Embed Size (px)
Citation preview
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 1/49
Shoulder Joint & Its Applied Anatomy
By
Dr.P.Sasikala
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 2/49
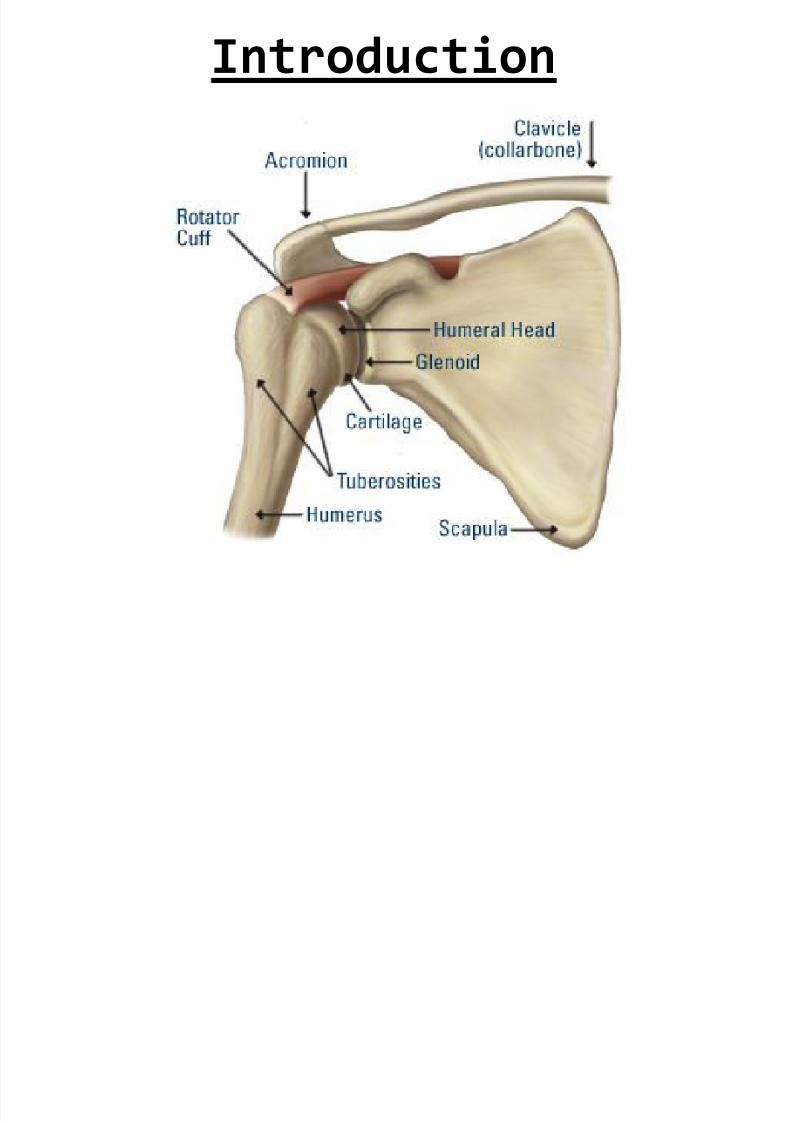
Introduction
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 3/49
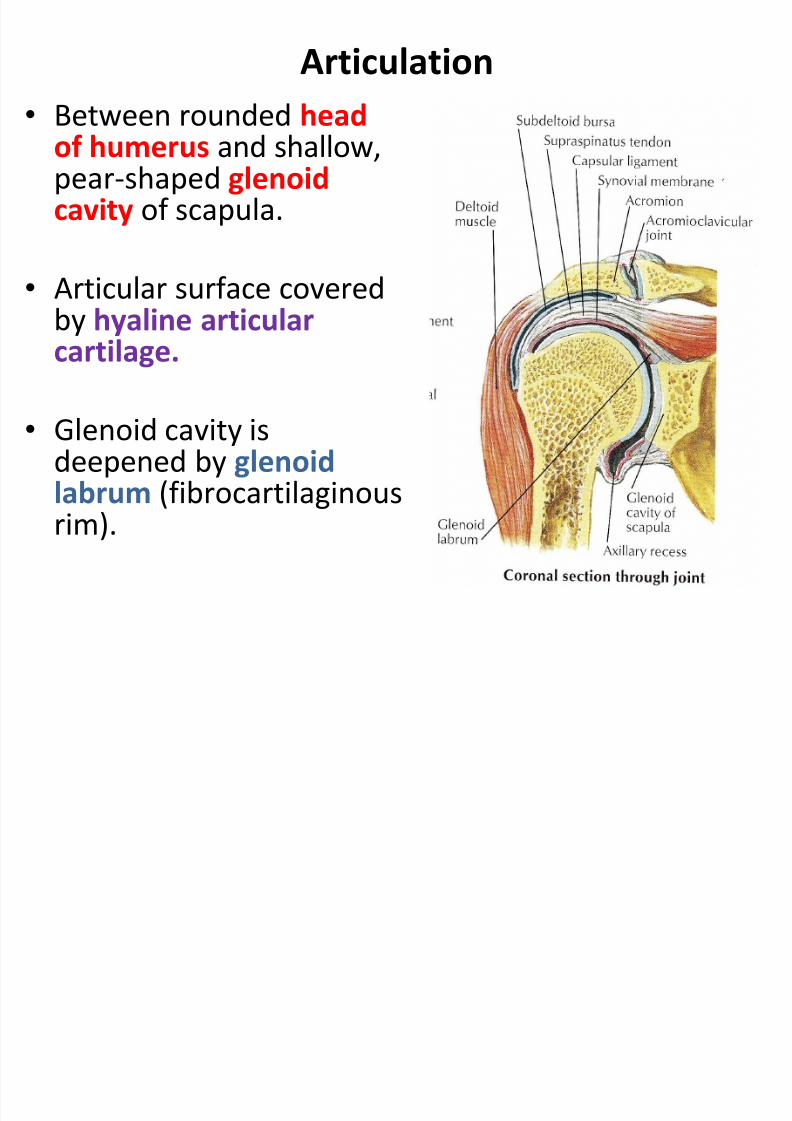
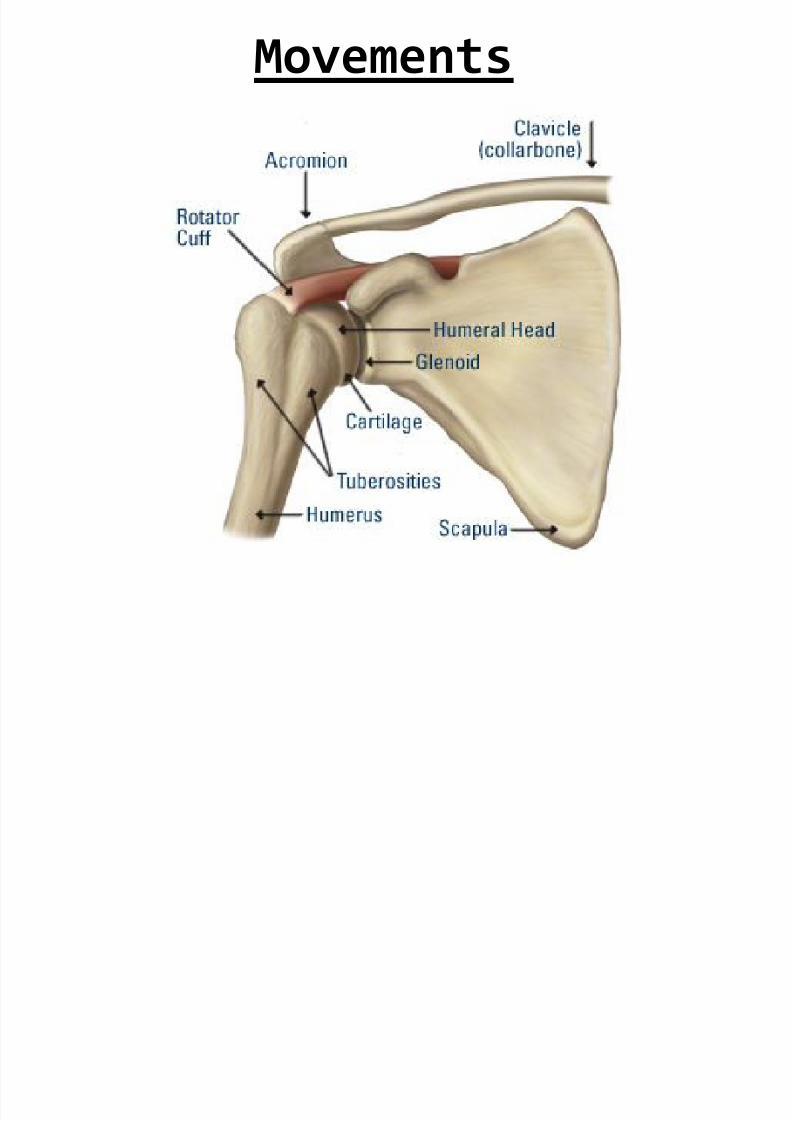
Articulation
• Between rounded headof humerus and shallow,pear-shaped glenoidcavity of scapula.
• Articular surface coveredby hyaline articularcartilage.
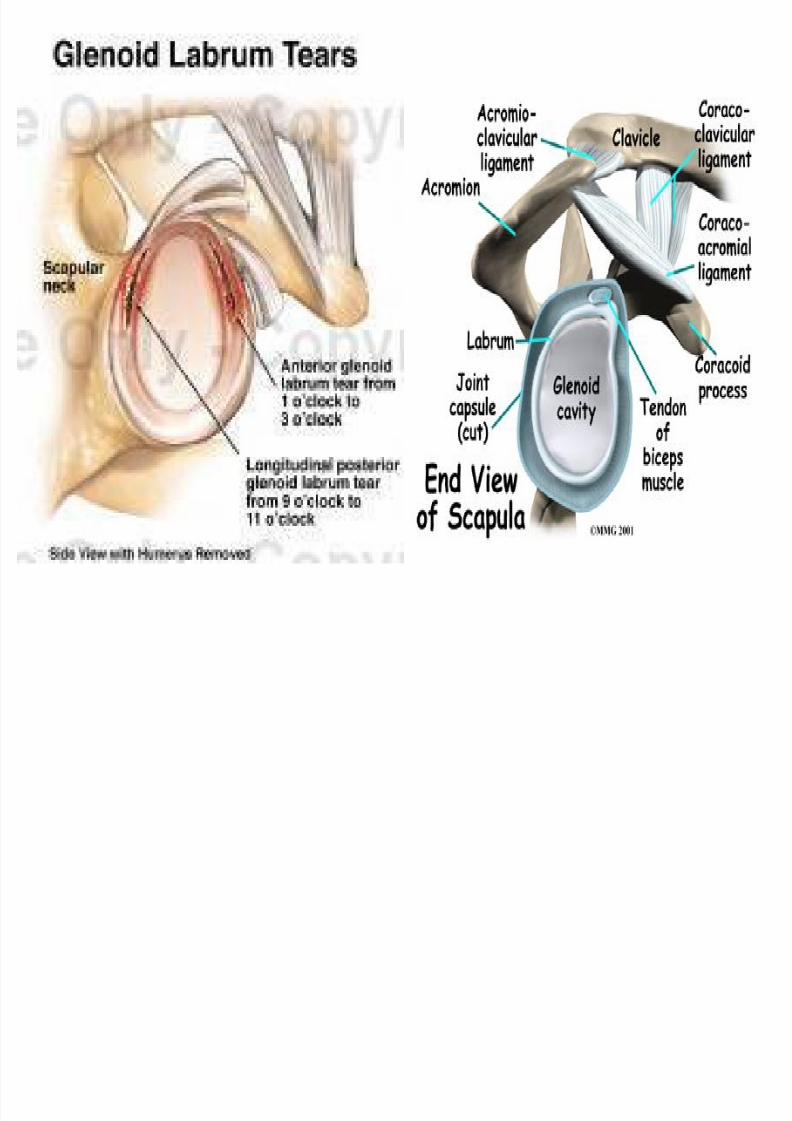
• Glenoid cavity isdeepened by glenoidlabrum (fibrocartilaginousrim).
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 4/49
Type
• Synovial ball-and-socket joint.
Capsule
• Surrounds joint and attached :
- Medially to the scapula beyond the supraglenoid
tubercle and the margins of the labrum.
- Laterally to the anatomical neck of humerus.
• Thin and lax, allow wide range of movement.
