Embed Size (px)
Citation preview
'1~w-- I
Resection of the lIver for colorectal carcinoma metastases: A multi-institutional study of indications for resection Registry of Hepali( Mt"taslases·
In an Inuesliga/lon of the indIcatIOns for hepatIc resectIOn In thc trealment of colorectat carcinoma melastases. thc records of 859 pallents who had undergone thIS procedure were revIewed ThIS pallfnl group. from 24 InstllutlOns, was found to haue a 5-year acluana! run'wal of 33% and a 5-yfQ T actuarial dIsease-free sunllllal oj 27%. The only jactors that might by themse/;'es be considered contraindlcatlOns to hepallc resection are the presence of posltll" hepatIc nodes, Ihc pusence oj resectabh extrahepallc melastases, or thc preSfna of jour or mOrt metastases. Other fac/on that had a nega/lve effect on long-term sun'lua! were margIns of reJ('ctlOn on the /zl'er me/as/ases less than or equal to 7 em (S (5-year actuanal sUTl'll'al) = 23%). the presence of pOSItIVe mesente[lc nodes In the pnmary tumor specImen (S = 23%), and a disease-free interl'al of less than 7 year (S = 24%). The effect of anyone of these factors was not greal enough to contraIndIcate resection. Howetler, combinatIons of prognostIC faclors must be ((Ins/dered before resec/wn IS recommended. The overall 5-year sun'Il'ai rate for thiS large senes has been very salislYlng. DecIsIon making In
the future must take Into account such factors as number of metastases, extrahepatic Involvement, and stage of the pnmary tumor.
Suppon~d in pan b\ Last'r Sonic. Inc.
AIT~pt~d for publication ~fa\ 14. 198~
R~print r~quests Knin S Hughes. MD. Departmenl of Surgen. l'ni\rrsl\\ of California Da"s. 4301 X St. Sacramento. CA 9;SJ-
·K~hes ~1 D. ~attc>nal Can~n Imtitute. B;;t:,~sda. ~'d.R7riiarir Simon. Ph D. :->allonal Cancer Institu". Sate Som;horabodl ~1.S ~ational Cancer InslI' tute. ~anin .... :\dson ~'D .. Maw Chnl(. Rochester.
Mmn. Duane ~l Ilmup. ~1.S . Mal''' Chnlr. Jo~ph G Fonner. M D, ~lemonal Sloan.Kellenng Canctr Cenler.
~r" York. ~ Y Barbara J Maclran. B S. ~'emonal Sloan·!\eutflng Canc~r een,er. Jam~; H Foslrr. ~1 D.
l'n"'ersit~ of ConnrclicuL Farmjn~on. Conn. John \1. Daly. M D. MrmorIa! Sloan-Kclltrin!! Cancer Crnter. Diane Fllzhrr~n. R~ . Memorial Sloan.Kellermg Can· ~r Center: Paul tr. MD .. :->allonal Cancer
Institute.~~~~~;;~~-:;-,~~:"':l burgh. PIttSburgh. Pa, .""'"'i~;;;';"';';';;"::::~~ Plltsburgh, Kenneth P
L'ni,·trsit\ of CalIfornia. !'icholas J P~trelli. ~1 D. Ros· well Park. Buffalo. ~ Y. Lemuel Herrera. MD. Roswell Parl. Blake Cady. ~ID :->e" England Dearon~~s Hospi. tal. Boston. Mass .. WIllIam McDrrmoll. M D. ~tW England Deaconess Hospital Thomas :->Ims. ~, D. Grant Hospital. Columbus. Ohio. Warren E Enker. M.D., MemOrIal Sloan·Krtltring Cancer C~ntrr, Genr F Coppa.
278 Sl'RGERY
MD. New York llni"trsity; Le51~ H. Blumgan. M.D .. Hammersmnh Hospital. London. England. Howard Brad· piece. M.D. Hammersmith Hospnal. Marshall l'rist. MD. l'ni'er>m of Alabama. Birmingham ..... la. Joaquin S Aldretr. MD. CniverslI) of Alabama. Prltr S(hlag. MD. Khnlkum der l'nl\enitat Htidel~rg. Hrldtl~rg. W Germam. Pctn Hohen~rger. M D. Klinikum d~r UnI'trSliai Heidtl~rg. Glrnn Strrk. Jr .. M.D. :->ew England Deaconess Hospilal; W John Hodgson. M D,
l"rw York ~ledical College. \'alhalla. !'Y, Thoma' G Hardy. M.D. Central Ohio Colon and Rntal Center. Columbus. Ohio. DrnIS<' Harbora. R ~. CroSI Cancer Instil ute ..... I~na. Canada. T .... Iexander !\lcPher,>on. MD. Cross Can~r Insulute. Christopher lim, MD. Cross Canc-er InslIlult. Daniel Dillon. MD .. The ~lrrn HospItal of PlIIsburgh. Pmsburgh, Pa, RIchard Happ. M D. The ~lrrcy Hospnal of Pillsburgh. Philhp RIp<'pi. MD. Tht ~'m) Hospital of Pillsburgh; Edward Vtllrlla. M.D., The ~fern Hospital of Pillsburgh: RIcardo L ROSSI. MD. Lahe\ Chni(. BurlInglon. Mass. Stephen G Remine. ~ID. Lahn Clinic. MaT) O;ttT. B.S. Lahe) Clinic, Da\ld P Connolly. MD. St Margaret's Hospllal. PlIIsburgh. Pa, Jerome Abrams. M.D .. l'niverslI) of Vermont. Burlington. Vt. Adel AI-Jud, M.D. lini\er>ity of Iowa. Iowa Cily. Iowa. KEF Hobbs. MD. ROl'al Free Hospital London. England. Michael K W LI. M.D. Royal Free Hospital. Ted Howard. MD., Kings ColI~ge H"spital London. England. Emonud L«. M D. John Radrliffr InfirmaT). Oxford. England.
\'"1",,,( 16 I Suo,,!.," 3
Hrr~TJ( Rf.'ICTIt" I' th~ onh curativ(" tr~atm~nt curr~ntly available for rolor~rtal carcinoma m!"ta~tasr~ to th~ Iiv~r, and it is estimat~d that ever) y~ar approxi-' mat~ly 6,000 to 12,000 patients in thr enited Statrs are candidates for this proc!"dure ' : Prniou~ studi!"s sugg!"st that th!" 5-nar sUT'\'ival from this procedurr is in the rangr of 25')0 to 35')' •. '" HowrvCf, at this time, only an estimated 1,000 hepatic resections are done each yrar in the l'nited Statrs (personal communication). The limited use of this procedure stems from three common beliefs: (1) Hrpalic mrtastases are fatal regardless of treatmrnt, (2) hepatic resection is effective only for solitary metastases, and (3) hepatic resection results in extreme morbidity and a high mortality rate. The third belief can be readily dismissed, as the mortality rate for hepatic resection has been addressed in several previous articles and is only about 5%. '-<,
This is a rate considered acceptable for a major surgical procedure, The purpose of this article is to evaluate the first two beliefs.
A collaborative effort involving 24 institutions intimately involved in hepatic resection provided data on a large series of patients in order to answer questions regarding the indications and contraindications to hepatic resection, Our results indicate that 5-year survival of patients is not unusual after hepatic resection and that multiple metastases, bilobar metastases, or large metastases are nOl, in themselves, contraindications to this procedure.
