Embed Size (px)
Citation preview

Chapter 2 Literature Review
Pharmaceutical Medicine 5 Jamia Hamdard
2.0 LITERATURE REVIEW
2.1 HISTORICAL PERSPECTIVE OF BIOEQUIVALENCE STUDIES
2.1.1 Generic drug approval process
Pre-1984: The process for generic drug approval has evolved along with changes in
federal drug law and regulations. Before enactment of the Food, Drug, and Cosmetic
Act (FDCA) in 1938, significant regulatory barriers to generic competition in the
market did not exist. Manufacturers of such products (e.g., codeine sulfate,
phenobarbital) could formulate, manufacture, and sell their products without submitting
bioequivalence or efficacy data to the FDA. The 1938 Act established a “new drug”
category, requiring manufacturers to document the safety of a product to the FDA and
established a 60-day delay before marketing could proceed, absent FDA objection.
Until 1962, generic versions of post-1938 drugs were marketed based on a“general
recognition” of safety. Typically, this designation was based on a history of safe use of
the innovator product. Such generic products were designate as “not new drugs.” (The
drugs/biologic approval process, 1998).
2.1.2 Drug price competition and patent term restoration Act of 1984 (Hatch-
Waxman Act)
The dual purposes of the Hatch-Waxman Act were to encourage the development of
new innovator drugs by extending patent rights and to establish procedures facilitating
the approval of low-cost generic drugs. These amendments to the FDCA codified in
statute an abbreviated process (ANDA) for post-1962 drugs whereby a generic company
could gain approval of its version of a drug without repeating the expensive and lengthy
clinical trials used to establish safety and efficacy of the innovator drug (Drug Price
Competition and Patent Term Restoration Act of 1984). Products approved under an
ANDA must be pharmaceutical equivalents (i.e. have the same active ingredient(s),
route of administration, dosage form, and strength) as the reference drug. They must
also be bioequivalent and the manufacturer must supply other basic technical
information related to manufacturing of the product that is normally required of an
NDA (Federal Food, Drug and Cosmetic Act, section 505(j) (8)). Generic drugs are
pharmaceutical equivalents only with respect to their active ingredients. The binders,
diluents, and excipients (filler) in the formulation, as well as the method of
manufacture, may vary. The FDA considers drug products to be therapeutic equivalents
if they are pharmaceutical equivalents and are bioequivalent. The publication,

Chapter 2 Literature Review
Pharmaceutical Medicine 6 Jamia Hamdard
Approved Drug Products with Therapeutic Equivalence Evaluations (the “Orange
Book”), identifies drug products approved by the FDA on the basis of safety and
effectiveness and includes therapeutic equivalence evaluations for approved multisource
prescription drug products. For every multiple-source product, the Orange Book cites a
letter code that indicates the FDA’s evaluation regarding the therapeutic equivalence of
the product relative to the reference innovator or brand-name product. These drugs are
placed in one of two categories as follows: “A”-rated products are considered to be
therapeutically equivalent to other pharmaceutically equivalent products; “B- rated
products are considered not to be therapeutically equivalent to other pharmaceutically
equivalent products. Class AB is a subset of “A “and includes DESI drug products and
post-1962 drug products for which actual or potential bioequivalence problems have
been resolved and that the FDA now considers to be therapeutically equivalent. Most
new generic products are defined as having “potential” problems until data is submitted
to establish their bioequivalence (The Orange book, CDER 2003).
2.1.3 Generic drug scandal and FDA reaction
In 1989 federal investigators implicated several generic industry officials in the conduct
of fraud, obstruction of justice, and noncompliance with various manufacturing
procedures. The investigations also revealed that several FDA employees had accepted
illegal gratuities or other compensation in exchange for information and assistance that
gave certain firms an advantage in the approval process. Investigators also discovered
that 10 or more generic companies had submitted fraudulent data related to
bioequivalence, stability testing, and manufacturing protocols for some of their products
(Featured Report of American Medical association: Generic Drugs (A-02)). The FDA
reacted to these findings by reorganizing its generic drug operations and conducting
comprehensive inspections. FDA investigators reevaluated data from hundreds of
generic drug applications. More than 2,550 samples of the top 30 prescribed generic
drugs or about 30% of all generic drugs on the market were collected and laboratory-
tested, and the agency conducted intensive inspections of 36 of the largest generic drug
firms and 12 contract laboratories. The agency determined that only 27 samples, or
approximately 1% of those tested, did not comply with standards of potency,
dissolution, content uniformity, product identification, moisture determination, or
purity. The FDA also tested 429 samples representing at least three different batches of
so-called narrow-therapeutic-range drugs that were currently marketed.

Chapter 2 Literature Review
Pharmaceutical Medicine 7 Jamia Hamdard
These 24 drugs, made by 73 brand-name and generic drug manufacturers, were
selected because of their potential for adverse reactions or therapeutic failure if they
lacked bioequivalence. Only five of the samples (all aminophylline tablets) failed to
meet United States Pharmacopoeia standards. None of the defects in the generic drugs
were judged to pose a public health hazard.
2.1.4 Determination of bioequivalence
Originally, bioequivalence was based on a demonstration that simple mean
bioavailability parameters differed by less than 20% from the brand-name product. In
1977 this was modified to include a “power” approach that tested the null hypothesis
that the rate and extent of bioavailability of the generic product was similar to the
innovator product, and the power of the study was sufficient to detect at least a 20%
difference.
In 1986, the FDA adopted the currently used average bioequivalence approach, which
involves a comparison of means. For immediate-release oral dosage forms, the standard
average bioequivalence determination employs a single-dose crossover study, typically
conducted in a limited number of healthy volunteers (usually 24 to 36 adults). Results
are analyzed according to whether the generic product (test), when substituted for the
brand-name product (reference), is significantly less bioavailable, and alternatively,
whether the brand-name product, when substituted for a generic product, is significantly
less bioavailable (the two 1-sided tests). The core of the bioequivalence concept is an
“absence of a significant difference.” A difference > ±20% is viewed by the FDA as
significant. By convention, all data are expressed as a ratio of the average response
(AUC and Cmax) for test/reference, so the limit expressed in the second analysis is
125% (reciprocal of 80%). Tests are carried out using an analysis of variance and
calculating a 90% confidence interval (CI) for the average of each pharmacokinetic
parameter, which must be entirely within the 80% to 125% boundaries. The width of
the CI reflects, in part, the within subject variability of the test and reference products
(CDER, 1997).
A common misconception, among manufacturers of generic products, is that the
average values between the reference and test product can vary by -20/+25%, which
could lead to large differences in efficacy between multisource products. In fact, when
applying these statistical criteria to studies involving 20 to 40 subjects, generic products

Chapter 2 Literature Review
Pharmaceutical Medicine 8 Jamia Hamdard
whose mean arithmetic bioavailability parameters differ by more than 5% to 10% from
the reference product begin failing the CI requirement. The FDA’s Office of Generic
Drugs has conducted two large surveys to quantify the differences between generic and
brand-name products. The first, conducted on 224 bioequivalence studies submitted in
approved applications during 1985 and 1986, found an average difference in AUC
measures between reference and generic products of 3.5% (Nightingale et al. 1987).
2.1.5 Current FDA guidance
The FDA in 2000 issued a final guidance for industry entitled Bioavailability and
Bioequivalence Studies for Orally Administered Drug Products–General
Considerations. In this guidance, the agency recommended non-replicated
bioequivalence study designs for most orally administered immediate-release drug
products and replicated bioequivalence study designs for modified-release dosage forms
(CDER, 2000). The guidance maintains the average bioequivalence criterion but allows
the option for a sponsor to provide rationale a priori for using another criterion to
declare bioequivalence, such as the individual bioequivalence criterion for highly
variable drug products. An additional concern with bioequivalence testing is that, with
certain drugs, it is the peak effect and not AUC that is important for the therapeutic
response or ADRs. This guidance was revised recently and recommended use of the
partial AUC as an early exposure measure instead of Tmax to address these concerns
(Bioavailability and Bioequivalence Studies for Orally Administered Drug Products--
General Considerations, CDER, 2003).
2.2 FDA REQUIREMENTS FOR BRAND-NAME AND GENERIC DRUGS
It is believed that anything which cost more is of better quality than the cheaper one.
The same is also true in case of therapeutic interventions. In general, innovator product
is believed to be better than the generic products. But FDA states that in the case of
generic drugs, this is not true. According to OGD (FDA's Office of Generic Drugs),
"The standards for quality are the same for brand name and generic products." Much of
FDA's review of generic drugs and brand name drugs is the same, as can be seen from
“FDA Requirements for Brand-Name and Generic Drugs" Table 2.1 [FDA-Available
at: http://www.fda.gov/cder/consumerinfo/generic_equivalence.htm].
There are eight major parts to the FDA's review of a firm's application to market a
generic drug:

Chapter 2 Literature Review
Pharmaceutical Medicine 9 Jamia Hamdard
1. There must be an FDA-approved brand-name drug that is the reference for the
proposed generic. The generic must have the same active ingredient or ingredients
and the same labeled strength as this reference product. It must have the same
dosage form-tablets, patches and liquids are examples of dosage forms. It must be
administered the same way, for example, swallowed as a pill or given as an
injection.
2. The manufacturer must show the generic drug is "bioequivalent" to the brand-name
drug.
3. The generic drug's labeling must be essentially the same as that of the approved
drug.
4. The firm must fully document the generic drug's chemistry, manufacturing steps,
and quality control measures. Each step of the process must be detailed for FDA
review.
5. The firm must assure the FDA that the raw materials and the finished product
meet USP specifications, if these have been set.
6. The firm must show that its generic drug maintains stability as labeled before it can
be sold. Once on the market, the firm must continue to monitor the drug's stability.
The firm must show that the container and its closure system won't interact with the
drug. Firms making sterile drugs must submit sterility assurance data showing
microbiologic integrity of these products.
7. The firm must provide a full description of the facilities it uses to manufacture,
process, test, package, and label and control the drug. It must certify that it
complies with federal regulations about current good manufacturing practices and
undergo FDA inspection of the manufacturing facility to assure compliance.
8. Before FDA approves a generic drug, it usually conducts an inspection at the
proposed manufacturing site to make sure the firm is capable of meeting its
application commitments and to ensure the firm can manufacture the product
consistently.