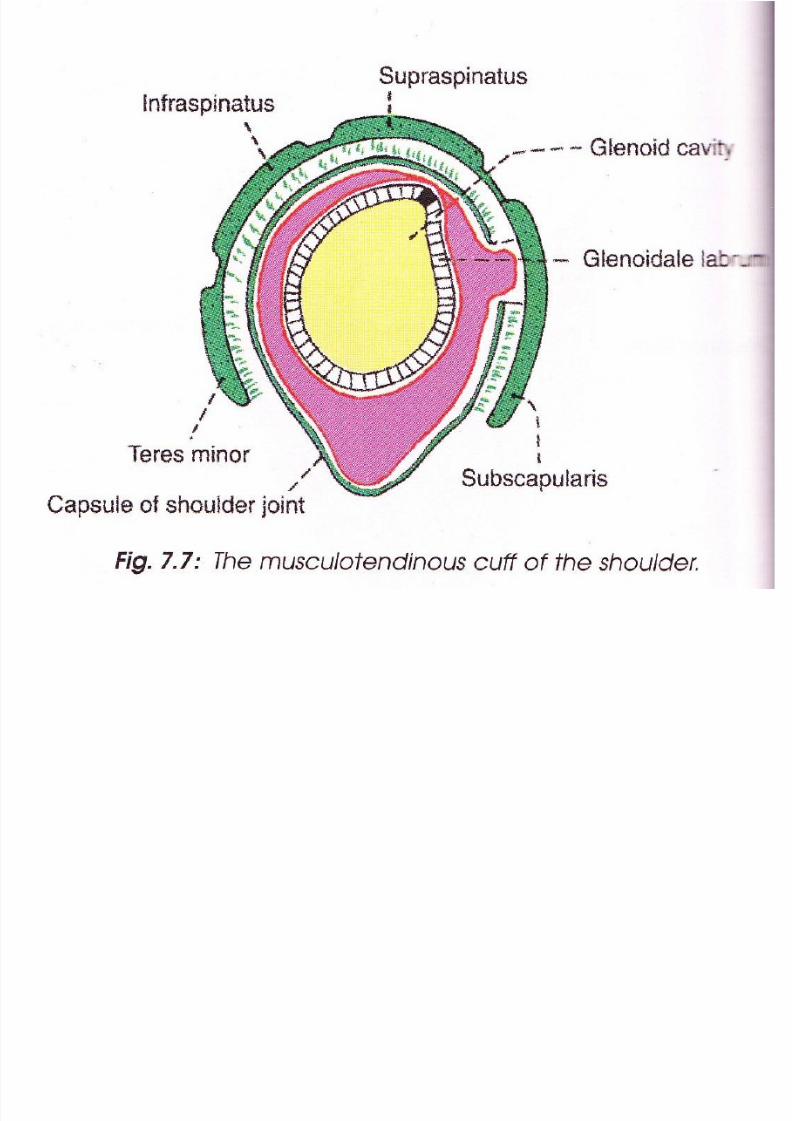
• Strengthened by slips of tendons of subscapularis m.,supraspinatus m., infraspinatus m. & teres minor(rotator cuff muscles).
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 5/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 6/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 7/49
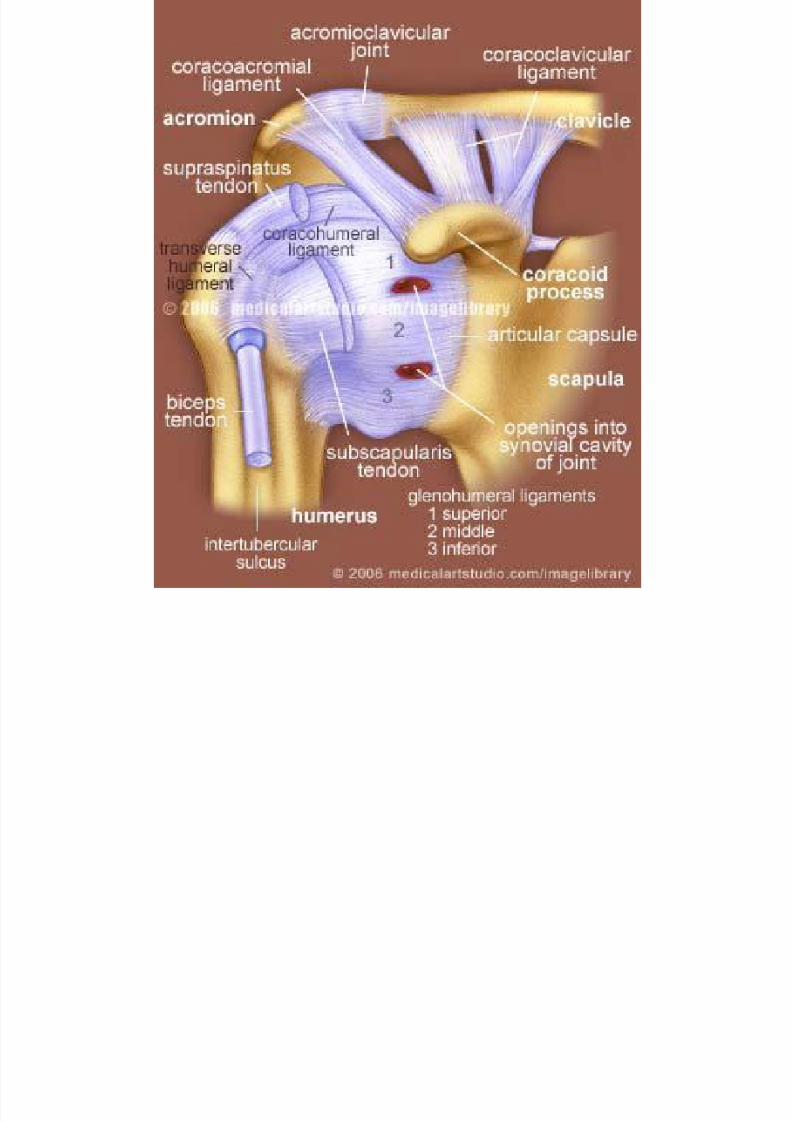
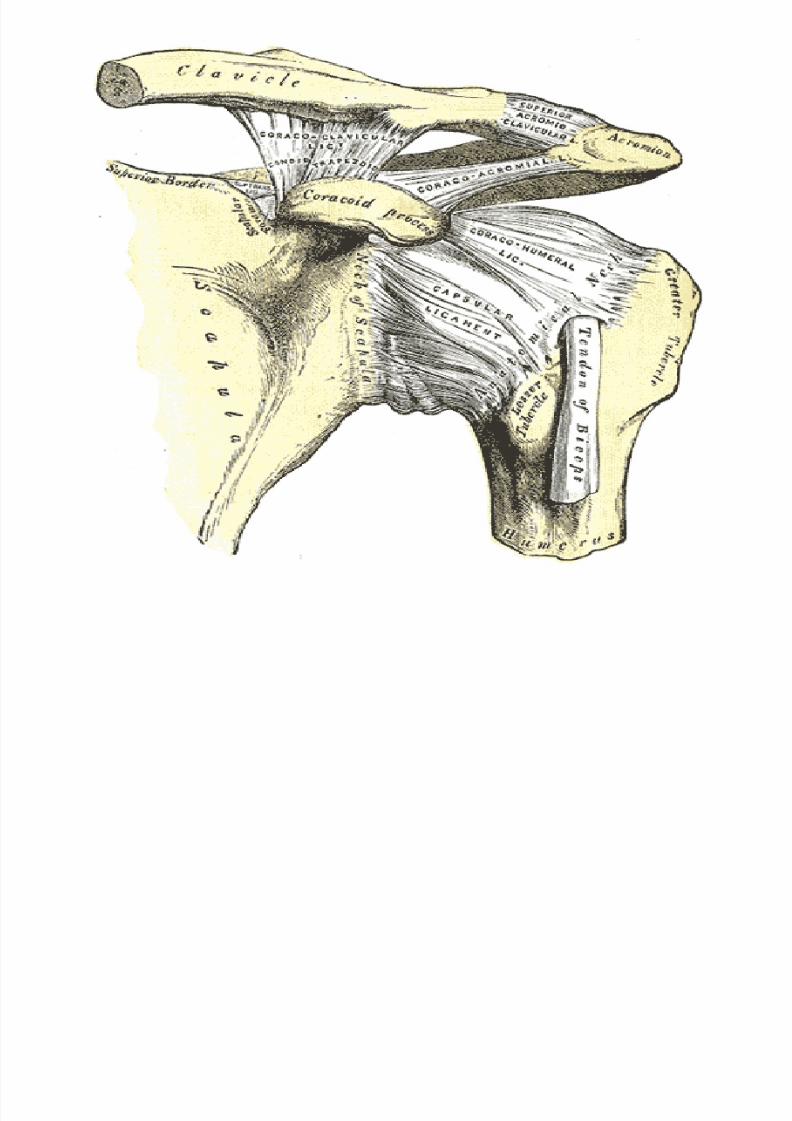
Ligaments
• Glenohumeral Ligament
- 3 weak bands (superior, middle & inferior) of fibrous tissue thatstrengthen the anterior (front) of capsule.
• Transverse humeral Ligament
- Bridge the upper part of bicipital grooves of humerus (between
greater and lesser tubercles).- Tendon of long head biceps brachii passes deep to it.
• Coracohumeral Ligament
- Stretches from root of the coracoid process of scapula to greatertuberosity of humerus.
- Strength the capsule above.• Coracoacromial Ligament
- Accessory ligament.
