, VOLUME 35, FEBRUARY 2012 259
C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o n / P s y c h o s o c i a l R e s e a r c hO R I G I N A L A R T I C L E

vary by patient sample, we separately an-alyzed data from two independent com-munity samples of patients with type 2diabetes.
RESEARCH DESIGN ANDMETHODS
SubjectsBaseline samples from two studies of de-pression and distress among adult type 2diabetic patients were included. Study 1,our primary sample, used baseline datafrom the Distress and Depression in Di-abetes Study (3D Study), a noninterven-tional, three-wave, 18-month study of theprevalence and persistence of DD and de-pressive symptoms among 506 adult type 2diabetic patients (2). Data were collectedbetween 2003 and 2006. Study 2 usedbaseline, preintervention data from the Re-ducing Distress and Enhancing EffectiveManagement (REDEEM) Study, a random-ized controlled trial designed to reduce DDand enhancemanagement among 392 type2 diabetic adults (12). These data were col-lected between 2008 and 2010. Patients inboth studies were recruited using the dia-betes registries of several Bay Area commu-nity-based medical groups and diabeteseducation centers.
Inclusion criteria for both studies werepatients with type 2 diabetes for 12monthsor more, age 21 years or older, read andspeak English fluently, no severe diabetescomplications, and no active psychosis,substance use, or dementia. Additional,more restrictive criteria for REDEEM Studypatients included displaying a mean itemscore of 1.5 or higher on the DDS2 toindicate elevated DD, displaying a scoreof 15 or higher on the Patient HealthQuestionnaire 8 to exclude patients withclinical depression, and displaying a def-icit in at least one of three areas of dia-betes self-management (diet, physicalactivity, medication use). A modificationof the Summary of Diabetes Self-care Ac-tivities (SDSCA) (13) was used to define adeficit as not following their diet or phys-ical activity plan 3 or more days duringthe last week or not taking prescribed di-abetes medications 2 or more days duringthe last week.
ProcedureFor both studies, letters were sent to eachpatient from their health care facility,cosigned by facility and project represen-tatives, informing them of the project andthat they would receive a phone call fromthe project office if one of two opt-out
procedures was not initiated: patient re-turned an enclosed postcard or called an800 phone number. A screening phonecall followed and, for eligible patients, anappointment was made to explain theproject in detail, collect informed con-sent, and begin the baseline assessment.Baseline assessment in both studies in-cluded a 1.5-h home visit for completionof questionnaires, physical measurements,and interviews, as well as a visit to a com-munity laboratory for collection of bloodand urine specimens. All data included inthe present report were from the baselineassessment only. Both studies were ap-proved by the institutional review boardsat theUniversity ofCalifornia, SanFrancisco,and at each participating facility.
MeasuresControl variables for both studies includedpatient age, sex (female = 1, male = 0),education, ethnicity (white = 1, nonwhite =0), years with type 2 diabetes, use of insulin(yes or no), and BMI.
The DDS is a 17-item measure thatuses a Likert scale to score each item from1 (no problem) to 6 (a serious problem)during the lastmonth (a = 0.93) (6).Mean-item scores are then calculated (DDS17).Previous analyses identified that theDDS2 had good sensitivity and specificitywith the DDS17 (7) and was considered areliable screening composite for use inclinical practice.
The DDS17 and DDS2 were associatedwith four diabetes-related variables. HbA1C
was collected at a community facility andprocessed at the same community labora-tory in both studies. Also included weremeasures of diabetes self-efficacy, diet, andphysical activity, although different mea-sures were used in each of the two studies.3D Study. Diabetes Self-Efficacy is a 10-item scale (a = 0.88), adapted fromCoyneand Smith (14), that assesses the patient’sperceived confidence about taking care ofdiabetes (15). Items are rated on a 4-pointscale from “not at all sure” to “very sure.”Diet and physical activity were assessedby the Summary of Diabetes Self-care Ac-tivities (13). Respondents indicated thenumber of days during the past weekthat they completed their diet and physi-cal activity regimens.REDEEM Study. Diabetes Self-Efficacywas assessed by a 15-item scale developedby Lorig et al. (16) (a = 0.88). Items arerated on a 10-point Likert scale. Diet wasassessed by five items from the “Startingthe Conversation” survey (17) that asksrespondents to indicate the number of
times per week during the past 4 monthsthat they ate certain types of unhealthyfoods (e.g., fast foods, sodas, sweet tea).Physical activity was assessed by theCommunity Healthy Activities ModelProgram for Seniors (18). Nineteen itemsregarding frequency of specific physicalactivities (e.g., walk fast or briskly, swim,ride a bicycle) assessed caloric expendi-tures per week in moderate-intensityphysical activity activities, capped at avalue of 6,000 calories (19).