Chapter 2 Literature Review
Pharmaceutical Medicine 10 Jamia Hamdard
Table 2.1: Similar FDA Requirements for Brand-Name and Generic Drugs
FDA RequirementsBrandDrug
GenericDrug
For reformulations of a brand-name drug or generic versions of a drug, FDAreviews data showing the drug is bioequivalent to the one used in the originalsafety and efficacy testing.FDA evaluates the manufacturer's adherence to good manufacturing practicesbefore the drug is marketed.
FDA reviews the active and inactive ingredients used in the formulationbefore the drug is marketed.
FDA reviews the actual drug product.
FDA reviews the drug's labeling.
Manufacturer must seek FDA approval before making major manufacturingchanges or reformulating the drug.
Manufacturer must report adverse reactions and serious adverse healtheffects to the FDA.
FDA periodically inspects manufacturing plants.
FDA monitors drug quality after approval.
a number of misconceptions about generic drugs still persist among physicians and
patients [FDA Ensures Equivalence of Generic Drugs, Jan 6, 2003. Available at:
http://www fdagov/cder/consumerinfo/generic equivalence html]. Some myths and facts
are as follow:
Myths and Facts about Generic Drugs
MYTH: Generics are not as potent as brand-name drugs.
FACT: FDA requires generics to have the same quality, strength, purity, and stability as
brand-name drugs.
MYTH: Generic drugs just won't do the job as well as brand-name drugs.
FACT: Under the new law, generic drugs must be bioequivalent to their brand-name
counterparts to gain FDA approval. That means that the generics must contain the
same active ingredients and must be identical in strength, dosage form (tablet, solution,
etc.), and route of administration (for example, taken by mouth or through injection).
Further, they must release the same amount of drug into the body as the brand-name
drug.
MYTH: Generics take longer to act in the body.
Chapter 2 Literature Review
Pharmaceutical Medicine 10 Jamia Hamdard
Table 2.1: Similar FDA Requirements for Brand-Name and Generic Drugs
FDA RequirementsBrandDrug
GenericDrug
For reformulations of a brand-name drug or generic versions of a drug, FDAreviews data showing the drug is bioequivalent to the one used in the originalsafety and efficacy testing.FDA evaluates the manufacturer's adherence to good manufacturing practicesbefore the drug is marketed.
FDA reviews the active and inactive ingredients used in the formulationbefore the drug is marketed.
FDA reviews the actual drug product.
FDA reviews the drug's labeling.
Manufacturer must seek FDA approval before making major manufacturingchanges or reformulating the drug.
Manufacturer must report adverse reactions and serious adverse healtheffects to the FDA.
FDA periodically inspects manufacturing plants.
FDA monitors drug quality after approval.
a number of misconceptions about generic drugs still persist among physicians and
patients [FDA Ensures Equivalence of Generic Drugs, Jan 6, 2003. Available at:
http://www fdagov/cder/consumerinfo/generic equivalence html]. Some myths and facts
are as follow:
Myths and Facts about Generic Drugs
MYTH: Generics are not as potent as brand-name drugs.
FACT: FDA requires generics to have the same quality, strength, purity, and stability as
brand-name drugs.
MYTH: Generic drugs just won't do the job as well as brand-name drugs.
FACT: Under the new law, generic drugs must be bioequivalent to their brand-name
counterparts to gain FDA approval. That means that the generics must contain the
same active ingredients and must be identical in strength, dosage form (tablet, solution,
etc.), and route of administration (for example, taken by mouth or through injection).
Further, they must release the same amount of drug into the body as the brand-name
drug.
MYTH: Generics take longer to act in the body.
Chapter 2 Literature Review
Pharmaceutical Medicine 10 Jamia Hamdard
Table 2.1: Similar FDA Requirements for Brand-Name and Generic Drugs
FDA RequirementsBrandDrug
GenericDrug
For reformulations of a brand-name drug or generic versions of a drug, FDAreviews data showing the drug is bioequivalent to the one used in the originalsafety and efficacy testing.FDA evaluates the manufacturer's adherence to good manufacturing practicesbefore the drug is marketed.
FDA reviews the active and inactive ingredients used in the formulationbefore the drug is marketed.
FDA reviews the actual drug product.
FDA reviews the drug's labeling.
Manufacturer must seek FDA approval before making major manufacturingchanges or reformulating the drug.
Manufacturer must report adverse reactions and serious adverse healtheffects to the FDA.
FDA periodically inspects manufacturing plants.
FDA monitors drug quality after approval.
a number of misconceptions about generic drugs still persist among physicians and
patients [FDA Ensures Equivalence of Generic Drugs, Jan 6, 2003. Available at:
http://www fdagov/cder/consumerinfo/generic equivalence html]. Some myths and facts
are as follow:
Myths and Facts about Generic Drugs
MYTH: Generics are not as potent as brand-name drugs.
FACT: FDA requires generics to have the same quality, strength, purity, and stability as
brand-name drugs.
MYTH: Generic drugs just won't do the job as well as brand-name drugs.
FACT: Under the new law, generic drugs must be bioequivalent to their brand-name
counterparts to gain FDA approval. That means that the generics must contain the
same active ingredients and must be identical in strength, dosage form (tablet, solution,
etc.), and route of administration (for example, taken by mouth or through injection).
Further, they must release the same amount of drug into the body as the brand-name
drug.
MYTH: Generics take longer to act in the body.

Chapter 2 Literature Review
Pharmaceutical Medicine 11 Jamia Hamdard
FACT: The firm seeking to sell a generic drug must show that its drug delivers the same
amount of active ingredient in the same timeframe as the original product.
MYTH: Brand-name drugs are made in modern manufacturing facilities, and generics
are often made in substandard facilities.
FACT: FDA allows no drugs to be manufactured in substandard facilities. FDA officials
inspect more than 5,000 drug plants a year to ensure that standards are met. Generic
firms have state-of-the-art plants that compare favorably with those of brand-name firms.
(In fact, brand-name firms account for an estimated 70 percent to 80 percent of generic
drug production, making duplicate versions of their own or other brand-name
companies' drugs, but selling them without the brand name.
MYTH: Generics are not as safe as brand-name drugs.
FACT: FDA requires that all drugs be safe and effective and that their benefits
outweigh their risks. Since generics use the same active ingredients and are shown to
work the same way in the body, they have the same risk-benefit profile as their brand-
name counterparts.
MYTH: Generic drugs are likely to cause more side effects.
FACT: There is no evidence of this. FDA monitors reports of adverse drug reactions
and has found no difference in the rates between generic and brand-name drugs.
MYTH: Generic manufacturers only have to prove that the active ingredients in their
products get to the bloodstream. That doesn't mean that their products are used by the
body in the same way.
FACT: When the same amount of the active ingredients of the generic version gets into
the bloodstream at the same rate as the brand-name version, there is no scientific
reason to believe that the effects of the two drugs will differ.
MYTH: Most drugs are tested for bioequivalence in healthy young volunteers, yet 25
percent of all prescription drugs are taken by the elderly who don't react the same to
drugs.
FACT: While the elderly may often absorb and process (metabolize) drugs differently
than younger people, there is no proof that drugs will perform differently in them.
Further, it isn't ethical to force already weakened or disabled patients to give blood
samples and face the other discomforts of bioequivalence testing. Further, such patients

Chapter 2 Literature Review
Pharmaceutical Medicine 12 Jamia Hamdard
cannot be used in bioequivalence testing because they are virtually always taking other
drugs concurrently.
MYTH: FDA requires that brand-name manufacturers test new drugs in thousands of
patients, but it lets generic firms get by with tests in only 20 or 30 healthy volunteers.
FACT: Generic drugs are duplicates of products that have already been tested for safety
and effectiveness. Therefore, generic manufacturers need only prove to FDA that their
drug behaves the same way in the body as the original version. That requires only small-
scale tests. In fact, the same small-scale testing is done for brand-name drugs whenever
they are reformulated.
Because of the stringent regulations and complete assurance of quality of generic
products, by the US FDA, there is increased tendency of switchover from brand to
generic products. This promotion of generic use has resulted in huge cost saving (30% -
80%) on one hand, but ended with increased number of counterfeit/substandard drug
products on the other hand. This may be due to fact that drug regulations in most of
the developing countries are still not as stringent as in USA or European Union. For
example, the dissolution procedures, specified by the United States Pharmacopoeia
(USP); to test batch-to-batch uniformity, to detect manufacturing or process variation
that might influence the bioavailability and to document formulation bioequivalence,
are still not in practice in many of the developing countries.
A generic copy of reference drug must contain identical amounts of the same active
ingredients in the same dose formulation and route of administration, as well as meet
standards for purity, quality and identity. Some inactive ingredients such as binders and
fillers are allowed to differ, but must occur in the similar ratio to the active compound
as that observed in the brand name drug [Federal Register 1999], moreover, all the
inactive ingredients used in generic product must be approved with defined purity &
quality. This is where many smaller manufacturing units (>10000) differ from the bigger
one (over 100 USFDA approved) in India.
Medical profession has also realized the problem of wide variations in the therapeutic
effectiveness of various marketed brands of oral formulations containing the same
active ingredient in equal amounts. A number of patients with a history of good results
on brand name drugs observed difficulties when a generic was substituted to decrease
the cost of therapy.