METHODS
Patient population. Eight hundred fifty-nine patients who had undergone curative hepatic resection for treatment of coloreetal carcinoma metastases between 1948 and 1985 made up the study population Patients who died postoperatively (within 30 days of operation) and patients who had gross tumor left in situ have been excluded. Consecutwe patients from each of 24 recording institutions were reviewed and entered into a central data base Two institutions recorded more than 100 patients, 3 institutions recorded 50 to 100 patients, 6 institutions recorded 20 to 50 patients, and 13 institutions recorded fewer than 20 patients. Confidentiality prevents our stating the exact number of patients from each hospital. However, we can confirm that each institution recorded all consecutive hepatic resections performed in the study period by participating surgeons. Chart review was governed by a standard data retrieval protocoL Investigators at each institution were asked to review their patient charts to complete the data form. The senior author (K. S. H.) visited the institutions where this was not feasible to
direct" r('\ 1('\\ thr p;1tirnt (harts ThiS re~ult('d In
approximate" two third, of the charts heIn\?, re\ln, ('d bva single author Thi~ samc author also re\lr\\ed all data sheet~ beforc their entn Into the computrr In an cffort to makr this a uniform interpretation of retro· spective data.
Data forms. A standard data form \\a~ de~ll?,n('d to retri('ve information on se\'eral aspects of the priman colorectal tumor, such as the date of primary resection. the location of the primary tumor, and the presen( e (If absence of metastases to local lymph nodes. The form also recorded information on the status of the patient before undergoing hepatic resertion, such as the date of diagnosis of the liver metastases. the carcinoembryonic antigen (CEA) assay before reseC'tion, and th(' presence of symptoms or signs of hepatic metastases (for example. nausea, abdominal fullness. abdominal mass. jaundict', and palpable ht'patomegaly). Signs and symptoms of liver metastases were considered only in patients with liver metastases in situ more than 2 months after colon resection. to avoid confusion with symptoms of the primary tumor In addition, information was recorded about the hepatic resection procedure, such as the date and type of resection, the presence or absence of extrahepatic disease, the presence of portal or celiac lymph nodes, the presence of contiguous spread (direct invasion or adhesion to adjacent structures). or the presence of discontiguous metastases (that is, simultaneous metastases outside the liver to the lungs, peritoneum, small bowell, etc.). The synchronous presence of the primary colon tumor was not considered a discon:inuous metastasis, but an anastomotic recurrence after removal of a primary colon carcinoma was considered to be discontinuous extrahepatic disease Data retrieved from the pathologic specimen included the number of metastases, the distance to the closest margin, and the largest diameter of each metastasis. Follow-up data recorded included the date of the most recent follow-up. the status of the patient (alive with disease., alive without dis('ase. dead without disease. dead with disease). thc sitc of initial recurrencc after hepatic resection, and all other sites of recurrence after the initial site of recurrence.
Statistical analysis, The data base was maintained under thc DBASE III data base management system on a microcomputer and uploaded to a main frame for analysis. The distribution of survival and disease-free survival was estimated with the standard KaplanMeier method, Disease-free survival was defined as time until death or recurrence, whichever occurred first. For patients who died of disease, if the date of recurrence was unknown the date of death was used for
1
I
\",. L:' .. ,\ 1 .' I • I .......
Tabl~ I. Sur-i\al and dis(,il'r·fr~e suni\al f(lr palifnl~ undrrg(}in~ rrs('Clicln (If isolalrd hepatic mf'IJ<t;l'(',
2 ~"\
}- (i : "
Pdlh"I"I!I( m.HI:,n (,n 11'('f sprllmrn P"',mr Of <11m >1 ern
DISlf1bu\i('n of multiple mrI.lSi~'(,' l'nilobar Bll(lbar
Slagr of priman tumor Dukt's' B (nt'g me,enteric
nodes 1 Duke,' C (IX'S mesentefll
nodes) Di"t'as('·free Inten .. 1
<1 rno 1 rno 10 1 H
> 1 yr Age (vr)
<40 40. 7 0 >-0
C[:\ before IiHr r('senion (ng mil
<5 ~·30
>30 Sizt' of solltan It's 10m (em)
<8 >8
Type of rest'rtion of solitar\ lesion Wedge AnalOrnic res('rtion
·~·\ea' aC1L.df!d.~ ~u~"l.dl
+~·Ytar ar:'Uar:,1.1 d:,-(,jl,r·frtr sU~\l\al
f\(l: adt'(,p.Jd't nl.imt~;:. (~f p3!It'n:' 11, d(~rrnllrH' :"'\CM sur"on,,]
\ ' "
~ll')
131 141)
~(13
1(1-
10' 79
~~6
31-
8(1
626 92
380 101
the calculation of disease·free survival. Distributions of survival or disease-free sur-'ival were compared bv means of the log rank test. If more than two groups were involved (such as free interval of less than 2 months, 2 to 12 months, more than 12 months) pain"'ise comparisons were made only if the overall test statistic was significant at the 0.05 level. In some cases results for merged groups were reported but the original significance tesl was based on group boundaries defined independently of the results The multivariate analyses were based on the proportional hazards model of Cox'"' Five-year sur-'ival and disease· free survival rates were estimated from the Kaplan-
.\;, . /)-,,,, " ."" ",', :
.'\- 2; r ,~
I~
~\ 1 "\ 4- .'\3
30 1 (,
* i
47 ~t<
~3 18
2- 1-31 ,~
42 20
r r 33 21 31 18
47 42 30 19 28 14
38 2, 27 21
35 21 41 29
Meier curves and multivariate analyses. The cur-es themselves appeared to plateau around 5 years for S{'ts with sufficient numbers of patients. In many cases the 5-year {'stimates are associated with wide confidence inter-'als, and this imprecision is mentioned. In some cases the estimation is so imprecise that estimates are not reported Even for a data set as large as this. there are many comparisons of interest that can be made onh with inadequate statistical power (for example, comparison of outcomes for stage C patients with two versus three metastases). \\'e try to indicate when "negative" results are not conclusive because of inadequate statistical power.
\ , I I
I I !
