Embed Size (px)
Citation preview

DOI: 10.1161/CIRCGENETICS.114.000819
1
22q11.2 Deletion Status and Disease Burden in Children and
Adolescents with Tetralogy of Fallot
Running title: Mercer-Rosa et al.; 22q11 deletion and outcome in tetralogy of Fallot
Laura Mercer-Rosa, MD1; Stephen M. Paridon, MD1; Mark A. Fogel, MD1; Jack Rychik, MD1;
Ronn E. Tanel, MD2; Huaqing Zhao, PhD3; Xuemei Zhang, MS4; Wei Yang, PhD5;
Justine Shults, PhD4; Elizabeth Goldmuntz, MD1
1Division of Cardiology, Department of Pediatrics, The Children's Hospital of Philadelphia & University of Pennsylvania Perelman School of Medicine, Philadelphia, PA;2Division of Pediatric Cardiology,
Department of Pediatrics, UCSF Benioff Children’s Hospital, UCSF School of Medicine, San Francisco, CA;3Temple Clinical Research Center, Temple University School of Medicine;4Department of
Biostatistics & Epidemiology, 5Center for Clinical Epidemiology & Biostatistics, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA
Correspondence:
Elizabeth Goldmuntz, MD
The Children's Hospital of Philadelphia
Abramson Research Center 702A
3615 Civic Center Boulevard
Philadelphia, PA 19104-4318
Tel: 215-590-5820
Fax: 267-426-9800
E-mail: [email protected]
Journal Subject Codes: [30] CT and MRI, [31] Echocardiography, [41] Pediatric and congenital heart disease, including cardiovascular surgery, [109] Clinical genetics, [125] Exercise testing
; g, ;
MD1111
f vy ot n
oi o
f CaCaCaardiology, DeDeDepappartttrtmemementtntnt ooof ff PePePePedidd atatatriics, TThe Childrdrdrenenn's's's HHHososo piipitatatal l l ooof PPPhhhhililili adadaddelelelelphphphphiaiaiaia & &&& UUUnU ivyllllvaaaania Perelmanann Schchhool ofofof Medicinne, PPPhhiladedelphihiia,a,a,a, PPPPAA;2DiDiivisiionnn ooof Pediaataatrrir ccc CCCardddiolot offf f PePePeP diatriiiricscscsc , UCUCCSFF BBBBenioioioi ffffff CCCChihh lddddrereen’nn ss s HHoH spspspitaaala , UCUCUCCSFSFSF SSSchchchhooooooo l offf MMMMedee icciccinininine,,,, SSSan Frranemple CCCllil nical ReReReReses arch CeCeCenter, Temple Unininiversity SSSchchc ool l of y Meeediddd cine;4444Department oics & Epidemiolololologygygyg ,, 5CeCeCentntntntererr fffforororo CCCClilililinininicacacacall ll EpEpEpidididememememioioioloooogyggygy & & & & BiBiBiiososoostatatatititistststiiicscscscs, ,,, Perelman Scho
Mediciine at thhe Uniiversiityyy of f Pennsyyylvania,,, Phhiladellphhp ia, ,, PA
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
2
Abstract
Background - Patients with repaired tetralogy of Fallot (TOF) experience variable outcomes for
reasons that are incompletely understood. We hypothesize that genetic variants contribute to this
variability. We sought to investigate the association of 22q11.2 deletion status with clinical
outcome in patients with repaired TOF.
Methods and Results - We performed a cross sectional study of TOF subjects who were tested
for 22q11.2 deletion, and underwent cardiac magnetic resonance (CMR), exercise stress test
(EST) and review of medical history..
We studied 165 subjects (12.3 3.1 years), of which 30 (18%) had 22q11.2 deletion syndrome
(22q11.2DS). Overall, by CMR the right ventricular (RV) ejection fraction was 60 8%,
pulmonary regurgitant fraction 34 17%, and RV end-diastolic volume 114 39 cc/m2. On EST,
maximum oxygen consumption (mVO2) was 76 16% predicted. Despite comparable RV
function and pulmonary regurgitant fraction, on EST the 22q11.2DS had significantly lower
percent predicted: forced vital capacity (61.5 16 vs. 80.5 14, p< 0.0001); mVO2 (61 17 vs.
80 12, p<0.0001); and work (64 18 vs. 86 22, p=0.0002). Similarly, the 22q11.2DS
experienced more hospitalizations (6.5 [5; 10] vs. 3 [2; 5], p<0.0001), saw more specialists (3.5
[2; 9] vs. 0 [0; 12], p<0.0001) and used one or more medications (67 vs. 34%, p <0.001).
Conclusions - 22q11.2DS is associated with restrictive lung disease, worse aerobic capacity, and
increased morbidity, and may explain some of the clinical variability seen in TOF. These
findings may provide avenues for intervention to improve outcomes, and should be re-evaluated
longitudinally as these associations may become more pronounced with time.
Key words: echocardiography, exercise test, genetics, magnetic resonance imaging, tetralogy of Fallot
q y
cctitititiononon wwwwasasasas 66660000 8%8%8%8%,
e 114 39393939 ccccc/c/c/c/mmmm222. OnOnOnOn E
o
n e
d 7
0
d s
[0 12] <0 0001) d d di ti (67 34% <0 001)
oxxygygygygeen cononnnsssumpmm tion (mVO2) was 76 16166%% predicted. DeD spsppiiiti e comparable RV
ndddd pppuulmonary reregurgrggiiti annnnttt ffraccctitionnn,,, onnn EESTT tthee 222q2q2q2q111.22DDS hhaaad sisiignifffficiccannntllly lllowwwe
dicccteteteted:d:d:: fffforororceccc d d d vvvvitiii alalal cacacapaaaacicicc tytytyy ((((616 .5.5.5.5 16 6 6 vsvsvsvs. 808000.5555 1114,4,4,4 ppp<<<< 00.0 00000000010111);););); mmmmVOVOVOVO2 (6(6(61111 17
0.0001); and worororork k k (6(6(6(6444 1818181 vvvvs.ss.s. 8886666 22222222,,,, p=p=p=0.00 00000000202020 ).... SiSiSiimimmim lalalaarlrlrlrly,yy ttthehehe 22222q222 11.2DS
d d d more hhhosssspipipip tatatalililizaatititionoo ss (6(6(6( .5.5.55 [[[[5;5;5; 11110]0]0] vvvs.s. 3333 [[[2;2;2;; 555],],], pppp<0<0<0.0.0.0.000000001)1)1), ,, sasasaw w momooreee sspepp iici llaliiiststts
[0 12] 0 0001) d d di ti (67 34% 0 001) by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
3
Introduction
Despite notable surgical success, many patients with tetralogy of Fallot (TOF) experience
significant morbidity and early mortality. Post-surgical pulmonary insufficiency (PI) with
consequential right ventricular (RV) remodeling and dysfunction is thought to contribute
significantly to long-term outcomes such as decreased exercise performance, increased incidence
of arrhythmias and risk of sudden death.1-3 Outcomes in adults have been extensively described,
though little is known about the intermediate cardiovascular status preceding symptoms and the
apparent need for pulmonary valve replacement.1, 2, 4-7 Moreover, clinical variability is not
explained on the basis of PI alone.
TOF is a disease of considerable genetic heterogeneity. The 22q11.2 deletion syndrome
(22q11.2DS) and trisomy 21 account for approximately 15% and 7% of all TOF cases
respectively. TOF is also a characteristic finding in many syndromes (e.g. Alagille, CHARGE
and VATER syndromes), and is associated with a growing list of copy number variants (e.g.
1p21.1) and single gene disorders (e.g. NKX2.5, FOG2/ZFPM2).8-12. As noted, 22q11.2DS is
the most common finding, present in 15 to 20% of TOF with pulmonary stenosis and nearly 50%
of those with pulmonary atresia and major aorto-pulmonary collaterals.13-16 22q11.2DS is a
multi-system disorder characterized by congenital heart disease, palate anomalies, hypocalcemia,
immunodeficiency, speech and learning disabilities, behavioral and psychiatric disorders, and
characteristic facial features17. We postulate that genotype could explain at least in part the
clinical variability seen in TOF. We therefore hypothesized that 22q11.2DS is independently
associated with clinical outcomes in TOF and sought to investigate the contribution of
22q11.2DS to RV function, exercise performance and disease burden in school age and
adolescent children with repaired TOF.
cal variability is nonononotttt
F r
S
y G
R g
d single gene disorders (e g NKX2 5 FOG2/ZFPM2) 8 12 As noted 22q11 2DS
F issss aaa ddddisisisseaeaeassse ooof fff considerable genetic heteteteeerogeneity. The 2222q222 11.2 deletion syndr
S))) aaana d trisomyy 2221 acacccounununu t foooorrr appppproxxximmatteely 151515%% % aanddd 7% of alalalllll TOOOOF F F Fd caaases
y. TOOOOFFFF isisisis alsoo aa chchhhararaca teririristtststiiicic findididingngngng iinin mmannanyyy ssssynynyndrddrdrommmmeses yyy ((e(e.g.g.g. AlAlAlAlagagagillee, CHCHCHCHARARARG
R syyyndromes)),,, and ddd iiisi associiiiat deddd wiiti h hhh a grgg owiniii g gg liliiist of ff copypypy numbbebb r variants ((e.g
ddd isi lle didi drd (( NKNKX2X2 55 FOFOG2G2/Z/ZFPFPM2M2)) 8-8-1212 AAs ot ded 2222 1q111 2D2DS by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
4
Methods
Study population and data collection
We performed a cross sectional study of subjects operated for TOF who underwent genetic
testing, cardiac magnetic resonance (CMR) and cardiopulmonary exercise testing (EST) within
at most three months of one another at The Children's Hospital of Philadelphia as part of a study
protocol. Subjects were identified from existing studies and clinical databases at our institution.
