Embed Size (px)
Citation preview

2
Integrating Primary and Behavioral Health Care
Filipino American Cardiovascular Health Summit
July 9, 2011
Trina Dutta, MPP, MPHHHS/Substance Abuse and Mental Health Services
Administration
33
What does the data tell us?
•Of those young adults who had an STD in the past year•3.9% used both alcohol and illicit drugs, •3.1% were heavy drinkers (drank 5 or more drinks on the same occasion on 5 or more days in the past month), •2.1% used only alcohol but no illicit drugs,•2.1% used only illicit drugs but no alcohol, •1.3% did not use alcohol or illicit drugs•Cocaine use is associated with myocardial infarction, acute myocardial ischemia, arrhythmias, sudden death, and cardiomyopathy (all exacerbated by alcohol use)•Amphetamine use causes many of the same cardiac problems as cocaine•Cardiomyopathy and arrhythmias can be caused by alcohol abuse alone•Injection drug use leads to endocarditis (inflammation of the inside lining of the heart chambers and heart valves)•Hospitalizations for endocarditis relating to injection drug use increased by 38-66% in the US between 2001-2002 and 2002-2003.
44
What does the data tell us?
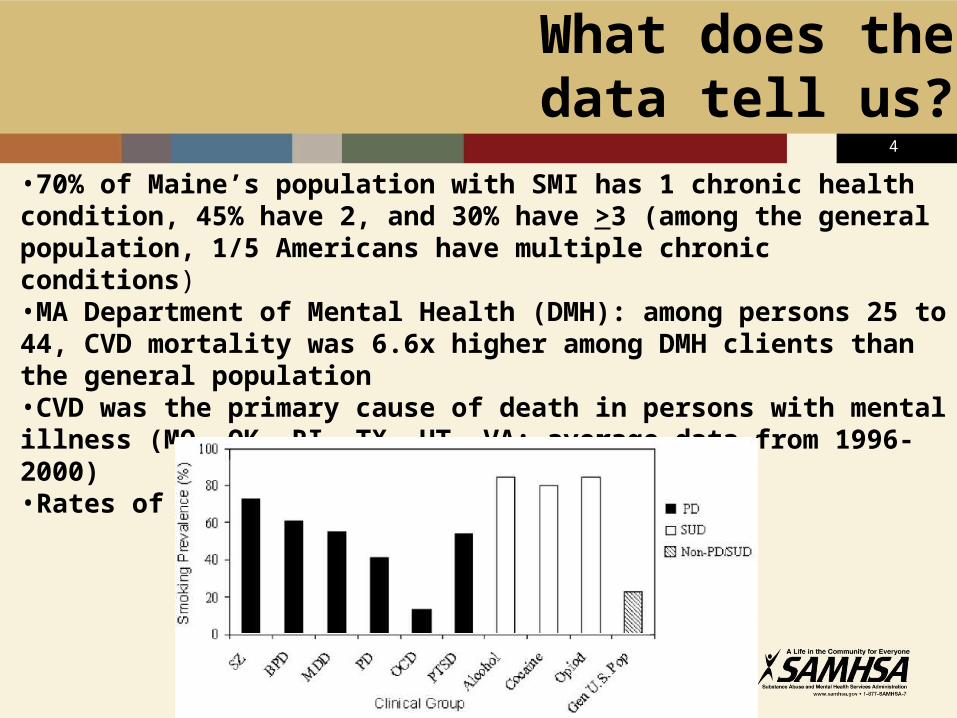
•70% of Maine’s population with SMI has 1 chronic health condition, 45% have 2, and 30% have >3 (among the general population, 1/5 Americans have multiple chronic conditions)•MA Department of Mental Health (DMH): among persons 25 to 44, CVD mortality was 6.6x higher among DMH clients than the general population•CVD was the primary cause of death in persons with mental illness (MO, OK, RI, TX, UT, VA: average data from 1996-2000)•Rates of smoking
55
What does the data tell us?
