Embed Size (px)
DESCRIPTION
paper
Citation preview

Vol. 116 No. 5 November 2013
Melorheostosis and central giant cell granuloma of the mandible ina 15-year-old girlK.M. Anderson,a W.H. Shintaku,a M.S. Rosebush,b Y.B. Rawal,a and E.S. Woodardc
University of Tennessee, Memphis, TN, USA; Louisiana State University, New Orleans, LA, USA; and Woodard and Sundell, Little Rock,AR, USA
Melorheostosis is a nonhereditary bone dysplasia primarily affecting the appendicular skeleton. Because clinical and
histologic features are often nonspecific, the diagnosis is often based on the radiographic presentation. Involvement of the
craniofacial skeleton is rare. We describe a case of a 15-year-old girl with appendicular and craniofacial melorheostosis with
adjacent central giant cell granuloma. We discuss the possible significance of this previously unreported finding. (Oral Surg
Oral Med Oral Pathol Oral Radiol 2013;116:e399-e404)
Melorheostosis is a nonhereditary bone dysplasia thatprimarily affects the appendicular skeleton and mayossify adjacent soft tissues.1-3 It was initially described in1922 by Léri and Joanny; the name was derived from theGreek words for limb (melos) and flow (rhein), becausethe radiographic appearance resembled melting waxdripping down the side of a candle.4 Because the clinicaland histologic features are nonspecific, the diagnosis isoften based on the radiographic presentation.2
The typical radiographic presentation of melo-rheostosis includes an irregular hyperostosis affectingthe outer cortical bone. Frequently, the hyperostosisextends into the cancellous bone and may be eithercompletely radiopaque or a mixed pattern. Commonlocations include the diaphysis of long bones, thepelvis, the ribs, and the bones of the hands and feet.Reports of changes in the craniofacial complex are lesscommon.1 Although 4 distinct types of melorheostosisare described in the literature, the condition is morepractically classified as monostotic or polyostotic.5 Wereport a case affecting several areas including the facialbones and jaws of a 15-year-old girl. A detaileddescription of the radiographic and histologic features isprovided, including a possible association of centralgiant cell granuloma with this condition.
CASE REPORTClinical findingsA 15-year-old white girl presented for evaluation of rightmandibular swelling of unknown duration and failure of propereruption of tooth 31. On examination, palpable expansion of
aDepartment of Diagnostic Sciences and Oral Medicine, University ofTennessee College of Dentistry.bDepartment of Comprehensive Dentistry and Biomaterials, LouisianaState University School of Dentistry.cWoodard and Sundell, Oral and Maxillofacial Surgery, Implant andPeriodontal Surgery.Received for publication Feb 22, 2013; returned for revision Jul 22,2013; accepted for publication Jul 29, 2013.� 2013 Elsevier Inc. All rights reserved.2212-4403/$ - see front matterhttp://dx.doi.org/10.1016/j.oooo.2013.07.028
the right posterior mandible was noted. Intraorally, theexpansion was seen extending from the premolar area to theramus. The expansion was asymptomatic. No lymphadenop-athy was noted, and blood studies were within normal limits.No significant family history of disease was known.
Radiographic findingsA computed tomography (CT) scan of the head and neck wasobtained to evaluate the extent of structural changes. Axialand coronal images were acquired using a helical CT withexposure settings of 100 kilovolt peak, 150 mA, slice thick-ness of 0.8 mm, and resolution of 0.468 mm2. Bone changeswere noted in the right parietal, temporal, zygomatic, sphe-noid, ethmoid, maxillary, and mandibular bone (Figure 1).The lesion presented with mixed density but mostly asground-glass changes with irregular but well-delimited marginsand cortical expansion. In the right parietal and temporal bones,thickening of the cortices with sclerosis was observed. In thesphenoid, the same irregular ground-glass sclerosis was noted,including thickening of the medial and lateral pterygoid plates.The sphenoid sinus was displaced to the left and diminishedin size. Constriction of the right superior and inferior orbitalfissures was also observed. In the maxilla, 3-dimensionalreconstructions clearly exhibited involvement of only the rightside, with expansion of the outer maxillary cortex showing theclassic dripping-wax appearance of melorheostosis (Figure 2).In the nasal cavity, the inferior nasal concha was hypoplasticand superiorly displaced. Owing to cortical expansion, the rightnasal cavity was partially obliterated. Other radiographicfindings in the maxilla included superior displacementof the floor of the right sinus and impaction of the fullydeveloped right second molar tooth and developing thirdmolar. In the mandible, the same ground-glass changes withcortical expansion extended posteriorly from the periapicalregion of the right mandibular canine to the posterior third ofthe ramus. Changes extended superiorly from the lowerborder of the mandible to the sigmoid notch and coronoidprocess. The right condyle was not involved. The mandib-ular canal was inferiorly displaced and constricted in someareas. The mandibular right second molar was buccally dis-placed, and the third molar was lingually displaced. The molarteeth of the right jaws exhibited a somewhat abnormalmorphology, with underdeveloped and stunted roots, whencompared with the left side. The mandibular right second
e399

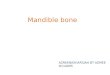
Fig. 1. Computed tomography (CT) examination. A, Panoramic reconstruction from CT data. Note ground-glass bone, dentaldisplacement, and widening of periodontal ligament spaces in the right maxilla and mandible. B, Coronal CT reconstruction depictsextension of lesion in the sphenoid and mandible. Note lateral displacement of the right sphenoid sinus and thickening of thepterygoid process and mandible, with cortical expansion and inferior displacement of the mandibular canal. C, In the axial CT scan,unilateral involvement is noted with typical ground-glass bone and cortical expansion of the anterior maxilla, as well as similarchanges of the right mandible. Note multilocular radiolucency in the medial aspect of the right mandible.
