Embed Size (px)
Citation preview
Rickets
Zulf Mughal
Consultant in Paediatric Bone Disorders
Department of Paediatric Endocriology
Royal Manchester Children's Hospital
Manchester
M13 0JH
Bone Study Day, 28th September 2012

Overview
� What is Rickets?
� Vitamin D Deficiency Rickets
� Calcium Deficiency Rickets
� Vitamin D Dependent Rickets type I & type II
� X-Linked Hypophosphataemic Rickets
What is Rickets ?
Rickets – Historical Perspective
Francis Glisson - "De Rachitide” 1650
� 19th CENTURY - Rickets rampant among the poor children living in the industrialised & polluted northern cities
� “Disappearance of Rickets” in early 20th
Century:� Cod-liver oil supplements in 1930s
� Improvement in nutrition
� Pollution control measures
� Recent resurgence of Rickets
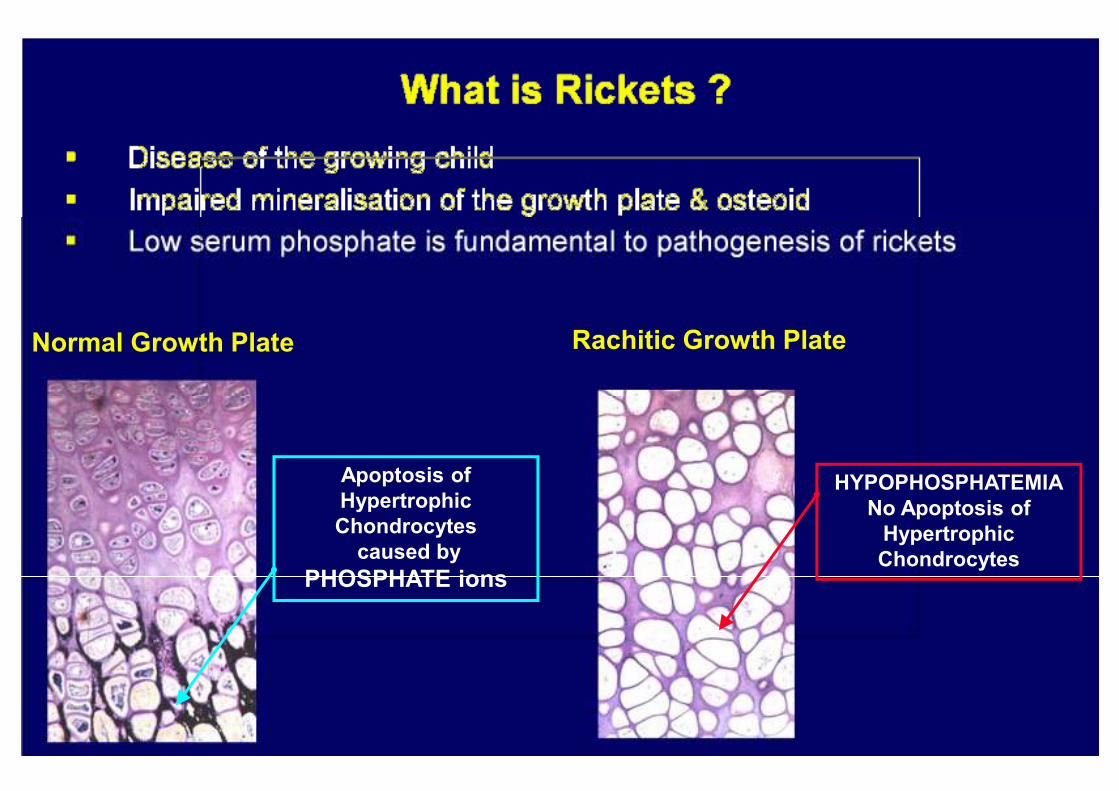
Normal Growth Plate Rachitic Growth Plate
Apoptosis of
Hypertrophic
Chondrocytes
caused by
PHOSPHATE ions
HYPOPHOSPHATEMIA
No Apoptosis of
Hypertrophic
Chondrocytes

What is Rickets ?