- Extends between coracoid process of scapula and acromion.
- Protects the superior aspect of joint.
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 8/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 9/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 10/49
Bursae Related To The Joint
• Subacromial (Subdeltoid)
bursa• Subscapularis bursa
• Infraspinatus bursa
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 11/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 12/49
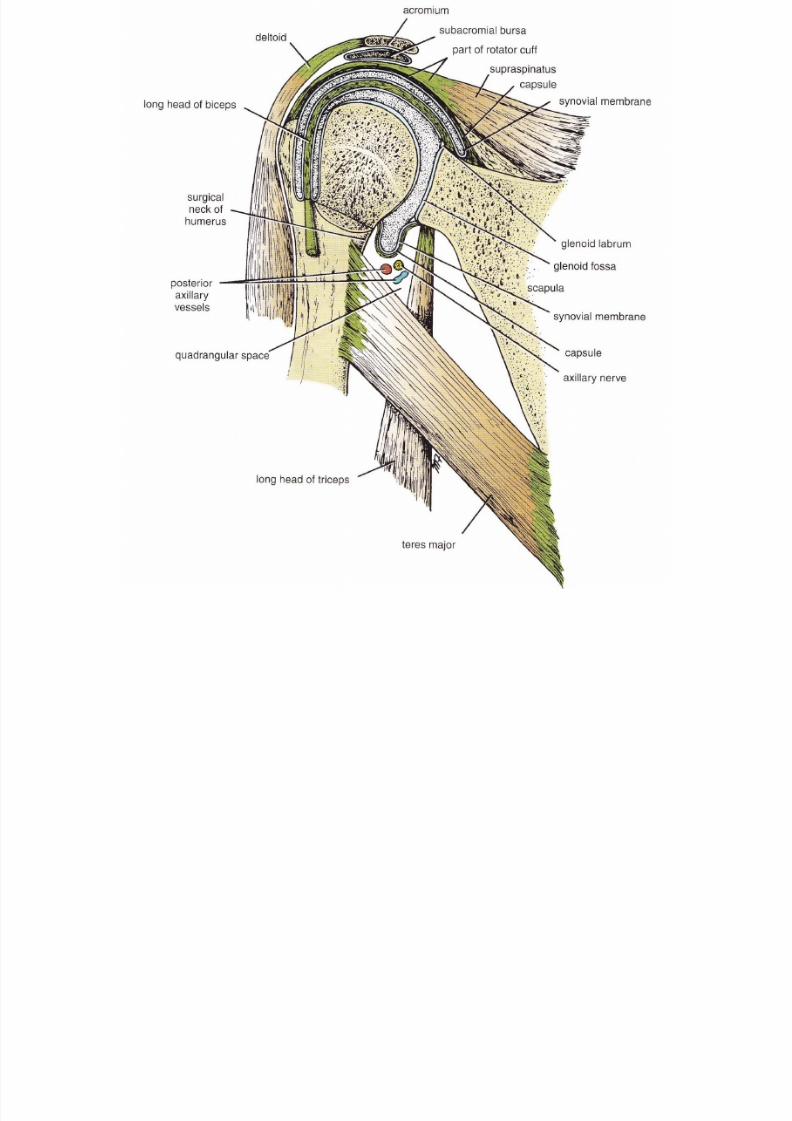
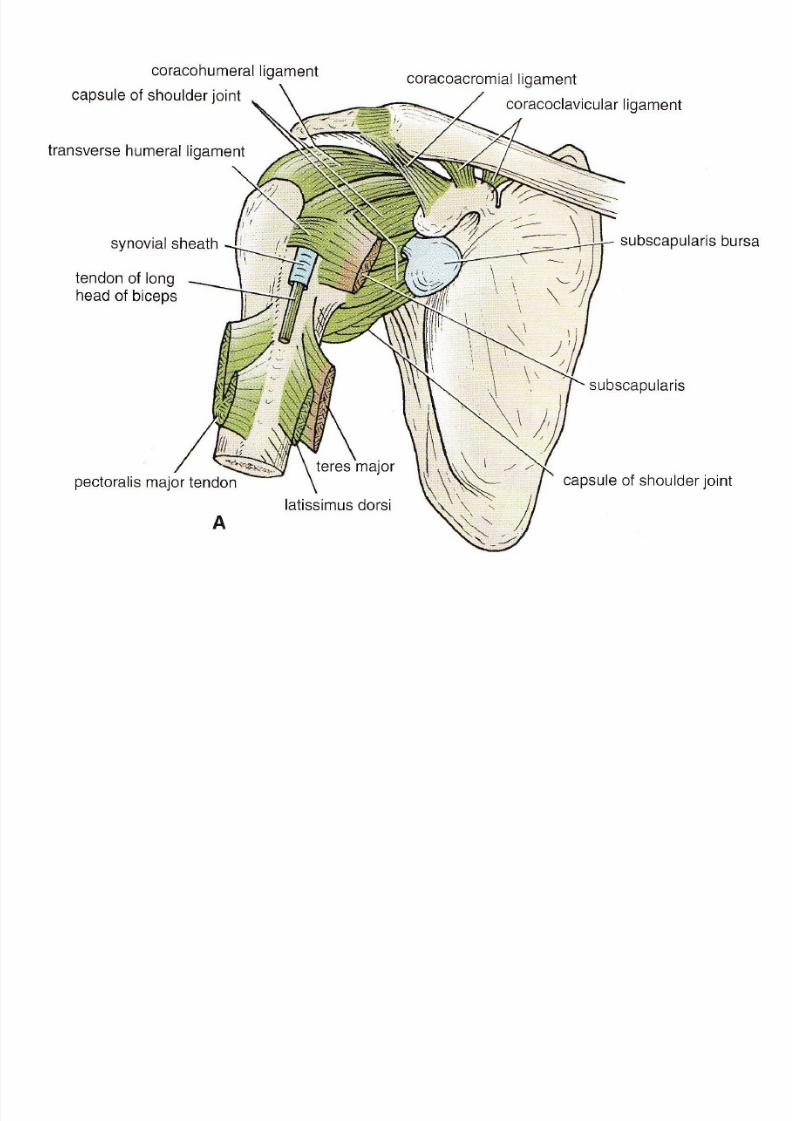
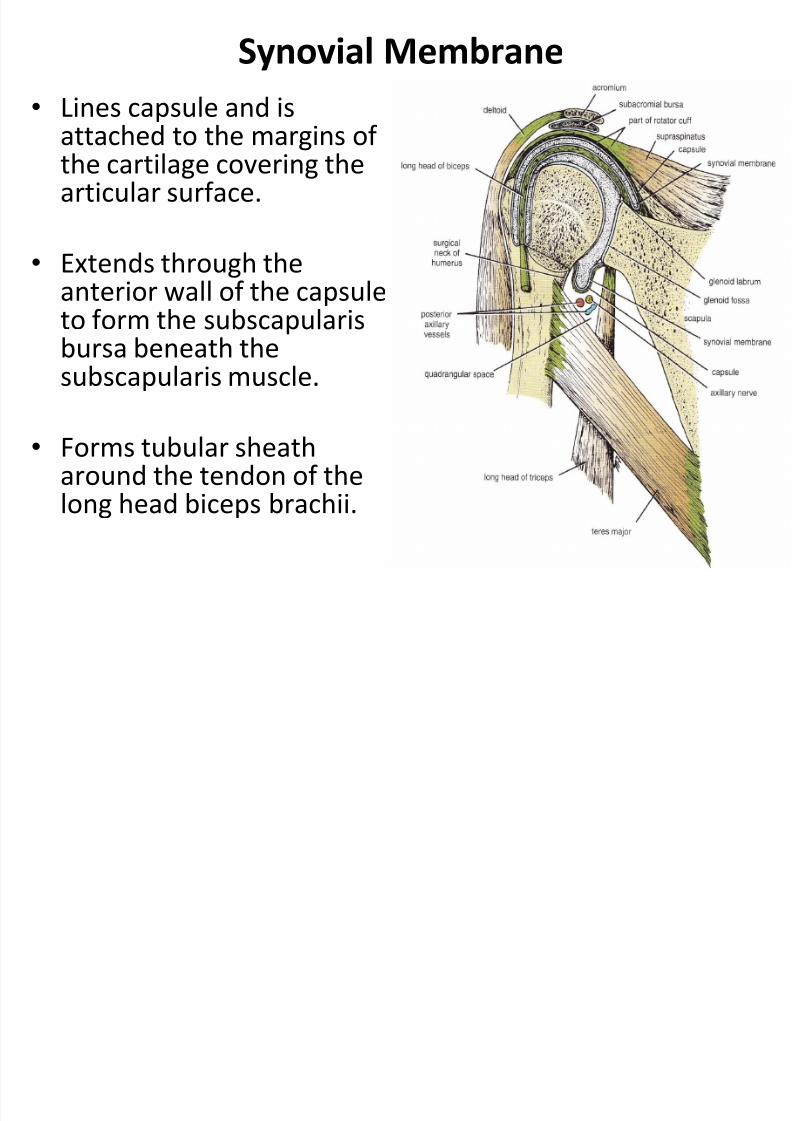
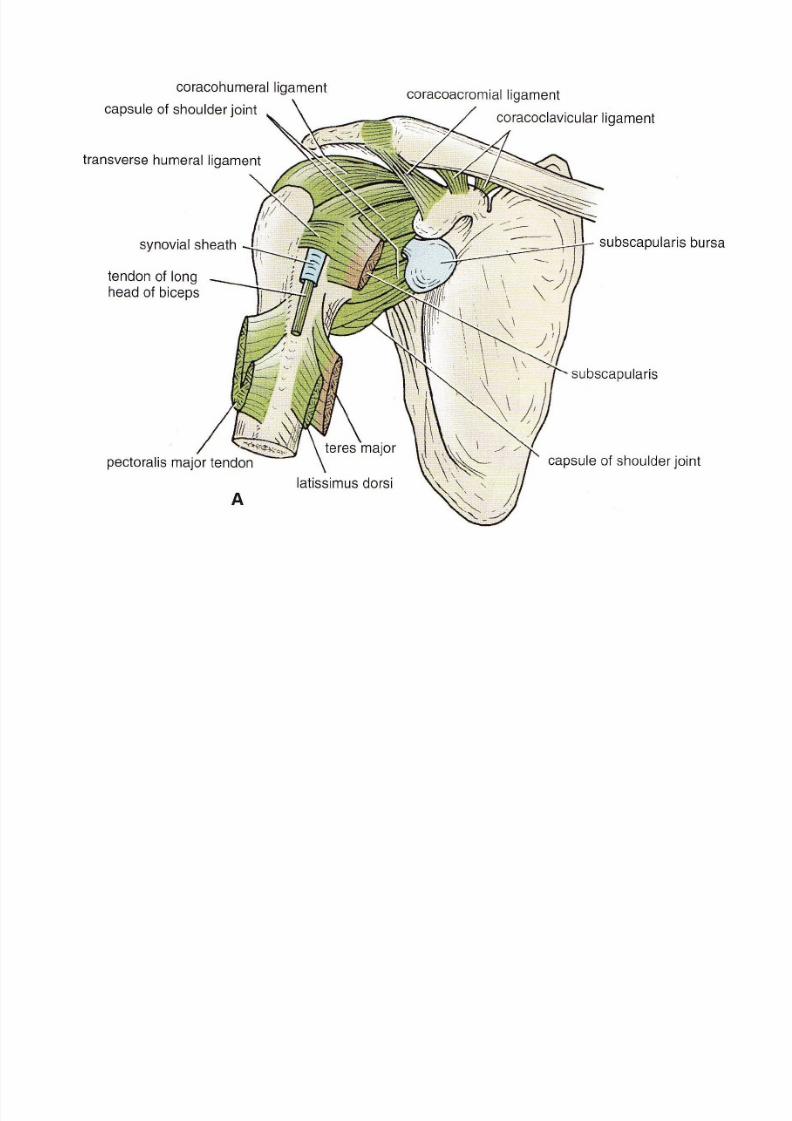
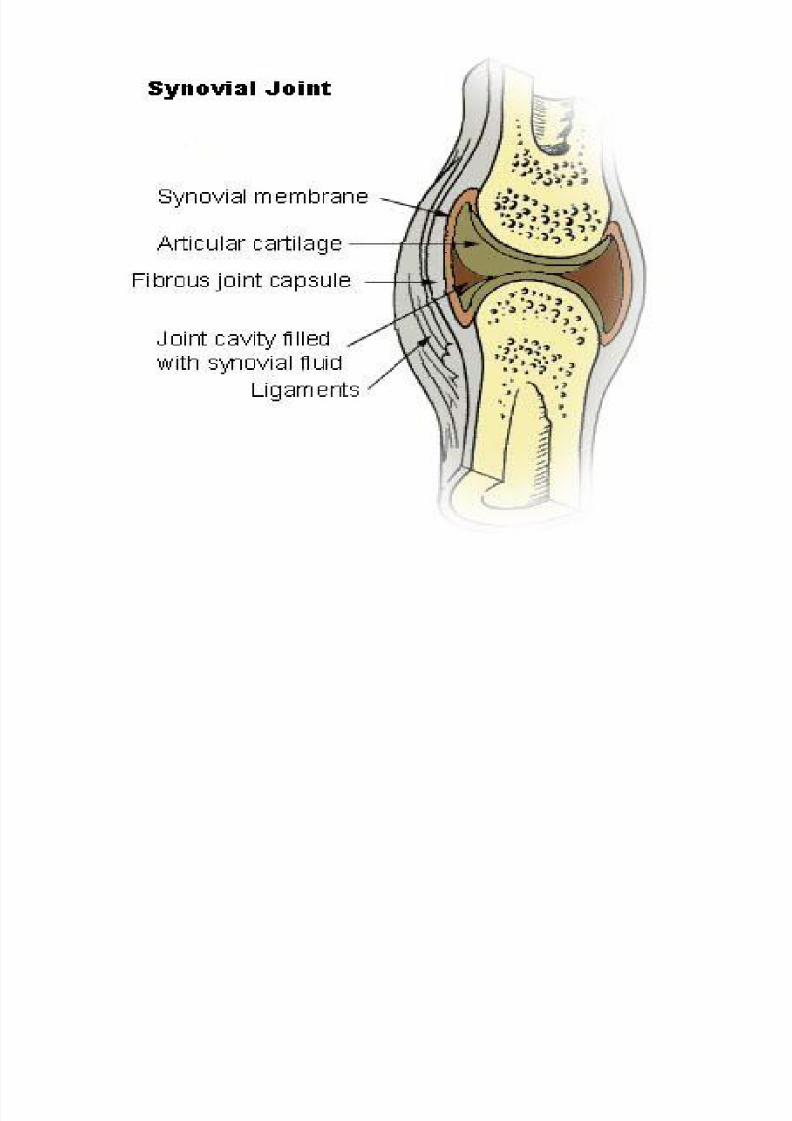
Synovial Membrane
• Lines capsule and is
attached to the margins of the cartilage covering thearticular surface.
•Extends through theanterior wall of the capsuleto form the subscapularisbursa beneath thesubscapularis muscle.
• Forms tubular sheatharound the tendon of thelong head biceps brachii.