Inclusion required the confirmed diagnosis of TOF by review of medical records, a history of
complete surgical TOF repair, and age 8 to 18 years upon study enrollment.18 TOF was defined
as the presence of anterior malalignment of the conal septum, override of the aorta and mitral to
aortic valve fibrous continuity. Pre-operative echocardiographic reports, cardiac catheterization
studies and operative notes were reviewed to confirm the diagnosis. Genetic testing was
performed using fluorescence in situ hybridization (FISH), multiplex ligation-dependent probe
amplification (MLPA), or both to classify subjects as del22q11.2 positive (22q11.2DS) or
del22q11.2 negative (non-deleted or ND).(17, 18) Both tests were performed in 47% of the
subjects, MLPA only in 28% (most of the ND had MLPA testing), and FISH only in 26%.19, 20
Cases with other recognized genetic syndromes were excluded, including those with Noonan
syndrome, CHARGE association, VACTERL, Williams syndrome, and Goldenhar syndrome.
Cases who were unrepaired, had only palliative procedures, or underwent a heart transplant were
likewise excluded. Patients with trisomy 21 and Alagille syndrome were enrolled in the study but
excluded from this analysis due to small numbers that would not allow for meaningful
comparisons. Detailed review of medical history was undertaken to assess resource utilization
and disease burden reflected by the number of significant medical encounters. Detailed review of
medical records and interviews with families provided data on cardiac and non-cardiac medical
ment.18 TOF was dedededef
e of ththhthe ao tttrta and d mimimimitr
e a
u r
o
negati e (non deleted or ND) (17 18) Both tests ere performed in 47% of the
e fibrbrbrbrououousss cococonnntinininnuiuuu ty. Pre-operative echocacacardrdiographic reportrtrttss,s cardiac catheteriza
oopoperee ative noteesss weerrre reveveve iewewwed totto conoonfirmm theee dddiaiaiaggnooosiis. GeGGeG neeetiiiic testststs iniii ggg wass
using gg flflflfluououou rescscenencece iiinn situ hhhhybybybybrididididizazazatitititiooon (F(F(FISISISSH)H)H), mumumulllltipipiplelelelex liililigggatiiiionononon-ddddeppenendddedentntt ppr
on (M( LPA)),,, or bbbbothhh h to clall ssifffy yy subjbjbjects as ddded l2ll 2q2q1111111 22.22 pppositiiivi e (2(2(2(22q2q22 11.2DS)) or
atii ((n dd lelet ded NDND)) (1(177 118)8) BBothh test ffo ded ii 4747%% fof thhe by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
5
and surgical history, sub-specialty visits, and prescribed medications at the time of enrollment.
Surgical repair for TOF was defined as: 1. Complete (relief of outflow tract obstruction
and closure of the ventricular septal defect in the same operative procedure), 2.Complete after
palliation (complete repair preceded by palliation with a Blalock Taussig shunt), or 3. Staged
(separate operations performed to achieve complete repair). Primary surgery was defined as the
initial operation(s) performed to achieve relief of outflow tract obstruction and closure of the
ventricular septal defect. Procedures performed thereafter were classified as subsequent
operations.
Cardiac Magnetic Resonance
CMR studies were performed on a 1.5-T Avanto Whole Body Magnetic Resonance System
(Siemens Medical Solutions, Erlanghen, Germany) using a standard imaging protocol, described
previously.21
Exercise Stress Test
Subjects exercised to maximal ability using a ramp cycle protocol on an electronically braked
cycle ergometer (SensorMedics, Yorba Linda, CA), as described previously.22 Eighteen subjects
who were < 130 cm tall exercised on a treadmill (Marquette Series 2000, Milwaukee, WI).
Resting spirometry included forced vital capacity, which was considered normal if >80% of
predicted. Breathing reserve was obtained as a measure of pulmonary function at peak exercise
(normal >15%). 23 At peak exercise, data included oxygen consumption (VO2), maximum
physical working capacity, oxygen pulse (a surrogate of ventricular stroke volume), and the
maximal respiratory exchange ratio (RER) to identify subjects who achieved maximum effort.
The percent predicted of maximum VO2 (mVO2), the VO2 at the anaerobic threshold and
maximum work were calculated for each patient according to normative values and considered
e m
M c
2
t
ercised to ma imal abilit sing a ramp c cle protocol on an electronicall brak
es wewewereere ppperererfofff rmrmrmed on a 1.5-T Avanto WWWhohohh le Body Magneteticiii Resonance System
Medededical Solutioonnns, ErErErrlangngngn hheh n,nn Gereermaaany) ususing g a a a a sstss aandaddard imamm ggig nnng prororor tooocoool, dededed sc
21
tress Test
ici dd to iim lal bibililit isi lcl ot lol llect ini llll bbr kak by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
6
normal if > 80% of predicted.24 25 Exercise performance (aerobic capacity) was defined by
percent predicted mVO2 and VO2 at the anaerobic threshold. An EST was considered maximal
. The anaerobic threshold was used as an effort-independent surrogate of the
ability of the cardiovascular system to support the metabolic demands during exercise.26
Impaired chronotropic response was defined as peak heart rate less than 180 bpm.
Electrocardiogram (ECG)
ECG was performed on MAC 5000’s machine (General Electric, USA) using a standard clinical
protocol, and interpreted by a single experienced reader (RT).
Statistical Analysis
Continuous variables are presented as mean and standard deviation or as median with the first
and third quartile range. Categorical variables are described using count and percentage. The
differences between 22q11.2DS and ND groups were tested with the Wilcoxon Rank Sum test
for continuous variables and the Chi-square test or Fisher's exact test for categorical variables.
Covariates were compared with Pearson’s correlation coefficient. Poisson regression adjusting
for age and years of follow-up with the Generalized Estimating Equations method for repeated
measurements was used to assess the independent associations between deletion status and
number of hospitalizations, procedures, medications and operations. Subgroup analyses were
performed for subjects with maximal EST. Statistical significance was reached for p-values <
0.05 (2-sided tests). All analyses were performed using SAS statistical software version 9.2
(Cary, NC, USA).
Results
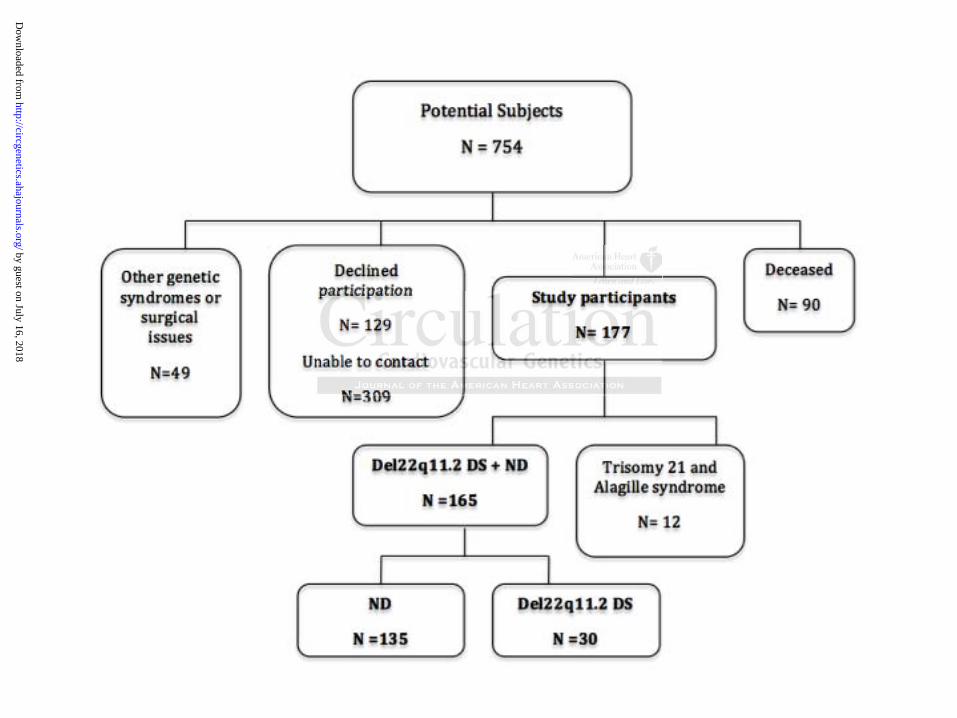
There were 754 age-appropriate potential subjects identified in our clinical and research
databases. Forty-nine subjects were excluded given the presence of other genetic syndromes
s variables are presented as mean and standard deviation or as median with the fi
u h
between 22q11.2DS and ND groups were tested with the Wilcoxon Rank Sum t
o l
ere compared ith Pearson’s correlation coefficient Poisson regression adj st
s vararariaiaiai blblblbleseses aaare pppresented as mean and staaandndnn ard deviation orr aaas median with the fi
uaara tttile range. CCCaaateggoooricalalala varrriaiaiabblees aarree deesccribbbededed usingnng couunnnt aaannndn peeere cccentntntageee. Th
betwwweeeeeeeennn n 2222q1q11111.2D2D2DSSSS and dd NDNDNDND groooupupups sss wewerere ttttesesteteteedddd wiiwiwithhh ttthehehehe WWWWiliii coxoxxoxonnn Raa kknknk SSSSumum
ous variables andddd thhheh CCCChihihi-sqqquare test or FFFisi hhheh r's exact test ffffor categggorical variabl
ded iithh PPe ’n’ lelatiio feffifi ici t PP ioi iio dadjj st by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
7
(Noonan syndrome, CHARGE association, VATER and VACTERL, Williams syndrome,
Goldenhar syndrome) or surgical issues that included unrepaired TOF, palliation only, single
ventricle-type operations, or heart transplant. Fifty-three percent of the potential 754 subjects
could not be contacted or were deceased (n=90).. Therefore, of the 309 potential subjects that
met inclusion criteria, 57% consented to the study (n=177). After exclusion of subjects with
trisomy 21 or Alagille syndrome, this analysis included 165 subjects, of which 30 had
22q11.2DS (18%) (Figure 1). In those subjects where both FISH and MLPA was performed to
identify a 22q11.2 deletion, there was 100% agreement between the two techniques. Age at
cardiac testing was 12.3 ± 3.1 years, with a predominance of males and whites. The groups were
comparable in terms of demographic, anatomic and surgical characteristics, as detailed in Table
1.