Impaired Apoptosis of Terminally Differentiated Chondrocytes in the Growth Plate
Responsible for Clinical & Radiological Signs of Rickets
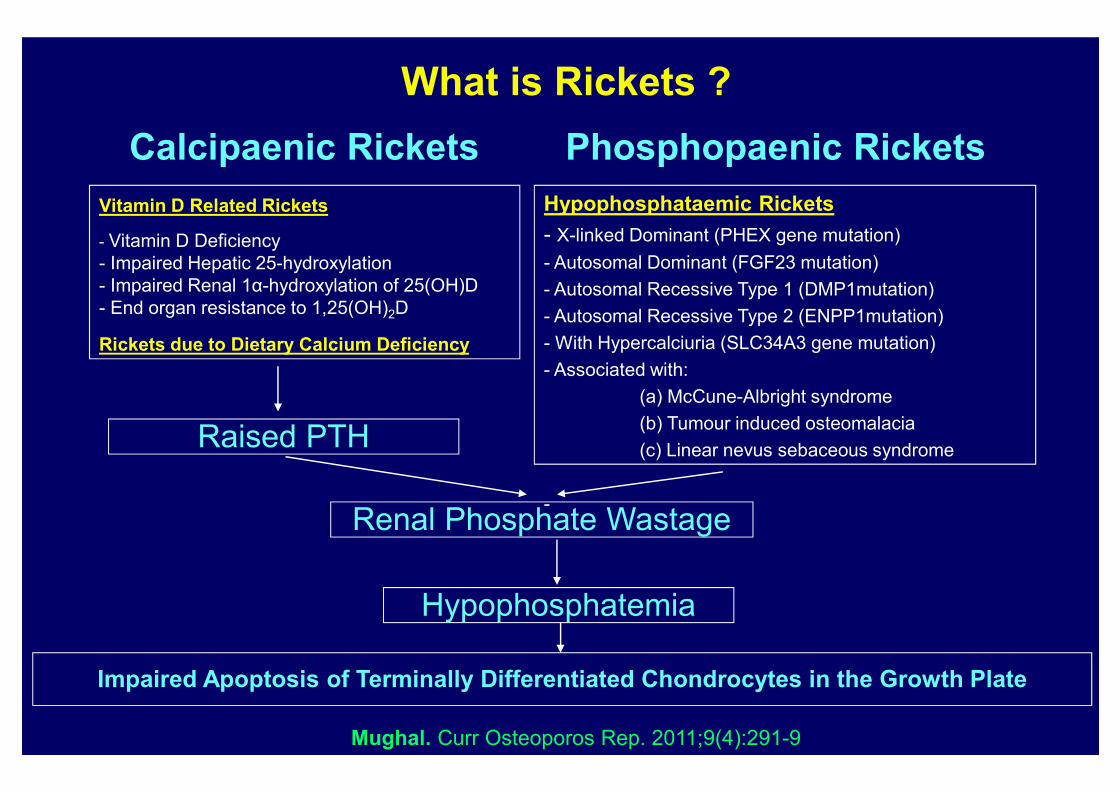
What is Rickets ?
Vitamin D Related Rickets
- Vitamin D Deficiency
- Impaired Hepatic 25-hydroxylation
- Impaired Renal 1α-hydroxylation of 25(OH)D
- End organ resistance to 1,25(OH)2D
Rickets due to Dietary Calcium Deficiency
Calcipaenic Rickets Phosphopaenic Rickets
Hypophosphataemic Rickets
- X-linked Dominant (PHEX gene mutation)
- Autosomal Dominant (FGF23 mutation)
- Autosomal Recessive Type 1 (DMP1mutation)
- Autosomal Recessive Type 2 (ENPP1mutation)
- With Hypercalciuria (SLC34A3 gene mutation)
- Associated with:
(a) McCune-Albright syndrome
