Embed Size (px)
Citation preview
Arteriovenous Malformation of the Mandible:Embolization and Direct Injection TherapyWilliam W.Y. Siu, MD, Alain Weill, MD, Jean Luc Gariepy, MD, Jacques Moret, MD, and Tom Marotta, MD
Arteriovenous malformation (AVM) of the mandible is a rare entity but one that can be potentially fatal as a result ofmassive hemorrhage. Traditional treatment involved extensive surgical resection of the mandible. With the advent ofimproved endovascular techniques, interventional radiology is now the best method to control active hemorrhage andultimately cure these lesions. The authors describe three cases of successfully treated mandibular AVM by percuta-neous and/or endovascular techniques.
Index terms: Arteriovenous malformations, mandibular • Embolization • Jaws, abnormalities
J Vasc Interv Radiol 2001; 12:1095–1098
Abbreviation: AVM 5 arteriovenous malformation
ALTHOUGH arteriovenous malfor-mation (AVM) of the mandible is arare entity, it must be recognized bydentists, oral surgeons, and radiolo-gists because of its potentially life-threatening complication. A commonpresentation is a spontaneously loos-ened tooth that if dislodged or ex-tracted may result in rapid massivehemorrhage and possibly death in anotherwise healthy young patient. Thediagnosis of an AVM should be sus-pected when radiographic imagingdemonstrates a lytic lesion in the man-dible associated with the loose tooth(1). Traditional treatments includedextensive surgical resection and man-dibular reconstruction to preserve theobvious functions and esthetics of themandible. With the advent of modernendovascular and percutaneous tech-niques, successful treatment of man-dibular AVM by interventional radio-logic means is possible.
CASE 1
A 15-year-old girl presented with aloose left lower second molar. Investiga-tions performed at another institutionincluded a computed tomographic (CT)scan that showed a lytic lesion of the leftmandible and an angiogram that dem-onstrated a mandibular AVM. Electivepreoperative arterial embolization fol-lowed by surgical resection were origi-nally planned. While waiting for theprocedure, massive hemorrhage beganto occur from around the loosenedtooth. The bleeding was controlled byextensive packing of the oral cavity. Shewas stabilized with blood transfusionsand transferred to our institution foremergency embolization. The emboliza-tion procedure was performed undergeneral anesthesia with transnasal en-dotracheal intubation because the oralcavity was filled with packing material.Right femoral arterial and venous punc-tures were performed. An initial left ex-ternal carotid artery angiogram demon-strated a high-flow mandibular AVMsupplied by the internal maxillary (Fig1a), facial, and lingual arteries. A largevenous pouch was present in the leftbody and ramus of the mandibledrained by the retromandibular veininto the left internal jugular vein. Theinternal maxillary artery was first embo-lized with large-sized particles (355–500mm Contour Emboli, Target Therapeu-tics, Fremont, CA) to decrease the flow
rate of the AVM. The facial artery wasthen catheterized and a venous “roadmap” was made, allowing transvenousplacement of a microcatheter into thevenous pouch (Fig 1b). A subsequentsynchronous injection of contrast mate-rial through the arterial and venouscatheters provoked massive rebleedingaround the loosened molar (Fig 1c). A2-mL mixture of 25% glue (Histoacryl;B. Braun, Melsungen, Germany) and75% lipiodol (Lipiodol Ultra-fluid;Guerbet/Therapex, Montreal, PQ, Can-ada) was immediately injected throughthe venous catheter while compressionof the internal jugular vein was appliedto prevent escape of glue into the sys-temic venous system. A small residualvenous pouch was still present andbleeding persisted, albeit slowed. Theoral packing was removed, emboliza-tion by direct puncture was performedinto the bleeding area around the loosemolar with a 18-gauge needle, and afurther 4 mL of 50% glue/lipiodol mix-ture was injected. A postembolizationexternal carotid injection showedcomplete eradication of the AVM(Figs 1d, e). Repeat angiograms 2days and 3 months later confirmedcontinued closure of the AVM. Theloosened molar was subsequentlyextracted along with removal of asmall amount of extruded glue ma-terial into the oral cavity without anyfurther bleeding complications.
