-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
1/44
22q11.2deletion syndrome
(DiGeorge syndrom)
Dr. Ahmed A. Azab MBBCH,MSc,MDAss.professor of pediatrics and
neonatology
Benha University ,EgyptConsultant of pediatrics and
neonatology
Alnoor Specialist hospital.
April 2011
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
2/44
Objectives
Summarize advances in understanding the: pathogenesis and
genetics of the syndrome
health needs and immune system of patients withChromosome
22qDeletion Syndrome
Understand the spectrum of clinical presentation
Overview of the multidisciplinary approach tocaring for these
patients
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
3/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
4/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
5/44
Historical Perspective
Common embryologic derivation of heart, thymus
and parathyroid glands as explanation formalformations.
Combination of lack of thymus, parathyroid
glands, hypocalcemia, congenital heart disease
(TOF)
Angelo DiGeorge,
04/15/21-10/11/09
DiGeorge Syndrome, 1965
Significant overlap, Deletion of 22q11.2
1671: Nicolai Stensencleft palate and truncus arteriosus
1829: LH Harringtonhypoplastic thymus & parathyroid
glands
1959: Eva Sedlackovavelopharyngeal insufficiency and DD
David Lobsdellhypoplastic thymus and parathyroid glands1978:
Robert Shprintzen--Velocardial Facial Syndrome (VCFS)
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
6/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
7/44
Chromosome 22q11.2 deletion syndrome
Hemizygous deletion of ch22q11.2
90% of patients with DiGeorge syndrome
80% of patients with VCFS
Also described in
CHARGE (coloboma, heart anomaly, choanal atresia, retardation
and
genital and ear anomalies) Conotruncal anomaly face syndrome
Cat eye syndrome
Some pts may have deletion but not fall into a clinically
defined syndrome, or have syndrome but not deletion
DiGeorge syndrome = cardiac anomaly, hypocalcemia,poor T cell
production
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
8/44
Chromosome 22q11.2 deletion syndrome
1 in 3000 children Typical: conotruncal cardiac anomaly and
mild
to moderate immune deficiency
Often: developmental delay, palatal dysfxn,feeding problems
Great phenotypic HETEROGENEITY!
Clinical suspicion is key to making the dx!
Compared to incidence of other diseases: Invasive MRSA 1 in 3000
(CDC, 2007)
CF 1 in 2000
Sickle cell disease: 1 in 500 African-American birthsand 1 in
every 1000 to 1400 Hispanic-American births.
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
9/44
Abnormality % affected Examples
Cardiac anomalies 49-83 TOF, IAA, VSD, TA
Hypocalcemia 17-60
Palatal anomalies 69-100 Cleft palate, submucous
cleft,velopharyngeal insufficiency, bifid uvula
Speech Delay 79-84
Developmental delay 75% - infancy
45% - childRenal anomalies 37 Absent/dysplastic, obstruction,
reflux
Ophthalmologic 7-70 Tortuous vessels, anterior
segmentdysgenesis
Skeletal 17-19C-spine, vertebral, lower extremity
Behavior, psychiatric 9-50 ADHD (25%); Schizoprenia (6-30%)
Neurologic 8 Cerbral atrophy, cerebellar hypoplasia
Growth hormone def. 4
Dental 2.5 Delayed eruption, enamel hypoplasia
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
10/44
Phenotype Frequency of deletion (%)
Interrupted aortic arch 50-60
Pulmonary atresia 33-45
Aberrant subclavian 25
TOF 11-17Conotruncal cardiac anomaly 7-50
Any cardiac lesion 1.1
Velopharyngeal insufficiency 64
Velopharyngeal insufficiency post
adenoidectomy
37
Neonatal hypocalcemia 74
schizophrenia 0.3-6.4
Frequency of 22q11.2 deletion
in Various Populations
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
11/44
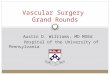
Facial appearance of patients withtypical and atypical 22q11.2
deletions.
Rauch A et al. J Med Genet 2005;42:871-876
Mild phenotype, sibling pair
3Mb and 1.5 Mb deletionsmall mouth, pointed nasal tip, mild
ptosis, lowset ears
thin upper lip, mild hypertelorism and broad, high nasal
bridge
F i l f i i h
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
12/44
Facial appearance of patients withtypical and atypical 22q11.2
deletions.
