Embed Size (px)
Citation preview

1
2015 MATERNAL IMMUNIZATION
STAKEHOLDER CONVENING PATH TO IMPACT
Jan 29-30, 2015
Berlin, Germany
MEETING REPORT

2
Report reviewed by:
Convening organizer:
Ajoke Sobanjo-ter Meulen, Senior Program Officer, Bill and Melinda Gates Foundation
Session chairs:
Jon Abramson, Professor of Pediatrics, Wake Forest Medical School
Keith Chirgwin, Deputy Director, Bill and Melinda Gates Foundation
Elizabeth Mason, Former Director MNCAH, WHO
Helen Rees, Executive Director, Wits Reproductive Health and HIV Institute
Nina Schwalbe, Principal Advisor for Health, UNICEF
Greg Widmyer, Deputy Director, Bill and Melinda Gates Foundation

3
Contents
Abbreviations ............................................................................................................................................ 4
Executive Summary ................................................................................................................................ 6
Part 1: Introduction and Investment Case ....................................................................................... 8
Conclusions and Key Takeaways ................................................................................................ 11
Part 2: Evidence Base ......................................................................................................................... 12
Conclusions and Key Takeaways ................................................................................................ 18
Part 3: Regulatory ................................................................................................................................. 19
Conclusions and Key Takeaways ................................................................................................ 23
Part 4: Policy ........................................................................................................................................... 24
Conclusions and Key Takeaways ................................................................................................ 31
Part 5: Market Dynamics ..................................................................................................................... 32
Conclusions and Key Takeaways ................................................................................................ 37
Part 6: Funding ....................................................................................................................................... 38
Conclusions and Key Takeaways ................................................................................................ 44
Part 7: Implementation ......................................................................................................................... 45
Conclusions and Key Takeaways ................................................................................................ 50
List of Conclusions and Key Takeaways ........................................................................................ 51
Coordination and Collaboration......................................................................................................... 54
Appendix A: List of Session Chairs and Speakers ...................................................................... 57
Appendix B: List Panel Chairs and Participants........................................................................... 70
Appendix C: Complete Meeting Participant List........................................................................... 71

4
Abbreviations
AFRO African regional office (WHO)
ALRI Acute lower respiratory-tract infection
ANC Antenatal care
AVAREF African Vaccine Regulatory Forum
BMGF Bill and Melinda Gates Foundation
CAGR Compound annual growth rate
CEA Cost-effectiveness analysis
CFR Case fatality ratio
CHERG Child health epidemiology research group
CIDA Canadian International Development Agency
DALY Disability-adjusted life years
DFID Department for International Development (UK)
EMA European Medicines Agency
ENAP Every Newborn Action Plan
EPI Expanded Program on Immunization
FDA Food and Drug Administration
GAVI The Global Alliance for Vaccines and Immunizations
GBD Global burden of disease
GBS Group B streptococcus
GFF Global Financing Facility
HHS U.S. Department of Health and Human Services
HPV Human papillomavirus
IDA International Development Association
IHME Institute of Health Metrics and Evaluation
IPTp Intermittent preventive treatment in pregnancy
ITN Insecticide treated net
JE Japanese encephalitis
JHU Johns Hopkins University
LBW Low birth weight
LIC Low income countries
LMIC Lower-middle income countries
LRI Lower respiratory-tract infection
LSHTM London School of Hygiene & Tropical Medicine
MDG Millennium development goal
MenA Meningitis A
MI Maternal immunization
MNCAH Maternal, newborn, child and adolescent Health
MNCH Maternal, newborn, and child health
MNH Maternal and neonatal health

5
MNTE Maternal and Neonatal Tetanus Elimination
MoH Ministry of Health
NGO Non-governmental organizations
NIH National Institutes of Health
NITAG National Immunization Technical Advisory Group
NMR Neonatal mortality rate
Norad Norwegian Agency for Development Cooperation
NRA National Regulatory Authority
PCV Pneumococcal vaccine
PDP Product development partnership
PDVAC Product Development for Vaccines Advisory Committee
PLLR Pregnancy and Lactation Labeling Rule
PMTCT Prevention of mother to child transmission
PQ Pre-Qualification
PT Pertussis toxoid
PW Pregnant women
RH/MNCAH Reproductive health / Maternal, newborn, child, and adolescent health
RMNCH Reproductive, maternal, newborn, and child health
ROI Return on investment
Rota Rotavirus
RSV Respiratory syncytial virus
SAGE Strategic Advisory Group of Experts
SDG Sustainable Development Goal
SIA Supplemental Immunization Activities
SGA Small for gestational age
TBA Trained birth attendant
Tdap Tetanus Diphtheria and Pertussis
TPP Target product profile
TT Tetanus toxoid
UNFPA United Nations Population Fund
UNICEF United Nations Children's Fund
USAID United States Agency for International Development
WHO World Health Organization
WRHI Wits Reproductive Health and HIV Institute

6
Executive Summary While concerted global efforts have led to the steady reduction of under-5 childhood mortality by ~5% per year over the past two decades, mortality reduction in neonates has been more gradual, declining on average ~3% per year since 1990. Due to this difference, neonatal deaths have risen from 35% of under-5 deaths in 1990 to 44% today, a trend that is expected to continue. Maternal immunization has emerged as a promising intervention to address infection-related neonatal and young infant deaths in developing countries, and is increasingly supported by global health stakeholders and industry. In addition to addressing difficult to reach neonatal and young infant deaths, maternal immunization may also provide substantial health benefits to fetuses, reduce morbidity & associated healthcare costs, and provide a number of socio-economic benefits. Given the growing evidence base, maturing product development pipelines and global policy momentum, now is a pivotal time for the alignment of key stake-holders on a strategic path to impact for maternal immunization in developing countries. On January 29-30, 2015, the foundation convened a meeting of global health stakeholders in maternal immunization in Berlin. The convening attracted major donors, as well as over 110 key leaders in vaccine manufacturing, regulatory agencies, academia, multilateral organizations, and country-level ministers of health from Africa and Asia. Representatives from the foundation's Pneumonia, MNCH, Vaccine Delivery, Vaccine Development, and LSP groups were also present. The meeting focused on maternal immunization as an intervention for addressing five pathogens: Influenza, Respiratory Syncytial Virus, Pertussis, Tetanus, and Group B Streptococcus. Goals for the convening included (1) Understanding the challenges, knowledge gaps and potential impact of maternal immunization at both the platform and pathogen level, (2) Setting strategic priorities for the maternal immunization community, and (3) Fostering alignment between the MNCH and Vaccine communities on an end-to-end “Path to Impact” for maternal immunization. Major conclusions included:
A stronger evidence base is needed, including burden of disease, maternal immunization efficacy and safety for mother, fetus and infant, and effects on morbidity & associated healthcare costs, in order to build a stronger investment case for manufacturer and donor investment, policy recommendations, licensure, and country-level uptake.
Integration of maternal immunization into the ANC channel is preferred, but research needed to identify the most attractive integration models for given countries and pathogens. These models should benefit women, fetuses and infants, provide benefits beyond mortality (e.g. maternal health and socio-economic benefits), strengthen existing healthcare systems rather than fragmenting them, and be sustainably funded.
The foundation & external stakeholders are engaged and willing to take on next steps, including sharing of learnings from existing maternal immunization efforts (e.g. MNTE, pertussis in Argentina), funding to improve the maternal immunization

7
evidence base and accelerate maternal vaccine development, development of maternal vaccine TPPs by WHO PDVAC and other stakeholders, and integration of SAGE and maternal immunization policy guidelines with WHO ANC guideline development.
The convening enabled discussions across pathogens, platforms, and stakeholder groups that led to novel strategic-level insight, especially between the vaccine and MNCH communities, and created momentum for collaboratively addressing key challenges on the maternal immunization path to impact.

8
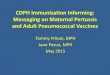
Part 1: Introduction and Investment Case Maternal Immunization in the Context of a Global Health Agenda Keith Klugman (BMGF), France Donnay (BMGF) Global under-5 (U5) mortality has declined from 90 deaths per 1,000 live births in 1990 to 48 deaths per 1,000 live births in 2012, a decline of ~5% per year. Neonatal mortality has only declined by ~3% per year, however, and by 2035 is projected to make up ~55% of all U5 mortality. Accelerated action in addressing neonatal mortality will therefore be required to continue making substantial progress in global health, and to reach the Sustainable Development Goals (currently under development) by 2030.
Global under-five (U5), infant and neonatal mortality rates (1990-2012)
From "Maternal Immunization in the Context of a Global Health Agenda" presentation, Keith Klugman & France Donnay
Maternal immunization is an approach that sits at the crossroads of the Vaccine and Maternal, Newborn, and Child Health Communities (MNCH), in which pregnant women are vaccinated in order to protect newborns who are too young to be vaccinated themselves. Neonatal mortality includes ~600k infection-related deaths per year, part of which may be addressed by the maternal immunization interventions under consideration at this convening. In addition, maternal immunization may address part of the ~965k deaths from pre-term birth, prevent a portion of the 10-50% of still-births estimated to be
25
50
75
100
1990 1995 2000 20102005 2015
Under-f ive mortality rateInfant mortality rateNeonatal mortality rate
90
48
MDG 4
target: 30
Global Under-five (U5), Infant and Neonatal Mortality Rates (1990-2012)
Neonatal: ~3% annual decline
Under-five: ~5% annual decline
Death
s p
er
1,0
00 L
ive B
irth
s
Global neonatal mortality 1
1. McClure EM, "Stillbirth in Developing Countries: A review of causes, risk factors and prevention strategies”, J. of Matern Fetal
Neonatal Med. (2014); 2. WHO-CHERG 2013

9
caused by infectious disease, and provide protection to mothers & infants < 5 months of age. To realize these benefits, outstanding issues regarding maternal immunization uptake, cost-effectiveness, affordability, and integration with antenatal care, particularly in low-income and lower-middle income countries (LIC/LMIC), will need to be addressed. The goal of the 2015 stakeholder convening will be to understand the challenges, knowledge gaps and potential impact of five maternal immunization initiatives, and to align on next steps to drive toward health impact. In particular, three desired outcomes were highlighted:
Identify challenges & potential solutions to achieve maternal immunization impact
Set strategic priorities for the maternal immunization community
Encourage increased collaboration of the Vaccine and MNCH communities Investment Case Ajoke Sobanjo-ter Meulen (BMGF)
Brief summary: Implementation of maternal immunization must be supported by a strong investment case that demonstrates cost-effective health benefits. The foundation recently completed a health impact and cost effectiveness analysis, which showed that maternal immunization has significant potential to avert neonatal and infant deaths (~40-85k per year) and morbidity (~4-8M disability adjusted life years (DALYs) per year) by 2040. Maternal immunization may also decrease the rate of pre-term and still-births, provide socio-economic benefits and, if implemented properly, strengthen the existing antenatal care (ANC) system. In order to build a more robust investment case, the pathogen-specific evidence base must be strengthened, and challenges in affordability, ANC coverage, and Vaccine/MNCH integration addressed. Maternal immunization progress and future directions: Maternal immunization has existed for over a century, with acceptance and investment increasing over the last decade in response to expanding safety and efficacy data. The foundation began significant investment in maternal immunization in 2009, primarily with evidence base and vaccine development focused on influenza and Respiratory Syncytial Virus (RSV). In 2014 the foundation expanded its maternal immunization program to five pathogens: Influenza, RSV, Pertussis, Tetanus, and Group B Streptococcus (GBS). The foundation aims, and plans to leverage this convening, to drive toward an end-to-end path to impact for maternal immunization, starting with evidence generation and product development, and ending with the delivery and monitoring of maternal immunization impact.

10
Long history of progress in maternal immunization
Source: "Maternal Immunization: Path to Impact" presentation by Ajoke Sobanjo-ter Meulen
The foundation's forecast of maternal immunization health impact: The foundation recently completed a health impact and cost effectiveness analysis of maternal immunization, based on a high-level model of disease burden, vaccine efficacy, and vaccine procurement and delivery costs. The model predicts a total of ~0.7-1.6 M deaths averted by 2040 if Pertussis, GBS, Influenza, and RSV vaccines are introduced into ANC channels in all current LIC/LMICs. By 2030, annual deaths averted are estimated at ~40-85k deaths (~1% of global under-5 burden) while DALYs averted are estimated at ~ 4-8 M DALYs. Cost per death averted is estimated to be high relative to most GAVI-funded vaccines, but comparable in cost per DALY averted to other MNCH interventions. Model results indicate the need for a stronger evidence base, affordable vaccine prices, increased ANC coverage, and collaboration between Vaccine and MNCH communities.
Range of deaths and DALYs averted after introduction of maternal immunization against four pathogens (RSV, GBS, influenza and pertussis) in LIC / LMIC
Source: BCG analysis. Note: Introduction date assumptions: Influenza – 2017, Pertussis – 2020, RSV – 2020, GBS – 2025.
Table of model assumptions used to predict future morbidity and mortality impact

11
Assumptions
Disease burden
Timeline
2015–2040
Geographical coverage All low and lower-middle income countries (82 LIC/LMIC)
Base burden data Based on IHME GBD, and CHERG1
Future disease trends Global neonatal mortality decline (~-3%)2
Health impact
Delivery channel Assume antenatal care with ANC1 coverage rate (~30-100%)3
Duration of protection BMGF projection by vaccine (3-5 months)
Vaccine efficacy BMGF projection by vaccine (45-70%)4
Vaccine intro. date BMGF assumption by vaccine (2017-2025)
Cost Vaccine / delivery cost $2.40 base assumption for price+delivery cost of all vaccines5
Averted cost of care No averted cost of care included (pending)
General Sensitivity analysis Univariate sensitivity analysis applied on burden, vaccine efficacy, vaccine cost, duration of protection, etc.
Source: BCG analysis. 1. Global burden of disease, Child Health Epidemiology Research Group. 2. Average neonatal decline from Liu, Li, et al. "Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis." The Lancet (2014). 3. GAVI strategic demand forecast 4. Influenza calculated from current BMGF MI trials. 5. Based on assumed COGS, markup, and delivery cost
Introduction and Investment Case: Conclusions and Key Takeaways
1. Neonatal mortality is a growing proportion of under-5 mortality and immunization provides an opportunity to prevent a portion of infection related neonatal mortality that is not addressed through any other intervention in LIC/LMIC settings. Therefore, the potential for maternal immunization to address unmet health needs will grow over time.
2. The foundation's impact model predicts significant mortality and morbidity aversion, on the higher end of cost per death averted compared to GAVI vaccines, and moderate cost per DALY averted compared to current MNCH interventions.
3. A better understanding of the disease burden, especially in LIC/LMIC is required to assess the full potential health impact of maternal immunization.
4. Additional benefits, currently uncaptured in the model, include the potential impact on infection-related pre-term and still-births, and non-DALY morbidity burden with associated healthcare costs.

12
Part 2: Evidence Base Context and Session Goals The foundation has focused its efforts in maternal immunization on five pathogens: Influenza, Tetanus, Group B Streptococcus (GBS), Pertussis, and Respiratory Syncytial Virus (RSV). The investment case for maternal immunization and the willingness of manufacturers and healthcare providers to allocate resources will depend on the strength of the disease burden evidence base and potential health impact of vaccination for each pathogen. This session discusses the current evidence base for each pathogen, including addressable mortality and morbidity from each disease in neonates, infants, and mothers, current vaccine candidate development status and likely profile, and potential effects on fetal outcomes (e.g. pre-term and still birth). The goal of the session is to use the current evidence base to identify key information gaps for each of the five pathogens addressable by maternal immunization. Influenza Evidence Base Shabir Madhi (National Institute for Communicable Diseases, University of Witwatersrand)
Brief summary: Influenza is estimated to cause ~30k-110k deaths annually in children, the vast majority in low-income and lower-middle income countries (LIC/LMICs). It also poses significant health risks to pregnant women, and may negatively affect fetal outcomes. Influenza may impact pre-term and still-birth rates, but significant knowledge gaps in these areas prevent estimation of the potential health impact. Burden of disease in pregnant women and infants: In 2008, influenza was estimated to have caused the deaths of between ~30k-110k children. ~99% of these deaths occurred in LIC/LMIC. Among pregnant women, recent evidence has suggested that pregnancy is not a risk factor for influenza. However, pregnancy appears to increase the risk of cardio-pulmonary events in pregnant women and may therefore represent a significant risk to both mother and child. Among children, one South African study demonstrated a case fatality rate (CFR) due to influenza-associated severe acute lower respiratory infection of ~4.5% for infants under six months of age, an estimate that may be higher among neonates and in lower income countries. Despite the high fatality rate, the relatively low incidence of severe influenza associated disease resulted in lower overall mortality burden than respiratory syncytial virus (CFR of ~1.2%) in South Africa. Vaccine efficacy in pregnant women and neonates: Maternal immunization has the potential to improve health outcomes for pregnant women, fetuses, and neonates. For pregnant, HIV- women, efficacy was estimated at ~50% (15-71% CI). Greater efficacy in women has been reported for pandemic flu. In young infants, maternal immunization was also estimated to be effective (~53% in Bangladesh and S. Africa, 25-71% CI). Beneficial

13
effects of maternal influenza immunization on fetal outcomes are unconfirmed, as mixed results have been reported for rates of premature birth and SGA (small for gestational age). Significant knowledge gaps affecting estimates of impact for maternal influenza immunization include the disease burden for young infants at the country level, the impact of vaccination on severe illness, and potential fetal benefits (pre-term, still birth, and SGA rates). Additional knowledge gaps that may affect impact in developing countries include the difficulty of strain matching in environments of year-round influenza as well as the logistical challenges of timely vaccine delivery.
Summary of key gaps and next steps for influenza
Key gaps Implications if not addressed Desired actions
Evidence for severe disease burden in young infants, including at country level
Poor awareness and demand among different countries due to lack of evidence
Active surveillance studies of severe illness in regions with high burden to improve current evidence
Impact of vaccination on severe illness
Questionability of extrapolation of current efficacy data
Effectiveness studies on severe illness, including HIV-exposed infants
Potential fetal benefits of MI Underestimation of potential health impact of MI
Clinical studies looking at birth outcomes in SEARO countries
Unpredictable efficacy of currently available Vx
Role of strain matching
Uncertain health impact of maternal immunization and more complicated logistics
Invest in development of universal vaccine to circumvent need of strain matching
Logistical challenges in timelines of vaccine availability and formulation
Low adoption at country-level Improve timeline for vaccine availability and regulatory framework for approval in countries
Source: “Influenza Evidence Base" presentation, Shabir Madhi
Maternal and Neonatal Tetanus Elimination (MNTE) Dr. Azhar Abid Raza (UNICEF New York) Brief summary: The Maternal and neonatal tetanus elimination (MNTE) program has
made substantial progress, with 35 nations achieving elimination (defined as <1 case per
1,000 live births in each district) in the last 15 years. This has been due both to
supplemental immunization activities and strengthening of routine vaccination services.
Learnings from the past 15 years of MNTE will be useful in targeting the remaining 24
non-eliminated nations and in designing maternal immunization programs for other
pathogens.
Background and disease burden: Maternal and neonatal tetanus (MNT) causes
~49,000 deaths annually and occurs primarily in areas with weak health infrastructure. It