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 13/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 14/49
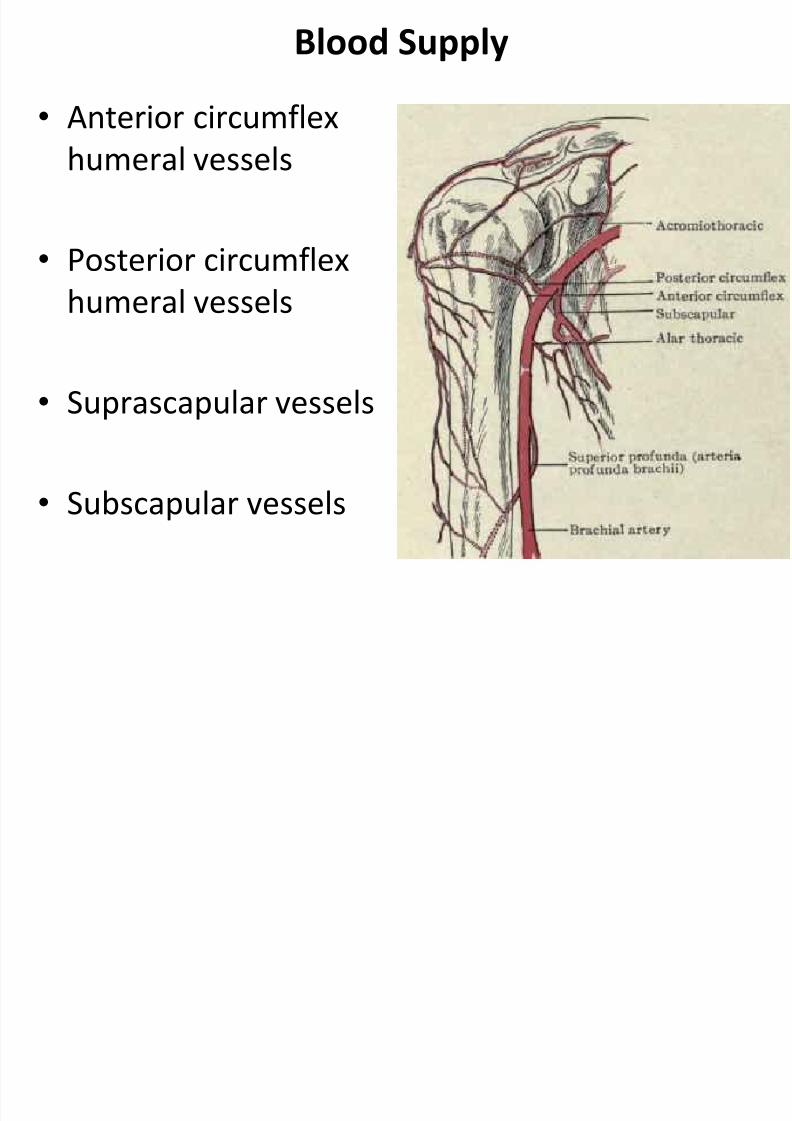
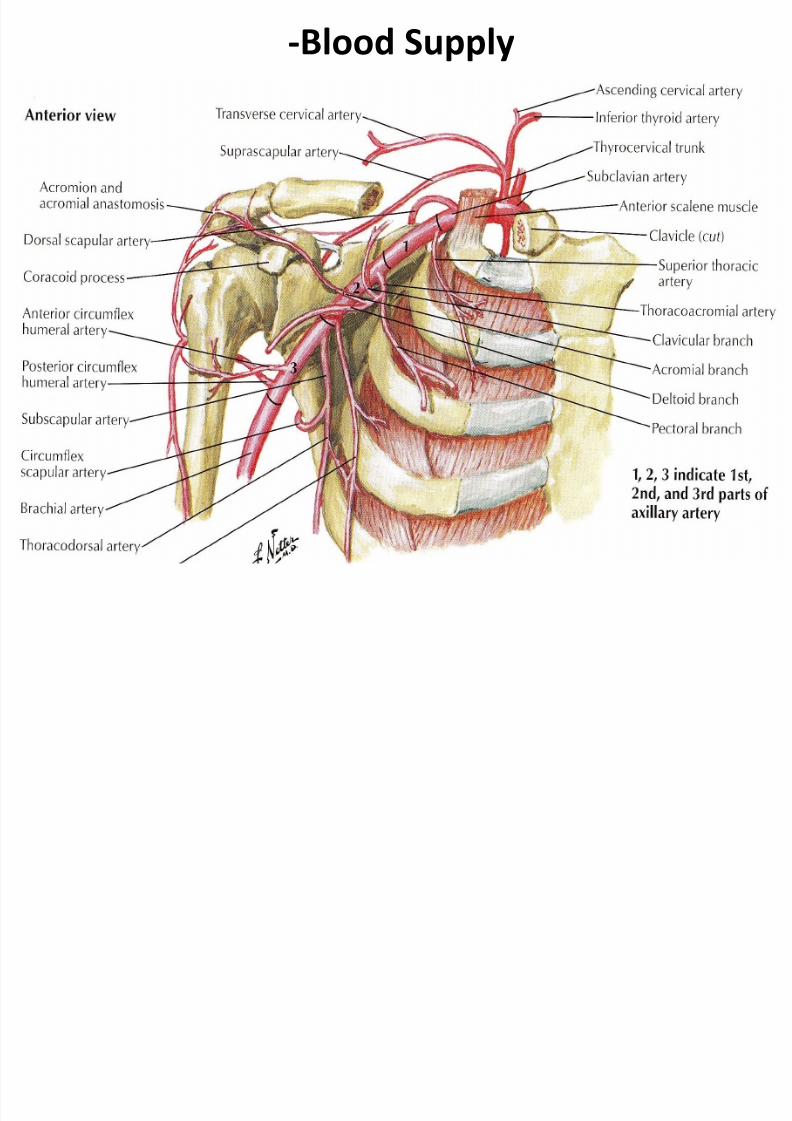
Blood Supply
• Anterior circumflex
humeral vessels
• Posterior circumflex
humeral vessels
•Suprascapular vessels
• Subscapular vessels
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 15/49
-Blood Supply
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 16/49
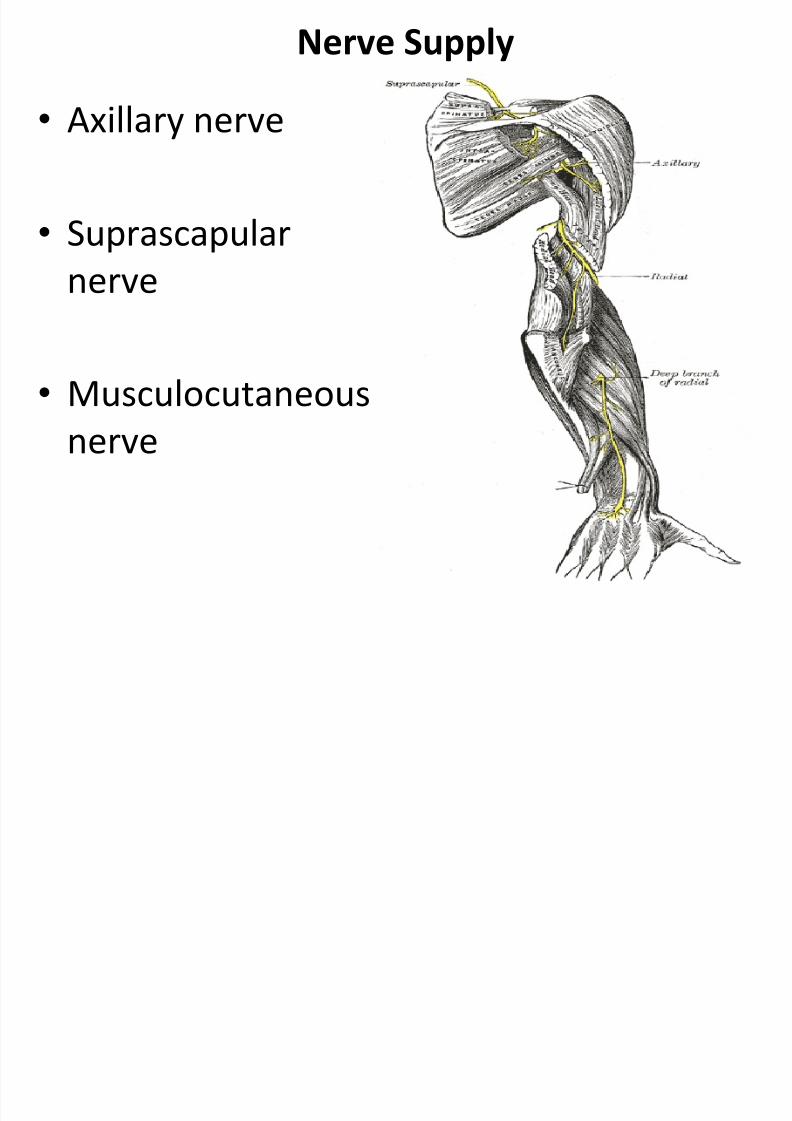
Nerve Supply
• Axillary nerve
• Suprascapular
nerve
• Musculocutaneous
nerve
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 17/49
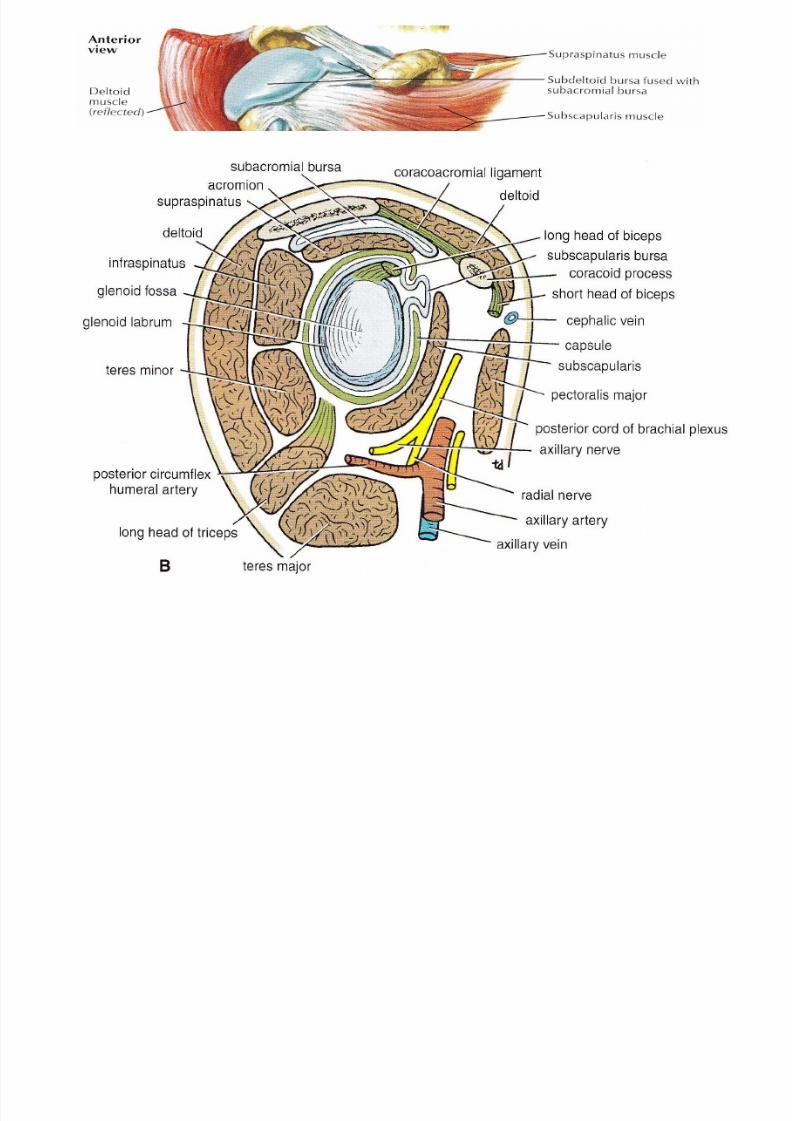
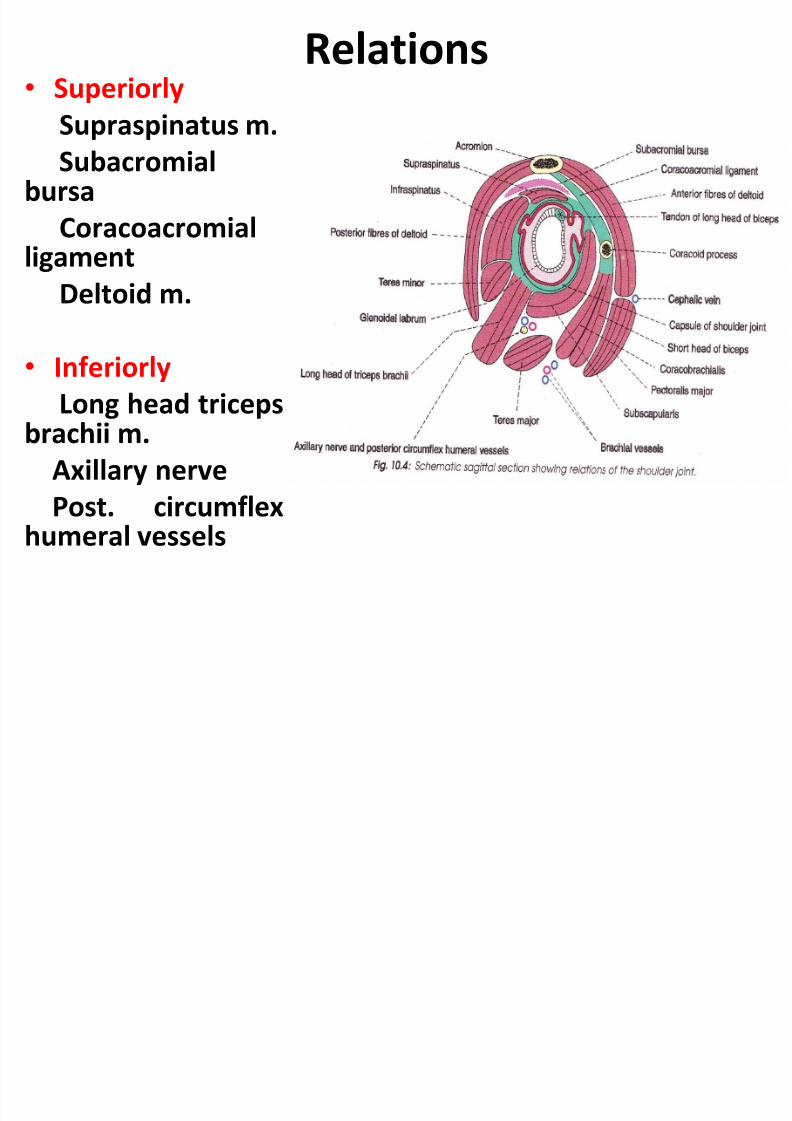
Relations • Superiorly
Supraspinatus m.
Subacromialbursa
Coracoacromialligament
Deltoid m.
• Inferiorly
Long head tricepsbrachii m.
Axillary nerve
Post. circumflexhumeral vessels
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 18/49
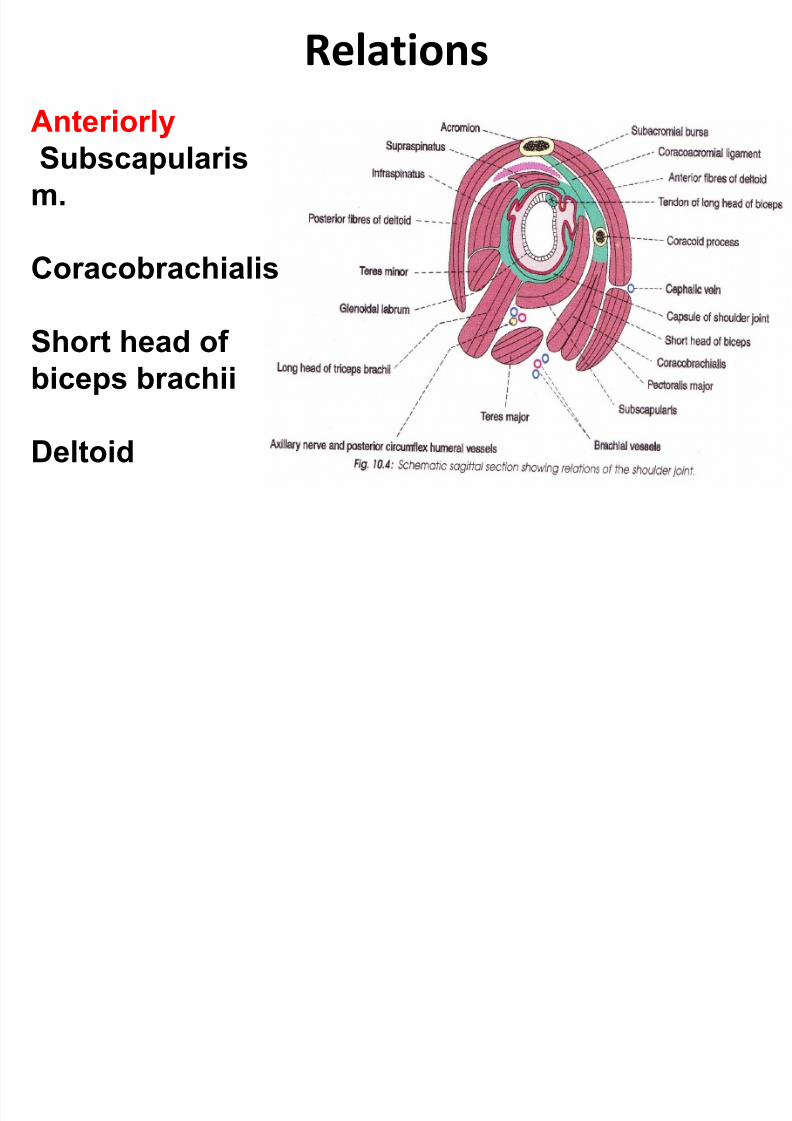
Relations
Anteriorly
Subscapularis
m.
