Embed Size (px)
Citation preview
2018 Summary of BenefitsEon Deluxe (HMO SNP)GEORGIA / SOUTH CAROLINA
For more information, call 1-844-895-8643 Y0122_0172 AcceptedDSNP
This page intentionally left blank

This is a summary of drug and health services covered by Eon Health January 1, 2018 - December 31, 2018.
Eon Health has a contract with Medicare to offer HMO and PPO plans. Eon Health also has a contract with the Georgia Medicaid program and a contract with the South Carolina Medicaid program. Enrollment in Eon Health depends on contract renewal.
The benefit information provided is a summary of what we cover and what you pay. It does not list every service that we cover or list every limitation or exclusion. To get a complete list of services we cover, please request the “Evidence of Coverage.” You can obtain a copy of our Evidence of Coverage by calling us at: Current Members: 1-888-906-3889, Prospective Members: 1-844-895-8643, TTY: 711 or visiting our website at www.eonhealthplan.com .
For coverage and cost of Original Medicare look in your current “Medicare and You” Handbook. View it online at www.medicare.gov or get a copy by calling 1-800-Medicare (1-800-663-4227). TTY users should call 1-877-486-2048.
Eon Health has a network of doctors, hospitals, pharmacies, and other providers. If you use the providers that are not in our network, the plan may not pay for these services.
You can see our Provider and Pharmacy Directory on our website at www.eonhealthplan.com
You can see our Formulary (List of Part D prescription drugs) on our website at www.eonhealthplan.com
2018 Summary of BenefitsEon Deluxe (HMO SNP)

IntroductionEon Deluxe
is a Medicare Advantage HMO Special Needs Plan (SNP) offered in Georgia and South Carolina.
Georgia: To join Eon Deluxe, you must be entitled to Medicare Part A, enrolled in both Medicare Part Band Georgia Medicaid Program, and live in our service area.
South Carolina: To join Eon Deluxe, you must be entitled to Medicare Part A, enrolled in both Medicare Part Band South Carolina Medicaid Program-Healthy Connections, and live in our service area.
Eon Deluxe Service Areas:
STATE SERVICE AREA
GEORGIA Baker, Baldwin, Banks, Barrow, Bibb, Bleckley, Bryan, Butts, Chatham, Cherokee, Clayton, Clinch, Crawford, Dawson, DeKalb, Dodge, Dooly, Fayette, Forsyth, Franklin, Greene, Hancock, Hart, Heard, Henry, Houston, Jasper, Jones, Lamar, Lumpkin, Macon, Madison, McIntosh, Meriwether, Monroe, Morgan, Newton, Oconee, Oglethorpe, Peach, Pickens, Pike, Pulaski, Putnam, Rabun, Rockdale, Schley, Screven, Stephens, Talbot, Taliaferro, Taylor, Twiggs, Walton, White, Wilcox, Wilkinson counties
SOUTH CAROLINA Beaufort, Chester, Colleton, Fairfield, Greenville, Hampton, Jasper, Lee, Saluda, Spartanburg, Union counties

Eon Deluxe (HMO SNP)SUMMARY OF BENEFITS
Health Maintenance Organization (HMO)
plans – in most HMOs, you can only go to
doctors, other health care providers, or
hospitals in the plan’s network. In an urgent
or emergency situation you can access in-
network and out of network providers.

Eon DeluxeHMO SNP / Plan Highlights
Monthly Premium:$0
Provider Copay:$0 PCP / $0 Specialist / $0 Hospital
Generic Prescriptions:As low as $0
Dental Care:Preventative • Comprehensive • Dentures
Vision Care:$225 towards glasses or contact lenses
Hearing Care:Exams and up to $750 for hearing aids
Over-The-Counter (OTC) items:$45 allowance per month
Transportation:30 one-way to plan-approved locations
Meals:Up to 20 meals after inpatient hospital stay
Fitness Program:SilverSneakers®