14
has a case fatality rate of ~70-100%. ~60% of the total MNT deaths are concentrated in
India, Nigeria, Pakistan and DRC.
Progress toward elimination: MNT elimination is achievable through vaccination and
has been achieved in 88 countries (defined as < 1 case per 1,000 live births in every
district). Of these, 35 achieved elimination between 2000 and 2014. 8 did so by
strengthening routine immunization and reproductive health services, while the rest used
supplemental immunization activities (SIA) or integrated campaigns. In 2014, 24 countries
had yet to achieve elimination. Four strategies have been applied to achieve and maintain
elimination: (1) SIA to target women of reproductive age, (2) Vaccination of pregnant
women through ANC or referral through midwives, (3) Enablement of clean delivery, and
(4) Surveillance systems to maintain elimination.
Lessons learned: Lessons learned include the need for strong political commitments
and secure financial flow, the need for planning and training to ensure campaign
effectiveness, and the need for community engagement to prevent misconceptions and
delays in implementation. Important operational principles learned from the MNTE effort
include the utility of supplemental immunization activities to target vulnerable populations
lacking regular health coverage, and the difficulty of surveillance in such populations,
particularly for neonates. During the Q&A, an audience member asked whether mothers
will opt for vaccination when the only health risk of the pathogen is to their child. UNICEF's
observation was that for tetanus this has not been a problem, and that acceptance has
been excellent so long as disease burden is clear (i.e. mothers are aware of the health
risks of tetanus to their child).
Summary of operational challenges and next steps for tetanus
Operational Challenges Next Steps
Most vulnerable population often not reachable through regular service - High-risk approach proved effective
Explore possible integrations and innovations to counter prevailing access and security issues.
Wide variations exist in access to services within & between countries
Demand creation by engaging communities and health workers
Missed opportunities during referral (EPI center ↔ ANC Clinic)
Expand partnerships and resource mobilization efforts to bridge funding gap of US$ 90 million.
TT Vaccination coverage – credited to EPI efficiency
Stay vigilant; periodically monitor progress in all countries
Difficulties in monitoring protection – serosurveys not an easy alternative.
Strengthen existing health services to achieve >80% TT/Td coverage and >70% access to clean delivery
Gaps in neonatal tetanus Surveillance while limited data on maternal tetanus.
Programmatic integrations to minimize missed opportunities
Source: "Maternal and Neonatal Tetanus Elimination (MNTE)" presentation, Dr. Azhar Abid Raza

15
Group B Streptococcal Infections in Neonates and Young Infants Carol J. Baker, M.D. (Baylor College of Medicine, Executive Director of the Center for Vaccine Awareness and Research at Texas Children’s Hospital) Brief summary: Group B streptococcus (GBS) causes pneumonia, meningitis and sepsis
in neonates and is associated with high rates of mortality and morbidity. Incidence of
GBS in LIC/LMIC is not well established and under reporting is believed to be significant.
Vaccine development is in the clinical stage with promising safety and immunogenicity
but efficacy is yet to be established.
Background and disease burden: GBS disease burden is estimated at 0.5 per 1,000
live births globally, but is believed to be underreported due to lack of laboratory
confirmation capacity in many countries. Surveillance studies have shown that GBS is
more common in AFRO (~2 cases per 1000 live births), but uncommon in SEARO (~0.02
cases per 1000 live births). The studies that make up the surveillance data have varying
detection mechanisms and methodology, and more consistent data is needed to confirm
the true disease burden in many places. The case fatality rate is at least 10% (higher in
AFRO). Among the ~25% who develop meningitis, ~50% of survivors are left with severe
disability. GBS is also thought to cause stillbirth in 1% of infected women. In the United
States and other high income countries, intrapartum prophylactic antibiotics are given to
GBS colonized mothers - an effective strategy, cost and operationally prohibitive in
LIC/LMIC. More accurate disease burden and impact estimates represent a key
knowledge gap, as infection rates and confirmation of sepsis are difficult to assess owing
to poor surveillance and detection.
Status and future of GBS vaccine: There are at least 2 GBS vaccines in development,
as Novartis currently has one GBS vaccine in clinical development and another
manufacturer has a vaccine in pre- clinical development. In the former, phase 2 trials in
non-pregnant and pregnant women indicate safety and immunogenicity, but efficacy has
yet to be demonstrated. It is unclear whether this vaccine will continue on to a clinical
case driven phase 3 efficacy trial due to the need for a very large study population
(~80,000 pregnant women). While the Novartis vaccine is trivalent and has a ~85%
serotype coverage, there is interest in increasing valency to improve vaccine coverage.
Although GBS vaccines will likely be marketed in developed countries, assessing clinical
efficacy in populations with low disease burden and alternative prophylactic antibiotic
treatments may prove difficult. Thus, a GBS vaccine may be a candidate for surrogate
efficacy endpoints (e.g. immunogenicity), or clinical trials in developing countries where
disease burden is higher.

16
Summary of key gaps and next steps for GBS
Gaps Actions
Epidemiology: disease burden and health impact in the developing world
Laboratory defined sepsis (blood/CSF cultures “always”)
Multivalent vaccine to provide greatest efficacy (Ia, Ib, II, III, IV, V)
Active, population-based, laboratory surveillance of early- and late-onset disease and CPS type %
Novel licensing pathway for resource rich regions
Initial R & D of multivalent cost-favorable vaccine
Source: "Group B Streptococcal Infections in Neonates and Young Infants" presentation by Carol J. Baker, M.D.
Pertussis Jussi Mertsola (Turku University Hospital, Finland)
Brief summary: Pertussis infection occurs in all age groups, but pertussis mortality primarily affects young infants in the first few months of life. Existing vaccines have good safety and efficacy profiles, however, short duration of protection and high vaccine cost (for acellular vaccinations) pose issues for LIC implementation. Background and disease burden: Pertussis is estimated to cause ~60,000 deaths per year in children under 5, though there may be significant underreporting due to the variable range of symptoms and lack of laboratory confirmation. ~90% of mortality occurs in the first few months of life and may therefore be addressable by maternal immunization. Immunity wanes over time and is mostly lost by 8.5 years after the last vaccination, necessitating rational planning of infant vaccination timing, consideration of boosters, and appropriate post-vaccination surveillance. It is possible that this limited immunity is due to the use of acellular pertussis vaccines; however, the safety profile of whole-cell vaccines is generally not considered favorable for use in pregnant women. Vaccine status: Immunity to pertussis wanes over time, which has resulted in spikes in pertussis cases and a resurgence in neonatal pertussis mortality in developed countries over the last two decades. A recent UK study showed that maternal immunization with trivalent Tdap was ~90% effective against pertussis in infants under three months of age. Safety in pregnant women has also been established, with no evidence of accelerated time to delivery, increased risk of stillbirth, hemorrhage, or low birth weight. PAHO countries have also provided Tdap via maternal immunization, and may provide important learnings for future maternal immunization efforts. Lower-cost alternatives to trivalent Tdap, such as PT-only Tdap and a pertussis-toxoid-only vaccine, are being considered for maternal immunization applications in LIC/LMIC. During the Q&A session, several attendees raised the point that pertussis vaccines are already provided in many AFRO countries. It will therefore be important to determine what vaccine is given during pregnancy, how this will affect current vaccination schedules, and whether boosters will be necessary.

17
Summary of key gaps and next steps for pertussis
Key gaps Implications if not addressed Desired actions
Disease burden in first months of life in LIC/LMIC
Potential under reporting due to lack of laboratory confirmed cases
Lower impact of pertussis MI
Conduct active surveillance studies to quantify disease burden in infants
Use lab confirmation to identify positive cases
Impact of maternal immunization on childhood DTwP vaccination
Dampening of immune response to childhood vaccination leading to increased burden in infants and children
Conduct controlled trials to evaluate the impact of maternal immunization with aP on childhood vaccination with wP
Source: "Pertussis" presentation, Jussi Mertsola
Respiratory Syncytial Virus Eric A.F. Simões, MB, BS, DCH, MD (University of Colorado, Denver) Brief summary: Deaths from Respiratory syncytial virus (RSV) occur primarily in children under 6 months of age, and early live cases can result in significant morbidity. High maternal antibody titers are effective in protecting against the virus and vaccines against RSV are currently in clinical development. One monoclonal antibody providing passive immunity against RSV is in use in developed countries for vulnerable populations. Background and disease burden: Globally, near-ubiquitous infection with RSV is estimated to cause between ~66k-199k deaths annually in children under 5, concentrated primarily in the first 6 months of life. Case fatality rates are estimated to be between ~2-10%, with higher rates concentrated in LIC/LMIC. Even in non-fatal cases, RSV can result in asthma and recurrent wheezing later in life. RSV is seasonal and patterns of infection vary between regions. Early evidence for maternal immunization and vaccine status: High maternal antibody titers have been shown to reduce the risk of neonatal RSV and resulting asthma, indicating the potential of maternal immunization to address a high percentage of neonatal RSV deaths. Achieving high antibody titers over the period required to provide neonatal protection may be challenging, however, due in part to natural antibody longevity and in part to the effects of background disease burdens such as HIV and malnutrition. Novavax currently has an RSV F protein-based vaccine in phase II clinical trials that has shown good immunogenicity and safety in women of child-bearing age. A multi-dose monoclonal antibody (palivizumab) is effectively used in high-income countries in premature infants to increase passive immunity against RSV. MedImmune is currently developing an alternative to palivizumab for prophylaxis in healthy infants that is single-dose, and may therefore be simpler, less expensive, and more attractive for LIC/LMIC.
Summary of key gaps and next steps for RSV

18
Key gaps Implications if not addressed Desired actions
Accurate identification of RSV burden in infants in the developing world
Under estimation of the disease burden and MI impact
Active surveillance studies with Focus on first 6 months especially Indian subcontinent, China, Nigeria
Understanding the kinetics of RSV antibody transfer and longevity
Overestimate the potential impact of MI
RSV neut antibody kinetics studies in different epidemiologic backgrounds
Disease burden in pregnant women
Might impact licensure in industrialized nations
Active surveillance studies focusing on pregnant women
Effect of MI on recurrent wheezing
Potential missed economic opportunity and burden prevented
Long term follow up with subjects in clinical trials
Source: "Respiratory Syncytial Virus" presentation, Eric A.F. Simões, MB, BS, DCH, MD
Evidence Base: Conclusions and Key Takeaways
1. Evidence base in LIC/LMIC must be strengthened for neonates and young infants, who have the poorest data quality but highest predicted disease burden.
2. Efforts to improve the evidence base, both for burden of disease and vaccine efficacy, should include birth outcomes, fetal health, severe disease and hospitalization, and information from autopsies.
3. Diagnostic tools and guidelines must be improved and standardized to accurately estimate disease burden, especially for pertussis.
4. Tetanus may provide a good learning agenda for the maternal immunization platform.

19
Part 3: Regulatory Context and Session Goals Keith Chirgwin (BMGF, Deputy Director of Regulatory Affairs) Maternal immunization poses a unique challenge for regulators, who must consider the safety and efficacy not only for the pregnant woman who receives the vaccine, but also for the fetus and infant. Developers of maternal immunization vaccine candidates must design clinical trials to take into account specific requirements for licensure of a vaccine intended for pregnant women. After primary licensure, the vaccines must also achieve marketing authorization in the target low-income and lower-middle income countries (LIC / LMIC), a path that may be aided by World Health Organization (WHO) prequalification and regional regulatory partnerships such as the African Vaccine Regulatory Forum (AVAREF) and the African Medicines Regulatory Harmonization Programme (AMRH). The current vaccine candidates are at different points in clinical development, which provides an opportunity for companies to engage early with regulators, and design clinical programs that will achieve impact in LIC/LMIC soon after licensure. The goal of this session is to determine the unique challenges for maternal immunization in safety, efficacy, labeling, and regulatory pathways into LIC/LMIC, and to outline a path forward.
Regulatory pathways in LIC/LMIC and current vaccine status
Source: "Context and Session Goals" presentation, Keith Chirgwin 1. Lower middle income countries/lower income countries 2. EMA program which allows EMA to issue a scientific opinion for medicines not intended to be used in the EU. 3. Most advanced candidate. 4. Pre-qualification, 5. Pertussis toxoid, 6. 3-Valent Note: NRA – National Regulatory Agency; EMA – European Medicines Agency;

20
Vaccines for Use in Pregnancy, US Food and Drug Administration (FDA) Considerations Marion Gruber (US FDA)
Brief summary: Current FDA labels do not include prescribing information for pregnancy unless clinical trials have been performed in pregnant women, but this does not preclude the use of such vaccines during pregnancy. Indications for use in pregnant women would require clinical trials in pregnant women to demonstrate safety and efficacy. Depending on the specific vaccine, the FDA may consider alternative efficacy endpoints. Additionally, the FDA can provide advice to sponsors for the development of vaccines not intended for use in the US through its investigational new drug (IND) program. Labeling for maternal immunization vaccines in the US: US labeling provisions require that prescribing information summarizes the information essential for safe and effective use without implying indications or uses. As a result, although there are no vaccines specifically licensed for use during pregnancy in the US, this does not preclude their use for maternal immunization. Re-labeling a vaccine to include an indication specifically for pregnant women, however, would require clinical trials demonstrating safety and efficacy in this population. Starting in June 2015, the updated Pregnancy and Lactation Labeling Rule (PLLR) will alter labeling to allow manufacturers to provide a concise narrative of risks and benefits of administration during pregnancy based on human or animal data. This is intended to assist healthcare professionals in advising women on the use of drugs during pregnancy and lactation. Considerations for demonstrating safety and efficacy in pregnant women: In order to identify pregnant women as an intended subgroup in indications, product-specific safety and efficacy data in pregnant women must be generated in controlled studies with pre-specified endpoints. This applies equally to vaccines already recommended by global health bodies for use in pregnancy (influenza, Tdap) and to new vaccines (RSV, GBS). Clinical trials in pregnant women must assess safety in both mother and infant, including maternal adverse event monitoring, pregnancy outcomes, perinatal events, and postnatal events (infant growth and development). Assessments of clinical efficacy will depend on the intended indication, for example prevention of disease in mother, infant, or both. Alternative efficacy endpoints, for example maternal immune response, may be permissible but would require discussion with the FDA. Assuming sufficient safety and efficacy can be demonstrated, the FDA is willing to provide US licensure for vaccines intended for use outside of the US.
Ethical Considerations for Maternal Vaccine Research in Low Resource Settings Amina White (NIH Department of Bioethics)
Brief summary: Ethical guidelines for conducting maternal immunization research in low resource settings (e.g. LIC/LMIC) were provided, including how to ensure that the host country is not exploited and that all participants are provided a favorable risk/benefit profile.

21
Avoiding exploitation of the host country: It is unethical to exploit developing countries for the purposes of conducting a clinical trial. Exploitation occurs when a country receives an unfair level of benefit or is forced to carry an unfair burden of risk. A specific situation in which the latter may occur is in the design of clinical trial control groups: experimental intervention should not be tested against a no-treatment control but against the best proven therapy that is globally available and plausible to provide. Exceptions to this rule may be warranted if no effective intervention exists, if there is minimal harm in withholding the proven intervention, or compelling scientific methodological reasons require it (and there is no added risk of serious harm) (CIOMS 2002, 2013 Declaration of Helsinki). It is also important to avoid "helicopter research" performed in a community that will not receive the benefits of that research (e.g. in the case of clinical trials performed in LIC/LMIC but ultimately meant to benefit HIC alone). Ensuring a favorable risk/benefit profile for participants: All clinical trials involve a level of risk and the potential for benefit. Acceptable study risks are determined in relation to the prospect of benefit, and risks must be kept as low as possible without compromising study objectives. In the specific case of pregnant women, accurate risk assessment is challenging due to the tendency to overestimate the risk of intervention and underestimate the risk of failing to intervene. The Council for International Organizations of Medical Sciences (CIOMS) has also provided ethical guidelines specific to pregnant women, which states that research in pregnant women is acceptable when it is relevant to the health needs of the pregnant woman, fetus, or pregnant women in general and, when appropriate, reliable evidence from animal models is available regarding risks of teratogenicity and mutagenicity. In general, a good guideline to establishing a reasonable risk/benefit profile is to ask the question, "would an informed doctor recommend participation in the study, based solely on the risks and potential benefits to the participant?" Additional considerations: During the Q&A, several important questions were raised that were not decisively answered, but merit further discussion: (1) What balance should be struck between community ethics and individual ethics when deciding whether to conduct a clinical trial, and how does the physician's role as advocate for individual patients affect this balance? (2) How should the recommendations of international and local institutional review boards (IRBs) be weighted when they conflict, and how can local IRBs be engaged better and earlier? (3) Is it ethical to use vaccines off-label in pregnant women indefinitely, or are clinical studies ethically necessary? Panel: Safety, Efficacy, and Labeling Panel Lead: Keith Chirgwin (BMGF) Panel Participants: Patrick Zuber (WHO), Laurent Brassart (EMA), Boonchai Somboonsook (Thai FDA)
Brief summary: Panel participants discussed the clinical path to safety, efficacy, and labeling to support maternal immunization uptake in LIC/LMIC.