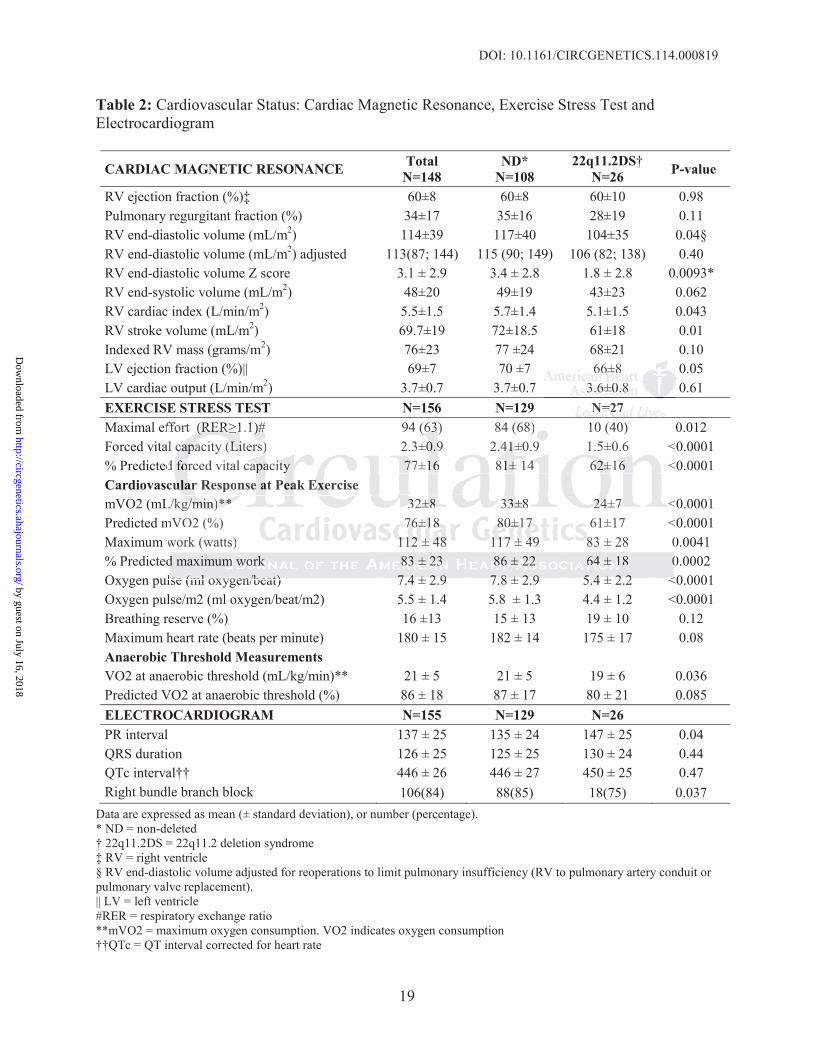
Cardiovascular Status
We examined the cardiovascular status of the study population by CMR, EST and ECG. The full
study cohort demonstrated normal ventricular function on CMR, with considerable pulmonary
insufficiency (PI) [pulmonary regurgitant fraction = 37% (26; 45)] and dilated RVs (Table 2).
On EST, most subjects achieved a maximal EST. Resting forced vital capacity was
diminished in 59% of subjects, suggesting restrictive lung disease. At peak exercise, mVO2 was
decreased, physical working capacity was low normal and breathing reserve was preserved
(Table 2). There was no association between aerobic capacity and measures of resting RV
ejection fraction (p=0.97) and PI (p = 0.49) by CMR. Impaired chronotropic response was
present in 42% of subjects. There was no association between peak heart rate and mVO2
(p=0.10) for subjects achieving a maximal test.
On ECG, most subjects had right bundle branch block. (Table 2) QRS duration and
wo techniquq es. AgAgAgge e e e a
d whhhhitititites. ThThThThe grgg ouououupppps
e T
c
ned the cardiovascular status of the study population by CMR, EST and ECG. Th
rt demonstrated normal entric lar f nction on CMR ith considerable p lmon
e in n n tetetermmrmss ofofofof dededeemmmographic, anatomic and ddd susurgical characterrisisisistics, as detailed in T
cularr SSSStatatatatttus
ned the cardiovasc llullar status of thhheh studydydd pppopppulatioiii n bybbyb CCCCMRMRMR, ,, ESESESEST and ECG. Th
rt dd st tedd lal triic ll ff ctiio CCMRMR ii hth isidde blbl llm by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
8
RVEDV were modestly associated (R=0.39, p<0.0001).
22q11.2 Deletion Status and Clinical Outcome
Cardiovascular Status
The 22q11.2DS and ND groups had comparable RV function and RV hypertrophy, measured as
RVEF and RV mass/m2 on CMR, respectively. The RV end-diastolic volume was comparable
when the analysis was adjusted for reoperations that would diminish PI (RV-pulmonary artery
conduit and pulmonary valve replacements) (Table 2).
On EST, however, the 22q11.2DS group performed worse as compared to the ND. On
resting spirometry, the forced vital capacity was significantly lower in the 22q11.2DS,
suggesting worse restrictive lung disease in the 22q11.2DS group. This association was not
affected by the presence of scoliosis, which was more prevalent in the 22q11.2DS group, present
in 8 subjects (27%) as compared to 10 in the ND group (7%) (p = 0.002). However, scoliosis was
neither an independent predictor of forced vital capacity nor was it a confounder of the
association between deletion status and forced vital capacity (data not shown). Although percent
predicted VO2 was similar at anaerobic threshold, at peak exercise, the 22q11.2DS subjects had
significantly impaired aerobic capacity with diminished mVO2, accomplished less work and had
lower oxygen pulse, in keeping with lower measured indexed stroke volume on CMR (Table 2).
22q11.2DS was independently negatively associated with physical working capacity and oxygen
pulse (p-values of 0.005 and <0.0001, respectively). A sub-analysis limited to the subjects that
achieved a maximal EST (RER 1.1) demonstrated similar results.
Intermediate Medical and Surgical History
The 22q11.2DS group reported more overall hospitalizations and significantly greater
medication use. Specifically, the 22q11.2DS group had significantly more cardiac
ompared to the ND.D.DD O
the 22222q2q2q2 11111111.2222DSDSDSDS,
t
the presence of scoliosis, which was more prevalent in the 2 11.2DS group, p
ts (27%) as compared to 10 in the ND group (7%) (p = 0.002). However, scolios
n
bet een deletion stat s and forced ital capacit (data not sho n) Altho gh pe
wooorsrsrsrseee rererestststriririricttivivivve lung disease in the 22q1q1q11.11 2DS group.p Thihihisss association was not
ttheeee presence oofff scollllio isisiiss,s whihihih chhh wwasss mmorree prrevevvvalalaleent inn thee 2222q2qq11111 .2222DDDSD grrrouupp,, p
ts (22227%7%7%7%) ))) aas comompapapareredddd to 111000 iiinin thehee NNNNDD DD grrrououpp (7(7(7%)%%)%) ((((p === 0000.0000002)2)2)2). HoHoHoHowwweveerr, sscocolililioso
ndepepp ndent prpp eddddiici tor offf ffforcedd d iivital capapp ciiitytyty nor was iiit a confffounder of the
bbet ddelle iti tat dd ffo ded iit lal iit (d(dat t hsh )n) AlAl hth hgh by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
9
hospitalizations and used one or more cardiac medications. Similarly, the 22q11.2DS group
reported significantly more non-cardiac hospitalizations as compared to the ND and significantly
greater non-cardiac medication use (Table 3). Cardiac medications used included aldactone (n=
1 22q11.2DS), aspirin (n=6 ND, n= 3 22q11.2DS), atenolol (n=1 ND), chlorothiazide (n= 1 ND),
digoxin (n= 9 ND, n= 4 22q11.2DS), enalapril (n= 2 ND, n= 1 22q11.2DS), lasix (3 in each
group), and mexiletine (n= 1 ND). One subject with 22q11.2DS used 5 medications, including
aldactone, aspirin, digoxin, enalapril and lasix.