Benefits Eon Deluxe / Health BenefitsMonthly Premium $0 per month
DeductiblePart C (Medical) $0Part D (Pharmacy) $0
Maximum Out-of-Pocket Responsibility(does not include prescription drugs)
$3,400 annually
Inpatient Hospital Coverage1 $0 / day for days 1-5$0 / day for days 6-90
Outpatient Hospital Coverage1 Ambulatory Surgical Center: $0 copayOutpatient Hospital: $0 copay
Doctor Visits(Primary and Specialist)
Primary Care Physician visit: $0 copaySpecialist visit: $0 copay
Preventive Care $0 copay
Emergency Care $0 copay
Urgently Needed Care $0 copay
Diagnostic Services / Labs / Imaging1
Diagnostic radiology services (such as MRIs, CT scans): 0% coinsuranceDiagnostic tests and procedures: $0 copayLab services: $0 copayOutpatient x-rays: $0 copayTherapeutic radiology services (such as radiation treatment for cancer):0% coinsurance
1May require prior authorization
Eon Deluxe (HMO SNP)SUMMARY OF BENEFITS
Benefits Eon Deluxe / Health Benefits
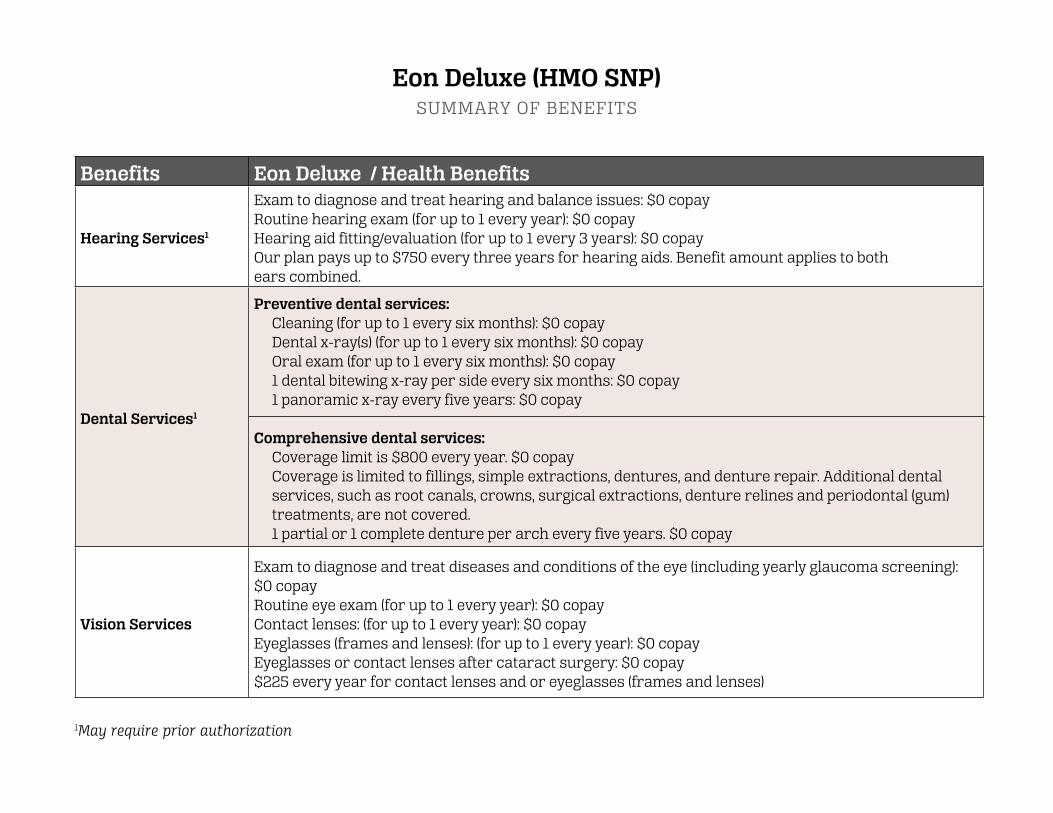
Hearing Services1
Exam to diagnose and treat hearing and balance issues: $0 copayRoutine hearing exam (for up to 1 every year): $0 copayHearing aid fitting/evaluation (for up to 1 every 3 years): $0 copayOur plan pays up to $750 every three years for hearing aids. Benefit amount applies to bothears combined.
Dental Services1
Preventive dental services:Cleaning (for up to 1 every six months): $0 copayDental x-ray(s) (for up to 1 every six months): $0 copayOral exam (for up to 1 every six months): $0 copay1 dental bitewing x-ray per side every six months: $0 copay1 panoramic x-ray every five years: $0 copay
Comprehensive dental services:Coverage limit is $800 every year. $0 copayCoverage is limited to fillings, simple extractions, dentures, and denture repair. Additional dental services, such as root canals, crowns, surgical extractions, denture relines and periodontal (gum) treatments, are not covered.1 partial or 1 complete denture per arch every five years. $0 copay
Vision Services
Exam to diagnose and treat diseases and conditions of the eye (including yearly glaucoma screening): $0 copay Routine eye exam (for up to 1 every year): $0 copayContact lenses: (for up to 1 every year): $0 copayEyeglasses (frames and lenses): (for up to 1 every year): $0 copayEyeglasses or contact lenses after cataract surgery: $0 copay$225 every year for contact lenses and or eyeglasses (frames and lenses)
1May require prior authorization
Eon Deluxe (HMO SNP)SUMMARY OF BENEFITS