22
What should be considered in evaluating safety to support maternal immunization indications? There is a clear desire to establish safety more rigorously through controlled, randomized trials and careful monitoring of perinatal and postnatal adverse events. Doing so will require better measurements of the background adverse event rate in pregnant women, particularly in LIC/LMIC, in order to accurately evaluate the risks of maternal immunization. Ethical study design is a top priority, with recommendations that phase I trials to establish safety be performed in healthy, non-pregnant adults. The Thai FDA perspective is that approval of vaccines for maternal immunization by a strong NRA would also increase confidence and likelihood of uptake by LIC/LMIC. What should be considered in evaluating efficacy to support maternal immunization indications? The evaluation of efficacy in maternal immunization should ideally include several features. First, trials should be performed on pregnant women, and show clear efficacy either for the mothers, infants, or both. Immune response may be an acceptable endpoint if trial design precludes efficacy as an endpoint. Second, trials should ideally be randomized and controlled. Finally, it is important to show that protection of mothers and/or infants is of sufficient duration to have a significant impact. What is considered appropriate labeling to support a recommendation for routine use of a vaccine in pregnant women? Labeling for use in pregnant women must require rigorous safety and efficacy standards, and must be as clear as possible to assist healthcare professionals in safely and effectively administering the vaccine. Where labeling for pregnant women is not warranted due to lack of data, it is unclear whether a statement should be made to indicate that the product has not been tested in pregnant women. Doing so may avoid undue risk to pregnant mothers and to manufacturers seeking to avoid liability. However, there are cases in which the risks of not being vaccinated may outweigh the risks of vaccination, and such labels may do more harm than good. In these cases, the major challenge is to accurately communicate the risks of intervention versus nonintervention. Pharmaceutical companies must also be proactive in updating labels whenever possible to incorporate the latest safety and efficacy data. Regulatory Pathway (WHO Prequalification) Carmen Rodriguez Hernandez (WHO), Olivier Lapujade (WHO) Brief summary: The WHO prequalification program verifies the quality, efficacy and safety of vaccines to facilitate registration and use in developing countries. Attaining prequalification is essential for implementation of maternal immunization in LIC/LMIC, as it is required for major funding mechanisms. What is prequalification? Prequalification (PQ) is a service offered by the WHO to UN purchasing agencies. It provides an independent opinion on the quality, efficacy and safety of vaccines, and ensures that they are suitable for the target population. To achieve this, PQ evaluates the NRA of the export country, clinical data from vaccine trials, the vaccine manufacturing process, and the quality of the actual product to determine

23
whether it meets WHO requirements. If the vaccine is prequalified and licensed, the WHO also performs ongoing tests to ensure continued vaccine quality. Process of prequalification: Selection of new vaccines for PQ is performed on a priority basis determined in part by demonstrated need and efficacy. Once selected for PQ, a vaccine must go through 30-90 days of screening followed by ~ 270 days of internal time, something that is currently being optimized to reduce time to licensure. For already prequalified vaccines that require re-labeling, for instance in the case of adding an indication for pregnant women, only ~90 days would be required. This can be done simultaneously with NRA labeling approval to reduce total labeling time. Relevance to maternal immunization: The UN already supplies WHO prequalified vaccines for maternal immunization including vaccinations against tetanus and influenza. For vaccines with existing WHO prequalification but without a label supporting use in pregnant women, a labeling change will require that the responsible NRA for PQ to approve a label change followed by a type A approval by WHO PQ. Supporting data for such a label change may include clinical, pharmacovigilance, or other data. Challenges to WHO PQ for vaccines intended for use in pregnant women include a lack of currently available data supporting safety and efficacy, and reluctance from manufacturers due to liability concerns.
Regulatory: Conclusions and Key Takeaways
1. Clinical trials must satisfy stringent ethnical concerns, and provide sufficient safety and efficacy data, to result in an indication for maternal immunization.
2. There is limited data available on maternal immunization, and what is available may not be reflected in labeling. This may in part be addressed by the FDA pregnancy and lactation labeling rule (PLLR).
3. Accurate measures of disease burden and efficacy are crucial to establishing whether maternal immunization has a favorable risk/benefit profile.
4. A major challenge in effectively labeling vaccines for maternal immunization will be to accurately communicate the risks of intervention versus the risks of nonintervention, in order to avoid obstructive fears of vaccination in the face of serious disease.

24
Part 4: Policy
Context and Session Goals Jon Abramson (SAGE, Wake Forest Medical School), Elizabeth Mason (Former Director MNCAH, WHO) Brief summary: Maternal immunization policy straddles both Vaccine and Maternal, Newborn, and Child Health (MNCH) policy. As such, it is important to understand the policy setting landscapes for both, including key players and issues at the global level, and considerations for translating global policy to the country level. The goal of this session was to determine the requirements for maternal immunization policy recommendations by Vaccine and MNCH policy-makers at the global and country level.
Matrix view of potential policy-makers
Source: "Context and Session Goals" presentation, Jon Abramson. 1. Strategic Advisory Group of Experts on Immunization. 2. Reproductive health/ Maternal, newborn, child and adolescent health. 3. Reproductive maternal newborn child health
Vaccine policy: The Strategic Advisory Group of Experts on Immunization (SAGE) at the World Health Organization (WHO) is the normative global policy setter for Vaccines. SAGE receives inputs from multiple committees and partners to understand the evidence base and impact of a vaccine, in order to weigh the risks and benefits of a vaccination strategy and make its final recommendation. Other key players include regional and national technical advisory groups (NITAGs). Translating global policy recommendations to country-level policy is not always straightforward, as each country needs to prioritize and weigh the risk / benefit for each vaccine. The process for this assessment is often delayed in part because some NITAGs are more functional than others. Vaccine policy has typically focused on saving young children, but integration with MNCH will bring with it new emphasis on saving mothers as well, and on improving training for midwives and birth attendants.

25
MNCH policy: Global MNCH policy is determined primarily by United Nations agencies such as the WHO. National governments then set country level policy based on global recommendations, as well as inputs from expert advisory groups, donors and NGOs. Maternal mortality reduction has not made the same progress in the last few decades as under-5 mortality reduction. MNCH sees the potential integration of maternal immunization into the package of standard care for pregnant women as a significant step forward for their objectives. This approach has received interest from the WHO. Historical Vaccine Learnings Kate O'Brien (Johns Hopkins University)
Brief summary: This presentation detailed key learnings for driving adoption of new vaccines in the developing world, and how these learnings can be applied to maternal immunization policy discussions. Difficulty of accelerating vaccine adoption in LIC/LMIC: There are multiple stakeholders and activities that must be coordinated in an iterative fashion to enable policy recommendations, program introduction, and impact generation. During the Q&A, the idea of establishing maternal immunization as its own program similar to the expanded program on immunization (EPI) was largely dismissed in favor of greater integration with existing healthcare systems. Each vaccine also poses unique policy challenges, as does the setting (country) in which it will be used, requiring customized approaches to ensure success. Factors that influence the pace and extent of new vaccine adoption: Evidence of disease burden is the starting point for driving vaccine demand and adoption. Strategic planning for the investments needed to demonstrate disease burden starts with literature review, an assessment of how new data can change estimates, targeted study design, and adaptation of existing data to facilitate policy-making within countries. However, compelling disease burden and the existence of an efficacious vaccine are not sufficient criteria to drive country-level adoption. Adequate financing, consistent supply, and appropriate policy are also required. Financing solutions must be creative, long term, and tightly linked to the recommendations for vaccine usage; a particular concern raised during the Q&A was the financing situation for MICs that have graduated from GAVI and must therefore secure sustainable vaccine funding themselves. Supply issues can also disrupt adoption/impact and should be forecasted early and proactively. Finally, a strong global recommendation and appropriate country-level policy are essential for driving adoption both directly, and indirectly through facilitating financing and supply. Policy decisions will be influenced by technical alignment and consensus within the Vaccine and MNCH communities.

26
Factors that influence country-level policy setting
Source: "Historical Vaccine Learnings" presentation by Kate O'Brien
Implications for maternal immunization: Maternal immunization is largely considered to be in the "establish and organize evidence" phase. Key considerations for maternal immunization therefore include technical consensus on disease burden and the safety and efficacy of vaccines, a vaccine administration schedule, planning for adequate vaccine supply and financing, foresight into operational issues, plans for monitoring of impact and safety, and alignment of the specific implementation plan with global policy recommendations. Country-level policy decisions pose a particular challenge, and hinge on coverage, acceptability, feasibility, and affordability. Panel: Vaccine Policy - From Global to Regional/Country Panel lead: Helen Rees (WRHI and University of Witwatersrand) Panel participants: Azhar Raza (UNICEF), Fredrick Were (University of Nairobi, Kenya), Carla Vizzotti (MoH, Argentina), Adenike Grange (Former MoH, Nigeria) Brief summary: The main drivers of vaccine decision-making at a country level are burden of disease, safety, and cost benefit considerations. Confidence in the level of disease burden and vaccine safety may be bolstered by global recommendations (e.g. from the WHO), inclusion of maternal immunization within trusted existing programs, and efforts to increase buy-in at the community and healthcare provider levels. Understanding of country culture, structure and leadership will be important to successfully achieve buy-in at the country level. Appropriate representation of MNCH and vaccine policymakers on regional and country NITAGs would greatly improve country-level policy setting.

27
How can we drive global maternal immunization policy at the regional / country level? Driving maternal immunization policy at the country level will first require understanding the country's epidemiology, concerns and objectives. While most countries are concerned with the evidence base, efficacy and safety of vaccines in pregnant women, individual countries often have unique considerations or objectives that may not be fully understood by outside countries or policy makers.
Common country-level concerns include cost-benefit, whether long-term financing is secure enough to ensure a sustainable maternal immunization platform, the level of difficulty in integrating maternal immunization into existing antenatal care infrastructure (something requiring cooperation with MNCH), and whether the various internal stakeholders of a given country are properly aligned. In some places, there is enough evidence to begin advocating for and implementing maternal immunization today.
Due to their epidemiological profile (an already decreasing maternal and U5 mortality) capacity for stronger and more secure financing, as well as the relative strength of their ANC programs and capacity for pharmacovigilance, middle income countries may be an easier starting point for maternal immunization. Argentina's experience implementing maternal immunization for pertussis and influenza may provide a learning experience for the entire platform. New WHO Antenatal Care Guidelines and Relevance to Maternal Immunization Metin Gulmezoglu (WHO)
Brief summary: This presentation reviewed the current process for ongoing review and revision of antenatal care (ANC) guidelines at the WHO, and specific considerations that must be addressed for maternal immunization to be included in the new guidelines for the ANC.
History and purpose of WHO ANC guidelines: Since 2002, the WHO ANC Guidelines have served as a roadmap for countries describing which interventions should be included in ANC and when. Goals include health promotion, disease prevention, early detection of and treatment for complications, birth preparedness, and complication preparedness. Process for updating of ANC guidelines: ANC guidelines identify which evidence-based practices during the ANC period improve outcomes, and specify how these practices must be delivered to achieve impact. These guidelines are updated using the DECIDE framework (Developing and Evaluating Communication strategies to support Informed Decisions and practice based on Evidence) and input from expert panels. Importance of integrating new interventions within ANC: When considering routes to implementation of maternal immunization, an important consideration is its relationship to ANC. Consensus was reached that successful integration of maternal immunization into ANC would have better outcomes than a vertical maternal immunization program, due to the ability to leverage existing healthcare systems and the simplicity (for patients) of integrated care. However, successful integration is not guaranteed. Integration

28
challenges highlighted by the panel included the variable coverage and strength of existing ANC programs in different countries, and the risk that quality of care may decline in less robust ANCs that take on additional work relating to maternal immunization.
Percentage of women aged 15–49 attended at least once during pregnancy by skilled health personnel (ANC1) and percentage attended by any provider at least four times (ANC4), by
region, LDCs and world, 2009–2013
1. Data for China were available for the estimates of ANC1 but not for the estimates of ANC4. Source: UNICEF
Implementation research will be required to identify integration models that improve, rather than degrade, existing ANC strength, and in doing so will need to investigate patient flow planning, the potentially increased complexity of ANC visits due to maternal immunization, and how to minimize points of contact for pregnant women. Successful integration may provide benefits both to core health services and to maternal immunization-specific goals. Potential benefits of integration include increased compliance with multiple interventions (rather than losing patients during the referral process), improved monitoring of maternal and newborn health, and resulting improvements in health outcomes for mother, fetus and child. Achieving successful integration will require thoughtful discussion and alignment between the Vaccine Delivery and MNCH communities, and strengthening of existing ANC systems.
PMTCT Learnings Viviana Mangiaterra (The Global Fund)
Brief summary: This presentation described how the Prevention of Mother-to-Child Transmission (PMTCT) program, which targets HIV, successfully integrated into the ANC channel, and how key learnings from this process could be applied to maternal immunization. Interventions based on scientific evidence: A large body of scientific research was generated between 1994 and 2010 on the use of antiretrovirals (ARVs) for PMTCT in HIV, which demonstrated benefit both for mother and child. This strong evidence base, plus the observed benefit for mothers, was instrumental in the WHO shifting PMTCT from Option A (limited ARV therapy of pregnant women depending on CD4 count) to Option

29
B+ (life-long ARV therapy for all HIV-infected pregnant women regardless of CD4 count), which resulted in a range of benefits for mother, child, program delivery, and public health.
Programmatic and systems-related implications: Integration of PMTCT into ANC began by adapting common tools and instruments at the country level. In the case of Kenya, The Global Fund strengthened the ANC platform during integration of PMTCT by providing intermittent preventative treatment, integrating tuberculosis (TB) screening services into the program, improving training and monitoring services, developing a stronger supply chain for drugs and commodities, and waiving fees for skilled-care deliveries to minimize demand-side barriers. One key takeaway from this process was that during ANC integration, quality improvement of ANC and the overall health system can and should occur together. The WHO's reproductive, maternal, newborn, and childhood health (RMNCH) policy has supported interventions to achieve this goal strengthening a number of activities across the continuum of care by addressing financial barriers, improving monitoring, providing effective healthcare provider hiring, training and retention strategies, and providing standard operating procedures for supply-chain integration and delivery of PMTCT through ANC.
Coverage of MNCH interventions across the continuum of care (African region, 2012)
Source: WHO/UNICEF 2013. PMTCT from WHO, UNICEF, UNAIDS Global HIV/AIDS Response, Progress Report 2013
Community involvement: Effectively leveraging the local community for successful PMTCT required both practical steps to target pregnant women, and efforts to engage them and their families. Practical steps included targeting young pregnant women for treatment, offering family-centered care with joint appointments, and providing a role for mentor mothers and Civil Society Organizations (CSOs). Efforts toward personal

30
engagement emphasized respectful treatment of clients, empowerment of clients and their families with health knowledge, creation of an environment of confidentiality and trust, and ensuring that patients understand the importance of following up with healthcare providers. Political and financial commitment and leadership: Strong country- and global-level buy-in for PMTCT was facilitated by The Global Plan towards the Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive. The financial support that followed this political commitment resulted in ~$200M in funding.
Comparison with and implications for maternal immunization: PMTCT provides a number of lessons for maternal immunization, particularly surrounding buy-in. The Global Fund's perspective is that greater buy-in from countries and key stakeholders is essential to drive action. This will require that maternal immunization have positive overall outcomes for both child and mother, that evidence for this is packaged in a palatable way for policy-makers, and that vaccine delivery is simple enough to drive adoption (something that should be reflected in target product profiles). Driving buy-in is difficult, and will require the maternal immunization community to make decisions on which countries should be their highest priority targets for maternal immunization.
Comparison of PMTCT and maternal immunization
Strategic Approach/Considerations PMTCT
Maternal Immunization
Scientific Evidence √ Partial, and must be packaged for policy-makers.
Operational & Programmatic Implications √ Must be better determined
Financial Support & Potential Partnership √ Will require country and financier buy-in
Political Commitment and Leadership √ BMGF helps, but country-level buy-in needed
Relevance for countries √ Must offer value within different national priorities
Source: "PMTCT Learnings" presentation, Viviana Mangiaterra
Panel: MNCH Policy Advancement & Integration with Vaccine Policy Panel lead: Elizabeth Mason (Former Director, WHO MNCAH) Panel participants: Charles Mwansambo (Health Services, Malawi), Abdullah Baqui (Johns Hopkins University), Ana Langer (Harvard School of Public Health), Martina Baye (Ministry of Public Health, Cameroon) Brief summary: The panel identified a number of policy focus areas for maternal immunization, and highlighted that the challenge was to prioritize them or identify opportunities to push them forward in parallel. Focus areas included (1) Critical factors for MNCH policymaking such as evidence, simplicity, commodity supply, health worker training and financing; (2) Developing an integrated MNH task force with inputs from the vaccine community to allow broad-based policy development; (3) The need to involve pregnant women and other stakeholders in policy discussions; and (4) The use of IT and health indicators to enable data-driven policy decisions.

31
What are the key challenges to drive towards global, regional, and country level MNCH recommendations for maternal immunization? Major challenges to MNCH recommendations for maternal immunization include a lack of disease burden and health impact information, supply chain difficulties, lack of vital registration, the impact of background disease burden on maternal immunization safety and efficacy, and the availability of human resources and vaccine supply. Many of these issues could be resolved by better understanding the disease burden both addressable and non-addressable by maternal immunization, by integrating maternal immunization into ANC, by obtaining a favorable recommendation from SAGE, and by securing sufficient financing to ensure sustainable provision of human resources and vaccine supply (and strengthen ANC in the process). How can vaccine and MNCH policymakers coordinate to enable maternal immunization? The maternal health task force is working to integrate MNCH and other initiatives, but there are multiple models by which maternal immunization might be integrated into MNCH and/or ANC that should be considered. Regardless of the integration model pursued, important considerations include ensuring that pregnant women's needs come first, that the final integrated structure is simple, and that care is organized and tracked effectively. Organizational simplicity was highlighted in a discussion after the talk, and consensus emerged that integration of maternal immunization with existing programs is essential to minimize resource use and ensure compliance. An anecdote was shared that before PMTCT was integrated with ANC, referrals from one group to the other did not work, even though they were located down the hall from one another. Tracking, potentially enabled by new technology, will also be important to monitor coverage and outcomes.
Policy: Conclusions and Key Takeaways
1. A strong global recommendation on vaccine safety and efficacy for maternal immunization is essential, but not sufficient on its own, for country-level uptake.
2. Major country-level considerations for maternal immunization include safety, local burden of disease, cost-benefit considerations, integration into the current health system, and the sustainability of financing.
3. Mechanisms must be put in place to ensure buy-in from key country-level stakeholders, including the political leadership, media, individual communities, NITAGs, and regional TAGs.
4. Integration of maternal immunization into MNCH/ANC will require a focus on the health of both child and mother, solid burden/efficacy data, simplicity of vaccine delivery, adequate vaccine supply, and health worker training.
5. Integration may benefit MNCH/ANC, but only if an appropriate integration model and sustainable financing are available.