Data analysisComparisons were undertaken between3D and REDEEM on key patient demo-graphics using x2 and t tests. Separatestep-wise multiple regression equationswere conducted for the DDS17 andDDS2 for each of the four dependent var-iables for each sample: step 1, demo-graphics and disease status; step 2, DDSscore (linear term); step 3, DDS score(quadratic term). Quadratic effects wereinterpreted only if the related t test, withone degree of freedom at step 3, was sig-nificant. The goal in these analyses was todetermine if the shape of the relationshipsyielded a common pattern that woulddefine a meaningful cut point for theDDS17 and DDS2. A minimum changeof 0.5 SD units in dependent variableswas used to help establish cut points(20). The results of each significant effectwere placed on scatterplots, with fittedlinear or quadratic lines, to examine theshape and start-point of the relationshipbetween each DDS score and each of thedependent variables. Mean-item DDS val-ues up to 4.0 were plotted because theseencompassedmore than 90%of the sampleand DDS values .4 were based on smallnumbers with greater error. Note that thedirection of the curves varies as a functionof the direction of the regression coefficientand the direction of the scale.
RESULTS
3D StudyDetails of the sample have been presentedpreviously (4). Screening identified 640eligible patients and 506 participated(79%), with no demographic or diabetesstatus differences between those who didand did not participate. The final samplewas 56.9% women, average age was57.79 (SD, 9.84) years, and average yearssince diagnosis was 8.14 (7.49) (Table 1).About 37% self-identified as white, 87.7%completed high school, and 15%of patientswere taking insulin.
260 DIABETES CARE, VOLUME 35, FEBRUARY 2012 care.diabetesjournals.org
DD cut points

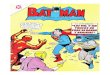
After step1 control variables wereentered into the equations, multiple re-gression analyses indicated significantlinear and quadratic effects between theDDS17 and each of the four dependentvariables (Table 2), with increases in DDassociated with poorer glycemic control(P , 0.02), self-efficacy (P , 0.001),diet (P , 0.001), and physical activity(P = 0.04). Figure 1 indicates that sub-stantive associations between DDS17and diabetes variables were evident atunexpectedly low levels of DDS17. Rela-tionships between the DDS17 and the de-pendent variables began linearly betweenDDS17 scores of 1 and 2, continued butwere somewhat muted between DDS17scores of 2 and 3, and reached a maxi-mum between DDS17 scores of 3 and 4.The significant increases in DDS17 mean-item scores across the four diabetes varia-bles increased by ;0.5 SD units for eachdependent variable for each of threeDDS17 score groups: below a DDS mean-item score of 2 (n = 276, 54.6%of patients),between a score of 2 and 3 (n = 139,27.4%), and above 3 (n = 91, 18.0%).
Findings from the DDS2 analyses ap-proximated those from the DDS17: aftercontrol variableswere entered into the equa-tions, significant linear and quadratic effectswere found for HbA1c (P = 0.02) and self-efficacy (P, 0.001), but only significant lin-ear effects were found for diet (P , 0.001)
and physical activity (P = 0.005; Table 1).Furthermore, where they occurred, theshape of the curvilinear relationships forthe DDS2 with the diabetes variables wasvirtually identical to those found for the fullDDS17 scale (data not shown): substantivelinear relationships began between a meanitem score of 1 and 2, continued but weremuted between scores of 2 and 3, andreached a maximum at a mean item scoreof ;4. Likewise, about a half-SD unit ofchange in each dependent variable oc-curred up to a mean-item score of 2, be-tween 2 and 3, and over 3.
REDEEM StudyOf 588 subjects who were screened aseligible, 392 (67%) completed the base-line assessment (Table 1). There were nosignificant differences between participat-ing and nonparticipating eligible patientson demographics or disease status. Aver-age age was 56.12 (SD, 9.5) years, 56.5%were women, and diabetes duration was7.9 (6.33) years. Almost all patients com-pleted high school (97.4%), ;40% iden-tified as white, and 18% were takinginsulin. Although REDEEM patients hadto meet more restrictive inclusion criteriathan 3D patients, between-group differ-ences were minimal: REDEEM Study pa-tients were slightly younger, had highereducation and initial diabetes distress, butdisplayed no HbA1C differences (Table 1).