1',,;:. "II 1(1.; SU, .. I .. , l
RLSl'LTS
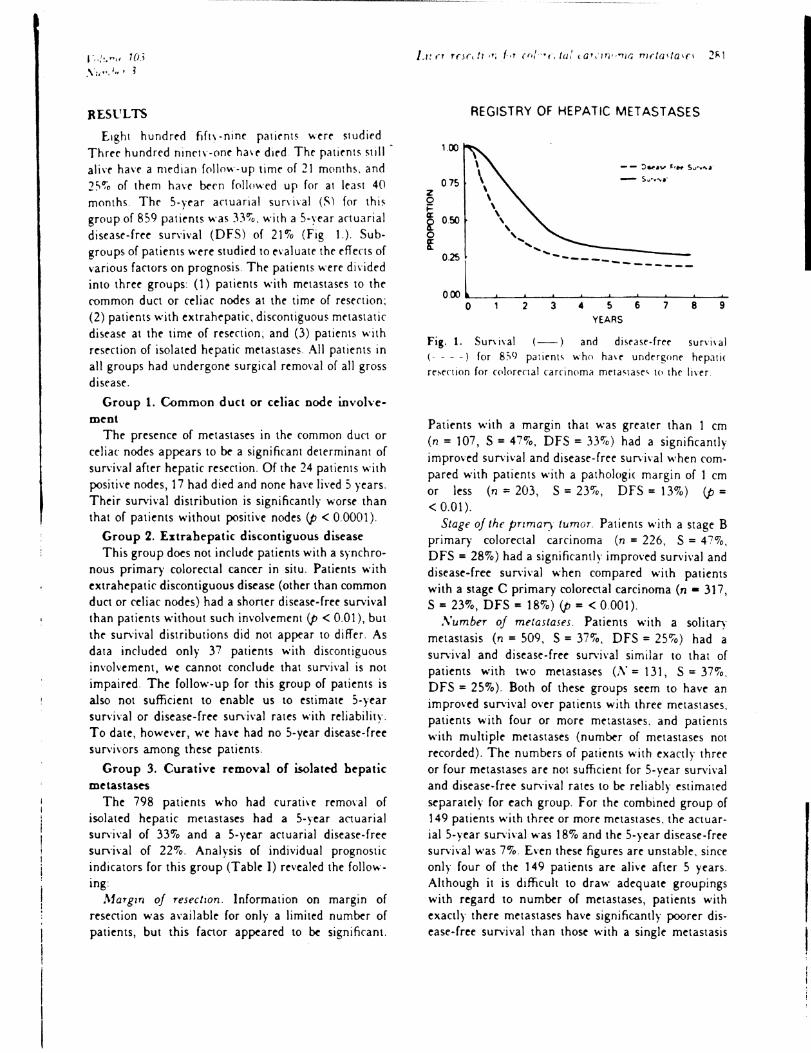
Eight hundred fift\ -nim patifnt~ wrrr studied Thrre hundred ninety-one ha'r died Thr patirnts stili ali'f havr a median f01low-up timr of 21 months. and 2"~o of them have been f0110wed up for at least 40 months The 5-yrar anuarial survival (S) for thiS group of 859 patients was 33~o. with a ,-yrar actuarial disease-frel" survival (DFS) of 21"lo (Fig 1) Subgroups of patil"nts werl" studil"d to evaluate thr eflens of various factors on prognosis. The patients were divided into three groups (1) patients with metastases to the common duct or celiac nodes at the timr of resrction; (2) patients with extrahepatic, disrontiguous mrtastatic disease at thr time of resenion; and (3) patients with resection of isolated hepatic metastasrs All patients in all groups had undergone surgical remO\al of all gross disease.
Group 1. Common duct or celiac node involvement
The presence of metastases in the common duct or celiac nodes appears to be a significant determinant of survival after hepatic resection. Of the 24 patil"nts with positive nodes, 17 had died and nonl" have Jived 5 years. Their survival distribution is significantly worse than that of patients without positive nodes (p < 0.0001).
Group 2. Lxtrahepatic discontiguous disease This group does not include patients with a synchro
nous primary colorectal cancer in situ. Patients with extrahepatic discontiguous disease (other than common duct or celiac nodes) had a shorter disease-free survival than patients without such involvement (p < 0.01), but the survival distributions did not appear 10 differ. As data included only 37 patients with discontiguous involvement, we cannot conclude that survival is nOI impaired. The follow-up for this group of patients is also not sufficient 10 enable us to estimate ,-year survival or disease-free survival rates with reliability. To date, however, we have had no 5-year disease-free survivors among these patients.
Group 3. Curative removal of isolated hepatic metastases
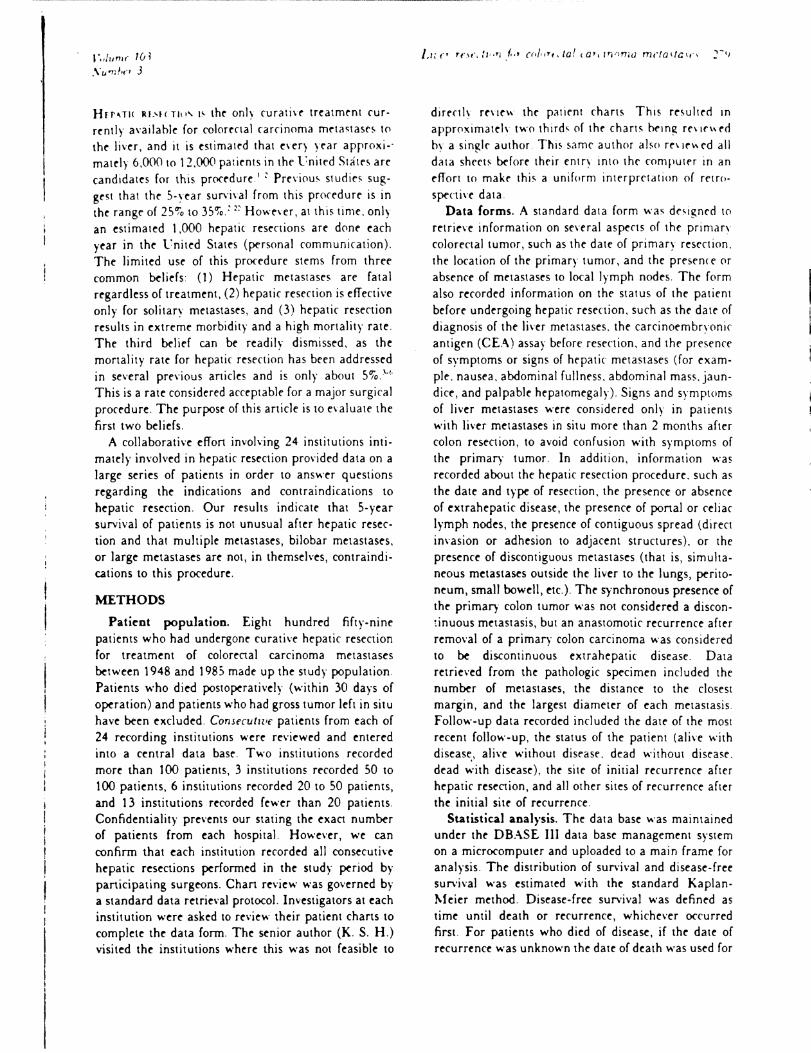
The 798 patients who had curative remO\'al of isolated hepatic metastases had as-year aClUarial survival of 33% and a S-year actuarial disease-free survival of 22~o. Analysis of individual prognostic indicators for this group (Table I) revealed the follow-109
.\.1aTgl1l of resectIOn. Information on margin of resection was available for only a limited number of patients, but this factor appeared to ~ significant.
100
0.75 z 0 ~ a: O!iO ~ 0 g:
::l 0
REGISTRY OF HEPATIC METASTASES
\ \ \ , , ,
' ... ... ........ -
2 3
-------------
4 5 YEARS
6 7 8 9
Fig. 1. Survival (-) and di,('Jse-free sun·i\al (. - - -) for 8:'9 PJ:I('nt~ who ha\e undergone hrpati( re,ectlon for wlor('rtal carcinoma m('ta~ta,(" to the liver.
Patients with a margin that was greater than 1 cm (n = 107, S = 47~o, DFS = 33"lo) had a significantly improved survival and disease-free survival when rompared with patients with a pathologic margin of 1 cm or less (n = 203, S = 23u,"o, DFS = 13%) (p = < 0.01).
Stage of the pnmaT) tumor Patients with a stage B primary colorectal carcinoma (n = 226, S = 47 %, DFS = 28%) had a significantly improved survival and disease-free survival when compared with patients with a stage C primary colorectal carcinoma (n - 317, S = 23%, DFS = 18"lo) (p = < 0.001).