32
Part 5: Market Dynamics Context and Session Goals Greg Widmyer (BMGF) Supply-side challenges for maternal immunization vaccines, a major focus of this session, revolve around the ability of pharmaceutical companies to ensure appropriate products, adequate volumes, and affordable prices, and vary by pathogen, vaccine development stage, and company type. Broadly speaking, these challenges include uncertain demand for new interventions, lower pricing structures (with pressure to show high cost-effectiveness), weak burden data and surveillance systems, challenging logistics for integration, complex regulatory pathways, and litigation risk. Despite these challenges, manufacturers may realize significant benefits. These include the potential for larger volumes to improve manufacturing economics, incremental revenue from new markets, goodwill from meeting important unmet needs in maternal and child health, and improved access to growing distribution channels. The global health community has many tools it can deploy to work with pharmaceutical companies to address challenges to the supply and demand of maternal vaccines in low-income and lower-middle-income countries (LIC/LMIC). Three Companies' Perspectives on Maternal Immunization: Jean Francois Toussaint (GSK), Russell Wilson (Novavax), Su-Peing Ng (Sanofi)
Brief summary: GlaxoSmithKline (GSK), Novavax and Sanofi Pasteur have identified key drivers and challenges for supplying maternal immunization globally and in LIC/LMIC, as well as a number of opportunities to address these challenges.
Status of vaccines: A number of vaccines are currently available to pregnant women (PW) or in clinical trials.
Partial list of vaccines available to support pregnant women from GSK and Sanofi
Vaccine Manufacturer Pathogen(s) WHO-PQ?
Fluarix GSK Influenza No
FluLaval GSK Influenza Yes
Fluzone Sanofi Influenza Yes
Vaxigrip Sanofi Influenza Yes
Pandemrix GSK Influenza (Pandemic) Yes
Panenza Sanofi Influenza (Pandemic) Yes
Tetavax Sanofi Tetanus (Toxoid) Yes
Boostrix GSK Tetanus, Diphtheria and Pertussis Yes
Adacel Sanofi Tetanus, Diphtheria and Pertussis No
Source: GSK and Sanofi product lists and WHO Vaccine Quality website, http://www.who.int/immunization_standards/vaccine_quality/PQ_vaccine_list_en/en/

33
Several GSK and Sanofi vaccines currently available to PW are listed below (though evidence to support use in PW is variable). GSK is also developing a Respiratory Syncytial Virus (RSV) vaccine specifically for maternal immunization. The vaccine has completed a phase 1 safety trial in non-PW, with clinical trials in PW expected in 2015. The Novavax vaccine program includes an RSV candidate for maternal immunization in phase 2 and seasonal and pandemic flu vaccines.
Drivers of maternal immunization (and LIC/LMIC) programs: Company interest in maternal immunization is driven by the significant potential for medical benefit, especially given the lack of pediatric vaccines capable of addressing the neonatal disease burden. This is particularly true in LIC/LMIC, where disease burdens are typically large and attitudes are often more favorable toward vaccinating PW. Growing evidence of a favorable risk/benefit ratio for immunizing PW with commercially available vaccines has catalyzed interest in maternal immunization among companies and in the global health community. Manufacturers may also benefit from incremental revenues from producing additional vaccine (especially when additional capacity is available, e.g. in the case of influenza), economies of scale resulting from larger production volumes, the goodwill associated with global health work, and the potential for novel vaccine development for LIC/LMIC to pave the way for supplying the same vaccines in HIC, where larger profits may be realized (e.g. in the case of Group B Streptococcus (GBS)).
Challenges of maternal immunization (and LIC/LMIC) programs: Market dynamics challenges are different for different pathogens (e.g. currently available influenza vaccines are appropriate for use in LIC/LMIC but seasonality will present a challenge for supply; for pertussis, however, seasonality is not an issue, but cheaper and simpler manufacture is required to make an attractive vaccine for LIC/LMIC). All three manufacturers agreed, however, that there are a number of general challenges to incentivizing supply and generating demand for maternal immunization. These fall into several categories, including evidence base and market size, demand forecasting, R&D feasibility, product development, policy, funding, implementation and vaccine coverage, and post-marketing challenges: Evidence base and market: manufacturer commitment to supplying a vaccine will depend on the existence of a market for the vaccine. Demonstrating sufficient evidence of disease burden for a given pathogen, evidence of safety and efficacy for maternal immunization against the pathogen, and demand for the vaccine (by patients, healthcare providers and global and country-level stakeholders) will be essential for stimulating vaccine supply. It is possible for there to be insufficient demand despite sufficient evidence base, in which case education and advocacy may be necessary to stimulate demand. An important consideration is whether safety and efficacy are sufficient in specific countries, which may vary considerably in terms of background disease burden (e.g. HIV, malnutrition, malaria) and existing healthcare practices (e.g. will co-administration of new vaccines with TT or Tdap be necessary?). Demand forecasting: A major challenge specific to LIC/LMIC is the inability to accurately forecast demand, a key prerequisite for planning production capacity. Demand forecasts

34
require estimates of disease burden and country/population level interest; however, these represent key knowledge gaps in LIC/LMIC. As vaccine efficacy will also influence demand, additional knowledge gaps include the effects of country-specific health burdens (e.g. background disease, malnutrition) and pathogen strain and seasonality (particularly in the case of influenza) on vaccine efficacy. Reducing R&D Risk: De-risking R&D requires ensuring that intellectual property is permissive to product development, that clinical endpoints are accessible through clinical trials and acceptable to regulatory bodies (e.g. efficacy versus immunogenicity), and that the size, cost, and level of risk of requisite clinical trials are both achievable for the manufacturer and attractive to it. If not, appropriate incentives and partnerships will need to be provided to make it both possible and attractive. Enrollment of PW in clinical trials may also be challenging, both from an ethical and regulatory perspective and in achieving sufficient interest from patients and healthcare providers. Product development and regulation: product development challenges may be categorized as ethical, technical, or regulatory. Ethical challenges include informed consent and whether a vaccine's benefits will include the vaccinated mother. Technical challenges include developing simpler, cheaper vaccines for some pathogens (e.g. pertussis), ensuring the vaccine adequately protects infants, ensuring capacity is sufficient for the desired level of production, and co-administration of novel and existing vaccines. Regulatory challenges include product registration and labeling for use in PW. Sanofi, for example, stated that it uses Canada, Europe and the US as "reference jurisdictions" to govern the content and format of labeling sections relating to pregnancy and facilitate the WHO prequalification process, but indicated that regulatory pathways for licensing vaccines specifically for use in PW remain unclear due to the lack of a harmonized regulatory framework. Policy: Obtaining favorable country-level policies and global policy recommendations for maternal immunization requires overcoming several other of the hurdles already mentioned, including developing a solid evidence base and investment case, generating individual- and country-level demand, and establishing momentum around maternal immunization among global health providers (e.g. WHO, GAVI). Funding: Companies highlighted the need for sustainable financing to ensure that their investments into providing vaccines in LIC/LMIC achieve sufficient return-on-investment (ROI). Innovative financing tools (e.g. volume guarantees, capital expenditure subsidies, volume buy-downs, etc.) to de-risk both technical and manufacturing investments may need to be applied to ensure that LIC/LMIC markets are served. It will also be important to design vaccines with product characteristics that attract funding (e.g. what labeling and product profiles are required for GAVI funding?). Implementation and vaccine coverage: challenges here emanate both from technical difficulties and individual perceptions. Technical challenges emanate from the need to achieve simultaneously high coverage (particularly in LIC/LMIC) and adequate supply (e.g. through properly managing the supply chain, cold chain, and storage) while

35
maintaining the integrity of the healthcare system through which supply is achieved (e.g. ensuring the ANC channel is not overburdened by maternal immunization). Perceptions of maternal immunization are also important: PW, obstetricians, and other healthcare providers may not be fully aware of the relative risks of pathogen infection versus maternal vaccination, and education may be required. Post-marketing challenges: Post-marketing challenges include pharmacovigilance and liability for manufacturers. Pharmacovigilance may be difficult for maternal immunization due to the need to track both mother and infant, and poses a special challenge in LIC/LMIC due to poor infrastructure and patient tracking. Concern over liability for adverse events during pregnancy is also a key hurdle for maternal immunization. The high background rate of adverse events in pregnancy makes it difficult to determine causality once an adverse event occurs during pregnancy, particularly in LIC/LMIC where pharmacovigilance is challenging. Company perspectives on where the maternal immunization community can provide supply-side support: Interventions to support maternal immunization globally
Assemble expert group to clarify maternal immunization liability risk, using US Vaccine Injury Compensation Program (VICP) as precedent
Assemble an independent ethics panel to advise the maternal immunization community
Measure the background adverse event rate in PW in different settings (HIC, MIC, and LMIC/LIC) to help understand vaccine safety in PW.
Increase R&D to expand the range of vaccine targets, improve immunogenicity, increase safety, and decrease cost
Develop and clarify regulatory pathways to licensing and labeling of vaccines for use specifically in pregnant women.
Interventions to support maternal immunization specifically in LIC/LMIC
Perform comprehensive overview of maternal immunization in LIC/LMIC and develop an effective strategy going forward
Generate evidence for disease burden, demand, & risk-benefit profile
Generate transparent, robust demand forecasts for market sizing
Better understand the effects of background disease burden (e.g. HIV, malaria, malnutrition) on maternal immunization safety and benefits
Begin discussing and securing funding / policy recommendations
Create a path to ensuring the sustainability of funding
Fund mfg. capacity and/or long-term purchase/price commitments
Fund and/or share clinical development costs
Accelerate the path to meeting regulatory requirements for LIC/LMIC, obtaining WHO prequalification, and delivering vaccines in LIC/LMIC.
Understand product characteristics & labeling required to support GAVI funding
Improve obstetric/healthcare provider education and training on safety, legal risks, risks of vaccination, and risks of not being vaccinated

36
Improve delivery logistics including supply chain, storage & cold chain
Develop and strengthen distribution and pharmacovigilance systems for measuring safety, efficacy and specific health outcomes
Most critical activities that the global health community should undertake in the next 1-2 years
Source: presentation by Dr. Su-Peing Ng, Sanofi-Pasteur. POC = proof of concept.
Panel: Enablement Levers Panel lead: Greg Widmyer Panel participants: Bruce Gellin (HHS), David Kaslow (PATH), Kim Bush (BMGF), Melissa Malhame (GAVI) Summary: There is a need, varying by pathogen, for additional data around disease burden and potential health impact via maternal immunization. The maternal immunization community must also produce greater clarity on the background rate for adverse events. Additional enablement levers focus on liability issues, ethical concerns, demand forecasts and target product profiles (TPPs). What "push" and "pull" mechanisms can the maternal immunization community leverage to promote development and supply of maternal immunization vaccine by pharma? Mechanisms for the foundation and the community as a whole to "push" pharma in the direction of maternal immunization include product development funding (including PDPs), purchasing equity stakes in early stage startups pursuing maternal immunization objectives, and providing technology assistance grants. Mechanisms to "pull" pharma toward maternal immunization on the supply side include supply volume guarantees and

37
purchase prepayments. Interventions that straddle these "push" and "pull" approaches include capacity scale-up loans, and co-investment approaches that involve the participation of other global health entities.
What are the most critical activities that the global health community should undertake in the next 1-2 years?
Establishing disease burden and evidence base for attractive risk-benefit profile of maternal immunization in LIC/LMIC. This will be essential to create demand among pregnant women, healthcare providers, and country-level stakeholders (e.g. ministers of health and finance, NRAs).
Measuring background adverse event rates in pregnant women and establishing a clear liability landscape for manufacturers and other stakeholders. Mechanisms for risk-sharing to protect manufacturers should also be discussed.
Creating predictability for manufacturers through unbiased strategic demand forecasts and minimum product profiles or TPPs. GAVI experience may be informative here, and WHO should be engaged for TPP development.
Identifying potential product development models that may be attractive for each pathogen, including:
o Development of vaccine in HIC, followed by adaptation for LIC. Tiered pricing model applied.
o Development and commercialization exclusively in LIC/LMIC (no demand in HIC). Paths to sustainable financing will have to be considered.
o Development and commercialization in LIC/LMIC first, where burden may be greater and demonstrations of efficacy may be more facile, followed by expansion to higher-margin HIC market.
Market Dynamics: Conclusions and Key Takeaways
1. Manufacturers face several common challenges in supplying vaccines for maternal
immunization, including incomplete knowledge of disease burden and market, need for strengthening of evidence base for safety and efficacy (especially in LIC/LMIC), R&D risk, unclear regulatory paths for pregnant women, concerns regarding ethics and liability, need for sustainable financing, and limited ANC/HCP strength and coverage in low-resource settings.
2. Public-private partnerships are key to overcoming these challenges, for instance through product development relationships, and methods of incentivizing supply (e.g. guaranteed sales volume and purchase prepayment).
3. In the next 1-2 years, critical activities for the global health community to undertake in partnership with manufacturers include establishing stronger evidence base for disease burden and risk-benefit of maternal immunization, assessment of background adverse events in pregnancy and liability landscape, creation of strategic demand forecasts and TPPs, and identification of pathogen-specific product development models that provide a plausible path to vaccine development and licensure for maternal immunization.

38
Part 6: Funding Context and Session Goals Elizabeth Mason (Former Director, WHO RMNCAH) Vaccine and Maternal, Newborn and Child Health (MNCH) efforts in low-income and lower-middle income countries (LIC/LMIC) are supported by a mixture of private donations and country spending. Non-governmental vaccine funding is chiefly coordinated by GAVI, which is expected to account for ~85% of the ~$11B total vaccine spend in LIC/LMIC from 2016-2020. The MNCH donor landscape is larger but more fragmented: in 2010 individual countries spent ~$50B while donors provided only ~$6.5B, although the World Bank Global Financing Facility, currently under design, may serve as a coordinating and consolidating body for MNCH funding in the future.
High-level donor funding landscapes for vaccination and MNCH
Source: "Context and Session Goals" presentation, Elizabeth Mason. 1. Global Financing Facility.2. Expanded Program on Immunization. Source: "The 2016-2020 Investment Opportunity", GAVI, May 2014; Hsu, Justine, et al. "Countdown to 2015: changes in official development assistance to maternal, newborn, and child health in 2009–10, and assessment of progress since 2003." The Lancet 380.9848 (2012): 1157-1168.
For maternal immunization there is the potential to create a joint funding structure to collaboratively cover the most significant cost buckets. Prior to funding, however, maternal immunization would need to be evaluated and approved by potential donors, a process that will likely include a 2018 GAVI Vaccine Investment Strategy (VIS) evaluation and other related MNCH evaluations. The overall goal of this session was to identify requirements for funding and push toward maternal immunization procurement and delivery funding from both Vaccine & MNCH (and national vs. global) perspectives.

