Embed Size (px)
Citation preview

2018 Plan OverviewGROUPS SIZED 51+

02 ProvidenceHealthPlan.com
Why Choose Providence
Have confidence that you’re partnering with a company that’s financially strong and stable. The state of Oregon
requires insurance carriers to have strong financial reserves so they are positioned to honor commitments to groups and members. Providence Health Plan is proud to exceed the state’s reserve requirement by four times, allowing us to steadfastly serve our members and the greater community.
• A range of quality products and choice of plan designs with broad or tailored provider networks help you better manage health benefit program costs.
• The Option Advantage plan offers four options, so you’re sure to find benefits that are right for your business.
• A full suite of health plans for a complete health benefit program: medical, pharmacy, dental, vision, chiropractic and acupuncture plus many free extras to encourage members to get and stay engaged with their health.
2014 2015 2016 2017 YTD100,000
200,000
300,000
400,000
500,000
600,000
700,000
MEMBERSHIP638,663
MEMBERSHIP638,759
MEMBERSHIP547,070
MEMBERSHIP469,568
We’ve grown steadily in the past four years—in every line of business—allowing us to serve more than 600,000 members throughout Oregon and southwest Washington. Our growth demonstrates that we are doing the right thing—offering the right products—for customers, and offering compassionate, quality care for members.
FINANCIALLY STRONG
GROWING RESPONSIBLY
HIGH-PERFORMING QUALTY PRODUCTS
YEARS
A TRUSTEDPARTNERSERVINGNORTHWESTBUSINESSES FOR

ProvidenceHealthPlan.com 03
MEDICARE 5-STAR QUALITY RATING
4.5 IN 2017
HISTORIC CMS STAR RATING2016: 4.52015: 52014: 5
RECOGNIZED FOR EXCELLENCE
Our quality rating for Providence Medicare Advantage Plans is 4.5 out of 5 stars. We apply the same rigor and quality standards for prevention, chronic condition management, member satisfaction and customer and pharmacy services to all of our product lines.
THE RIGHT CARE TO MANAGE RISING COSTSREADMISSION AVOIDANCE
In 2016, we averaged a 7% readmission rate – 85% better than the national readmission rate.
Best of all – our approach to the right care means that employees are present and healthy at work and our community is healthier.
SUPERIOR, LOCAL SERVICE AND TRUE TO OUR MISSION
We know that excellent, accurate and compassionate service means a better experience for you and your employees:
97.8% 97.2% 99.8%
Of total clean claims are processed within 30 days
Of overall claims are processed accurately – the first time
Of financial payments are accurate
85% BETTER
MANAGING RISING PRESCRIPTION DRUG COSTS
Optimizing care guidelines: We’re optimizing site-of-care guidelines to help curb escalating prescription drug costs. We’re also providing assistance to members to help them adhere to taking medications as prescribed. For example, more than 80% of members who are prescribed medications for a mental health diagnosis take them as prescribed.
Best-in-class generic drug utilization: Our 91% generic drug prescribing rate helps manage rising costs of prescription medications.
04 ProvidenceHealthPlan.com
New for 2018Providence is offering new, innovative products, benefit enhancements, plenty of plan design options and more affordable services as part of the 2018 product lineup – helping deliver benefits that are priced right, meet employers’ business objectives and keep employees healthy and happy.
*Members on HSA plans must first meet the plan’s deductible.
OPTION ADVANTAGE PLANSYOU HAVE FOUR OPTION ADVANTAGE PLANS TO CHOOSE FROM:
• Option Advantage Plan (our base plan)
• Option Advantage Plan A (most similar to Core Advantages)
• Option Advantage Plan B (most similar to Open Option)
• Option Advantage Plan AB (the richest of our Option Advantage plans)
These plans are easy to understand and use. Members have full access to the Providence Signature Network as well as thousands of out-of-network providers.
ENHANCED BENEFITS
• Virtual visits (Express Care Virtual) or Web-direct visits fully covered (in-network only)*
• Express Care clinic visits fully covered*
• New Connect XT plan with additional cost share options
• More generous Allergy Shot and Serums benefit
• Richer in-network Physical Therapy benefit
• Out-of-pocket maximum credit for mid-year new groups
CANOPY PLAN
Canopy plan members receive a $1,000 in-network defined health benefit. It pays for many common health care needs, such as PCP and Alternative Care visits, and Urgent Care and Outpatient Rehabilitative Physical Therapy, all covered in full – no out of pocket costs. For other health care needs, or once a member reaches $1,000 in eligible health care services, standard insurance coverage kicks in and services are subject to deductible and coinsurance.
PREVENTIVE DENTAL PLAN
The Preventive Dental plan is affordable. It offers full coverage for preventive dental services (i.e., teeth cleaning, exams, etc.), which makes the Preventive Dental plan attractive and care easy to access.
ProvidenceHealthPlan.com 05
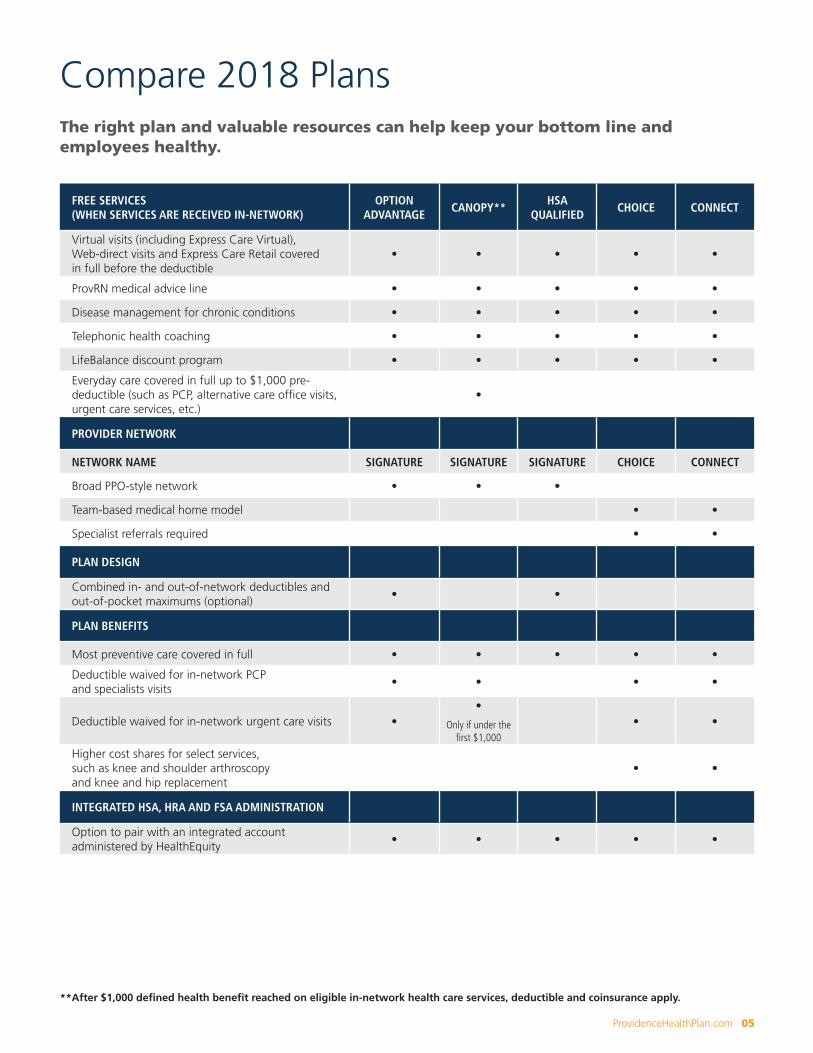
FREE SERVICES (WHEN SERVICES ARE RECEIVED IN-NETWORK)
OPTION ADVANTAGE
CANOPY**HSA
QUALIFIEDCHOICE CONNECT
Virtual visits (including Express Care Virtual), Web-direct visits and Express Care Retail covered in full before the deductible
• • • • •
ProvRN medical advice line • • • • •
Disease management for chronic conditions • • • • •
Telephonic health coaching • • • • •
LifeBalance discount program • • • • •
Everyday care covered in full up to $1,000 pre-deductible (such as PCP, alternative care office visits, urgent care services, etc.)
•
PROVIDER NETWORK
NETWORK NAME SIGNATURE SIGNATURE SIGNATURE CHOICE CONNECT
Broad PPO-style network • • •
Team-based medical home model • •
Specialist referrals required • •
PLAN DESIGN
Combined in- and out-of-network deductibles and out-of-pocket maximums (optional)
• •
PLAN BENEFITS
Most preventive care covered in full • • • • •
Deductible waived for in-network PCP and specialists visits
• • • •
Deductible waived for in-network urgent care visits ••
Only if under the first $1,000
• •
Higher cost shares for select services, such as knee and shoulder arthroscopy and knee and hip replacement
• •
INTEGRATED HSA, HRA AND FSA ADMINISTRATION
Option to pair with an integrated account administered by HealthEquity
• • • • •
The right plan and valuable resources can help keep your bottom line and employees healthy.
Compare 2018 Plans
**After $1,000 defined health benefit reached on eligible in-network health care services, deductible and coinsurance apply.
06 ProvidenceHealthPlan.com
Your Plan is Complemented by these FREE Member Resources
EXPRESS CARE*
Members get quality, on-demand health care from folks who know health, either in person at a clinic or virtually from a computer, tablet or smartphone.
HEALTH COACHING
If enrolled employees or their enrolled dependents are looking for some extra support to meet their health goals, a Providence health coach is available. The optional program offers 12 free visits providing personal support for losing weight, quitting tobacco, managing diabetes or meeting any healthy lifestyle goal.
WELLNESS CENTRAL
This secure wellness hub within myProvidence supports member health goals and employer-specific wellness campaigns and challenges. It includes a personal health assessment, health trackers for challenges and expert health and wellness information, including classes and articles.
WELLNESS DISCOUNTS
Members get discounts on wellness services, such as chiropractic care, acupuncture, massage therapy, vision care, hearing aids and health-related classes.
*Members enrolled in a high-deductible plan (such as Providence HSA Qualified plans)
must first meet the plan’s deductible to access this service for free.

ProvidenceHealthPlan.com 07
myPROVIDENCE
This secure website allows members to get custom benefit information, view plan details and check their claims history. They can also see the cost of care or prescriptions using the cost calculator, so they know the cost of care before receiving it, and find easy-to-understand health education resources.
ProvRN
Members can get free health advice 24/7 from a registered nurse. After-visit summaries are sent to their providers, so the care team is informed about the health incident.
TREATMENT COST ESTIMATOR
Prices vary widely among providers and places of care – even for the same service or procedure. Members have online access to our cost calculator to estimate their specific cost of care before they receive it. Estimates are custom based on a member’s health plan benefits.
MOBILE MEMBER ID CARD
Members have access to their Providence Health Plan member ID card on their smart phone. The Providence member ID card app is available to download from Google Play or the App Store. Search for “Providence E-card.”
LifeBalance
This lifestyle discount program offers members savings on health club memberships, fitness classes, massage therapy, weight-loss programs and recreational, cultural and wellness events, including family activities, movies, travel and more.
08 ProvidenceHealthPlan.com
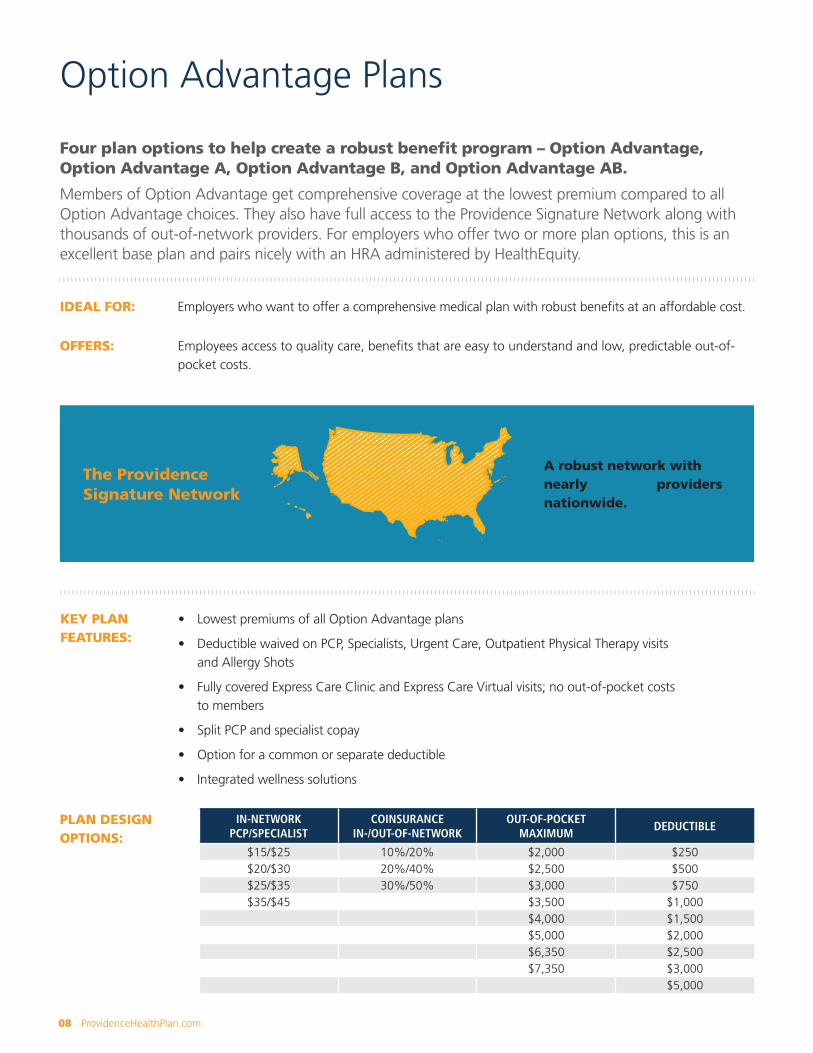
Four plan options to help create a robust benefit program – Option Advantage, Option Advantage A, Option Advantage B, and Option Advantage AB.
