Embed Size (px)
Citation preview

1 | P a g e
ظظظ/
-2
-Dana Alrafaiah
-Amani Nofal
- MousaAlabbadi

2 | P a g e
• You don’t need to go back to slide from 34-77 to any info. Only check the
clinical picture .
From the last lecture, adenomas can be functional or non- functional
The old literature: nonfunctioning adenomas are more common but
recent studies are finding more gonadotroph adenomas and old
nonfunctional ones are now mostly FSH/LH containing adenomas.
For exam purposes, the answer depends on old literature.
Thyroid gland
Revision:
Thyroid gland is composed of a right lobe, a left lobe and an isthmus in-
between with 4 parathyroid glands located on its posterior aspect.
Feedback inhibition loop:
Increased serum levels of T3 and T4 will have negative feedback effect
on both the pituitary gland and the hypothalamus; it will inhibit the
release of TSH from the anterior pituitary and TRH from the
hypothalamus.
Thyroid disorders
Thyroid diseases are very common, and like other endocrine glands
there’s hyper and hypofunction- hyperthyroidism and hypothyroidism.

3 | P a g e
Inflammation “Thyroiditis” also occurs leading to the destruction of the
gland and has types that are autoimmune(majority) and others.
Enlargements are mostly Euthyroid; not associated with hyper or
hypothyroidism (T3 and T4 levels are normal). An example is Diffuse and
Multinodular Goiter “MNG” which is the most common disease of the
thyroid gland and will be further discussed as we proceed.
Neoplasms of the thyroid are relatively common. Recall that there are
functional adenomas and non-functional adenomas, when discussing the
thyroid gland the nonfunctional adenomas are the most common type.
This is at least according to older literature from 10-15 years ago,
recently more sensitive tests that depend on transcriptional factors and
other molecules say gonadotrophic adenomas are more common now.
HYPERTHYRODISIM/THYROTOXICOSIS
Endocrine pathology is associated with biochemical changes that can be
observed in the serum. Hyperthyroidism is hyper function of the thyroid
gland leading to increased T3 and T4 levels and decreased TSH( negative
feedback inhibition) . TSH serum levels is the most sensitive test that
indicates hyperthyroidism. Hyperthyroidism with increased levels of TSH
is an indication of a TSH producing pituitary adenoma.(In this case only )
Signs and symptoms:
Palpitations, tachycardia,nervousness, impaired fertility, weight loss
despite eating a lot, heat intolerance (the opposite happens in
hypothyroidism) and other signs and symptoms all over the body; GI
tract, mood swings and the menstrual cycle etc.
4 | P a g e
(
High TSH)
After a complete thyroidectomy, Hormone
Replacement Therapy (HRT) should be administered
to maintain normal thyroid function in its absence. A
dose of 30 or 50 mg of thyroxin is given and
monitored to make sure no abnormalities occur.
However, if the levels increase abnormally leading to
hyperthyroidism we call this condition factitious
thyrotoxicosis.
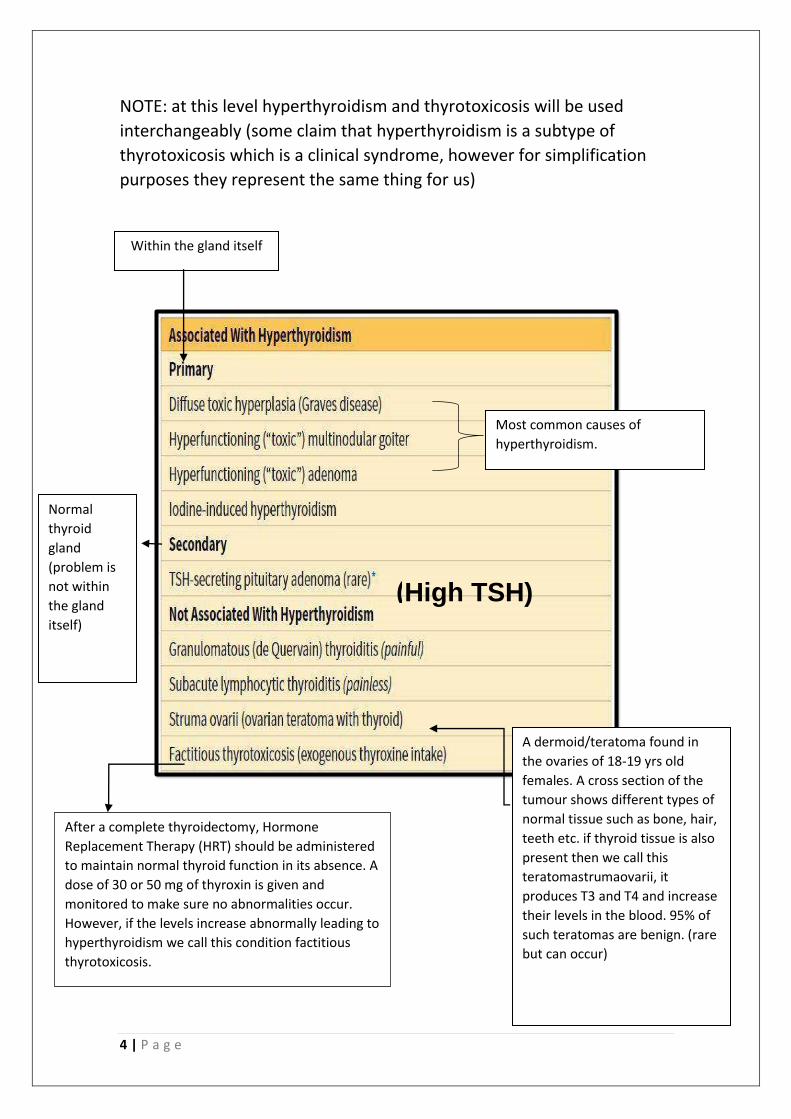
NOTE: at this level hyperthyroidism and thyrotoxicosis will be used
interchangeably (some claim that hyperthyroidism is a subtype of
thyrotoxicosis which is a clinical syndrome, however for simplification
purposes they represent the same thing for us)
Within the gland itself
Most common causes of
hyperthyroidism.
Normal
thyroid
gland
(problem is
not within
the gland
itself)
A dermoid/teratoma found in
the ovaries of 18-19 yrs old
females. A cross section of the
tumour shows different types of
normal tissue such as bone, hair,
teeth etc. if thyroid tissue is also
present then we call this
teratomastrumaovarii, it
produces T3 and T4 and increase
their levels in the blood. 95% of
such teratomas are benign. (rare
but can occur)