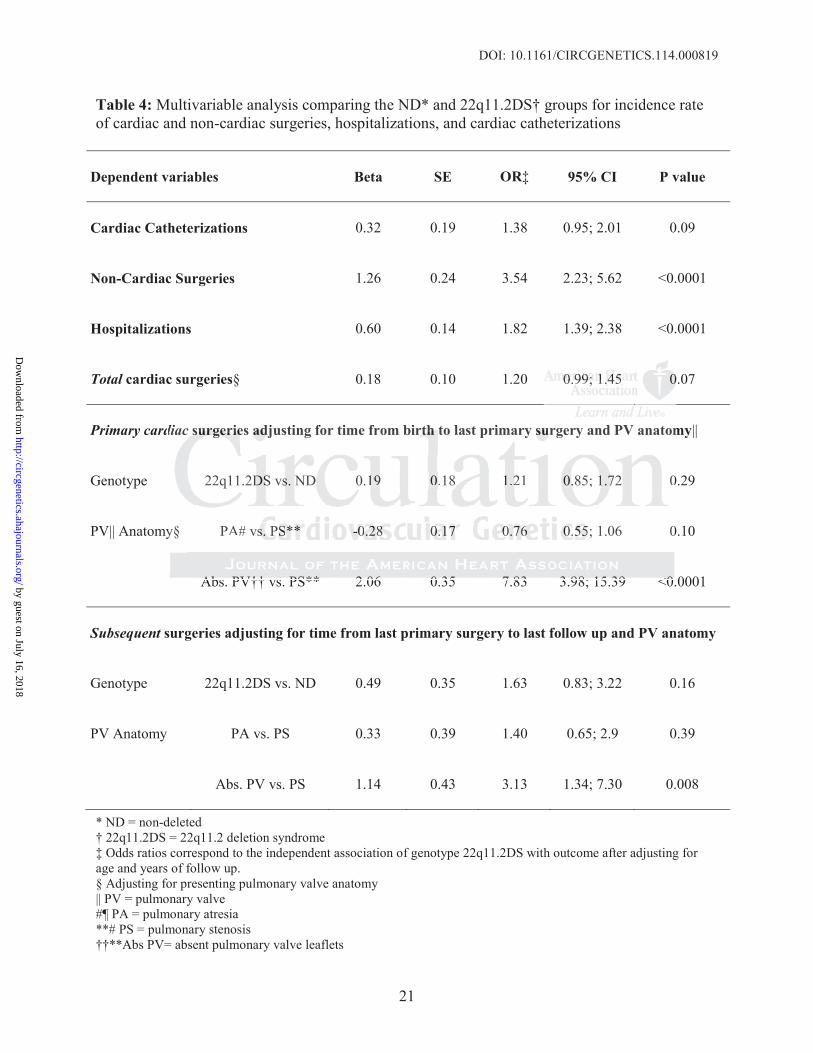
On multivariable analysis, there was a difference in the incidence of cardiac surgeries
(primary and/or subsequent); however this difference did not reach statistical significance
(P=0.007), There was no significant difference in cardiac catheterizations according to 22q11.2
deletion status. However, absent pulmonary valve leaflets was an independent predictor of
primary and subsequent cardiac surgeries when compared to pulmonary valve stenosis (Table 4).
Finally, the 22q11.2 DS group saw significantly more specialists as compared to the ND [3.5 (2;
9) vs. (0; 1), p<0.0001, respectively) (Table 4).
Discussion
In this study, we found that children and adolescents with repaired TOF demonstrate relatively
preserved ventricular performance despite significant PI, and yet demonstrate diminished
exercise performance. Further, we found that the 22q11.2DS subset display worse exercise
performance and markedly increased resource utilization as compared to their ND counterparts.
Given that in general exercise performance peaks in adolescence and decreases with age, our
cohort and the 22q11.2DS subset in particular would appear to be at a distinct disadvantage
starting adolescence with decreased exercise performance.27
Previous studies report conflicting results with respect to exercise performance in the
nce of cardiac surgrgggererereri
atisticallll iiisignifififificiii annncececece
q
a
d b
e 3
) p<0 0001 respecti el ) (Table 4)
Thererere e wawawas s nnno sssigiii nificant difference in cccararardid ac catheterizatititiooons according to 22q
atuuus. However,, aaabseennnt pulululu monann ryyy valvvee leeafflettss wwaww ss annn indepeppennnddded nt pppprrredddiccctorrr oof
d subsbsbbseqeqeqequuuenttt ccarardididiacac ssurgegegeriririries whehhehen cccompmpmpararededed tttto ppupulmmmonoononaaryryry valalllvevveve stenono isisiss (T(T(Taba
e 22qq11.2 DS grgg oup pp saw signgg ififificantly yy more spepp ciallliisi ts as compppared to the ND [[3
) 0<0 00000011 ctii lel )) (T(T bablle 44)) by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
10
operated TOF population, some observing decreased mVO2 and others reporting normal exercise
performance.28-30 The precise mechanisms leading to decreased exercise performance in TOF
have not been fully elucidated. Proposed etiologies include chronotropic impairment,
cardiovascular limitations, restrictive pulmonary function and more recently, deficient habitual
exercise22, 31-34. In our cohort maximal heart rate was not associated with mVO2, measures of
cardiac performance on CMR were relatively well preserved, and the high RER achieved by the
majority of subjects (62%) suggests that in many cases the cardiovascular function did not limit
exercise performance despite abnormal resting pulmonary function. Thus, the mechanisms
underlying poor exercise performance in this cohort are likewise poorly defined and likely
represent a combination of factors, including perhaps genotype and/or a lack of habitual physical
exercise. Our group recently demonstrated that habitual exercise correlates with mVO2 better
than CMR measures of function, such that subjects in this age group and range of ventricular
function that exercise regularly perform better on EST.22 This is not surprising given that both
cardiopulmonary as well as peripheral muscular conditioning contribute significantly to the
overall variance in aerobic capacity for any population.29, 30, 35
Our study further demonstrates that 22q11.2 deletion status is associated with outcome as
measured by exercise performance, non-cardiac interventions and resource utilization. Subjects
with 22q11.2DS performed significantly worse on exercise testing, a finding that persisted in a
subset analysis of those achieving a maximal effort. Several factors including decreased effort or
executive function may explain why fewer 22q11.2DS subjects completed a maximal exercise
study as compared to their ND counterparts.36, 37 Given that resting lung mechanics are highly
effort dependent, limited ability to properly perform the maneuver may underestimate pulmonary
capacity in the 22q11.2DS. However, given that the 22q11.2DS subset achieving a maximal
hus, the mechanismsmsmm
ly defifififinedddd andddd llllikkkkeeeeddd lylylyly
h
ur group recently demonstrated that habitual exercise correlates with mVO2 bet
m l
a
monar as ell as peripheral m sc lar conditioning contrib te significantl to the
combmbmbm ininininatatatioioioon ofofofof factors, including perhapapaps genotype and/ooor r a aa lack of habitual ph
uuuru ggggroup recenntlly dededeemoooonsnnn tratatateede thhat hhaabitutual eexexeeercrcrr iseee ccorreelelateseses witttth hhh mVmVmVVO2O2O2O2 bbbbet
measususurerereresss of fffunun tctctioioi n,n suchhh ththththat suuuubjbjbjbjececece tsts ininii tttthihihisss agaagageee grouououup p anand ddd rangngnngeee offf venentrtrt iiciculu
at exercise regggullllarlyllyl ppperffform bbbetter on EEESTSTSTS .22222 Thihihih s isiii not surprpp iiisiinii g gg gig ven that b
llll iri hph lal lla dndiitiio ini tribib t isi ififiic ltl to thhe by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
11
performance demonstrated diminished exercise capacity by a number of EST measures, the
presence of a 22q11.2 deletion likely confers as of yet unexplained deficiencies that could
become more apparent with time. These findings could also reflect decreased participation of
22q11.2DS subjects in habitual exercise.22
Measures of RV volume were slightly lower in the 22q11.2DS subgroup as compared to
the ND. This finding could either represent less RV dilation for a given amount of PI in the
22q11.2DS subgroup or reflect more interventions aimed at limiting the degree of PI resulting in
less RV dilation. The difference in RV volume disappeared after controlling for re-interventions
addressing the right ventricular outflow tract (i.e.: conduit and valve replacements), and yet we
did not find a statistically different rate of subsequent intervention in the 22q11.2DS cohort in
this age group. Our inability to detect a difference between cardiac surgical rates of re-
intervention may be due to the age of study subjects and the relatively small number of
subsequent surgeries to date, leaving open the possibility that such differences exist and become
more apparent with age.