Members of Option Advantage get comprehensive coverage at the lowest premium compared to all Option Advantage choices. They also have full access to the Providence Signature Network along with thousands of out-of-network providers. For employers who offer two or more plan options, this is an excellent base plan and pairs nicely with an HRA administered by HealthEquity.
IDEAL FOR: Employers who want to offer a comprehensive medical plan with robust benefits at an affordable cost.
OFFERS: Employees access to quality care, benefits that are easy to understand and low, predictable out-of-pocket costs.
Option Advantage Plans
KEY PLAN FEATURES:
• Lowest premiums of all Option Advantage plans
• Deductible waived on PCP, Specialists, Urgent Care, Outpatient Physical Therapy visits and Allergy Shots
• Fully covered Express Care Clinic and Express Care Virtual visits; no out-of-pocket costs to members
• Split PCP and specialist copay
• Option for a common or separate deductible
• Integrated wellness solutions
PLAN DESIGN OPTIONS:
IN-NETWORK PCP/SPECIALIST
COINSURANCE IN-/OUT-OF-NETWORK
OUT-OF-POCKET MAXIMUM
DEDUCTIBLE
$15/$25 10%/20% $2,000 $250$20/$30 20%/40% $2,500 $500$25/$35 30%/50% $3,000 $750$35/$45 $3,500 $1,000
$4,000 $1,500$5,000 $2,000$6,350 $2,500$7,350 $3,000
$5,000
The Providence Signature Network
A robust network with nearly 1 million providers nationwide.
ProvidenceHealthPlan.com 09
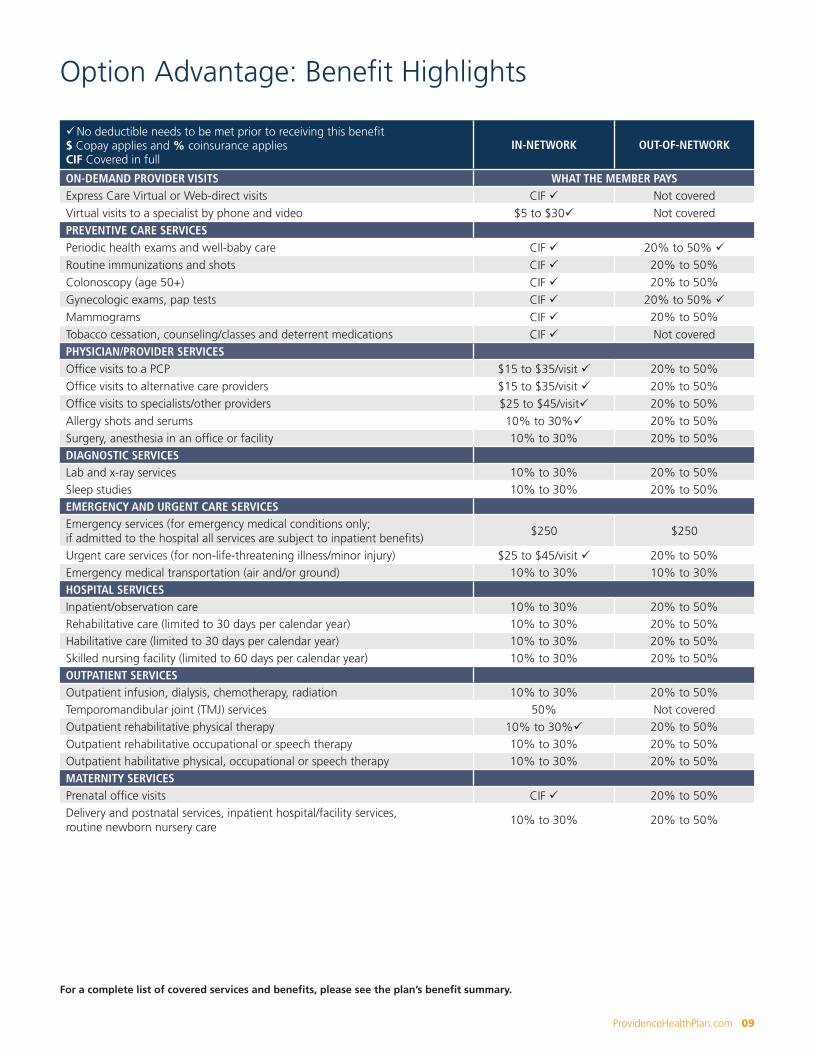
Option Advantage: Benefit Highlights
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredVirtual visits to a specialist by phone and video $5 to $30ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 20% to 50% üRoutine immunizations and shots CIF ü 20% to 50%Colonoscopy (age 50+) CIF ü 20% to 50% Gynecologic exams, pap tests CIF ü 20% to 50% üMammograms CIF ü 20% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP $15 to $35/visit ü 20% to 50% Office visits to alternative care providers $15 to $35/visit ü 20% to 50% Office visits to specialists/other providers $25 to $45/visitü 20% to 50%Allergy shots and serums 10% to 30%ü 20% to 50%Surgery, anesthesia in an office or facility 10% to 30% 20% to 50%DIAGNOSTIC SERVICESLab and x-ray services 10% to 30% 20% to 50%Sleep studies 10% to 30% 20% to 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250 $250
Urgent care services (for non-life-threatening illness/minor injury) $25 to $45/visit ü 20% to 50% Emergency medical transportation (air and/or ground) 10% to 30% 10% to 30%HOSPITAL SERVICESInpatient/observation care 10% to 30% 20% to 50%Rehabilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Habilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Skilled nursing facility (limited to 60 days per calendar year) 10% to 30% 20% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation 10% to 30% 20% to 50%Temporomandibular joint (TMJ) services 50% Not coveredOutpatient rehabilitative physical therapy 10% to 30%ü 20% to 50%Outpatient rehabilitative occupational or speech therapy 10% to 30% 20% to 50%Outpatient habilitative physical, occupational or speech therapy 10% to 30% 20% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 20% to 50%Delivery and postnatal services, inpatient hospital/facility services, routine newborn nursery care
10% to 30% 20% to 50%
For a complete list of covered services and benefits, please see the plan’s benefit summary.
10 ProvidenceHealthPlan.com
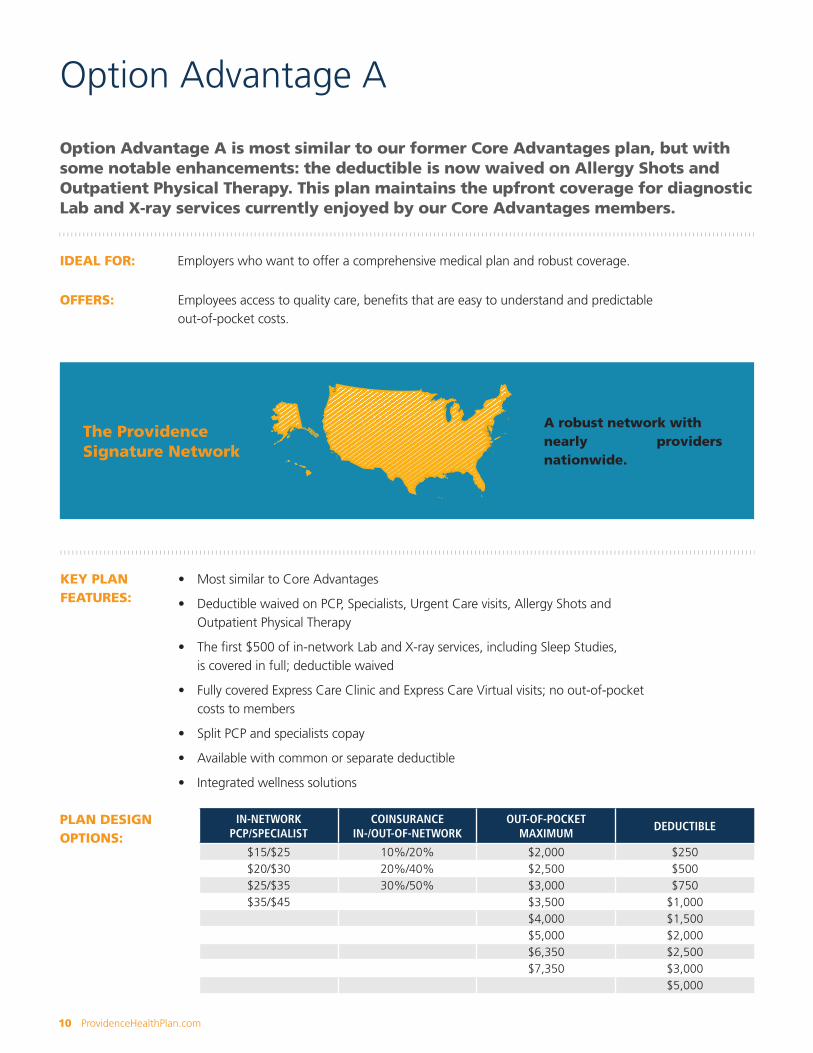
Option Advantage A is most similar to our former Core Advantages plan, but with some notable enhancements: the deductible is now waived on Allergy Shots and Outpatient Physical Therapy. This plan maintains the upfront coverage for diagnostic Lab and X-ray services currently enjoyed by our Core Advantages members.
IDEAL FOR: Employers who want to offer a comprehensive medical plan and robust coverage.
OFFERS: Employees access to quality care, benefits that are easy to understand and predictable out-of-pocket costs.
Option Advantage A
KEY PLAN FEATURES:
• Most similar to Core Advantages
• Deductible waived on PCP, Specialists, Urgent Care visits, Allergy Shots and Outpatient Physical Therapy
• The first $500 of in-network Lab and X-ray services, including Sleep Studies, is covered in full; deductible waived
• Fully covered Express Care Clinic and Express Care Virtual visits; no out-of-pocket costs to members
• Split PCP and specialists copay
• Available with common or separate deductible
• Integrated wellness solutions
PLAN DESIGN OPTIONS:
IN-NETWORK PCP/SPECIALIST
COINSURANCE IN-/OUT-OF-NETWORK
OUT-OF-POCKET MAXIMUM
DEDUCTIBLE
$15/$25 10%/20% $2,000 $250$20/$30 20%/40% $2,500 $500$25/$35 30%/50% $3,000 $750$35/$45 $3,500 $1,000
$4,000 $1,500$5,000 $2,000$6,350 $2,500$7,350 $3,000
$5,000
The Providence Signature Network
A robust network with nearly 1 million providers nationwide.
