-
Review article Annals and Essences of Dentistry
Vol. - II Issue 3 July Sept. 2010 137
XEROSTOMIA: DENTAL IMPLICATIONS AND MANAGEMENT.
*Ramandeep Dugal
*Professor, Department of Prosthodontics, MA Rangoonwala Dental
College, Pune
ABSTRACTXerorstomia or dry mouth is common among older adults
and may be caused by systemic diseases,medications and head and
neck radiotherapy. Individuals with Xerostomia complain of problems
withmastication, phonetics, deglutition and wearing dentures. Lack
of saliva may predispose one to oral infectionssuch as Candidiasis
and increased risk of dental caries. Dentists should be able to
diagnose this condition andadminister appropriate treatment to
provide acceptable level of comfort and function to their
patients.
KEYWORDS: Xerostomia, Saliva, Dental implications,
Management.
INTRODUCTION:Xerostomia is defined as dry mouth resulting
from
reduced or absent salivary flow. Saliva plays acritical role in
the preservation of oropharyngealhealth and persistent dry mouth
and salivarydysfunction can impair a persons quality of
life.Xerostomia is a common complaint among olderadults and
according to a study 30 percent ofpopulation aged 65 and above
experience thisdisorder1. Though salivary functions remain intact
inhealthy older people yet a plethora of systemicdiseases,
medications and head and neckradiotherapy cause Xerostomia
particularly in elderlypatients2. With increase in longevity, we
have amuch larger population of older adults and thereforeit
becomes even more important to understandproblems associated with
dry mouth and theirtreatment to improve the patients
oropharyngealhealth and quality of life.
Common causes of XerostomiaXerostomia is a common complaint
associated withseveral conditions, which include side effects of
widevariety of medications3,4, therapeutic radiation tohead and
neck, systemic diseases and diseasesinvolving the salivary glands.
Common causes aresummarized the in the table below (Table 1)
Evidence suggests that salivary glands arevulnerable to
deleterious effects of all theseconditions in the elderly people
which contribute toincreased prevalence of salivary problems with
age.
Clinical Manifestations of Xerostomia
Saliva is essential for the preservation oforopharyngeal health,
and it serves many functionsin the oral and gastrointestinal
environment. Salivaaids in swallowing, oral cleansing,
speech,digestion and taste. When salivary hypofunctionand
xerostomia occur, transient and permanent oraland extraoral
disorders can develop2. Xerostomia isoften a contributing factor
for both minor andserious health problems. It can affect nutrition
aswell as psychological health. Individuals withXerostomia complain
of dry mouth and problemswith eating, speaking and swallowing.
There is oralburning or soreness and a sensation loss of oraltered
taste (Dysgeusia)5. Another manifestation isincreased need to drink
water while swallowing anddry crumbly foods are difficult to
swallow.
Dental Implications Patients with Xerostomia experience
various
oral symptoms that are as follows: Increased susceptibility to
periodontal disease:
Xerostomia decreases the oral pH andincreases the development of
plaque and dentalcaries. Caries is a frequently occurring
dentalproblem in such patients and this process isaccelerated owing
to reduction of salivary flowand inability to clear the food from
oral cavityparticularly sugary and acidic foods5. Thedevelopments
of rampant caries particularly atcervical area have been observed
have beenobserved within few weeks after radiationtherapy to head
neck10.
-
Review articles Annals and Essences of Dentistry
Vol. - II Issue 3 July Sept. 2010 138
Reduced denture retention and generalizeddenture intolerance.
Decreased salivary
lubrication makes denture use unpleasant andpainful and chronic
denture movement results in irritation and ulceration of already
compromised
mucosa9. Decreased buffering capacity in the oral cavity
with increased risk of opportunistic infections.Reduction of
saliva predisposes the patient toan over growth of the fungus C.
albicans11. Thismay be augmented by use of denture,bysmoking or by
presence of diabetes12. Increased oral sensitivity, soft tissue
erythema,
burning mouth and intolerance to wearing ofdenture.
Demineralization of tooth tissue, rapidly
progressive dental caries and dental attrition6.
DiagnosisDiagnosis can be obtained from patients history
andexamination of oral cavity and/or sialometry i.emeasuring the
flow rate of saliva13. Four clinicalmeasures, when concurrently
identified onexamination, have been shown to be reliablepredictors
of salivary gland hypofunction: dryness ofthe lips, dryness of the
buccal mucosa, absence ofsaliva production during gland palpation,
anddecayed/missing/filled teeth (i.e, DMFT) score.14
Sialography may be used to identify salivary glandstones and
masses. Salivary scintigraphy can beused in assessing salivary
gland function. Minorsalivary gland biopsy is used for diagnosis
ofSjgren's syndrome, HIV salivary gland disease,sarcoidosis and
amyloidosis. Biopsy of majorsalivary glands is an option when
malignancy issuspected.