It is evident that subjects with a 22q11.2 DS experience a heavier disease burden than the
ND. As noted, there was no statistically significant difference in the number of cardiac
procedures, though some data, including the number of cardiac-related hospitalizations, the
smaller RV volumes on CMR, and the number of prescribed cardiac medications, suggest
otherwise. In all likelihood this study was underpowered to detect a difference in this younger
cohort and could have been affected by selection bias; therefore larger and/or longitudinal
studies might reveal otherwise. A study by Kyburz in 2008 examining long-term outcomes in
patients with 22q11.2DS and various heart defects found a significant number of cardiac re-
interventions in subjects with 22q11.2DS.17
rollingg for re-interrrrvevevv n
eplacementsttt ),))) and ddd yyyyet
d t
o
n
rent ith age
d a ssstatatatititiisttststiciciccalaaa lyyy ddddifferent rate of subsequeeentntnt intervention in ttthehhh 22q11.2DS cohort
ouupu ... . Our inabilllittty to deteteeecctc a dddiffefferennncee beettweeeen n n n cacacc rdiaiiac suurgggicccalalalal ratesesese off rrre-
n mayayy bbbbeee e ddduee ttoto tttheheh aagegege offf ststststudy sususubjbjbjbjeectststt aa dndnd ttthehehehe rrrellelelatttivviviv llelely smsmallllllll nununumbbberer oof fff
surgegg ries to date, ,, lllel aviiini g gg opppen thheh pppos iisiibibibililililitytyty that suchhh ddddifififfefff rences exist and be
t ii hth by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
12
Our study found a remarkable difference in non-cardiac health-related issues in the subset
of TOF subjects with 22q11.2DS as compared to the ND, represented by significantly more
hospital admissions, non-cardiac surgical interventions, subspecialty care and prescribed
medications. Such findings could significantly impact upon quality of life for the 22q11.2DS
subgroup. Though not well defined in the literature, one study similarly reported that subjects
with 22q11.2DS had six non-psychiatric admissions in a lifetime, mostly in childhood and
adolescence, in keeping with our findings.38 Of note, while the 22q11.2DS cohort reported a
wide and predictable range of medical issues, including speech and educational problems, they
did not report more frequent psychiatric diagnoses or neuropsychiatric medication use as
compared to the ND subgroup at this age. These findings suggest that either psychiatric
disorders present in older 22q11.2DS subjects, or quite possibly, that psychiatric conditions were
under-diagnosed in this age group.39, 40
There are several acknowledged limitations to this study. The cross sectional design
identifies associations without necessarily identifying causation. We acknowledge potential
recall bias when interviewing parents for medical history. In addition, our study incurred the risk
of selection bias by subjects not enrolled (death, contact issues) and because we were limited by
those willing to participate in a full day of testing. However all subjects were equally invited to
participate in the study. As such, our results may not be generalizable to all subjects operated for
TOF. However, this study represents one of very few performed in this age group. Future
longitudinal studies in this population will allow us to identify pre-symptomatic changes that
predict outcomes and allow for better informed pre-emptive interventions. In addition, this study
included research driven assessments (CMR and EST) scheduled in close proximity to one
another, which were performed and interpreted by research technicians and single physicians
ucational prp oblemsmsmsms,,,, t
c meddddiciii attttiiioi n use asasasas
o
r s
n
e
ssociations itho t necessaril identif ing ca sation We ackno ledge potentia
o thhhheee NDNDNDND sssubuuu grgrgrouo p at this age. These fiiiindndnn ings suggest thaaat t either psychiatric
reese eeene t in olderr 2222qq11111.22DSDSDSD suuubbjb eeectts, oroor quuitte pposossssisisibblb y,,, ttthat psyyychchchhiatrricicicic conononditttit oons
noseddd inininin ttthhhis agagee grgrououp.39393939,,,, 40000
ere are several ackknkk owlell dgddgedddd lllimiiti atioiii ns to hhthhisii studyddy. ThThThThe cross sectional desiggg
iia iti ii hth t ilil idid itiff iin atiio WWe kck ll ded ot itia by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
13
respectively to minimize variability in data acquisition and provide temporally related
hemodynamic data.
In conclusion, this study provides unique insight into the clinical status of TOF cases at
an interim age between infancy and adulthood, and the contribution of 22q11.2 deletion status to
clinical outcomes. Although 22q11.2 DS and ND cases demonstrate similar cardiac function as
measured by cardiac MRI, those with a 22q11.2 deletion demonstrate even worse exercise
performance and increased morbidity relative to their ND counterparts. Whether subtle
cardiovascular differences and the consequences of poor exercise performance become more
pronounced over time remain to be explored in a longitudinal study. Regardless future studies
should incorporate genotype, and in particular 22q11.2 deletion status, into their analyses of TOF
outcomes. Our study also serves to highlight the multisystem nature of 22q11.2DS and brings
attention to non-cardiac factors that contribute to the variability seen in TOF outcomes. As such,
this study serves as a paradigm for the relationship to be explored between specific genotypes
and clinical outcomes in the congenital heart disease population. Moreover, our results also
provide avenues for early intervention and contribute to our ability to counsel subjects and
families about potential outcomes. Early diagnosis might lead to better management in the
newborn period regarding hypocalcemia, immunodeficiency and feeding difficulties; it also may
allow for identifying exercises that are skill appropriate and that will ultimately lead to improved
exercise capacity and quality of life. In addition, early diagnosis and understanding of the causes
for additional hospital admissions may allow for identification of elements of the non-cardiac
care that can impact overall status. Finally, early diagnosis allows for anticipation of problems,
thus avoiding the so-called “medical odyssey”, decreasing the burden to patients and families.
The burden to this patient population might be alleviated by a multidisciplinary approach to
ormance become momomm r
Regarddddlelll ss ffff tttuture ststststuududud
orporate genotype, and in particular 22q11.2 deletion status, into their analyses o
n
erves as a paradigm for the relationship to be explored between specific genotyp
l o tcomes in the congenital heart disease pop lation Moreo er o r res lts also
orpooorararatetete gggenenenottypypype, and in particular 22q111111.2. deletion statuss,,, into their analyses o
OOOuuuru study alsoo serrveees toooo hhhih ghghhhllil ghgghtt thhhe muulttisysysteeeem mmm naaatuure oofff 22222qqq1q 1.2D2D2D2DSSS aaanddd d bbbrb in
non-cacacacardrdrdr iiiac fafaf tctctororss thththt at cocococonnnntribuuutetete to ooo thththhee vaariaiaiabibibibilililityttyty sseeeeeeen n iinin TTTTOFOFOFOF oooutcoomemes.s AAAAs
erves as a papp radidididigmgg fffor thheh relllatiioi nshihihih ppp to bbbbe expllplor dded bbbbetween spepp cific gegg notyyyppp
l t iin thhe initall hhe t didi lla iti MMo llt lal by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
14
22q11.2DS.
Acknowledgments: The authors acknowledge Sharon Edman, MS, who acted as a database manager for this project
Funding Sources: This work was supported by the National Institutes of Health [P50-HL74731 (EG), 5T32HL007915 (LMR)], as well as Grant UL1TR000003 from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official view of the National Center for Research Resources or the NIH.
Conflict of Interest Disclosures: None
References:
1. Nollert G, Fischlein T, Bouterwek S, Bohmer C, Klinner W, Reichart B. Long-term survival in patients with repair of tetralogy of fallot: 36-year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol. 1997;30:1374-1383.
2. Hickey EJ, Veldtman G, Bradley TJ, Gengsakul A, Manlhiot C, Williams WG, et al. Late risk of outcomes for adults with repaired tetralogy of fallot from an inception cohort spanning four decades. Eur J Cardiothorac Surg. 2009;35:156-164.
3. Valente AM, Gauvreau K, Assenza GE, Babu-Narayan SV, Schreier J, Gatzoulis MA, et al. Contemporary predictors of death and sustained ventricular tachycardia in patients with repaired tetralogy of fallot enrolled in the indicator cohort. Heart. 2014;100:247-253.
4. Murphy JG, Gersh BJ, Mair DD, Fuster V, McGoon MD, Ilstrup DM, et al. Long-term outcome in patients undergoing surgical repair of tetralogy of fallot. N Engl J Med.1993;329:593-599.
5. Carvalho JS, Shinebourne EA, Busst C, Rigby ML, Redington AN. Exercise capacity after complete repair of tetralogy of fallot: Deleterious effects of residual pulmonary regurgitation. Br Heart J. 1992;67:470-473.
6. Garne E, Nielsen G, Hansen OK, Emmertsen K. Tetralogy of fallot. A population-based study of epidemiology, associated malformations and survival in western denmark 1984-1992. Scand Cardiovasc J. 1999;33:45-48.
7. Knauth AL, Gauvreau K, Powell AJ, Landzberg MJ, Walsh EP, Lock JE, et al. Ventricular size and function assessed by cardiac mri predict major adverse clinical outcomes late after tetralogy of fallot repair. Heart. 2008;94:211-216.
G, Fischlein T, Bouterwek S, Bohmer C, Klinner W, Reichart B. Long-term survt a
E ts for adults with repaired tetralogy of fallot from an inception cohort spanning f
u
G, FiFiFiFisscs hleiiinn nn T, BBBouterwek S, Bohmer C, KlKKlinner W, RRReiee chhhart B. Long-term survthh h rereepair of teetttraaalogogy y y ofofoff ffffalalala lolooot:t:t: 3336666---yeaaarr folllowow-u-up ofofof 4449000 sssuurvvvivovoorrrs oof f f f thththt eee fifififirsrsst tt yeyy aalalal rrrrepeee air. J Amm Colll Cardrdrdr iol. 19977;300::137474-13838838333.3
EJ, Veldtman GGG,,, BrBrBradleleleey yyy TJTJJ, ,,, GeG ngggsakuul A,AA, Manlhlhlhlhioii t C,C,, WWWilililliliiliamamams WG, et al. Lats for adults witttthhh h rerereepappap iririrrededede tttetetetetrararalololologygygy oooof fff fafafafalllllototott fffrrom mmm ananann iiiincncn epepepeptititiononono ccccohohohohort spanning f
uuurr JJJ CCaCa drdrdioioioothththororacac SSSururgggg. 202020090909;3;3;35:5:5:5 151515666-161616444.