Coracobrachialis
Short head of
biceps brachii
Deltoid
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 19/49
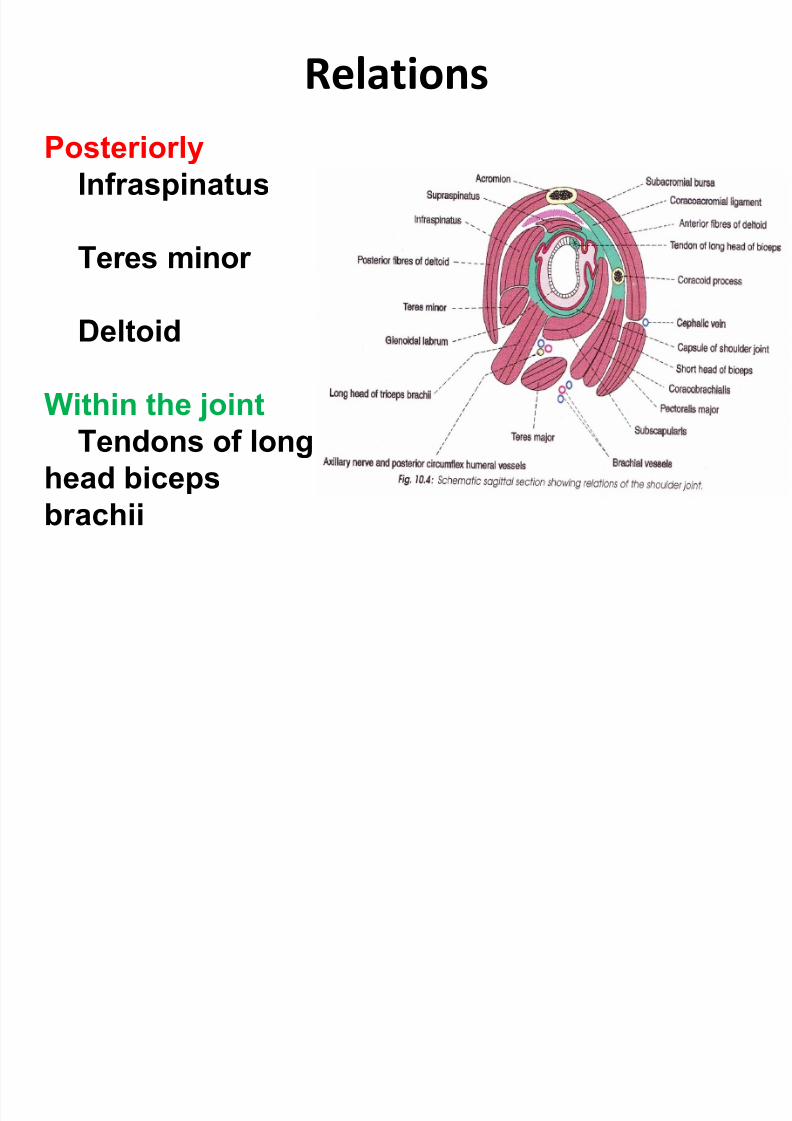
Relations
PosteriorlyInfraspinatus
Teres minor
Deltoid
Within the jointTendons of long
head biceps
brachii
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 20/49
Movements
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 21/49
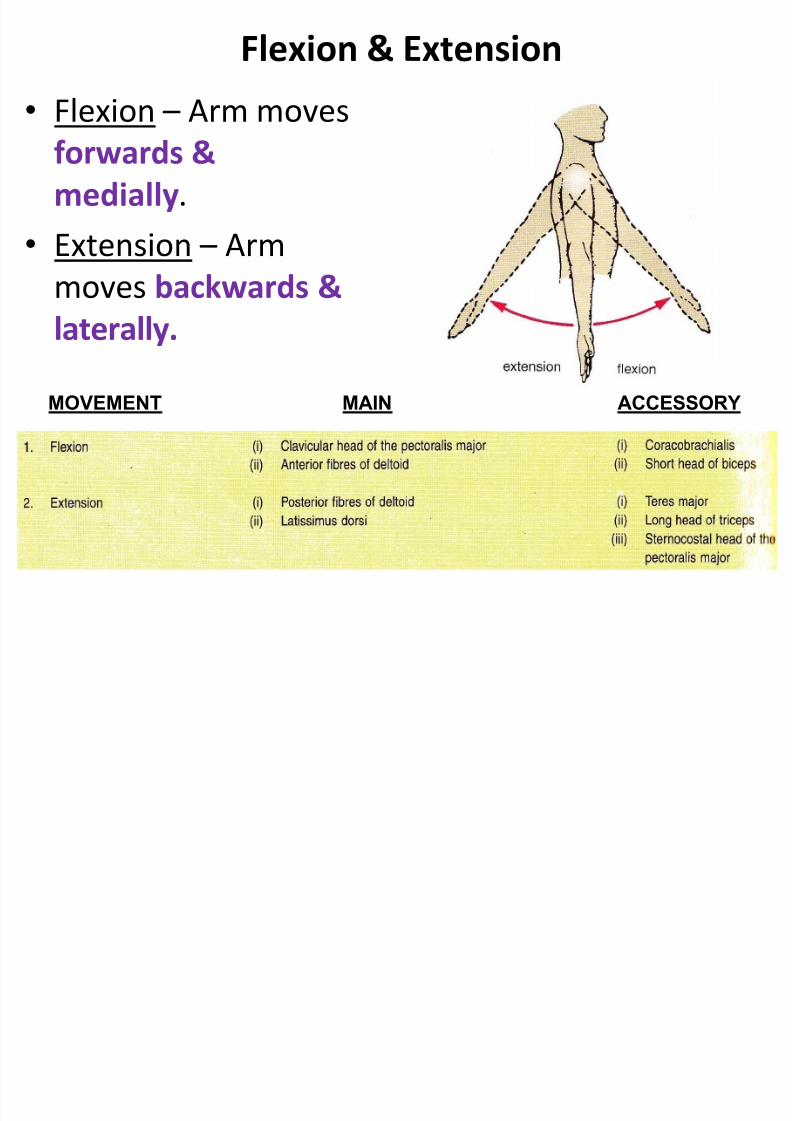
• Flexion – Arm moves
forwards &
medially.
• Extension – Arm
moves backwards &laterally.
Flexion & Extension
MAIN ACCESSORYMOVEMENT
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 22/49
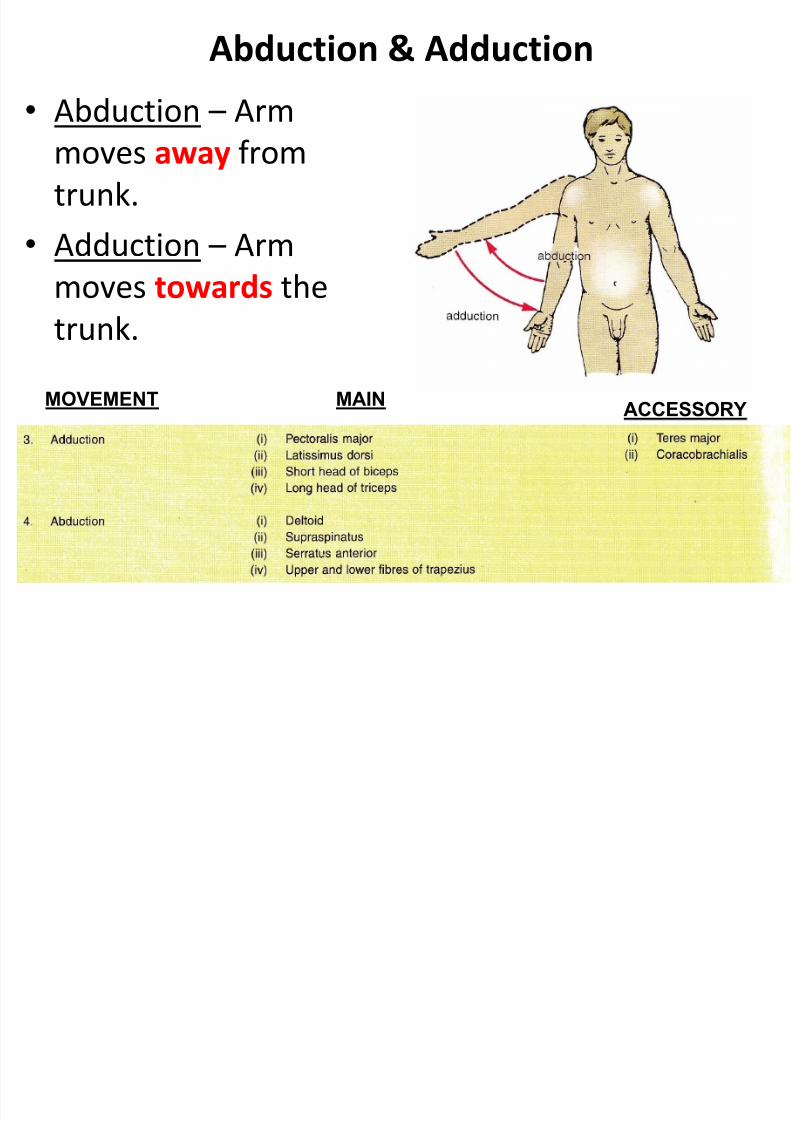
• Abduction – Arm
moves away from
trunk.
• Adduction – Arm
moves towards thetrunk.
Abduction & Adduction
MAIN
ACCESSORY
MOVEMENT
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 23/49
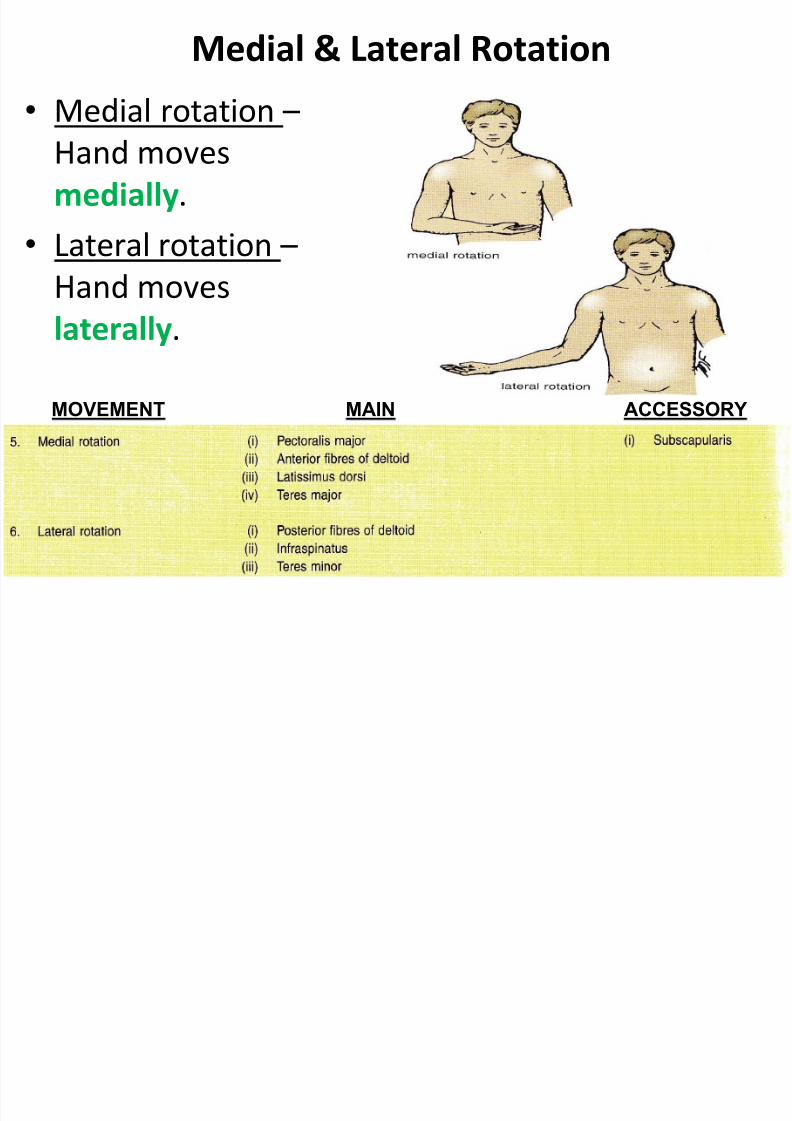
• Medial rotation –
Hand moves
medially.
• Lateral rotation –
Hand moveslaterally.
Medial & Lateral Rotation
MAIN ACCESSORYMOVEMENT
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 24/49
• Combination of
dif. movements,
results in hand
moving along acircle.