,\'umber of metastases. Patients with a solitary metastasis (n = S09, S = 37"lo, DFS = 2Su,"o) had a survival and disease-free survival similar to that of patients with two metastases (;\" = 131, S = 37 "lo , DFS = 25%). Both of these groups seem to have an improved survival over patients with three metastases, patients with four or more metastases, and patients with multiple metastases (number of metastases not recorded). The numbers of patients with exactly three or four metastases are not sufficient for S-year survival and disease-free survival rates to be reliably estimated separately for each group. For the combined group of 149 patients with three or more metastases, the actuarial 5-year survival was 18% and the 5-year disease-free survival was 7%. £\'en these figures are unstable, since only four of the 149 patients are alive after 5 years. Although it is difficult to draw adequate groupings with regard to number of metastases, patients with exactly there metastases have significantly poorer disease-free survival than those with a single metastasis

, I t
I.p < 001) or two mrta~tase5 IJ> < (101) Patients with four or mor~ metastases appor w d{l at Ir.]q as poorly
DI'itlhlJllnn of mrtol/a\(\ Patirnts with muftirlr. unilobar mrtastase" did not ha\e a si~nif\(anth
impro\('d survival (1' > 020) or dlSclsc-frcr suni\'al I.p > 0.40) whrn (omparcd with patients with multiple. bilobar metasta"e, There were onl\ -, patients with bilobar disease. and their follow-up is not adequat~ to enable us to reliably estimate a ,-,ear survival or disease-free suni\al for them (onl\' two such patients are alive with more than 5 years' follow-up). Although we find no evidence that distribution is an important prognostic factor for patients with multiple metastases, definitive ronclusions require longer follow-up of these patients,
S!ZC of solzlary mflasla.lt'5. Patients with a solitary metastasis that was less than or equal to 2 em (n = 113. S = 35~0, DFS = 24'70), patients with a solitary metastasis 2 to 4 em in diameter (n = 130. S = 37%. DFS = 27%), and patients with a solitary metastasis that was 4 to 8 em in diameter (n = 143. S = 43%, DFS = 27'70) appeared to have similar survival and disease-free survival. Patients with a solitary metastasis greater than or equal to 8 em (n = lOl, S = 27%, DFS = 21'70) appeared to have a somewhat decreased 5-year survival and disease-free sunival. though these differences were not statistically significant. Similar differences appeared to exist for patients with two metastases.
Symptoms oj izl'er metastases. Patients with symptoms of metachronous metastases (n = 93, S = 32'70 )
appeared to have a small but statistically significant reduction in sun'\\'al when compared with patients without symptoms ('1 :: 226. S = 45'7,) (p = O.OS)
CEA tel'el before tWCT resectIOn. Data on CEA level were available for a minority of patients. Patients with a CEA of nglml or less (n = 45. S = 47%, DFS = 42%) appeared to have an improved survival (p = 008) and disease-free survival (p = 0 15) when compared with patient> with a CEA of 4 to 30 ngml (n = 126, S = :: 30%, DFS = 19~~) or patients with a CEA greater than 30 ng'ml ('1 = 145, S = 28%, DFS = 14%) Larger numbers and longer follow-up of patients in the group with a CEA of less than 4 ng ml are necessary to substantiate this trend.
ContIguous Invo/t'ement of adJacent structures. Patients with contiguous spread of disease appear to have somewhat reduced disease-free survival compared with patients without contiguous spread (p = 007), The extent of follow-up for patients with contiguous spread is inadequate to estimate 5-year disease-free
\',' C' ". ,\ f,;, i, 7 fJ" •
suni\'al rate~ (Onh fpur of 104 ~u( h patient, arr alne with(>ut returren!e With :, year~ follow-up \
[)l\ca\/··{r(, lroi,'r: at. Patirnts with a disr.lsr-frer intfT\'al grrater than 1 year ('1 = 3}}, S = 42"', DFS = 26(7,'0) had a signifHanth Impru\cd SUr\!\d!
(p < 0.01) and discd~('-free survival V, < 0(2) when (Ompared with patimt~ with a disease-free intenJI b, than or equal to 1 year ('1 = 214. S = 240-0 .
DFS:: 16<'io) Patients with disease-free inteT\als less than 1 month had survival rates to similar to those with intervals of 2 to 12 months.
Agc a/ l!i'er resectIOn. There were 74 patients younger than 40 years old and 88 patients older than 70 years Although there was some suggestion that the older group had somewhat shorter survivals than those younger than 70. this difference did not approach statistical signiflcance on this uni\ariate anahsis
SurgIcal prulfdurc JOT a soh/a r) m<'laJtas!S. Patients who underwent a major anatomic resection ('1 = 26'7. S = 41 ~o, DFS = 29%) did not have a signiflcantly improved survi\'al or disease-free survival when compared with patients who underwent a wedge resection of a solitary metastasis ('1:: 235, S = 35%. DFS = 210/0). However, when patients were considered by size of the solitary metastases and type of resection, a difference was suggested The 54 patients who underwent a wedge resection for a solitary lesion greater than 4 cm in diameter had a decreased survival and disease-free sun iva) when compared with the 177 patients who underwent an anatomic resection for a solitary lesion greater than 4 cm (p < 0.02), Patients with lesions less than 4 cm appeared to have similar survivals and disease-free survivals. regardless of whether a wedge or an anatomic resection was performed Of patients with solitary lesions greater than 4 em, those who underwent anatomic resection had more favorable prognoses with regard to Dukes' stage (51% C) and disease-free inten'al (37% synchronous) than did those who underwent wedge resections (69% C and 57% synchronous). We compared the procedures with Cox's proponional hazard regressIOn model to adjust for stage and disease-free inten'al. The effect of surgica.l procedure appeared to persist as statistically significant, even after adjustment. The limited sample size for the number of factors included, however, renders the result less than conclusive.
The two subsets determined by size greater than or less than 4 cm for patients with solitary metastases were the only subsets for which procedures were compared. Hence this finding is not the result of excessive data manipulation. Nevertheless, the comparison is not based on random allocation of treatments
1 I" ":.",, , Ii ; ,\ 1,,,,1,,. j
Tabk II. ~atural hi~ton (.f (,plorrctal i1,'n mrta'ta~("s
Oxln ;tnrl till," C.,rll fl .,1>
:-':Irl,rn rl al , ..
Jaf1e el al'-
Brnl:m:trk and Hafslf<,m:' Ahr.lms and Lerner:'" B~dt'n and :\ndt'rson" \\'(.(.d 1"1 al 'I
Blln el ai"
GoslIn ('I al '"
Lahr t'l all'
Finan ('I al k
Bacon and !l.larun l -
St('arns and Blnkle," Palltnl' 'i. ':It. h;o mCIG5!(;i<.< M1/\
\\' agner ("t al 'Q
:-':ielsen et al'"
CadI el al.': Oxlel and Ellis" Jaffe el al :-
a!\irdr.5uf'ol\al
.~f('d;Jf'l ~ur\:\al
t,tr:.1\ ~,rr\n(lU\ §PrllT,,an rrfoC'(1td nc· r"':fJh('pa~l\ dlSCd,1,I'
!~o: pr(\\~ at bH'pq
" " • ,j ...
,\11
\Ji All All
,\11
All ,\1\
~"II:af\
~I ultlplr \I(){ allzt'd) \\ Idespread <2~cro
2;rro_ -~D:'"(,
> - S"c; t· nilc,b:n Bilnbar >4
<4 t'nilnbar
BiJobar Solilan \lul1ipk All All
Sohtar~
\lultiple (unilobar) ~fultiple
(\\idespread)
Few melaSlases Seleral WIdespread All :\11 .\11
and the groups may be prognostically differ("nt in ways we could not detect or appropriateh' adjust for.