Results from the multiple regressionanalyses for REDEEM paralleled 3D find-ings. After the control variableswere enteredinto the equations, significant quadraticeffects occurred for the DDS17 on HbA1c(P = 0.03), self-efficacy (P , 0.004), anddiet (P = 0.04), but not on physical activity(P = NS): high DDS17 was associated withpoor glycemic control, low self-efficacy, andpoor diet. As in the 3D Study, notable linearassociations between DDS17 and the diabe-tes variables occurred between DDS17scores of 1 and 2 (n = 135, 34.5% of pa-tients), continued between DDS17 scores of2 and 3 (n = 162, 41.3%), and a maximumwas observed between a mean-item score of3 and 4 (n = 95, 24.2%), with approximatechanges in half-SD units of the dependentvariables for each of the 3 DDS score inter-vals. Where they occurred, the degree andshape of the quadratic effects were virtuallyidentical to those in the 3D Study (Fig. 1).
For the DDS2, significant curvilineareffects occurred for HbA1c (P = 0.02), forself-efficacy (P = 0.05), and for physical ac-tivity (P = 0.03; Table 2).Where curvilineareffects were found, substantive linear rela-tionships occurred between a mean-itemscore of 1 and 2, with more muted linearincreases between scores of 2 and 3, and amaximumwas reached betweenmean-itemscores of 3 and 4. Approximate half-SD in-creases in the dependent variables occurredfor each DDS2 score interval and the degreeand shape of the curves were identical tothose in the 3D Study (Fig. 1). Only signif-icant linear effects occurred for the DDS2on diet (b= 0.21, P , 0.001), with highdistress associated with poor diet.
CONCLUSIONSdSignificant curvilin-ear relationships occur between the DDS17and measures of glycemic control, diabetes-specific self-efficacy, diet, and physical activ-ity in two community-based samples of type2 diabetic adults, with the exception ofphysical activity in REDEEM. The degreeand shape of these relationships are almostidentical for two patient samples of type 2diabetic adults: a highly diverse communitysample (3D Study) and a more restrictedcommunity sample that displayedhigh initiallevels of distress, no clinical depression, andpoor self-management (REDEEM Study).
The similar degree and shape of rela-tionships across studies, across dependentvariables, and across the DDS17 and DDS2highlight two important findings with re-spect to establishing a clinically meaningfulcut point for high distress. First, the signif-icant relationship of diabetes-specific dis-tress with each of the four dependent
Table 1dSample descriptions of 3D and REDEEM studies
Variable
3D Study REDEEM Study x2 orMean/n SD/% Mean/n SD/% t test P
Age (years) 57.80 9.85 56.10 9.56 2.60 0.01Female sex 288 56.9% 211 53.8% 0.85 0.36Education (years) 14.57 3.34 15.65 2.43 25.41 ,0.001Years since diagnosis 8.14 7.50 7.93 6.33 0.45 0.66White ethnicity 186 36.8% 157 40.1% 1.01 0.31Insulin 76 15.0% 70 17.9% 1.28 0.26BMI (kg/m2) 32.74 7.74 33.07 7.76 20.62 0.53HbA1c 7.25 1.44 7.41 1.60 21.52 0.13DDS17 2.10 0.96 2.40 0.88 24.72 ,0.001DDS2 2.26 1.31 2.82 1.27 26.42 ,0.001DDS4 2.25 1.26 2.79 1.19 26.45 ,0.001Self-efficacyStudy 1 2.98 0.62 d d d dStudy 2 d d 6.51 1.6 d d
DietStudy 1 4.13 1.56 d d d dStudy 2 d d 0.53 0.37 d d
Physical activityStudy 1 3.11 2.32 d d d dStudy 2 d d 1,899.52 1,797.27 d d
DDS4, four-item Diabetes Distress Scale.
care.diabetesjournals.org DIABETES CARE, VOLUME 35, FEBRUARY 2012 261
Fisher and Associates

variables begins at unexpectedly low levelsof distressdfar less DD is required todemonstrate a relationship with diabetes-specific biologic and behavioral indicatorsthan was previously considered. A previ-ous report suggested that a mean itemscore of 3.0 provided a valid cut pointfor highDD (7). Our new findings confirmand expand these findings: even rela-tively low levels of DD are associatedwith diabetes-related indicators.