Circumduction
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 25/49
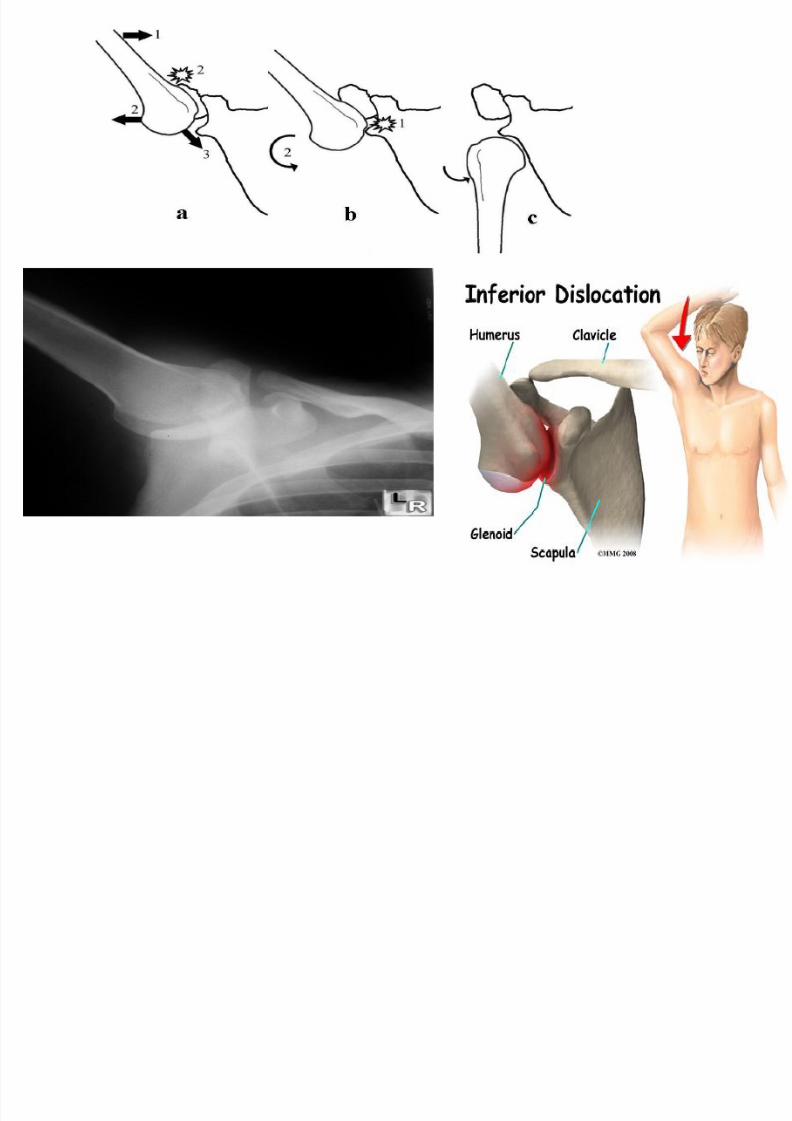
Applied AnatomyDislocation
is an injury to your joint in which the ends of your bones areforced from their normal positions.
This injury temporarily deforms and immobilizes your joint and
may result in sudden and severe pain.
The shoulder is more prone to dislocate than any other joint.
This due to :• laxity of the capsule
• Disproportionate area of articular surfaces
Occurs when the arm is abducted
3 types of shoulder joints:
• Glenohumeral joint
• Acromioclavicular joint
• Sternoclavicular joint
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 26/49
Applied Anatomy Dislocation of glenohumeral joint
Glenohumeral joint Extremely mobile
Providing wide movement at the
expense of stability
Relatively small bony glenoid cavity
Supplemented by :• Robust fibrocartilagious glenoid labrum
• Ligamentous support
Make it susceptible to dislocation
Divided into :
Anterior dislocation
Posterior dislocation
A li d A t
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 27/49
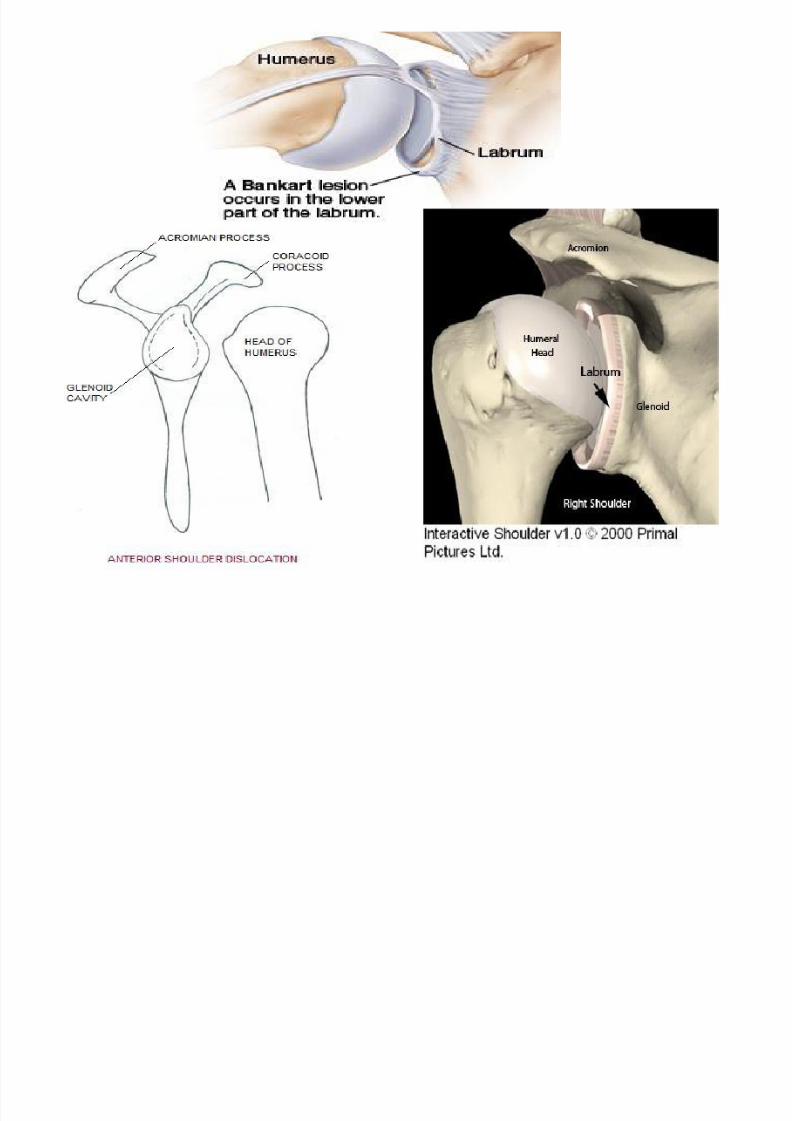
Applied Anatomy Anterior dislocation
Occurs most frequently.
Usually associated with an isolated traumatic incident.
Clinically, all anterior dislocation are anteroinferior.
Once joint capsule and cartilage disrupted
Joint is susceptible to further (recurrent) dislocation
When dislocation occurs,
During abduction, the head of humerus presses against the lower unsupported partof capsular ligament
Thus, almost always the dislocations primarily subglenoid, later it may becomesubcoracoid, subclavicular or subspinous.
Dislocations ends with :
a) Axillary nerve injured (by direct compression of humeral head on the nerveinferiorly as it passes through quadrangular space)
b) Lengthening effect of humerus may stretch the radial nerve which cause radialnerve paralysis
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 28/49
Applied Anatomy