Chapter 2 Literature Review
Pharmaceutical Medicine 13 Jamia Hamdard
Doctors in India are unlikely to prescribe unbranded generics despite two advisories
from the Medical Council issued in 2012 and 2013 urging them to do so, some private
and government doctors have said.
Krishan Kumar Aggarwal, a senior cardiologist in New Delhi who is also head of the
ethics committee of the Delhi Medical Council, told the BMJ: “Doctors in India are
already prescribing generic drugs, but through their brand names. If the authorities want
us to prescribe drugs through chemical names, why do they allow so many brand names
and why are there such wide price variations?” The first step should be to ensure
quality standards, quality monitoring, and quality assurance—unless doctors become
convinced [that] there is uniform quality, independent of the source of the compound, I
don’t expect doctors in India will routinely write out prescriptions with chemical names
of drugs,” Kapoor told the BMJ.
Regardless of the quality concerns, the idea to prescribe using chemical names has
some supporters, including doctors who say that the Medical Council’s advisories are a
reminder of the code of ethics physicians are expected to follow. For example, Amar
Jesani, a physician and editor of the Indian Journal of Medical Ethics, said that the
quality argument was “a hoax” at times conveniently used to prescribe specific brands.
“Doctors in India rarely think about price considerations,” Jesani told the BMJ. “With
generic prescriptions, at least consumers can demand cheaper drugs—let consumers
decide and fight it out with chemists.”
Figures from the Monthly Index of Medical Specialities (MIMS), India, suggest that 10
tablets of unbranded cetirizine, a second-generation antihistamine, were available in
2012 for about 1.50 rupees (£0.017; €0.019; $0.025), while a branded generic product
was sold at 27 rupees, and a branded version cost 39 rupees.( Zuzanna Fimińska July 02
2013)

Chapter 2 Literature Review
Pharmaceutical Medicine 14 Jamia Hamdard
BIOAVAILABILITY AND BIOEQUIVALENCE
2.3 BIOAVAILABILITY
Bioavailability is defined by the US-FDA as the rate and extent to which the active
ingredient or active moiety is absorbed from a drug product and becomes available at
the site of action. For drug products that are not intended to be absorbed into the
bloodstream, bioavailability may be assessed by measurements intended to reflect the
rate and extent to which the active ingredient or active moiety becomes available at the
site of action [Bioavailability and Bioequivalence Studies for Orally Administered Drug
Products--General Considerations. CDER, 2003].
The EMEA guidance defines Bioavailability as the rate and extent to which the active
substance or active moiety is absorbed from a pharmaceutical form and becomes
available at the site of action [Note for guidance on the investigation of bioavailability
and bioequivalence, EMEA].
The CDSCO, India, defines Bioavailability as the relative amount of drug from an
administered dosage form which enters the systemic circulation and the rate at which
the drug appears in the systemic circulation.
2.3.1 Types of bioavailability
Bioavailability can be classified into four different types depending on the purpose of
the study and scientific questions to be solved [Ritschel and Kearns 1998].
2.3.1.1 Absolute bioavailability
Absolute bioavailability is the ratio of the total area under the blood level time curve
upon extra vascular route of administration to the area under the blood level time curve
upon intravenous administration, corrected for the difference in the dose size.
Absolute bioavailability = AUC extravascular x dose i.v. / AUC i.v.x dose extravascular
2.3.1.2 Relative bioavailability
The relative bioavailability is the rate and extent of the bioavailability of a drug from two
or more different dosage forms given by the same route of administration. For
determination of rate and extent, blood level or urinary excretion data upon single or
multiple dosing can be used. According to the FDA regulation the standard used in this

Chapter 2 Literature Review
Pharmaceutical Medicine 15 Jamia Hamdard
procedure is an approved marketed drug product, a solution of the drug or suspension
of the micronized drug.
Relative bioavailability = AUCof A / AUC of B
Where B is the reference standard.
2.3.1.3 Relative optimal bioavailability
This term was suggested for optimizing extent and rate of bioavailability for a drug
product during the development phase.
For determination of EBA rel. opt, the active drug is administered in aqueous solution
without the addition of any further excipients by the same route which is intended for
the drug product under development.
EBA rel. opt. = AUC (drug + vehicle; granules; tablets) / AUC solution x 100
2.3.1.4 Bioavailability in presence of first-pass effect
Drugs showing a first-pass effect may result in considerably lower blood level time
curves. Even though the entire parent drug was absorbed from the site of
administration, it does not reach systemic circulation in unchanged form.
The fraction of a peroral (po) or in part, rectal dose reaching systemic circulation F,
under the assumption of otherwise linear kinetics can be described by eqn.
F = 1- Dose iv x fm / LBF x AUCiv x 60 x
LBF - liver blood flow
fm - fraction of drug metabolised in liver
- Ratio of the concentration of the drug in whole blood to that in plasma
2.3.2 Different approaches used for measurement of bioavailability
There are several direct and indirect methods for the measurement of bioavailability in
humans. The selection of method depends on the purpose of the study, analytical
method and nature of the drug product. The methods can be broadly divided into two
categories: (a) Pharmacokinetic methods (b) Pharmacodynamic methods.

Chapter 2 Literature Review
Pharmaceutical Medicine 16 Jamia Hamdard
2.3.2.1 Pharmacokinetic Methods
These are very widely used and are based on the assumption that the pharmacokinetic
profile reflects the therapeutic effectiveness of a drug. Thus these are indirect methods.
The two major pharmacokinetic methods are;
Plasma level-time studies
Unless determination of plasma drug concentration is difficult or impossible, it is the
most reliable method and method of choice in comparison to urine data. This method
is based on the assumption that two dosage forms that exhibit “superimposable” plasma
level-time profiles in a group of subjects should result in identical therapeutic activity.
The three parameters of plasma level-time studies, which are considered important for
determining bioavailability, are:
1. Cmax: The peak plasma concentration that gives an indication whether the drug is
sufficiently absorbed systemically to provide a therapeutic response.
2. Tmax: The time of peak plasma concentration corresponds to the time required
to reach maximum drug concentration after drug administration. At Tmax,
absorption is maximized and the rate of drug absorption equals the rate of drug
elimination. When comparing drug products, tmax can be used as an approximate
indication of the drug absorption rate.
3. AUC: The area under the plasma level-time curve that gives a measure of the
extent of absorption or the amount of drug that reaches the systemic circulation.
The extent of bioavailability can be determined by equation-
F = AUCoral Div / AUCiv Doral
Urinary excretion studies
This method of assessing bioavailability is based on the principle that the urinary
excretion of unchanged drug is directly proportional to the plasma concentration of
drug. This method is particularly useful for drugs extensively excreted unchanged in the
urine. The method involves collection of urine at regular intervals for a time span equal
to 7-10 biological half-lives, analysis of unchanged drug in the collected sample and
determination of the amount of drug excreted in each interval and cumulative amount
excreted. The three major parameters examined in urinary excretion data obtained with
a single dose study are:

Chapter 2 Literature Review
Pharmaceutical Medicine 17 Jamia Hamdard
1. (dxu/dt)max: The maximum urinary excretion rate, is obtained from the peak of
plot between rate of excretion versus midpoint time of urine collection
period. It is analogous to Cmax derived from plasma level studies since the rate
of appearance of drug in the urine is proportional to its concentration in the
systemic circulation.
2. (tu)max: The time for maximum excretion rate, is analogous to the tmax of plasma
level data. Its value decreases as the absorption rate increases.
3. Xu: The cumulative amount of drug excreted in the urine, is related to the
AUC of plasma level data and increases as the extent of absorption
increases.
The extent of bioavailability can be calculated using equation given below:
F = (Xu) oral Div / (Xu) iv Doral
2.3.2.2 Pharmacodynamic Methods
These methods are complimentary to pharmacokinetic approaches and involve direct
measurement of drug effect on a physiologic process, as a function of time.
The two pharmacodynamic methods involve determination of bioavailability from:
(a) Acute pharmacologic response
(b) Therapeutic response
Acute pharmacologic response
In some cases quantitative measurement of a drug is difficult, inaccurate or non
reproducible. In such cases an acute pharmacologic effect such as effect on pupil
diameter, heart rate or blood pressure can be a useful index of drug bioavailability.
Bioavailability can be determined by construction of pharmacologic effect-time curve as
well as dose-response graphs. The method requires measurement of responses for at
least 3 biological half-lives of drug in order to obtain a good estimate of AUC.
Therapeutic response
Theoretically the most definite, this method is based on observing the clinical response
to a drug formulation given to patients suffering from disease for which it is intended to
be used. Bioequivalent drug products should have the same systemic drug
bioavailability and therefore the same predictable drug response.

Chapter 2 Literature Review
Pharmaceutical Medicine 18 Jamia Hamdard
However, variable clinical responses among individuals that are unrelated to
bioavailability might be due to differences in the pharmacodynamics of the drug.
Various factors affecting pharmacodynamic drug behaviour may include age, sex, drug
tolerance, drug interactions and unknown pathophysiologic factors.
2.3.2.3 In vitro methods
Under certain circumstances, product quality BA and BE can be documented using in
vitro approaches. For highly soluble, highly permeable, rapidly dissolving, orally
administered drug products, documentation of BE using an in vitro approach
(dissolution studies) is appropriate based on the biopharmaceutics classification system
(BCS) [CDER, 2000]. The preferred dissolution apparatus is USP apparatus I (basket)
or II (paddle), used at compendially recognized rotation speeds (e.g., 100 rpm for the
basket and 50-75 rpm for the paddle). In other cases, the dissolution properties of
some ER formulations may be determined with USP apparatus III (reciprocating
cylinder) or IV (flow through cell).
2.3.3 Factors affecting bioavailability
Bioavailability of any product varies with many factors, which are conveniently divided
into drug factors and host factors (Brahmankar and Jaiswal 1999). The drug factors
include physicochemical properties of drug substance and dosage form characteristics.
The host factors include age, blood flow to gastrointestinal tract (GIT), presence of
food or other contents in GIT, GIT pH, gastric emptying, disease state and pre-
systemic metabolism by enzymes in the gut wall or in the liver. The various factors
affecting bioavailability of drugs can be classified as shown in Table 2.2.
2.3.3.1 Physicochemical properties of drug
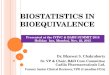
Drug solubility and dissolution rate
Dissolution is the rate-determining step (RDS) for hydrophobic, poorly aqueous soluble
drugs like griseofulvin and spironolactone; absorption of such drugs is said to be
dissolution rate-limited. If the drug is hydrophilic with high aqueous solubility e.g.
cromolyn sodium or neomycin, then dissolution is rapid and the RDS in the absorption
of such drugs is rate of permeation through the bio-membrane. Adsorption of such
drugs is said to be permeation rate limited or transmembrane rate limited. Fig. 2.1
shows a schematic representation of this concept.