Management of XerostomiaManagement should include identification
of theunderlying cause. Substances and habits thatpotentiate oral
dryness, such as smoking, alcohol,and caffeine should be
avoided.When xerogenic drugs are implicated, alternativemedication,
dose reduction, or drug withdrawalshould be considered. Another
option is to alternatepharmaceutical regimens: nocturnal xerostomia
canbe minimized by taking the xerogenic drug duringthe day time
when salivary production is optimal9.
Caries prevention: A low sugar diet and daily useof topical
fluoride, placement of sealants andantimicrobial mouth rinses are
critical to preventdental caries15. Patients should be instructed
to
drink plenty of fluids especially while eating dry andrough
foods, but should avoid sugar containing
juices and soft drinks. Topical fluorides may beuseful when
there is increased incidence of coronalcaries, root caries or
bothand may be helpful inprevention of caries as well as reversal
ofdecalcification. Supplements containing sodium
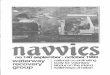
Table 1: Common causes of Xerostomia
Medications Antihistamines Antidepressants and
antipsychotics Antihypertensives Antianxiety agents Diuretics
Antiparkinsonism drugs Antiematics Bronchodilators Sedatives
Diseasesaffecting thesalivary glands
Sjgren's syndrome Sarcoidosis Amyloidosis
SystemicDiseases
Diabetes HIV infections Chronic graft-vs-host
disease after allogenicbone marrow transplant Emotional Stress
and
mental depression
RadiationTherapy (Causespermanentchanges)
Radiation therapy tohead and neck region forSquamous cell
cancersof oral cavity,oropharynx, nasopharynx and sinuses Brain
tumours Tumours of salivary
gland
Chemotherapy(causestemporarychanges)
-
Review articles Annals and Essences of Dentistry
Vol. - II Issue 3 July Sept. 2010 139
fluoride, acidulated phosphate fluoride or
sodiummonofluorophosphate are available for professionalapplication
and for home use. These products are
available in form of gels and rinses. Use of fluoridecontaining
varnishes that provide prolongedfluoride exposure have also been
advocated. Incase of active caries, caries should be controlledand
lesions should be properly restored.
Saliva stimulation and substitution: For patientswith remaining
viable salivary gland tissue, salivarystimulation may be helpful.
Sugar free chewinggum,candies and mints can be used for
stimulationof saliva. Pilocarpine hydrocholoride and
Cevimilinehydrochloride are commonly used drugs for
salivarystimulation and produce clinically significantincrease in
salivary flow in xerostomic patients16.These drugs are
contraindicated in patients withuncontrolled asthma, narrow angle
glaucoma oriritis. Varieties of salivary substitutes are
availableand are effective in decreasing oral dryness. Theyare
useful for patients in whom saliva can not bestimulated.
Treatment of oral candidiasis: Oral candidiasis isa frequent
complication in xerostomic patients andis treated with topical
antifungal agents in the formof oral rinses, ointments and troches.
Systemicantifungal therapy is indicated in cases of activeinfection
or in immunocompromised patients.
Prosthodontic Management of Xerostomiapatients
Fixed prosthothesis.In the dry oral environment,fixed non tissue
bearing prosthesis are preferredwhere indicated. Fixed partial
dentures shouldhave full coverage retainers and easily
cleanedpontics and connectors. The margins of retainersshould be
supragingival.
Removable partial denture In case of partiallyedentulous
patients using removable prosthesisspecial attention should be
given to residual teethand periodontal tissues. The use of
gingivallyapproaching clasps should be avoided as it tendsto catch
on the cheeks. Whenever possible toothsupported denture with
minimal tissue coverageshould be used. Metal denture bases
arepreferred due to their better wettability.
Complete denture treatment When consideringcomplete denture
treatment for xerostomic patient,close attention should be given to
clinical andlaboratory procedures aimed at optimizing
dentureretention and stability. Dentures incorporatingmetal bases
may exhibit improved accuracy of fitand effective wetting
contributing to betterretention17,18. Metal based prosthesis are
alsoeasier to clean and have less plaqueaccumulation. Soft denture
liners may be used toimprove comfort. Dentures adhesives can be
usedto augment retention in Xerostomic patients. Inaddition to
improved retention and stability, use ofa well hydrated denture
adhesive providescushioning and lubricating effect19.
Denturepatients are more prone to Candida albicansinfections.