Second, to help determine where anappropriate DDS cut point should be, wefocus on the notable consistency in theshape of the significant curvilinear relation-ships between the DDS17 across the de-pendent variables in both 3DandREDEEM:the curve rises linearly from a DDS17 meanitem score of 1 to 2, continues linearly butin a more muted fashion between scoresof 2 and 3, and reaches a maximum be-tween scores 3 and 4. We note also that,in general, there is an ;0.5 SD increase ineach of the four dependent variables corre-sponding to increases in DDS17mean itemscores from 1 to 2, 2 to 3, and above 3.
Findings for the DDS2 approximatethose for the DDS17, even with the manyfewer items and far less information con-tained in DDS2. The similar pattern ofsignificant linear and curvilinear effectsacross the four diabetes variables, thesimilar degree of association, and the sim-ilar shape of the respective curves of asso-ciation all suggest that the DDS2 behavesrelatively similarly to the DDS17 with re-spect to the four diabetes variables westudied.
These findings suggest that dichoto-mizing the distribution of DDS17 scores todenote a “high distress” group and a “lowdistress” group does not accurately reflectthe shape of the relationships between theDDS17 and the four diabetes indicators. Ittherefore may be more helpful to definethree DDS categories: “little or no DD”(DDS ,2.0), “moderate DD” (DDS = 2.0–2.9), and “high DD” (DDS$3.0). Creatingdefined categories of moderate and highDDprovides a better reflection of the shapeof these relationships across diabetes indi-cators than a single cut point and allows
greater flexibility for use in clinical and re-search settings.
3D Study results, based on a diversecommunity sample, indicate that 45.4% ofpatients with type 2 diabetes display at leastmoderate DD. (Percentages for REDEEMare considerably higherd65.5%dbecausethis study required high DD as an inclusioncriterion.) These findings suggest that sig-nificant levels of DD occur among almosthalf of patients with type 2 diabetes andthat the possible reciprocal influence ofDD on diabetes indicators indicates in-creased risk for poor treatment outcomes.Because ;70% of these patients are notclinically depressed (2), interventions forDD may best be focused on ongoing con-versations about DD and diabetes manage-ment in the clinical setting. Highly ratedDDS17 items can be used to identify areasof specific patient concern, and patients areoften relieved when clinicians initiate a dis-cussion that labels feelings overtly, linksthem with diabetes-related difficulties,and normalizes them in ways that provideboth reassurance and perspective (1). Even
Table 2dStandardized coefficients for DDS17 and DDS2 linear and curvilinear effects
Study
HbA1c Self-efficacy Healthy diet Physical activity
b P b P b P b P
3DStep 1 Sex (female = 1) –0.02 0.58 –0.01 0.79 –0.01 0.99 –0.08 0.07
Age –0.12 0.01 0.14 0.01 0.18 ,0.001 0.07 0.12Education –0.07 0.14 0.05 0.32 0.06 0.18 –0.01 0.97Ethnicity (white = 1) –0.15 0.001 –0.16 0.001 –0.04 0.44 –0.01 0.90Time since diagnosis 0.02 ,0.001 –0.13 0.02 –0.05 0.33 –0.04 0.42Insulin 0.19 ,0.001 0.03 0.60 0.05 0.35 –0.03 0.59BMI 0.06 0.20 –0.17 ,0.001 –0.15 0.001 –0.21 ,0.001
Step 2 DDS17 item linear 0.15 ,0.001 –0.44 ,0.001 –0.32 ,0.001 –0.10 0.03Step 3 DDS17 item linear 0.25 ,0.001 –0.71 ,0.001 –0.48 ,0.001 –0.19 0.003
DDS17 item quadratic –0.14 0.02 0.39 ,0.001 0.22 ,0.001 0.13 0.04Step 2 DDS2 item screener linear 0.17 ,0.001 –0.50 ,0.001 –0.32 ,0.001 –0.13 0.01Step 3 DDS2 item screener linear 0.26 ,0.001 –0.61 ,0.001 –0.35 ,0.001 –0.17 0.006