Chapter 2 Literature Review
Pharmaceutical Medicine 19 Jamia Hamdard
Fig. 2.1: Schematic presentation of absorption processes of oral dosage forms
Particle size and effective surface area
Particle size and surface area of a solid drug are inversely related to each other. Particle
size is of importance for drugs of low solubility. The critical point is solubility of less
than 0.3 percent. With decreasing particle size, the surface area increases, thus
increasing the area of solid matter being exposed to the dissolution media and, hence,
dissolution rate increases. However, the actual solubility does not significantly change
with particle size reduction (micronization) in the range used in pharmaceutical
manufacture. The following eqn. describes the dissolution rate:
dc/dt = k. a. (Cs-Ct)
dc/dt = dissolution rate (amount per unit time) (Noyes Whitney equation)
k = constant depending on intensity of agitation, temperature, structure of solid surface,
and diffusion coefficient
a = surface area of undissolved solute
Cs = solubility of drug in solvent
Ct = concentration of dissolved drug at time t
Examples of drugs for which therapeutic differences have been found depending on
particle size are: amphotericin, aspirin, bishydroxycoumarin, chloramphenicol, digoxin,
acetonide, griseofulvin, meprobamate, nitrofurantoin, phenobarbital, phenothiazine,
prednisolone, procaine penicillin, reserpine, spironolactone, sulfadiazine and
tolbutamide (Ritschel and Kearns, 1998).
SolidDosageForm
SolidDrug
Particles
Disintegration
Deaggregation
Dissolution
RDS for Lipophilic drugs
Drug inSolution atabsorption
Site
Permeation acrossbiomemebrane
RDS for Hydrophobic drugs
Drug inthe
body

Chapter 2 Literature Review
Pharmaceutical Medicine 20 Jamia Hamdard
Polymorphism and amorphism
Polymorphism is the phenomenon that a drug may exist in different crystalline forms,
polymorphs. The most stable form has highest stability but lowest dissolution rate. The
least stable form usually has the most rapid dissolution rate. The unstable (metastable)
forms convert more or less slowly into the more stable form. e.g. chloramphenicol
palmitate appears in three different polymorphs, but only polymorph B is biologically
active, since the other forms do not dissolve and are not hydrolysed. The polymorphs
differ from each other with respect to their physical properties such as solubility,
melting point, density, hardness and compression characteristics. Some drugs can exist
in amorphous form (i.e. having no internal crystal structure). In general, the amorphous
state is more soluble and has a higher dissolution rate than the crystalline form. The
crystalline form requires a higher amount of energy to free a molecule of drug from it
than does the amorphous form. e.g. amorphous novobiocin and amorphous
chloramphenicol esters are biologically active while their crystalline forms are inactive.
Salt form of a drug
Most drugs are either weak acids or weak bases. One of the easiest approaches to
enhance the solubility and dissolution rate of such drugs is to convert them into
their salt forms. At a given pH, the solubility of a drug, whether acidic/basic or its
salt form, is a constant.
Drug pKa and lipophilicity and GI pH
The pH Partition theory explains in simple terms, the process of drug absorption from
the GIT and its distribution across all biologic membranes. The theory states that for a
drug compound of molecular weight greater than 100, which are primarily transported
across the biomemebrane by passive diffusion, the process of absorption is governed
by:
1. The dissociation constant (pKa) of the drug.
2. The lipid solubility of the unionized drug (a function of drug Ko/w).
3. The pH at the absorption site.
Lipophilicity and drug absorption
The pKa of a drug determines the degree of ionization at a particular pH and that only

Chapter 2 Literature Review
Pharmaceutical Medicine 21 Jamia Hamdard
the unionized drug, if sufficiently lipid soluble, is absorbed into the systemic circulation.
Thus, even if the drug exists in the unionized form, it will be poorly absorbed if it has
poor lipid solubility. Ideally, for optimum absorption, a drug should have sufficient
aqueous solubility to dissolve in the fluids at the absorption site and lipid solubility (Ko/w)
high enough to facilitate the partitioning of the drug in the lipoidal membrane and into
the systemic circulation. Hence, a perfect hydrophilic-lipophilic balance (HLB) should
be there in the structure of the drug for optimum bioavailability.
2.3.3.2 Patient related factors
Age
In infants, the gastric pH is high and intestinal surface and blood flow to the GIT is low
resulting in related absorption pattern in comparison to adults. In elderly persons,
causes of impaired drug absorption include altered gastric emptying, decreased
intestinal surface area and GI blood flow.
Gastric emptying
Apart from dissolution of a drug and its permeation through the biomembrane, the
passage from stomach to the small intestine, called as gastric emptying can also be rate
limiting step in drug absorption because the major site of drug absorption is intestine.
Thus generally speaking, rapid gastric emptying increases bioavailability of a drug.
Rapid gastric emptying is desired where:
A rapid onset of action is desired e.g. sedatives
Dissolution of drug occurs in the intestine e.g. enteric coated dosage forms
The drugs are not stable in the gastric fluids e.g. penicillin G, and erythromycin
The drugs is best absorbed from the distal part of the small intestine e.g. vitamin
B12
Intestinal Transit
Since small intestine is the major site for absorption of most drugs, long intestinal transit
time is desirable for complete drug absorption. The residence time depends upon the
intestinal motility or contractions. The mixing movement of the intestine that occurs
due to peristaltic contractions promotes drug absorption, firstly, by increasing the drug-
intestinal membrane contact, and secondly, by enhancing the drug dissolution especially
of poorly soluble drugs, through induced agitation.

Chapter 2 Literature Review
Pharmaceutical Medicine 22 Jamia Hamdard
Blood flow to the GIT
GIT is extensively supplied by blood capillary network and the lymphatic system. The
absorbed drug can thus be taken by the blood or the lymph. Since the blood flow rate
to the GIT (splanchnic circulation) is 500 to 1000 times (28% of cardiac output) more
than the lymph flow, most drugs reach the systemic circulation via blood whereas only a
few drugs, especially low molecular weight, and lipid soluble compounds are removed
by lymphatic system. The high perfusion rate of GIT ensures that once the drug has
crossed the membrane, it is rapidly removed from the absorption site thus maintaining
the sink conditions and concentration gradient for continued drug absorption.
Table 2.2: Factors affecting absorption of a drug from its dosage form [Brahmankar and
Jaiswal 1999]
PHARMACEUTICAL FACTORS PATIENT RELATED
Physicochemical properties ofdrug substances
Dosage form relatedfactors
Drug solubility and dissolutionrate
Disintegration time Age
Particle size and
effective surface areaDissolution time Gastric emptying time
Polymorphism and amorphism Manufacturing variables Intestinal transit time
Hydrates / solvates Pharmaceuticalingredients
GIT pH
Salt form of the drug Nature and type ofdosage form
Disease states
Lipophilicity of the drug Product age and storageconditions
Blood flow through GIT
pKa of the drug and p
Gastrointestinal contents:
Other drugs, Other normal GIcontents, Food, Fluids
Drug stability
Pre-systemic metabolism
by: Luminal enzymes, Gut wallenzymes, Bacterial enzymes,
Hepatic enzymes

Chapter 2 Literature Review
Pharmaceutical Medicine 23 Jamia Hamdard
2.4 BIOEQUIVALENCE
Bioequivalence (BE) is a relative term. It is defined as the absence of significant
difference in the rate and extent to which the active ingredient or active moiety in
pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site
of drug action when administered at the same molar dose and under similar conditions
in an appropriately designed study (CDER, 2003). In bioequivalence studies, the
primary question is to compare measures of release of drug substance between the test
and reference product. Hence bioequivalence is primarily a product quality question.
As product’s bioavailability and bioequivalence are closely related, similar approaches
for establishing BA and BE may be followed.
2.4.1 Historical perspective of bioequivalence
The fundamental mission of the Drug Regulatory Agencies is protection of the
consumers. The Drug Regulations require the regulatory agencies to assess safety,
efficacy and quality of all new drug formulations, before they are marketed.
Bioequivalence studies are performed to demonstrate that two pharmaceutically
equivalent products are equal in rate and extent of absorption in vivo. Following on
from developments in the pharmaceutical industry and government mandates in the
1970's and 1980's and since the early 1990's, average bioequivalence has served as the
international standard for demonstrating that two formulations of drug product will
provide the same therapeutic benefit and safety profile when used in the marketplace.
Population (PBE) and Individual (IBE) bioequivalence has been the subject of intense
international debate since methods for their assessment were proposed in the late
1980's. Guidance has been proposed by the Food and Drug Administration of the
United States government for the implementation of these techniques in the pioneer
and generic pharmaceutical industries. Implementation of these techniques may follow
a data collection period to evaluate the operating characteristics, efficiency, and metrics
involved in PBE and IBE assessment. The historical milestones of drug law are
summarized in Table 2.3.

Chapter 2 Literature Review
Pharmaceutical Medicine 24 Jamia Hamdard
Table 2.3: Chronology of regulatory events [Modified from Truman HS, 1992]
Year Event
1902 Biologics Control Act
1906 Pure Food and Drugs Act / Wiley Act
1912 Shirley Amendment to Pure Food and Drugs Act- No false claim
1936 Elixir Sulfanilamide Disaster
1938 Food Drug & Cosmetics Act: FDA control over safety of new drugs
1951 Durham-Humphrey Amendments to FD & C Act: Prescription drugs
1961 Thalidomide disaster in Europe
1962 Kefauver-Harris amendment-FDA Control over both safety and efficacy of drugs-
1963 Initial Good Manufacturing Practices (GMP) regulations
1974 World Health organization, recommendations for conduct of bioavailability studies
1974 Dissolution test adopted as standard for in vitro comparison of bioavailability in UK
1977 US FDA regulations for approval of BE. The + 20% rule with p<0.05
1983 Orphan drug act
1984 ANDA for generics approval-Waxman-Hatch act (Drug price competition and patentterm restoration act)
1985 New 80-125% for CI law for approval of generic products
1987 Standard 2x2 crossover test design for BE studies
1989 Generics scandal in USA. Concern for adequate documentation and validation of BEstudies
1992 90-111% CI for narrow therapeutic index drugs: Canadian FDA
1995 EEC-70-143% limit for Cmax only for drug with wide safety margin
1999 Draft regulations for BE studies: In India
2005 Regulations for BE studies: In India
2.4.2 Need for bioequivalence study
2.4.2.1 Bioequivalence for first entry products
BE studies may be useful during drug development and registration for a first entry
product during the Investigational New Drug (IND) or New Drug Application (NDA)
period to establish links between (i) early and late clinical trial formulations (ii)
formulations used in clinical trial and stability studies, if different (iii) Clinical trial
formulations and to be marketed drug products (iv) other comparisons as appropriate.
In each comparison, the new formulation or new method of manufacture is the test
product and the prior formulation or method of manufacture is the reference product.