Benefits Eon Deluxe / Health Benefits
Mental Health Services1
Inpatient:$0 / Day for Days 1-5$0 / Day for Days 6-90
Outpatient:Group therapy visit: $0 copayIndividual therapy visit: $0 copay
Skilled Nursing Facility (SNF)1$0 / Day for Days 1-20$0 / Day for Days 21-100
Physical Therapy Facility1 Physical therapy visit: $0 copay
Ambulance1 $0 copay
Transportation $0 copay / 30 one-way trips
Medicare Part B drugs1 $0 copay
1May require prior authorization
Eon Deluxe (HMO SNP)SUMMARY OF BENEFITS

Benefits Eon Deluxe / Prescription Drug Benefits
Initial Coverage Retail
For generic drugs (including brand drugs treated as generic), either$0 copay / $1.25 copay / $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay / $8.35 copay
Coverage Gap
For generic drugs (including brand drugs treated as generic), either$0 copay / $1.25 copay / $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay / $8.35 copay
Catastophic Coverage
For generic (including brand drugs treated as generic):$0 copay
For all other drugs:$0 copay
1May require prior authorization
Eon Deluxe (HMO SNP)SUMMARY OF BENEFITS
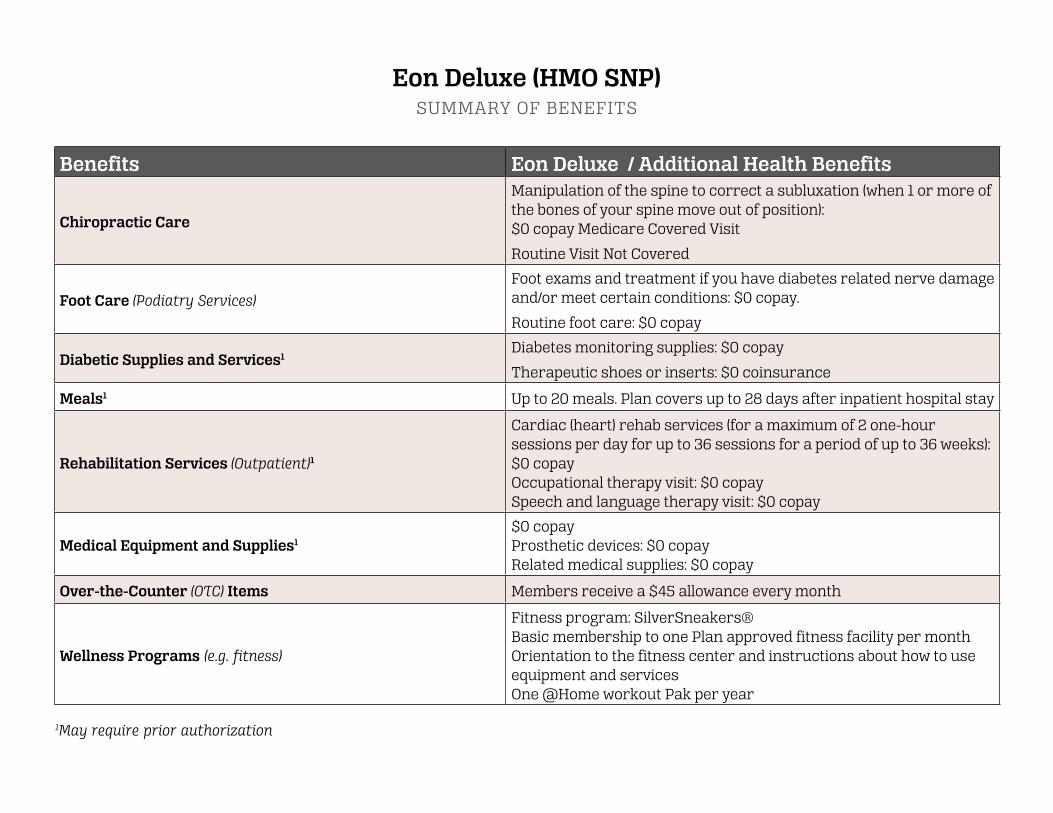
Benefits Eon Deluxe / Additional Health Benefits
Chiropractic Care
Manipulation of the spine to correct a subluxation (when 1 or more of the bones of your spine move out of position):$0 copay Medicare Covered Visit
Routine Visit Not Covered
Foot Care (Podiatry Services)Foot exams and treatment if you have diabetes related nerve damage and/or meet certain conditions: $0 copay.
Routine foot care: $0 copay
Diabetic Supplies and Services1Diabetes monitoring supplies: $0 copay
Therapeutic shoes or inserts: $0 coinsurance
Meals1 Up to 20 meals. Plan covers up to 28 days after inpatient hospital stay
Rehabilitation Services (Outpatient)1
Cardiac (heart) rehab services (for a maximum of 2 one-hour sessions per day for up to 36 sessions for a period of up to 36 weeks): $0 copayOccupational therapy visit: $0 copaySpeech and language therapy visit: $0 copay
Medical Equipment and Supplies1
$0 copayProsthetic devices: $0 copayRelated medical supplies: $0 copay
Over-the-Counter (OTC) Items Members receive a $45 allowance every month
Wellness Programs (e.g. fitness)
Fitness program: SilverSneakers®Basic membership to one Plan approved fitness facility per monthOrientation to the fitness center and instructions about how to use equipment and servicesOne @Home workout Pak per year
1May require prior authorization
Eon Deluxe (HMO SNP)SUMMARY OF BENEFITS