DDS2 screener quadratic –0.14 0.02 0.22 ,0.001 0.05 0.37 0.07 0.28REDEEMStep 1 Sex (female = 1) –0.02 0.61 –0.07 0.18 0.01 0.97 –0.29 ,0.001
Age –0.20 ,0.001 0.12 0.02 –0.06 0.32 –0.12 0.02Education 0.02 0.76 0.03 0.61 –0.05 0.38 0.01 0.94Ethnicity (white = 1) –0.11 0.04 0.03 0.53 –0.04 0.42 0.01 0.81Time since diagnosis 0.16 0.01 0.06 0.29 –0.02 0.76 –0.01 0.89Insulin 0.23 ,0.001 –0.05 0.66 0.03 0.65 –0.02 0.65BMI –0.01 0.83 –0.11 0.03 0.13 0.01 0.01 0.82
Step 2 DDS17 item linear 0.04 0.42 –0.38 ,0.001 0.22 ,0.001 –0.07 0.15Step 3 DDS17 item linear 0.11 0.07 –0.47 ,0.001 0.22 ,0.001 –0.12 0.05
DDS17 item quadratic –0.13 0.03 0.16 0.01 –0.13 0.04 0.08 0.17Step 2 DDS2 item screener linear 0.10 0.06 –0.37 ,0.001 0.21 ,0.001 –0.05 0.37Step 3 DDS2 item screener linear 0.15 0.007 –0.42 ,0.001 0.22 ,0.001 –0.10 0.08
DDS2 screener quadratic –0.13 0.02 0.10 0.05 –0.02 0.69 0.12 0.03
262 DIABETES CARE, VOLUME 35, FEBRUARY 2012 care.diabetesjournals.org
DD cut points

the verbalization of emotional experiencessurrounding diabetes can be therapeuticand can lead to action planning for behav-ioral change.
Several limitations are worthy of note.First, we included only four diabetes var-iables for study. The DDS17 may displaydifferent levels and patterns of associationwith other diabetes-related indicators. Sec-ond, we did not explore how patient de-mographic and diabetes-related factorsqualify these relationships; instead, wecontrolled for many of them in equations.Although our goal was to report findingswith the greatest generalizability, differ-ences in results may occur for subgroupsof patients. Last, our findings are cross-sectional and associational, such thatcausation between DD and diabetes indi-cators cannot be inferred. A previous studysuggested that these associations are bidi-rectional (2), with one affecting the othersequentially over time.
We used a data-oriented approach toestablish empirically DDS cut points forsignificant diabetes distress among adultpatients with type 2 diabetes. In two com-munity samples we show a consistent pat-tern of curvilinear relationships between theDDS and HbA1c, diabetes self-efficacy, diet,and physical activity. The degree and shapeof these relationships suggest cut points onthe DDS17 and the DDS2 for three patientsubgroups: those with little or no distress,moderate distress, and high distress.
AcknowledgmentsdThis research was sup-ported by grants DK062732 and DK061937from the National Institute of Diabetes andDigestive and Kidney Diseases.No potential conflicts of interest relevant to
this article were reported.L.F. wrote the manuscript. D.M.H. re-
searched data, completed the data analysis,contributed to discussion, and edited themanuscript. W.H.P. and J.M. researched data,
contributed to discussion, and edited themanuscript.Parts of this study were presented at the 71st
Scientific Sessions of the American DiabetesAssociation, SanDiego, California, 24–28 June2011.The following medical groups and diabetes
education centers collaborated in this research:Alta Bates Diabetes Education Center, Berkeley,California; Brown and Toland Medical Group,San Francisco, California; California PacificDiabetes Education Center, San Francisco,California; Hill Physicians Medical Group,San Ramon, California; and University ofCalifornia, San Francisco Hospital and Clin-ics, San Francisco, California.
References1. Gonzalez JS, Fisher L, Polonsky WH.