ProvidenceHealthPlan.com 11
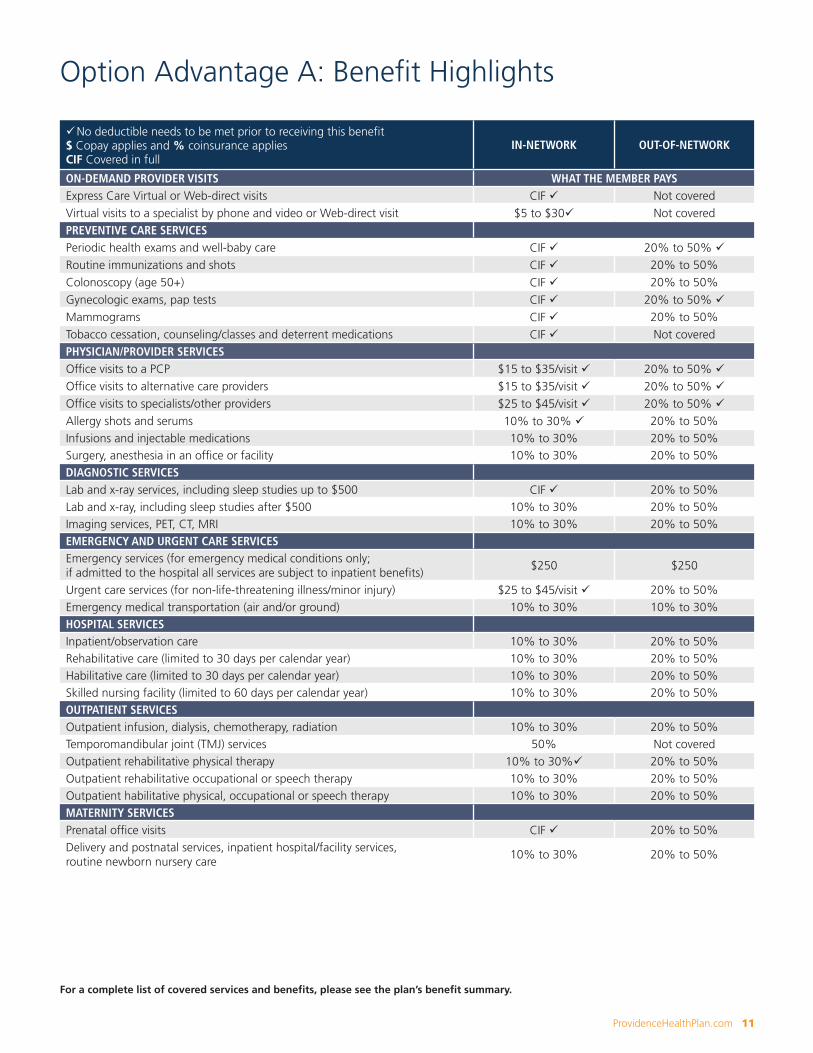
Option Advantage A: Benefit Highlights
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredVirtual visits to a specialist by phone and video or Web-direct visit $5 to $30ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 20% to 50% üRoutine immunizations and shots CIF ü 20% to 50%Colonoscopy (age 50+) CIF ü 20% to 50% Gynecologic exams, pap tests CIF ü 20% to 50% üMammograms CIF ü 20% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP $15 to $35/visit ü 20% to 50% üOffice visits to alternative care providers $15 to $35/visit ü 20% to 50% üOffice visits to specialists/other providers $25 to $45/visit ü 20% to 50% üAllergy shots and serums 10% to 30% ü 20% to 50%Infusions and injectable medications 10% to 30% 20% to 50%Surgery, anesthesia in an office or facility 10% to 30% 20% to 50%DIAGNOSTIC SERVICESLab and x-ray services, including sleep studies up to $500 CIF ü 20% to 50%Lab and x-ray, including sleep studies after $500 10% to 30% 20% to 50%Imaging services, PET, CT, MRI 10% to 30% 20% to 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250 $250
Urgent care services (for non-life-threatening illness/minor injury) $25 to $45/visit ü 20% to 50% Emergency medical transportation (air and/or ground) 10% to 30% 10% to 30%HOSPITAL SERVICESInpatient/observation care 10% to 30% 20% to 50%Rehabilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Habilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Skilled nursing facility (limited to 60 days per calendar year) 10% to 30% 20% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation 10% to 30% 20% to 50%Temporomandibular joint (TMJ) services 50% Not coveredOutpatient rehabilitative physical therapy 10% to 30%ü 20% to 50%Outpatient rehabilitative occupational or speech therapy 10% to 30% 20% to 50%Outpatient habilitative physical, occupational or speech therapy 10% to 30% 20% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 20% to 50%Delivery and postnatal services, inpatient hospital/facility services, routine newborn nursery care
10% to 30% 20% to 50%
For a complete list of covered services and benefits, please see the plan’s benefit summary.

12 ProvidenceHealthPlan.com
A comprehensive plan on its own, Option Advantage B is most similar to our former Open Option plan, but with some notable enhancements: the deductible is now waived on Allergy Shots and Outpatient Physical Therapy. Plan members have full access to the Providence Signature Network along with thousands of out-of-network providers. Employers also offer it as a companion buy-up plan.
IDEAL FOR: Employers who want to offer a comprehensive medical plan and robust coverage with generous benefits.
OFFERS: Employees access to quality care, generous benefits that are easy to understand and predictable out-of-pocket costs.
Option Advantage B
KEY PLAN FEATURES:
• Most similar to Open Option
• Deductible waived on many services, such as PCP, Specialists, ER, Lab and X-ray, Imaging Services (PET, CT, MRI), Urgent Care, Allergy Shots, Routine Immunizations, Outpatient Physical Therapy
• Deductible waived on in-network delivery, postnatal and routine newborn nursery care; copay applies and delivery is 10 x PCP copay
• Fully covered Express Care Clinic and Express Care Virtual visits; no out-of-pocket costs to members
• Option for a common or separate deductible
• Integrated wellness solutions
PLAN DESIGN OPTIONS:
IN-NETWORK PCP/SPECIALIST
COINSURANCE IN-/OUT-OF-NETWORK
OUT-OF-POCKET MAXIMUM
DEDUCTIBLE
$15/$15 10%/20% $2,000 $250$20/$20 20%/40% $2,500 $500$25/$25 30%/50% $3,000 $750$35/$35 $3,500 $1,000
$4,000 $1,500$5,000 $2,000$6,350 $2,500$7,350 $3,000
$5,000
The Providence Signature Network
A robust network with nearly 1 million providers nationwide.
ProvidenceHealthPlan.com 13
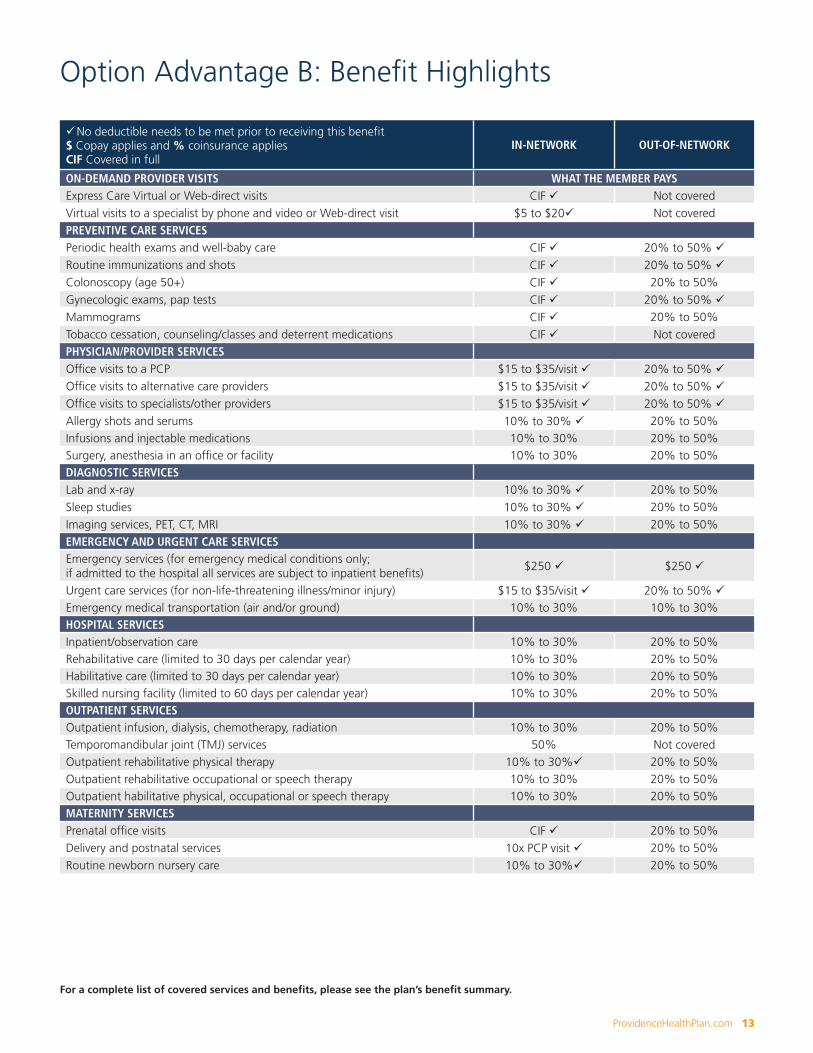
Option Advantage B: Benefit Highlights
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredVirtual visits to a specialist by phone and video or Web-direct visit $5 to $20ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 20% to 50% üRoutine immunizations and shots CIF ü 20% to 50% üColonoscopy (age 50+) CIF ü 20% to 50% Gynecologic exams, pap tests CIF ü 20% to 50% üMammograms CIF ü 20% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP $15 to $35/visit ü 20% to 50% üOffice visits to alternative care providers $15 to $35/visit ü 20% to 50% üOffice visits to specialists/other providers $15 to $35/visit ü 20% to 50% üAllergy shots and serums 10% to 30% ü 20% to 50%Infusions and injectable medications 10% to 30% 20% to 50%Surgery, anesthesia in an office or facility 10% to 30% 20% to 50%DIAGNOSTIC SERVICESLab and x-ray 10% to 30% ü 20% to 50%Sleep studies 10% to 30% ü 20% to 50%Imaging services, PET, CT, MRI 10% to 30% ü 20% to 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250 ü $250 ü
Urgent care services (for non-life-threatening illness/minor injury) $15 to $35/visit ü 20% to 50% üEmergency medical transportation (air and/or ground) 10% to 30% 10% to 30%HOSPITAL SERVICESInpatient/observation care 10% to 30% 20% to 50%Rehabilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Habilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Skilled nursing facility (limited to 60 days per calendar year) 10% to 30% 20% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation 10% to 30% 20% to 50%Temporomandibular joint (TMJ) services 50% Not coveredOutpatient rehabilitative physical therapy 10% to 30%ü 20% to 50%Outpatient rehabilitative occupational or speech therapy 10% to 30% 20% to 50%Outpatient habilitative physical, occupational or speech therapy 10% to 30% 20% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 20% to 50%Delivery and postnatal services 10x PCP visit ü 20% to 50%Routine newborn nursery care 10% to 30%ü 20% to 50%
For a complete list of covered services and benefits, please see the plan’s benefit summary.

14 ProvidenceHealthPlan.com
Option Advantage AB is our most robust plan. This premier offering combines the richest benefits of Option Advantage A and Option Advantage B, including the deductible waived on PCP, Specialist, ER, Urgent Care, Allergy Shots, Outpatient Physical Therapy and Lab and X-ray (including Imaging Services). Plan members have full access to the Providence Signature Network along with thousands of out-of-network providers.
IDEAL FOR: Employers who want to offer a comprehensive medical plan with rich benefits.
OFFERS: Employees access to quality care, increased benefits that are easy to understand and predictable out-of-pocket costs.
Option Advantage AB
KEY PLAN FEATURES:
• A premier plan with comprehensive coverage and enriched benefits
• Deductible waived on many services, such as PCP, Specialists, ER, Lab and X-ray, Imaging Services (PET, CT, MRI) Urgent Care, Allergy Shots, Routine Immunizations, Outpatient Physical Therapy
• The first $500 of in-network Lab and X-ray services, including Sleep Studies, is covered in full; deductible waived
• Deductible waived on in-network delivery, postnatal and routine newborn nursery care; copay applies and delivery is 10 x PCP copay
• Fully covered Express Care Clinic and Express Care Virtual visits; no out-of-pocket costs to members
• Option for a common or separate deductible
• Integrated wellness solutions
PLAN DESIGN OPTIONS:
IN-NETWORK PCP/SPECIALIST
COINSURANCE IN-/OUT-OF-NETWORK
OUT-OF-POCKET MAXIMUM
DEDUCTIBLE
$15/$15 10%/20% $2,000 $250$20/$20 20%/40% $2,500 $500$25/$25 30%/50% $3,000 $750$35/$35 $3,500 $1,000
$4,000 $1,500$5,000 $2,000$6,350 $2,500$7,350 $3,000
$5,000
The Providence Signature Network
A robust network with nearly 1 million providers nationwide.