From the Department of Radiology (W.W.Y.S.,A.W., T.M.), Vancouver General Hospital, Vancou-ver, British Columbia; Department of Radiology(J.L.G.), Hopital De L’enfant-Jesus, Quebec City,Quebec, Canada; and Department of InterventionalNeuroradiology (J.M.), Fondation OphtalmologiqueAdolphe De Rothschild, Paris, France. Received Jan-uary 25, 2001; revision requested March 20; revisionreceived and accepted May 15. Address correspon-dence to A.W., Vancouver General Hospital, 855West 12th Ave., Vancouver, BC, Canada V5Z 1M9.
© SCVIR, 2001
Brief Reports
1095
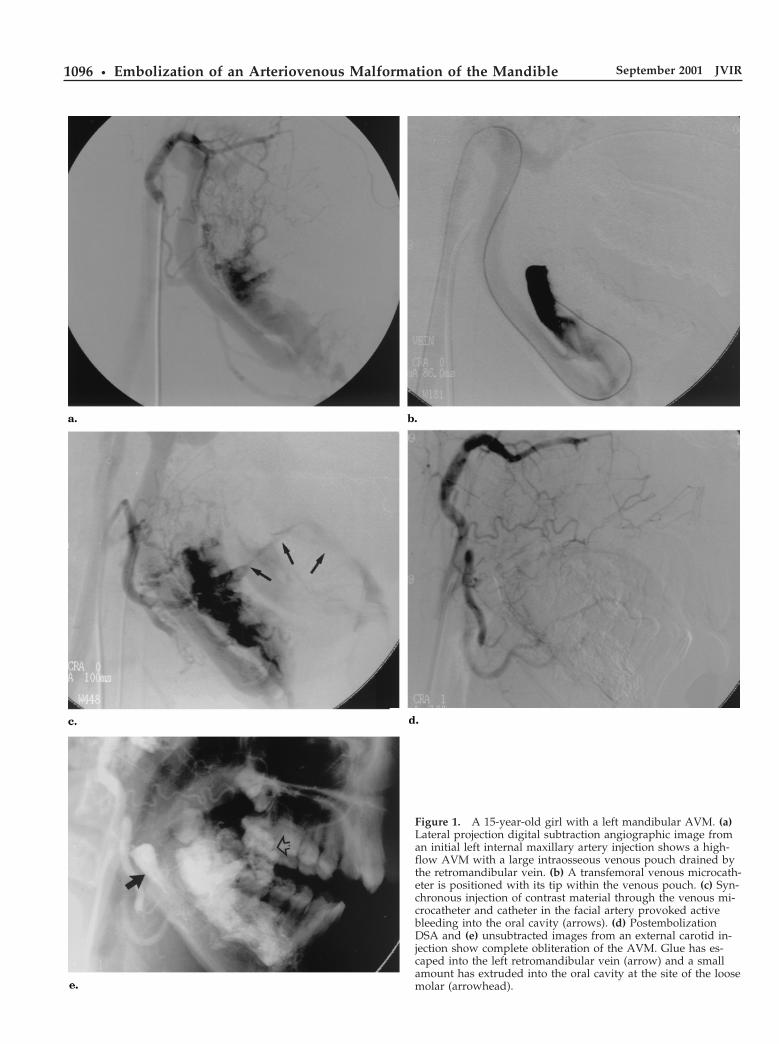
Figure 1. A 15-year-old girl with a left mandibular AVM. (a)Lateral projection digital subtraction angiographic image froman initial left internal maxillary artery injection shows a high-flow AVM with a large intraosseous venous pouch drained bythe retromandibular vein. (b) A transfemoral venous microcath-eter is positioned with its tip within the venous pouch. (c) Syn-chronous injection of contrast material through the venous mi-crocatheter and catheter in the facial artery provoked activebleeding into the oral cavity (arrows). (d) PostembolizationDSA and (e) unsubtracted images from an external carotid in-jection show complete obliteration of the AVM. Glue has es-caped into the left retromandibular vein (arrow) and a smallamount has extruded into the oral cavity at the site of the loosemolar (arrowhead).