Eon Deluxe (HMO SNP)STATEMENT OF MEDICAID BENEFITS AND COST SHARING PROTECTIONS
Eligibility
Eon Deluxe (HMO SNP) The Eon Deluxe Plan is available to anyone with both Medicare Parts A and B and who receives Medical Assistance from the state Medicaid program to cover Medicare cost-sharing.
• Eon Deluxe (HMO SNP) members with Full benefit Medicaid status (Full Benefit Dual Eligible (FBDE), Qualified Medicare Beneficiary (QMB), Qualified Medicare Beneficiary Plus (QMB +), and Specified Low-Income Medicare Beneficiary Plus (SLMB +) are covered by the state Medicaid program for their Medicare cost sharing.
• Eon Deluxe (HMO SNP) plan with full Medicaid coverage are enrolled in the State Medicaid program that pays their Medicare cost sharing. These members are also eligible to receive additional Medicaid benefits describe below.
Cost Sharing and Cost-sharing Protection for All MembersIn the Eon Deluxe plan, the state Medicaid program pays the cost sharing for Medicare-covered medical services you receive. You pay no cost sharing for the Medicare-covered benefits described in the Covered Medical and Hospital Benefits section of this Summary of Benefits. You will pay small copayments for prescriptions covered under the Medicare Part D prescription drug benefit. When you receive health services, the provider should only bill Eon Deluxe (HMO SNP) or the state Medicaid program for the cost of those services and cost-sharing amounts. The provider should not bill you for services or cost sharing.
If you receive care from a non-contracted provider, the provider may not understand Eon Deluxe or these billing rules. If you receive a bill from a provider for Medicare-covered services, please notify Member Services so we can help you.
Please see chapter 7 of your Eon Deluxe Evidence of Coverage for more information.
The benefits described below are covered by Medicaid. The benefits described in the Covered Medical and Hospital Benefits section of the Summary of Benefits are covered by Medicare. For each benefit listed below, you can see what your state Medicaid covers and what our plan covers. What you pay for covered services may depend on your level of Medicaid eligibility.