Occasionally, anteroinferior dislocation associated with
fracture and require surgical reduction.
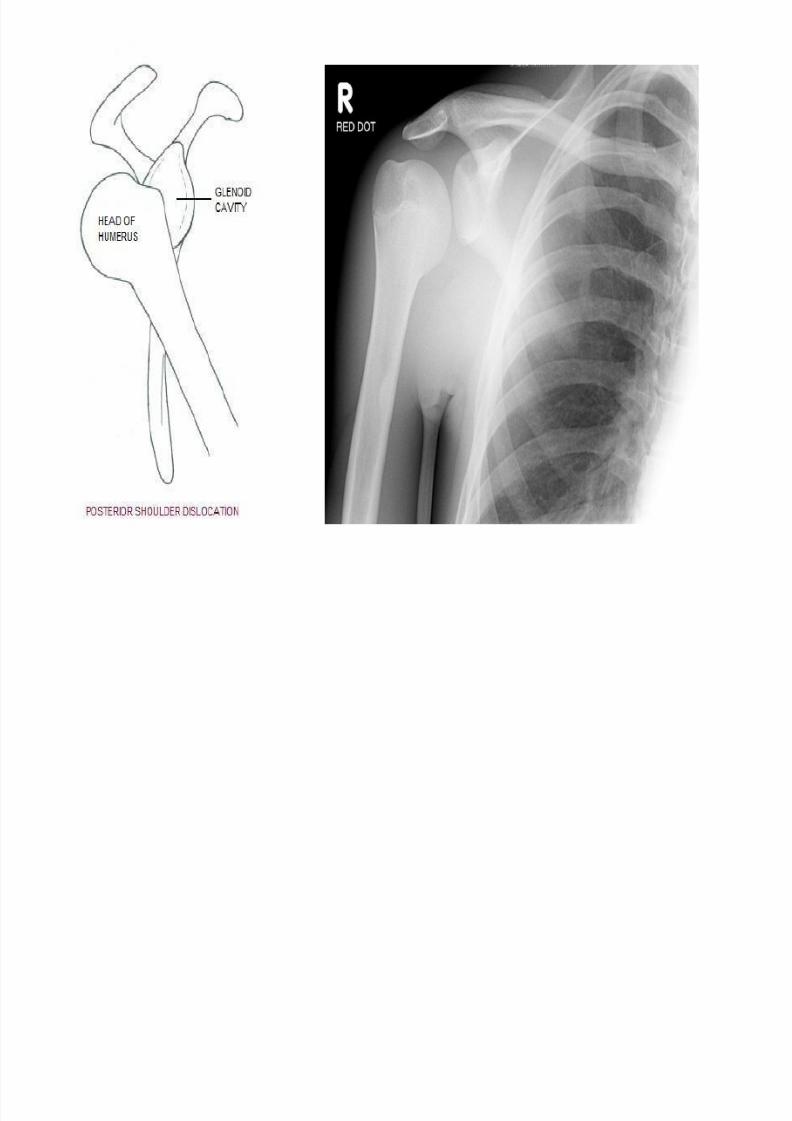
Posterior dislocation
Rare
Most common cause :
• Extremely vigorous muscle contraction
associated with
An epileptic seizure
caused by
electrocution
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 29/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 30/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 31/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 32/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 33/49
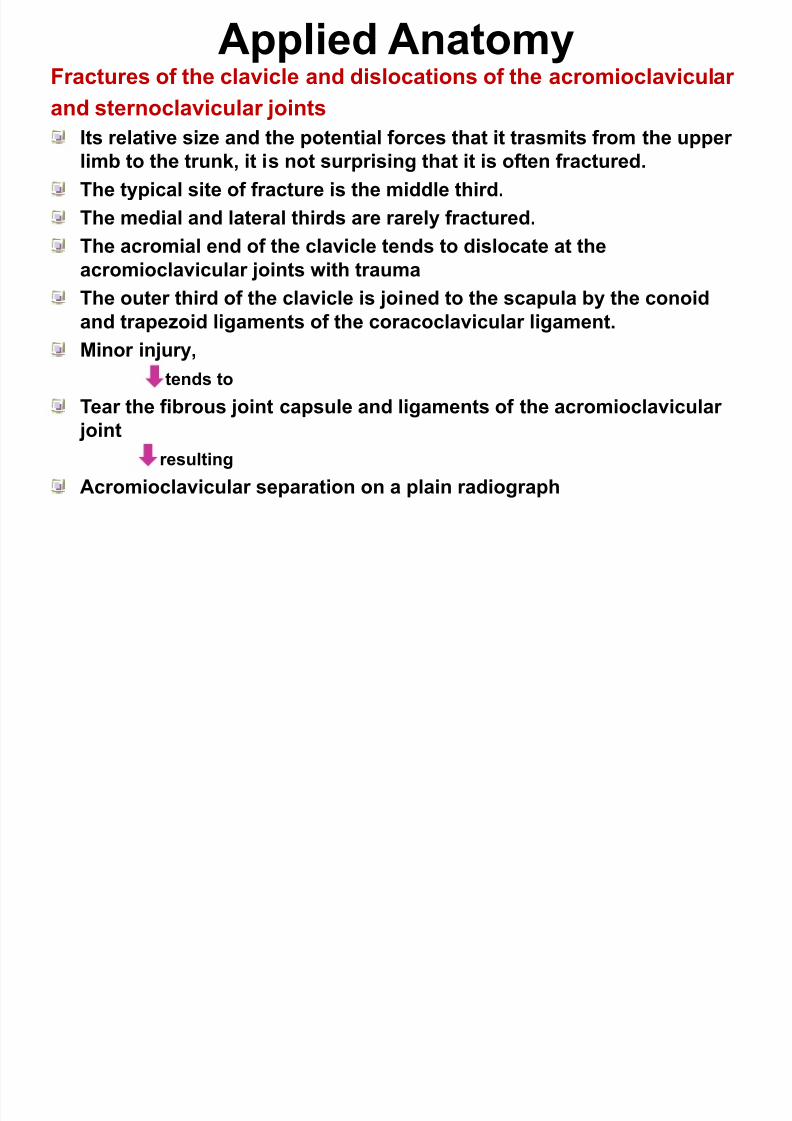
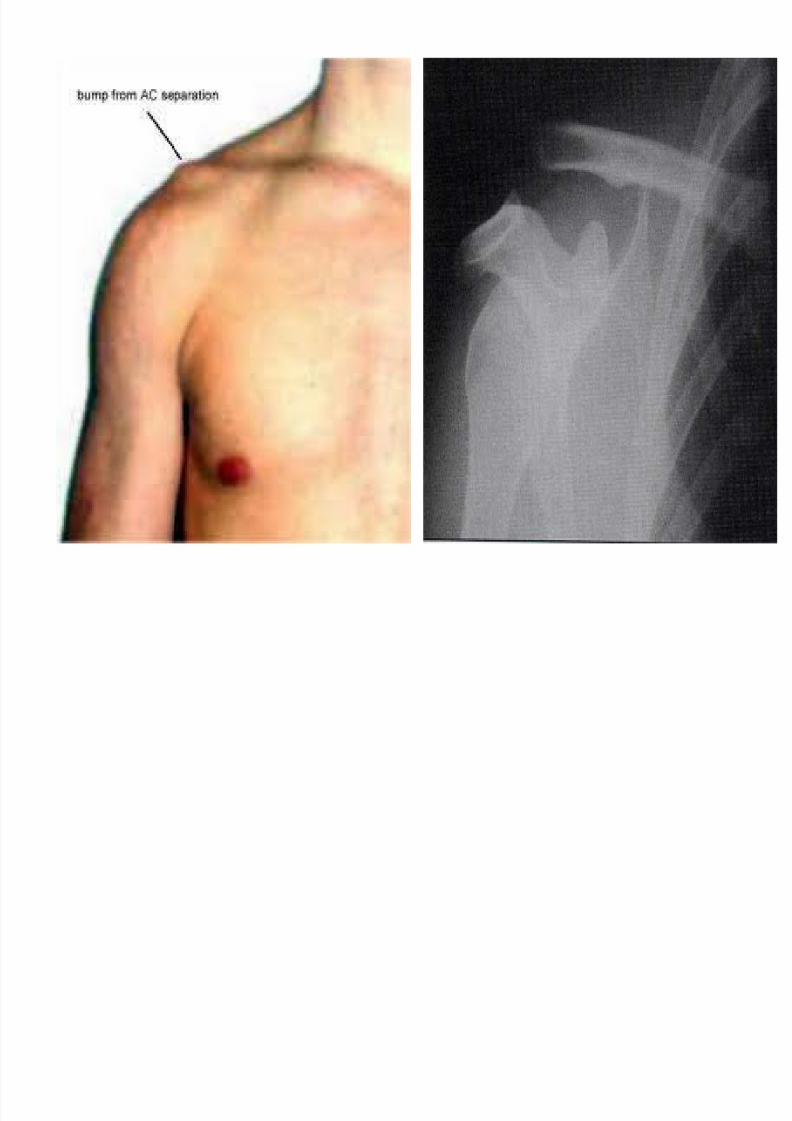
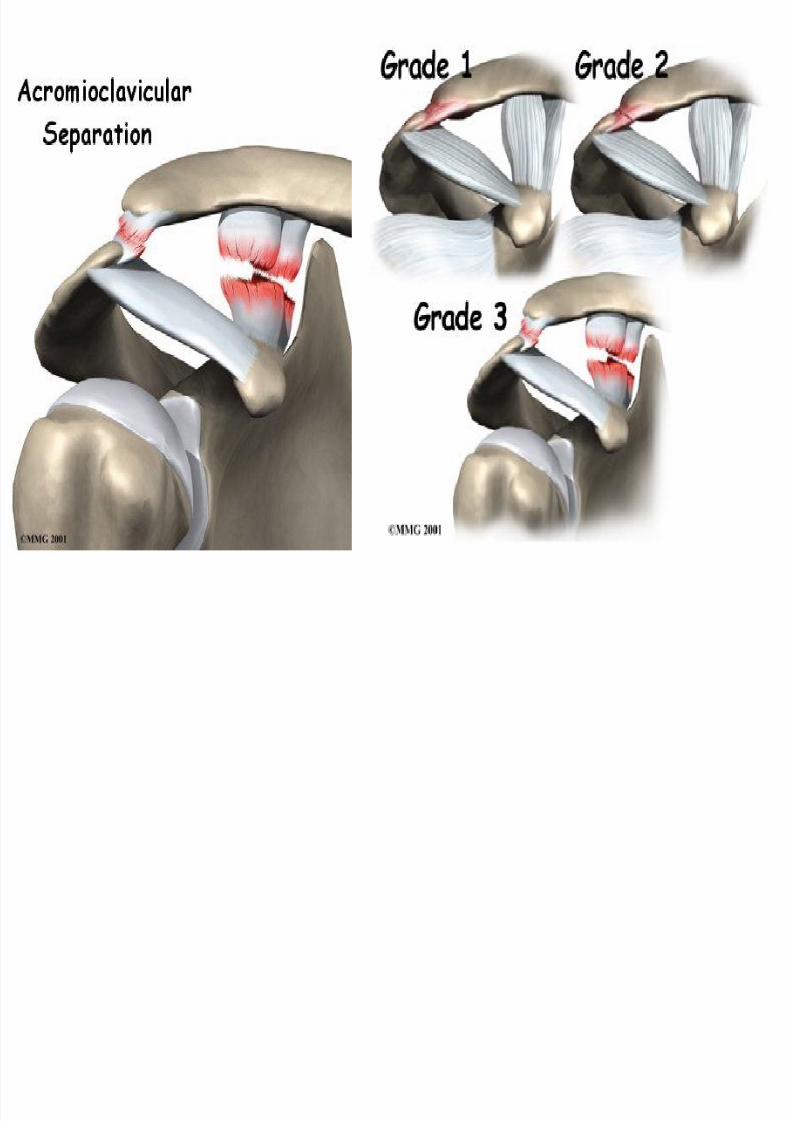
Applied Anatomy Fractures of the clavicle and dislocations of the acromioclavicular
and sternoclavicular joints
Its relative size and the potential forces that it trasmits from the upper limb to the trunk, it is not surprising that it is often fractured.
The typical site of fracture is the middle third.
The medial and lateral thirds are rarely fractured.
The acromial end of the clavicle tends to dislocate at the
acromioclavicular joints with trauma
The outer third of the clavicle is joined to the scapula by the conoid
and trapezoid ligaments of the coracoclavicular ligament.
Minor injury,
tends to
Tear the fibrous joint capsule and ligaments of the acromioclavicular
joint
resulting
Acromioclavicular separation on a plain radiograph
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 34/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 35/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 36/49
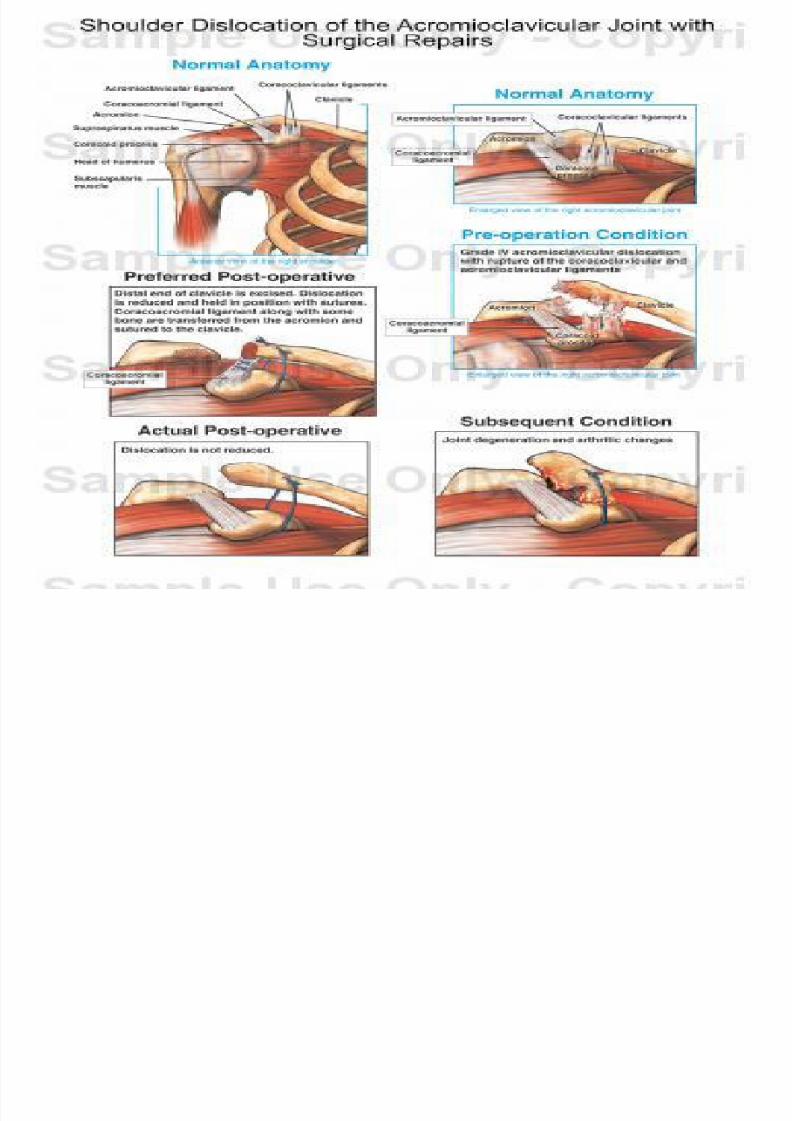
Applied Anatomy More severe trauma
disrupt the conoid and trapezoid ligaments of coracoclavicular
ligament
results in elevation and upward subluxation of the clavicle
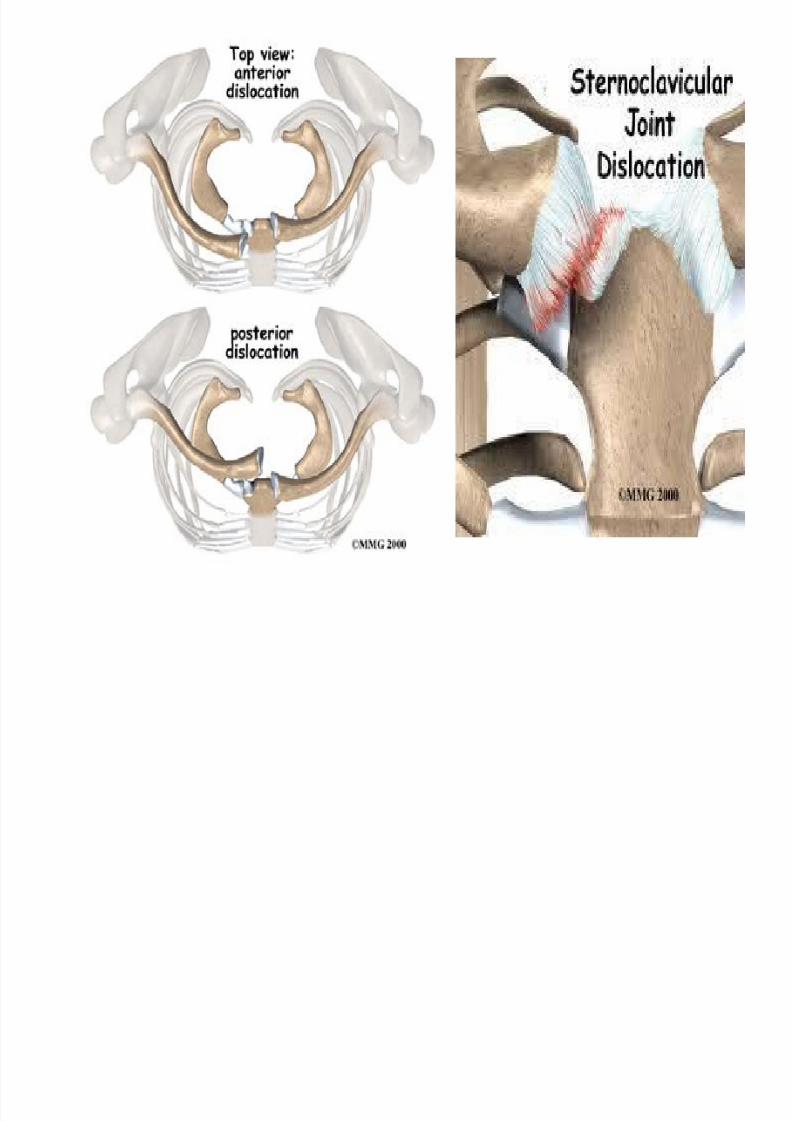
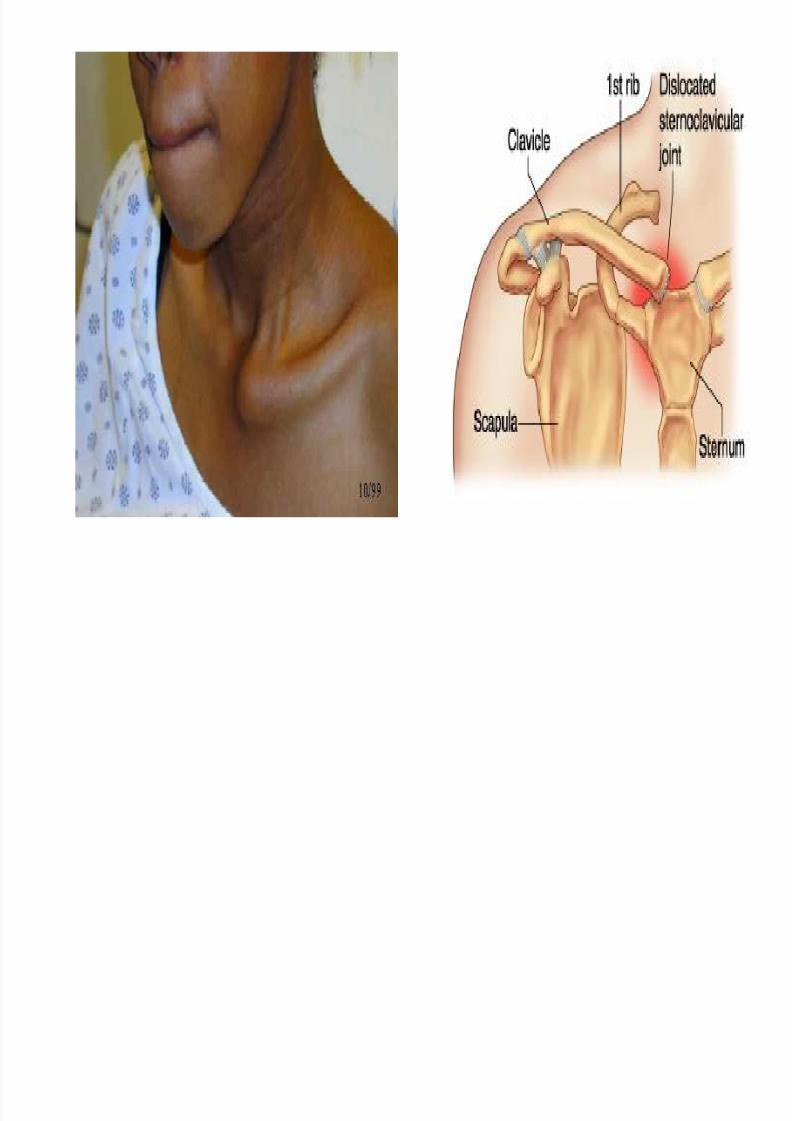
The typical injury at the medial end of the clavicle is an anterior or posterior dislocation of the sternoclavicular joint.