ProvidenceHealthPlan.com 15
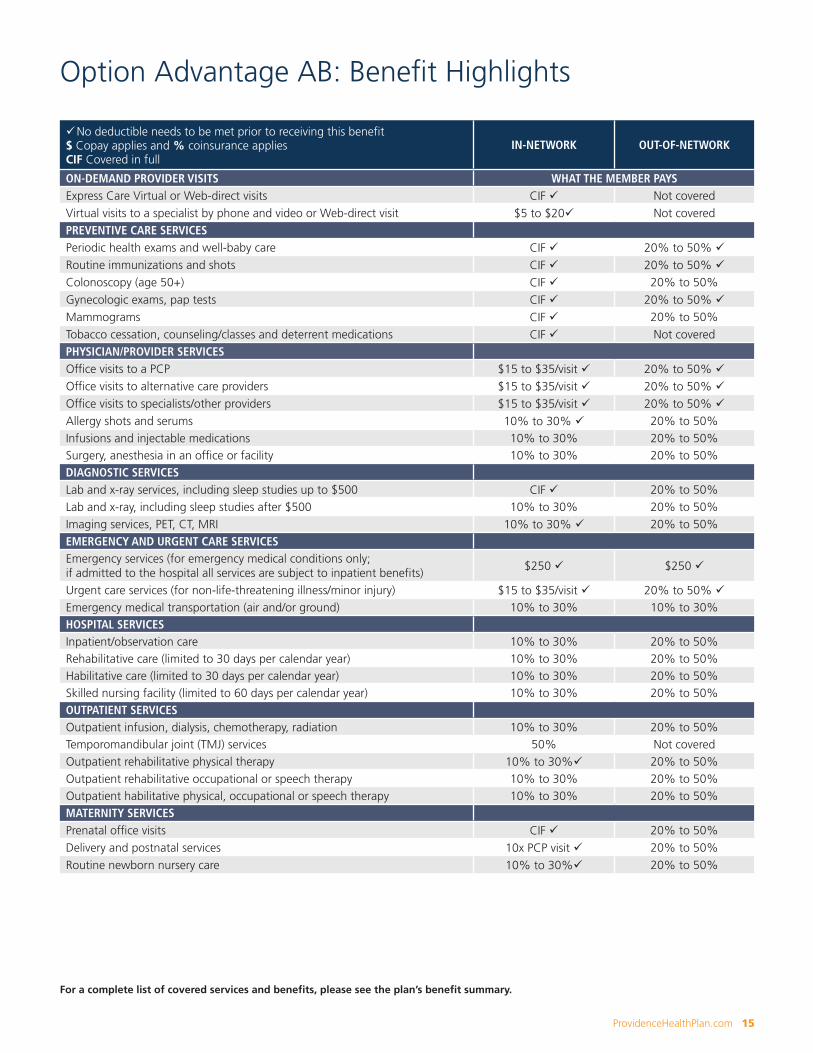
Option Advantage AB: Benefit Highlights
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredVirtual visits to a specialist by phone and video or Web-direct visit $5 to $20ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 20% to 50% üRoutine immunizations and shots CIF ü 20% to 50% üColonoscopy (age 50+) CIF ü 20% to 50% Gynecologic exams, pap tests CIF ü 20% to 50% üMammograms CIF ü 20% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP $15 to $35/visit ü 20% to 50% üOffice visits to alternative care providers $15 to $35/visit ü 20% to 50% üOffice visits to specialists/other providers $15 to $35/visit ü 20% to 50% üAllergy shots and serums 10% to 30% ü 20% to 50%Infusions and injectable medications 10% to 30% 20% to 50%Surgery, anesthesia in an office or facility 10% to 30% 20% to 50%DIAGNOSTIC SERVICESLab and x-ray services, including sleep studies up to $500 CIF ü 20% to 50%Lab and x-ray, including sleep studies after $500 10% to 30% 20% to 50%Imaging services, PET, CT, MRI 10% to 30% ü 20% to 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250 ü $250 ü
Urgent care services (for non-life-threatening illness/minor injury) $15 to $35/visit ü 20% to 50% üEmergency medical transportation (air and/or ground) 10% to 30% 10% to 30%HOSPITAL SERVICESInpatient/observation care 10% to 30% 20% to 50%Rehabilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Habilitative care (limited to 30 days per calendar year) 10% to 30% 20% to 50%Skilled nursing facility (limited to 60 days per calendar year) 10% to 30% 20% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation 10% to 30% 20% to 50%Temporomandibular joint (TMJ) services 50% Not coveredOutpatient rehabilitative physical therapy 10% to 30%ü 20% to 50%Outpatient rehabilitative occupational or speech therapy 10% to 30% 20% to 50%Outpatient habilitative physical, occupational or speech therapy 10% to 30% 20% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 20% to 50%Delivery and postnatal services 10x PCP visit ü 20% to 50%Routine newborn nursery care 10% to 30%ü 20% to 50%
For a complete list of covered services and benefits, please see the plan’s benefit summary.

16 ProvidenceHealthPlan.com
HSA Qualified plans are high-deductible health plans that encourage enrolled employees to take accountability for their health and health care spending. These plans offer tax advantages for employers and enrolled employees.
IDEAL FOR: Employers seeking to manage health care costs and engage enrolled employees in taking accountability for managing their personal health care costs.
OFFERS: Robust coverage, virtually unlimited provider choice and individual savings opportunities. HSA plans encourage employees to become smart health care consumers when paired with a tax-advantaged savings account because members become more aware of how much they pay for care.
ADVANTAGES: • Optional partnership with HealthEquity, the leading health savings and reimbursement accounts provider since 2002 with more than 27,000 employers served
• Funds in a health savings account are set aside pre-tax
• Employees can use funds to pay for eligible health expenses or save them for future health care needs
• Option for employers to contribute to HSA accounts – a tax deduction for companies
KEY PLAN FEATURES:
• Affordable monthly premiums
• Employee engagement in managing health care costs
• Tax-advantaged savings for employees when paired with an HSA account
• Flexible plan designs
• Simple payment for qualified medical expenses with HealthEquity debit card
• Fully covered Express Care Clinic and Express Care Virtual visits after deductible
• Integrated wellness solutions
PLAN DESIGN OPTIONS:
IN-NETWORK COINSURANCE PCP/SPECIALIST
IN-NETWORK OUT-OF-POCKET MAXIMUM
IN-NETWORK DEDUCTIBLE
0%/0%* $3,000 $1,50020%/40% $4,000 $2,00050%/50% $5,500 $2,500
$6,650 $3,000$3,500$4,000$5,500$6,650
HSA Qualified Plans
*Option available when deductible and out-of-pocket maximum match
The Providence Signature Network
A robust network with nearly 1 million providers nationwide.
ProvidenceHealthPlan.com 17
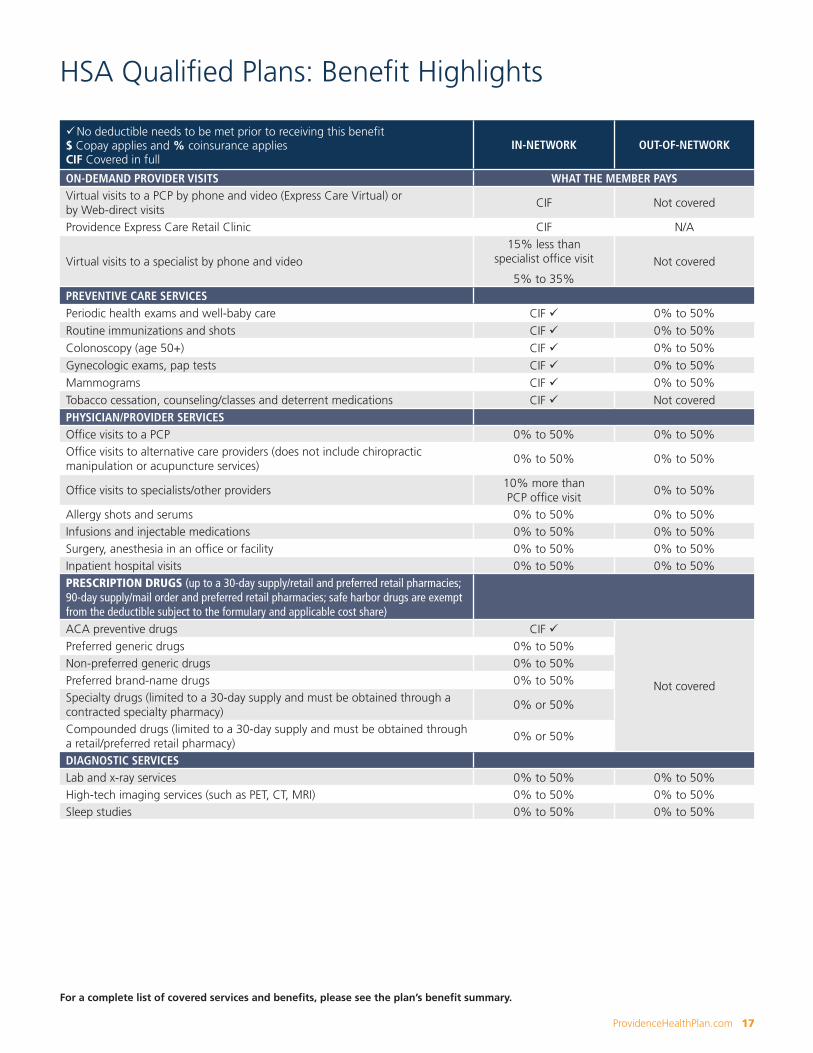
HSA Qualified Plans: Benefit Highlights
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSVirtual visits to a PCP by phone and video (Express Care Virtual) or by Web-direct visits
CIF Not covered
Providence Express Care Retail Clinic CIF N/A
Virtual visits to a specialist by phone and video15% less than
specialist office visit
5% to 35%Not covered
PREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 0% to 50%Routine immunizations and shots CIF ü 0% to 50%Colonoscopy (age 50+) CIF ü 0% to 50%Gynecologic exams, pap tests CIF ü 0% to 50%Mammograms CIF ü 0% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP 0% to 50% 0% to 50%Office visits to alternative care providers (does not include chiropractic manipulation or acupuncture services)
0% to 50% 0% to 50%
Office visits to specialists/other providers10% more than PCP office visit
0% to 50%
Allergy shots and serums 0% to 50% 0% to 50%Infusions and injectable medications 0% to 50% 0% to 50%Surgery, anesthesia in an office or facility 0% to 50% 0% to 50%Inpatient hospital visits 0% to 50% 0% to 50%PRESCRIPTION DRUGS (up to a 30-day supply/retail and preferred retail pharmacies; 90-day supply/mail order and preferred retail pharmacies; safe harbor drugs are exempt from the deductible subject to the formulary and applicable cost share)ACA preventive drugs CIF ü
Not covered
Preferred generic drugs 0% to 50%Non-preferred generic drugs 0% to 50%Preferred brand-name drugs 0% to 50%Specialty drugs (limited to a 30-day supply and must be obtained through a contracted specialty pharmacy)
0% or 50%
Compounded drugs (limited to a 30-day supply and must be obtained through a retail/preferred retail pharmacy)
0% or 50%
DIAGNOSTIC SERVICESLab and x-ray services 0% to 50% 0% to 50%High-tech imaging services (such as PET, CT, MRI) 0% to 50% 0% to 50%Sleep studies 0% to 50% 0% to 50%
For a complete list of covered services and benefits, please see the plan’s benefit summary.