ORAL AND MAXILLOFACIAL RADIOLOGY OOOO
e400 Anderson et al. November 2013
molar was impacted, with root dilaceration. A multilocularradiolucency with scalloped margins and cortical thinningwith expansion was noted in the right posterior mandible. Allinvolved maxillary and mandibular teeth exhibited irregularwidening of the periodontal ligament spaces and absence oflamina dura.
In addition to the CT scan, radiographic plain projectionsof the lower limb were available and demonstrated addi-tional characteristic findings associated with appendicularmelorheostosis. In the lateral projection of the left femur(Figure 3, A) and anteroposterior projection of the lower limb(see Figure 3, B), endosteal hyperostosis, linear ground-glasssclerosis, and mild expansion were present in the diaphysis ofboth the femur and tibia. In the epiphyses of these bones,rounded areas of hyperostosis with irregular contours char-acteristic of melorheostosis were present. Dorsiplantar andlateral projections of the left foot showed similar irregularendosteal hyperostosis involving the first and second distal,intermediate, and proximal phalanges; metatarsals I and II; themedial and intermediate cuneiforms; and the navicular bones.Lateral deviation of the second toe was also evident (seeFigure 3, C).
Histopathologic findingsMicroscopic examination of the radiolucent lesionremoved from the right posterior mandible showed a benign
proliferation of ovoid to spindle-shaped cells within a back-ground of dense fibrous connective tissue. Scatteredthroughout the tissue were numerous multinucleated giantcells, with prominent erythrocyte extravasation and hemo-siderin deposition (Figure 4). Based on these features,a diagnosis of central giant cell granuloma was made. Asubsequent biopsy of the mandibular bony changes was laterdone, with a diagnosis of dense cortical bone, consistent withmelorheostosis.
At the 3-year follow-up in March 2010, no recurrence ofthe giant cell granuloma was seen clinically or radiographi-cally. However, some clinical deformity was noted involvingthe right temporal region as the patient’s melorheostosiscontinued to progress. Ocular symptoms, consisting of partialblindness, had also developed, necessitating optic nervedecompression the previous year. Additional sensory distur-bances were not reported.
DISCUSSIONMelorheostosis is a rare, benign bone disorder char-acterized by hyperostosis that, in later stages, radio-graphically resembles melting candle wax. It isclassified among the “sclerosing bone dysplasias,”which also include disorders such as craniometaphy-seal and diaphyseal dysplasias, osteopetrosis, pykno-dysostosis, osteopoikilosis, and osteopathia striata.6

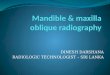
Fig. 2. Three-dimensional model. Note the dripping-waxappearance distinctive of melorheostosis in the anterior aspectof the right maxilla.