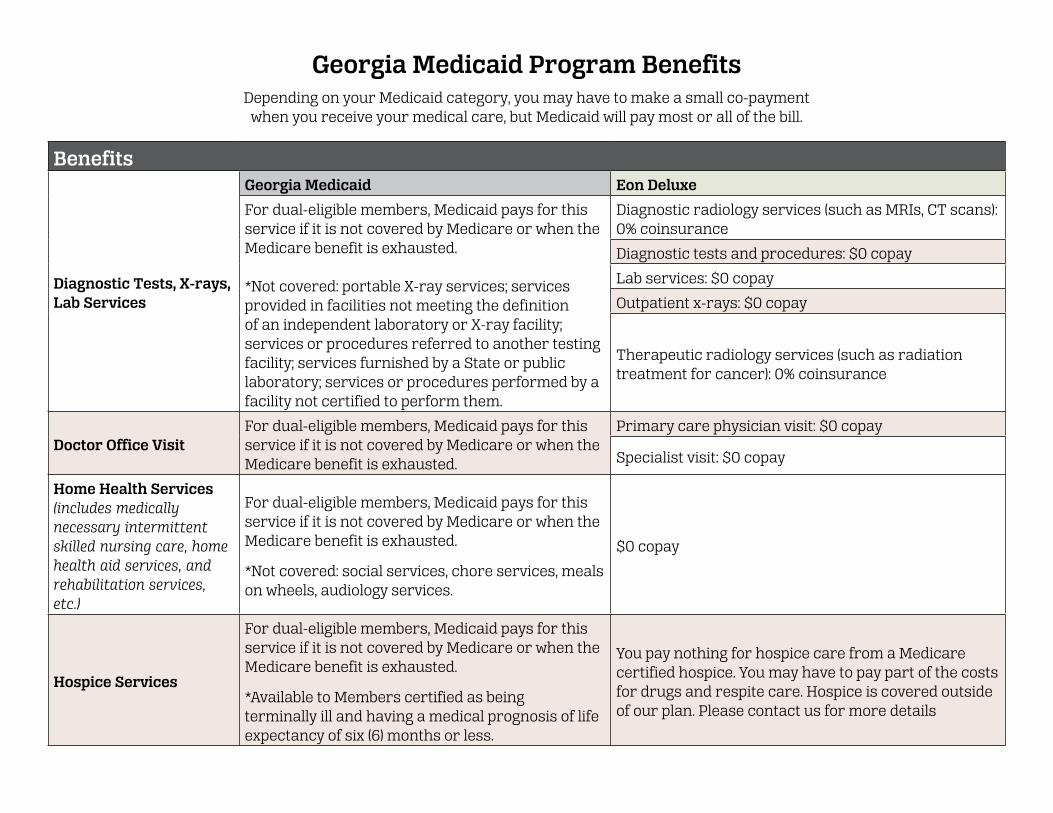
Georgia Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Ambulance Services
Georgia Medicaid Eon Deluxe
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
$0 copay
Ambulatory Surgical Services
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
Ambulatory surgical center: $0 copay
Dental Services
Medicaid covers certain emergency dental care for adults.
Preventive dental care, fillings and oral surgery for children
Preventive dental services: Cleaning (for up to 1 every six months)$0 copay -Dental x-ray(s) (for up to 1 every six months)$0 copay -Oral exam (for up to 1 every six months) $0 copay -1 dental bitewing x-ray per side every six months$0 copay -1 panoramic x-ray every five years: $0 copay
Comprehensive dental services coverage limit is $800 every year. $0 copay
• Coverage is limited to fillings, simple extractions, dentures, and denture repair. Additional dental services, such as root canals, crowns, surgical extractions, denture relines and periodontal (gum) treatments, are not covered.
• 1 partial or 1 complete denture per arch every five years: $0 copay
Georgia Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Diagnostic Tests, X-rays, Lab Services
Georgia Medicaid Eon Deluxe
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
*Not covered: portable X-ray services; services provided in facilities not meeting the definition of an independent laboratory or X-ray facility; services or procedures referred to another testing facility; services furnished by a State or public laboratory; services or procedures performed by a facility not certified to perform them.
Diagnostic radiology services (such as MRIs, CT scans):0% coinsurance
Diagnostic tests and procedures: $0 copay
Lab services: $0 copay
Outpatient x-rays: $0 copay
Therapeutic radiology services (such as radiation treatment for cancer): 0% coinsurance