•Nearly 12M visits made to hospital EDs in 2007 involved people with a mental disorder, substance abuse problem, or both (accounts for 1/8 of the 95M visits to EDs by adults in 2007)•Of these visits, 2/3 involved those with a mental disorder, 1/4 was for those with a substance abuse problem, and the rest involved those dealing with both •Of the 12M ED visits:•Depression and other mood disorders accounted for 43% of the visits; 26% were for anxiety disorders; 23% involved alcohol-related problems•Mental health and/or substance abuse-related visits were 2½ times more likely to result in hospital admission than visits not involving these•41% of mental disorder and/or substance abuse-related visits resulted in hospitalization•Medicare was billed for 30% of all mental health and/or substance abuse emergency department visits; private insurance was billed for 26%; the uninsured for 21%; and Medicaid for 20%
66
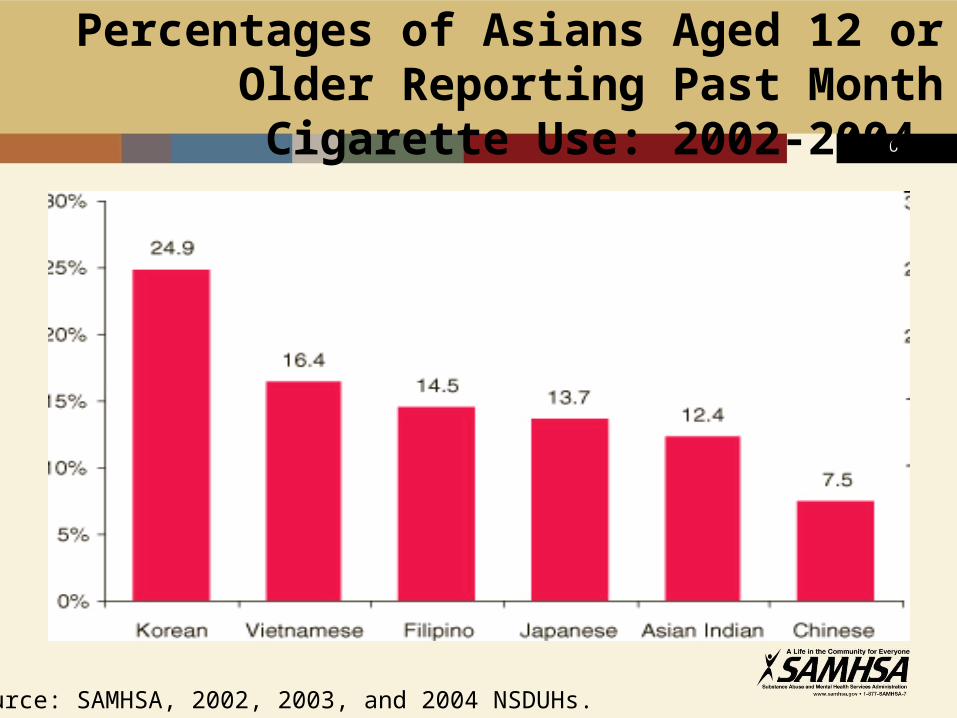
Percentages of Asians Aged 12 or Older Reporting Past Month
Cigarette Use: 2002-2004
Source: SAMHSA, 2002, 2003, and 2004 NSDUHs.