18 ProvidenceHealthPlan.com
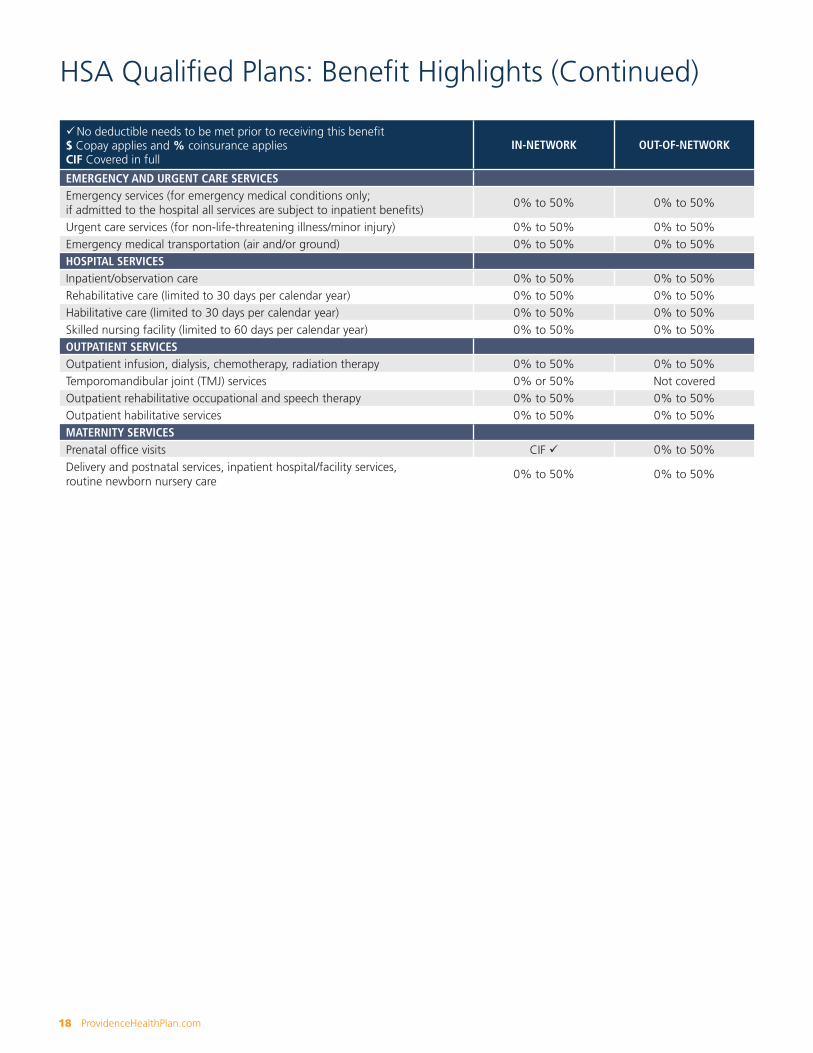
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
0% to 50% 0% to 50%
Urgent care services (for non-life-threatening illness/minor injury) 0% to 50% 0% to 50% Emergency medical transportation (air and/or ground) 0% to 50% 0% to 50%HOSPITAL SERVICESInpatient/observation care 0% to 50% 0% to 50%Rehabilitative care (limited to 30 days per calendar year) 0% to 50% 0% to 50%Habilitative care (limited to 30 days per calendar year) 0% to 50% 0% to 50%Skilled nursing facility (limited to 60 days per calendar year) 0% to 50% 0% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation therapy 0% to 50% 0% to 50%Temporomandibular joint (TMJ) services 0% or 50% Not covered Outpatient rehabilitative occupational and speech therapy 0% to 50% 0% to 50%Outpatient habilitative services 0% to 50% 0% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 0% to 50%Delivery and postnatal services, inpatient hospital/facility services, routine newborn nursery care
0% to 50% 0% to 50%
HSA Qualified Plans: Benefit Highlights (Continued)
ProvidenceHealthPlan.com 19
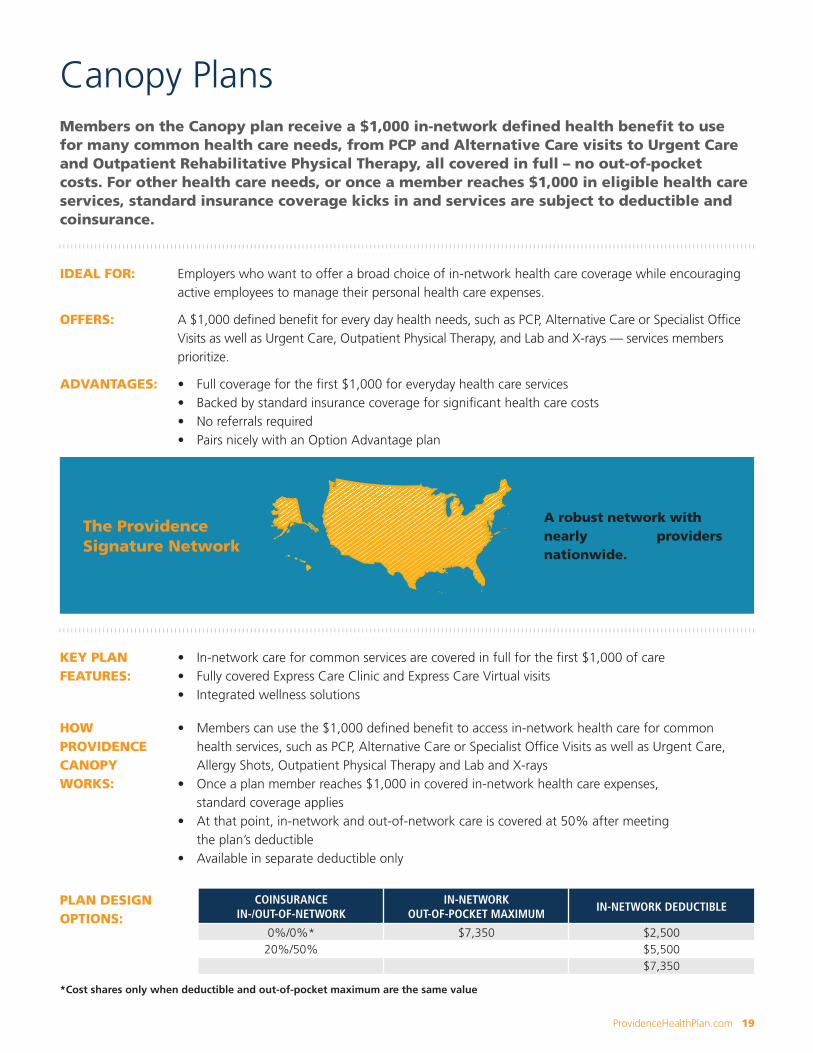
Members on the Canopy plan receive a $1,000 in-network defined health benefit to use for many common health care needs, from PCP and Alternative Care visits to Urgent Care and Outpatient Rehabilitative Physical Therapy, all covered in full – no out-of-pocket costs. For other health care needs, or once a member reaches $1,000 in eligible health care services, standard insurance coverage kicks in and services are subject to deductible and coinsurance.
IDEAL FOR: Employers who want to offer a broad choice of in-network health care coverage while encouraging active employees to manage their personal health care expenses.
OFFERS: A $1,000 defined benefit for every day health needs, such as PCP, Alternative Care or Specialist Office Visits as well as Urgent Care, Outpatient Physical Therapy, and Lab and X-rays — services members prioritize.
ADVANTAGES: • Full coverage for the first $1,000 for everyday health care services• Backed by standard insurance coverage for significant health care costs• No referrals required• Pairs nicely with an Option Advantage plan
KEY PLAN FEATURES:
• In-network care for common services are covered in full for the first $1,000 of care• Fully covered Express Care Clinic and Express Care Virtual visits• Integrated wellness solutions
HOW PROVIDENCE CANOPY WORKS:
• Members can use the $1,000 defined benefit to access in-network health care for common health services, such as PCP, Alternative Care or Specialist Office Visits as well as Urgent Care, Allergy Shots, Outpatient Physical Therapy and Lab and X-rays
• Once a plan member reaches $1,000 in covered in-network health care expenses, standard coverage applies
• At that point, in-network and out-of-network care is covered at 50% after meeting the plan’s deductible
• Available in separate deductible only
Canopy Plans
PLAN DESIGN OPTIONS:
COINSURANCE IN-/OUT-OF-NETWORK
IN-NETWORK OUT-OF-POCKET MAXIMUM
IN-NETWORK DEDUCTIBLE
0%/0%* $7,350 $2,50020%/50% $5,500
$7,350
*Cost shares only when deductible and out-of-pocket maximum are the same value
The Providence Signature Network
A robust network with nearly 1 million providers nationwide.
20 ProvidenceHealthPlan.com
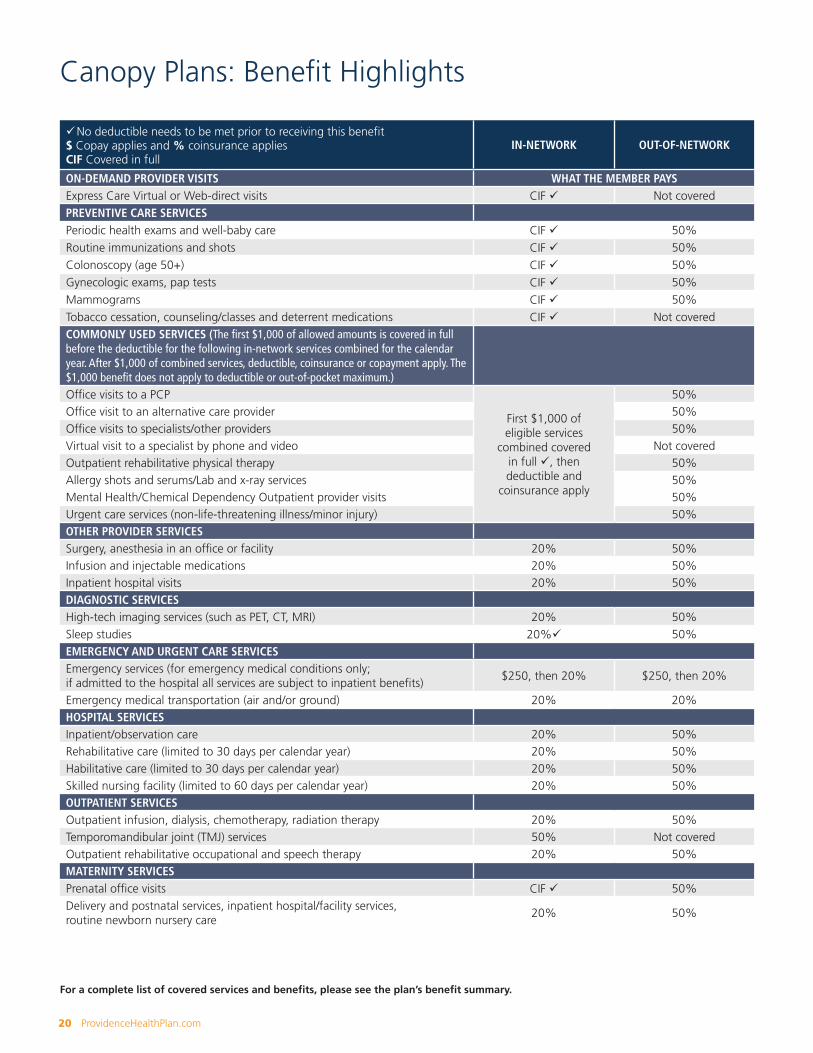
Canopy Plans: Benefit Highlights
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 50%Routine immunizations and shots CIF ü 50%Colonoscopy (age 50+) CIF ü 50%Gynecologic exams, pap tests CIF ü 50%Mammograms CIF ü 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredCOMMONLY USED SERVICES (The first $1,000 of allowed amounts is covered in full before the deductible for the following in-network services combined for the calendar year. After $1,000 of combined services, deductible, coinsurance or copayment apply. The $1,000 benefit does not apply to deductible or out-of-pocket maximum.)Office visits to a PCP
First $1,000 of eligible services
combined covered in full ü, then deductible and
coinsurance apply
50%Office visit to an alternative care provider 50%Office visits to specialists/other providers 50%Virtual visit to a specialist by phone and video Not coveredOutpatient rehabilitative physical therapy 50%Allergy shots and serums/Lab and x-ray services 50%Mental Health/Chemical Dependency Outpatient provider visits 50%Urgent care services (non-life-threatening illness/minor injury) 50%OTHER PROVIDER SERVICESSurgery, anesthesia in an office or facility 20% 50%Infusion and injectable medications 20% 50%Inpatient hospital visits 20% 50%DIAGNOSTIC SERVICESHigh-tech imaging services (such as PET, CT, MRI) 20% 50%Sleep studies 20%ü 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250, then 20% $250, then 20%
Emergency medical transportation (air and/or ground) 20% 20% HOSPITAL SERVICESInpatient/observation care 20% 50%Rehabilitative care (limited to 30 days per calendar year) 20% 50%Habilitative care (limited to 30 days per calendar year) 20% 50%Skilled nursing facility (limited to 60 days per calendar year) 20% 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation therapy 20% 50%Temporomandibular joint (TMJ) services 50% Not covered Outpatient rehabilitative occupational and speech therapy 20% 50%MATERNITY SERVICESPrenatal office visits CIF ü 50%Delivery and postnatal services, inpatient hospital/facility services, routine newborn nursery care
20% 50%
For a complete list of covered services and benefits, please see the plan’s benefit summary.