Depression in diabetes: have we beenmissing something important? DiabetesCare 2011;34:236–239
2. Fisher L, Mullan JT, Arean P, Glasgow RE,Hessler D, Masharani U. Diabetes distressbut not clinical depression or depressivesymptoms is associated with glycemiccontrol in both cross-sectional and lon-gitudinal analyses. Diabetes Care 2010;33:23–28
3. Fisher L, Skaff MM, Mullan JT, Arean P,Glasgow R, Masharani U. A longitudinalstudy of affective and anxiety disorders,depressive affect and diabetes distress inadults with Type 2 diabetes. Diabet Med2008;25:1096–1101
4. Fisher L, Skaff MM, Mullan JT, et al.Clinical depression versus distress amongpatients with type 2 diabetes: not just aquestion of semantics. Diabetes Care 2007;30:542–548
5. Fisher L, Mullan J, Skaff M, Glasgow R,Arean P, Hessler D. Predicting diseasedistress among primary care patients withtype 2 diabetes: a longitudinal study. Di-abet Med 2009;26:622–627
6. Polonsky WH, Fisher L, Earles J, et al.Assesing psychosocial stress in diabetes:development of the diabetes distress scale..Diabetes Care 2005;28:626–631
7. Fisher L, GlasgowRE,Mullan JT, SkaffMM,Polonsky WH. Development of a brief di-abetes distress screening instrument. AnnFam Med 2008;6:246–252
8. O’Brien SM. Cutpoint selection for cate-gorizing a continuous predictor. Biometrics2004;60:504–509
9. Williams BA, Mandrekar JN, Mandrekar SJ,Cha SS, Furth AF. Finding Optimal Cutpointfor Continuous Covariates With Binary adTime-to-Event Outcomes. Rochester, MN,Mayo Clinic, Technical Report Series, 2006
10. Spitzer RL, Kroenke K, Williams JB. Val-idation and utility of a self-report versionof PRIME-MD: the PHQ primary carestudy. Primary Care Evaluation of MentalDisorders. Patient Health Questionnaire.JAMA 1999;282:1737–1744
Figure 1dAssociations between 3D Study DDS17 scores and the key diabetes variables ofHBA1c (A), self-efficacy (B), healthy diet (C), and physical activity (D) using fitted quadraticlines.
care.diabetesjournals.org DIABETES CARE, VOLUME 35, FEBRUARY 2012 263
Fisher and Associates

11. Wittchen HU. Reliability and validity stud-ies of the WHOdComposite InternationalDiagnostic Interview (CIDI): a critical re-view. J Psychiatr Res 1994;28:57–84
12. Hessler DM, Fisher L, Naranjo D, MullanJT, Masharani U. Why do Younger AdultsHave Higher HbA1c Than Older Adults? TheRole of Diabetes Distress and MedicationAdherence (abstract). San Diego, CA, Amer-ican Diasbetes Association, 2011
13. Toobert DJ, Hampson SE, Glasgow RE. Thesummary of diabetes self-care activitiesmeasure: results from7 studies and a revisedscale. Diabetes Care 2000;23:943–950
14. Coyne JC, Fiske V. Couples coping withchronic and catastrophic illness. In FamilyHealth Psychology. Akamatsu TJ, Stephens
MA, Hobfoll SE, Crowther JH, Eds. Kent,Ohio, Hemisphere Publishing Corp, 1992,p. 94–113
15. Fisher L, Chesla CA, Skaff MM, et al. Thefamily and disease management in Hispanicand European-American patients with type2 diabetes. Diabetes Care 2000;23:267–272
16. Lorig K, Stewart A, Riter P, Gonzalez V,Laurent D, Lynch J. Outcome Measures forHealth Education and Other Health CareInterventions. Thousand Oaks, CA, SagePublications, 1996
17. Ammerman A. Starting the Conversation -Diet. Instrument Developed by the Univer-sity of North Carolina, in Conjunction withthe NC Prevention Partners, and the HeartDisease and Prevention Branch. Raleigh,
NC, North Carolina Department of Healthand Human Services, 2004
18. Stewart AL, Mills KM, King AC, HaskellWL, Gillis D, Ritter PL. CHAMPS physicalactivity questionnaire for older adults:outcomes for interventions. Med Sci SportsExerc 2001;33:1126–1141
19. GlasgowRE, Christiansen SM, KurzD, et al.Engagement in a diabetes self-managementwebsite: usage patterns and generalizabilityof program use. J Med Internet Res 2011;13:e9
20. Norman GR, Sloan JA, Wyrwich KW.Interpretation of changes in health-relatedquality of life: the remarkable universalityof half a standard deviation. Med Care2003;41:582–592
264 DIABETES CARE, VOLUME 35, FEBRUARY 2012 care.diabetesjournals.org
DD cut points