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
15
8. Greenway SC, Pereira AC, Lin JC, DePalma SR, Israel SJ, Mesquita SM, et al. De novo copy number variants identify new genes and loci in isolated sporadic tetralogy of fallot. Nat Genet.2009;41:931-935.
9. Rauch R, Hofbeck M, Zweier C, Koch A, Zink S, Trautmann U, et al. Comprehensive genotype-phenotype analysis in 230 patients with tetralogy of fallot. J Med Genet. 2010;47:321-331.
10. Benson DW. The genetics of congenital heart disease: A point in the revolution. Cardiol Clin. 2002;20:385-394, vi.
11. Cyran SE, Martinez R, Daniels S, Dignan PS, Kaplan S. Spectrum of congenital heart disease in charge association. J Pediatr. 1987;110:576-578.
12. Michielon G, Marino B, Formigari R, Gargiulo G, Picchio F, Digilio MC, et al. Genetic syndromes and outcome after surgical correction of tetralogy of fallot. Ann Thorac Surg.2006;81:968-975.
13. Hofbeck M, Rauch A, Buheitel G, Leipold G, von der Emde J, Pfeiffer R, et al. Monosomy 22q11 in patients with pulmonary atresia, ventricular septal defect, and major aortopulmonary collateral arteries. Heart. 1998;79:180-185.
14. Momma K, Kondo C, Matsuoka R. Tetralogy of fallot with pulmonary atresia associated with chromosome 22q11 deletion. J Am Coll Cardiol. 1996;27:198-202.
15. Peyvandi S, Lupo PJ, Garbarini J, Woyciechowski S, Edman S, Emanuel BS, et al. 22q11.2 deletions in patients with conotruncal defects: Data from 1,610 consecutive cases. Pediatr Cardiol. 2013;34:1687-1694.
16. Carotti A, Albanese SB, Filippelli S, Rava L, Guccione P, Pongiglione G, et al. Determinants of outcome after surgical treatment of pulmonary atresia with ventricular septal defect and major aortopulmonary collateral arteries. J Thorac Cardiovasc Surg. 2010;140:1092-1103.
17. McDonald-McGinn DM, Sullivan KE. Chromosome 22q11.2 deletion syndrome (digeorge syndrome/velocardiofacial syndrome). Medicine. 2011;90:1-18.
18. Anderson RH, Weinberg PM. The clinical anatomy of tetralogy of fallot. Cardiol Young.2005;15 Suppl 1:38-47.
19. Goldmuntz E, Clark BJ, Mitchell LE, Jawad AF, Cuneo BF, Reed L, et al. Frequency of 22q11 deletions in patients with conotruncal defects. J Am Coll Cardiol. 1998;32:492-498.
20. Jalali GR, Vorstman JA, Errami A, Vijzelaar R, Biegel J, Shaikh T, et al. Detailed analysis of 22q11.2 with a high density mlpa probe set. Hum Mutat. 2008;29:433-440.
lio MC, et al. Genenenenetittt c AnAnAnAnnnn n ThThThThororororacacacac SSSSuruuurgggg....
k M, Rauch A, Buheitel G, Leipold G, von der Emde J, Pfeiffer R, et al. Monosoatients with pulmonary atresia, ventricular septal defect, and major aortopulmonr
a K, Kondo C, Matsuoka R. Tetralogy of fallot with pulmonary atresia associatem
di S, Lu PJ, Garbarini J, Wo iechowski S, Edman S, Emanuel BS, et al. 2 qn patients ith conotr ncal defects: Data from 1 610 consec ti e cases P di t
k M,M,M, RRRRauauauchchchh AAA,,, BuBB heitel G, Leipold G, vvvonoon der Emde J, Pfefefeifiii fer R, et al. Monosoatiieiennntn s withhhh ppulullulmomommonanananaryryry atrrtresesesesiaiaiai , vevevev ntntnttriririr cucc laar septptptalalalal dddeffffeeece t,t,t andnddnd majajajajororoor aaaaortotootopupuppulmlmlmmonrtttterrrries. Heart. 119988;;7;79:181180-18181 5.
a K, KKKKonononondddo CCC, MMMaMattstsuou ka RRRR. TTTTetralalalogogogogy ofofff fff lalalllooottt wiwiwithhthth ppullululmomonanary aaaatrtrtrt eeesiaa aassssocociiaiatettmosome 22q11 dededed leleetitititiononono . J JJ AmAmAmAm CCCCololololl l l CaCaCaCardrdrdioioiolllCCCC . 1919191 9696966;2;2;2; 7:7:7:7:1919191 8-8-8-8-2020202 2.2.2.2
dddi S, Lupoo PPPPJ,JJ, GGGGarararbababbariririnininini JJJ, , WoWoWWoycycycycieieiechchchchowowwowsksksski i ii S,S,S,S EEEEdmddmdmanaanan SSSS,,, EmEmEmEmananaanueueueuel l l BSBSBSBS,, et al. 22qqatiient ii hth ot lal dd fef ts DData ff 11 616100 tii PP didi t by guest on July 16, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
16
21. Mercer-Rosa L, Yang W, Kutty S, Rychik J, Fogel M, Goldmuntz E. Quantifying pulmonary regurgitation and right ventricular function in surgically repaired tetralogy of fallot: A comparative analysis of echocardiography and magnetic resonance imaging. Circ Cardiovasc Imaging. 2012;5:637-643.
22. O'Byrne ML, Mercer-Rosa L, Ingall E, McBride MG, Paridon S, Goldmuntz E. Habitual exercise correlates with exercise performance in patients with conotruncal abnormalities. Pediatr Cardiol. 2013;34:853-860.
23. G P. Pulmonary function in children: Techniques and standards. Saunders; 1971..
24. Cooper DM, Weiler-Ravell D, Whipp BJ, Wasserman K. Aerobic parameters of exercise as a function of body size during growth in children. J Appl Physiol. 1984;56:628-634.
25. Howley ET, Bassett DR, Jr., Welch HG. Criteria for maximal oxygen uptake: Review and commentary. Med Sci Sports Exerc. 1995;27:1292-1301.
26. Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol (1985). 1986;60:2020-2027.
27. Kipps AK, Graham DA, Harrild DM, Lewis E, Powell AJ, Rhodes J. Longitudinal exercise capacity of patients with repaired tetralogy of fallot. Am J Cardiol. 2011;108:99-105.
28. Mahle WT, McBride MG, Paridon SM. Exercise performance in tetralogy of fallot: The impact of primary complete repair in infancy. Pediatr Cardiol. 2002;23:224-229.
29. Mulla N, Simpson P, Sullivan NM, Paridon SM. Determinants of aerobic capacity during exercise following complete repair of tetralogy of fallot with a transannular patch. Pediatr Cardiol. 1997;18:350-356.
30. O'Meagher S, Munoz PA, Alison JA, Young IH, Tanous DJ, Celermajer DS, et al. Exercise capacity and stroke volume are preserved late after tetralogy repair, despite severe right ventricular dilatation. Heart. 2012;98:1595-1599.
31. Reybrouck T, Mertens L, Kalis N, Weymans M, Dumoulin M, Daenen W, et al. Dynamics of respiratory gas exchange during exercise after correction of congenital heart disease. J Appl Physiol (1985). 1996;80:458-463.
32. Takkunen O, Mattila S, Nieminen MS, Sovijarvi AR, Luosto R, Merikallio E. Cardiorespiratory function after correction of tetralogy of fallot. Modifying effect of previous shunt operation. Scand Cardiovasc J. 1987;21:21-26.
33. Horneffer PJ, Zahka KG, Rowe SA, Manolio TA, Gott VL, Reitz BA, et al. Long-term results of total repair of tetralogy of fallot in childhood. Ann Thorac Surg. 1990;50:179-183; discussion 183-175.
geg n upptake: Revieweweww a
g anaaaaererererobobobobicicicic tttthrhrhrhreseseseshohohoh ldg
AK, Graham DA, Harrild DM, Lewis E, Powell AJ, Rhodes J. Lon tudinal exer
WT, McBride MG, Paridon SM. Exercise performance in tetralogy of fallot: Thep
N Simpson P S lli an NM Paridon SM Determinants of aerobic capacit d rin
ge. J J J ApApAApplplplp PPPPhyyysiss ol (1985). 1986;60:2020-0-0-2022 27.
AKKK,,, , Graham DDAAA, HHHaaarriildldldd DM,MMM LLLewisss EE, PoPoweellll AAAJJ,J RRRhhodees J. LLLLongigigigituuuddiinnnal exeexerpaaatitiiene ts wititith rereepaiireed tttetete rar loogyg oof faaalllot. AmAAm JJJ Carardiiioll. 2001111;1;1;100080 :99-9-9-9-1000555.
WT, McBride MGMGMGM ,,,, PaPaPaP riririridododon n n n SMSMSMSM. ... ExExExxererere ciciisesese ppppererererfoff rmrmrmrmanananancececec iiiin n n n teteteetrtrtralalalogogogogyy y of fallot: Theprimary yy comppplete reppp iaiir iiin iiii ffnfancyyy. PePP dididid atr CCCaC rdioi l. 2020202 0202022;2;222333:3 222224-444 229.