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
13/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
14/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
15/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
16/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
17/44
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
18/44
Diagnosis Most deletions spontaneous
(1 in 4000 to 1 in 6000)
At least 10 fold > than next most frequent human
deletionsyndrome
1 in 3000 births Estimated from spontaneous mutation rate plus
growing number of
familial cases
Increased survival of pts w/ cardiac anomalies
Hemizygous deletion inherited Autosomal Dominant
Affected sib w/ negative FHx relies on recognition of s/sx
Flourescence In Situ Hybridization (FISH) for 22q11.2 deletion
Accurate, but time consuming and expensive
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
19/44
The diagnosis is established by FISH
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
20/44
FISH for 22q11.2
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
21/44
When FISH is negative but classic
features present Point mutations in TBX1
Transcription factor involved in regulation ofdevelopmental
processes
Expressed during embryogenesis in pharyngeal arches,
pouches and otic vesicle Candidate gene for some features seen
in 22q11.2
Non-ch22 basis: Chromosome 10 terminal deletions
CHD7 (chromodomain helicase DNA-binding protein)
Prenatal exposure to teratogens isotretinoin, a vitamin A analog
or acne treatment
No clear etiologic basis for some (risk of recurrence in
these, unknown)
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
22/44
Deletion of Chromosome 22q11.2
This region contains >35 genes
Which genes contribute to phenotype?
Mouse studies:
TBX-1 cardiac abnormalities
All embryos w/ defects of branchial arch precursor of
Hear t and thymus!
BUT, only a subset with cardiac defect at birth could there be
in utero intervention?
TBX-1: cardiac, thymus and parathyroid phenotypes
Retinoic acid is a repressor of TBX1
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
23/44
TBX-1 (T-box transcription factor)
CRKL
UFD1L (Ubiquitination degradation)
HIRA (transcription factor)
Centromere
DGCR6
IDD/DGCR2TSK/DGS-GES2/DGS1
GSCL (Goosecoid-like homeobox gene)CTP (Citrate transporter)
CLTCL
TMVCF
CDCrel-1
GP1b (Platelet glycoprotein)
T10
COMT (Catechol-O-methyltransferase)
ARVCF
LZTR-1 (Transcription factor)
ZNF74
CDC45L
RANBP1
Human Ch22q11.2
Heparin cofactor
90% 8%
22 well-characterized genes
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
24/44
DGCR6
IDD/DGCR2TSK/DGS-GES2/DGS1
GSCL (Goosecoid-like homeobox ge ne)CTP (Citrate
transporter)
HIRA (transcription factor)
TMVCF
UFD1L (Ubiquitination de gradation)
GP1b (Platelet glycoprotein)
TBX-1 (T-box transcription factor)
T10
COMT (Catechol-O-methyltransferase)
ARVCF
ZNF74
CDC45L
RANBP1
Murine Deletions (Ch16)
VpreB2
NLVCF
Pnufl
Miceh
avecardiacdefects
Miceare
normal
Candid
ateGenes
The critical region was established by generating mice with
comparable deletions
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
25/44
Tbx-1
Expressed in developing mesenchyme
Expressed in pharyngeal arches, otic vesicle, toothbuds,
sclerotome
Heterozygous mutations of Tbx-1 are associated withgreat vessel
defects in mice
Homozygous deficient mice have a small mandible,low set ears, a
single cardiac outflow tract, deficient
thymus/parathyroid/salivary glands
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
26/44
Age-specific health needs in 22q11.2 deletion
Coordinated approach (multi-specialty needs)
Phenotypes and outcomes vary tremendously
Dx mostly shortly after birth (Cardiac anomaly)
Sullivan, KE 2008
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
27/44
Early Immunologic concerns:
Low T cell numbers (Mild to Moderate)75 to 80% of infants with
deletion
Lack of T cells =
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
28/44
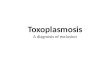
Normal Thymus & T cell development
Hassalls corpuscle
Savina, PLOS Patho ens, June 2006 Volume 2 Issue 6 e62
earliest events in thymocyte
development TCR gene rearrangement
positive selection
later events negative selection
expression of CD4 or CD8
http://upload.wikimedia.org/wikipedia/commons/9/94/Thymic_corpuscle.jpg
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
29/44
Role of the Thymic Microenvironment
in T cell development