OOOO CASE REPORT
Volume 116, Number 5 Anderson et al. e401
Occasionally, patients exhibit more than one scle-rosing disorder; such comorbidity is referred toas mixed sclerosing bone dysplasia or overlapsyndrome.7
The estimated incidence of melorheostosis is 0.9per 1 million persons.8 There is an equal distributionbetween males and females.1 The disease most oftenmanifests in childhood or early adolescence, withmost patients showing evidence of the disease byage 20.8,9 However, the initial presentation mayoccur as late as age 61, with a second peak occur-ring in the fourth and fifth decades.8 In rare cases,the deformity or limitation of motion has been notedat birth.10
Melorheostosis may be monostotic, polyostotic, ormonomelic (affecting a single limb).2 Although thedisease is primarily seen in the long bones, any bonemay be affected. The lower extremities are morecommonly affected than the upper extremities.11
Uncommon sites of involvement include the skull,spine, and ribs.4 Involvement tends to be unilateral, andthis case was unusual, owing to its bilateral presentationof lesions in the left appendicular skeleton and rightcraniofacial bones.
Four distinct types and one combination of types ofmelorheostosis have been described, based on radio-graphic presentation.11 Type A is characterized by anosteoma-like appearance. Type B represents the classic“flowing” hyperostosis. Type C shows a myositisossificanselike pattern, especially around the joints.
Type D demonstrates features similar to osteopathiastriata. A mixture of patterns is seen in Type E.Although the practical classification of the submittedcase would be polyostotic melorheostosis, theinvolvement of the craniofacial regions and appendic-ular skeleton with both ground-glass sclerosis and theclassic “flowing” hyperostosis would fall under themixed pattern, or Type E.
Radiographic changes of melorheostosis typicallyshow endosteal sclerosis of the long axis of the bone,primarily limited to one limb.8 The hyperostosis isusually confined to one lateral side of the bone, butsmall bones of the hand may be completely involved.12
There is usually a distinct demarcation between lesionaland normal bone, a feature readily seen on CT scans.6
Extraosseous bone deposition may also occur.12
In infancy and childhood, the hyperostosis may notbe a prominent feature. However, with the naturalprogression of the disease, radiographic changes becomemore apparent. Early lesions show a streaky or patchyendosteal distribution, with the more distinct “flowing”periosteal distribution seen later and primarily inadults.3,4 The linear hyperostosis often extends alonga limb, from one bone to the next, continuing into thecarpus or the tarsus, and potentially as far as thephalanges.4 Typically, the diagnosis of melorheostosisis based on the radiologic signs and bone histologyshowing sclerosis without cellular abnormalities.8
Although CT or magnetic resonance imaging is notneeded in most cases, scintigraphy reveals abnormaltracer uptake in melorheostosis and can be helpful in thediagnosis of equivocal cases.6
Numerous clinical features have been described inpatients with melorheostosis, and signs and symptomsmay appear before any radiographic changes.4 Typi-cally, more severe symptoms are associated withextensive hyperostosis, as well as a greater number ofaffected bones.11 Chronic pain, which ranges inseverity, is a relatively consistent finding. However, it isoften less prominent in children than in adults.11 Whenpresent, the pain is usually felt when the patient is atrest and during the night.
In younger patients, the initial presentation mayinvolve limb length discrepancy or joint contractures,sometimes several years before the onset of pain.2,3
Premature closure of the epiphyseal plate results inshortening of the limbs or angulation.12 Reported softtissue findings include joint stiffness, limitation ofmotion, muscle atrophy, subcutaneous fibrosis, cir-cumscribed scleroderma, skin hyperpigmentation,paresthesia, palpable soft tissue masses, and vascularmalformations.4,8,11,12 Blood test results are withinnormal limits.1 Involvement of the craniofacial skeletonby melorheostosis is exceedingly rare, and most ofthese patients will also have involvement of the

Table I. Published reports of craniofacial melorheostosis
Reference Person affected (age, gender) Year published Craniofacial involvement
Franklin and Matheson13 41-year-old woman 1942 Enlargement of the right skulland mandible
Williams et al.2 Elderly woman 1990 None*
Tueche et al.14 21-year-old man 1999 None*
Mariaud-Schmidt et al.9 11-year-old girl 2002 Facial asymmetry andcontractural deformities
Ethunandan et al.1 66-year-old woman 2004 Left facial swellingKuttenberger et al.8 18-year-old (gender not given) 2006 Left mandibular painParashar et al.7 11-year-old girl 2007 Right maxillary swellingParashar et al.7 27-year-old man 2007 Left mandibular swellingAnderson et al. (current case) 15-year-old girl 2013 Right mandibular swelling
*Craniofacial involvement was subclinical and was discovered after discovery at other skeletal sites.
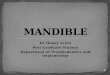
Fig. 3. A, Lateral 2-dimensional image of the left femur depicts ground-glass endosteal hyperostosis with cortical expansion in theepiphysis and diaphysis. B, Anteroposterior projection of the left tibia and fibula, with involvement of the tibia exhibitinghyperostosis of the epiphysis and diaphysis. C, Various 2-dimensional projections depict involvement of the left foot, withhyperostosis and lateral deviation of the second toe.