5 | P a g e
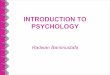
This diagram illustrates the needed work up to diagnose a patient with suspected hyperthyroidism.
EXAMPLE: a man comes to the clinic, he is often agitated, has
tachycardia, eats a lot but doesn’t gain any weight. You suspect
hyperthyroidism. What is the first test that you should conduct?
TSH levels. (Remember it’s the most sensitive test)
If the TSH levels are elevated, this indicates a pituitary adenoma. You
refer your patient to imaging for an MRI to examine sellaturcica and the
tumor, and find out with it’s a micro or a macro adenoma etc.
If the TSH levels are low, you have to know the reason behind that. This
can be determined by obtaining a radioactive iodine uptake scan; here
we inject the blood with radioactive iodine and let some time pass, then
we measure iodine levels in the blood to see if it has been up taken by
the thyroid gland - high uptake or if the levels are the same- low uptake.
Low uptake indicates a primary thyroid problem (problem within the
gland itself; the gland cannot take iodine from the blood to synthesize its
hormones due to a problem with its cells), such problems include:
thyroiditis, ectopic thyroid hormone, exogenous thyroid hormone.
High uptake poses another question, how is the distribution of the
radioactive iodine? It could be Homogenous or nodular; Homogenous
indicates Graves disease,while nodular distribution can be one of two:
single or multiple areas.Multiple areas indicate Toxic multinodular goiter
(rare but can happen). A single area indicates Toxic adenoma.