,\luI/Il'anale analyszs Multivariate analysis of the joint effects of the above factors on survival and dis~ase-free survi\al was performed for patients without extrahepatic nodal or disrontiguous imoh'ement. Single-variabk analyses, such as described above, are sometimes miskading because of the confounding effects of other variables, The multivariate analysis
.\" ' f '71 \
.," 4"
4 1 t 4+
(,+ 7"
10-167-10.0" 31· 0" 6" 3-9" 6-
10" 24-12· 4.5-
I ;S-S-
II-S"
24-16-II-
18+ 9+ 5+
13.S+ 12-10· 6;
. ,r ,"'
~~
21'-(, :,
<)4
38 :'8 10~
15 11 S7
:, 13
i
20 53 S": 38 4S 99 21 65 ,0 2:!
39 31
182
20 5 7
241 86 13 60
,;. \' \)i"; I; ,'PI
0 n (I
0
0 0
111 111 0 0
° 0 0
° 0 0 0
111 0 0 0 3
111
o
~I 111 111
indicated that (I) stage of tht' primary tumor, (2) number of metastases, (3) presence of a metastasis greater than 8 em in size. (4) disease-free interval before hepatic resection, and (5) age older than 70 were independent prognostic determinants of survival. All of these factors, except for age. were highly significant I.p < 0.01) in the multi\'ariate analysis. Age was of borderline significance I.p < 0.05). The analysis indicated that there is a gradation of risk associated with an

~ .
.-
•
--_._-----
2R4 RrgD/'1 (~f IIrl'alll .\lrlal/ClI'-'
Table III. P()tenllall~ re~( tahl~ IiHT
meta~tas~5 Idt In Situ· «('Ondrn5~d fr(lm Tahle II)
Sllr; I: .,:, y. ----------
Slae. . \ I, ::';-1 .'1. a' . f' .. ,,",!I
Allf II . \~ (, . 1.11< b-.\
SOlilU\ 1011
Lo( ahzrdj: (,. ~4 11' 142
5· \ 7
~ ~. ,; l: . . , 9; 1 ~ 1 ~
·P·lman tumor '1'mr'lnl("~ Iff: Ir, \1:LJ 'c.ton(l: rI:tlr~rnil.l\r fron, r(p,'r~:
["', lint' app.lfrnl!\ un~f"(,,«"lldhlr, 4.U(~, ,1" ""Idrl.t'rr,trl' "'., ">:,:..ro-, "Bll, )\UIJf ,")\ t' "2:" ....... "mul, qdr ,"'" and . '\.(" \ ('r,)i
tThnr "("fir" d{· nil' fur:hrr .. uhdl~ldr r).l("r1l (1f InrI rrpld'rmrn:
tonh ;~rtT pr0\rd .)1 hIlT"\
§~(ll fU1.\("d at hlnp .... \ IPn(ludr" "\oc.llizrd .. ' ··<~-"I"CI •. ,~ <4,1. l ndr,bulJ:'''" and "ft'" "M
increasing number of metastases: one. two. three, and greater than or equal to four. The analysis also indicated that the less favorable prognosis associated with the presence of a metastasis of at \east 8 cm was not limited to solitary metastases, this probably was also the case for patients with two metastases. Large size does appear to have a detrimental effect, but even this set of data is inadequate. with the current limited degree of follow-up, to determine the exact nature of this interaction between size and number of metastases.
The predictions based on the multivariate model indicate that patients with stage C disease and three or more metastases do extremely poorly. In our data there are no patients with stage C disease and three or more metastases who have survived 5 years. The model predicts that the 5-year survival rate for stage C patients with three or more mt'tastases is less than 100/0, even if the disease is metachronous. For patients with synchronous stagt' C disease, who art' either older than 70 or have a lesion greater thar, 8 em, the predicted 5-year survival rate is less than 151fo, regardless of the number of metastases. Patients with stage B disease and fewer than four metastases are predicted to have relatively good ,-year survi\'al probabilities These probabilities are reduced substantially for those with large metastases or for those older than 70 and are increased for those with metachronous disease. The predicted probabilities of 5-year survival and diseasefree survival are limited in precision bera '.lse of the limitation of follow-up of these patients.
DISCUSSION
Approximately 40,000 persons with colorenal carcinoma die of hepatic metastases each year. The only curative treatment currently available is hepatic resec-
.\r., .... r-. ,\1,;'. f. /<:.11'
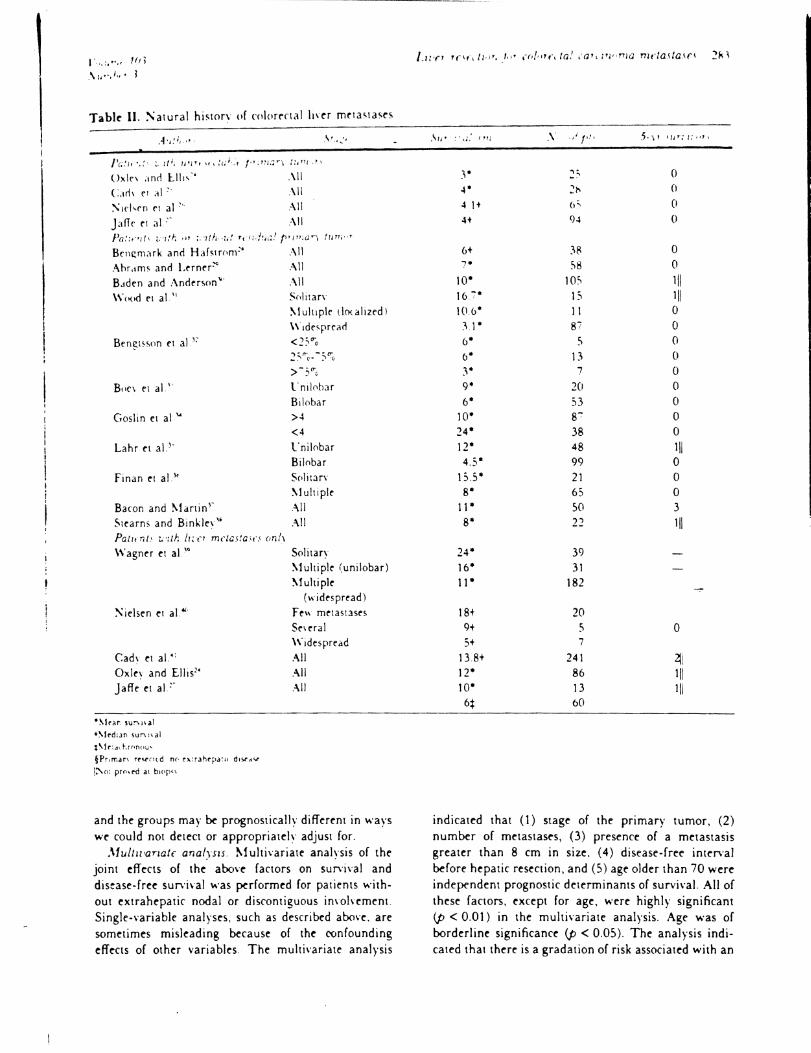
tion ThiS study has dC'momtrat~d a 5-p~ar sunl\al rate- of 3:\~o, which should be C'Ompar~d with thenume-rous studl~s of th~ natural history of he-p,,:i( m~taqasC's for colore-etal canr~r that comistc-nth show fe-w or no patients sun'i\'ing bqond :\ ye-ars Of 16S0 patients with untreated colorectal metaqases to the IiH'T reponed in the literature (Table II )~. ", th('rC' ar~ onh four who sunived beyond::' years with histologically documented metastas~s and an additional s('\en who survived beyond 5 years without biopsy proof of hepatic metastases. These 5-year survivors all ultimately died of hepatic metastases, and no chemotherapeutic regimen has improved this situation.
