-
7/31/2019 1996 a Novel Computer-Assisted Volumetric Stereotactic
Approach for Resecting Tumors of the Posterior Parahippo
1/6
UMORS of the posterior parahippocampal gyrus rep-resent a
formidable technical challenge to neuro-surgeons. The proximity of
such lesions to vital
structures surrounding the posterior mesial temporal lobein the
dominant hemisphere, including the brainstem, cra-nial nerves,
posterior cerebral and anterior choroidal ar-teries, basal vein of
Rosenthal, as well as the vein ofLabb and the language cortex,
raises the possibility ofpotentially disastrous operative
morbidity. Several surgi-cal approaches to this region have been
described for
resecting epileptogenic lesions in the amygdala and
hip-pocampus.3,8,1214,16,17 However, these approaches requireeither
resection or significant retraction of eloquent cor-tex and have
been associated with several postoperativecomplications, including
dysphasia and visual field de-fects. Moreover, exposure of the
posterior hippocampusby means of an anterior approach is
technically difficult. 8
Using both computer-assisted stereotactic and micro-surgical
techniques, the senior author (P.J.K.) has imple-mented a novel
approach for volumetrically resectingtumors of the mesial posterior
temporal lobe and parahip-pocampal gyrus. By avoiding resection or
retraction of thetemporal lobe, this approach avoids injuring
surroundingneural and vascular structures. In this report, we
describe
our recent experience using this lateral occipitosubtempo-ral,
computer-assisted volumetric stereotactic approachin seven
patients, all operated on since 1994 by a singlesurgeon.
Clinical Material and Methods
Patient Characteristics
Seven patients (six males and one female) underwent
stereotactic resection of posterior mesial temporal lobetumors
via a lateral occipitosubtemporal approach. Theoperations were all
performed by the senior author (P.J.K.)at New York University
Medical Center between January1994 and March 1995 (a 15-month
period). Clinical infor-mation pertaining to these cases is
summarized in Table 1.Patient ages at presentation ranged from 15
to 67 years(mean 39 years). Five tumors were located in the
domi-nant (left) posterior hippocampusparahippocampal gyrusand two
were located in the nondominant (right) hemi-sphere. Three patients
presented with seizures, one withvisual field loss and hemiparesis,
one with visual field lossand dysphasia, and one with headache. One
patient har-bored a tumor found incidentally.
J Neurosurg 85:272277, 1996
272
A novel computer-assisted volumetric stereotactic approachfor
resecting tumors of the posterior parahippocampal gyrus
HOWARD L. WEINER, M.D., AND PATRICK J. KELLY, M.D.
Department of Neurosurgery, New York University Medical Center,
New York, New York
The authors report their experience using a novel surgical
approach for resecting tumors located in the posterior
parahip-pocampal gyrus. Prior attempts to resect epileptogenic foci
in this location have been limited by a significant risk of
injuryto lateral temporal lobe cortical and vascular structures. To
avoid these potential complications, the authors have used alateral
occipitosubtemporal, computer-assisted stereotactic volumetric
approach to resect radiographically defined tumorsin seven patients
with intraaxial neoplasms of the posteromedial temporal lobe. This
series included one female and sixmale patients, ranging in age
from 15 to 67 years, who presented with seizures, visual field
loss, or headache. Gross-total
resection of three high-grade gliomas, two gangliogliomas, and
one mixed glioma was accomplished with no permanentmorbidity or
operative mortality. The authors conclude that this approach is
advantageous for resecting tumors in this loca-tion because, by
avoiding unnecessary brain resection or retraction, it
significantly reduces the risk of injury to lateral tem-poral lobe
structures, helps maintain precise spatial and anatomical
orientation for the surgeon, and, like all computer-assisted
volumetric approaches, delineates the margin between the tumor and
surrounding neural tissue.