Cortex
Medulla
Savina, PLOS Pathogens, June 2006 | Volume 2 | Issue 6 | e62
T cell precursors
enter here
Thymic nurse cells
TREC Assay for NBS of SCID and T cell
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
30/44
TREC Assay for NBS of SCID and T cell
lymphopenia (Complete DiGeorge)
Quantitation of TRECs DNA excision circles
Byproduct of TCR gene rearragement in
developing thymocytes
Assayed in blood by quantitative PCR
(# diluted with each cell division)
DX: based on the inability to make normal #
of T cells
Results:
low or undetectable TRECs in SCID or
complete DiGeorge
High in healthy newborns
Challenges/caveats:
Maternal engraftment
poor DNA recovery/intermediate results
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
31/44
Endocrine Concerns:
Hypocalcemiaexacerbated by cardiac surgery
Ca++ supplementation perioperatively Endocrine referral for:
Vit D requirements, calcium, phosphorus mngmt
Oversupplementation nephrocalcinosis
Most do well, but rare cases of late onset or recurrence
Feeding Concerns:
Poor coordination of pharyngeal muscles, tongue,
esophagus, dyspnea 2ndary to cardiac defect
D l t l
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
32/44
Developmental concerns:
Speech delay: phonation, language development,comprehension
Laryngeal webs, velopharyngeal insufficiency, or VC paralysis
Speech delay > receptive skills > social language skills
Speech delay + weakness pattern = typical of 22q11.2 del
Sign language vs. Speech therapy or both
Most learn to speak and communicate effectively
IQ: mean 70 with wide range normal to moderately disabled
Visuoperceptual and planning = weakest
Learning disability may be the ONLY manifestation of
22q11.2 deletion syndrome!!! School based interventions
important
Neuro: 10-30% of older ptsbipolar, autistic spectrum
orschizophrenia/schizoaffective d/o (significant increase over
other conditions with Dev Delay)
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
33/44
Immunodeficiency
Thymic hypoplasia decreased T cell #
20% no evidence of low T cells
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
34/44
Mild or moderate T cell deficiency
Normal Immunoglobulins (majority)
Infrequent humoral dysfxn: IgA deficiency, impaired responses
tovaccines, hypogammaglobulinemia
Normal T cell proliferative response
Most common infxn = URI Anatomy > T cell count
Opportunistic infxn infrequent
Slower age associated decline in T cell # Homeostatic
proliferation of existing T cells
Normal cytokine production
Increased autoimmunity:
JIA, ITP*, celiac disease Decreased Treg, selection for
self-reactive T cells
Increased allergic disease (Th2)
Live vaccines tolerated in this group T cell count >300, MMR,
Varicella efficacious*
Homeostatic proliferation
*Perez E, et al. Safety of live viral vaccines in patients with
chromosome 22q11.2 deletion syndrome. Pediatrics 2003
Th mic aplasia (Se ere)
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
35/44
Thymic aplasia (Severe)
22q11.2 deletion in 50% of these cases
True thymic aplasia and absent T cells Spectrum of T cell counts
from 0 normal
Difficulty in identifying pts who need transplant
Transplantation
Thymus
Fully matched peripheral blood
Peripheral T cells so that thymic education is not
required(thymic aplasiaT cells have nowhere to develop)
Donor lymphocyte infusions Nave T cell compartment assessment
early
CD4+CD45RA vs. CD4+CD45RO
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
36/44
Thymus transplantation*
Donor thymic tissue harvested, cultured to
remove mature T cells (GVH risk) Implanted under quadriceps
muscle
Partial HLA matching desirable, not required
Fxnl T cells in 3-4 months post transplant T cell repertoire
initially normal but
Thymic involution prevents sustained production of T
cells sufficient #s produced to provide adequate defense
Follow up studies needed for long term outcomes
* Duke University, Dr. Louise Markert
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
37/44
Oligoclonal Expansion of T cells in Thymic Aplasia
1/3 of infants with thymic aplasia caused bych22q11.2 deletion
have dramatic oligoclonalexpansion of a few founding T cells
T cell count does not reflect adequacy of T cell
compartment Expanded from very small number of fxnl T cells
Clues: erythroderma (similar to Omenns syndrome)
Predominance or exclusively Memory T cells (CD45RO)
TREC negative
Oligoclonal
Referral to Immunologist!