ORAL AND MAXILLOFACIAL RADIOLOGY OOOO
e402 Anderson et al. November 2013
appendicular skeleton.1 Currently, 8 cases of cranio-facial melorheostosis have been reported in theEnglish-language literature and are summarized inTable I, along with the current case. Most cases havebeen seen in girls and women and initially present asswelling of the maxilla or mandible. Pain is nota consistent finding. Displacement of teeth is not seen.Although symptoms may also include paresthesia orsensory disturbances, no loss or impairment of sensoryor motor function has been reported in cases of thecraniofacial region.7
The radiographic features of craniofacial melo-rheostosis can be quite different from those of appendic-ular melorheostosis. In contrast to the classic melted-waxappearance seen in the long bones, melorheostosis ofthe craniofacial skeleton shows either homogeneoussclerosis, with an increase in volume, or focal irregularsclerosis, without changes in volume.8 Melorheostosisof the jaws can mimic other bone tumors such as
osteoma and osteosarcoma. As observed in this case,a ground-glass radiographic appearance similar tofibrous dysplasia may also be seen.
The histopathology of melorheostosis is typicallynonspecific and rarely provides a definitive diagnosis.Rather, its utility lies in the exclusion of other conditions,and biopsy is therefore recommended to rule out osteo-sarcoma, which is also painful.7 Microscopic specimensshow a mixture of immature woven bone and somewhatdisorganized lamellar bone. The haversian patterns areoften irregular and may be obliterated by thickenedtrabeculae. Vessels are frequently surrounded by wovenbone or osteoid rather than lamellar bone. Within themarrow spaces, osteoid and fibrous tissue may be seensurrounding areas of new bone formation. Osteoblasticor osteoclastic activity is not prominent, and cellularatypia or anaplasia is absent.1,8,11,15
Lesions resembling giant cell granuloma have notbeen previously reported in the setting of melorheostosis.

OOOO CASE REPORT
Volume 116, Number 5 Anderson et al. e403
Central giant cell granuloma of the jaws typicallypresents as a unilocular to multilocular radiolucency.The differential diagnosis of these lesions includesodontogenic keratocyst, ameloblastoma, intraosseousvascular malformation, and odontogenic myxoma.Our patient was diagnosed with a giant cell granu-loma of the mandible associated with an uneruptedtooth and within an area of increased bone density.It is unclear whether this lesion is related to thepatient’s melorheostosis or is a concurrent but sepa-rate process. Giant cell granulomas have been re-ported in association with fibro-osseous processes,such as ossifying fibroma or Paget disease of bone.In these conditions, it is thought that the giant cellgranuloma may be a reaction to changes in stromawithin the original lesion. These changes couldinvolve osteoblasts, which in turn have the capacityto activate osteoclasts. It is possible that a similarmechanism may be in effect in the present case andmay be a previously unreported feature in theevolution of this condition.16,17
The differential diagnosis of melorheostosis isextensive and includes sclerosing osteomyelitis, osteo-sarcoma, fibrous dysplasia, and the sclerosing bonedysplasias.6,8 Differentiating melorheostosis from theseother conditions requires careful assessment of theclinical, radiographic, histopathologic, and laboratoryfindings in combination. Osteopetrosis is typicallya bilateral condition and can often be excluded clini-cally. Fibrous dysplasia and osteosarcoma can bedifferentiated from melorheostosis microscopically.Bone scintigraphy also can be a useful diagnostic tool.Increased uptake of technetium 99 m pyrophosphate isseen in melorheostosis, but not in osteopoikilosis orosteopathia striata.5 Melorheostosis may be differenti-ated from sclerosing osteomyelitis by a normal bloodcell count and C-reactive protein level.