ProvidenceHealthPlan.com 21
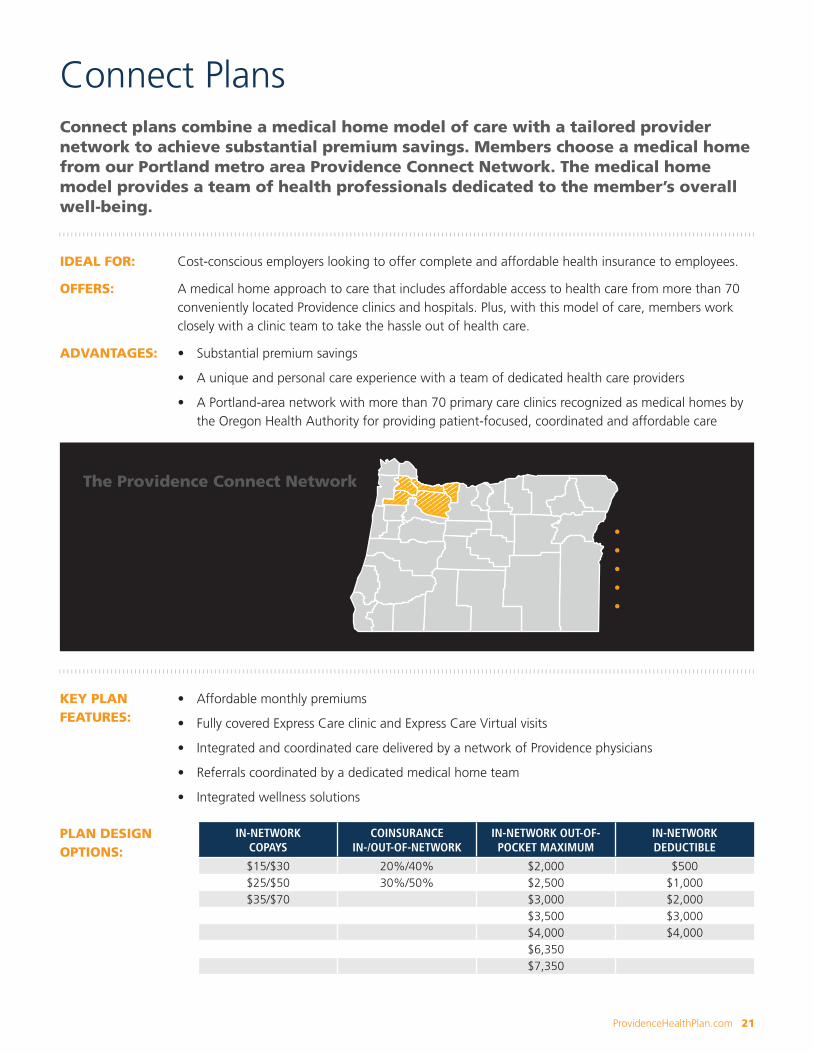
• Clackamas County• Hood River County• Multnomah County• Washington County• The city of Newberg
in Yamhill County
The Providence Connect NetworkA Portland-area network with more than 70 medical home clinics in Washington, Multnomah, Clackamas and Hood River counties, and the city of Newberg in Yamhill county, all designated as medical homes for providing patient-focused, coordinated and affordable care.
Connect plans combine a medical home model of care with a tailored provider network to achieve substantial premium savings. Members choose a medical home from our Portland metro area Providence Connect Network. The medical home model provides a team of health professionals dedicated to the member’s overall well-being.
IDEAL FOR: Cost-conscious employers looking to offer complete and affordable health insurance to employees.
OFFERS: A medical home approach to care that includes affordable access to health care from more than 70 conveniently located Providence clinics and hospitals. Plus, with this model of care, members work closely with a clinic team to take the hassle out of health care.
ADVANTAGES: • Substantial premium savings
• A unique and personal care experience with a team of dedicated health care providers
• A Portland-area network with more than 70 primary care clinics recognized as medical homes by the Oregon Health Authority for providing patient-focused, coordinated and affordable care
KEY PLAN FEATURES:
• Affordable monthly premiums
• Fully covered Express Care clinic and Express Care Virtual visits
• Integrated and coordinated care delivered by a network of Providence physicians
• Referrals coordinated by a dedicated medical home team
• Integrated wellness solutions
Connect Plans
PLAN DESIGN OPTIONS:
IN-NETWORK COPAYS
COINSURANCE IN-/OUT-OF-NETWORK
IN-NETWORK OUT-OF-POCKET MAXIMUM
IN-NETWORK DEDUCTIBLE
$15/$30 20%/40% $2,000 $500$25/$50 30%/50% $2,500 $1,000$35/$70 $3,000 $2,000
$3,500 $3,000$4,000 $4,000$6,350$7,350

22 ProvidenceHealthPlan.com
Connect Plans: Benefit Highlights
For a complete list of covered services and benefits, please see the plan’s benefit summary.
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in fullA referral from your medical home is required to receive in-network benefits
IN-NETWORK OUT-OF-NETWORK
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredVirtual visits to a specialist by phone and video $15 to $55ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 40% to 50% Routine immunizations and shots CIF ü 40% to 50%Colonoscopy (age 50+) CIF ü 40% to 50% Gynecologic exams, pap tests CIF ü 40% to 50% Mammograms CIF ü 40% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP $15 to $35/visit ü 40% to 50%Office visits to alternative care providers $15 to $35/visit ü 40% to 50%Office visits to specialists/other providers $30 to $70/visitü 40% to 50%Allergy shots and serums 20% to 30%ü 40% to 50%Infusions and injectable medications 20% to 30% 40% to 50%Surgery, anesthesia in an office or facility 20% to 30% 40% to 50%DIAGNOSTIC SERVICESLab and x-ray services 20% to 30% ü 40% to 50%High-tech imaging services (such as PET, CT, MRI) 20% to 30% 40% to 50%Sleep studies 20% to 30% ü 40% to 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250 $250
Urgent care services (for non-life-threatening illness/minor injury) $30 to $70/visit ü 40% to 50% Emergency medical transportation (air and/or ground) 20% to 30% 20% to 30%HOSPITAL SERVICESInpatient/observation care 20% to 30% 40% to 50%Rehabilitative care (limited to 30 days per calendar year) 20% to 30% 40% to 50%Habilitative care (limited to 30 days per calendar year) 20% to 30% 40% to 50%Skilled nursing facility (limited to 60 days per calendar year) 20% to 30% 40% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation 20% to 30% 40% to 50%Temporomandibular joint (TMJ) services 50% Not coveredOutpatient rehabilitative physical therapy 20% to 30%ü 40% to 50%Outpatient rehabilitative occupational or speech therapy 20% to 30% 40% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 40% to 50%Delivery and postnatal services (PCP or certified nurse midwife) 10% to 20% 40% to 50%Delivery and postnatal services (OB/GYN physician/provider, all other licensed providers)
20% to 30% 40% to 50%
Inpatient hospital/facility services 20% to 30% 40% to 50%Routine newborn nursery care 20% to 30% 40% to 50%

ProvidenceHealthPlan.com 23
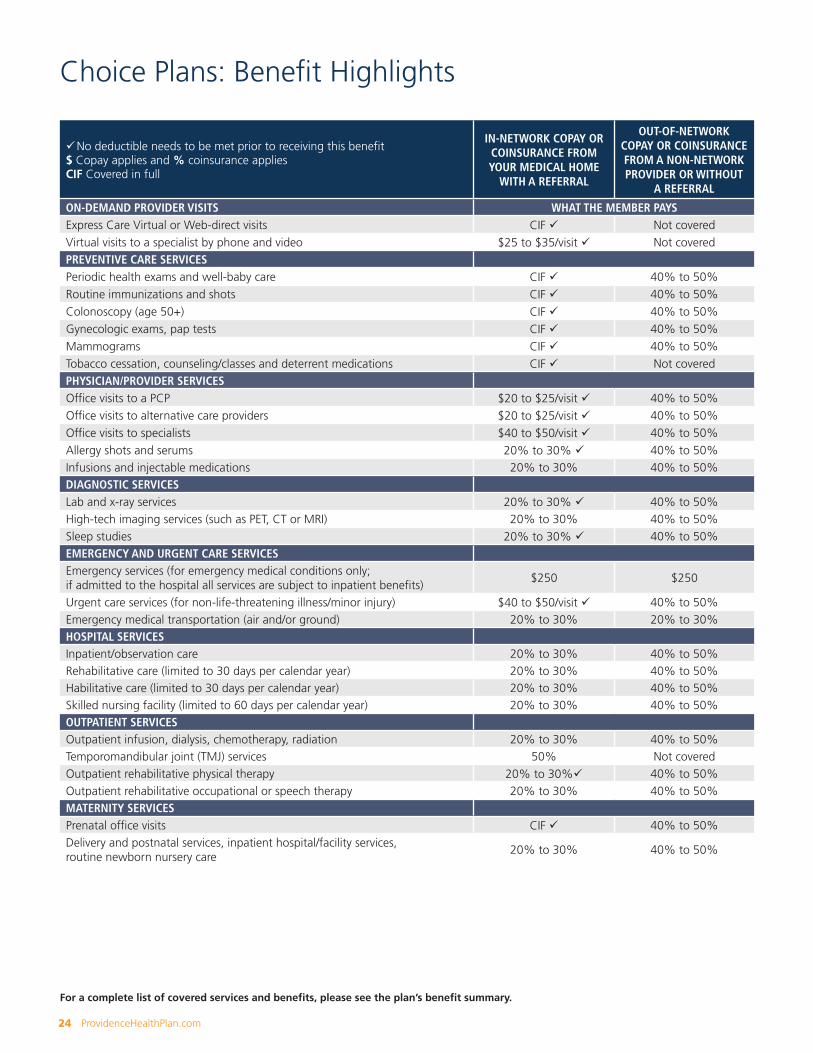
Choice PlansChoice plans combine a medical home model of care with a tailored provider network. Care is coordinated by a team of health professionals uniquely dedicated to a patient’s overall well-being. Members select a recognized medical home from the Providence Choice Network. The medical home team supports all aspects of a member’s health from wellness and prevention to active management of chronic conditions.
IDEAL FOR: Cost-conscious employers looking to offer complete and affordable health insurance to employees.
OFFERS: A medical home plan that includes access to health care from nearly 300 conveniently located clinics and hospitals in Oregon and southwest Washington. Plus, with this model of care, members work closely with a clinic team to take the hassle out of health care.
ADVANTAGES: • Premium savings• A unique and personal care experience with a team of dedicated health providers • A tailored network with nearly 300 primary care clinics recognized for providing patient-focused,
coordinated and affordable care
• Baker• Benton• Clackamas• Clark (WA)• Coos• Crook• Curry• Deschutes
• Douglas• Hood River• Josephine• Klamath• Lane• Lincoln• Linn• Malheur
• Marion• Multnomah• Polk• Umatilla• Union• Wallowa• Washington• Yamhill
The Providence Choice Network
Nearly 300 medical home clinics in Oregon and southwest Washington designated as medical homes for providing patient-focused, coordinated and affordable care.
Providence Choice is available to businesses located in select counties in Oregon and southwest Washington. It must be offered with
another Providence health plan with the Providence Signature Network (Option Advantage, Canopy or an HSA qualified plan).
KEY PLAN FEATURES:
• Affordable monthly premiums• Fully covered Express Care Clinic and Express Care Virtual visits• Integrated and coordinated care delivered by a network of recognized physicians• Referrals coordinated by a dedicated medical home team• Integrated wellness solutions
PLAN DESIGN OPTIONS:
IN-NETWORK COPAYS PCP/SPECIALIST
COINSURANCE IN-/OUT-OF-NETWORK
IN-NETWORK OUT-OF-POCKET
IN-NETWORK DEDUCTIBLE
$20/$40 20%/40% $4,000 $1,500$25/$50 30%/50% $7,350 $3,000
24 ProvidenceHealthPlan.com
Choice Plans: Benefit Highlights
For a complete list of covered services and benefits, please see the plan’s benefit summary.