39
How Does GAVI Make Funding Decisions? Judith Kallenberg (GAVI)
Brief summary: In the 2013 VIS analysis, GAVI evaluated maternal immunization for influenza but decided against including maternal influenza in its portfolio. Reasons included uncertainty of health impact size, low country demand, and logistical supply challenges for seasonal vaccines.
GAVI overview: GAVI's four strategic goals are vaccine uptake, health system strengthening, global financing, and market shaping. GAVI has supported a wide range of vaccines include pentavalent, Hep B, HiB, measles, pneumococcal, rotavirus, meningitis B, IPV, HPV, measles/rubella, cholera, yellow fever and Japanese encephalitis. The GAVI Vaccine Investment Strategy (VIS): To decide which vaccines to fund, GAVI performs an analysis of potential vaccines every 5 years. The most recent of these was VIS 2013, and inclusion criteria included Phase IIb or III clinical trials and expected licensure by 2019. Hitherto, RSV and GBS were therefore not included because phase 2b safety and efficacy data were not available, and tetanus and pertussis were not included because GAVI already supports pentavalent immunization in the infant schedule. Maternal Immunization for influenza was considered, however. Primary evaluative criteria for vaccines included the anticipated health impact on morbidity and mortality, additional health and equality considerations, the feasibility of implementation, and the cost-effectiveness of intervention. Information requirements for evaluation included quantitative estimates of disease burden and impact, efficacy in different target populations, cold chain and other delivery logistics, and forces shaping vaccine supply and demand. Shortlisted candidates from this process in 2013 included cholera, maternal influenza, IPV, Rabies, malaria and yellow fever.
GAVI VIS evaluative criteria and indicators for comparison across vaccines
Category VIS Criteria Phase I Indicator
Health impact
Child mortality U5 future deaths averted, 2015 – 2030
U5 future deaths averted per 100k vaccinated population
Overall mortality Total future deaths averted, 2015 – 2030
Total future deaths averted per 100k vaccinated population
Overall morbidity
Total future cases averted, 2015 - 2030
Total future cases averted per 100k vaccinated population
Long-term sequelae
Additional impact consid-erations
Epidemic potential Epidemic potential of disease
Global/regional health Presence of global / regional (UN) resolution on elimination
Herd immunity Herd immunity threshold
Other interventions Current alternative intervention use & potential for scale-up
Socio-ec. inequity Disproportionate impact on poor

40
Gender inequity Disproportionate impact on one gender
Regional importance Burden concentrated in GAVI country subset in same region
Implemen- tation feasibility
Capacity & suppliers Capacity to meet GAVI demand, # of manufacturers by 2020
Market shaping potential GAVI demand as % of global demand
Supply chain integration Packed volume (cm3) compared to benchmarks
Program integration Alignment with existing vaccine and health worker practices
Vaccine safety, efficacy Efficacy (by clinical endpoints) & safety (causal link to SAE)
Cost and value for money
Vaccine procure. cost Total procurement cost to GAVI and countries, 2015 – 2030
In-country op. costs In-country operational cost per vaccinated person
Procurement cost averted Procurement cost per death / case averted
Source: Adapted from presentation "How does GAVI make funding decisions?” Judith Kallenberg
Key elements of the 2013 VIS maternal influenza vaccine evaluation: Key benefits of maternal influenza vaccination include the potential health impact for three high-risk groups (pregnant woman, fetus, and child) and the potential impact on vaccine markets, which are not currently set up to provide seasonal supply. Key challenges included the uncertainty of health impact size, the logistics of seasonal vaccine supply, and poor awareness of and demand for influenza vaccines among countries, pregnant women, and healthcare workers. The Gavi Board decided against opening the funding window for maternal influenza in 2013 given the limited evidence base for impact beyond pregnant women, but agreed to re-evaluate in VIS 2018 when better data would be available.
Information required to support re-evaluation of influenza as part of 2018 VIS: Further information needed to support maternal influenza in VIS 2018 includes the health impact beyond pregnant women, supply and logistics for seasonal delivery, and strategies to drive demand. In addition to maternal influenza, GAVI will likely evaluate also evaluate pertussis, tetanus, GBS, and RSV as part of the 2018 VIS.
USAID MNCH Program Priorities Claudia Morrissey Conlon (USAID)
Brief summary: The United States Agency for International Development (USAID) is committed to improving maternal and newborn health. It views maternal immunization as a potential intervention to be funded primarily through contributions to GAVI.
Overview of USAID goals and mission: USAID's mission is to end preventable child, maternal, and newborn deaths by 2035 in 24 priority countries. Additional USAID endorsed goals include the Every Newborn Action Plan, Ending Preventable Maternal Mortality, and Family Planning 2020. USAID has made five strategic shifts to meet development goals. These include increasing efforts in countries accounting for the largest share of under-five and maternal deaths, reaching the most vulnerable populations, targeting priority causes with innovations and proven interventions, investing to create an enabling environment for women and girls, and increasing transparency and

41
accountability at all levels. USAID has a particular focus on tracking of mothers and newborns to ensure accountability for, and success in, health outcomes.
USAIDs current funding activity: USAID's FY 2015 budget for maternal and child health (MCH) is ~$715M, of which ~28% goes to GAVI, and ~59% goes to 24 priority countries in the African and South East Asian Regions. Beyond their funding portfolio, USAID hopes to have broader impact in the MNCH community by coordinating disparate MNCH activities for governments and key stakeholders, and identifying novel financing opportunities.
USAID perspective on maternal immunization: USAID funds immunization primarily through GAVI, and supports country-led policies and programs for antenatal care (ANC). USAID views maternal immunization as part of ANC rather than a stand-alone intervention. USAID is interested in ongoing participation in this emerging technical area as additional evidence is generated on the disease and economic burden of the diseases targeted through maternal immunization. Global Financing Facility in Support of Every Woman Every Child Christina Schrade (SEEK Development)
Brief summary: The Global Financing Facility (GFF) is a MNCH funding body orchestrated by the World Bank. It is currently in the planning phase, including developing strategies to quickly scale up. Its goal is to increase efficiency and effectiveness of RMNCH investment while also supporting long-term domestic financing.
The need for GFF: There are many challenges to reducing maternal, newborn and child mortality, including inefficient use of current Reproductive, Maternal, Newborn, Child, and Adolescent Health (RMNCAH) funding due to poor targeting and fragmented financing, a lack of adequate vital statistics systems, and a ~$30B funding gap. Reaching the 2030 Sustainable Development Goals currently under development will only be possible if this ~$30B funding gap can be closed. The GFF's goal is to scale up sustainable investments to meet this funding gap and prevent ~4M maternal deaths, ~107M child deaths, and ~22M stillbirths by 2030. The initial focus will be on countries with the largest financing gaps and needs. The GFF has already received commitments from Canada, Norway, the U.S. and the International Development Association (IDA). GFF investment approach: The GFF takes a systematic approach to channel donor and domestic resources to fund investments with clearly defined plans for sustainable long-term domestic support. Key focus areas for the GFF are mobilizing additional domestic and international resources, supporting the transition to long-term sustainable domestic financing for RMNCAH, and scaling up civil registration and vital statistics, with a focus on the 63 high burden LIC/LMIC countries that account for ~92% of maternal and ~87% of childhood deaths. The GFF's goal is to integrate and prioritize existing and novel funding sources in the short, medium and long-term. This will be achieved in part by focusing on interventions capable of garnering broad support, including needs assessment, best buy

42
interventions, delivery strategies, and resource mapping. All interventions will be determined and prioritized using a data-driven approach.
Approach to sustainable long-term financing: The GFF will base funding decisions on the RMNCAH investment case, which looks at investments on a ~3-5 year timeline and prioritizes interventions that are cost effective and can be supported by multiple financiers. This is complemented by a long-term financing strategy to ensure that by 2030 sustainable financing for these interventions is available from both public and private sources. Their process involves working long-term with financiers and other sectors to coordinate in-country efforts, produce financing assessments, achieve mobilization of country resources, resolve critical bottlenecks, identify opportunities for cost reduction, make policy changes, and sustain the gains achieved by other development partners as countries transition to higher income levels.
Visualization of GFF path towards universal coverage of RMNCAH interventions
Source: "Global Financing Facility in Support of Every Woman Every Child" presentation, Christina Schrade.

43
Panel: Donor Perspectives Panel lead: Elizabeth Mason Panel participants: Adenike Grange (former Nigerian MoH), Judith Kallenberg (GAVI), Viviana Mangiaterra (The Global Fund), Susan McKinney (USAID), Carla Vizzotti (Argentina MoH) Brief summary: The goal of this panel was to identify current donor perspectives on maternal immunization as a funding target, including ways to structure funding along Vaccine and MNCH axes and on country/global levels. What are the current perspectives on maternal immunization as a funding target for the Vaccine and MNCH communities at the global and country level? There is agreement among donors that the global health community must enhance understanding of the investment case for maternal immunization, including better estimates of disease mortality and morbidity, impact, and opportunity cost. Even with a stronger investment case, donors will not fund maternal immunization efforts until country buy-in has been achieved. This is particularly important as it will be essential for individual countries to provide funds and a sustainable future financing plan.
What is a potential funding structure for maternal immunization among the various contributors? For maternal immunization there is the potential to create a joint funding structure to collaboratively cover the most significant cost buckets. One potential funding structure is procurement and supply chain cost being covered by Vaccine donors, while integration of maternal immunization into the ANC delivery channel could be funded through MNCH channels. Partnership between donors and countries will also be required. While GAVI funding has been successful, domestic financing is essential for program sustainability. Whatever structure is pursued, it should be simple to understand (in order to encourage financing and implementation) and connected to country-level representatives. What would encourage a platform-based funding environment rather than isolated pathogen/geographical efforts? While platform-level funding is attractive, USAID's perspective was that differing levels of disease burden and potential impact for different pathogens in different countries may require a more pathogen- or country-focused funding model, at least while an evidence base for maternal immunization is being built. GAVI's perspective is that maternal immunization is not a platform at all, but rather part of the maternal and newborn care platform, and therefore likely to be subject to the same funding environment as MNCH. One suggestion was that, due to the stronger MNCH and ANC systems in MIC, it may be an effective strategy to begin maternal immunization there in order to build up an evidence base and develop learnings that can be imported into LIC/LMIC.

44
Funding: Conclusions and Key Takeaways
1. Evidence base for disease burden & health impact are a top consideration for funding decisions. Morbidity is currently considered less significant but requires enhanced attention. Calls have been made to place greater importance on morbidity.
2. Funding decisions vary by country in LIC/LMIC due to different sets of priorities, and the value proposition of maternal immunization is likely stronger in MIC than LIC/LMIC.
3. Country-level funding is essential and supplemented by Vaccine and MNCH donors.
4. Simple financing mechanisms (e.g. a combination of GAVI, GFF and country support) will likely be needed to integrate maternal immunization into ANC, and should focus on integrated solutions (e.g. healthcare channel integration, combination vaccines) that minimize complexity and maximize impact.

45
Part 7: Implementation Context and Session Goals Nina Schwalbe (UNICEF) Successfully implementing maternal immunization will require a three-prong approach: encouraging vaccine acceptance to drive demand, carefully integrating maternal immunization into existing healthcare systems to ensure supply without disrupting other services, and monitoring the safety and impact of interventions.
Strong vaccine acceptance is possible through proactive community engagement and communication at the country and global level. Delivery of maternal immunization should be through an integrated rather than vertical program.
Delivery through antenatal care (ANC) will require support from stakeholders in the existing ANC system, and understanding and addressing the many logistical challenges of integration into the system without disrupting current services.
Establishing adequate monitoring of safety and impact will require a better understanding of background disease burden and adverse events, and is best accomplished through an active surveillance system.
The goal of this session was to determine challenges in demand generation, vaccine supply enablement, and safety/impact monitoring of maternal immunization, and outline a path forward.
Demand generation at the country and population levels
Source: "Context and Session Goals" presentation, Nina Schwalbe
Key learnings from tetanus efforts: Many learnings from the implementation of maternal and neonatal tetanus elimination (MNTE) efforts are broadly applicable to maternal immunization. These include the importance of ANC providers in driving acceptance of vaccination by pregnant women, and the potential value of coordinating and incentivizing expanded program on immunization (EPI) and ANC channels to work

46
together to jointly implement maternal immunization. Tetanus vaccination was introduced before being offered for maternal immunization and may therefore have eased acceptance through ANC. Maternal Immunization: Why Confidence Matters Pauline Paterson (LSHTM, The Vaccine Confidence Project) Brief summary: This talk describes the importance of vaccine confidence in improving vaccine uptake and minimizing outbreaks due to vaccine hesitancy, and strategies for improving vaccine acceptance in low-income and lower-middle income countries (LIC/LMIC). Relevance of vaccine confidence: Confidence in the safety and efficacy of vaccines, among both pregnant women and healthcare providers, is central to driving adoption. The beliefs of providers and pregnant women directly affect vaccination rates, and a temporary decrease in the vaccination rate of a birth cohort can have dangerous implications. In 2003, a polio vaccine boycott in Nigeria led to outbreaks in more than 10 countries. Unwarranted sterilization concerns have also derailed some tetanus efforts.
Findings on vaccine confidence: Research on attitudes toward vaccination has been performed. Media sentiments toward vaccines were tracked and found to mostly support vaccination, with confidence increasing over time; however, this may only be the case in high-income countries, as there is limited data on vaccine acceptance in LIC/LMIC. In these countries, there is a need for better tools to measure attitudes toward vaccination in order to accurately inform strategies for driving demand. This will be especially important in maternal immunization, where safety concerns are greater than usual due to the vaccination of pregnant women. Strategies to increase vaccine confidence: Strategies to increase vaccine confidence should include building trust prior to implementation, as well as training healthcare providers and public media to understand the true risks and benefits of vaccination.

47
Panel: Barriers to Demand, Uptake and Maternal Immunization Integration into ANC Panel lead: Nina Schwalbe (UNICEF) Panel participants: Martina Baye (Cameroon), Sylvia Deganus (Ghana) Lisa Noguchi (JHPIEGO), Pauline Paterson (LSHTM)
Brief summary: This panel addressed major challenges to implementing maternal immunization in LIC/LMIC through the ANC channel, including challenges in demand generation at the patient, provider, and community levels, demonstration of maternal health benefits, and ANC/EPI integration issues. Is vaccine acceptance a key issue for maternal immunization in pregnant women, and how can we increase acceptance either directly or through other stakeholders? Tetanus was used as an example to demonstrate that if mothers are aware of the diseases a vaccine is targeting, are aware of the benefits of vaccination to themselves and to their children, and believe in the safety of the vaccine for themselves and their children, then vaccine acceptance and uptake will likely be high. Belief in the safety of a vaccine requires community engagement, and ideally a strong one-on-one connection between pregnant women and vaccine providers. Providers must also endorse the vaccine, provide quality information, and make clear the intended outcome of the vaccine (i.e. what are we vaccinating against and why). An example where poor trust between healthcare providers and patients undermined vaccination efforts was provided: a measles outbreak occurred in Thailand due to fear among refugee populations that the vaccinations were efforts by the Thai government to poison them. What is needed to get support from key stakeholders (particularly healthcare providers and midwives) for maternal immunization? In addition to demonstrating vaccine safety and efficacy, successfully enlisting support from stakeholders will require careful consideration of their concerns and needs, as well as an engagement plan. Midwives and healthcare providers are generally overburdened and may be unable to shoulder new responsibilities without additional support. Implementation will also need to be designed with healthcare providers in mind: vaccinators have previously been hesitant to open multi-dose vaccine vials for a single pregnant woman as it is perceived as a waste. Healthcare provider needs must therefore be taken into account in the design of vaccine implementation strategies, product profile and presentation, and delivery mechanisms. What are the major challenges of integrating maternal immunization into the ANC channel in LIC/LMICs? Major challenges fall broadly into three categories: ANC coverage, basic logistics and healthcare provider management. Acceptance of new vaccines into ANC will require demonstration of maternal health benefits, for which the existing evidence base is relatively weak compared to neonatal health benefits. Basic logistics include the specifics of delivering maternal immunization, such as presentation (e.g. single or multi dose vials), cold chain requirements, storing vaccines at

48
the ANC clinics, training of ANC healthcare providers, and timing of delivery and distribution. Failures in implementation can affect both the safety and efficacy of vaccination programs: in one case Uniject oxytocin was given in place of maternal vaccination because the products were kept in the same cold storage and not appropriately labeled. Attention to program implementation details such as this one will be critical. It is also important to keep in mind that ANC coverage in LICs and LMICs is often low and quality is variable.
Selected interventions received during antenatal care by women with at least one antenatal visit with skilled health personnel (% of total)
Source: UNICEF analysis based on DHS data in 10 high neonatal mortality countries. The source for the aggregates for sub-Saharan Africa and LDCs is UNICEF global
To address healthcare provider management, the structure of a typical ANC visit and patient flow must be taken into account. ANC providers are typically already overextended with many services being required at each visit. Due to patient flow, there is often too little time to effectively counsel mothers hesitant about vaccination. Additionally, because TT is often delivered through the EPI program, there can be specific issues relating to the completeness of ANC medical records, as it may be difficult to assess whether or not the woman is fully immunized. Moreover, most women only receive a single ANC visit, which may create a challenge for the administration of vaccines requiring multiple doses. Finally, there is a risk that adding tasks to an already overloaded health worker will result in less effective coverage of currently offered interventions (e.g. a risk that ANC providers will focus primarily on vaccination – something an audience member suggested has occurred in India with EPI programs). There is also a risk of fragmented, assembly-line care, something that has previously been shown to decrease quality of care and patient retention.

49
As such, integration with ANC will require careful consideration of how to maintain and improve patient retention, coverage and outcomes, both for maternal immunization and existing ANC services. Indeed, ANC acceptance of maternal immunization will depend on it providing net positive outcomes for maternal health. Achieving this will require investing now to strengthen existing ANC systems and improve effective coverage. How can we facilitate cooperation between EPI and ANC channels? General considerations for integrating efforts between EPI and ANC to achieve maternal immunization were proposed, including the need to avoid detrimental competition between ANC and EPI, and the potential for facilitating integration by collocating maternal immunization EPI with existing ANC structure. Furthermore, there must be a concerted global effort to increase effective ANC coverage past the first visit (which is extremely low globally) if rolling out a multi-dose vaccine schedule for pregnant women is to be successful. Panel: Monitoring Safety & Impact Panel lead: Nina Schwalbe (UNICEF) Panel participants: Janet Englund (Seattle Children's Hospital), Saad Omer (Emory University), Alba Maria Ropero Alvarez (PAHO)
Brief summary: This panel addressed the unique challenges of monitoring maternal immunization initiatives for safety and efficacy, as well as the cultural and emotional decision-making factors that drive vaccine demand. What are the unique considerations for monitoring maternal immunization safety, especially given adverse event rates in the target population (pregnant women)? Monitoring of maternal immunization safety is challenging across a number of dimensions. First, there is little data available on the baseline rate of adverse events in pregnant women in LIC/LMIC, making it difficult to accurately assess vaccine safety. Second, pharmacovigilance is challenging, in part because those being monitored may only receive ANC once with no follow-up, and in part because the unique nature of maternal immunization means that not only the mother, but the fetus and child, must be monitored (including for pre-term and still births). Finally, due to the limited coverage of ANC4 in LIC/LMIC, a woman would potentially receive multiple vaccines in a single visit, and studies should be performed to assess the potential interactions and unique safety considerations of administering multiple vaccines simultaneously during pregnancy. There was broad agreement among panel members that passive surveillance was inadequate for AEFI monitoring, and that it was essential for countries to invest in active surveillance to accurately monitor vaccine safety. How can maternal immunization impact be evaluated to enable evidence-based adoption by additional countries? The panel began with an acknowledgment that a strong evidence base is essential for a country to make a decision around vaccine adoption. For example, understanding the health impact of pandemic influenza on pregnant women, coupled with availability of an effective vaccine, led 27 countries to

50
adopt it for maternal immunization. However, this does not necessarily relate to uptake or demand from women themselves. As such, the majority of the discussion focused on cultural and social factors that drive decision-making at the household/individual level.
A few consistent issues were raised. First, women in low income countries may not have the right/power to be decision makers on vaccination during their pregnancies. Second the decision to vaccinate (or obtain ANC care) is likely to be informed by the opinions of a trusted source in the community such as a healthcare provider or family members. Along similar lines, it was highlighted that for a maternal immunization program to be effective, its conductors would have to engage with the community, build and maintain trust, and communicate effectively. Finally it was noted that in instances where trust was not successfully established between vaccine providers and communities (e.g. in the case of rumors that vaccines cause sterility), it is important to work together with opinion leaders to quickly address rumors. Ideally this would be managed through an organized rumor control system.
Implementation: Conclusions and Key Takeaways
1. Acceptance and uptake of maternal immunization will require trust generated by community engagement, buy-in by local opinion leaders, an emphasis on healthcare provider education, and careful communication of vaccine risks & benefits.
2. Integration of maternal immunization into ANC will require consideration of the workload of providers, patient flow, training and education, and attention to the quality and continuity of care. It will also require scale-up of effective ANC coverage (including multiple ANC visits) in low income settings.
3. Adequate monitoring of safety and impact will require new methods to quantify baseline adverse event data, and should ideally incorporate active surveillance of AEFI and impact. Monitoring systems should also cover opinion and rumors, as rumor control systems will be important to ensure continued vaccine uptake and to prevent outbreaks due to the spread of vaccine hesitancy.