Doctor Office VisitFor dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
Primary care physician visit: $0 copay
Specialist visit: $0 copay
Home Health Services (includes medically necessary intermittent skilled nursing care, home health aid services, and rehabilitation services, etc.)
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
*Not covered: social services, chore services, meals on wheels, audiology services.
$0 copay
Hospice Services
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
*Available to Members certified as being terminally ill and having a medical prognosis of life expectancy of six (6) months or less.
You pay nothing for hospice care from a Medicare certified hospice. You may have to pay part of the costs for drugs and respite care. Hospice is covered outside of our plan. Please contact us for more details
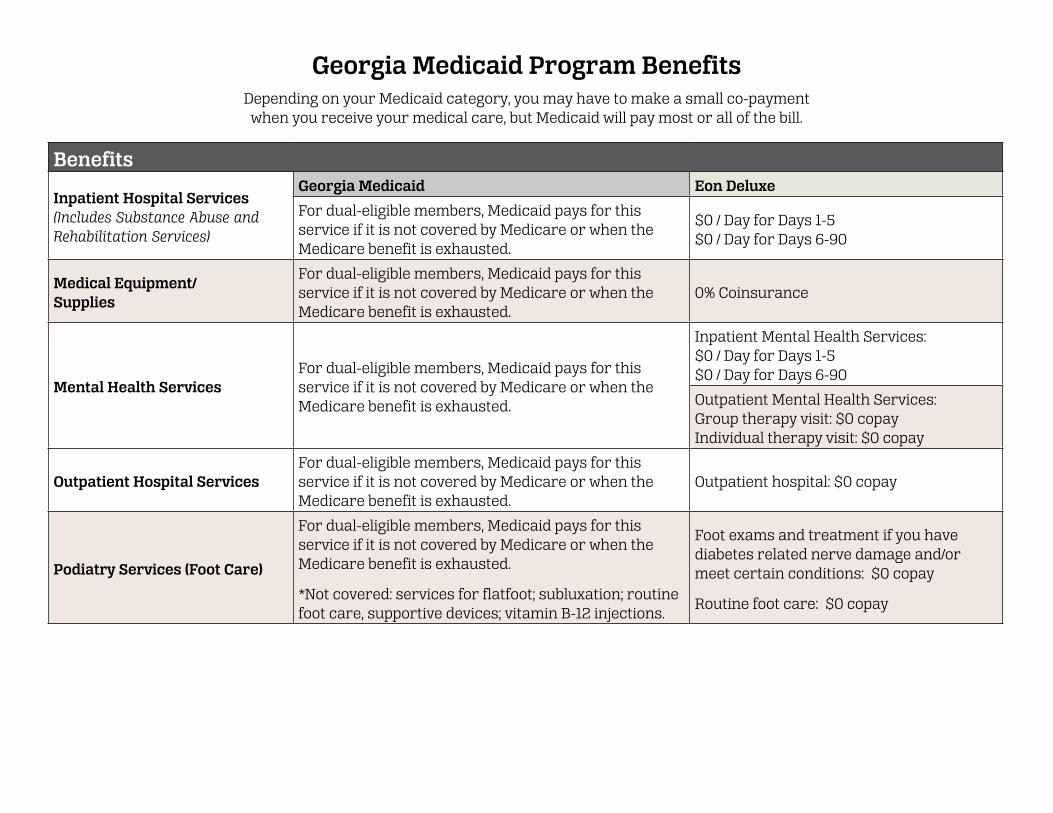
Georgia Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Inpatient Hospital Services (Includes Substance Abuse and Rehabilitation Services)
Georgia Medicaid Eon Deluxe
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
$0 / Day for Days 1-5$0 / Day for Days 6-90
Medical Equipment/Supplies
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
0% Coinsurance
Mental Health ServicesFor dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
Inpatient Mental Health Services:$0 / Day for Days 1-5$0 / Day for Days 6-90
Outpatient Mental Health Services:Group therapy visit: $0 copayIndividual therapy visit: $0 copay
Outpatient Hospital ServicesFor dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
Outpatient hospital: $0 copay
Podiatry Services (Foot Care)
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
*Not covered: services for flatfoot; subluxation; routine foot care, supportive devices; vitamin B-12 injections.
Foot exams and treatment if you have diabetes related nerve damage and/or meet certain conditions: $0 copay
Routine foot care: $0 copay