üNo deductible needs to be met prior to receiving this benefit$ Copay applies and % coinsurance appliesCIF Covered in full
IN-NETWORK COPAY OR COINSURANCE FROM YOUR MEDICAL HOME
WITH A REFERRAL
OUT-OF-NETWORK COPAY OR COINSURANCE FROM A NON-NETWORK PROVIDER OR WITHOUT
A REFERRAL
ON-DEMAND PROVIDER VISITS WHAT THE MEMBER PAYSExpress Care Virtual or Web-direct visits CIF ü Not coveredVirtual visits to a specialist by phone and video $25 to $35/visit ü Not coveredPREVENTIVE CARE SERVICESPeriodic health exams and well-baby care CIF ü 40% to 50%Routine immunizations and shots CIF ü 40% to 50%Colonoscopy (age 50+) CIF ü 40% to 50%Gynecologic exams, pap tests CIF ü 40% to 50%Mammograms CIF ü 40% to 50%Tobacco cessation, counseling/classes and deterrent medications CIF ü Not coveredPHYSICIAN/PROVIDER SERVICESOffice visits to a PCP $20 to $25/visit ü 40% to 50%Office visits to alternative care providers $20 to $25/visit ü 40% to 50%Office visits to specialists $40 to $50/visit ü 40% to 50%Allergy shots and serums 20% to 30% ü 40% to 50%Infusions and injectable medications 20% to 30% 40% to 50%DIAGNOSTIC SERVICESLab and x-ray services 20% to 30% ü 40% to 50%High-tech imaging services (such as PET, CT or MRI) 20% to 30% 40% to 50%Sleep studies 20% to 30% ü 40% to 50%EMERGENCY AND URGENT CARE SERVICESEmergency services (for emergency medical conditions only; if admitted to the hospital all services are subject to inpatient benefits)
$250 $250
Urgent care services (for non-life-threatening illness/minor injury) $40 to $50/visit ü 40% to 50%Emergency medical transportation (air and/or ground) 20% to 30% 20% to 30%HOSPITAL SERVICESInpatient/observation care 20% to 30% 40% to 50%Rehabilitative care (limited to 30 days per calendar year) 20% to 30% 40% to 50%Habilitative care (limited to 30 days per calendar year) 20% to 30% 40% to 50%Skilled nursing facility (limited to 60 days per calendar year) 20% to 30% 40% to 50%OUTPATIENT SERVICESOutpatient infusion, dialysis, chemotherapy, radiation 20% to 30% 40% to 50%Temporomandibular joint (TMJ) services 50% Not coveredOutpatient rehabilitative physical therapy 20% to 30%ü 40% to 50%Outpatient rehabilitative occupational or speech therapy 20% to 30% 40% to 50%MATERNITY SERVICESPrenatal office visits CIF ü 40% to 50%Delivery and postnatal services, inpatient hospital/facility services, routine newborn nursery care
20% to 30% 40% to 50%
ProvidenceHealthPlan.com 25
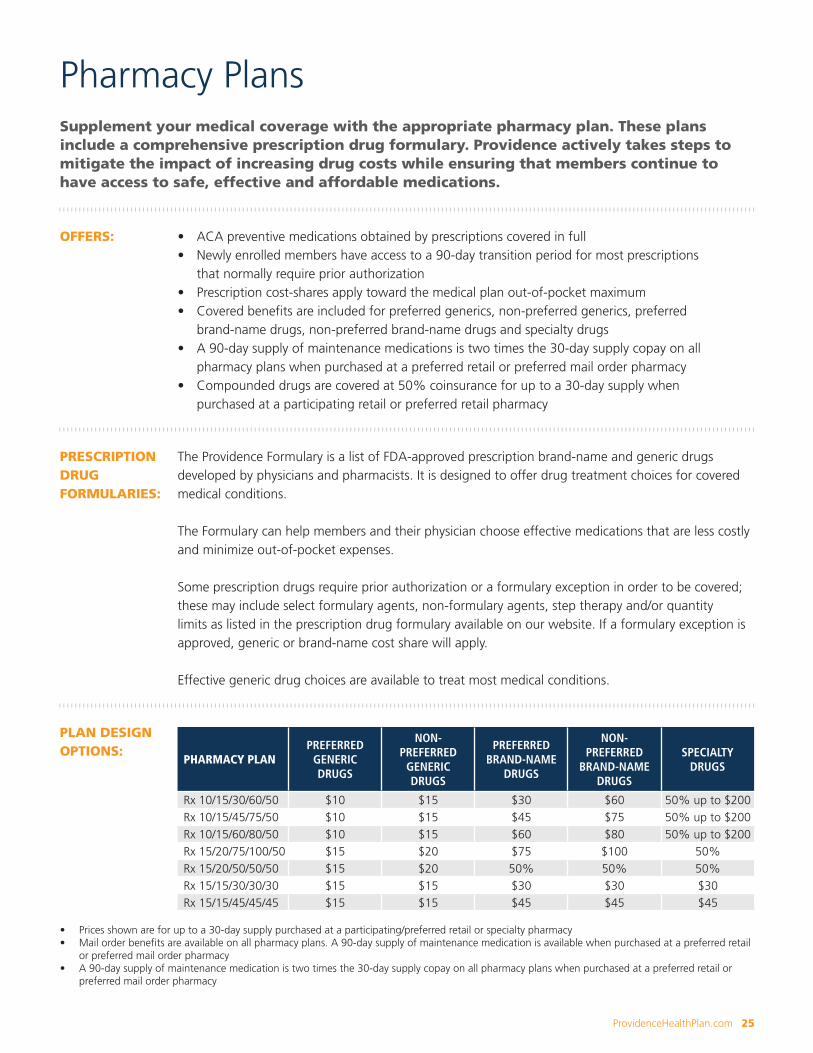
Supplement your medical coverage with the appropriate pharmacy plan. These plans include a comprehensive prescription drug formulary. Providence actively takes steps to mitigate the impact of increasing drug costs while ensuring that members continue to have access to safe, effective and affordable medications.
OFFERS: • ACA preventive medications obtained by prescriptions covered in full• Newly enrolled members have access to a 90-day transition period for most prescriptions
that normally require prior authorization• Prescription cost-shares apply toward the medical plan out-of-pocket maximum• Covered benefits are included for preferred generics, non-preferred generics, preferred
brand-name drugs, non-preferred brand-name drugs and specialty drugs• A 90-day supply of maintenance medications is two times the 30-day supply copay on all
pharmacy plans when purchased at a preferred retail or preferred mail order pharmacy• Compounded drugs are covered at 50% coinsurance for up to a 30-day supply when
purchased at a participating retail or preferred retail pharmacy
PRESCRIPTION DRUG FORMULARIES:
The Providence Formulary is a list of FDA-approved prescription brand-name and generic drugs developed by physicians and pharmacists. It is designed to offer drug treatment choices for covered medical conditions.
The Formulary can help members and their physician choose effective medications that are less costly and minimize out-of-pocket expenses.
Some prescription drugs require prior authorization or a formulary exception in order to be covered; these may include select formulary agents, non-formulary agents, step therapy and/or quantity limits as listed in the prescription drug formulary available on our website. If a formulary exception is approved, generic or brand-name cost share will apply.
Effective generic drug choices are available to treat most medical conditions.
PLAN DESIGN OPTIONS:
PHARMACY PLANPREFERRED
GENERIC DRUGS
NON-PREFERRED
GENERIC DRUGS
PREFERRED BRAND-NAME
DRUGS
NON-PREFERRED
BRAND-NAME DRUGS
SPECIALTY DRUGS
Rx 10/15/30/60/50 $10 $15 $30 $60 50% up to $200Rx 10/15/45/75/50 $10 $15 $45 $75 50% up to $200Rx 10/15/60/80/50 $10 $15 $60 $80 50% up to $200Rx 15/20/75/100/50 $15 $20 $75 $100 50%Rx 15/20/50/50/50 $15 $20 50% 50% 50%Rx 15/15/30/30/30 $15 $15 $30 $30 $30Rx 15/15/45/45/45 $15 $15 $45 $45 $45
• Prices shown are for up to a 30-day supply purchased at a participating/preferred retail or specialty pharmacy• Mail order benefits are available on all pharmacy plans. A 90-day supply of maintenance medication is available when purchased at a preferred retail
or preferred mail order pharmacy• A 90-day supply of maintenance medication is two times the 30-day supply copay on all pharmacy plans when purchased at a preferred retail or
preferred mail order pharmacy
Pharmacy Plans
26 ProvidenceHealthPlan.com
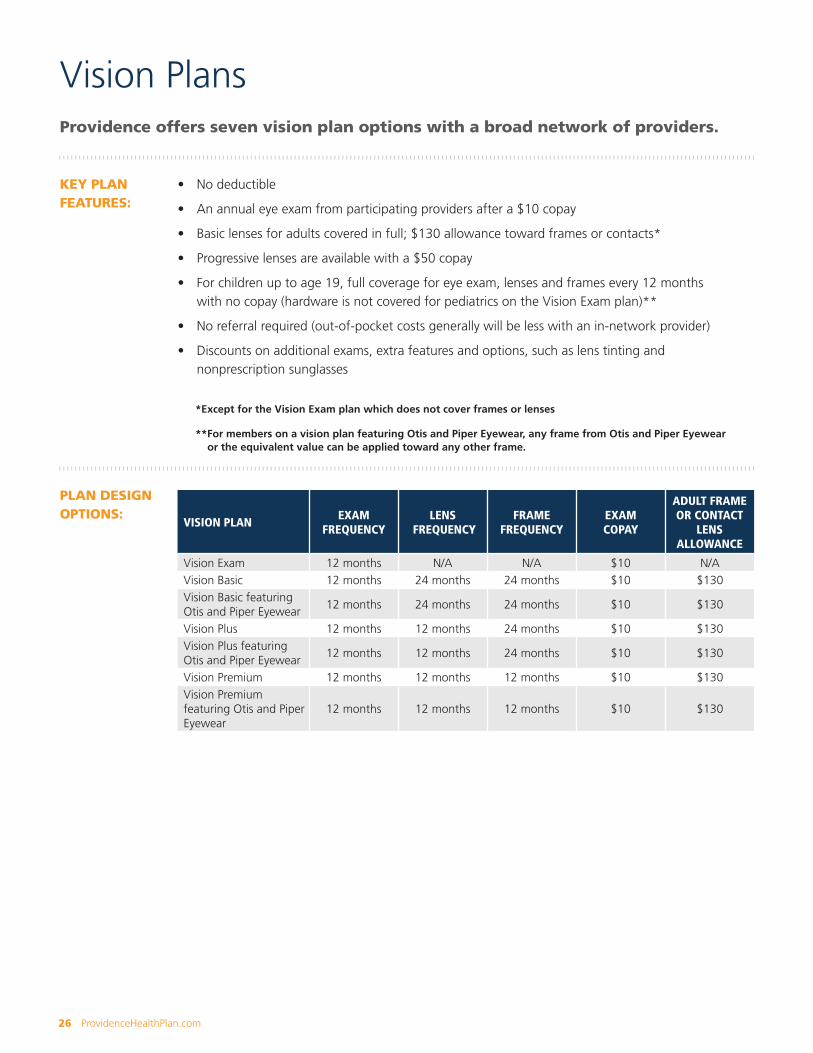
Vision PlansProvidence offers seven vision plan options with a broad network of providers.
KEY PLAN FEATURES:
• No deductible
• An annual eye exam from participating providers after a $10 copay
• Basic lenses for adults covered in full; $130 allowance toward frames or contacts*
• Progressive lenses are available with a $50 copay
• For children up to age 19, full coverage for eye exam, lenses and frames every 12 months with no copay (hardware is not covered for pediatrics on the Vision Exam plan)**
• No referral required (out-of-pocket costs generally will be less with an in-network provider)
• Discounts on additional exams, extra features and options, such as lens tinting and nonprescription sunglasses
PLAN DESIGN OPTIONS:
VISION PLANEXAM
FREQUENCYLENS
FREQUENCYFRAME
FREQUENCYEXAM COPAY
ADULT FRAME OR CONTACT
LENS ALLOWANCE
Vision Exam 12 months N/A N/A $10 N/AVision Basic 12 months 24 months 24 months $10 $130Vision Basic featuring Otis and Piper Eyewear
12 months 24 months 24 months $10 $130
Vision Plus 12 months 12 months 24 months $10 $130Vision Plus featuring Otis and Piper Eyewear
12 months 12 months 24 months $10 $130
Vision Premium 12 months 12 months 12 months $10 $130Vision Premium featuring Otis and Piper Eyewear
12 months 12 months 12 months $10 $130
*Except for the Vision Exam plan which does not cover frames or lenses
**For members on a vision plan featuring Otis and Piper Eyewear, any frame from Otis and Piper Eyewear or the equivalent value can be applied toward any other frame.