51
List of Conclusions and Key Takeaways
Introduction and Investment Case
1. Neonatal mortality is a growing proportion of under-5 mortality and immunization provides an opportunity to prevent a portion of infection related neonatal mortality that is not addressed through any other intervention in LIC/LMIC settings. Therefore, the potential for maternal immunization to address unmet health needs will grow over time.
2. The foundation's impact model predicts significant mortality and morbidity aversion, on the higher end of cost per death averted compared to GAVI vaccines, and moderate cost per DALY averted compared to current MNCH interventions.
3. A better understanding of the disease burden, especially in LIC/LMIC is required to assess the full potential health impact of maternal immunization.
4. Additional benefits, currently uncaptured in the model, include the potential impact on infection-related pre-term and still-births, and non-DALY morbidity burden with associated healthcare costs.
Evidence Base
1. Evidence base in LIC/LMIC must be strengthened for neonates and young infants, who have the poorest data quality but highest predicted disease burden.
2. Efforts to improve the evidence base, both for burden of disease and vaccine efficacy, should include birth outcomes, fetal health, severe disease and hospitalization, and information from autopsies.
3. Diagnostic tools and guidelines must be improved and standardized to accurately estimate disease burden, especially for pertussis.
4. Tetanus may provide a good learning agenda for the maternal immunization platform.
Regulatory
1. Clinical trials must satisfy stringent ethnical concerns, and provide sufficient safety and efficacy data, to result in an indication for maternal immunization.
2. There is limited data available on maternal immunization, and what is available may not be reflected in labeling. This may in part be addressed by the FDA pregnancy and lactation labeling rule (PLLR).
3. Accurate measures of disease burden and efficacy are crucial to establishing whether maternal immunization has a favorable risk/benefit profile.
4. A major challenge in effectively labeling vaccines for maternal immunization will be to accurately communicate the risks of intervention versus the risks of nonintervention, in order to avoid obstructive fears of vaccination in the face of serious disease.

52
5. FDA guidance on non-US vaccines and European Medicines Agency article 58 may provide regulatory pathways to maternal immunization in LIC/LMIC.
6. For a vaccine with demonstrated need, safety and efficacy evaluation via the WHO PQ process takes about a year, though efforts to expedite the process are under way. For labeling of existing vaccines for use in pregnant women, this process may take as little as 90 days including NRA approval.
Policy
1. A strong global recommendation on vaccine safety and efficacy for maternal immunization is essential, but not sufficient on its own, for country-level uptake.
2. Major country-level considerations for maternal immunization include safety, local burden of disease, cost-benefit considerations, integration into the current health system, and the sustainability of financing.
3. Mechanisms must be put in place to ensure buy-in from key country-level stakeholders, including the political leadership, media, individual communities, NITAGs, and regional TAGs.
4. Integration of maternal immunization into MNCH/ANC will require a focus on the health of both child and mother, solid burden/efficacy data, simplicity of vaccine delivery, adequate vaccine supply, and health worker training.
5. Integration may benefit MNCH/ANC, but only if an appropriate integration model and sustainable financing are available.
Market Dynamics
1. Manufacturers face several common challenges in supplying vaccines for maternal immunization, including incomplete knowledge of disease burden and market, need for strengthening of evidence base for safety and efficacy (especially in LIC/LMIC), R&D risk, unclear regulatory paths for pregnant women, concerns regarding ethics and liability, need for sustainable financing, and limited ANC/HCP strength and coverage in low-resource settings.
2. Public-private partnerships are key to overcoming these challenges, for instance through product development relationships, and methods of incentivizing supply (e.g. guaranteed sales volume and purchase prepayment).
3. In the next 1-2 years, critical activities for the global health community to undertake in partnership with manufacturers include establishing stronger evidence base for disease burden and risk-benefit of maternal immunization, assessment of background adverse events in pregnancy and liability landscape, creation of strategic demand forecasts and TPPs, and identification of pathogen-specific product development models that provide a plausible path to vaccine development and licensure for maternal immunization.

53
Funding: Conclusions and Key Takeaways
1. Evidence base for disease burden & health impact are a top consideration for funding decisions. Morbidity is currently considered less significant but requires enhanced attention. Calls have been made to place greater importance on morbidity.
2. Funding decisions vary by country in LIC/LMIC due to different sets of priorities, and the value proposition of maternal immunization is likely stronger in MIC than LIC/LMIC.
3. Country-level funding is essential and supplemented by Vaccine and MNCH donors.
4. Simple financing mechanisms (e.g. a combination of GAVI, GFF and country support) will likely be needed to integrate maternal immunization into ANC, and should focus on integrated solutions (e.g. healthcare channel integration, combination vaccines) that minimize complexity and maximize impact.
Implementation: Conclusions and Key Takeaways
1. Acceptance and uptake of maternal immunization will require trust generated by community engagement, buy-in by local opinion leaders, an emphasis on healthcare provider education, and careful communication of vaccine risks & benefits.
2. Integration of maternal immunization into ANC will require consideration of the workload of providers, patient flow, training and education, and attention to the quality and continuity of care. It will also require scale-up of effective ANC coverage (including multiple ANC visits) in low income settings.
3. Adequate monitoring of safety and impact will require new methods to quantify baseline adverse event data, and should ideally incorporate active surveillance of AEFI and impact. Monitoring systems should also cover opinion and rumors, as rumor control systems will be important to ensure continued vaccine uptake and to prevent outbreaks due to the spread of vaccine hesitancy.

54
Coordination and Collaboration
A major goal of the 2015 maternal immunization stakeholder convening was to facilitate coordination and collaboration between the Vaccine and Maternal, Newborn and Child Health (MNCH) communities, as well as among stakeholders across functions - e.g. policy makers, regulators, vaccine manufacturers, and MNCH implementers. Due to the cross-platform and cross-functional nature of maternal immunization, such collaboration is essential to creating momentum to achieve an end-to-end path to impact. In order to promote collaboration among stakeholders following the convening, several steps still need to be taken, including:
Completing and disseminating a post-meeting survey to gather and communicate feedback on the convening and the most essential next steps for the community
Holding debriefs with session chairs to identify key convening takeaways, next steps, and potential owners
Disseminating a meeting summary and report to all attendees
Informing programmatic and function-level meetings focused on next steps and implementation, e.g. WHO pathogen specific meetings
Initiating collaboration between the stakeholders to implement next steps identified during convening
Ongoing creation of opportunities for continuing discussion of maternal immunization (e.g. in journals and conferences) to ensure the community maintains communication and momentum around maternal immunization
The convening also led to a number of tangible next steps to advance the maternal immunization agenda. Owners were identified for some of these next steps; for others, continued dialogue between the foundation and key stakeholders will be necessary to identify the group or groups best suited to own and champion them. The foundation is committed to working with the maternal immunization community to push these next steps forward on the path to impact. Next steps: Investment Case
[Foundation]: Refine impact model to incorporate more accurate estimates of disease burden, vaccine protection, and costs as they become available to provide donors, policy-makers and countries with the most accurate possible cost-effectiveness data on maternal immunization.
Add to model the effects of maternal immunization on other mortality, including maternal mortality and that due to pre-term and still births
Refine investment case to include effects of maternal immunization on non-DALY morbidity, averted healthcare costs, and socio-economic benefits.

55
Next steps: Evidence Base
Identify countries suspected of having a high disease burden and paucity of data and eventual funding of epidemiological studies to verify disease burden and generate plausible investment case for maternal immunization.
[Clinical Investigators]: Design and conduct clinical efficacy / epidemiology studies with fetal benefits as primary outcome (while engaging MNCH).
Support biopharma companies in designing clinical trials with severe disease as a clinical end point in addition to mortality.
Measure and define health impact beyond immediate mortality and disability burden.
Strengthen/develop diagnostic capacity at clinical sites in developing countries, and provide assistance to national Ministers of Health to adopt standardized diagnostic /procedures to enable extrapolation of data across regions.
Capture key lessons from existing maternal and neonatal tetanus elimination (MNTE) programs, especially across different delivery strategies, to inform future maternal immunization efforts.
Next steps: Regulatory
Industry engagement with FDA/EMA/WHO to promote manufacturer-regulator communications. This should include early 1-on-1 discussions on pipeline products, as well as workshops and open Advisory Committees for non-product specific discussions.
Consider the role of AVAREF/regulatory networks to facilitate review of maternal immunization clinical trials and vaccine registration in LIC/LMIC countries.
EMA, FDA, NRAs, and WHO PQ to coordinate & accelerate maternal immunization regulatory process. This should include a discussion on expected data requirements with the FDA.
o It will also be important to determine where FDA / EMA / WHO support for NRAs would be most helpful to facilitate the development and licensure of vaccines for maternal immunization.
WHO consultation on maternal immunization to build consensus on regulatory issues
Next steps: Policy
Regional TAGs to review and discuss country specific barriers to maternal immunization at upcoming meetings
Ensure proper representation of various stakeholders (esp. MNCH) on NITAGs for maternal immunization discussion
Argentina to publish and distribute learnings from adoption of influenza and pertussis maternal immunization policy
Tools to facilitate country decision making should be developed including decision making tools to evaluate burden of disease

56
o For some pathogens / countries, existing burden of disease may be sufficient to begin driving uptake now
o WHO/BMGF to refine maternal immunization impact model to address country level questions of burden/impact
Co-chairs to independently publish an editorial to update global community on status and rationale
Next steps: Market Dynamics
[The foundation and Other Donors]: Continue to support supply/demand stimulating activities including evidence base expansion, product development efforts, and long term financing, pricing, and supply agreements.
[WHO (including PDVAC), the foundation, and Other Stakeholders]: Support creation of stronger target product profiles (TPP) for prioritized pathogens, including a version with minimum requirements.
[GAVI]: Support maternal immunization demand projections, including potentially setting up a pre-competitive industrial-academic working group to understand supply requirements under different scenarios.
Set up multidisciplinary working group to better understand background safety risks and develop proposals for litigation protection in LIC/LMIC. This could potentially involve WHO coordination, and leverage HHS learnings in the US.
Next steps: Funding
Build out investment case for maternal immunization for key vaccine and MNCH donors. This will require covering the currently available evidence base and identifying further gaps required for funding.
[Vaccine and MNCH Funders]: consider maternal immunization in portfolio for investment assessment: GAVI to consider maternal immunization as part of 2018 Vaccine Investment Strategy (VIS), and Global Financing Facility (GFF) and MNCH donors to consider maternal immunization as potential MNCH intervention.
[Argentina and Other Countries]: Provide a model in promoting maternal immunization, and offer analysis of maternal immunization efficacy / impact from existing programs.
Next steps: Implementation
Continue strengthening evidence base for maternal immunization to capture buy-in at the funding, policy and country levels.
Work with MNCH and countries with existing maternal immunization programs (e.g. in PAHO) to identify plausible models for integrating maternal immunization into existing healthcare systems.
Fund research into baseline adverse events in pregnant women, particularly in LIC/LMIC, to enable appropriate safety and impact monitoring in this population

57
Appendix A: Speakers and Session Chairs Maternal Immunization: Path to Impact
2015 Stakeholder Convening
January 29-30, 2015 – Berlin, Germany
Maternal Immunization: Path to Impact 2015 Stakeholder Convening Speakers and Session Chairs ………………………………………………………………………………………………………………
Jon Abramson
Dr. Jon S. Abramson received his undergraduate degree at Boston University and
medical degree from Wake Forest University School of Medicine (WFUSM). He did
a pediatric residency at Wake Forest University Baptist Medical Center and a
pediatric infectious diseases fellowship at the University of Minnesota. He joined the
faculty at WFUSM in 1981 and has served as Chair of the Department of Pediatrics
at WFUSM and Physician-in-chief of Brenner Children’s Hospital since 1996. He
also served as the elected Chair of the Wake Forest University Physicians clinical
practice group from 2001 – 2007.
Dr. Abramson served as a council member of the Society for Pediatric Research
(SPR) and was elected President of the SPR in 1995. From 1995 – 2003 he was a member and Chair (1999
– 2003) of the American Academy of Pediatrics (AAP) Committee on Infectious Diseases and as part of
this activity was involved in the publication of the 1997, 2000 and 2003 Red Book. From 2003 – 2007 he
was a member and Chair (2005 – 2007) of the Centers for Disease Control and Prevention (CDC) Advisory
Committee on Immunization Practices (ACIP).
Since 2009 he has served as a member of the World Health Organization (WHO) Strategic Advisory Group
of Experts on Immunizations (SAGE) and as of September 2013 has served as the Chair of the SAGE.
Previous roles on SAGE have included serving as the Chair of the Cholera Vaccine and the Meningococcal
Vaccine working groups, as well as a member of the Rubella Vaccine and Global Vaccine Action Plan
working groups. Currently he serves as the Chair of Varicella Vaccine working group and as a member of
the Influenza Seasonal and Pandemic Vaccine working group. Additionally, he serves on the Program and
Policy Committee for the Global Alliance for Vaccines and Immunizations (GAVI).
………………………………………………………………………………………………………………
Carol J. Baker
Dr. Baker is a Professor of Pediatrics, Molecular Virology and Microbiology at Baylor
College of Medicine and Executive Director of the Center for Vaccine Awareness and
Research at Texas Children’s Hospital. She was Head of the Division of Pediatric
Infectious Diseases at Baylor for 25 years, and is immediate past Chair of the Advisory
Committee of Immunization Practices to the Centers for Disease Control and
Prevention.
Dr. Baker’s work has focused on aspects of pediatric infectious diseases, particularly
all aspects of group B streptococcal infections including research to develop a vaccine.
Her work in the early 1990s led to the first recommendations for maternal intrapartum chemoprophylaxis
to prevent early-onset group B streptococcal disease in neonates. However, her life work has focused on

58
developing a GBS vaccine for pregnant women, and more recently on other vaccines that would prevent
infectious diseases in pregnant women and their young infants.
A widely published researcher in pediatrics and infectious diseases, Dr. Baker has authored or co-authored
more than 400 original articles, reviews and book chapters. She was an associate editor of the 2000, 2003,
2006, 2009 and 2012 Red Book published by the American Academy of Pediatrics. She also is the recipient
of many awards and honors, including a Citation from the Infectious Diseases Society of America in 2011
for outstanding research and service.
Dr. Baker received her medical degree, completed her residency and held fellowships in the department of
pediatrics, infectious disease section at Baylor College of Medicine. She was a research fellow in medicine
at Harvard Medical School and a clinical fellow in medicine at Boston City Hospital in Boston,
Massachusetts. Dr. Baker received her undergraduate degree from the University of Southern California
in Los Angeles, California.
………………………………………………………………………………………………………………
Keith Chirgwin
Dr. Keith Chirgwin joined the foundation in 2013 as a Deputy Director for the Regulatory Affairs team of Integrated Development. He leads regulatory program strategies, working with the foundation’s strategy teams and development partners to ensure that regulatory strategies support the timely and successful development and registration of products in the foundation’s portfolio. An infectious disease physician with over 25 years of experience across both academia and the industry, Keith is recognized as a regulatory affairs expert who is
able to navigate the entire landscape from vaccine development to commercialization. He spent the last 16 years with Merck, most recently serving as Vice President of Vaccines Pipeline and Project Leadership and before that, Vice President of Regulatory Affairs. While at Merck, Keith oversaw the regulatory strategy and regulatory support for the successful development and global licensure of several new vaccines and drugs. ………………………………………………………………………………………………………………
Claudia Morrissey Conlon
Claudia Morrissey Conlon began her career as a community organizer in poor
communities in the US while serving as a VISTA Volunteer. She then spent a year
mobilizing residents in a large peri-urban slum outside of Mexico City,
Netzahualcoyotl, around public health issues. These experiences led to her lifelong
interest in strengthening community-based primary healthcare. Dr. Conlon received
her MD degree from the Chicago Medical School and completed her residency in
Internal Medicine at the University of Iowa. She is a board-certified Internist and
practiced primary care medicine in disadvantaged communities in the US for over a
decade before earning an MPH in health policy from Johns Hopkins University Bloomberg School of Public
Health and focusing her career on global health challenges.
In the mid-nineties, Dr. Conlon joined USAID as the Senior Technical Advisor for the MotherCare project,
the USG’s flagship maternal health program. She returned to USAID in December 2012 as a Senior
Maternal Newborn Health Advisor and USG Lead for the Saving Mothers, Giving Life (SMGL) public
private partnership. SMGL was established by then Secretary of State, Hillary Clinton in June 2012, to
dramatically reduce maternal mortality in high-burden SSA countries. Immediately prior to rejoining

59
USAID, Dr. Conlon served as a Senior Director at Save the Children, US, heading up the technical unit for
the Gates-funded Saving Newborn Lives project.
Throughout her career, Dr. Conlon’s technical work has centered on increasing gender equity and
improving maternal and newborn survival and well-being, both domestically and internationally. She has
held positions at the:
• World Health Organization in the Department of Gender, Women and Health
• John Snow Incorporated—as Senior Technical Advisor for an integrated urban family health
project in Bangladesh, and Deputy Director of the JSI Center for Women’s Health
• University of Illinois—as Deputy Director of the Center for Research on Women and Gender, an
Associate Professor at the School of Public Health, and as Assistant Dean at the College of Medicine.
Dr. Conlon is on the editorial board of the Journal of Women’s Health. She is Past President of the
American Medical Women’s Association and Past Vice President for North America for the Medical
Women’s International Association, the global organization of women physicians.
………………………………………………………………………………………………………………
France Donnay
France Donnay, MD, ObGyn, MPH, is Senior Program Officer for maternal health on
the Maternal, Neonatal and Child Health team based in Integrated Health Solutions
Development. France practiced obstetrics and gynecology in public and private
hospitals as well as family planning clinics in Brussels for 15 years. She also worked
as a consultant to the World Health Organization, the World Bank, the United Nations
Population Fund (UNFPA), and Doctors without Borders, and visited 60 + countries
in all regions of the world. From 1994 to 1999, France was the Women’s Health
Adviser at UNICEF Headquarters. She then moved to UNFPA where she was Chief
of the Reproductive Health Branch, Technical Support Division, from 1999 to 2005
before leading the UNFPA Pakistan office from 2005 to 2008.
In 2009 she was made Fellow honoris causa at the Royal College of Obstetricians and Gynecologists, and
in 2010 Fellow of the American College. Also, she has written more than 50 articles and reports on maternal
health. Dr. Donnay manages a substantial portfolio of grants at the foundation focused on the reduction of
maternal mortality in developing nations. She is also the foundation representative to the Partnership for
Maternal, Newborn and Child Health (PMNCH), a global health alliance of almost 300 members working
together to improve health for all women, infants and children.
………………………………………………………………………………………………………………
Marion Gruber
Marion F. Gruber, PhD is the Director of the Office of Vaccines Research and Review (OVRR) in the
Center for Biologics Evaluation and Research (CBER), Food and Drug Administration. In this position,
she directs the review, monitoring, and evaluation of investigational new drug applications and biologic
license applications encompassing vaccines and related biological products as well as research pertaining
to the development, manufacturing and testing of vaccines.
From 2009 - 2011 Dr. Gruber served as OVRR Deputy Director and from 2005 – 2009 as OVRR Associate
Director for Policy. In these positions she has gained extensive experience in developing policies and
programs affecting the regulation of vaccines. Dr. Gruber has served on numerous agency and interagency
working groups and committees and has represented the OVRR on national and international task forces to
foster communications and collaborations related to the safety, quality and efficacy of vaccines.