Importantly, a posterior dislocation of the clavicle may impinge on
the great vessels of the superior mediastinum and compress or
disrupt them.
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 37/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 38/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 39/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 40/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 41/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 42/49
SHOULDER TIP PAIN
Irritation of the diaphragm from any surrounding pathology
causes referred pain in the shoulder
This is so because the phrenic nerve and supraclavicular
nerves both arise from spinal segment C3,C4
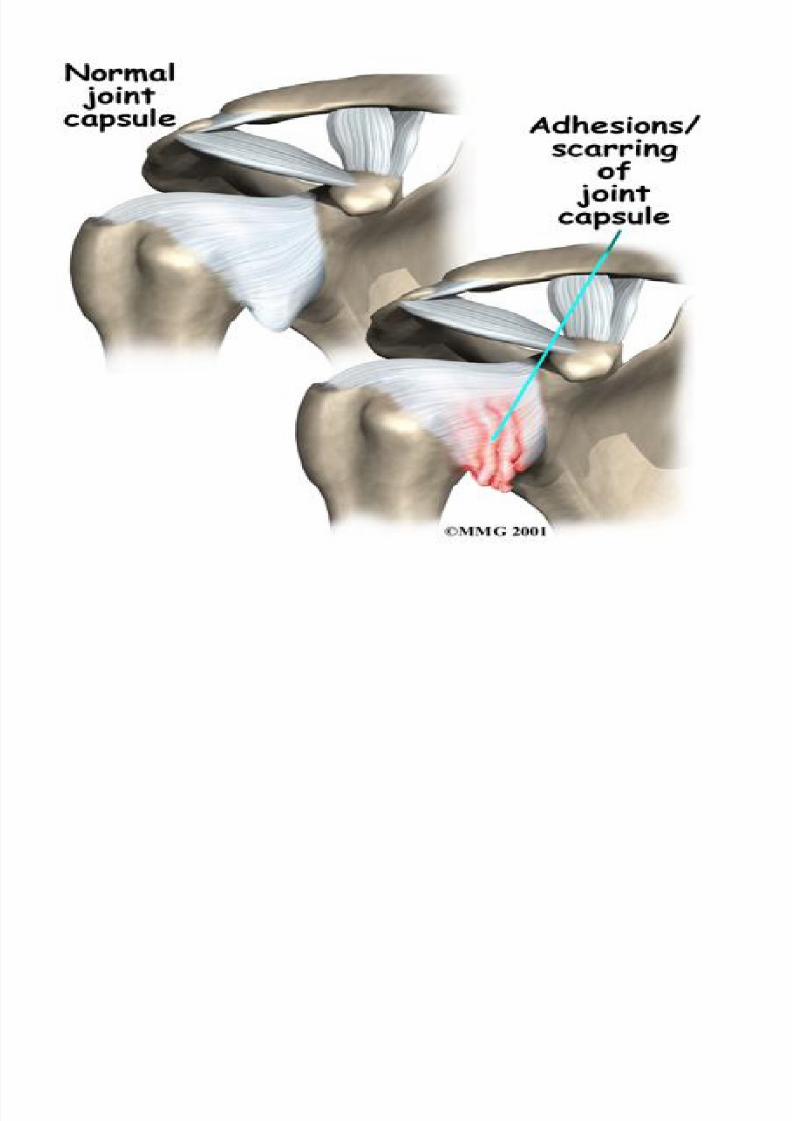
FROZEN SHOULDER / ADHESIVE CAPSULITIS Is a disorder in which capsule and CT surrounding the
glenohumeral joint becomes inflamed and stiff, and grows
together with abnormal bands of tissue, called adhesions,
greatly restricting motion and causing chronic pain
The patient may recover spontaneously in about 2 years
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 43/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 44/49
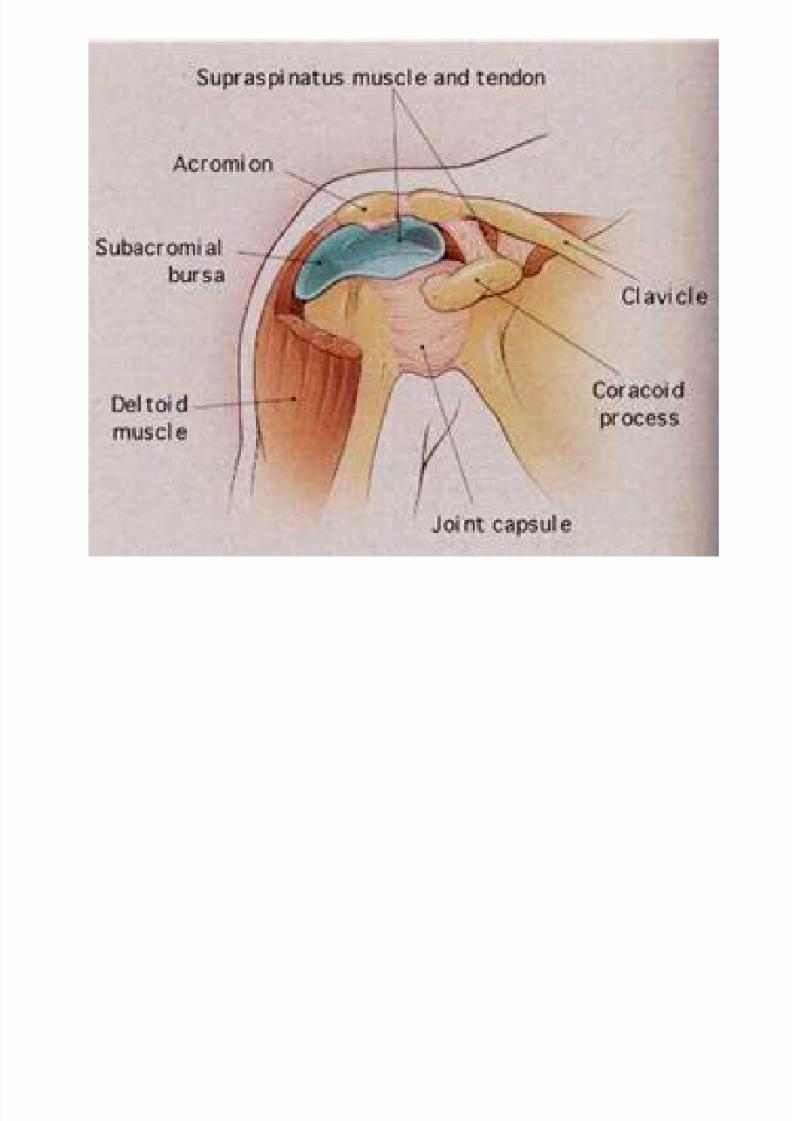
INFLAMMATION OF THE SUBACROMIAL
(SUBDELTOID) BURSA
Subacromial Bursa between supraspinatus and deltoid
muscles laterally and acromion medially
Supraspinatus tendinopathy
-this bursa may become inflamed, making movements of the
glenohumeral joint painful
Treated by injection of corticosteroid
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 45/49
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 46/49
CLINICAL CASE
A 35-year-old baseball pitcher came to the clinic with a historyof a recurrent dislocation of the shoulder. An MRI scan wasperformed to assess the shoulder joint prior to any treatment.
The MRI demonstrates the anatomical structures in multiple planes,
allowing the physician to obtain an overview of the shoulder and toassess any structures that may have been damaged and requiresurgical repair
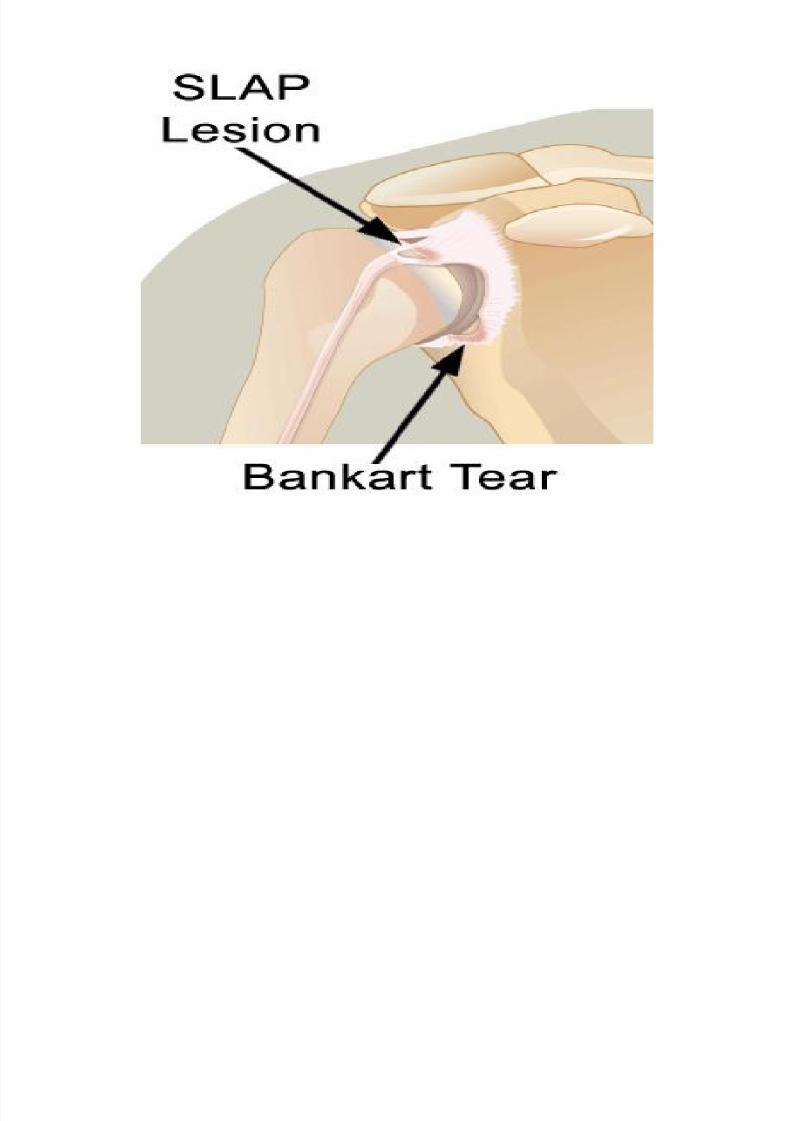
The MRI findings are typical for an anterior inferior dislocation
These injuries include the abutment of the posterior superior aspectof the humeral head on the anterior inferior aspect of the glenoidcavity
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 47/49
Continued…
• This type of injury (when recurrent) may avulse a small
fragment of the glenoid labrum and some cases this may attach
to a small fragment of bone (the Bankart lesion).
• When the shoulder is relocated, the intergrity of the capsular
atttachment antero-inferiorly has been disrupted and make it
more prone to dislocate
• An arthroscopic repair was performed
(is surgery that uses a tiny camera called an arthroscope to examine or
repair the tissues inside or around shoulder joint. The arthroscope is
inserted through a small incision (cut) in your skin)
7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 48/49

7/27/2019 2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01
http://slidepdf.com/reader/full/2-shoulderjointitsappliedanatomy-071-100602035807-phpapp01 49/49
Thank You!







![Stemcell 110417211605-phpapp01[2]](https://img.pdfslide.us/doc/110x75/557a2927d8b42a48458b4d70/stemcell-110417211605-phpapp012.jpg)




![2011spanishgrammarbook 111207201547-phpapp01[2]](https://img.pdfslide.us/doc/110x75/557e5ddbd8b42a506d8b4713/2011spanishgrammarbook-111207201547-phpapp012.jpg)