ProvidenceHealthPlan.com 27
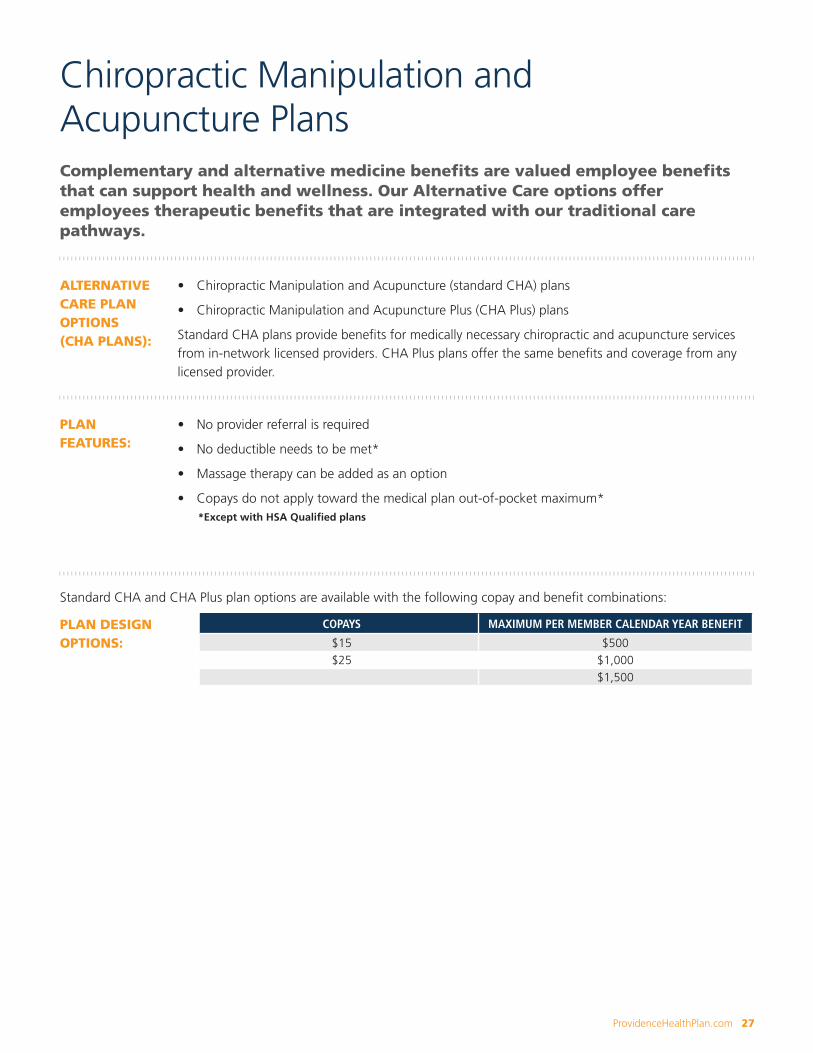
*Except with HSA Qualified plans
Chiropractic Manipulation and Acupuncture PlansComplementary and alternative medicine benefits are valued employee benefits that can support health and wellness. Our Alternative Care options offer employees therapeutic benefits that are integrated with our traditional care pathways.
ALTERNATIVE CARE PLAN OPTIONS (CHA PLANS):
• Chiropractic Manipulation and Acupuncture (standard CHA) plans
• Chiropractic Manipulation and Acupuncture Plus (CHA Plus) plans
Standard CHA plans provide benefits for medically necessary chiropractic and acupuncture services from in-network licensed providers. CHA Plus plans offer the same benefits and coverage from any licensed provider.
PLAN FEATURES:
• No provider referral is required
• No deductible needs to be met*
• Massage therapy can be added as an option
• Copays do not apply toward the medical plan out-of-pocket maximum*
Standard CHA and CHA Plus plan options are available with the following copay and benefit combinations:
PLAN DESIGN OPTIONS:
COPAYS MAXIMUM PER MEMBER CALENDAR YEAR BENEFIT
$15 $500$25 $1,000
$1,500

28 ProvidenceHealthPlan.com
Providence Dental PlansProvidence Dental Plans provide comprehensive benefits that help promote overall good health and are available when paired with a Providence medical plan. The Providence Dental Plan options are available with or without orthodontia benefits. Members have access to more than 2,300 in-network dental providers in Oregon and southwest Washington and more than 270,000 in-network provider listings nationwide.
KEY PLAN FEATURES:
• Plan options available with or without orthodontia benefits• Flexible enrollment, so employees have full ability to select coverage for
dependents who need it• Robust coverage for services received in- and out-of-network• No waiting period for in- or out-of-network• No deductible for in- and out-of-network diagnostic and preventive services• In-network diagnostic and preventive services covered in full• Diagnostic and preventive services do not apply toward calendar year benefit maximum
DENTAL PLAN OPTIONS:
Plans with Plus in the name indicate that orthodontia coverage is included.
• Preventive Dental• Essential• Essential Plus• Essential Access• Essential Access Plus
• Advantage Access 1500• Advantage Access 1500 Plus• Advantage Access 2000• Advantage Access 2000 Plus
DENTAL QUOTE ASSUMPTIONS (SHELF RATES):
• Shelf Rates are valid for up to 200 subscribers• Must comply with the first three Medical Underwriting Requirements• Quoted rates and requirements are based upon the census and other information provided to PHP by
the producer and/or group. In the event of material changes or errors in the information provided, PHP reserves the right to modify the quoted rates and requirements
• If at any time during a Contract Year any federal or state law enacts a tax or assessment associated with this Group Contract, Providence Health Plan may change the premium. The change in Premium shall be effective on the effective date of the tax or assessment, as stated in the notice
• Group must qualify as a large employer with primary legal situs in the State of issue• Matching and Member Level (flexible) enrollment options are available. If matching enrollment
option is selected, participation requirements are based on the medical plan and dental contribution requirements are waived
• If member level (flexible) enrollment option is selected, a member may not select coverage that has not been selected by the subscriber
• Any exceptions to the quote assumptions above are subject to Underwriting review • Must be Employer-Sponsored coverage (contract is with the employer not the employees)• Shelf rates are not valid for Associations, PEO, Dental offices, or Unions/Multi-employer Trusts• No carve outs allowed for shelf rates (e.g., Retirees only, Management only, etc.)

ProvidenceHealthPlan.com 29
Providence Dental Plans: Standard
PREVENTIVE DENTAL
ESSENTIAL DENTAL
ESSENTIAL ACCESS
ADVANTAGE ACCESS 2000
ADVANTAGE ACCESS 1500
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
Deductible None$50 per person $150 per family
(3 or more)
$50 per person $150 per family
(3 or more)
$25 per person $75 per family
(3 or more)
$25 per person $75 per family
(3 or more)
Benefit maximum None $1,000 $1,000 $2,000 $1,500
Diagnostic and Preventive services (includes routine exams, cleanings, bitewing x-rays, topical fluoride [age 16 and younger], space maintainers)
CIF CIF ü 10% ü CIF ü 10% ü CIF ü CIF ü
Basic services (includes restorative fillings, oral surgery, endodontics, periodontics)
Not covered 20% 30% 20% 30% 20% 20%
Major services (includes crowns, dentures, bridge work)
Not covered 50% 60% 50% 50% 50% 50% 50% 50%
ORTHODONTICS (PLUS PLANS)
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
IN- NETWORK
OUT-OF-NETWORK
Common lifetime maximum
NA $1,500 $1,500 $1,500 $1,500
Adult NA 50% up to $1,500 50% up to $1,500 50% up to $1,500 50% up to $1,500
Children NA 50% up to $1,500 50% up to $1,500 50% up to $1,500 50% up to $1,500
Reimbursement MAC MAC MAC MAC MAC UCR MAC UCR MAC UCR
All plan benefits are based on a calendar year. After meeting the deductible, the member pays the following amounts for covered services. The deductible does not apply to some covered services. They are marked with ü
30 ProvidenceHealthPlan.com
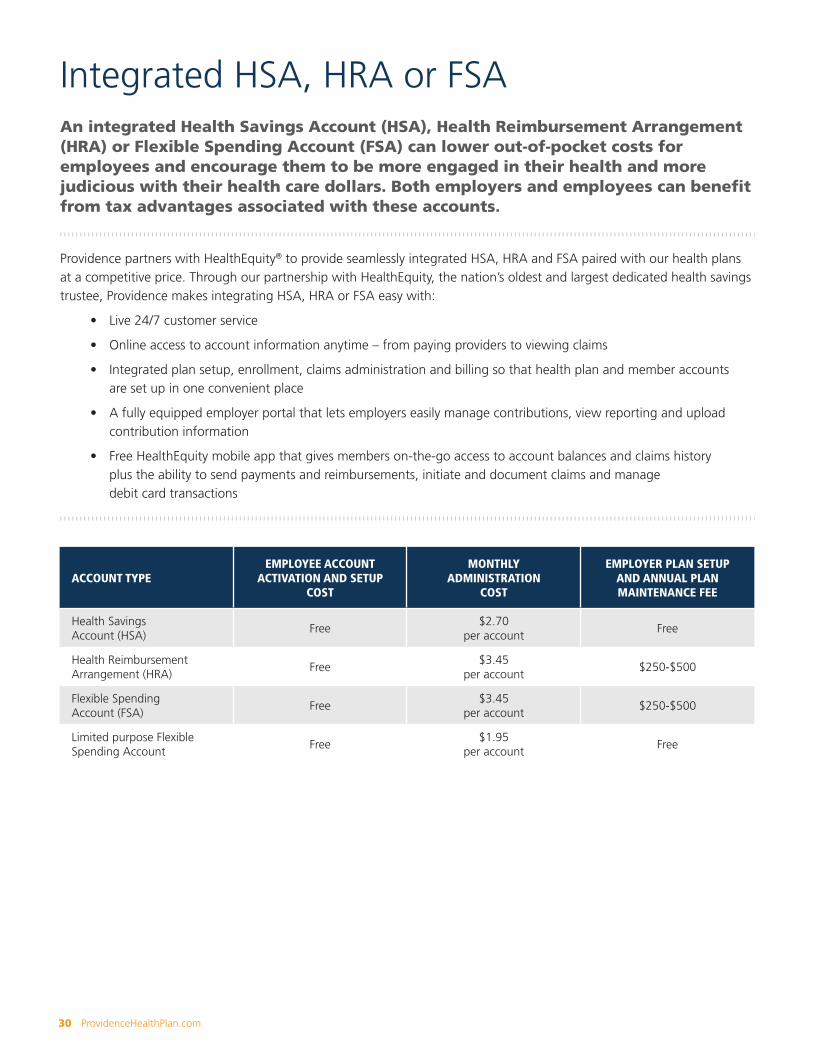
Integrated HSA, HRA or FSAAn integrated Health Savings Account (HSA), Health Reimbursement Arrangement (HRA) or Flexible Spending Account (FSA) can lower out-of-pocket costs for employees and encourage them to be more engaged in their health and more judicious with their health care dollars. Both employers and employees can benefit from tax advantages associated with these accounts.
Providence partners with HealthEquity® to provide seamlessly integrated HSA, HRA and FSA paired with our health plans at a competitive price. Through our partnership with HealthEquity, the nation’s oldest and largest dedicated health savings trustee, Providence makes integrating HSA, HRA or FSA easy with:
• Live 24/7 customer service
• Online access to account information anytime – from paying providers to viewing claims
• Integrated plan setup, enrollment, claims administration and billing so that health plan and member accounts are set up in one convenient place
• A fully equipped employer portal that lets employers easily manage contributions, view reporting and upload contribution information
• Free HealthEquity mobile app that gives members on-the-go access to account balances and claims history plus the ability to send payments and reimbursements, initiate and document claims and manage debit card transactions
ACCOUNT TYPEEMPLOYEE ACCOUNT
ACTIVATION AND SETUP COST
MONTHLY ADMINISTRATION
COST
EMPLOYER PLAN SETUP AND ANNUAL PLAN MAINTENANCE FEE
Health Savings Account (HSA)
Free$2.70
per accountFree
Health Reimbursement Arrangement (HRA)
Free$3.45
per account$250-$500
Flexible Spending Account (FSA)
Free$3.45
per account$250-$500
Limited purpose Flexible Spending Account
Free$1.95
per accountFree

Important Contact Information2018 large group benefit summaries ProvidenceHealthPlan.com
Express Care Clinics and Express Care Virtual Providence.org/expresscare
Employer website ProvidenceHealthPlan.com/employers
HealthEquity HealthEquity.com/providence
Health and wellness for members ProvidenceHealthPlan.com/findyourfit
myProvidence myProvidence.com
Pharmacy resources ProvidenceHealthPlan.com/pharmacy
Producer compensation, news and notices ProvidenceHealthPlan.com/producernotices
Producer website ProvidenceHealthPlan.com/producers
Providence Dental ProvidenceHealthPlan.com/largegroupdental
Providence Employee Assistance Program ProvidenceHealthPlan.com/eap
Providence Health Coaching ProvidenceHealthPlan.com/healthcoach
Provider directory ProvidenceHealthPlan.com/findaprovider
ProvidenceHealthPlan.com 31

Our MissionAs people of Providence, we reveal God’s love for all, especially the poor and vulnerable, through our compassionate service.
Our Core ValuesRespect, Compassion, Justice, Excellence, Stewardship
ProvidenceHealthPlan.com
32 ProvidenceHealthPlan.comPHP17-0056_LG_Overview_Guide_V07 08/25