NNN SSiim PP SS llllii NNMM PP idid SSMM DDet imi nt fof bobiic iit dd iri by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
17
34. Wessel HU, Weiner MD, Paul MH, Bastanier CK. Lung function in tetralogy of fallot after intracardiac repair. J Thorac Cardiovasc Surg. 1981;82:616-628.
35. Fredriksen PM, Ingjer F, Nystad W, Thaulow E. A comparison of vo2(peak) between patients with congenital heart disease and healthy subjects, all aged 8-17 years. Eur J Appl Physiol Occup Physiol. 1999;80:409-416.
36. Sinderberry B, Brown S, Hammond P, Stevens AF, Schall U, Murphy DG, et al. Subtypes in 22q11.2 deletion syndrome associated with behaviour and neurofacial morphology. Res Dev Disabil. 2013;34:116-125.
37. Angkustsiri K, Leckliter I, Tartaglia N, Beaton EA, Enriquez J, Simon TJ. An examination of the relationship of anxiety and intelligence to adaptive functioning in children with chromosome 22q11.2 deletion syndrome. J Dev Behav Pediatr. 2012;33:713-720.
38. Bassett AS, Chow EW, Husted J, Weksberg R, Caluseriu O, Webb GD, et al. Clinical features of 78 adults with 22q11 deletion syndrome. Am J Med Genet A. 2005;138:307-313.
39. Butcher NJ, Chow EW, Costain G, Karas D, Ho A, Bassett AS. Functional outcomes of adults with 22q11.2 deletion syndrome. Genet Med. 2012;14:836-843.
40. Bassett AS, Hodgkinson K, Chow EW, Correia S, Scutt LE, Weksberg R. 22q11 deletion syndrome in adults with schizophrenia. Am J Med Genet A. 1998;81:328-337.
b bbb GDGDGDGD,,,, etetetet aaaal.l.l.l CCCClilililinininnicaaaallllA. 20000000055;55 131313138888:303030307-7 313131313
r NJ Chow E Costain G Karas Ho Bassett AS. Functional outcomes of
AS, Hodgkinson K, Chow EW, Correia S, Scutt LE, Weksberg R. 22q11 deletion
r NJNJJ, ChChChChowowow EW,WWW Costain G, Karas D, Hooo A,AA Bassett AS. FFFunununctional outcomes of222222qqq1q 1.2 deeeeletitiitionooo ssssynynyyndrdrdrdrommme.e.e.e. GeGeGenenenet t MeMeMeM d. 2201222;1;11;14:4:44:833336-6-6-6 8484843.3.3.
ASASAS, Hodgggkikik nssooon KK,,, Chhhowow EW,,W, CCorrrrerreia SS,, Scccuutt LLE, WWeksbbbergrgg R. 222222q111111 deeeleetion addddululultstststs wwwith hh scschihhihizozo hphphrenininiaaaa. AAAm JJJJ MMMMededede GGGGenettt AAAA. 19191999898989 ;88;8;811:1:1 32323228-888 33333777.7
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
18
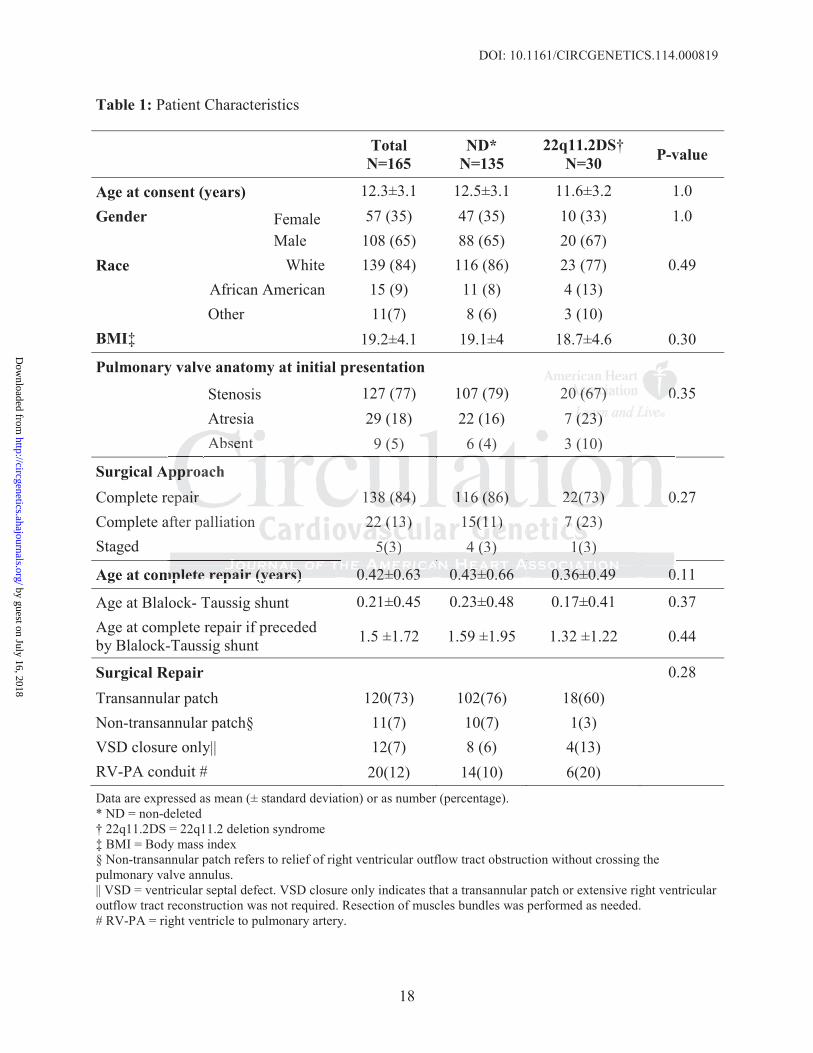
Table 1: Patient Characteristics
Total N=165
ND*N=135
22q11.2DS†N=30 P-value
Age at consent (years) 12.3±3.1 12.5±3.1 11.6±3.2 1.0Gender Female 57 (35) 47 (35) 10 (33) 1.0
Male 108 (65) 88 (65) 20 (67) Race White 139 (84) 116 (86) 23 (77) 0.49
African American 15 (9) 11 (8) 4 (13) Other 11(7) 8 (6) 3 (10)
BMI‡ 19.2±4.1 19.1±4 18.7±4.6 0.30
Pulmonary valve anatomy at initial presentation
Stenosis 127 (77) 107 (79) 20 (67) 0.35Atresia 29 (18) 22 (16) 7 (23) Absent 9 (5) 6 (4) 3 (10)
Surgical ApproachComplete repair 138 (84) 116 (86) 22(73) 0.27Complete after palliation 22 (13) 15(11) 7 (23) Staged 5(3) 4 (3) 1(3)
Age at complete repair (years) 0.42±0.63 0.43±0.66 0.36±0.49 0.11
Age at Blalock- Taussig shunt 0.21±0.45 0.23±0.48 0.17±0.41 0.37Age at complete repair if preceded by Blalock-Taussig shunt 1.5 ±1.72 1.59 ±1.95 1.32 ±1.22 0.44
Surgical Repair 0.28Transannular patch 120(73) 102(76) 18(60) Non-transannular patch§ 11(7) 10(7) 1(3) VSD closure only|| 12(7) 8 (6) 4(13) RV-PA conduit # 20(12) 14(10) 6(20) Data are expressed as mean (± standard deviation) or as number (percentage). * ND = non-deleted † 22q11.2DS = 22q11.2 deletion syndrome‡ BMI = Body mass index§ Non-transannular patch refers to relief of right ventricular outflow tract obstruction without crossing the pulmonary valve annulus. || VSD = ventricular septal defect. VSD closure only indicates that a transannular patch or extensive right ventricular outflow tract reconstruction was not required. Resection of muscles bundles was performed as needed. # RV-PA = right ventricle to pulmonary artery.