60
Dr. Gruber has over 20 years of experience in the regulatory review and approval of preventive vaccines
and related biologics. She has generated guidance for industry documents critical to the development of
preventive vaccines and has contributed to rule making affecting the regulation of vaccines. She has
represented OVRR in numerous FDA wide initiatives, as well as national and international meetings.
………………………………………………………………………………………………………………
A. Metin Gülmezoglu
Dr. A. Metin Gülmezoglu is the coordinator for the maternal and perinatal health and preventing unsafe abortion team. Dr. Gülmezoglu qualified as an obstetrician and gynecologist in Turkey. He worked as a clinician and researcher in South Africa and obtained his PhD at the University of the Witwatersrand. He then worked at the National Perinatal Epidemiology Unit at Oxford University and at the United Kingdom Cochrane Centre focusing on systematic reviews. In 1998 he joined The UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, the Department of
Reproductive Health and Research, WHO in Geneva as a medical officer.
Dr. Gülmezoglu conducted research on major causes of maternal mortality and morbidity since 1992. He
contributed to large multicentre randomized controlled trials evaluating promising clinical interventions
and improving the quality of maternal and perinatal health care. He joined the Cochrane Collaboration in
1994 conducted over 30 Cochrane systematic reviews on a wide ranging topics including maternal and
perinatal health, newborn health, safe abortion techniques, contraception and sexually transmitted
infections. He is in the editorial boards of the Cochrane Pregnancy and Childbirth and Fertility Regulation
review groups.
Since 1997, he also coordinates the WHO Reproductive Health Library, a specialist database in sexual
reproductive health that focuses on providing access to key systematic reviews and WHO guidelines
together with educational videos, currently published on the WHO web site in five UN languages.
………………………………………………………………………………………………………………
Judith Kallenberg
Judith Kallenberg is the Head of Policy at Gavi, the Vaccine Alliance, leading the
team responsible for the development of programmatic policies. These include
eligibility, graduation and co-financing policies, as well as policies on risk
management, gender and Gavi’s support in fragile settings. Judith previously led the
development of Gavi’s Vaccine Investment Strategy to identify new vaccines for
Gavi’s portfolio. She has ten years of experience in global health programming and
financing policy and strategy, including several years in Africa. Judith is a Dutch
national with degrees in Medicine and International Relations.
………………………………………………………………………………………………………………

61
Keith Klugman
Professor Keith Klugman is the Director of Pneumonia at the Bill and Melinda Gates Foundation in Seattle WA. He is currently on extended leave from his academic appointment as the William H. Foege Chair of Global Health in the Hubert Department of Global Health at Emory University, in Atlanta, Georgia, where he is also Professor of Epidemiology and Professor of Medicine in the Division of Infectious Diseases. In addition, he still serves as an Honorary Professor in the Respiratory and Meningeal Pathogens Research Unit at the University of the Witwatersrand, in Johannesburg, South Africa.
Professor Klugman is currently the Past - President of the International Society of Infectious Diseases; he
is Treasurer of the Board of the International Symposium of Pneumococci and Pneumococcal Diseases;
past Chair of the International Board of the American Society for Microbiology. Keith has chaired or served
on numerous expert committees for the World Health Organization (WHO), the Wellcome Trust and the
Centers for Disease Control and Prevention (CDC). He serves as an editor or member of the editorial board
of 12 journals.
Professor Klugman has made major contributions to the field of pneumococcal disease. His work, including
the demonstration of pneumococcal conjugate vaccine efficacy in the developing world, has led to
interventions that have saved millions of lives especially in Africa. He has published more than 500
scientific papers which have been cited more than 24,000 times to date. His current position allows him the
opportunity to contribute to the mission of the Gates Foundation to reduce deaths from pneumonia in
children, thus allowing them the chance to lead healthy and productive lives.
………………………………………………………………………………………………………………
Shabir Madhi
Professor Shabir Madhi is Executive Director of the National Institute for
Communicable Diseases, Professor of Vaccinology and Director of the MRC
Respiratory and Meningeal Pathogens Research Unit at Wits. He also holds the
position of DST/NRF SARChI Chair in Vaccine Preventable Diseases. Professor
Madhi completed his undergraduate and postgraduate training at University of
Witwatersrand (Johannesburg, South Africa), qualified as a pediatrician in 1996 and
obtained his PhD in 2003. He is certified in Infectious diseases as a sub-specialty.
Shabir has been involved in research on vaccine-preventable diseases and on infections in HIV-infected children for 17 years. He has undertaken pivotal studies on
pneumococcal conjugate vaccine (PCVs) and rotavirus vaccines which have contributed to WHO recommendations for the introduction of these life-saving vaccines into public immunization programs globally. More recently his research Unit has focused on maternal immunization aimed at protection of young infants, including the first randomized trial of influenza vaccination in pregnant HIV-infected and HIV-uninfected women in Africa and phase II studies on trivalent GBS conjugate vaccines. Professor Madhi has contributed to nine book chapters and over 200 peer reviewed articles in international journals. He has received multiple national research awards, including the South African Medical Research Council: Life Time Achievement Award (Platinum Medal). ………………………………………………………………………………………………………………

62
Elizabeth Mason
Elizabeth Mason was Director of the department of Maternal, Newborn, Child and
Adolescent Health at WHO HQ in Geneva, from 2004 until her retirement at the end
of May 2014. She a specialist in Public Health - Maternal, Newborn, Child and
Adolescent Health and has more than 30 years’ experience in Clinical care; Policy
and Strategy development; Planning, management, implementation and monitoring of
maternal, newborn and child health programmes at all levels of the health service.
She spent 24 years living and working in the African region. Working in Zimbabwe,
at all levels of the health system, before joining WHO, where she worked at country,
intercountry and Regional levels. She qualified in Medicine from the University of
Leeds, UK, has an MPH from LSHTM, is a Fellow of the Faculty of Public Health, UK and an Honorary
Fellow of the Institute for Global Health, University College London.
………………………………………………………………………………………………………………
Jussi Mertsola
Jussi Mertsola has worked as a Professor of Pediatrics at the Turku University Hospital,
Finland, since 2001 and since 2010 he has been the Chairman of the Department of
Pediatrics and Adolescent Medicine in Turku.
He made his medical thesis in 1985 about serology and epidemiology of pertussis and
specialized in Pediatrics in Turku (1987). After that he did research and was in training
of PID in The University of Texas Medical Center at Dallas Southwestern Medical
School in 1988-1990 in the group of McCracken and Nelson.
He was specialized in Pediatric Infectious Diseases in 1993. He has been the Chairman
of the National Advisory Committee for Vaccination in Finland in 2002-9. He was the president of Finnish
Pediatric Society in 2010-13. He has been an active member of European Society for Pediatric Infectious
Diseases (ESPID) since the beginning of the society in 1983.
Jussi Mertsola has more than 170 scientific articles and has supervised several medical theses projects. His
research is focused on pediatric respiratory infections and especially pertussis. With Qiushui He Jussi
Mertsola is chairing the European EUpertstrain group studying the evolution of B.pertussis organisms and
epidemiology of pertussis in Europe.
………………………………………………………………………………………………………………
Su-Peing Ng
Dr. Su-Peing Ng has been the Head of Global Medical Affairs at Sanofi Pasteur since
September 2013. She leads a dedicated team of physicians and scientists involved in a
range of activities including medical-scientific exchange and communications, training
and education relevant to vaccine-preventable diseases and vaccines developed and
commercialized by Sanofi Pasteur, the design and conduct of Phase IIIb/ IV and
registration studies and post-marketing benefit-risk evaluations and documentation.
Prior to this, she worked for over 6 years at GSK Vaccines, serving as VP Head of
Global Medical Affairs for Pediatric Vaccines, Regional Director of Medical Affairs
for Asia Pacific and Director of Clinical R&D and Medical Affairs in Australasia.
During this time, she was involved in the launch and introduction of Human Rotavirus Vaccine,
Pneumococcal-Non-typeable Haemophilus Influenzae Protein D conjugate vaccine, Human papillomavirus
vaccine and combined measles, mumps, rubella and varicella vaccine.
She has also worked in biotechnology companies PowderJect Pharmaceuticals as Business Development
Director in Oxford, England and Cortical as Chief Executive Officer in Melbourne, Australia and as a
management consultant at the Boston Consulting Group. She has a medical degree from the University of

63
Western Australia and a MBA from the Melbourne Business School. She is passionate about the value of
vaccination as a physician, a global citizen and as a mother.
………………………………………………………………………………………………………………
Katherine O’Brien
Kate O’Brien, Professor in the Department of International Health and Pediatrics at
Johns Hopkins Bloomberg School of Public Health (JHSPH), is a pediatric infectious
disease physician, an epidemiologist and a vaccinologist who earned her M.D. at
McGill University and her MPH at Johns Hopkins University. Following residency
and fellowship at Johns Hopkins, and time living in Haiti conducting research into
maternal-infant HIV transmission, she joined the Bacterial Respiratory Diseases
Branch at the Centers for Disease Control and Prevention as an Epidemic Intelligence
Officer. Kate returned to Johns Hopkins in 1998 to lead the Infectious Disease
Prevention group at the Center for American Indian Health (CAIH) conducting
clinical trials of vaccines for diseases of importance to American Indian tribes. She
served as the Deputy Director for the GAVI Alliance PneumoADIP project, and is now the Executive
Director of the International Vaccine Access Center (IVAC) at JHSPH.
Her work domestically and internationally has focused on vaccine preventable childhood illnesses including
surveillance, epidemiology, and vaccine clinical trials of pneumococcal disease; rotavirus; Haemophilus
influenzae type b; respiratory syncytial virus and influenza vaccines. She has worked extensively in Africa
and Asia, partnering with local scientists to develop rigorous scientific evidence and bring it into the vaccine
policy arena, thereby accelerating the use and access to life-saving vaccines for children living in low
resource countries and settings.
She serves as a member of the World Health Organization Strategic Advisory Group of Experts (SAGE)
on Immunization, the global vaccine advisory committee. She has been honored with the U.S. Department
of Health and Human Services Secretary’s Distinguished Service Award in 1998, awarded by Secretary
Shalala for outstanding service in response to the epidemic of acute renal failure from diethylene glycol
poisoning in Haiti, the Sabin Vaccine Institute Young Investigator award in 2008, and the U.S. Presidential
Early Career Award in Science and Engineering (PECASE), the highest honor awarded in the United States
for early and mid-career scientists and engineers, in 2011. She recently served as the co-chair of the 9th
International Symposium on Pneumococci and Pneumococcal Diseases, a multidisciplinary scientific
conference attended by approximately 1,000 scientists from over 70 countries, held for the first time in Asia
(Hyderabad, India). She was named as the Robert Austrian Invited Lecturer, an honor recognizing
outstanding contributions to the field of pneumococcal disease control.
………………………………………………………………………………………………………………
Pauline Paterson
Dr. Pauline Paterson is a Research Fellow and co-lead of The Vaccine Confidence
Project with Dr. Heidi Larson at the London School of Hygiene and Tropical
Medicine, UK. The Vaccine Confidence Project conducts global research on vaccine
confidence, examining local and global dynamics which influence vaccine decision-
making. Dr. Paterson, together with Dr. Larson, established a global, internet-based
information surveillance system on public concerns around vaccines and vaccination
programmes. The Vaccine Confidence research group has also been conducting
qualitative research on specific vaccine confidence issues and risk perceptions
globally since 2010. Country level analyses include HPV vaccine acceptance in India
and Japan, a systematic review on public trust in vaccination, and a literature review on acceptance of
maternal and pregnancy vaccines and vaccinations.

64
Dr. Paterson is a member of the National Institute for Health Research (NIHR) Health Protection Research
Unit (HPRU) in Immunization in partnership with Public Health England.
Specific activities include qualitative analysis of parental reasons for not vaccinating their child with
influenza vaccine in England and factors influencing vaccination uptake among ethnic minorities during
pregnancy in England. This research involves a literature review of factors leading to poor uptake of
vaccines in pregnant women, focusing on maternal acceptability, concerns and trust, and in-depth
interviews with pregnant women and health care workers about reasons for non-vaccination during
pregnancy.
Dr. Paterson has a PhD in Epidemiology, an MBA, and an MSc in Environmental Technology from
Imperial College London.
………………………………………………………………………………………………………………
Azhar Abid Raza
Azhar Abid Raza is a medical doctor, born in Multan, Pakistan – one of the oldest
cities not only in the Asian subcontinent but also in the world. He did his M.B; B.S.
from Nishtar Medical College Multan and hold Master of Science degree in Public
Health from Health Services Academy of Pakistan.
Currently he is working as Immunization Specialist at UNICEF Headquarter for
Maternal and Neonatal Tetanus Elimination Programme, since last 3 years. In this
capacity, he is also supporting EPI Unit by sharing responsibility for HQ immunization
focal person for some countries.
He has more than 15 years working experience with immunization Programme; starting as Additional
Director EPI with the Government of Punjab; Polio Officer WHO & UNICEF; and Project Officer and
Health Specialist UNICEF in Pakistan. In these capacities he had the privilege of working in emergencies,
for polio eradication and programmatic integration while working with WHO and UNICEF Pakistan.
Before moving to preventive health in 1999, he had been working as Monitoring & Evaluation of Health
Management Information System (HMIS) in Punjab; teaching Anatomy, Forensic Medicine and
Toxicology at King Edward Medical College Lahore, and Medical Officer in various provincial and
national departments.
………………………………………………………………………………………………………………
Helen Rees
Professor Helen Rees OBE MB BChir, MA (CANTAB), MRCGP, DCH, DRCOG Professor Helen Rees is the Executive Director and founder of the Wits
Reproductive Health and HIV Institute (Wits RHI) of the University of
Witwatersrand and is also a personal Professor in the Department of Obstetrics and
Gynecology. She is an Honorary Professor at the London School of Hygiene and
Tropical Medicine and an alumnus of Cambridge University and Harvard Business
School. Professor Rees is an internationally renowned expert in vaccines
and immunization, HIV prevention and reproductive health, and was the Chair of
the South African Medicines Control Council. She serves on numerous national and
international scientific boards and committees. She was the Chair of the WHO’s
Strategic Advisory Group of Experts on Immunization (SAGE) when she also she served on the Global
Vaccines Advisory Committee on Vaccine Safety and on the GAVI Programme and Planning
Committee. She Chaired the SAGE Working Group on the Use of Vaccines in Humanitarian Emergencies,
the SAGE Working Group on Rubella and was the SAGE focal point for HPV and HIV vaccines. She

65
currently chairs the WHO’s African Task Force on Immunization, and is the Chair of the SAGE Working
Group on Ebola Vaccines having recently co-chaired the WHO High Level Meeting on Ebola vaccines. She
is the Chair of the Emergency Committee advising on Polio Vaccines under the International Health
Regulations. Prof Rees is a member of the SAGE Working Group on Measles and Rubella vaccines, and the
SAGE Working Group that monitors progress on the Global Vaccine Action Plan. She is the Chair
of the WHO/PATH Technical Advisory Group on Maternal Influenza Immunization and is a member of the
South African National Advisory Group on Immunization.
………………………………………………………………………………………………………………
Carmen Amelia Rodriguez Hernandez
Carmen Rodriguez Hernandez is a Pharmacist with specialization in Microbiology
applied to the Quality control of Food, Cosmetics, medicines and Biologicals.
Currently, scientist group lead of vaccines assessment within the WHO
Prequalification Programme, Regulation of Medicines and other Health Technologies.
Twenty-four years of experience in the area of regulation of biologicals, including
Quality Control of vaccines, blood products and recombinant products.
Rodriguez Hernandez has written several publications in the area of quality control of
vaccines. She participated in the revision of the Venezuelan regulations of
Pharmaceutical and Biologicals, as well as Coordination of activities for the
Latinoamerican network, PAHO, in Washington, DC. As part of the work in WHO, responsible for the
Assessment of vaccines submitted as part of the prequalification: Review of the quality information,
organizing site audit to vaccine manufacturers.
Coordination of the WHO Testing program as part of the prequalification. Participation in several
International conferences and workshops as lecturer and facilitator. Assessment of vaccine quality
complaints and adverse event with prequalified vaccine received from the field. Participation in the
assessment of National regulatory Authorities located in the Americas, Europe and Asia.
………………………………………………………………………………………………………………
Christina Schrade
Christina Schrade is founder and director of SEEK Development, a consulting group
based in Berlin, Germany, dedicated to supporting and shaping human development
globally. She combines deep expertise in strategy, organizational development and
evaluation with comprehensive knowledge of international development and health
issues. Key areas of her work are the global financing architecture, public-private and
results-based approaches in international development cooperation, reproductive,
maternal and child health, as well as the development of high-performance organizations
in the non-profit sector. Her analytical skills are complemented by years of experience in
facilitating large-scale multi-stakeholder projects and building up new organizations and
business lines. Amongst many other assignment, Christina currently advises the World Bank on the
development of the Global Financing Facility for Reproductive, Maternal, Newborn, Adolescent and Child
Health.
Before founding SEEK Development, Christina was Senior Advisor to the Global Fund’s Executive
Director and then Senior Manager of Global Strategic Initiatives at the Global Fund. She led the
development of the Fund’s first corporate strategy and associated KPIs, as well as the business planning for
the Affordable Medicines Facility for Malaria and the development of the partnership with UNITAID. Prior
to her time at the Global Fund, Christina worked as an Engagement Manager at McKinsey & Company,
focusing on strategy and organizational development of large corporate, multilateral and other non-profit
clients, and as a research fellow at the Center for Public Leadership at Harvard University. Christina
received her MPA from the Kennedy School of Government/Harvard University, and holds a Master’s