The etiology of melorheostosis is unclear.Proposed theories include vascular disturbances,inflammatory and degenerative processes, defects inembryogenesis, and abnormalities in innervation.1
The segmental bony and soft tissue pattern lendssupport to the theory of an embryonic insult to thesensory nerves.6,11 The distribution of lesions inmelorheostosis corresponds to distinct sclerotomes, orareas of bone innervated by individual spinal sensorynerves.5 Although germ line mutations have beenidentified in some cases, a consistent genetic defectremains unidentified.18
Treatment primarily consists of symptomatic care,surgical correction of deformity, and physical therapy.12
Nonsteroidal anti-inflammatory medications are effec-tive in the relief of pain, and some benefit has been seenwith vasodilators or diphosphonates.8 Because thecontractures are difficult to manage and recurrence is
not uncommon, surgical intervention should ideally bepostponed until skeletal maturity is achieved.3 Beyondthe associated deformity and variable disability, theoverall prognosis is good. The condition is typicallybenign; however, osteosarcoma arising in melo-rheostosis has been reported.7 Although progression israpid during active growth, the disease tends to slowduring adulthood, with periods of recurrence.9 Sponta-neous cessation is occasionally seen, and surgery is notalways necessary.6,8
In conclusion, we report a case of craniofacialmelorheostosis with concomitant central giant cellgranuloma. Although previously unreported, the rela-tionship between these 2 processes is considered.Further reports of craniofacial melorheostosis mayclarify this relationship.
REFERENCES1. Ethunandan M, Khosla N, Tilley E, Webb A. Melorheostosis
involving the craniofacial skeleton. J Craniofac Surg. 2004;15:1062-1065.
2. Williams JW, Monaghan D, Barrington NA. Craniofacial melo-rheostosis: case report and review of the literature. Br J Radiol.1991;64:60-62.
3. Younge D, Drummond D, Herring J, Cruess RL. Melorheostosisin children: clinical features and natural history. J Bone JointSurg. 1979;61B:415-418.
4. Campbell CJ, Papademetriou T, Bonfiglio M. Melorheostosis:report of the clinical, roentgenographic, and pathologicalfindings in fourteen cases. J Bone Joint Surg. 1968;50A:1281-1303.
5. Jain VK, Arya RK, Bharadwaj M, Kumar S. Melorheostosis:clinicopathological features, diagnosis, and management. Ortho-pedics. 2009;32:512.
6. Azouz ME, Greenspan A. Melorheostosis. In: Orphanet Encyclo-pedia. Paris, France: Orphanet; 2005. Available at: http://orpha.net/data/patho/GB/uk-Melorheostosis.pdf.
7. Parashar P, Musella A, Novak T, Greer RO. Melorheostosis:report of two cases affecting the jaw. Oral Surg Oral Med OralPathol Oral Radiol Endod. 2007;104:e66-e70.
8. Kuttenberger JJ, Hardt N, Gebbers JO, Hofer B. Osteoscleroticbone dysplasia (melorheostosis) of the mandible. Int J OralMaxillofac Surg. 2006;35:1164-1167.
9. Mariaud-Schmidt RP, Bitar WE, Perez-Lamero F, Barros-Nunez P. Melorheostosis: unusual presentation in a girl. J ClinImaging. 2002;26:58-62.
10. Morris JM, Samilson RL, Corley CL. Melorheostosis: review ofthe literature and report of an interesting case with a nineteen-yearfollow-up. J Bone Joint Surg. 1963;45A:1191-1206.
11. Freyschmidt J. Melorheostosis: a review of 23 cases. Eur Radiol.2001;11:474-479.
12. Rozencwaig R, Wilson MR, McFarland GB. Melorheostosis. AmJ Orthoped. 1997;26:83-89.
13. Franklin EL, Matheson I. Melorheostosis: report on a case witha review of the literature. Br J Radiol. 1942;15:185-191.
14. Tueche SG, Gebhart M, Dewolf J, Baillon JM, Limbosch JM.Craniofacial and humeral melorheostosis. Acta Chir Belg.1999;99:47-50.
15. Hoshi K, Amizuka N, Kurokawa T, Nakamura K, Shiro R,Ozawa H. Histopathological characterization of melorheostosis.Orthopedics. 2001;24:273-277.

ORAL AND MAXILLOFACIAL RADIOLOGY OOOO
e404 Anderson et al. November 2013
16. Farzaneh AH, Pardis PM. Giant cell granuloma and fibrousdysplasia occurring in the same jaw. Med Oral Patol Oral CirBucal. 2005;10(suppl 2):E130-E132.
17. Penfold CN, McCullagh P, Eveson JW, Ramsay A. Giant celllesions complicating fibro-osseous conditions of the jaws. Int JOral Maxillofac Surg. 1993;22:158-162.
18. Hellemans J, Debeer P, Wright M, et al. Germline LEMD3mutations are rare in sporadic patients with isolated melo-rheostosis. Hum Mutat. 2006;27:290.
Reprint requests:
K. Mark AndersonDiagnostic Sciences and Oral MedicineUniversity of Tennessee College of Dentistry875 Union AveMemphis, TN [email protected]