6 | P a g e
*note: the most common disease of thyroid is multinodular goiter (most cases are
euthyroid ) rarely goiter can be associated with hyperthyroidism (toxic goiter )
NOTE: check your patients eyes when hyperthyroidism is suspected; as
you will find many signs associated with it there, such as exophthalmos,
wide gaze vision etc. (will be further discussed).
NOTE: Another diagnostic scan is PETscan- stands for Positron Emission
Tomography- which is used in staging cancer. This scan uses a
radioactive sugar molecule-fludeoxyglucose (FDG). It measures its
uptake by the body in addition to creating a 3D image that allows us to
examine the region properly; it detects 1 cm nodules which can lead to
diagnosis of papillary thyroid carcinoma. This type of scanning increases
the detection of thyroid cancer and is the cause for the increased
detected incidences in recent years.
HYPOTHYROIDSM
The biochemical formula is increased TSH levels (primary) and decreased
T3 and T4 levels.
Clinical presentation:
In children- Cretinism. Remember that T3 and T4 are needed for mental
growth in addition to physical growth, so in their absence the child
would have impaired CNS and bone growth, mental retardation, short
stature, coarse facial features, protruding tongue and umbilical hernia.
Early detection and treatment of cretinism is extremely vital to prevent
mental retardation (most importantly) in addition to all other
complications. Cretinism is now supposedly gone since in most countries
children are screened early on for thyroid abnormalities and parents
have better awareness about signs and symptoms that indicate
hypothyroidism, all leading to early detection and treatment .

7 | P a g e
For treatment of squamous cell
carcinoma of the tongue or
larynx, that leads to damage to
neck causing hypothyroidism
MOST COMMON
Currently the most common
cause of hypothyroidism in non-
iodine deficient areas. (In the
Himalayas and South America
where iodine is deficient,
iodinated salt is sold everywhere
in order to prevent iodine
deficiency, so even in those
areas we find Hashimoto
thyroiditis to be the most
common cause of
hypothyroidism).
Result of end organ
resistance, one of the
mechanisms of
endocrine dysfunction
Lithium based drugs are used in
treatment of psychic illnesses
like mania.
In adults-Myxedema. Here growth is over( no mental or physical
retardation), and complications include: slow physical and mental
activity, cold intolerance(opposite of hyperthyroidism), overweight, low
cardiac output, GI symptoms like constipation, decreased sweating, cool
pale thick skin especially on the chin(opposite of pretibial myxedema).
Causes of hypothyroidism:
For localized tumours in one lobe Ablation is damaged to
thyroid gland

8 | P a g e
Notice how the signs and symptoms of hyper and hypothyroidsm are
mostly the opposite of each other and involve all bodily functions.
Clinically speaking it’s not difficult to differentiate the two from each
other.
AUTOIMMUNE TYROID DISEASES
a very common and large group that includes: Hashimoto thyroditis,
Granulomatous thyroditis(de Quervain) and subacute lymphocytic
thyroditis.
NOTE: some do not consider Granulomatous thyroditis atrue immune
disease because it’s not associated with anti-thyroid antibodies.
However, it is still included as some argue that it has an underlying
autoimmune cause.
HASHIMOTO THYRODITIS (CHRONIC LYMPHOCYTIC THYRODITIS)
Most common cause of hypothyroidism in areas with no iodine
deficiency (very important).Initial presentation (phase) includes a
transient increase in T3 and T4 levels (thyrotoxicosis) before it develops
into hypothyroidism. This may lead to misdiagnosis if the patient
presents to the hospital at this stage (gradual hypothyroidism, rarely
initial transient Hashitoxicosis). It is also common in middle aged females
(45-60 years).

9 | P a g e
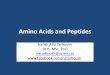
Basic pathogenesis:
Autoimmune destruction of thyroid epithelial follicular cells -which
release T3 and T4- by high anti-thyroid antibodies.
People who have it are at an increased risk of developing papillary
thyroid carcinoma and primary B-cell NH lymphoma (4-6 times more at
risk).
The body’s tolerance towards its own thyroid epithelial cells is
maintained by memory cells that recognize those cells as normal and do
not produce antibodies against them. If this tolerance is disrupted then
antibodies will be produced (can be detected in the serum) and will
attack thyroid cells by antibody-dependent cell-mediated cytotoxicity
(1). CD4+ T cells will react with thyroid antigens and produce cytokines
such as interferon ɣ (IFN-ɣ), which in turn activates macrophages
resulting in thyrocyte injury(2). CD8+ cytotoxic T cells will be activated as
well leading to T-cell-mediated cytotoxicity.
1 3
2