(b) Tumour induced osteomalacia
(c) Linear nevus sebaceous syndrome
-
Raised PTH
Renal Phosphate Wastage
Hypophosphatemia
Impaired Apoptosis of Terminally Differentiated Chondrocytes in the Growth Plate
Mughal. Curr Osteoporos Rep. 2011;9(4):291-9
Calcipaenic Rickets
Vitamin D Related Rickets
� Vitamin D Deficiency Rickets
� Impaired Hepatic 25-hydroxylation
� Vitamin D Dependent Rickets Type I (Impaired Renal
1α-hydroxylation of 25(OH)D)
� Vitamin D Dependent Rickets Type II (End organ resistance to
1,25(OH)2D)
Rickets due to Dietary Calcium Deficiency
Vitamin D Deficiency Rickets
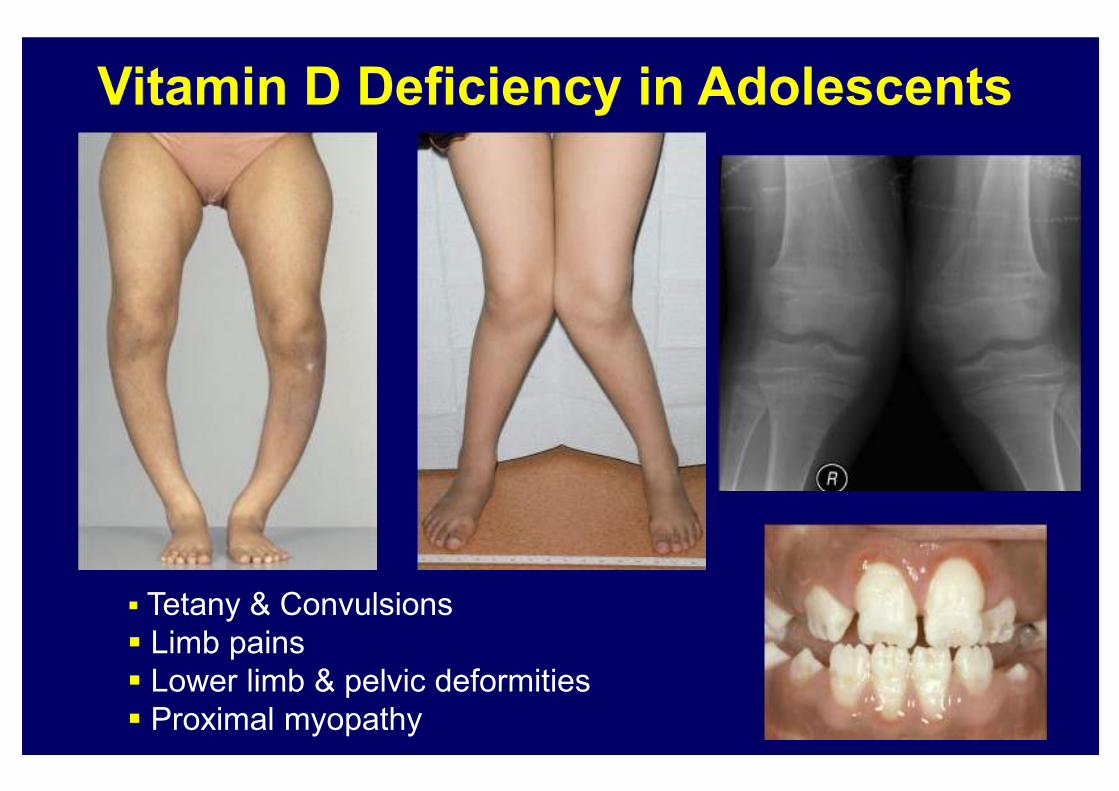
Vitamin D Deficiency in Adolescents
� Tetany & Convulsions
� Limb pains