We can limit this literature review to dis~ase that was potentially excisable by exrluding what appear to be "unexcisable" metastases, such as "primary tumor left in plact'," "multiple liver metastases," and "widespread liver metastases," (Table III). This reduces the number of evaluable cases but does not remove any ,-year survivors. There are 11 5-year survivors here. but seven did not have hepatic metastases proved at biopsy and may not have had liver metastases at all. (Bengmark and Hafstrom~' found a 5% to 8% rate of false-positive diagnoses of liver metastases by surgical palpation when biopsy was not performed.) We find, restrospectively, that there is a 1 % to 2"10 ,-year sun'ival rate in this collected series. When we include three case reports from the literature of long-term sun'ival with biopsy-proved liver metastases'·': .' (all three with widespread and unexcisable metastases). we still have only 14 5-year survivors in the Englishlanguage literature, and all died eventually of cancer. Com part' this with the 88 ,-year survivors after hepatic reseCtion reported here, 58 of whom remain fret' of disease to the present time.
In interpreting our rt'sults in terms of recommendations for which patients should undergo hepatic resections, we are implicitly employing a historical control group. It has been documented that patients with onlv a few metastases confined to the liver have a favorable natural history compared wtih all patients with hepatic metastases.}l }Q 4{. and no on~ doubts that patients ..... ho undergo hepatic resections are a selected subs~t. !'Oe\ertheless, the available published lit~rature suggests that the ,-year sun'ival rat~ even for this subset. if untreatt'd, does not exceed ,lfo 10 10'70 (Tables II and III). Hence we belie\e that the survival rates reponed here indicate that hepatic resection has in fact r~sult~ in patient benefit.
Despite the lack of efficacy of any other treatment, physicians continue 10 avoid hepatic resection. When it is considered that in the United States approximateh

1',,/ /, "" 1(';
10,000 pJ'lmt. ~arh year ar(, candldate-~ for he-patic rcsC(!Jon and th:l1 onh approxlm.11ch I,O{l(1 patients per Har anualh' undrrgo re~cCli()n, it I~ ob\iou~ that thl~ pr(>(rdurc IS shunnt'd by thr maJorm of ph\sicians
In r\aluil1Jng the d~mahilit\, of rest'ction for an indi\ldual patit'nt, one must take into ac(()unt the risk of operative mortality, thr likelihood that the patient's disease will be found removablr and the likelihood that the patient will be in a prognostic subset for which a meaningful 5-year survival rate after resection is obtainable It is generally reported that SO'7o or fewer patients operated on are found to be eligible for resection.:' Increased ability to predict successful resection preoperatively awaits improved diagnostic methods Even if the surgical mortality ratr were 10%, a s-p'ar survival rate of 2~lfo to 30"'0 after hepatic reseC'tion still represents a rate of 22':0 to 27'70 when corrrned for surgical mortality. Such rates make hepatic resection appear to be a worthwhile procedure, especiallY when we consider that operative mortality rates of much less than 10lfo are common in major centers ~evertheless, it was our belief that the risk! benefit ratio could be improved if we could identify subsets of patients who did poorly aftrr hepatic resection, as such patients could be spared the procedure. \\'e also would like to reemphasize that this series represents prognostic factors in those patients SUT"<'l1'lng
the resection. It is not the purpose of this article to discuss the morbidity and mortality of he-patic resection, as this has been addressed in several previous articles.}.· The individual surgeon must determine not only whether his patient falls into a good prognostic group after resection but also whether his patient can come through the procedure with an acceptable risk of morbidity and mortality. For example. though patients olde-r than 70 years appear to have a good prognosis, not all patients more than 70 years old can withstand this major procedure.
We hoped that the results of thIS multi-institution r('Vle-w would help elucidate the indications and contraindications for hepatic resection. Thr numerous series that have appeared in the literat ure over the past 10 years have been relatively- inconsistent in their conclusions because of the inability of any single institution to accumulate a large enough sefles of patients to answer questions definitively.~·~' Though this is a retrospective collection of data that includes patients treated by many different surgeons at 24 separate institutions, all patients are similar in that they ha\'e undergone curative excision of all gross disease We believe that this analysis has been successful. but even this large
serie-s leave~ some questions unanswered First, even a serir~ a~ lar~r as thiS is n(lt sufllClt'nt to allow us to look adequJtrh at comhinations of facton or e'en some low-freque-nn subsets of a sim:ir factor. Second. in re-trospnti\e mulll-instituticlD studit's that cover a long period of time suhstantial amounts of data on factors of interest are missing Third, the patients who have undergone hepatic resection constitute a selected sample and thr selection factors probably differ across institutions and years. This last point must be borne in mind as a caveat for interpretation of the prognostic evaluations. For example, the bilobar patients who underwe-nt rese-ction are not a random sample of "resectable-" bilobar patients, but they may have been selected on the basis of factors that are not all identifiable-. and the-se patients could have a betler prognosis than those selected for resection in the future.
We have identified a number of factors that influence prognosis after hepatic resection. The only factors that might be considered by themselves as eontraindications to rese-ction are the presence of positive hepatic nodes, the presence of extrahepatic metastases (even if removable), or the presence of four or more metastases. ~fany other factors did act, however, as prognostic indicators and should be considered in combination in evaluation of the possible benefits of resection.
Those factors that have some effect on prognosis include- the pathologic margin of the liver specimen. Patients with a greater than I em margin had a 4S~0 S-year survjval, whereas patients with a margin of 1 em or less had a 23% 5-year survival. Data on margin width were unavailable for most of our cases, Hence we could not include this factor in our multivariate analysis Margin should be taken into account as a stratification faclOr for a prospecti\'e re\'iew, and our analysis would suggest that a 1 em margin be obtained whenever a liver resection is performed At this time, however, this margin d~s not act as a contraindication to resection. even if a 1 em margin cannot be obtained. There are not enough patients with a lesser margin for us to adequately estimate their 5-year sun'i\,al rate. but there are ~-year sur\'ivors with such margins.
The stage of the primary tumor d~s have a strong effect on sun'ival. Patients with stage B primary tumors do much better than patients with stage C primary cancer. Although the patients with a Dukes' C primary tumor do have a reasonable 5-year sun'ival overall, our multivariate analysis suggests that those with multiple metastases and synchronous disease are not good candidates for resection Further follow-up will help clarify this.
The disease-free interval d~s act as a prognostic

j ,
indicator. Patient~ with a longn dISC'3sC'-frrr InU'rval have an impnwrd sunl\al whC'n comparrd ..... ith patiC'nt~ with a bnd di~easr-frre intenal The prr,ence of synchronoU' mrtastases is not in itself sufflcirot to ('Xclude patient< from hepatic resrnion. but thi~ must be romldered in ronjunction with othrr fa(!ors
The sIze of a solItary metastasis d~s seem \() affect surviva\. in that patients with yen large metastases (greater than 8 em) will fare worse than patients with small metastases. The number of patients with very large metastases is not adequate to enable us to precisely estimate their 5-year survival rate; ho ..... ever, the actuarial estimate at this time is 2~% Hence it does not seem appropriate to employ this factor in itself to deny patients hepatic resertion Reanalysis with further follow-up may provide additional guidelines in the f ut ure.