Chapter 2 Literature Review
Pharmaceutical Medicine 25 Jamia Hamdard
2.4.2.2 Bioequivalence for interchangeable multi-source products
BE studies are a critical component of Abbreviated New Drug Applications (ANDA).
The purpose of these studies is to compare relative BA measures between a
pharmaceutically equivalent multi-source test product and the corresponding reference
pioneer product. The innovator product is termed as reference listed drug (RLD).
Together with the determination of pharmaceutical equivalence, demonstrating BE
allows a regulatory conclusion of therapeutic equivalence and interchangeability
between the test and reference product [The Orange book, CDER, 2007].
2.4.2.3 Bioequivalence for post approval changes
Generally specifications are adequate to assure product quality on the assumption that
no important change occurs post-approval. In the presence of major changes in
components and composition, and/or method of manufacture of a dug product after
approval, BE may need to be re-demonstrated. For approved first-entry products, the
drug product after the change should be compared to the drug product before change.
For approved interchangeable multi-source products, the drug product after the change
should be compared to the reference listed drug.
2.4.3 Average bioequivalence versus Therapeutic equivalence
Clinical studies comparing pioneer and generic drugs are rarely performed, and studies
comparing one generic product with another are almost never performed. However, in
the 1970s it was recognized that differences in the formulation of products containing
the same amount of active ingredient could result in significant differences in
bioavailability and several cases of therapeutic inequivalence involving generic products
were reported (Kluznik et al. 2001, Weidekamm et al. 1998, Joshi et al. 1990).
Similarly, several more recent reports involving clinical differences or serious
bioequivalence problems with generic products have involved “B”-rated products.
(Campagna 1963, Lander 1971, Alvarez et al. 1981, Lund, 1974, Meyer et al. 1982,
Dubovsky, 1987, Baker et al. 1988; Ansbacher, 2001). However, numerous case
reports have also noted problems temporally related to generic switches for a number
of “A”-rated products. (MacDonald et al. 1987, Wyllie et al. 1987, Hope and Havrda
et al. 2001, Meyer et al. 1992, Welty et al, 1992, Gilman et al. 1993, Reiffel and Kowey
et al. 2000, Wagner and Dent et al. 2000, Rosenbaum et al. 2001, Sajbel et al. 2001,
Kluznik et al. 2001).

Chapter 2 Literature Review
Pharmaceutical Medicine 26 Jamia Hamdard
In response to such reports of possible therapeutic inequivalence, the FDA established
the Therapeutic Inequivalence Action Coordinating Committee (TIACC) housed
within the FDA Center for Drug Evaluation and Research to identify, evaluate, and
when appropriate, investigate reports of apparent therapeutic inequivalence and take
appropriate corrective action. Since the formation of the TIACC in 1988, the FDA has
investigated more than 60 reports of potential generic product inequivalence but could
not find a single example of therapeutic failure when an FDA-designated therapeutically
equivalent generic product, which was manufactured to meet its approved
specifications, was substituted for the corresponding brand-name drug listed in the
FDA’s Approved Drug Products with Therapeutic Equivalence Evaluations. Moreover
other independent studies have confirmed the bioequivalence and/or therapeutic
equivalence of many other “A”-rated generic products (Francisco et al. 1984, Midha et
al. 1984, Zaman et al. 1986, Eldon et al. 1989, Sharoky et al. 1989, Midha et al. 1990,
Hartley et al. 1991, Meyer et al. 1998).
The perception persists that the current bioequivalence approach for approving generic
products does not adequately account for intra-individual variation in drug
disposition. Pharmacokinetic bioequivalence studies are a surrogate for clinical
outcomes. The critical question is whether assessment of bioequivalence (average)
assures therapeutic equivalence. Concerns have been raised about use of the average
bioequivalence approach to assure interchangeability for multisource products. It has
been suggested that this approach may not be adequate for all drugs and that modified
procedures and additional data may be necessary (Schall and Luus 1993).
Average bioequivalence approach has been indicated to be insufficient to warrant
bioequivalence of the test formulation and the reference formulation, since it compares
the average bioavailability values of the test and the reference formulations and does not
consider differences in variance of test and reference formulation (Nakai et al. 2002).
Measures of average bioequivalence lack any measure of intrasubject variability, and no
such information is provided to physicians in the package inserts. Due to these
concerns raised over the years, on the use of average bioequivalence for evaluation of
comparability between formulations, scientists from academia, industry and regulatory
agencies, propose the use of concepts of individual and population bioequivalence
(Chen et al.2000).

Chapter 2 Literature Review
Pharmaceutical Medicine 27 Jamia Hamdard
An individual bioequivalence approach has been advocated as a more appropriate
measure to ensure interchangeability (William et al. 2000). Because of the within-
subject focus, individual bioequivalence assessments are usually based on a replicate
study design in which each subject receives both the test and reference products on at
least two occasions. This approach requires a criterion and statistical analysis of within-
individual variance for both test and reference products, and also estimates if two
pharmaceutically equivalent products exhibit a subject-by-formulation interaction.
Presence of a subject-by-formulation interaction means that the difference between
formulations is not the same from subject to subject. The FDA also has proposed
replacing the 1992 average bioequivalence approach with population and individual
bioequivalence (PBE and IBE) (CDER, 1997).
2.4.4 Individual bioequivalence
The IBE criterion encourages BE studies in subjects more representative of the general
population or even in patients for whom the drug is intended, as opposed to healthy
young males where detection of S*F interaction is less likely. This feature addresses a
frequently expressed concern that BE studies in healthy young males lack clinical
relevance. A key concept underlying IBE criterion relates to the term switchability,
which denotes the situation where a patient currently on one formulation switches to
another with the expectation that the safety and efficacy of the drug will remain
essentially unchanged. The criterion uses, in the aggregate, a distance concept that
compares means and variances of T and R products. For individual BE, a subject-by-
formulation (S*F) interaction variance, and within-subject variance for both T and R
products are estimated. By expanding the variance terms, the proposed criterion offers
many consumer and producer advantages, including: (i) assurance of switchability; (ii)
rewards for reduction of variance in the T product; (iii) scaling for highly variable
and/or narrow therapeutic range drugs.
In the IBE criterion, replicate designs are required, in which at least the R, and
commonly both R and T drug products, are each administered on two separate
occasions. The re-test characteristics of replicate study design allow scrutiny of outliers.
IBE can be calculated as:
2D = [(2
BT - 2BR)2 + 2(1-) BT BR

Chapter 2 Literature Review
Pharmaceutical Medicine 28 Jamia Hamdard
1= [(T - R)2 + 2D + 2
WT - 2WR ]/ 2
WR when WR > 0.2
1= [(T - R)2 + 2D + 2
WT - 2WR ]/ 0.22 when WR < 0.2
Where,
T = mean (test)
R = mean (reference)
2WT = within subject variance (test)
2WR = within subject variance (reference)
2BT = between subject variance (test)
2BR = between subject variance (reference)
Again, 2WR is set to 0.20 (that is, constant scaled versus reference standard) in the
denominator of the formula 1 when the point estimate of the parameter based on the
original data set falls below 0.20 (CDER, 1997).
Individual BE is demonstrated when; 1 (0.95) < 2.45, where p (0.95) is defined as the
95th quartile of 1 based on the non-parametric percentile method using 2000 bootstrap
samples. The bootstrap is used, as the exact distribution for the parameter p has not yet
been derived.
2.4.5 Population bioequivalence
Population bioequivalence approach, which evaluates the total bioavailability variances
in addition to the average bioavailability values, has been proposed as a method to
overcome the disadvantages of average bioequivalence approach (Hauschke and
Steinijans, 2000). FDA has also proposed the use of population bioequivalence as a
bioequivalence study which might guarantee prescribability and which is applicable in
the development stages of novel drugs (CDER, 1997). Based on earlier published
reports of bioequivalence in literature, it was concluded that population bioequivalence
value was affected more extensively by the bioavailability variance rather than by the

Chapter 2 Literature Review
Pharmaceutical Medicine 29 Jamia Hamdard
average bioavailability (Nakai et al, 2002). PBE criteria aggregate the difference between
the population means and variances.
The key motivation behind the proposed changes in BE criteria lie in answering more
appropriate questions regarding bioequivalence. In the case of pre-marketing approval,
one can formulate the bioequivalence question as “Can a patient begin their therapy
with either formulation (commercial or clinical trial) and be assured of same results in
terms of safety and efficacy” This has been called the concept of prescribability (CDER,
1997) and is linked to PBE criteria. In case of post-marketing changes, the BE question
becomes “Can I safely and effectively switch my patient from their current formulation
to another” This has been called the concept on switchability and is linked to the IBE
criteria. PBE can be calculated as:
p= [(T - R)2 + 2TT - 2
TR]/ 2TR when TR > 0.2
p= [(T - R)2 + 2TT - 2
TR]/ 0.22 when TR < 0.2
Where, T = mean (test)
R = mean (reference)
2TT = total variance (test)
2TR = total variance (reference)
p is calculated in one of the two ways depending on the point estimate for 2TR based on
the original data set. When this estimate falls below 0.20, a constant scaling procedure
is used. Otherwise, the scaling is proportional to 2TR. This has been referred to as
‘constant scaled’ and ‘reference scaled’ respectively (CDER, 1997). Population BE is
demonstrated when; p (0.95) < 1.75, where p (0.95) is defined as the 95th quantile of p
based on the non-parametric percentile method using 2000 bootstrap samples. The
bootstrap is used, as the exact distribution for the parameter p has not yet been derived.
2.4.6 Design and evaluation of bioequivalence study
The preferred approach is an in vivo study carried out in healthy volunteers to whom
the 2 preparations (generic and innovator) are alternatively administered.