� Lower limb & pelvic deformities
� Proximal myopathy
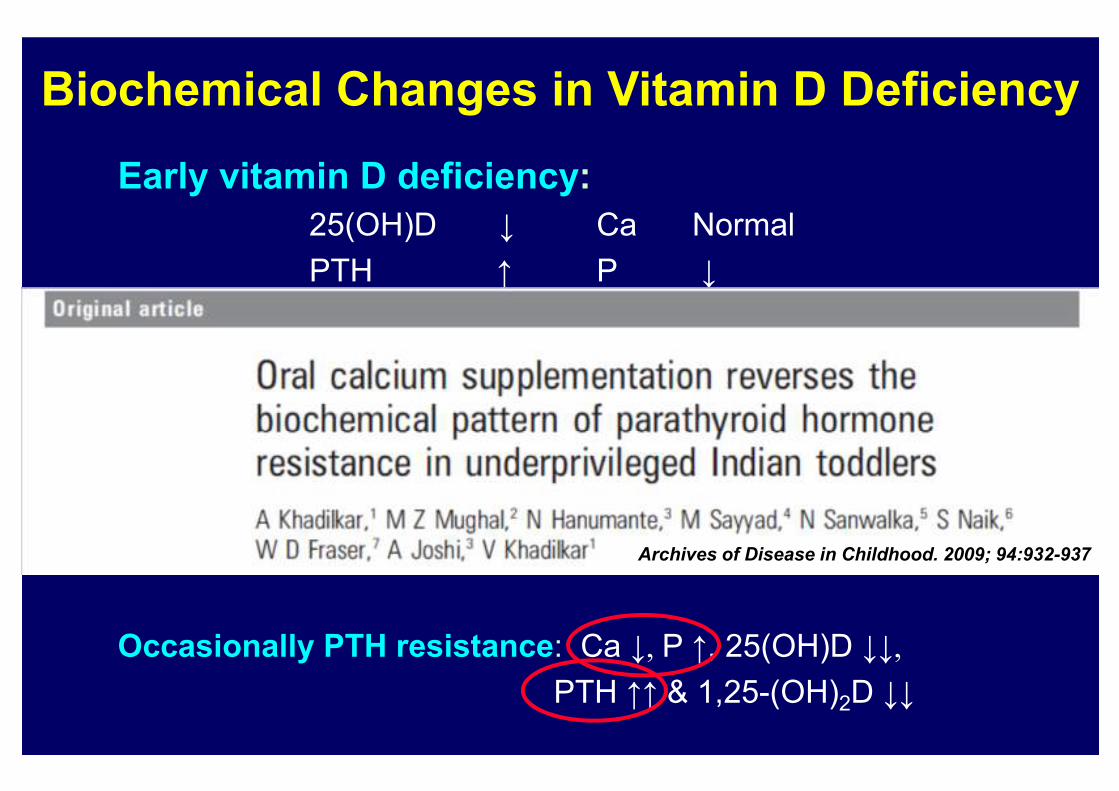
Biochemical Changes in Vitamin D Deficiency
Early vitamin D deficiency:
25(OH)D Ca Normal
PTH ↑ P
1,25(OH)2D ↑ ALP ↑
Severe vitamin D deficiency:
25(OH)D Ca
PTH ↑ ↑ P
1,25-(OH)2D ALP ↑ ↑
Occasionally PTH resistance: Ca P ↑, 25(OH)D
PTH ↑↑ & 1,25-(OH)2D
Archives of Disease in Childhood. 2009; 94:932-937
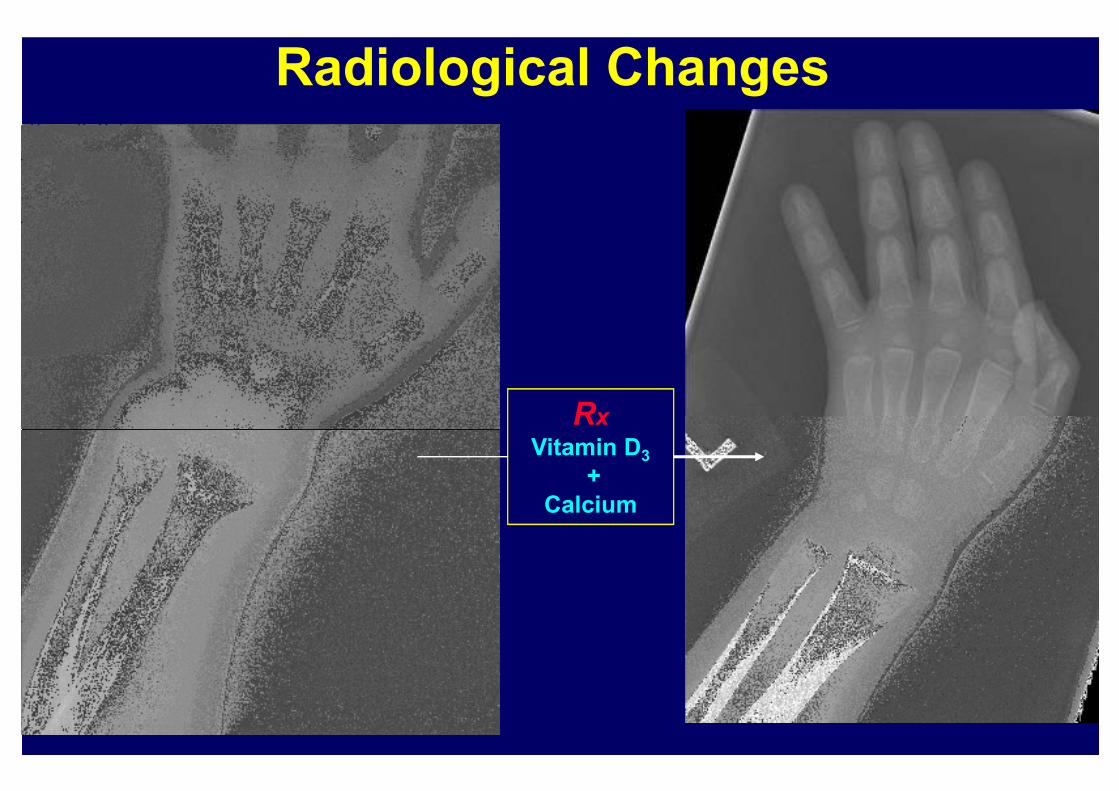
Radiological Changes
Rx
Vitamin D3
+
Calcium
Treatment of Vitamin D Deficiency Rickets
� Oral vitamin D2 or D3, 3000 - 6000 i.u./day for 6 to 8 weeks
� Oral calcium supplements if necessary
� Monitoring:
� Improvement in symptoms (~ 2weeks)
� ↓ in serum PTH & alkaline phosphatase