10 | P a g e
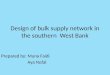
Histologically: we can observe:
1-lymphoid inflammation: the thyroid gland
is destroyed due to inflammation resulting in
abnormal lymphoid follicles.
2- Atrophy of follicles. And no colloid
3- Hurthle cell change: enlarged thyroid
follicular cells with large cytoplasm that
appear pinkish and eosinophilic due to
increased number of mitochondria.
Under the microscope:
Lymphocytic follicular inflammation
and atrophy+ Hurthle cell change.
SUBACUTE GRANULOMATOUS (DE Quervian) THYROIDITIS
Granulomatous inflammation (thyroiditis), more acute with neck pain
and results in a firm thyroid.
Remember: granulomatous inflammation is associated with chronic
inflammation that includes epithelioidhistocytes, reactive T cells and
plasma cells. It could be necrotizing(TB) or non-necrotizing (sarcidosis).
Some trace de quervian thyroiditis to viral causes; they claim the
presence of coxsackievirus or EPV antibodies in the serum but nothing is
proved yet. De Quervian is also more common in females aged 30-50
years and has an initial transient thyrotoxicosis phase before developing
into hypothyroidism (same as in Hashimoto thyroiditis). This
inflammation is a self-limiting disease that resolves on its own within 6-8
weeks, it is usually diagnosed clinically and patients are not referred to
pathologists.

11 | P a g e
OTHER LESS COMMON THYROIDITIS:
1. Subacute lymphocytic thyroiditis: a chronic lymphoid
inflammation with no granulomas or Hurthle cell change.
Common in middle aged women who are post-partum. Like the
previous two inflammation, has an initial transient thyrotoxicosis
then gradual hypothyroidism. It’s an autoimmune disease where
circulating anti-bodies are found. The gland’s size is normal.
2. Riedel thyroditis: specific type of inflammation characterized by
IgG4 mediated destruction of the gland with severe fibrosis to the
point where the thyroid becomes stony-hard.
IgG4 can cause the same destruction in many organs. Fibrosis is
mediated by Transforming Growth Factor-β (TGF-β).
GRAVES DISEASE (TOXIC DIFFUSE GOITER)
Remember: toxic indicates thyrotoxicosis (hyperthyroidism) due to
high homogeneous uptake.
This disease was described by Robert Graves in 1835. It is the most
common cause of endogenous hyperthyroidism and includes the
triad of: thyrotoxicosis(with its associated signs and symptoms),
opthalmopathy (eye signs, like exopthalmos) and dermopathy(skin,
like pretibial myxedema).
*The doctor said this picture is not important*

12 | P a g e
Histologically:
Observe that the follicles are surrounded by a
white columnar cells that resorb the colloid , the
colloid is pale with scalloped margin
Exopthalmos
AUTOANTIBODIES OF GRAVES DISEASE:
Normally T3 and T4 are released upon stimulation of the thyroid
gland by TSH, which is released from the anterior pituitary. Thyroid
hormones release is regulated; when their levels increase in the
blood there’s feedback inhibition on the release of TSH to prevent
further secretion of T3 and T4.
In Graves this mechanism is lost; there are antibodies that bind to
TSH receptor on the thyroid continuously stimulating it and resulting
in overproduction of T3 and T4 withno response to the feedback
inhibition on the pituitary gland that would normally occur due to
these increased levels.
**autoimmune ,HLA-DR3 and CTLA-4 / women 20-40 years
** sometimes TSH- binding inhibitor Ig , may cause hypothyroidism.

13 | P a g e
Pretibial Myxedema:
subcutaneous deposition of fat
tissue on the shin.
DIFFUSE AND MULTINODULAR GOITER
This is a very common disease and it is the most common disease of the
thyroid gland. It is usually euthyroid; the goiter is not associated with
hyper or hypothyroidism, however there are rare cases in which we have
goitrous hypothyroidism.
The underlying pathogenesis in not yet understood; some claim there’s
hormonal imbalance with continuous stimulation and inhibition of the
gland causing it to enlarge and shrink throught the years, leading to
hyperplasia, hypertrophy and elevated TSH levels.
This disease is more common in females, and can be endemic-more
prevalent in certain geographical regions or sporadic. It starts initially
diffused then becomes multinodular, however it usually is detected in
the nodular phase. The goiter will enlarge and cause pressure on the
surrounding tissue leading to difficulty in swallowing, breathing, pain
and spontaneous hemorrhage(mass and cosmetic effect). In certain rare
cases, one or two of the nodules will release T3 and T4 increasing their
levels and leading to toxic MNG also known as “Plummer syndrome”.
Clinical features:
Middle aged female with
multiple masses.