Therefore frequent recalls arenecessary and if infection is present
systemic anti-fungal treatment is required. Dentures
supportingtissues can be treated locally with antifungalagents by
coating the tissue surface of the dentureprior to placement. The
use of dental implants tosupport both fixed and removable
prosthesis is anow a routine treatment option for restoration
ofedentulous and partially edentulous patients.Patients wearing
implant supported denturesreport improved oral comfort and function
whencompared with conventional, mucosa-supportedprosthesis6.
Regular review Patients with xerostomia should bemade to
understand the importance of regular recallvisits every three
months to prevent uncontrolledcaries and denture patients should be
reviewed atregular intervals to prevent candida infections
andproblems associated with denture wear inxerostomic patients.
CONCLUSIONXerostomia is a common problem encountered inolder
adults and if not recognized and treated canhave significant effect
on patients quality of life.Dental practitioner should be able to
diagnose drymouth disorder in their elderly patients and
providepreventive and definitive treatment to achieveacceptable
levels of comfort and function.
References1. Ship JA, Pillemer SR, Baum BJ. Xerostomia and
the
geriatric patient. J Am Geriatr Soc 2002;50(3):53543.
-
Review articles Annals and Essences of Dentistry
Vol. - II Issue 3 July Sept. 2010 140
2. Michael D. Turner and Jonathan A. Ship. Dry mouthand its
Effects on the oral health of elderly people.JADA 2007, Vol.
138:15-20.
3. Sreebny LM, Schwartz SS. A reference guide todrugs and dry
mouth. Gerodontology 1986;5:7599.
4. Byrne BE. Oral manifestations of systemic agents.In: ADA
guide to dental therapeutics. Chicago: ADAPublishing;
1998:46975.
5. James Guggenheimer and Paul A. Moore.Xerostomia Etiology,
recognition and treatment. JAM Dent Assoc 2003 Vol.
134,No.1,61-69.
6. Removable prosthodontic therapy and xerostomia.Treatment
considerations. Joseph J Massad, DavidR Cagna Dent Today June 2002
,vol. 21, Issue 6,80-7.
7. Chen MS, Daly TE. Xerostomia and completedenture retention.
Tex Dent J. 1979;97:6-9.
8. Fox PC, van der Ven PF, Sonies BC, et al.Xerostomia:
Evaluation of a symptom withincreasing significance. J Am Dent
Assoc.1985;110:519-525.
9. Katherine Chiu-Man Leung. Prosthodonticmanagement of patients
with xerostomia. HongKong Dent. J 2005;2:132-134.
10. International Dental Federation. Working Group 10of the
Commission on Oral Health, Research andEpidemiology (CORE). Saliva:
its role in health anddisease. Int Dent J 1992;42(4)supplement(2):
287304.
11. Samaranayake LP. Host factors and oralcandidosis. In:
Samaranayake LP, MacFarlane TW,eds. Oral candidosis. London:
Wright; 1990:66103.
12. Guggenheimer J, Moore PA, Rossie K, et al.Insulin-dependent
diabetes mellitus and oral softtissue pathologies, part II:
prevalence andcharacteristics of Candida and candidal lesions.Oral
Surg Oral Med Oral Pathol Oral Radiol Endod2000;89:5706.
13. Deborah Greenspan. Xerostomia: Diagnosis andmanagement.
Oncology 1996; 10(Suppl):7-11.
14. Navazesh M, Christensen C, Brightman V. Clinicalcriteria for
the diagnosis of salivary glandhypofunction. J Dent Res.
1992;71:1363-1369.
15. Ship JA. Diagnosing, managing, and preventingsalivary gland
disorders. Oral Dis 2002;8(2):7789.
16. Niedermeier W, Matthaeus C, Meyer C, Staar S,Muller RP,
Schulze HJ. Radiation-inducedhyposalivation and its treatment with
oralpilocarpine. Oral Surg Oral Med Oral Pathol OralRadiol Endod
1998;86:541-9.
17. Lloyd PM. Complete-denture therapy for thegeriatric patient.
Dent Clin North Am. 1996;40:239-254.
18. Hummel SK, Marker VA, Buschang P, et al. A pilotstudy to
evaluate different palate materials formaxillary complete dentures
with xerostomicpatients. J Prosthodont. 1999;8:10-17.
19. Grasso JE, Rendell J, Gay T. Effect of dentureadhesive on
the retention and stability of maxillarydentures. J Prosthet Dent.
1994;72:399-405.
Corresponding AuthorDr. Ramandeep Dugal MDS
ProfessorDepartment of Prosthodontics
MA Rangoonwala Dental College,Pune
Phone: 02032914104Email: [email protected]