� ↑ in serum phosphate, calcium & 25(OH)vitamin D
� Radiological healing (~ 3 months)
� Improvement of bow legs or knock-knees (~ 2 years)
� Provide vitamin D supplements (~ 400 iu/day) after the rickets
has healed
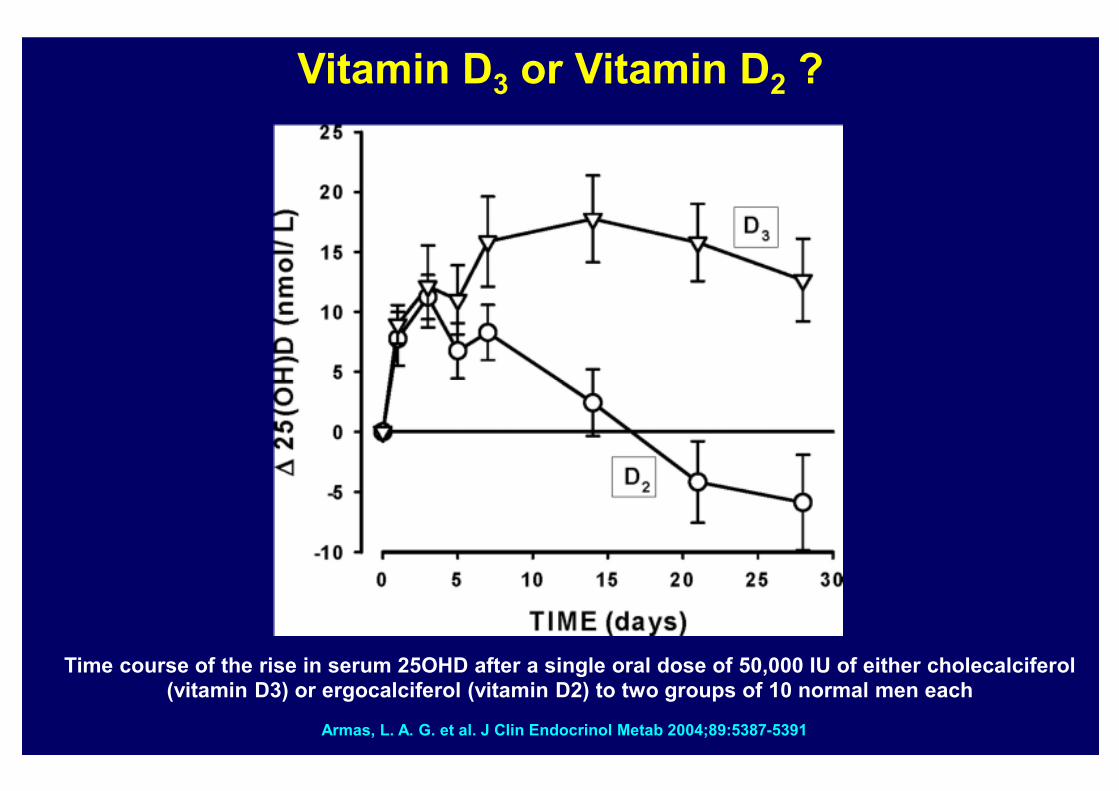
Armas, L. A. G. et al. J Clin Endocrinol Metab 2004;89:5387-5391
Time course of the rise in serum 25OHD after a single oral dose of 50,000 IU of either cholecalciferol (vitamin D3) or ergocalciferol (vitamin D2) to two groups of 10 normal men each
Vitamin D3 or Vitamin D2 ?
Prevention of Vitamin D Deficiency
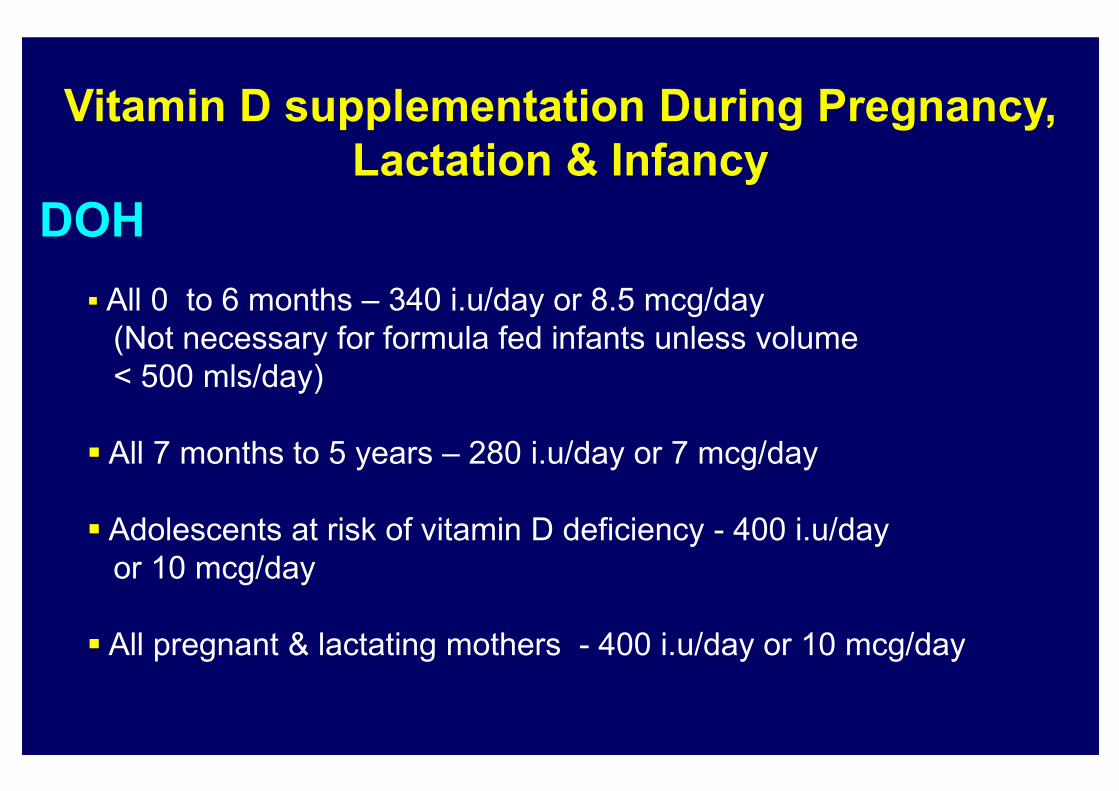
Vitamin D supplementation During Pregnancy,
Lactation & Infancy
DOH
� All 0 to 6 months – 340 i.u/day or 8.5 mcg/day