1096 • Embolization of an Arteriovenous Malformation of the Mandible September 2001 JVIR
CASE 2
A 15-year-old boy presented to adentist with a loose left second lowermolar associated with a small amountof bleeding when the tooth wasslightly mobilized. A CT studyshowed a lytic lesion (Fig 2a) and aninitial diagnosis of an adamantinomawas made. Biopsy was performed onthe lesion in an operating room undergeneral anesthesia, which resulted inmassive hemorrhage that could not becontrolled with packing. An emergentsurgical ligation of the left external ca-rotid artery was then performed, butthe bleeding did not stop. Blood trans-fusions were given and a tracheos-tomy was made. The bleeding site waspacked and the patient underwent an-giography, which demonstrated an
AVM of the left mandible. Because ofligation of the left external carotid ar-tery, the AVM was now fed by thevertebrobasilar system via collateralwith the left occipital artery (Fig 2b).Transarterial embolization was at-tempted but was unsuccessful becauseof an inability to navigate a catheterthrough these newly formed collateralvessels. The patient was then trans-ferred to our institution for treatment.A direct percutaneous puncture intothe venous pouch was performed witha bone marrow aspiration/intraosse-ous infusion 15-gauge needle (IllinoisNeedle, McGaw Park, IL) under fluo-roscopic guidance (Fig 2c). A 2.6-mLmixture of 50% glue/lipiodol (Histo-acryl, B. Braun; Lipiodol Ultra-fluid,Guerbet/Therapex) was injected, with
near complete filling of the venouspouch, but a small pool of contrastmaterial remained near the second leftmolar. The packing was removed andthe tooth spontaneously dislodged.Active hemorrhage resumed from thealveolar socket. An 18-gauge needlewas inserted into the socket and 3.2mL of 50% glue mixture was injected.The hemorrhage ceased and the AVMbecame completely obliterated on im-mediate control angiogram. Follow-upangiograms 1 month and 1 year latershowed continued obliteration of theAVM.
CASE 3
A 9-year-old boy reported left lowertooth discomfort. An orthopantomo-gram and subsequent CT demonstrateda well-defined lytic mandibular lesionwith erosion of the roots of the first andsecond molars. A dentist extracted oneof the molars in his office and massivehemorrhage occurred. The bleeding wasinitially controlled with packing so thepatient was discharged home from theoffice. The bleeding resumed later thatday. The patient’s father, with use ofdigital pressure on the bleeding area,was able to gain some control of thehemorrhage and the pair presented toour institution. An angiogram was per-formed showing a left mandibularAVM. The patient was moved to theoperating room and under fluoroscopiccontrol, a direct puncture was madewith an 18-gauge needle from the lin-gual buccal surface. A 3-mL mixture of33% glue and 66% lipiodol (Histoacryl,B. Braun; Lipiodol Ultra-fluid, Guerbet/Therapex) was injected. Intraoperativeangiography initially showed no furtherfilling of the AVM, but when digitalpressure was removed, bleeding re-sumed. The bleeding site was found anda further 2.5 mL of 50% glue mixturewas injected and the AVM was obliter-ated. A control angiogram 3 days latershowed continued closure of the AVMand a repeat orthopantomogramshowed glue material completely fillingthe venous pouch.