Georgia Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Prescription Drugs
Georgia Medicaid Eon Deluxe
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
*Not covered: certain outpatient drugs pursuant to Section 1927(d) of the Social Security Act. Additionally, certain over the counter (OTC) drugs must be included, pursuant to the Georgia State Policies and Procedures Manual.
Initial CoverageRetail:
Mail Order:
Coverage Gap:
Catastrophic Coverage:
Skilled NursingFacility (In a Medicare-certified Skilled Nursing Facility)
For dual-eligible members, Medicaid pays for this service if it is not covered by Medicare or when the Medicare benefit is exhausted.
$0 / Day for Days 1-20$0 / Day for Days 21-100
Non-Emergency Transportation (NET)
Medicaid covers NET emergency transportation as medically necessary.
$0 copay / 30 one-way trips
For generic drugs (including brand drugs treated as generic), either: $0 copay / $1.25 copay/ $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay / $8.35 copay
For generic drugs (including brand drugs treated as generic), either: $0 copay / $1.25 copay / $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay / $8.35 copay
For generic drugs (including brand drugs treated as generic), either: $0 copay / $1.25 copay/ $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay/ $8.35 copay
Not Covered

Georgia Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Vision Services
Georgia Medicaid Eon Deluxe
Medically necessary diagnostic services may be covered. Ser-vices may only be covered if per-formed for medical reasons and not for refractive purposes for members twenty-one (21) years of age or older.
Exam to diagnose and treat diseases and conditions of the eye: $0 copay
Glaucoma Screening: $0 copay
Routine eye exam (for up to 1 every year): $0 copay
Contact lenses: (for up to 1 every year): $0 copayEyeglasses (frames and lenses): (for up to 1 every year): $0 copayEyeglasses or contact lenses after cataract surgery: $0 copay
$225 every year for contact lenses and or eyeglasses (frames and lenses).

South Carolina Medicaid Program Statement of Understanding
Within limits, Medicaid will pay for services that are medically necessary.For Medicaid payment purposes, the following definitions apply:
• Children - birth through 20 years of age• Adults - 21 years of age and older
Co-payments - The South Carolina Medicaid program requires many beneficiaries to pay a small part of their medical bill for some services called a co-payment. Certain groups do not pay co-payments for the medical services they receive: Children, Pregnant Women, People in a Nursing Home, People receiving Home and Community Based Waiver Services, and People receiving Family Planning.

South Carolina Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
AmbulanceServices
South Carolina Medicaid Eon Deluxe
Medicaid covers ambulance services. Copayment may apply.
$0 copay
DentalServices
Medicaid covers dental services. Copayment may apply.
Preventive dental services: Cleaning (for up to 1 every six months)$0 copay - Dental x-ray(s) (for up to 1 every six months)$0 copay - Oral exam (for up to 1 every six months) $0 copay - 1 dental bitewing x-ray per side every six months$0 copay - 1 panoramic x-ray every five years: $0 copay
Comprehensive dental services:Coverage limit is $800 every year. $0 copayCoverage is limited to fillings, simple extractions, dentures, and denture repair. Additional dental services, such as root canals, crowns, surgical extractions, denture relines and periodontal (gum) treatments, are not covered.1 partial or 1 complete denture per arch every five years.$0 copay

South Carolina Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Diagnostic Tests, X-rays, Lab Services
South Carolina Medicaid Eon Deluxe
Medicaid covers laboratory and x-ray services. Copayment may apply.
Diagnostic radiology services (such as MRIs, CT scans): 0% coinsurance
Diagnostic tests and procedures: $0 copay
Lab services: $0 copay
Outpatient x-rays: $0 copay
Therapeutic radiology services (such as radiation treatment for cancer): 0% coinsurance
Doctor Office VisitMedicaid covers doctor visits. Copayment may apply.
Primary care physician visit: $0 copay
Specialist visit: $0 copay
Emergency Room Services
Medicaid covers emergency room services. Copayment may apply.
$0 copay
Home Health ServicesMedicaid covers home health services. Copayment may apply.
$0 copay
Hospice ServicesMedicaid covers hospice services.Copayment may apply.
You pay nothing for hospice care from a Medicare certified hospice. You may have to pay part of the costs for drugs and respite care. Hospice is covered outside of our plan. Please contact us for more details