CEA does appear to affect long-term survival but the manner of patients is small, and we would be cautious suggesting that low CEAs will lead to a better longterm survival.
The type of resection that should be JXrformed has been debated in the past. The consensus has been that it is unimportant ..... hether a wedge resection or a lobectomy is performed. The data from this registry are in general agreement with that conclusion. It ..... ould appear that patients who undergo a wedge resection will fare the same as patients who undergo a lobectomy ..... hen only small solitary metastases are considered. However, patients with large solitary metastases (greater than 4 cm) do seem have a worse prognosis when undergoing a wedge resection. Patients undergoing anatomic resections, however, have more favorable prognoses with respect to stage of disease and free interval. We attempted to adjust for this imbalance and still found that those patients undergoing wedge resection appeared to do worse. We think that this is due to an inadequate margin on the metastases, since it is difficult to do a large wedge resection without coming close to the tumor at some point during the dissection. \"hen we consider our eXJXrience that anatomic resections are often less complicated and cause less blood loss than large wedge resections. we recommend that patients with large metastases (greater than 4 cm) undergo anatomic resection, even though this nonrandomized evaluation cannot be definitive. In addition to gi\ing an improved pathologic margin, this also will most likely decrease complications and blood loss.
Our analysis pro\ided no evidence that the presence of bilobar disease is a prognostic factor. There were only 79 such patients. however, and their long-term survival and disease-free survival cannot be estimated
St,'C o • . \f,,·,f; 19~,~
without furthrr follow-up. At this time, howner. wr srr no rrason to takr bilobar disrasr is a contraindication to resertion
Patirnts with Pnrtastatic disra~e in hrpatic or crliac nodes havr a significantly decrrasrd sunival drspite node dissrction. Wr thInk that these patients should not undergo hepatic resection. rxcept a~ part of a trial with adjuvant therapy. since resection alone is not adequate treatment.
Patients with extrahrpatic metastases resectrd simultaneously with liver metastases do appear to have survivals similar to those of patients who do not undergo extrahepatic resection, although with only 37 such patients we cannot say this conclusively. The diseasr-free survival of these patients is decreased. however. From the results of this review, we would recommend that patients who have simultaneous extrahepatic disease that is removable should undergo both liver resection and removal of the extrahepatic disease as part of a prospective trial of adjuvant therapy.
The number of metastases excised was also found to be an important prognostic factor. In this series, patients with three or more metastases did worse than patients with one or two metastases. The multivariate analysis suggested that prognosis decreases continuously as the number of metastases increases from one to five. That analysis suggests that stage C patients with multiple synchronous metastases are not good candidates for resection but that stage B patients with one to three metastases are. The precision of these predictions is limited by the small number of patients with multiple metastases and the amount of follow-up. We recommend that patients with three or more metastases should undergo resection only as part of a clinical trial and that for patients with two to three metastases the decision should take into consideration other factors, such as stage. disease-free inten'al, size, margin, and age. The effect of number of metastases should be reexamined in the future, with further follow-up of these patients.
Many of our patients underwent chemotherapy before and after hepatic resection. Agents included 5-fluorouracil, FCDR, methotrexate, and mitomycin C. Routes of administration included hepatic artery. portal vein. systemic vein, and intraJXritoneal In this retrospective review the variability between route of administration and drugs used was too great to permit us to come to a firm conclusion as to whether chemotherapy improved prognosis It is beyond the capability of this analysis to confirm or deny the value of chemotherapy combined with hepatic resection; however, this question has been addressed by several of the
j'plum. 103 Sumhr-. 3
ro-authors of this article in singl~-institutlOn series Fortner et al.: tried both intra-arterial and IntrafXlnal chemotherapy after resection, but in the absence of a concurrent control group no definite roncJusion can be drawn regarding its efficacy August et al < found a suggestion of lessened survival ..... ith use of intrapc-ritoneal S-Auorouracil after resection, and this is currently undergoing a randomized trial at the :\ational Cancer Institute O'Connell et al. ... administered intravenous 5-Auorouracil and semustine after hepatic resection and found no improved survival compared ..... ith a historical control. Currently there is no evidence that chemotherapy after hepatic resection ..... ill improve survival; patients should receive chemotherapy only as part of a randomized trial.
REFERENCES
A,ugust OA. Otto" RT. Sugarhaker PH Cltnl(al ~rs~ctl\e,
on human colon can('~r metastas~s Canc~r ~Ictastasl' Re\ 1984,3.303·24.
2 Fortnn JG, Silva JS. Golbn RB. Cox EB. Macuan BJ Multi·variate analvsts of a ~rsonal ~ne, of ~4- cpnscrutl\e pallents with It\'er metastas~s from rolorcnal cancer. Ann Surg
1984,199306·16.
3. P~trelll 1'J 1'ambisan R~. Herrera L. ~lll!dman A. Hepatic resection for isolated metasta~s from colorenal carcInoma Am J Surg 1985.149205-<1
4. AdS<ln MA, "an Heerden JA. AdS<ln ~IH. Wagner JS. llstrup O~! Resection of hepatic metastases from colorenal cancer Arch Surg 1984,119.&47
5 August DA, Sugarbaker PH. Ottow R T. Glanola F j, Schneid· er PD Hepatic resection of colorectal metastases inAuen('( of
cltnlC41 factors and adju\'ant intra~ritoneal 5·Fl· via Tenck· hoff C4thrter. Ann Surg 198",:!01.210-8
6 CadI B. ~lcDcrmou w\' ~Iajor hrpall( r~srnJOn for meta·
chronou! m~tasta~' from rolon cancer Ann Surs: 1(8),201 204.9
7 Kamoouris :\A The role of major h~palic resectlons for hvcr
mrtastases from coloreetal cancer Henr; Ford Hosp !l.led J 1983;3125
8 Lim C. MrPhuS<ln TA Surg~n a~ an altnnatl\e to chemo·
therapy for hepauc metasta~s from colorectal C4nrer Can J Sung 1983,26458.
9 Brngmark S. Hafst rom L. Jeppswn B. jc>ns<,('\n P. R \'der. S. SundqUIst K !'-Irtaslatlc d"ease In Ine lIver from col",e('\al
cancer An appraIsal of !tIer sungen World J Surg I QS2;6 61
10 Butler J Aui,'eh FF, Dah J!'-1 Hepatic resection for mcta!· lases of the colon and rectum Surg G,necol Obslct 1986,162109·113
II Gennan L. Doci R. Bignami P. Bourt:1 F SurgIcal treatment of hrpallc metastases from colorectal C4ncer Ann Surg 1986.20349·54
12 Coppa GF, Eng K. Ranson JHC. Gonge TH. Locallc, SA
Hepatic re~rtion for metastatic colon and r~ctal canctf An e\aluation of preoperalive and postc'peratlH fanors Ann Surg 1985,202.203-8
13 Kortz Wj, Meyers WC. Hanks JB. Schirmer BO, Jones RS
HepatJ( re,rrt"'~ 1M mrtd<tdtl< canrrr Ann ~ur~
lQ~4.IQQ I"~·tl
14 Steek C;. ~tcen RT Wd .. N: RE rl al Patlrrn< of f.dure .. fler
surglcdl cure of lar,!, !tICr tumnn Am J ~ur!( 191<4. 14-
'~4.9
I~ Toma,·dr la \·C!(.l ]E. DnnJhue EJ. Do"!.,, A. rt al A ten ~'ear experIence "\t~. hepa:lc resrfll0n Sur!: G,nnol Oh,trt
1984.150 2~\·~
16 !'-lorr0w CE. Grage TB. Sutherland [lE. ~apflan JS Hepat.