DISCUSSION
Mandibular AVM has traditionallybeen treated by surgery. Surgical re-section generally requires extensivebony resection and complicated recon-struction to try to maintain function of
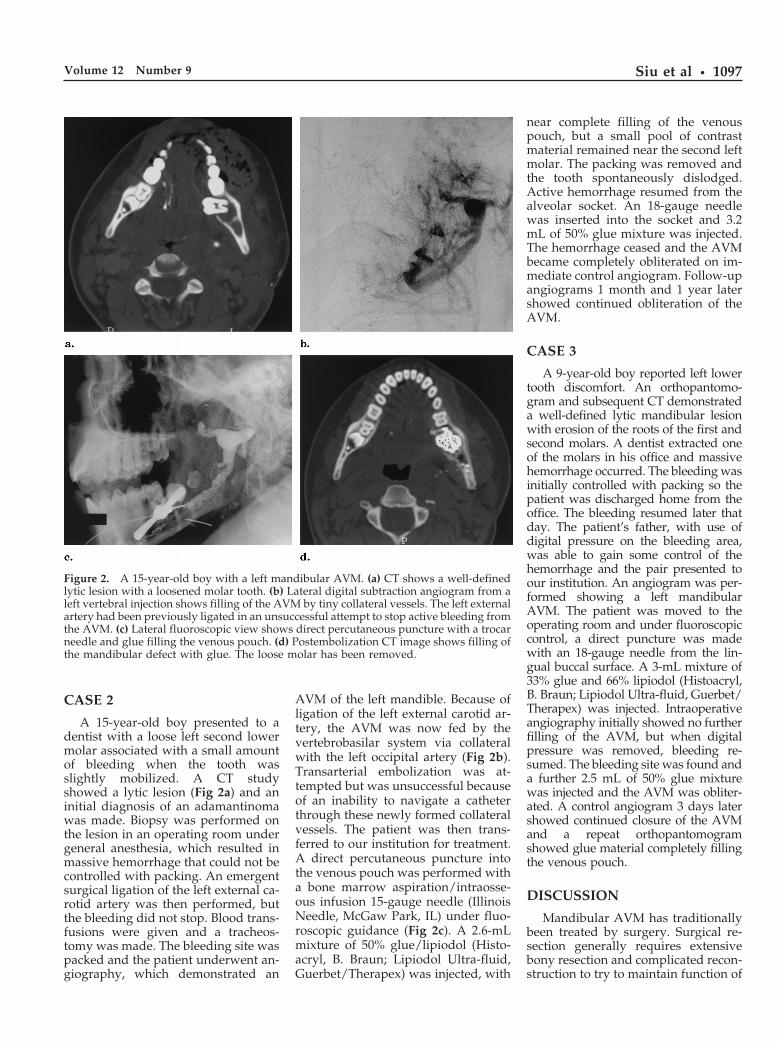
Figure 2. A 15-year-old boy with a left mandibular AVM. (a) CT shows a well-definedlytic lesion with a loosened molar tooth. (b) Lateral digital subtraction angiogram from aleft vertebral injection shows filling of the AVM by tiny collateral vessels. The left externalartery had been previously ligated in an unsuccessful attempt to stop active bleeding fromthe AVM. (c) Lateral fluoroscopic view shows direct percutaneous puncture with a trocarneedle and glue filling the venous pouch. (d) Postembolization CT image shows filling ofthe mandibular defect with glue. The loose molar has been removed.
Siu et al • 1097Volume 12 Number 9

the mandible and prevent disfigure-ment. Substantial intraoperative hem-orrhage may occur, which can be re-duced somewhat with preoperativeintraarterial embolization. Radiationhas been tried with some success (1,2).Ligation or endovascular occlusion ofthe feeding vessel, often an externalcarotid artery, is a mistake: it will notcontrol the bleeding (3,4) because col-lateral vessels are rapidly recruitedfrom either the contralateral externalcarotid artery or the vertebral system,as illustrated in case 2. Additionally,embolization will be difficult, if notimpossible.
AVM of the mandible is effectivelytreated by percutaneous and/or endo-vascular methods without the need forsurgery, as shown in these three cases.Intraarterial embolization alone is of-ten ineffective because the arterialpedicles occlude before complete fill-ing of the venous pouch, leading to ahigh recurrence rate (2).
The main embolic agent used in ourcases was cyanoacrylate (ie, glue). Weused a higher concentration of glue/lipiodol when injecting through a nee-dle versus through a catheter forquicker polymerization and because,even when glued, a needle can alwaysbe retrieved safely. The volume of glueneeded to cure the AVM is impossibleto determine in advance. The injec-tions should be continued until nomore angiographic shunt or bleedingare observed. Treatment with cyano-acrylate has been described beforewith good results, but any liquid ad-hesive will also do (5–8).