77
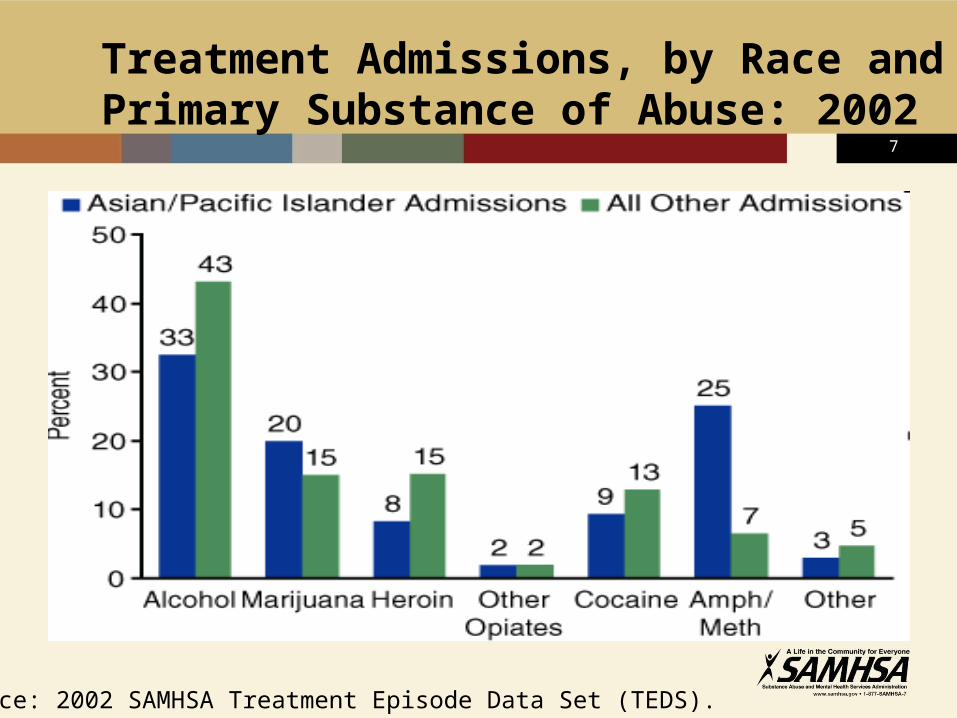
Treatment Admissions, by Race and Primary Substance of Abuse: 2002
Source: 2002 SAMHSA Treatment Episode Data Set (TEDS).
88
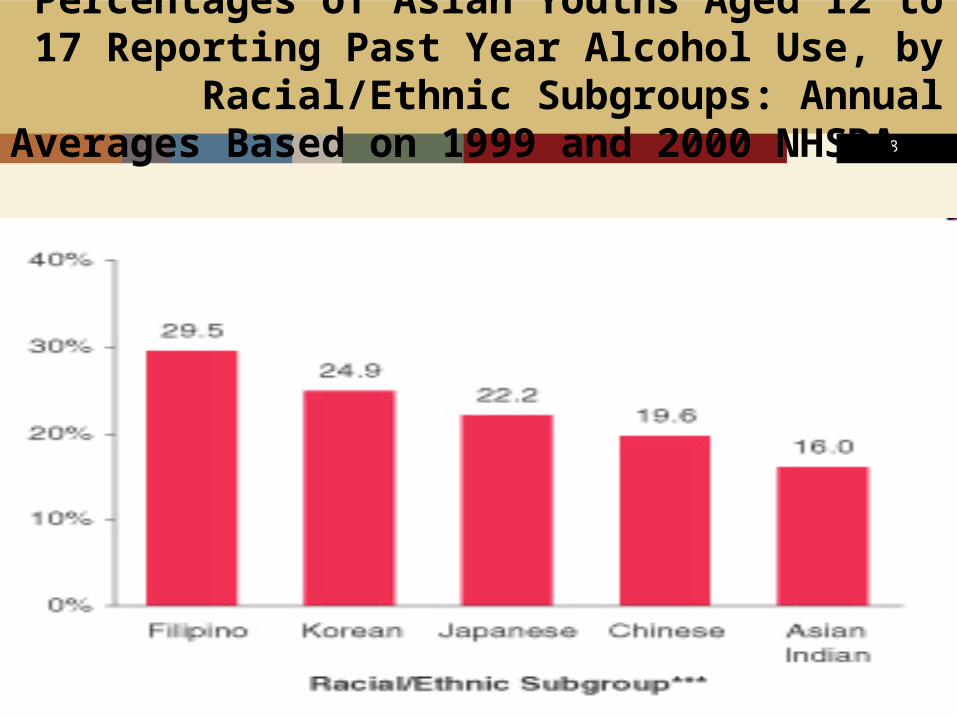
Percentages of Asian Youths Aged 12 to 17 Reporting Past Year Alcohol Use, by
Racial/Ethnic Subgroups: Annual Averages Based on 1999 and 2000
NHSDAs
99
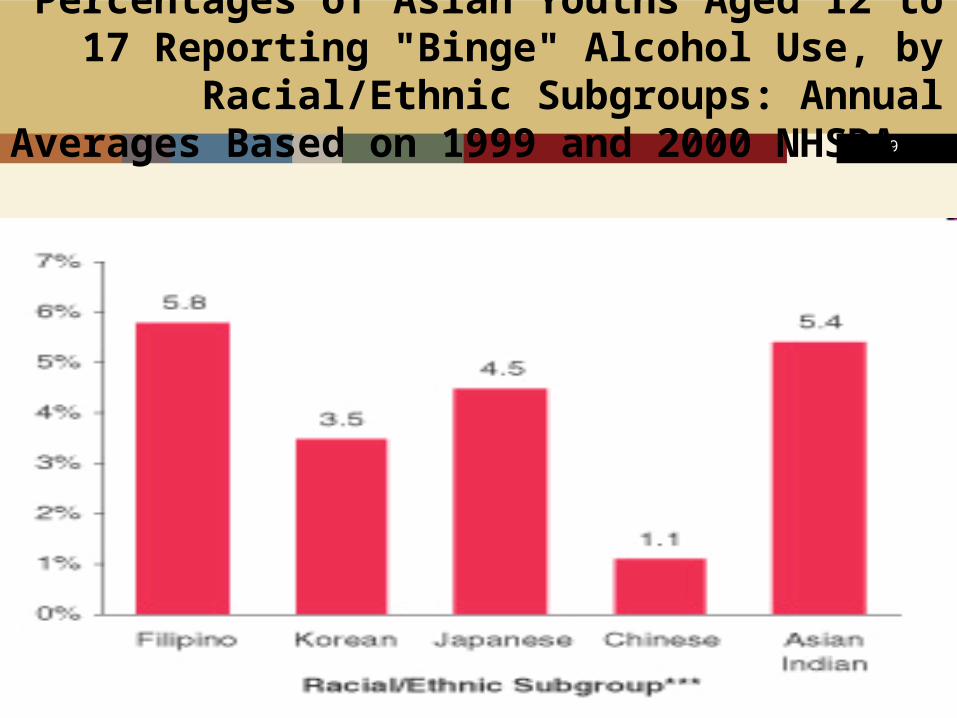
Percentages of Asian Youths Aged 12 to 17 Reporting "Binge" Alcohol Use, by
Racial/Ethnic Subgroups: Annual Averages Based on 1999 and 2000
NHSDAs
1010
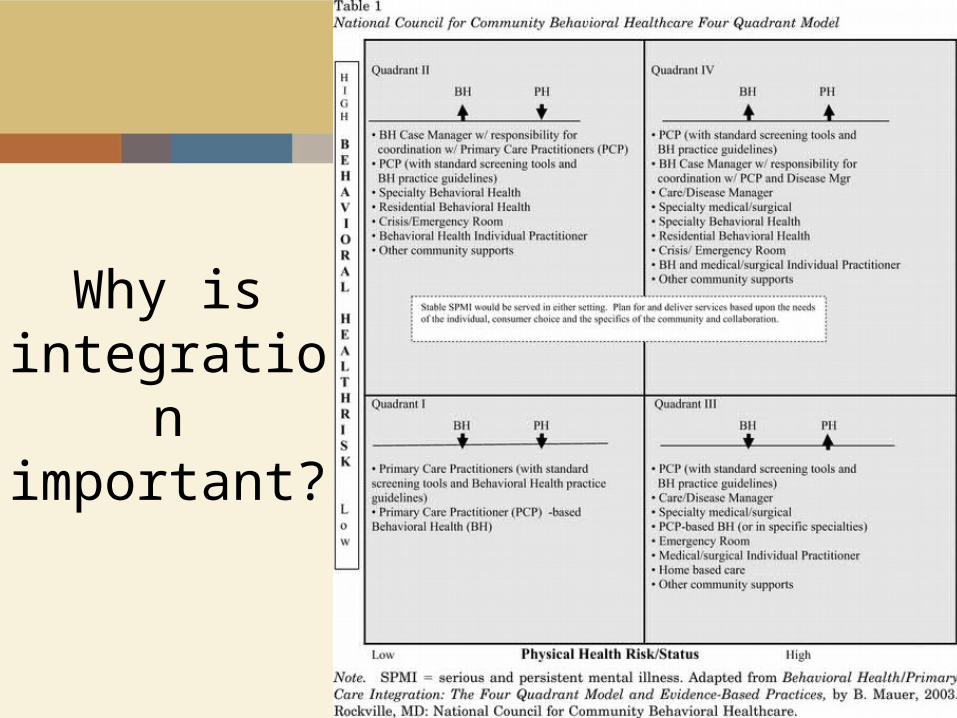
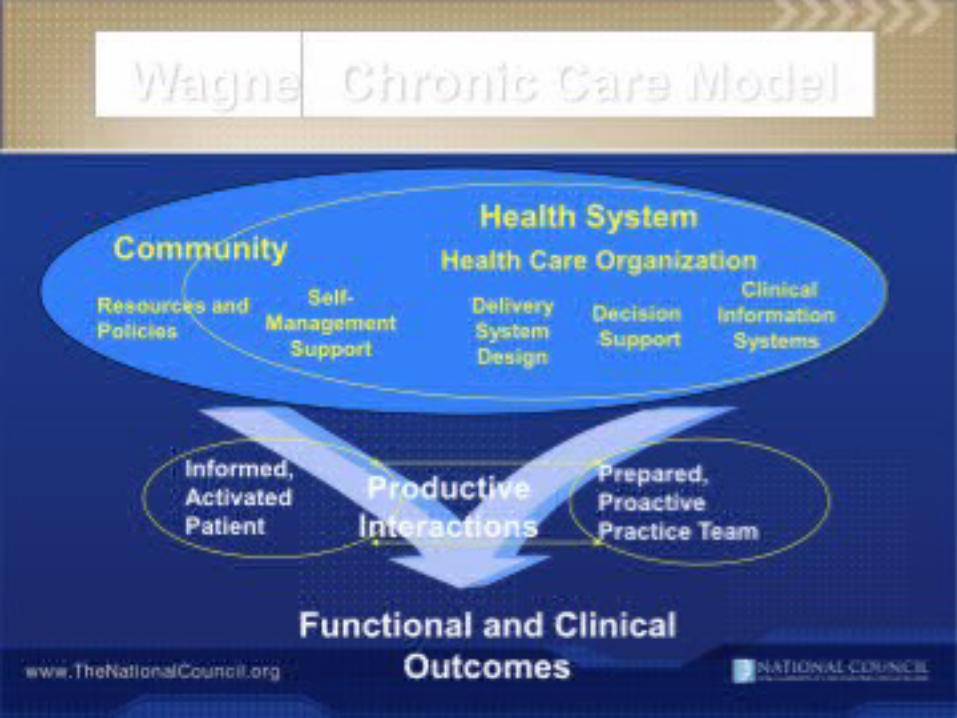
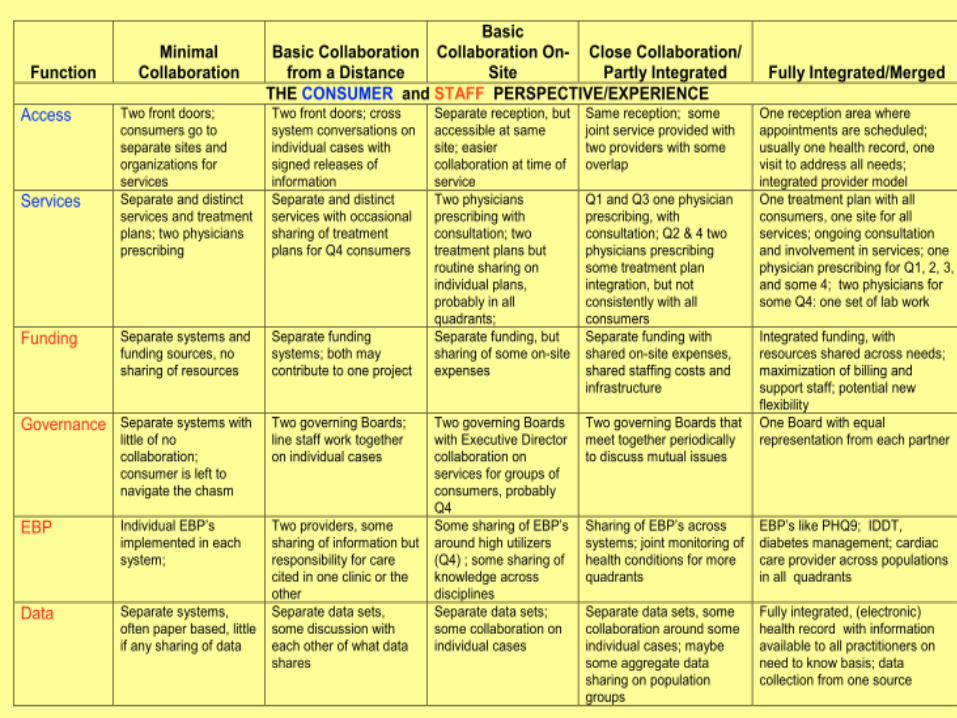
Why is integration important?
1111
1212
1313
Technical Assistance Center: SAMHSA/HRSA Center for