IC resrctl0n for st('Dndan ncnplasm< 5t ~(.f.R \ 19~3.92
610·4 17 Th0mps0n HH. Tompklm RK. Longmire WP ~lajor hepatIC
resecoon A 2~ ,ear experience Ann Surl!, 198.'.1973~'·88 18 (watsukl S. Sha" B\\'. Starzl TE Experienrr with 1~0 h"er
resections Ann Surg I Q83.19i24i·:'3
19. Tal'lor B. Langer B. Falk RE. Ambus l' Role of resenion in the manas:emmt of meta,lase, to the liver Can j !l.1ed
1983.26 215·"
20 Blumgar: LH. Alltson Dj Reserll0n and emb.:,lizaoon in the management of ~[(1ndan hepatJ( tumors. World J Surg 198~;6 32(1.4.,
21 Fostcr JH. Lund\ J Patholog\ of h'er metastasIS Curr Prohl
Surg 1981.18 1~-·~OO 22. ~Ims TA. Resection of the livcr for metastatic cancer Surg
Gl'necol Obstet 1984.15846·8
23. Cox DR R~gression ~Iodeh and Life Tables. J Royal Stat Soc. Sems B. 19-2,34 18-·220
24 Oxlcv E~L EllIS H Prog:nosis of (afClnOma of the large bowel
in the presence of h,er metastases Br J Surg 1969.:'6149. 52.
25. ~ielsen ]. Balslc\ I. Jensen HE Carcinoma of the colon with liver mctastases :\cta Chir Scand 1971.1 r 463·:,
26 ~ielsen j. Balsle\ I. Jen~n HE Carnnoma of the colon wilh liver metastases :\cta Chir Scand 1971;lr463·'
27. Jaffc B~1. Donegan WL. Watwn F, Spratt JS. factors
inAu~ncing sun'ival in patients with untreatr-d hepatic metasta· ses Surg Gynerol Obstet 1968.12il-11.
28 Bengmark S, Hafmom L The natural hiswn of pnmary and secondan ma"~nant tumors of the liver I The prognosis for
patients with hepam metastase, from colonIC and rectal carci· noma by laparotom\ Cancer 19-0.23198·202
29. Abrams MS. umer HJ Sunl\al of pallents at Pcnnsll\'anla hospital with hepauc metasla~s from carcinoma of the colon and rertum DIS Colon Renum 19:1,14.431-4
30. Baden H. Anderson B Sun'i'al of patients with untreated liver
metastases from colorenal C4nccr. Scand ] Gastrocntcrol 1973;10221·3
31 Wood CB. Gtlils CR. Blum~ar; LH A retrospertiv'e stud, of the natural hlston of pauents iwth !tHr metastases from colorenal cancer J Cltn Oneol 19'76,2:!8~-8
32 Bengtsson G. Carlsson G. Hafstrom L. johnS<ln P 1'atural histon of paticnts with un;reated !t\cr metastases from color· enal cancer Am J Sur~ 1')81.141 ;86·Q
33 Boc\']. Cnol TK. Wong J Ong GB Cam noma of the colon and ITCtum wlln Ii\'er Inv'ol,ement Surg Gynecol Obstet 1981; 153864-8
34 GoslIn R. Stede G. Zamchcck :\. Ma)er R. ~laclnt\Tc J Factors influencing sunival in patients wnh hepau( metastases
from adenocarCInoma of the colon and r~flum Dts Colon Rectum 1982.25 7 49.,4
35 Lahr Cj. Smng S.]. Cloud G. Smlln jW, Lrist MM. Balch CM A mulufanonal analYSIS of prognostic factors in palients
"" lin jl\rf mrta\uv\ (rpm (lllpr('f'ldl ran Inf,m,1 J Chn ()ncol
1 I)~ \,1 - ::,,,.(,
3<> hr"", PJ \\."h.111 RJ. (:'.'1)("' Ell. (;d~, (:R }-<tl\"r'
aflr\:lnliZ, \unl\allr. p.t~lrn!t "lIh s\nchr(,n.ln<.. hrp.\:1( mrl.·p.·
Idc"t"'" frpm rcdflrr-i1.11 (iinefr :\ (hnhrl! ann (omputrr a-n;,h"'ls
BT J "un: lQ~, -: '-'.-
.'1 - B .• " 'n H L 'I.IC"" 1'\ Thr r d', ,,'n .. I, of p.tlh;l: II r r,'rel"'" fOJ
rrim,}f\ {aOln t""\( thr (\II(\Jl ann frnum {'(lnlpIH.I1t-rl h~ h\("r
ano lun~ mr:.t<' .. "" I)" C(ll"n Rr<:um 11)(,4,- 211·-
~R SI('drn, \\\\', Blnklrl (,r Palhalllr sur~fr\ I", (anirr (,f Ih~ r~cum and cnl"" Can"r 11);4,- WI('·O
.'\9 \\a~nrr JS. Ads"n \\'\ v;In H~rrdrn J:\, Ads('n \HI, II 'If up
D\\' Th~ natural h,slon of hrpJII\ mrlastase, lrom colorfll;;1
canerr Ann Sur~ 11)84199 :'02·fI 40 ",~Isrn J Balsl~, I. Jrm('n HE Carcinoma 01 Ihr colon with
11\., mrlastas" :\rla Ch" Srand 19-1,1 r .46'\·"
.\"',I:r"l .\1. .. , t, 19U
~I (:ao, B. \\""',,', DO ,"'""n!on ,,\\ SUr>lIal of p..:,rn:, .. f,,· n.J(lnH rr· ... r( llfifl for (.H( lfillrTl.l \"11th ~"mull..tn("(lu\ li\rr mr:tl~
Id'" ~ur~ C;,nr,,,1 (It",,: 1'1-11,1.11 (",-.-O()
~~ '\:ll\rh l-l-, '\ and., HJ Slr.Hn, \\'\ Hq'JII' '''', \I,)r, f,,: mr~.~c.;.I~I' (rom rnt(,rrr:.11 can(rr I)I~ C(.\r.n Rr\ :rur..
1'1-1<'1 1()f\·2
4'\ Ltl tnr :\ \\. D, 'nrc ,II \\'1. ) r" In \ \ '\drn",If' tn\ ,m,t (>f I hr
('<.1,·., ""h hrrJ:.' mr:J"."r~ hflrrn 'rM sUC\IIJI J \\\ \ 1<)~2.:~- 2R(I'J.1f1
44 O'C"nnrll \\ "d~\'n \1. Schutt -\, Ruh.n J \\'oCr:d C. )J<1'U~' D ("hnt( al I flal (>f ad lUI ,I n: chrm(>: hrrap' aft" ,ur~""
rt~r(\I(>n of col"rr(1al rancrr mrtJ"JIII \(' Ihr h,t! \1a", Clir. Pr<)( 11)8~,6[) ~1-·2(1























![;Ti~;{'.i]W;;t ~~ 1, . . .- ',·';,)':1 I](https://img.pdfslide.us/doc/110x75/621a9acc6da7ac599a3e1ba4/tiiwt-1-1-i.jpg)