Chapter 2 Literature Review
Pharmaceutical Medicine 30 Jamia Hamdard
The design and evaluation of well controlled bioequivalence studies require the
cooperative input from pharmacokineticists, statisticians, clinicians, bio-analytical
chemists, and others. The design of a bioavailability and/or bioequivalence study is
dependent upon the drug, dosage form and study objectives. For BE studies, both the
test and reference drug formulations contain the pharmaceutical equivalent drug in the
same dose and are given by the same route of administration.
A pilot study in small number of subjects can be carried out before proceeding with a
full BE study. This study can be used to validate analytical methodology, assess
variability, optimize sample collection time intervals or provide any other information.
Non replicate crossover study designs are recommended by FDA for immediate release
and modified release dosage forms (CDER, 2003). However replicate designs can also
be used. The recommended method for analysis to establish bioequivalence is average
bioequivalence. The study should be of crossover designs and suitably randomized as
far as possible. Some of the designs are discussed below-
2.4.6.1 Two-Period Crossover Design
In case of two formulations, an even number of subjects should be randomly divided
into two equal groups. In the first period, each member of one group will receive a
single dose of the test formulation and each member of the other group will receive
standard formulation. After a suitable washout period (generally 5 half lives), in the
second period, each member of the respective groups will receive a dose of an
alternative formulation and the experiment will be repeated.
The design can be depicted as follows:
Volunteer No. Period 1 Period 2
1 A B
2 B A
3 A B
4 A B
5 B A
6 B A

Chapter 2 Literature Review
Pharmaceutical Medicine 31 Jamia Hamdard
2.4.6.2 Latin Square Design
In case of more than two formulations, a Latin square design should be used. For
example in a bioequivalence study of 3 formulations, a group of volunteers will receive
formulations in the sequence shown below:
VolunteerNo.
Period 1 Period 2 Period 3
1 A B C
2 B C A3 C A B
The next group of 3 volunteers will receive formulations in the same sequence as
shown above.
2.4.6.3 Balance Incomplete Block Design (BIBD)
In case there are more than 3 formulations, the Latin square design will not be ethically
advisable, mainly because each volunteer may require the drawing of too many blood
samples. However, if each volunteer is expected to receive at least two formulations,
then such a study can be carried out using Balanced Incomplete Block Design. As per
this design, if there are four formulations, six possible pairs or formulations can be
chosen from four formulations. Then, the first 6 volunteers will receive these six pairs
of formulations and the next six volunteers will receive the same six pairs in reverse
order. The design is depicted below:
Volunteer No. Period 1 Period 2
1 A B
2 A C
3 A D
4 B C
5 B D
6 C D
7 B A
8 C A
9 D A
10 C B
11 D B
12 D C

Chapter 2 Literature Review
Pharmaceutical Medicine 32 Jamia Hamdard
The minimum acceptable number of volunteers will be 12.
n> {[]2}/2D2 [t+t]2 + 0.25 t2
Where,
n = no. of volunteers
= Required level of significance (0.05)
= Required power of test (0.80)
2 = Error mean sum of squares from ANOVA (estimated/guess)
D = Minimum difference between the means which if present, ought to be detected
The bioequivalence studies are conducted according to a well-defined protocol.
Some elements of a bio-equivalence protocol are listed in Table 2.5:
2.4.7 STATISTICAL ISSUES IN BIOEQUIVALENCE STUDIES
2.4.7.1 Log transformation before ANOVA
The primary comparison of interest in a bioequivalence study is the ratio of average
parameter data (AUC & Cmax) from the test and reference formulations rather than the
difference between them. Log transformation of the data allows the general linear
statistical model to draw inferences about the ratio of the two averages on the original
scale. Log transformation thus achieves the general comparison based on the ratio
rather than on the difference. Moreover, plasma concentration data, including AUC
and Cmax tend to be skewed and their variances tend to increase with the means. Log
transformation corrects this situation and makes the variances independent of the
mean. Further, the frequency distribution skewed to the left, i.e., those with a log tail to
the right is made symmetrical by log transformation. In case no suitable transformation
is available, the non-parametric method should be used. Tmax values being discrete, data
on Tmax should be analysed using non-parametric methods.
The pharmacokinetic parameters, Cmax, Tmax and AUC should be subjected to a three-
way analysis of variance (3-way ANOVA) in order to test differences due to
formulations, period and subjects.

Chapter 2 Literature Review
Pharmaceutical Medicine 33 Jamia Hamdard
A more complex ANOVA may be appropriate in some circumstances, e.g. if
treatments are replicated. The standard parametric ANOVA assumes homogeneity of
variances, normality and additivity of independent variables. In order to ensure
homogeneity of variances between treatments, Barttlet’s test or a similar test should be
carried out prior to performing the ANOVA.
2.4.7.2 Two one-sided tests procedures (TOST)
This procedure is also referred to as confidence interval approach. This method is used
to demonstrate if the bioavailability of the drug from the test formulation is too high or
low in comparison to the reference drug product. The 90% confidence limits are
estimated for the sample means. In this test, presently required by the FDA, a 90%
confidence interval about the ratio of means of the two drug products must be within
±20% for measurement of the rate and extent of drug bioavailability. The lower 90% CI
for the ratio of means cannot be less than 0.8, and the upper 90% CI for the ratio of the
means cannot be greater than 1.20. The 90% CI is a function of sample size and study
variability, including inter and intra subject variability (CDER, 2003).
Current DCGI requirements for bio-equivalence approval is that 90% confidence
interval should be within 80-125% for log transformed AUC and 70-143% for log
transformed Cmax provided that the drug is safe otherwise 80-125% will be applicable.
For narrow therapeutic index drugs, the log transformed Cmax should be within 90-111%
and for log transformed AUCs 80-125% is applicable. The T/R ratio should be as close
as possible to 95-105%. Intra subject CV should be as low as possible (<15%). The
bioequivalence criteria followed by various regulatory agencies in the world are
mentioned in the Table 2.4.

Chapter 2 Literature Review
Pharmaceutical Medicine 34 Jamia Hamdard
Table 2 4: Criteria of bio-equivalence of various regulatory agencies
AgencyLog transformed Parameter
Cmax using 90% CI AUC0-t using 90% CI
USFDA 80-125% of reference 80-125% of reference
DCGI80-125% of reference
70-143% of reference for WTIa
80-125% of reference
90-111% of reference for NTI b
drugs.
CPMP (EU)
80-125% of reference NTI drugs)
75-133% of reference (if clinicallyacceptable)
80-125% of reference
90-111% of reference for NTI b
drugs.
CANADIANFDA (CEC)
80-125% of reference
70-143% of reference for WTIa
drugs.
80-125% of reference
90-111% of reference for NTI b
drugs.
WTIa –Wide Therapeutic Index
NTI b - Narrow Therapeutic Index
DCGI: Drug Control General of India.
USFDA: United State Food and Drug Administration.
CPMP (EU): The Committee for Proprietary Medicinal Products, European Union.
CEC: Canadian Education Centre.

Chapter 2 Literature Review
Pharmaceutical Medicine 35 Jamia Hamdard
Table 2.5: Elements of the bioavailability Protocol
S. No. CONTENTS
1 INVESTIGATORS' DECLARATION
2 FACILITIES
2.1 Clinical Services & Clinical Laboratory
2.2. Analytical, Pharmacokinetics & Statistical Services
3 OBJECTIVE
4 PRODUCTS TO BE EVALUATED
4.1 REFERENCE (R)
4.2 TEST (A)
4.3 TEST (B)
5 INTRODUCTION
6 PHARMACOLOGY
6.1 Absorption, Distribution, Metabolism and Excretion
6.2 Adverse Effects
6.3 Dosage
7 STUDY DESIGN
7.1 Summary
7.2 Number of Subjects
7.3 Admissions and Stay
7.4 Fasting/Meals
7.5 Sampling Schedule
7.7 Washout Period
8 RESTRICTIONS
8.1 Medications
8.2 Diet

Chapter 2 Literature Review
Pharmaceutical Medicine 36 Jamia Hamdard
8.3 Activity
9 SELECTION OF SUBJECTS
9.1 Inclusion Criteria
9.2 Exclusion Criteria
10 SCHEDULE OF ASSESSMENTS
11 STUDY MEDICATION
11.1 Handling, Storage and Accountability Procedures
11.2 Dose
11.3 Assignment to Treatment Sequences
11.4 Assessment of Compliance
12 HAEMODYNAMIC MEASUREMENTS
13 PHARMACOKINETICS
13.1 Blood Sampling
13.2 Analytical Procedures
13.3 Pharmacokinetic Parameters
14 SAFETY
14.1 Clinical Safety Measurements
15 HANDLING OF SAFETY PARAMETERS
15.1 Adverse Events
16 STATISTICAL ANALYSIS
17 DEVIATIONS
18 ETHICAL CONSIDERATION
18.1 Basic Principles
18.2 Institutional Review Board
18.3 Informed Consent
18.4 Withdrawal/Drop-out of Subjects from Study
18.5 Volunteer Compensation

Chapter 2 Literature Review
Pharmaceutical Medicine 37 Jamia Hamdard
19 TERMINATION OF THE STUDY
20 STUDY DOCUMENTATION
21 QUALITY ASSURANCE AUDIT
22 CONFIDENTIALITY OF DATA
23 ARCHIVES
24 PUBLICATION POLICY
25 REFERENCES
26 LIST OF APPENDICES

Chapter 2 Literature Review
Pharmaceutical Medicine 38 Jamia Hamdard
2.5 DRUG PROFILE
2.5.1 CHEMISTRY
Olmesartan medoxomil, a prodrug, is hydrolyzed to olmesartan during absorption from
the gastrointestinal tract. Olmesartan is a selective AT1 subtype angiotensin II receptor
antagonist.
Olmesartan medoxomil is described chemically as 2,3-dihydroxy 2- butenyl 4-(1-
hydroxy-1-methylethyl)- 2 - propyl- 1- [p-(o-1H-tetrazol-5-ylphenyl)benzyl] - imidazole 5-
carboxylate, cyclic 2,3-carbonate.
Its empirical formula is C29H30N6O6 and its structural formula is:
2.5.2 DESCRIPTION
Olmesartan medoxomil is a white to light yellowish-white powder or crystalline powder
with a molecular weight of 558.59. It is practically insoluble in water and sparingly
soluble in methanol. It is available for oral use as film-coated tablets containing 10 mg,
20 mg, or 40 mg olmesartan medoxomil.

Chapter 2 Literature Review
Pharmaceutical Medicine 39 Jamia Hamdard
2.5.3 PHARMACOLOGY
2.5.3.1 Pharmacodynamics
Angiotensin II is formed from angiotensin I in a reaction catalyzed by angiotensin
converting enzyme (ACE, kininase II). Angiotensin II is the principal pressor agent of
the reninangiotensin system, with effects that include vasoconstriction, stimulation of
synthesis and release of aldosterone, cardiac stimulation and renal reabsorption of
sodium. Olmesartan medoxomil is an orally active angiotensin II receptor (type AT1)
antagonist. It has more than a 12,500-fold greater affinity for the AT1 receptor than for
the AT2 receptor. It is expected to block all actions of angiotensin II mediated by the
AT1 receptor, regardless of the source or route of synthesis of angiotensin II. The
selective antagonism of the angiotensin II (AT1) receptors results in increases in plasma
renin levels and angiotensin I and II concentrations, and some decrease in plasma
aldosterone concentrations.
Angiotensin II plays a significant role in the pathophysiology of hypertension via the
type 1 (AT1) receptor.
In hypertension, olmesartan medoxomil causes a dose-dependent, long-lasting
reduction in arterial blood pressure. There has been no evidence of first-dose
hypotension, of tachyphylaxis during long-term treatment, or of rebound hypertension
after cessation of therapy.
Once daily dosing with olmesartan medoxomil provides an effective and smooth
reduction in blood pressure over the 24-hour dose interval. Once daily dosing
produced similar decreases in blood pressure as twice daily dosing at the same total
daily dose.
With continuous treatment, maximum reductions in blood pressure are achieved by 8
weeks after the initiation of therapy, although a substantial proportion of the blood
pressure lowering effect is already observed after 2 weeks of treatment. When used
together with hydrochlorothiazide, the reduction in blood pressure is additive and co
administration is well tolerated.
The effect of olmesartan on mortality and morbidity is not yet known.