Integrated Health Solutions (CIHS)In partnership with HHS/Health Resources and
Services Administration (HRSA)
• Goal: To promote the planning and development of integrated primary and behavioral health care for those with SMI, addiction disorders and/or individuals with SMI and a co-occurring substance use disorder, whether seen in specialty mental health or primary care safety net provider settings across the country
• Purpose: – To serve as a national training and technical assistance
center on the bidirectional integration of primary and behavioral health care and related workforce development
www.centerforintegratedhealthsolutions.org

1414
1515
Affordable Care Act, Section 2703
“State Option to Provide Health Homes for Enrollees with Chronic Conditions”*
Goal: enhanced integration and coordination of primary, acute, behavioral health (mental health and substance use), and long-term services and supports for persons across the lifespan with chronic illness
The health home provision provides an opportunity to build a person-centered system of care that achieves improved outcomes for beneficiaries and better services and value for State Medicaid programs
*Led by Centers for Medicaid and Medicare (CMS), in partnership with SAMHSA, ASPE, HRSA, and AHRQ
1616
Affordable Care Act, Section 2703
Population Served• Eligible individuals are those with chronic
conditions, meaning an individual who is eligible for medical assistance under the State plan or under a waiver of such plan and has at least– 2 chronic conditions; or– 1 chronic condition and is at risk of having a second chronic
condition; or– 1 serious and persistent mental health condition
• Chronic conditions must include:– A mental health condition– A substance use disorder– Asthma– Diabetes– Heart disease– Being overweight, as evidenced by having a BMI >25
1717
Required Services
• Comprehensive care management;• Care coordination and health promotion;• Comprehensive transitional care, including
appropriate follow-up, from inpatient to other settings;
• Patient and family support (including authorized representatives);
• Referral to community and social support services, if relevant; and
• Use of health information technology to link services, as feasible and appropriate.