South Carolina Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Inpatient Hospital Services
South Carolina Medicaid Eon Deluxe
Medicaid covers inpatient hospital services.Copayment may apply.
$0 / Day for Days 1-5$0 / Day for Days 6-90
Medical Equipment/Supplies
Medicaid covers medical equipment and supplies.Copayment may apply.
0% Coinsurance
Mental Health Services
Medicaid covers mental health services. Copayment may apply.
Inpatient Mental Health Services:$0/Day for Days 1-5$0/Day for Days 6-90
Outpatient Mental Health Services:Group therapy visit: $0 copayIndividual therapy visit: $0 copay
Outpatient Hospital Services
Medicaid covers outpatient hospital services.Copayment may apply.
Outpatient hospital: $0 copay
Outpatient Rehabilitation Services (Physical Therapy, Speech and Language Therapy)
Medicaid covers outpatient rehabilitation services. Copayment may apply.
Physical therapy visit: $0 copay
Speech and language therapy visit: $0 copay
Outpatient Substance Abuse Services
Medicaid covers outpatient substance abuse services. Copayment may apply.
Outpatient group therapy visit: $0 copayOutpatient individual therapy visit: $0 copay
Podiatry Services (Foot Care)
Medicaid covers podiatry services. Copayment may apply.
Foot exams and treatment if you have diabetes related nerve damage and/or meet certain conditions: $0 copayRoutine foot care: $0 copay

South Carolina Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
PrescriptionDrugs
South Carolina Medicaid Eon Deluxe
Medicaid covers prescription drugs (not all drugs are covered). Copayment may apply.
Initial CoverageRetail:
Mail Order:
Coverage Gap:
Catastrophic Coverage:
Skilled NursingFacility
Medicaid covers nursing facility. Copayment may apply.
$0 / Day for Days 1-20$0 / Day for Days 21-100
Non-Emergency Transportation (NET)
Medicaid covers non-emergency transportation services to medical appointments. Copayment may apply.
$0 copay / 30 one-way trips
For generic drugs (including brand drugs treated as generic), either: $0 copay / $1.25 copay / $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay / $8.35 copay
For generic drugs (including brand drugs treated as generic), either: $0 copay / $1.25 copay / $3.35 copay
For all other drugs, either:$0 copay / $3.70 copay / $8.35 copay
For generic drugs (including brand drugs treated as generic), either: $0 copay
For all other drugs: $0 copay
Not Covered

South Carolina Medicaid Program BenefitsDepending on your Medicaid category, you may have to make a small co-payment
when you receive your medical care, but Medicaid will pay most or all of the bill.
Benefits
Vision Services
South Carolina Medicaid Eon Deluxe
Medicaid covers vision services. Copayment may apply.
Exam to diagnose and treat diseases and conditions of the eye: $0 copay
Glaucoma Screening: $0 copay
Routine eye exam (for up to 1 every year): $0 copay
Contact lenses: (for up to 1 every year): $0 copayEyeglasses (frames and lenses): (for up to 1 every year): $0 copayEyeglasses or contact lenses after cataract surgery: $0 copay
$225 every year for contact lenses and or eyeglasses (frames and lenses).

This page intentionally left blank

This information is not a complete description of benefits. Contact the plan for more information. Limitations, copayments and restrictions may apply. Benefits, premiums and/or copayments/coinsurance may change on January 1 of each year. You must continue to pay your Medicare Part B premium – The State pays the Part B premium for full dual members.
Premium, co-pays, co-insurance, and deductibles may vary based on the level of Extra Help you receive. Please contact the plan for further details.
Eon Health complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex.
Current Members: 1-888-906-3889 TTY: 711
Prospective Members: 1-844-895-8643 TTY: 711
Hours of Operation: October 1 – February 14:Seven days a week, 8:00am – 8:00pm EST
February 15 – September 30: Monday through Friday, 8:00am – 8:00pm EST
(You may leave a voicemail Saturday, Sunday and Federal Holidays)

























![Type 8643 - burkert.itII 2 (1) D Ex tb [ia IIIC Da] IIIC T65 °C Db IP65 • IECEx approval: Ex e mb [ia IIC Ga] IIC T4 Gb Ex tb [ia IIIC Da] IIIC T65 °C Db IP65: 8643 - 11: with](https://img.pdfslide.us/doc/110x75/60b0d0f5f954e865755e9b44/type-8643-ii-2-1-d-ex-tb-ia-iiic-da-iiic-t65-c-db-ip65-a-iecex-approval.jpg)