Chapter 2 Literature Review
Pharmaceutical Medicine 40 Jamia Hamdard
2.5.3.2 Pharmacokinetics
Absorption and distribution
Olmesartan medoxomil is a prodrug. It is rapidly converted to the pharmacologically
active metabolite, olmesartan, by esterases in the gut mucosa and in portal blood during
absorption from the gastrointestinal tract.
No intact olmesartan medoxomil or intact side chain medoxomil moiety have been
detected in plasma or excreta. The mean absolute bioavailability of olmesartan from a
tablet formulation was 25.6%.
The mean peak plasma concentration (Cmax) of olmesartan is reached within about 2
hours after oral dosing with olmesartan medoxomil, and olmesartan plasma
concentrations increase approximately linearly with increasing single oral doses up to
about 80 mg.
Food had minimal effect on the bioavailability of olmesartan and therefore olmesartan
medoxomil may be administered with or without food.
No clinically relevant gender–related differences in the pharmacokinetics of olmesartan
have been observed.
Olmesartan is highly bound to plasma protein (99.7%), but the potential for clinically
significant protein binding displacement interactions between olmesartan and other
highly bound co-administered drugs is low (as confirmed by the lack of a clinically
significant interaction between olmesartan medoxomil and warfarin). The binding of
olmesartan to blood cells is negligible. The mean volume of distribution after
intravenous dosing is low (16 – 29 L).
Kun-Yan Li et.al conduct a study in 2010 investigated the relative bioavailability and
fasting pharmacokinetic properties of olmesartan after single doses of a 20-mg test
tablet, a 20-mg test capsule, and a commercially available 20-mg reference tablet in
healthy Chinese male volunteers. The study was conducted to satisfy Chinese State
Food and Drug Administration regulatory requirements for approval of a generic
formulation of olmesartan medoxomil. Blood samples were obtained at baseline and at
0.5, 1, 1.5, 2, 2.5,3,4,6,8,12,24,36, and 48 hours after dosing. The value of Cmax found
for tests and reference formulation were 495.0, 396.0, and 530.0 (ng/ml) respectively.
The value of AUC0-t, AUC0-∞ were 3993, 3567, 3849 and 3091, 2847, 2956 ng.hr/ml

Chapter 2 Literature Review
Pharmaceutical Medicine 41 Jamia Hamdard
respectively. Results of this study conclude that formulations of olmesartan medoxomil
20-mg capsules and tablets met the regulatory criteria for assuming bioequivalence
Metabolism and elimination
Total plasma clearance was typically 1.3 L/h (CV, 19%) and was relatively slow
compared to hepatic blood flow (ca 90 L/h). Following a single oral dose of 14C
labelled olmesartan medoxomil, 10 - 16% of the administered radioactivity was excreted
in the urine (the vast majority within 24 hours of dose administration) and the
remainder of the recovered radioactivity was excreted in the faeces. Based on the
systemic availability of 25.6%, it can be calculated that absorbed olmesartan is cleared
by both renal excretion (ca 40%) and hepato-biliary excretion (ca 60%). All recovered
radioactivity was identified as olmesartan. No other significant metabolite was detected.
Enterohepatic recycling of olmesartan is minimal. Since a large proportion of
olmesartan is excreted via the biliary route, use in patients with biliary obstruction is
contraindicated.
The terminal elimination half life of olmesartan varied between 10 and 15 hours after
multiple oral dosing. Steady state was reached after the first few doses and no further
accumulation was evident after 14 days of repeated dosing. Renal clearance was
approximately 0.5 – 0.7 L/h and was independent of dose.
2.5.3.3 Pharmacokinetics in special populations
Elderly:
In hypertensive patients, the AUC at steady state was increased by ca 35% in elderly
patients (65 – 75 years old) and by ca 44% in very elderly patients ( 75 years old)
compared with the younger age group. This may be at least in part related to a mean
decrease in renal function in this group of patients.
Renal impairment:
In renally impaired patients, the AUC at steady state increased by 62%, 82% and 179%
in patients with mild, moderate and severe renal impairment, respectively, compared to
healthy controls.
Hepatic impairment:
After single oral administration, olmesartan AUC values were 6% and 65% higher in
mildly and moderately hepatically impaired patients, respectively, than in their

Chapter 2 Literature Review
Pharmaceutical Medicine 42 Jamia Hamdard
corresponding matched healthy controls. The unbound fraction of olmesartan at 2
hours post-dose in healthy subjects, in patients with mild hepatic impairment and in
patients with moderate hepatic impairment was 0.26%, 0.34% and 0.41%, respectively.
Following repeated dosing in patients with moderate hepatic impairment, olmesartan
mean AUC was again about 65% higher than in matched healthy controls. Olmesartan
mean Cmax values were similar in hepatically-impaired and healthy subjects.
Olmesartan medoxomil has not been evaluated in patients with severe hepatic
impairment.
2.5.4 Market experience
The following adverse reactions have been reported in post-marketing experience.
They are listed by System Organ Class and ranked under headings of frequency using
the following convention: very common ( 1/10); common ( 1/100, <1/10);
uncommon ( 1/1,000, <1/100); rare ( 1/10,000, <1/1,000); very rare (<1/10,000)
including isolated reports.
System Organ Class Very rare
Blood and lymphatic system disorders Thrombocytopenia
Metabolism and nutrition disorders Hyperkalaemia
Nervous system disorders Dizziness, headache
Respiratory, thoracic and mediastinal disorders Cough
Gastrointestinal disorders Abdominal pain, nausea, vomiting
Skin and subcutaneous tissue disorders Pruritus, exanthem, rash
Allergic conditions such as angioneurotic oedema,dermatitis allergic, face oedema and urticaria
Musculoskeletal and connective tissue disorders Muscle cramp, myalgia
Renal and urinary disorders Acute renal failure and renal insufficiency (Seealso under Investigations)
General disorders and administration siteconditions
Asthenic conditions such as asthenia, fatigue,lethargy, malaise
Investigations Abnormal renal function tests such as bloodcreatinine increased and blood urea increased
Increased hepatic enzymes

Chapter 2 Literature Review
Pharmaceutical Medicine 43 Jamia Hamdard
Single cases of rhabdomyolysis have been reported in temporal association with the
intake of angiotensin II receptor blockers. A causal relationship, however, has not been
established.
2.5.5 Special warnings and precautions for use
Intravascular volume depletion
Symptomatic hypotension, especially after the first dose, may occur in patients who are
volume and/or sodium depleted by vigorous diuretic therapy, dietary salt restriction,
diarrhoea or vomiting. Such conditions should be corrected before the administration
of olmesartan medoxomil.
Other conditions with stimulation of the renin-angiotensin-aldosterone system
In patients whose vascular tone and renal function depend predominantly on the
activity of the renin-angiotensin-aldosterone system (e.g. patients with severe congestive
heart failure or underlying renal disease, including renal artery stenosis), treatment with
other drugs that affect this system has been associated with acute hypotension,
azotaemia, oliguria or, rarely, acute renal failure. The possibility of similar effects
cannot be excluded with angiotensin II receptor antagonists.
Renovascular hypertension
There is an increased risk of severe hypotension and renal insufficiency when patients
with bilateral renal artery stenosis or stenosis of the artery to a single functioning kidney
are treated with medicinal products that affect the renin-angiotensin-aldosterone system.
Renal impairment and kidney transplantation
When olmesartan medoxomil is used in patients with impaired renal function, periodic
monitoring of serum potassium and creatinine levels is recommended. Use of
olmesartan medoxomil is not recommended in patients with severe renal impairment
(creatinine clearance < 20 mL/min).There is no experience of the administration of
olmesartan medoxomil in patients with a recent kidney transplant or in patients with
end-stage renal impairment (i.e. creatinine clearance <12 mL/min).
Hepatic impairment
There is no experience in patients with severe hepatic impairment and therefore use of
olmesartan medoxomil in this patient group is not recommended.

Chapter 2 Literature Review
Pharmaceutical Medicine 44 Jamia Hamdard
Hyperkalaemia
The use of medicinal products that affect the renin-angiotensin-aldosterone system may
cause hyperkalaemia.
The risk, that may be fatal, is increased in elderly, in patients with renal insufficiency
and in diabetic patients, in patients concomitantly treated with other medicinal products
that may increase potassium levels, and/or in patients with intercurrent events.
Before considering the concomitant use of medicinal products that affect the renin-
angiotensin-aldosterone system, the benefit risk ratio should be evaluated and other
alternatives considered.
The main risk factors for hyperkalaemia to be considered are:
- Diabetes, renal impairment, age (> 70 years)
- Combination with one or more other medicinal products that affect the renin-
angiotensin-aldosterone system and/or potassium supplements. Some medicinal
products or therapeutic class of medicinal products may provoke a hyperkalaemia: salt
substitutes containing potassium, potassium-sparing diuretics, ACE inhibitors,
angiotensin II receptors antagonists, non steroidal anti-inflammatory drugs (including
selective COX-2 inhibitors), heparin, immunosuppressor as ciclosporin or tacrolimus,
trimethoprim
- Intercurrent events, in particular dehydration, acute cardiac decompensation,
metabolic acidosis, worsening of renal function, sudden worsening of the renal
condition (e.g. infectious diseases), cellular lysis (e.g. acute limb ischemia,
rhabdomyolysis, extended trauma).
Close-monitoring of serum potassium in at risk patients is recommended.
Lithium
As with other angiotensin-II receptor antagonists, the combination of lithium and
olmesartan medoxomil is not recommended.
Aortic or mitral valve stenosis; obstructive hypertrophic cardiomyopathy:
As with other vasodilators, special caution is indicated in patients suffering from aortic
or mitral valve stenosis, or obstructive hypertrophic cardiomyopathy.