(Not necessary for formula fed infants unless volume
< 500 mls/day)
� All 7 months to 5 years – 280 i.u/day or 7 mcg/day
� Adolescents at risk of vitamin D deficiency - 400 i.u/day
or 10 mcg/day
� All pregnant & lactating mothers - 400 i.u/day or 10 mcg/day
(www.healthystart.nhs.uk)
Children’s Healthy Start Vitamin drops
contain (5 drops daily):
• 233 micrograms of vitamin A
• 20 milligrams of vitamin C
• 7.5 micrograms of vitamin D3
Calcium Deficiency Rickets
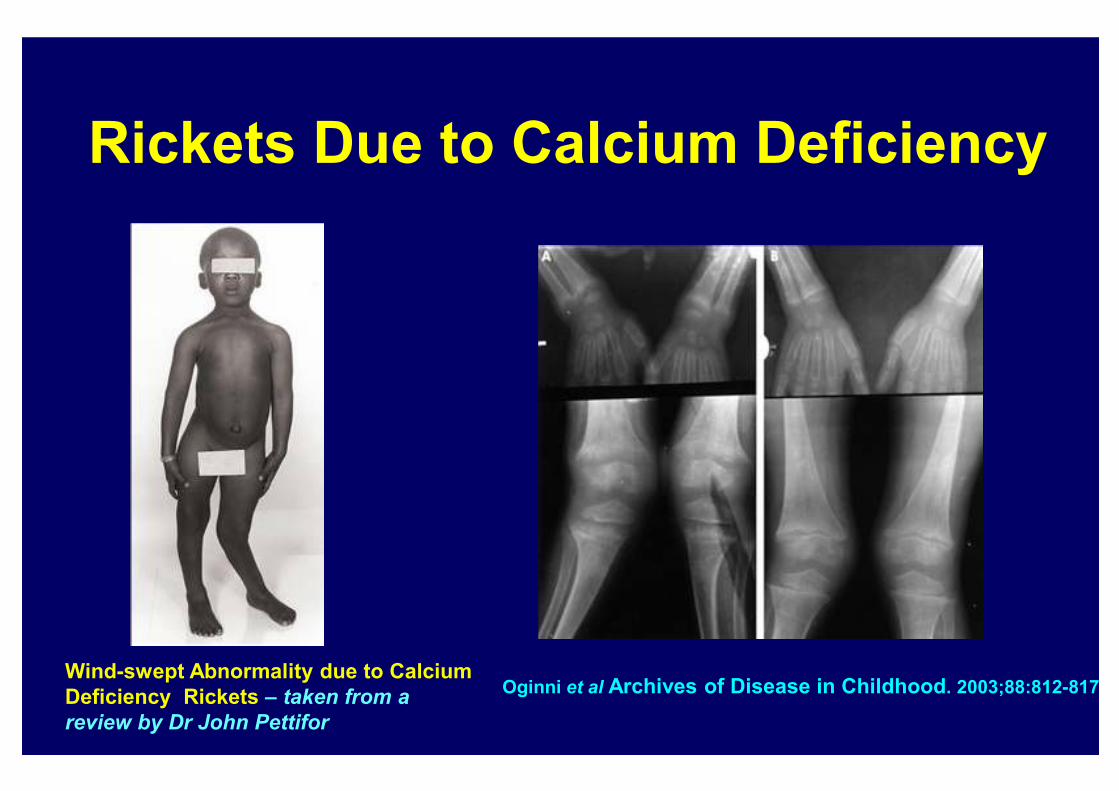
Rickets Due to Calcium Deficiency
Wind-swept Abnormality due to Calcium
Deficiency Rickets – taken from a
review by Dr John Pettifor
Oginni et al Archives of Disease in Childhood. 2003;88:812-817
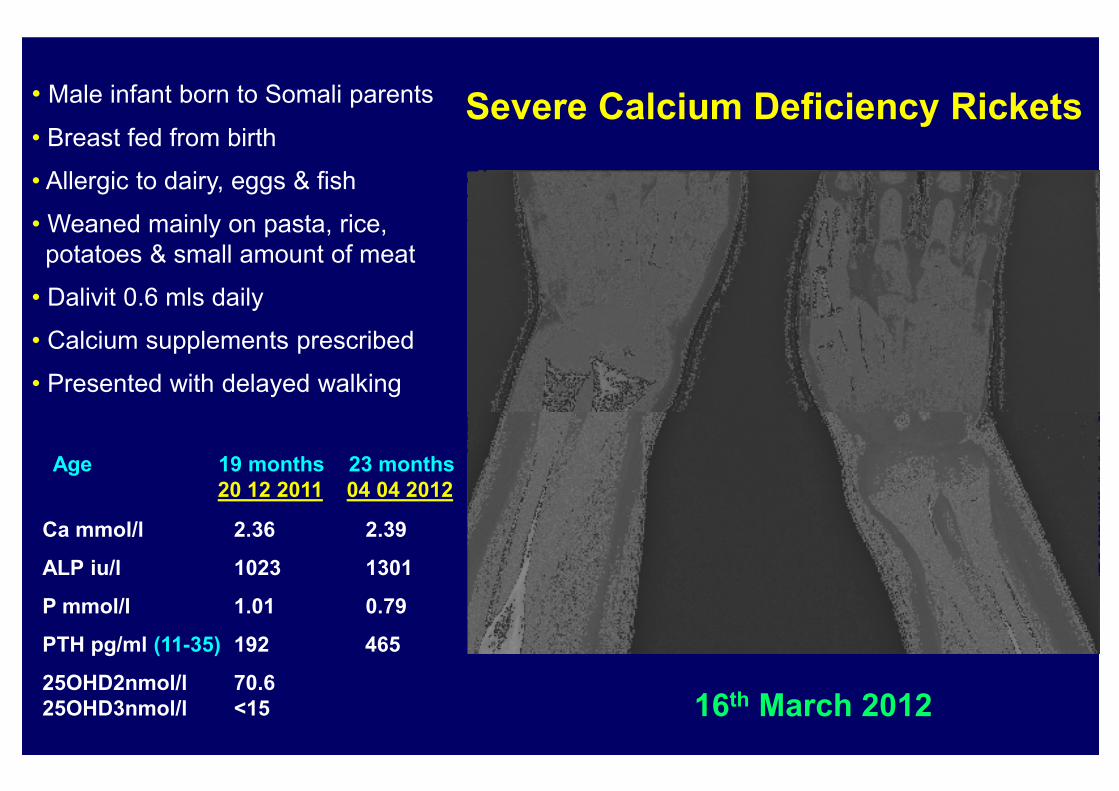