20000 ((((67676767)))) 00007 (2(2(2(23)3)3)3)
mplete repair (years) 0.42 0.63
( ) ( ) ( )
Ae
a
0.43 0.66 0.36 0.49 0
( ) ( ) ( )Abbbseseeent 9 (5) 6 (4) 3 (10)
Apppp rrror achepaiaiaiairr 133338 88 (8(8(884)4)4) 11116 6 66 (8(886)6)6)) 2222222(7((73)3)3)3) 0
after palliation 22222222 ((((13131313) ) 15555(1(1(1( 1)1)1)1) 7777 (2(2(2(23) 5(5((3)3)) 4 (3(3( ) )) 1(3(3( )))
mmmplpletetee rerepapairiir (((yeyearar )s)s) 0.00 4242424 ±0±0±00 6.663333 000.0 43434343±0±0±00 66.66666 0.00 3636366±0±0±0 44.4499 9 000 by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
19
Table 2: Cardiovascular Status: Cardiac Magnetic Resonance, Exercise Stress Test and Electrocardiogram
CARDIAC MAGNETIC RESONANCE TotalN=148
ND*N=108
22q11.2DS†N=26 P-value
RV ejection fraction (%)‡ 60±8 60±8 60±10 0.98Pulmonary regurgitant fraction (%) 34±17 35±16 28±19 0.11RV end-diastolic volume (mL/m2) 114±39 117±40 104±35 0.04§RV end-diastolic volume (mL/m2) adjusted 113(87; 144) 115 (90; 149) 106 (82; 138) 0.40 RV end-diastolic volume Z score 3.1 ± 2.9 3.4 ± 2.8 1.8 ± 2.8 0.0093*RV end-systolic volume (mL/m2) 48±20 49±19 43±23 0.062RV cardiac index (L/min/m2) 5.5±1.5 5.7±1.4 5.1±1.5 0.043RV stroke volume (mL/m2) 69.7±19 72±18.5 61±18 0.01Indexed RV mass (grams/m2) 76±23 77 ±24 68±21 0.10LV ejection fraction (%)|| 69±7 70 ±7 66±8 0.05LV cardiac output (L/min/m2) 3.7±0.7 3.7±0.7 3.6±0.8 0.61EXERCISE STRESS TEST N=156 N=129 N=27Maximal e # 94 (63) 84 (68) 10 (40) 0.012Forced vital capacity (Liters) 2.3±0.9 2.41±0.9 1.5±0.6 <0.0001% Predicted forced vital capacity 77±16 81± 14 62±16 <0.0001Cardiovascular Response at Peak ExercisemVO2 (mL/kg/min)** 32±8 33±8 24±7 <0.0001Predicted mVO2 (%) 76±18 80±17 61±17 <0.0001Maximum work (watts) 112 ± 48 117 ± 49 83 ± 28 0.0041% Predicted maximum work 83 ± 23 86 ± 22 64 ± 18 0.0002Oxygen pulse (ml oxygen/beat) 7.4 ± 2.9 7.8 ± 2.9 5.4 ± 2.2 <0.0001Oxygen pulse/m2 (ml oxygen/beat/m2) 5.5 ± 1.4 5.8 ± 1.3 4.4 ± 1.2 <0.0001Breathing reserve (%) 16 ±13 15 ± 13 19 ± 10 0.12Maximum heart rate (beats per minute) 180 ± 15 182 ± 14 175 ± 17 0.08Anaerobic Threshold MeasurementsVO2 at anaerobic threshold (mL/kg/min)** 21 ± 5 21 ± 5 19 ± 6 0.036Predicted VO2 at anaerobic threshold (%) 86 ± 18 87 ± 17 80 ± 21 0.085ELECTROCARDIOGRAM N=155 N=129 N=26PR interval 137 ± 25 135 ± 24 147 ± 25 0.04QRS duration 126 ± 25 125 ± 25 130 ± 24 0.44QTc interval†† 446 ± 26 446 ± 27 450 ± 25 0.47Right bundle branch block 106(84) 88(85) 18(75) 0.037
Data are expressed as mean (± standard deviation), or number (percentage). * ND = non-deleted † 22q11.2DS = 22q11.2 deletion syndrome‡ RV = right ventricle § RV end-diastolic volume adjusted for reoperations to limit pulmonary insufficiency (RV to pulmonary artery conduit or pulmonary valve replacement).|| LV = left ventricle#RER = respiratory exchange ratio**mVO2 = maximum oxygen consumption. VO2 indicates oxygen consumption††QTc = QT interval corrected for heart rate
66666±8±8±±3.3.3.3 6±6±6±6±0.0.0.0 8888N=NNN 27272727
# 94 (63) 84 (68) 10 (40)<
d <c
L <m <w 0d 0lse (ml oxygen/beat) 7 4 ± 2 9 7 8 ± 2 9 5 4 ± 2 2 <
### 94 ((((6363) 84 (68) 10 (40)l cccapapapapacity (LLLLiiiters) 2.3±00.99 2.414141±0.9 1.5±0.6 <d foorrced ff vital capapaaacititityy 777±1166 8111±± 1444 62626262±1±1±1± 6666 <cuuulararara Responsee aaat Peaeaak ExExExeree cisee
L/kg/g/g/g/mimimim n)n)n)n)******** 3232323 ±8±8±8± 33333333±8±8±8±8 24242424±777 <mVO2 (%) 7676766±1±±1± 888 8080880±1±1±117777 61±17 <work (watts) 1111111222 ±±± 4848488 111111117777 ±±± 4949449 83 ± 28 0ddd maximum mm wowwoworkrkkrk 83838383 ±±±± 2223333 8688686 ±±± 22222222 6464644 ±±±± 1118 00lsl e ((mll oxygen/b/beat)t) 77 44 ±± 22 99 77 88 ±± 22 99 55 44 ±± 22 22 << by guest on July 16, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
20
Table 3: Comparison of ND and 22q11.2DS groups for number of hospitalizations and use of medications
ND 22q11.DS P value
Overall hospitalizations [n, interquartile range (IQR)] 3 [2; 5] 6.5 [5; 10] <0.0001
Used one or more medication (%) 34 67 <0.0001
Cardiac hospitalizations (n, IQR) 2 [1; 3] 3 [1; 4] 0.032
Used one or more cardiac medication (%) 13 23 0044
Non-cardiac hospitalizations (n, IQR) 1[0; 3] 4 [2; 7] <0.0001
Used one or more non-cardiac medication (%) 25 60 <0.0001
23232323 0
a
o
acccc hhhhospitalilililizaazatitititionnnssss (n(n(n, IQIQIQR)R)R)R) 1[1[1[1[0;0;0; 333] ] ] 4 44 [2[2[22; ; 7]7]]7] <0
or morererere non-ca ddrdiiiac medididication ((((%)%)%)% 2525255 66606 <<<0
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.114.000819
21
Table 4: Multivariable analysis comparing the ND* and 22q11.2DS† groups for incidence rate of cardiac and non-cardiac surgeries, hospitalizations, and cardiac catheterizations
Dependent variables Beta SE OR‡ 95% CI P value
Cardiac Catheterizations 0.32 0.19 1.38 0.95; 2.01 0.09
Non-Cardiac Surgeries 1.26 0.24 3.54 2.23; 5.62 <0.0001
Hospitalizations 0.60 0.14 1.82 1.39; 2.38 <0.0001
Total cardiac surgeries§ 0.18 0.10 1.20 0.99; 1.45 0.07
Primary cardiac surgeries adjusting for time from birth to last primary surgery and PV anatomy||
Genotype 22q11.2DS vs. ND 0.19 0.18 1.21 0.85; 1.72 0.29
PV|| Anatomy§ PA# vs. PS** -0.28 0.17 0.76 0.55; 1.06 0.10
Abs. PV†† vs. PS** 2.06 0.35 7.83 3.98; 15.39 <0.0001
Subsequent surgeries adjusting for time from last primary surgery to last follow up and PV anatomy
Genotype 22q11.2DS vs. ND 0.49 0.35 1.63 0.83; 3.22 0.16
PV Anatomy PA vs. PS 0.33 0.39 1.40 0.65; 2.9 0.39
Abs. PV vs. PS 1.14 0.43 3.13 1.34; 7.30 0.008
* ND = non-deleted † 22q11.2DS = 22q11.2 deletion syndrome‡ Odds ratios correspond to the independent association of genotype 22q11.2DS with outcome after adjusting for age and years of follow up.§ Adjusting for presenting pulmonary valve anatomy|| PV = pulmonary valve #¶ PA = pulmonary atresia **# PS = pulmonary stenosis††**Abs PV= absent pulmonary valve leaflets
00.00 99999999;;;; 1.1.11 45454545 0000
diac i dj sting for time from birth to last primary surgery and PV anatom
0
y 0
Abs PV†† s PS** 2 06 0 35 7 83 3 98; 15 39 <0
diac susuusurgrgrgrgereerieieiei s adadaddjusting for time from birtrtrtrthh hh to last primary sususuurgery and PV anatom
22q11.2DDSSS vss. NDND 0.19119 0.18 11.221 0...85; 111.1 7727 0
y§ PA# vsss. PSPSPSS******** -0-0-0-0.2.2.2.2888 0.0.0.0.1717171 0.000 7676766 0.0.0.0 55555555; 1.06 0
AbAbs PPV†V††† s PSPS**** 22 0606 00 3535 77 8383 33 9898; 1515 3399 0<0 by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.114.000819
22
Figure Legends:
Figure 1: Description of the study population. The flow chart represents the number of subjects
with TOF that were available for recruitment from our institution’s databases and the final
composition of the study cohort.
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

Xuemei Zhang, Wei Yang, Justine Shults and Elizabeth GoldmuntzLaura Mercer-Rosa, Stephen M. Paridon, Mark A. Fogel, Jack Rychik, Ronn E. Tanel, Huaqing Zhao,
Fallot22q11.2 Deletion Status and Disease Burden in Children and Adolescents with Tetralogy of
Print ISSN: 1942-325X. Online ISSN: 1942-3268 Copyright © 2015 American Heart Association, Inc. All rights reserved.
TX 75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas,Circulation: Cardiovascular Genetics
published online January 5, 2015;Circ Cardiovasc Genet.
http://circgenetics.ahajournals.org/content/early/2015/01/04/CIRCGENETICS.114.000819World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circgenetics.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Genetics Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information aboutnot the Editorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center,Circulation: Cardiovascular Genetics Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 16, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from




![Association between phenotype and deletion size in 22q11.2 ......deletion in 43 of them [13]. Hwang et al. (2014) included 80 individuals from a neurodevelopmental clinic in the United](https://img.pdfslide.us/doc/110x75/6131b9161ecc51586944ea4f/association-between-phenotype-and-deletion-size-in-22q112-deletion-in-43.jpg)
