Affordable Care Act, Section 2703
1818
1919
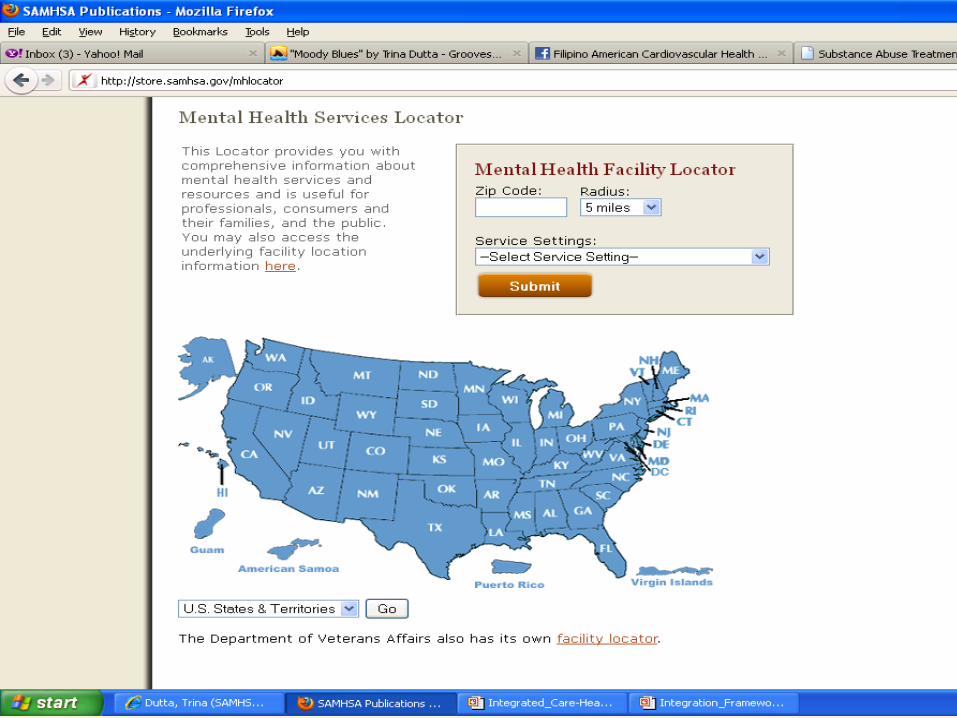
Substance Abuse Treatment Facility Locator
• Services Provided:– Substance abuse treatment– DetoxificationMethadone maintenance (facility may also use
buprenorphine in maintenance)– Methadone detoxification (facility may also use buprenorphine in
detoxification)– Halfway house– Buprenorphine services
• Type of Care:– Outpatient– Partial hospitalization/Day treatment– Residential short-term treatment (30 days or less)– Residential long-term treatment (more than 30 days)– Hospital inpatient
• Special Language Services:– ASL or other assistance for hearing impaired– American Indian and Alaska Native languages– Spanish– Foreign languages other than Spanish
2020
• Special Programs/Groups:– Adolescents– Persons with co-occurring mental and substance abuse disorders– Persons with HIV/AIDS– Gays and lesbians– Seniors/older adults– Pregnant/postpartum women– Women/Men– Residential beds for clients' children– DUI/DWI offenders– Criminal justice clients
• Forms of Payment Accepted:(NOTE: Check with facility for details. Applicability varies according to individual circumstances.)
– Medicaid– State financed insurance (other than Medicaid)– Medicare– Private health insurance– Military insurance (e.g., VA, TRICARE)– Self payment– Access to Recovery (ATR) voucher
• Payment Assistance:(NOTE: Check with facility for details. Applicability varies according to individual circumstances.)
– Sliding fee scale (fee based on income and other factors.)– Payment assistance (Check with facility for details)
Substance Abuse Treatment Facility Locator
2121
2222