Severe Calcium Deficiency Rickets
16th March 2012
Age 19 months 23 months
20 12 2011 04 04 2012
Ca mmol/l 2.36 2.39
ALP iu/l 1023 1301
P mmol/l 1.01 0.79
PTH pg/ml (11-35) 192 465
25OHD2nmol/l 70.6
25OHD3nmol/l <15
• Male infant born to Somali parents
• Breast fed from birth
• Allergic to dairy, eggs & fish
• Weaned mainly on pasta, rice,
potatoes & small amount of meat
• Dalivit 0.6 mls daily
• Calcium supplements prescribed
• Presented with delayed walking
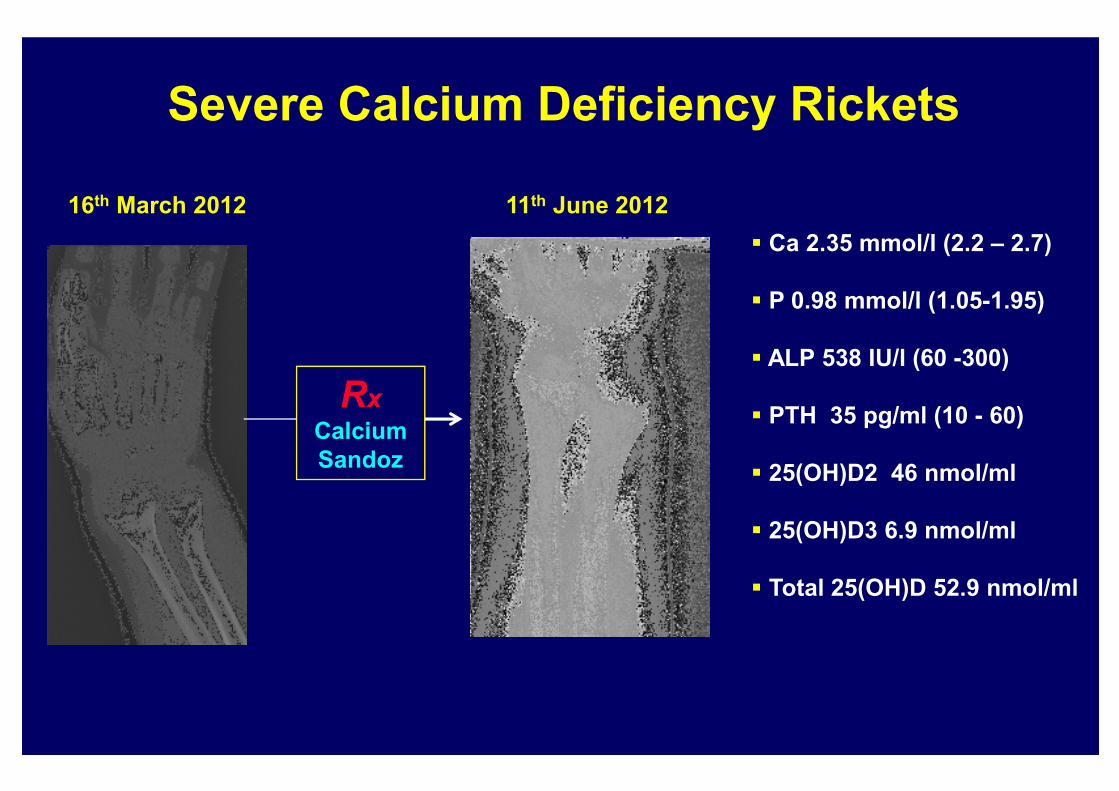
Severe Calcium Deficiency Rickets
16th March 2012 11th June 2012
� Ca 2.35 mmol/l (2.2 – 2.7)
� P 0.98 mmol/l (1.05-1.95)
� ALP 538 IU/l (60 -300)
� PTH 35 pg/ml (10 - 60)
� 25(OH)D2 46 nmol/ml
� 25(OH)D3 6.9 nmol/ml