14 | P a g e
Note the fibrosis along with the nodules. Under the microscope: variable size follicles.
THYROID NEOPLASMS
Benign neoplasms are much more common the malignant ones. Most of
those benign neoplasms are non-functional adenomas as was
mentioned before. However, risk of malignancy increases with:
- Solitary nodules more than multiple nodules.
- Male nodules more than female nodules.
- Ages younger than 20 and older than 70 years old.
- Family history and previous history of radiation.
- Cold nodules much more than hot nodules.
What is cold/hot nodule?
Thyroid gland after resection: note the right and
left lobe, the isthmus and the nodules.

15 | P a g e
In iodine uptake scan, a cold nodule has no iodine uptake(inactive),
while a hot nodule uptakes iodine and has zero(less than 1%) chance of
becoming malignant.
NOTE: MNG is more common than benign neoplasms.
FINE NEEDLE ASPIRATION
Routine initial tool for evaluating thyroid neoplasms. Simple, cost
effective, very accurate and is now well-standardized. If the mass is
palpable then the procedure can be carried out normally, however if it is
not the case is referred to a radiologist who conduct it under the
guidance of ultrasounds. After the sample is obtained it is put on a slide,
stained and examined under the microscope for features of follicular
carcinoma for example. Recent recommendations suggest that ALL FNA
procedures should be done under ultrasound’s guidance.
FOLLICULAR ADENOMAS
NOTE: the word follicle could be associated with adenoma or
carcinomas. However, the word adenoma-in the context of thyroid
neoplasms- indicates only follicular adenomas as there’s no such thing as
papillary adenomas only papillary carcinomas.
Most common adenomas are follicular adenomas. The underlying
pathogenesis is driver mutations in TSH stimulation and less commonly
RAS mutations, leading to autonomous adenoma.
Follicular adenomas come solitary, they are well-circumscribed within an
intact thick capsules that has no infiltrations in it or vascular invasion.
Bland cells or Hurthle cells may be present and in that case it is called
Hurthle cell adenoma. Occasional atypia can be seen as well.
The aforementioned intact capsule is the main feature through which
we distinguish between follicular adenomas and follicular
carcinomas(carcinomas have both capsular and vascular invasion).

16 | P a g e
Normal compressed resected
lobe.
Capsule (note that there’s no
infiltration).
Tumor tissue
Hurthle cell adenoma
Remember Hurthle cells are large cells with
pinkish cytoplasm due to increased
number of mitochondria
Note: some people claim that hurthle cell
carcinoma is more dangerous than
follicular carcinoma.
THYROID MALIGNANCIES
Common but not aggressive, they generally have good prognosis even in
the presence of lymph node metastasis. They’re more common in
females and risk factors include: ionizing radiation (Chernobyl 1986) and
iodine deficiency.
Primary malignancies of the thyroid gland:
1- Papillary carcinoma: represent 75-85% of thyroid malignancies.
Metastasizes to cervical lymph nodes. Treatment of this
carcinoma includes total thyroidectomy and lymph node
dissection on right and left side of the neck.(note: remember
there’s no papillary adenoma).
2- Follicular carcinoma: 5-15% of all malignancies. Metastasizes
through the hematogenous route to the bones and the lungs.
3- Anaplastic carcinoma: one of the most aggressive human cancers,
patients live up to only one year after diagnosis. <5%

17 | P a g e
4- Medullary carcinoma: not very common(5%), tumor arises in
parafollicular cells that produce calcitonin. May be a part of
Multiple EndocrineNeoplasia syndrome type2 (MEN2).
5- Lymphomas: remember patients with Hashimoto thyroiditis have
an increased risk of developing Papillary Thyroid Carcinoma(PTC)
and B-cell non Hodgkin lymphoma.
In recent years studies began on what is the underlying genetic
abnormalities resulting in malignancies, it was found that RET/PTC and
BRAF are linked to papillary carcinoma while RAS is linked to follicular
and anaplastic carcinomas. This can help in determining the best
candidates for thyroidectomies and aids in avoiding unnecessary
surgeries which will reduce costs and possible complications.
PAPILLARY THYROID CARINOMA
The most common thyroid carcinoma, relatively inactive (indolent). Has
good prognosis with 95% 10 years survival case, even in the presence of
lymph node metastasis(50% of PTC have lymphoid metastasis at the
time of presentation, which is why when thyroidectomy is preformed,
lymph node dissection is automatically done in the same surgery).