I l i t R l
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
38/44
Immunologists Role
Intervention Timing
T cell enumeration ASAP, and prior to live vaccines @ 1yr of
age
T cell functional testing ASAP
TREC If suspect severe phenotype
B cell function
(Igs, titers)
ASAP then prn depending on recurrent infection
history
Calcium level ASAP and prn
FISH analysis If not known or performed
Referral for developmental
evaluation
Asap, 1yr, 18m, yearly after 2y
Antibiotic prophylaxis (TMP) CD4
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
39/44
Live Vaccines in 22q11.2del Syndrome Live vaccines
contraindicated in
Immunodeficiency (package insert)
T cell immunity crucial in fighting viral
infectionseffectively
Better understanding of risk/benefit necessary
for 22q11.2del syndrome due to high incidenceand phenotypic
heterogeneity
Less than 1% of cases severe but need to beconfident of normal T
cell function and assure nosevere immunodeficiency prior to
exposure
Few publications/studies examining this:
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
40/44
Safety of Live Viral Vaccines in 22q11.2 Deletion Syndrome
AIM: to investigate the incidence of side effects after live
viral vaccine administration in
22q11.2 deletion syndrome retrospective analysis of vaccine
adverse to evaluate the frequency of live vaccine
administration and the consequences of both vaccination and
withholding the vaccine.
Flow cytometric enumeration of T cells
Results:
32/59 responders vaccinated with varicella vaccine 9% of
patients reported adverse events (mild)
63% of unvaccinated children developed chickenpox.
Tolerated vaccine vs. adverse events group:
no statistically significant differences in:
current ageor age at vaccination (3 vs 2.5 years) T-cell subset
counts:
CD3 (1951 vs 2083 cells/uL)
CD4 (1283 vs 1463cells/uL)
CD8 (530 vs 502 cells/uL)
Perez, et al. PEDIATRICS Vol. 112 No. 4 October 2003
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
41/44
Safety of Live Viral Vaccines in 22q11.2 Deletion Syndrome
Results (continued):
--52/59 responders vaccinated with measles-mumps-rubella
(MMR).
Twelve (23%) of 52 reported mild side effects, including fever,
rash, and constitutional
symptoms.
No severe adverse reactions were reported.
No patient reported natural disease with measles, mumps, or
rubella.
No statistically significant differences between the T-cell
counts in the vaccinated group
reporting side effects versus the vaccinated group without side
effects
mean CD3 counts: 1928 vs 1736 cells/uL
CD4 counts: 1250 vs 1127 cells/uL
CD8 counts: 528 vs 483 cells/uL
Perez, et al. PEDIATRICS Vol. 112 No. 4 October 2003
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
42/44
Safety of Live Viral Vaccines in 22q11.2 Deletion Syndrome
Conclusion: This is a cohort of patients with 22q11.2deletion
syndrome who
have tolerated live viral vaccinations without evidence
ofsignificant side effects.
A prospective study could address whether there are
T-cellthresholds below which vaccination is unsafe
Data suggests that vaccinating children with chromosome
22q11.2deletion with live viral vaccines does not carry a
significantlyhigher risk of adverse reactions compared with the
generalpopulation,provided that they have no evidence of
severeimmunocompromise.
withholding vaccination, can result in a high frequency of
wild-type disease.
Perez, et al. PEDIATRICS Vol. 112 No. 4 October 2003
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
43/44
Interdisciplinary managementCardiology
Cleft palate team
Endocrinology
Immunology
Otolaryngology/Audiology
Genetics
OrthopedicsOphthalmology
Urology
Neurology
Psychologist/PsychiatristSpeech therapy
Occupational therapy
Feeding team
Early intervention
-
8/3/2019 22q11-grand rounds-9-2310- ep - Copy
44/44
Considerations for the Primary Care Doctor
Incidence is 1 in 3000increase your clinical suspicion
Refer to immunologist for evaluation esp in setting ofrecurrent
infection in patient with: congenital heart defect, esp any of the
following:
Interrupted aortic arch (50-60%)
Pulmonary atresia (33-45%)
Aberrant subclavian (25%) TOF (11-17%)
Conotruncal cardiac anomaly (7-50%)
Neonatal hypocalcemia (74%)
Velopharyngeal insufficiency (64%)
FISH for 22q11.2 deletion Consider the heterogeneity / spectrum
of the disorder and
know that outcomes are generally good but highly variablepatient
to patient.
NO LIVE VACCINES UNTIL CLEARED BY IMMUNOLOGY!