� Total 25(OH)D 52.9 nmol/ml
Rx
Calcium
Sandoz
Vitamin D Dependent Rickets (VDDR)
Type I & Type II
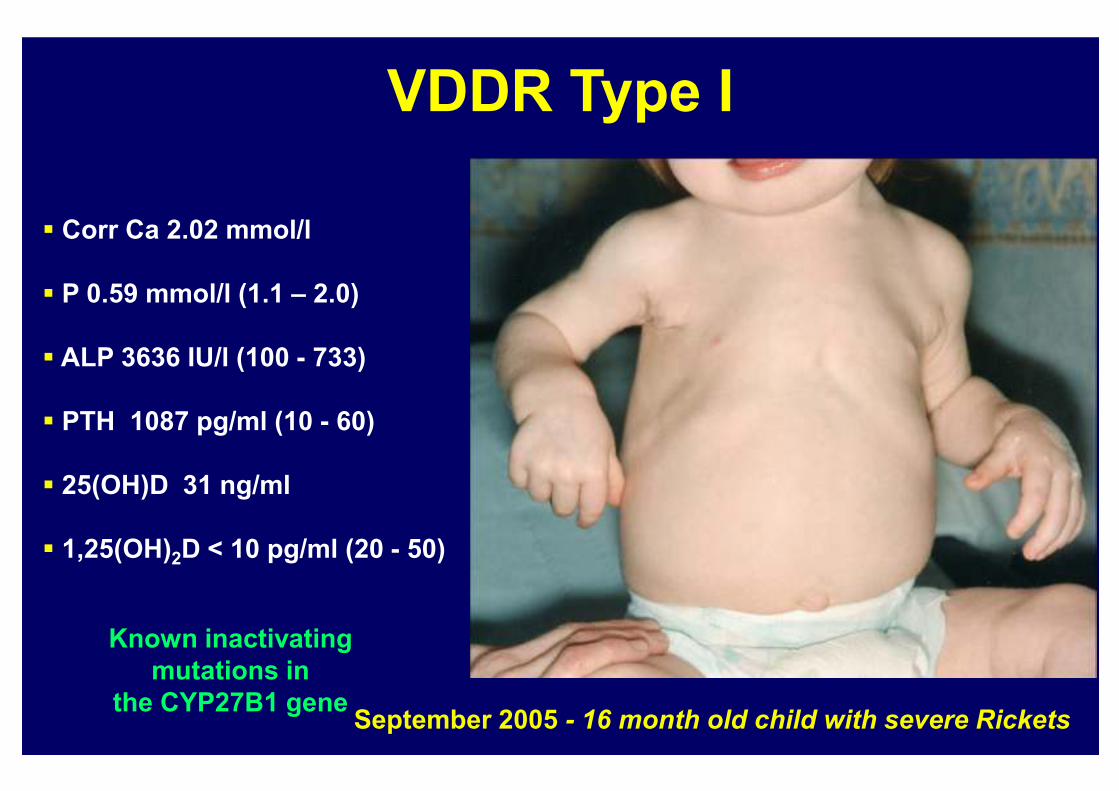
VDDR Type I
� Corr Ca 2.02 mmol/l
� P 0.59 mmol/l (1.1 – 2.0)
� ALP 3636 IU/l (100 - 733)
� PTH 1087 pg/ml (10 - 60)
� 25(OH)D 31 ng/ml
� 1,25(OH)2D < 10 pg/ml (20 - 50)
September 2005 - 16 month old child with severe Rickets
Known inactivating
mutations in
the CYP27B1 gene
Vitamin D Dependent Rickets Type I & Type II
VDDR Type I
� Physiological doses of calcitriol (1,25(OH)2D) or alphacalcidiol
VDDR Type II
� Pharmacological doses of calcitriol or alphacalcidiol
(e.g. 3-6 mcg/day)
+
Oral calcium – 2 to 3 grams/day
� Long-term treatment calcium infusions (especially patients
with alopecia )