Chapter 2 Literature Review
Pharmaceutical Medicine 45 Jamia Hamdard
Primary aldosteronism
Patients with primary aldosteronism generally will not respond to antihypertensive drugs
acting through inhibition of the renin-angiotensin system. Therefore, the use of
olmesartan medoxomil is not recommended in such patients.
Ethnic differences
As with all other angiotensin II antagonists, the blood pressure lowering effect of
olmesartan medoxomil is somewhat less in black patients than in non-black patients,
possibly because of a higher prevalence of low-renin status in the black hypertensive
population.
Pregnancy
Angiotensin II antagonists should not be initiated during pregnancy. Unless continued
angiotensin II antagonists therapy is considered essential, patients planning pregnancy
should be changed to alternative anti-hypertensive treatments which have an established
safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with
angiotensin II antagonists should be stopped immediately and, if appropriate,
alternative therapy should be started.
Others
As with any antihypertensive agent, excessive blood pressure decrease in patients with
ischaemic heart disease or ischaemic cerebrovascular disease could result in a
myocardial infarction or stroke.
This medicinal product contains lactose. Patients with rare hereditary problems of
galactose intolerance, the Lapp-lactase deficiency or glucose-galactose malabsorption
should not take this medicinal product.
2.5.6 Contraindications
Hypersensitivity to the active substance or to any of the excipients.
Second and third trimesters of pregnancy.
Biliary obstruction.
2.5.7 Overdose
Only limited information is available regarding overdosage in humans. The most likely
effect of overdosage is hypotension. In the event of overdosage, the patient should be

Chapter 2 Literature Review
Pharmaceutical Medicine 46 Jamia Hamdard
carefully monitored and treatment should be symptomatic and supportive. (SPC:
Summary product Characteristics 2009).
2.5.8 Drug Treatment of Hypertension
Treatment with drugs should be started in patients with blood pressures >140/90 mm
Hg in whom lifestyle treatments have not been effective. Different classes of
antihypertensive drugs along their mechanism of action are shown as:
Angiotensin-converting enzyme Inhibitors
These agents reduce blood pressure by blocking the renin-angiotensin system. They do
this by preventing conversion of angiotensin I to the blood pressure raising hormone
angiotensin II. They also increase availability of the vasodilator bradykinin by block-ing
its breakdown. Angiotensin-converting enzyme inhibitors are well tolerated. Their main
side effect is cough (most common in women and in patients of Asian and African
background). Angioedema is uncommon but potentially serious complications that can
threaten airway function, and it occurs most frequently in black patients.
These drugs have established clinical outcome benefits in patients with heart failure,
post–myocardial infarction, left ventricular systolic dysfunction, and diabetic and non
diabetic chronic kidney disease.
Thiazide and Thiazide-like Diuretics
These agents work by increasing excretion of sodium by the kidneys and additionally
may have some vasodilator effects. Clinical outcome benefits (reduction of strokes and
major cardiovascular events) have been best established with chlorthalidone,
indapamide, and hydrochlorothiazide, although evidence for the first two of these
agents has been the strongest. Chlorthalidone has more powerful effects on blood
pressure than hydrochlorothiazide (when the same doses are compared) and has a
longer duration of action.
The main side effects of these drugs are metabolic (hypokalemia, hyperglycemia, and
hyperuricemia). The likelihood of these problems can be reduced by using low doses
(eg, 12.5 mg or 25 mg of hydrochlorothiazide or chlorthalidone) or by combining these
diuretics with angiotensin-converting enzyme inhibitors or angiotensin receptor
blockers, which have been shown to reduce these metabolic changes. Combining
diuretics with potassium-sparing agents

Chapter 2 Literature Review
Pharmaceutical Medicine 47 Jamia Hamdard
Note: Thiazides plus b-blockers are also an effective combination for reducing blood
pressure, but since both classes can increase blood glucose concentrations this
combination should be used with caution in patients at risk for developing diabetes.
Calcium Channel Blockers
These agents reduce blood pressure by blocking the inward fow of calcium ions
through the L channels of arterial smooth muscle cells. There are two main types of
calcium channel blockers: dihydropyridines, such as amlodipine and nifedipine, which
work by dilating arteries; and nondihydropyridines, such as diltiazem and verapamil,
which dilate arteries somewhat less but also reduce heart rate and contractility.
The main side effect of calcium channel blockers is peripheral edema, which is most
prominent at high doses; this finding can often be attenuated by combining these agents
with angiotensin-converting enzyme inhibitors or angiotensin receptor blockers.
Beta- Blockers
β-blockers reduce cardiac output and also decrease the release of renin from
the kidney.
They have strong clinical outcome benefts in patients with histories of
myocardial infarction and heart failure and are effective in the management of
angina pectoris.
They are less effective in reducing blood pressure in black patients than in
patients of other ethnicities.
β-blockers may not be as effective as the other major drug classes in preventing
stroke or cardiovascular events in hypertensive patients, but they are the drugs
of choice in patients with histories of myocardial infarction or heart failure.
Many of these agents have adverse effects on glucose metabolism and therefore
are not recommended in patients at risk for diabetes, especially in combination
with diuretics. They may also be associated with heart block in susceptible
patients.
The main side effects associated with b-blockers are reduced sexual function,
fatigue, and reduced exercise tolerance.
The combined α and β-blocker, labetalol, is widely used intravenously for
hypertensive emergencies, and is also used orally for treating hypertension in
pregnant and breastfeeding women.

Chapter 2 Literature Review
Pharmaceutical Medicine 48 Jamia Hamdard
Alpha -Blockers
α-Blockers reduce blood pressure by blocking arterial α-adrenergic receptors
and thus preventing the vasoconstrictor actions of these receptors.
These drugs are less widely used as first-step agents than other classes because
clinical outcome benefits have not been as well established as with other agents.
However, they can be useful in treating resistant hypertension when used in
combination with agents such as diuretics, b-blockers, and angiotensin-
converting enzyme inhibitors.
To be maximally effective, they should usually be combined with a diuretic.
Since a-blockers can have somewhat beneficial effects on blood glucose and
lipid levels, they can potentially neutralize some of the adverse metabolic effects
of diuretics.
The α-blockers are effective in treating benign prostatic hypertrophy, and so can
be a valuable part of hypertension treatment regimens in older men who have
this condition. Weber, et al (ASH/ISH Hypertension Guidelines)
Centrally Acting Agents
These drugs, the most well-known of which are clonidine and a-methyldopa,
work primarily by reducing sympathetic outflow from the central nervous
system.
They are effective in reducing blood pressure in most patient groups.
Bothersome side effects such as drowsiness and dry mouth have reduced their
popularity. Treatment with a clonidine skin patch causes fewer side effects than
the oral agent, but the patch is not always available and can be more costly than
the tablets.
In certain countries, including the United States, α-methyldopa is widely
employed for treating hypertension in pregnancy.
Direct Vasodilators
Because these agents, specifically hydralazine and minoxidil, often cause fluid
retention and tachycardia, they are most effective in reducing blood pressure
when combined with diuretics and β blockers or sympatholytic agents. For this
reason, they are now usually used only as fourth-line or later additions to
treatment regimens.

Chapter 2 Literature Review
Pharmaceutical Medicine 49 Jamia Hamdard
Hydralazine is the more widely used of these agents. The powerful drug
minoxidil is sometimes used by specialists in patients whose blood pressures are
difficult to control. Fluid retention and tachycardia are frequent problems with
minoxidil, as well as unwanted hair growth (particularly in women). Furosemide
is often required to cope with the fluid retention.
Mineralocorticoid Receptor Antagonists
The best known of these agents is spironolactone. Although it was originally
developed for the treatment of high aldosterone states, it recently has become
part of standard treatment for heart failure.
Eplerenone is a newer and better-tolerated agent, although most experience in
difficult-to-control hypertension has been with spironolactone.
In addition, these agents can be effective in reducing blood pressure when
added to standard 3-drug regimens (angiotensin-converting enzyme inhibitor or
angiotensin receptor blocker/ calcium channel blocker/diuretic) in treatment-
resistant patients. This may be because aldosterone excess can contribute to
resistant hypertension. NICE Clinical Guidelines. February 2011.
Choice of antihypertensive agent in patients with co morbid and associated
conditions is shown in table 2.6( Guide to management of Hypertension 2010).
Table 2.6 Antihypertensive agents in co morbid and associated condition
Condition Potentially beneficialPotentially harmful
Caution Contraindicated
Angina
β-blockers(exceptoxprenolol,pindolol),calcium channel blockers,ACE inhibitors
Atrial fibrillation
Remodelling: ACEinhibitors, angiotensin II
receptor antagonists,Ratecontrol: verapamildiltiazem,beta blockers
Asthma/COPD Cardioselective βblockers(except

Chapter 2 Literature Review
Pharmaceutical Medicine 50 Jamia Hamdard
β- blocker (e.gatenolo,metoprolol) usecautiously inmild/moderateasthma COPD
cardioselectiveagents)
Bradycardia, 2nd or3rddegree-eatrioventricularblock
Beta-blockers,verapamil,diltiazem
Depression
Beta-blockers,clonidine,
methyldopa,moxonidine
Gout Losartan Thiazidediuretics
Heart failure
ACE inhibitors,angiotensin II receptorantagonists, Thiazide
diuretics, Beta-blockers(bisoprolol, carvidilol,metoprolol controlled
release),spironoloactone
Calcium channelblockers
(especiallyverapamil,diltiazem)
Alpha blockersin aortic stenosis
Beta-blockers inuncontrolledheart failure
Post myocardial
infarction
Beta-blockers (exceptoxprenolol, pindolol),
ACE inhibitors,eplerenone
Pregnancy Atenolol,oxprenolol
ACE inhibitors,angiotensin II
receptorantagonists
Chronic kidneydisease
ACE inhibitors,angiotensin II receptor
antagonists†Tight bilateral
renal arterystenosis (unilateral
in patient withsolitary kidney)
ACE inhibitors,angiotensin II
receptorantagonists
Post stroke
ACE inhibitors,angiotensin II receptorantagonists, low-dosethiazide-like diuretics
Type 1 or type 2diabetes withproteinuria or
microalbuminuria
ACE inhibitors,angiotensin II receptor
antagonists
Beta-blockers,Thiazidediuretics




![BeST - Bioequivalence Study Templatestudy carried out to evaluate the bioequivalence of two medicinal products. The bioequivalence studies are strictly regulated [1] and are therefore](https://img.pdfslide.us/doc/110x75/5ed9f97c28db2d5ca2492e81/best-bioequivalence-study-template-study-carried-out-to-evaluate-the-bioequivalence.jpg)