18 | P a g e
Orphan Annie eye nuclei
Can be uni and multifocal- the two lobes and the isthmus all have
nodules.
Preoperative diagnosis by FNA is accurate because since there’s no
papillary adenoma, once papillary features are detected that
automatically indicates papillary carcinoma. There are 15 papillary
features such as: papillae, psammomabodies(calcification),
pseudonuclear inclusions and nuclear features (which are of great
importance in diagnosis): nuclear grooves and Orphan Annie eye nuclei.
Resected thyroid: firm and
calcified
This section shows well-formed
papillae lined by empty appearing
nuclei or “Orphan Annie eye”
Orphan Annie eye

19 | P a g e
Nuclear groove
Inclusions
Calcifications
Vascular invasion Capsular invasion
Notice the “mushrooming” of the
tumor tissue into the capsule and how
it pierces it.
FOLLICULAR CARCINOMA(macro follicles that lack papillary nuclear features).
Solitary cold nodule that upon evaluation exposes capsular and vascular
invasion; these two characteristics differentiates it from follicular
adenoma. Common in women aged 40-60 years old and in iodine
deficient regions. Metastasizes through the hematogenous route to the
bones, lungs and liver. It doesn’t metastasize to the lymph nodes which
is why when follicular carcinoma is removed no lymph node dissection is
carried out. 50% of patients die within 10 years.

20 | P a g e
This pinkish material is amyloid
which is protein deposition
produced by cancer cells.
ANAPLASTIC CARCINOMA
This type is rare, representing less than 5% of all thyroid malignancies. It
is extremely aggressive and infiltrates the surrounding it can enlarge to
the point where it suffocates the patient. It has a mortality rate of 100%.
The cells are undifferentiated and can be easily distinguished using FNA.
Occurs in 25% of people with previous history of a well-differentiated
carcinoma-papillary or follicular carcinoma. >than 65 years .
MEDULLARY CARINOMA
Arises from C-cells or parafollicular cells which are neuroendocrine cells
of the thyroid gland that release calcitonin, which in turn leads to
decreased calcium serum levels and hypocalcemia. It can be a part of
Multiple Endocrine Neoplasia syndrome type 2(MEN2)a &b, and can be
sporadic(70%) and in this case patients are of older-ages 50-60 yrs or
familial(30%) and patients here are of younger ages.
RET receptor tyrosine kinase mutations on chromosome 11 result in
medullary carcinoma ( as what doctor said in record sec.4 (1:07: 28). If a
person is diagnosed with this type of carcinoma his/her entire family
should be tested for this mutation, and those who appear to be positive
have to undergo a prophylactic thyroidectomy even if no medullary
carcinoma is present, because future risk remains high.
Medullary carcinoma ismulticentric and contains amyloid. It is also a
great mimicker; underthe microscope it can look like any tumor
(plasmatic, spindle etc), so usually when you examine a tumor that
doesn’t look strictly papillary or follicular you always think of medullary
carcinoma.