66
Degree in Development Policy/Political Science from the University of Tübingen, Germany, and an
Executive MBA. She also completed formal training in systems approaches for organizational
development, facilitation, negotiation, and leadership coaching and development.
………………………………………………………………………………………………………………
Nina Schwalbe
Nina Schwalbe joined UNICEF as Principal Health Advisor in 2014 in a newly
created position to co-lead UNICEFs health efforts. In addition to direct
management of programs on maternal, child and new born health including in
emergency settings, Nina’s role is to advise UNICEF leadership on strategic
planning and special projects and improve program integration within health and
across sectors.
Prior to joining UNICEF, Nina served as a managing director at the GAVI Alliance. Her responsibilities included performance management, policy development, market shaping, and monitoring and evaluation. Key achievements in her tenure there included development of a five year strategy and business plan, GAVI’s vaccine investment and supply and procurement
strategies, policies including country eligibility, evaluation, and gender, and a review and revision of GAVI’s performance based financing initiative. Before working at GAVI, Nina directed the policy department at the Global Alliance for TB drug
development. She came to the TB Alliance from the Soros’ Foundations, where she directed global public
health programme, which focused on strengthening health systems, TB, HIV/AIDS, and programs aimed
at vulnerable populations. She also worked in maternal/child health, first with the Population Council and
then with AVSC International (now Engender Health) and spent two years working with Hmong refugees
in Thailand. Nina holds degrees from Harvard and Columbia Universities, is member of the Council on
Foreign Relation, and has served on the faculty of the Mailman School of Public Health at Columbia
University.
………………………………………………………………………………………………………………
Eric Simoes
Eric A. F. Simoes is a Professor of Pediatrics at the University of Colorado Denver,
School of Medicine, and a Professor of Epidemiology at the Colorado School of
Public Health in Denver Colorado. He is the Co-Director of the Mother and Child
Health Initiative of the Center for Global Health at the Colorado School of Public
Health, a WHO Collaborating Institution. He received his DCH and MD from the
University of Madras, India, in 1982 and 1984 and subsequently obtained his
Fellowship in Pediatric Infectious Disease from the University of Colorado, where
he still works. He has been involved with the Integrated Management of Childhood
Illness since its inception in the early 1990’s. The World Health Organization in
conjunction with UNICEF and other organizations to reduce childhood and infant mortality in the
developing world developed the strategy. His research interests focus on the epidemiology and prevention
of acute respiratory infections, including RSV, Influenza and Streptococcus pneumoniae. Specifically he
has been involved in understanding the epidemiology and burden of RSV disease both in developing
countries and industrialized ones. He has conducted studies in this regard in India, Indonesia, Philippines,
Denmark, South Africa and USA. In addition he has been involved in studies on the prevention of RSV and
its long-term effects in Europe, USA, Indonesia and Japan.
………………………………………………………………………………………………………………
Viviana Mangiaterra

67
Viviana Mangiaterra is a specialist in international public health with a primary
expertise in reproductive, maternal, child, adolescent health. She has a medical degree
with further training (Ph.D Level) in pediatrics and epidemiology and she has worked
in Italy as clinician and researcher for several years. She joined the World Health
Organization in 1987 working at all levels of the WHO system, national (Rwanda and
Indonesia), regional (European Region) and HQ. She worked at the World Bank as
Advisor Children and Youth from 2002 to 2007. During that period she was responsible for the
preparation of a comprehensive Children and Youth strategy and she was instrumental in the development
of the World Development Report 2007 on Youth. She was with the WHO at the HQ office from 2007 to
2013, responsible for the integration and partnerships work of the Cluster of Family, Women and Child
Health with the Commission of Commodities, the H4+, HIV, Malaria programs within WHO and with
other relevant partners. Since 2012 she is the co-chair of the Roll Back Malaria, Malaria in Pregnancy
Working Group. She has joined in 2014 the GF as Senior Coordinator RMNCH/ HSS.
During her career she has gained an extensive experience in policy and strategy
development, implementation and evaluation of programs embracing reproductive, maternal and child
health interventions including programmatic areas related to health system strengthening and integration
across MDG 4, 5 and 6.
………………………………………………………………………………………………………………
Ajoke Sobanjo-ter Meulen
Ajoke Sobanjo-ter Meulen is a Senior Program Officer in the Global Health Division
at the Bill & Melinda Gates Foundation. She leads the maternal immunization and
meningococcus initiatives. Most recently, Ajoke was Executive Director (Cluster
Head) at Novartis, Cambridge, where she managed the maternal immunization
clinical development program for the Group B streptococcus vaccine. She was
responsible for the clinical content of a successful IND filing for the first clinical trials
in pregnant women in the US, to the Food and Drug Administration (FDA).
Previously, Ajoke served as Associate Director Vaccine Clinical Research at Merck
Research Laboratories where she managed the global phase III clinical development
program of the S. aureus vaccine. She was a key clinical development leader in several vaccine programs
in Discovery through phase 3 and was instrumental in achieving successful outcomes on two IND filings
to the US Food and Drug Administration. Before joining industry, she worked as the program coordinator
for Child Health and Neglected Diseases at the German bilateral agency (GIZ) providing strategic and
policy advice to the German Ministry of Development Cooperation. Ajoke also coordinated a large multi-
center trial on HIV drug resistance monitoring and surveillance in Africa and Asia for the Netherlands Aids
Foundation, under the Dutch Ministry of Foreign Affairs. Ajoke completed her residency in pediatric and
adolescent medicine at the University of Wuerzburg, Germany, and did her pediatric infectious disease
fellowship at Mount Sinai Medical School, New York. She holds a M.D. degree from the Free University
of Berlin, and a medical doctorate (Dr. med.) degree from the Institute of Tropical Medicine at the
University of Hamburg, both in Germany. She also holds a M.Sc. degree in Epidemiology from the London
School of Hygiene and Tropical Medicine in England.
………………………………………………………………………………………………………………

68
Jean-Francois Toussaint
Bio-engineer with a PhD in animal sciences and an executive MBA from HEC Paris,
I started my career in the Belgian reference laboratory for animal health. I joined
GSK’s immunology department in 2006 and then became project leader for the dengue
vaccine candidate. I am currently the project leader for the RSV pediatric and RSV
maternal vaccine candidates.
………………………………………………………………………………………………………………
Amina White
Dr. Amina White is an obstetrician-gynecologist and bioethicist on faculty in the
Clinical Center Department of Bioethics at the National Institutes of Health in
Bethesda, Maryland. Her research focuses primarily on ethical challenges that
physicians face in clinical care and research when interacting with vulnerable patient
populations. In addition to exploring ethical and regulatory issues that arise when
involving pregnant women in clinical trials, she has conducted qualitative research,
written articles, and given presentations related to patient-physician communication,
patient activation and engagement of disadvantaged or marginalized patient groups,
and trauma-informed practices in obstetrics and gynecology for women who disclose
a past history of abuse. Prior to joining the bioethics faculty at the National Institutes of Health, Dr. White
completed her undergraduate education at Yale University, obtained her medical degree from Harvard
Medical School, completed her OB/GYN residency training at Georgetown University Hospital, and
pursued bioethics training through a Master’s program at Georgetown University and a bioethics fellowship
at the National Institutes of Health. She continues to practice medicine and teach medical students and
residents as an Assistant Professor in the Department of Obstetrics and Gynecology at Howard University
in Washington, DC.
………………………………………………………………………………………………………………
Greg Widmyer
Greg Widmyer is the Deputy Director of Vaccine Delivery within the Global
Development Division at the Bill & Melinda Gates Foundation. Within the Vaccine
Delivery team, Mr. Widmyer leads the Vaccine Introduction (VI) and Market
Dynamics (MD) groups. These teams focus on working with GAVI to strengthen
country efforts to introduce new vaccines; supporting program strategy teams to
develop effective delivery strategies for their portfolio of vaccines; and developing an
evidence base for vaccine introduction approaches. The MD group spearheads efforts
to engage with vaccine manufacturers to achieve stable and low-priced vaccines for
low-income countries. He also leads efforts to strengthen the availability and use of
quality programmatic data for immunization under the Vaccine Delivery team’s recently approved Routine
immunization strategy. Previously, Mr. Widmyer was Vice President and General Manager of Monogram
Biosciences where he led the commercial and operational aspects of the company. He held a variety of
commercial positions within Monogram including Director of Marketing, and Director of Commercial
Operations. Prior to joining Monogram, Mr. Widmyer, was head of Finance and New Business Ventures at
SCORE Learning, a division of Kaplan Inc, focusing on its online learning businesses and expansion of
their learning-center based programs into lower income communities. From 1992 – 1998, Mr. Widmyer
worked for Population Services International where he served as Country Director for projects in Cameroon

69
(interim), Rwanda and Myanmar leading social marketing programs in HIV/AIDS prevention, maternal
and child health and nutrition. Mr. Widmyer was also a Peace Corps Volunteer in Togo from 1990-1992.
He received his BA in Russian Studies from Yale University and his MBA from Stanford University.
………………………………………………………………………………………………………………
Russell Wilson
Mr. Wilson joined Novavax in November 2011 as Senior Vice President, Business
Development. He is responsible for developing business alliances, license
arrangements, and partnering opportunities with pharmaceutical companies and
government agencies. Mr. Wilson was most recently the Chief Financial Officer at
Supernus Pharmaceuticals. He was previously Senior Vice President, Chief Financial
Officer and General Counsel of Iomai Corporation, which was acquired in 2008 by
Intercell AG, during which time he successfully negotiated a $128 million government
contract with the Office of Biomedical Research and Development Authority (BARDA)
at the U.S. Department of Health and Human Services. Mr. Wilson was also the Acting General Counsel
of North American Vaccine, Inc. until its acquisition by Baxter International in 2000. He is a graduate of
Princeton University and received his Master's in Business Administration and Juris Doctorate degrees from
the University of Virginia.

70
Appendix B: Panel Chairs and Participants Maternal Immunization: Path to Impact
2015 Stakeholder Convening
January 29-30, 2015 – Berlin, Germany
Name Organization
Safety & Labeling Panel
Keith Chirgwin (Chair) BMGF
Marion Gruber FDA
Patrick Zuber WHO
Daniel Brasseur EMA
Laurent Brassart EMA
Boonchai Somboonsook Thai FDA
Vaccine Policy
Helen Rees (Chair) WRHI
Azhar Raza UNICEF
Fredrick Were University of Nairobi, Kenya
Carla Vizzotti MoH, Argentina
Adenike Grange Former MoH, Nigeria
MNCH Policy Advancement and
Integration into Vaccine Policy
Elizabeth Mason (Chair) WHO, Former Director MNCAH
Charles Mwansambo Health Services, Malawi
Abdullah Baqui JHU
Ana Langer Harvard School of Public Health
Martina Baye Ministry of Public Health, Cameroon
Enablement Levers
Greg Widmyer (Chair) BMGF
David Kaslow PATH
Bruce Gellin HHS
Kim Bush BMGF
Melissa Malhame GAVI
Donor Perspective
Elizabeth Mason (Chair) WHO, Former Director MNCAH
Viviana Mangiaterra The Global Fund
Claudia Conlon USAID
Judith Kallenberg GAVI
Adenike Grange Former MoH, Nigeria
Carla Vizzotti MoH, Argentina
Barriers to Demand and Uptake, and
Integration into ANC
Nina Schwalbe (Chair) UNICEF
Sylvia Deganus Tema General Hospital, Ghana
Tajul Islam Bari EPI HQ DGHS Bangladesh
Pauline Paterson LSHTM
Lisa Noguchi JHPIEGO
Martina Baye Public Health Services, Ghana
Monitoring Safety and Impact
Nina Schwalbe (Chair) UNICEF
Alba Maria Ropero Alvarez PAHO
Janet Englund Seattle Children's Hospital
Saad Omer Emory University
Shabir Madhi University of Witwatersrand

71
Appendix C: Participant List Maternal Immunization: Path to Impact
2015 Stakeholder Convening
January 29-30, 2015 – Berlin, Germany
Name Affiliation
Abelin, Atika Sanofi Pasteur
Bellah, Ahmed WHO
Abramson, Jon Wake Forest Medical School
Bergquist, Sharon BMGF
Alderson, Mark PATH
Berkley, James Oxford University
Alvarez, Alba Maria Ropero PAHO
Bhat, Niranjan PATH
Amadi, Ovid BCG
Brassart, Laurent European Medicines Agency
Anderson, Larry Emory University
Brasseur, Daniel European Medicines Agency
August, Allison Novavax
Bresee, Joseph CDC
Baker, Carol J Baylor College of Medicine
Brown, Tyler BMGF
Baqui, Abdullah JHU
Bush, Kim BMGF
Bari, Tajul EPI HQ, Director General of Health Services
Cairns-Smith, Sarah BCG
Baye, Martina Lukong Ministry of Public Health, Cameroon
Chirgwin, Keith BMGF
Becker, Julie Rabin Martin
Chotpitayasunondh, Tawee Queen Sirikit National Institute of Child Health
Conlon, Claudia USAID
Glenn, Gregory Novavax
Deganus, Sylvia Tema General Hospital, Ghana
Grange, Adenike Adegrange Child Foundation
Donnay, France BMGF
Gruber, Marion FDA/CBER
Donnelly, John PATH
Gülmezoglu, Ahmet Metin WHO
Duclos, Philippe WHO
Gupta, Swati Merck
Dull, Peter BMGF
Halperin, Scott Dalhousie University
Englund, Janet Seattle Children's Hospital
Hanssens, Linda GSK
Eppel, Gerd GIZ
Heath, Paul St Georges, University of London
Fischer, Per MinervaX
Higgins, Deborah PATH
Frank, Becky BMGF

72
Name Affiliation
Hombach, Joachim WHO
Gasse, Francois UNICEF, Retired
Hutubessy, Raymond WHO
Gellin, Bruce Department of Health and Human Services
Hwang, Angela BMGF
Jansen, Kathrin Pfizer
Langer, Ana Harvard School of Public Health
Johnson, David Sanofi Pasteur
Lavery, Jim St. Michael's hospital
Kallenberg, Judith GAVI
Libster, Romina Fundacion INFANT
Kang'ethe, Alice Clinton Health Access Initiative
Liu, Li JHU
Karron, Ruth JHU
Macina, Denis Sanofi Pasteur
Kaslow, David PATH
Madhi, Shabir University of the Witwatersrand
Keller-Stanislawski, Brigitte Paul-Ehrlich-Institut
Malhame, Melissa GAVI
Kennedy, Shaina BMGF
Mangiaterra, Viviana The Global Fund
Kettler, Hannah BMGF
Mao, Kangyi BCG
King, Susan GSK
Mason, Elizabeth WHO, Retired
Klugman, Keith BMGF
McKinney, Susan USAID
Lambach, Philipp WHO
Mertsola, Jussi Turku University hospital, Finland
Murphy, William BCG
Pfleiderer, Michael Paul-Ehrlich-Institut
Mwansambo, Charles Ministry of Health ,Malawi
Pollard, Andrew University of Oxford
Nair, Harish University of Edinburgh
Privor-Dumm, Lois JHU
Nesin, Mirjana NIH
Raza, Azhar UNICEF
Neuzil, Kathleen PATH
Rees, Helen WRHI
Ng, Su Peing Sanofi Pasteur
Rodriguez, Carmen WHO
Noguchi, Lisa JHPIEGO
Savage, Kristin BMGF
O'Brien, Katherine JHU
Schmoele-Thoma, Beate Pfizer
Omer, Saad Emory University
Schrade, Christina SEEK Development / World Bank Consultant
Ozan, Esra Pfizer
Schwalbe, Nina UNICEF

73
Name Affiliation
Paterson, Pauline LSHTM
Serazin, Emily BCG
Patterson, Janna BMGF
Siegrist, Claire-Anne University of Geneva
Simoes, Eric University of Colorado
Vizzotti, Carla National Minister of Health, Argentina
Sinha, Anushua Rutgers University
Vonghangool, Vitoon Bionet-Asia Co., Ltd
Slobod, Karen Novartis
Wairagkar, Niteen BMGF
Smith, Jeffrey JHPIEGO
Were, Fredrick University of Nairobi
Sobanjo-ter Meulen, Ajoke BMGF
White, Amina NIH
Somboonsook, Boonchai Thai Food and Drug Administration
Widmyer, Greg BMGF
Steinhoff, Mark Cincinnati Children’s Hospital Medical Center
Wilson, Russell Novavax
Toussaint, Jean-François GSK
Wood, David WHO
Tsu, Vivien PATH
Yadav, Prashant University of Michigan
Veitch, Rowland Keithveitch communications
Zuber, Patrick WHO
Villafana, Tonya MedImmune/AstraZeneca