Other nonliquid embolization ma-terials have also been used with suc-cess (6,7,9). Chiras et al (6) describedtwo cases treated with initial intraar-terial particle embolization followedby direct puncture into the venouspouches for injection of Gelfoam(Pharmacia & Upjohn, Kalamazoo, MI)soaked in a thrombotic agent. In one of
their cases, direct percutaneous de-ployment of a detachable balloon wasalso performed. Kiyosue et al (7) andBeek (8) each described case reports ofsuccessful treatment with use of in-traarterial particle embolization plustransvenous coil embolization.
Reossification of the lytic lesion af-ter successful treatment is expected onlong term follow-up, as shown byShira (5), Chiras (6), and Flandroy (8).
Important points can be made fromour experiences treating AVM of themandible. Careful review of the liter-ature (3–9) and our three cases showsthat AVM limited to the mandibledrains almost exclusively through anintramandibular pouch. As a result,during treatment, if the pressure inthis pouch is increased (ie, contrast in-jection in the pouch as in case 1, orocclusion of the venous exit of thepouch before complete thrombosis asin cases 2 and 3), massive oral bleed-ing can occur. Therefore, the pro-cedure should be performed undergeneral anesthesia with transnasal en-dotracheal intubation to allow easieraccess to the oral cavity. A syringewith the glue mixture should bereadily available for percutaneous in-jection directly into the bleeding site.
Although clinically and angio-graphically impressive, AVMs of themandible are easier to cure than mostother facial AVMs (10) because, whenocclusion of the venous pouch withoutbleeding to the oral cavity is achieved,the malformation is cured. This is trueregardless of the type of treatmentused (endovascular vs direct punc-ture) or the material used (glue, Gel-foam, coil, balloons, Ethibloc [Johnson& Johnson International, Brussels,Beglium]) to occlude the outlet of theAVM.
Acknowledgments: The authors thankMark Lee (Research Assistant, Departmentof Radiology, Vancouver General Hospital)
for the help provided in the preparation ofthis manuscript.
References1. Anderson JH, Grisius RJ, McKean TW.
Arteriovenous malformation of themandible. Oral Surg Oral Med OralPathol 1981; 52:118–125.
2. Svane TJ, Smith BR, Wolford LM, PaceLL. Arteriovenous malformation ofthe mandible and its treatment: a casereport. Oral Surg Oral Med Oral Pathol1989; 67:379–383.
3. Remonda L, Schroth G, Ozdoba C,Lovblad K, Ladrach K, Huber P. Fa-cial intraosseous arteriovenous malfor-mations: CT and MR features. J Com-put Assist Tomogr 1995; 19:277–281.
4. Sofferman RA, Summers GW. Bilat-eral arteriovenous malformation of themandible. Ann Otol Rhinol Laryngol1991; 100:759–767.
5. Shira RB. Treatment of a central arte-riovenous malformation of the mandi-ble with cyanoacrylate: a 4-year follow-up. Oral Surg Oral Med Oral Pathol1988; 65:267–271.
6. Chiras J, Hassine D, Goudot P, MederJF, Guilbert JF, Bories J. Treatment ofarteriovenous malformations of themandible by arterial and venous embo-lization. Am J Neuroradiol 1990; 11:1191–1194.
7. Kiyosue H, Mori H, Hori Y, OkaharaM, Kawano K, Mizuki H. Treatmentof mandibular arteriovenous malfor-mation by transvenous embolization: acase report. Head Neck 1999; 21:574–577.
8. Flandroy P, Pruvo JP. Treatment ofmandibular arteriovenous malforma-tions by direct transosseous puncture:report of two cases. Cardiovasc Inter-vent Radiol 1994; 17:222–225.
9. Beek FJA, ten Broek FW, van SchaikJPJ, Mali WPTM. Transvenous embo-lisation of an arteriovenous malforma-tion of the mandible via a femoralapproach. Pediatr Radiol 1997; 27:855–857.
10. Han MH, Seong SO, Kim HD, ChangKH, Yeon KM, Han MC. Craniofacialarteriovenous malformation: preopera-tive embolization with direct punctureand injection of n-butyl cyanoacrylate.Radiology 1999; 211:661–666.
1098 • Embolization of an Arteriovenous Malformation of the Mandible September 2001 JVIR