21 | P a g e
Sometimes you can’t tell
whether the cells are C-cells or
follicular cells, so we stain using
Immunohisto chemistry (IHC),
the brown colour indicates
calcitonin which conforms that
this is medullary carcinoma.
Diagnosis of medullary carcinoma: amyloid deposition and calcitonin.
Parathyroid gland
Chief cells produce PTH, the gland is controlled by free calcium levels in
the blood more than by tropic hormones. Like other endocrine glands
there’s hypo/hyper functions and tumors, but tumors here rarely have a
mass effects because the parathyroid glands themselves are very small,
so even a 1 cm mass is considered massive, meaning the gland doesn’t
enlarge to the point where it can have a mass effect.
Functions of the parathyroid glands:
- Reabsorption of Ca from renaltubules.
- Excretion of PO4 into urine.
- Vitamin D conversion to active form.
- Stimulates osteoclast activity on bone resorption.
The end result is increased calcium levels in the blood.
HYPERPARATHYROIDISM
It can be primary, secondary and tertiary. Complications include:
Osteitisfibrosacystica, Brown tumor of bone, nephrolithiasis,
nephrocalcinosis and metastatic calcifications.
Primary HPT is due to adenomas in 85-95% of the cases, hyperplasia in
5-10% and carcinoma in 1% of the cases. Mutations in Cyclin D1 gene on
22 | P a g e
chromosome 1 or MEN1 mutations can be the underlying genetic
abnormalities leading to HPT. ( go to slide 73)
When calcium and PTH levels are elevated we carry out an uptake scan
to see which of the 4 parathyroid glands is actively causing this, we
suspect parathyroid gland abnormalities because it is known that
parathyroid adenoma is one of the most common causes of
hypercalcemia and hyperparathyroidism. Once the abnormal gland is
identified, it is resected, and samples of the serum before and after the
resection are obtained and compared to make sure the correct gland has
been removed (PTH will be more sensitive that calcium).
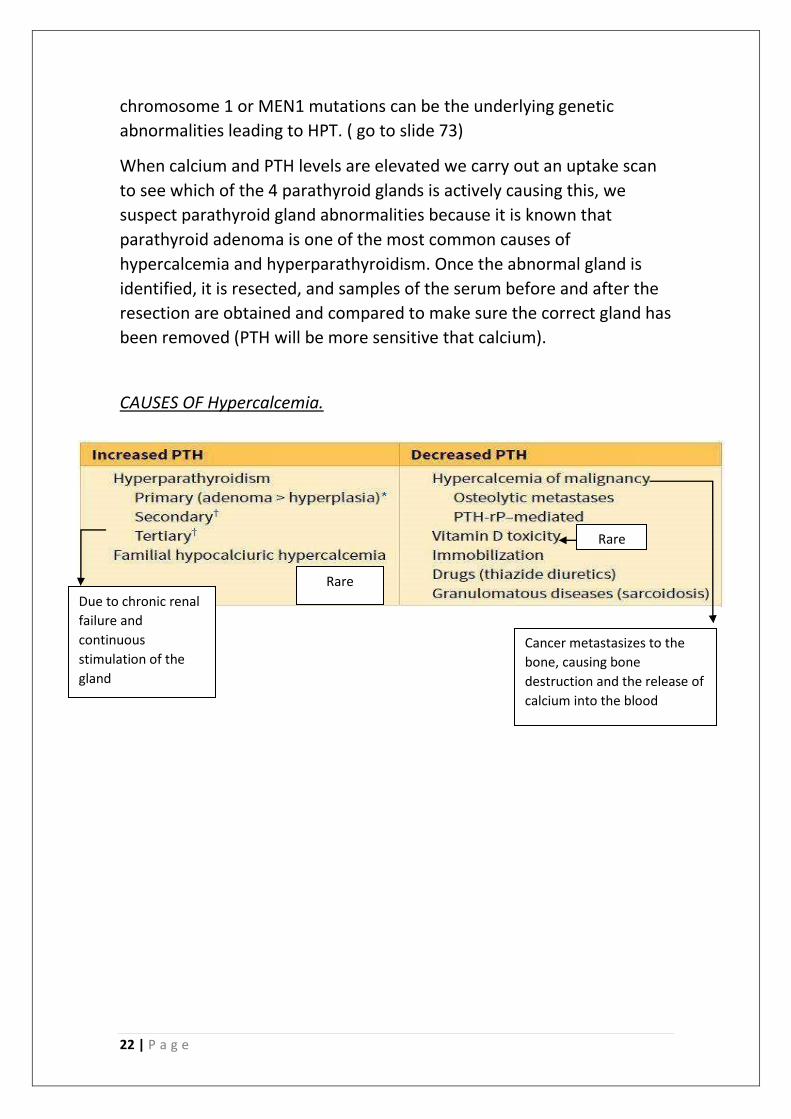
CAUSES OF Hypercalcemia.
Due to chronic renal
failure and
continuous
stimulation of the
gland
Rare
Cancer metastasizes to the
bone, causing bone
destruction and the release of
calcium into the blood
Rare

23 | P a g e
*Focus on primary and secondary HPT as tertiary HPT is more difficult to dignose*
HYPOPARATHYROIDSIM