KEY WORDS brain neoplasm computer hippocampus stereotaxis
temporal lobe
T
J. Neurosurg. / Volume 85 / August, 1996
-
7/31/2019 1996 a Novel Computer-Assisted Volumetric Stereotactic
Approach for Resecting Tumors of the Posterior Parahippo
2/6
Several patients were referred for stereotactic volumet-ric
resection after previous neurosurgical interventionshad failed. One
patient (Case 1) had undergone previousstereotactic biopsy and
radiation therapy at another insti-tution followed by stereotactic
volumetric resection of aright posterior hippocampal
oligoastrocytoma 30 monthsprior to his current admission. A second
patient (Case 2)
presented after undergoing stereotactic biopsy of a
domi-nant-hemisphere high-grade glioma at another hospital.Another
patient (Case 3) was also referred for stereotac-tic volumetric
resection of a dominant-hemisphere hippo-campal glioblastoma
multiforme following stereotactic bi-opsy at an outside
institution. A fourth patient (Case 6)was referred for resection of
a right hippocampal glioblas-toma multiforme after a stereotactic
biopsy performed atour institution revealed the lesion. A fifth
patient with adominant-hemisphere cystic ganglioglioma (Case 7)
hadundergone multiple unsuccessful procedures over a 10-year period
including: two subtotal surgical resections,three stereotactic cyst
aspirations, two stereotactic implan-tations of iodine-125,
fenestration of the cyst into the ven-
tricular system, and placement of an intracystic reservoir,which
eventually became infected.
The preoperative computerized tomography (CT) andmagnetic
resonance (MR) imaging characteristics foundin this group were as
follows: three tumors (Cases 2, 3,and 5) were contrast-enhancing
ring lesions with sur-rounding T
2prolongation (Type II); two (Cases 1 and 4)
showed T1
and T2
prolongation but no contrast enhance-ment (Type III); one (Case
6) had solid contrast enhance-ment with surrounding T
2prolongation (Type II); and
one (Case 7) showed homogeneous contrast enhancementwith an
associated cyst (Type I).4,5
Data Acquisition and Surgical Planning
The technical aspects of the computer-assisted volu-metric
stereotactic craniotomy have been described previ-ously.1,49 After
local anesthesia has been induced in thepatient, a CT- and
MR-compatible stereotactic headframeis attached to the head by
means of four carbon-fiber pinsinserted through holes drilled into
the diploe of the skull.Data acquisition is begun as the patient
undergoes stereo-tactic CT and MR imaging, followed by stereoscopic
dig-ital subtraction internal carotid and vertebral
angiography.These data are then transferred into the operating
roomcomputer system (COMPASS Stereotactic System; Ste-reotactic
Medical Systems, Inc., Rochester, MN). On theimage-display console,
the surgeon views each CT and
MR image that demonstrates the target lesion. A singlepoint
located in the approximate center of the lesion onone of the CT or
MR imaging slices is digitized and re-tained as the reference
target point. The most inferior andsuperior slices that demonstrate
the lesion are indicated,and the computer then reads in each
intermediate slice.Using the display cursor, the surgeon digitizes
successivetumor contours on contiguous CT and MR imaging slicesby
tracing the outline of the lesion. The interpolated CT-and MR
imagingdefined volumes are constructed aroundthe reference target
point, which is placed in the focalpoint of the stereotactic
arc-quadrant frame. The com-puter then reconstructs the digitized
CT- and MR im-agingdefined tumor outlines into a volume within
stereotactic space with reference to the target point.
Thecomputer can then slice these CT- and MR imagingdefined volumes
perpendicular to any specified viewlinethat is expressed in arc and
collar angles on the stereotac-tic instrument. Tumor volume slices
viewed perpendicularto an intended trajectory may then be displayed
with re-spect to the stereotactic trephine craniotomy (1.5- or
2-in
diameter) or the stereotactic retractor (2- or 3-cm diame-ter).
The tumor volume may also be superimposed on thedigital subtraction
angiographic images so that when plan-ning the operative
trajectory, the surgeon can avoid im-portant arteries, veins,
sulci, and gyri. The stereoscopicangiographic images of the
cortical arteries and veins helpto establish the sulcal
anatomy.
Data acquisition and surgery take place on separatedays. The
stereotactic headholder is removed followingCT and MR imaging and
angiography and is subsequent-ly reapplied at the time of surgery.
Detachable microme-ters that record the distance from the end of
the carbon-fiber pins to the vertical supports of the headframe
are
used to ensure precise replacement of the frame for
latersurgical procedures. Therefore, surgical planning can
takeplace at the computer console in a relaxed environment.
Surgical Procedure
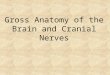
Figure 1 illustrates the operative approach to the poste-rior
parahippocampal gyrus that is made using a stereo-tactic volumetric
lateral occipitosubtemporal approach.Each procedure is performed
after general anesthesia hasbeen induced endotracheally in the
patient. The CT-com-patible stereotactic headframe is replaced
using the samepin placements and micrometer settings that were used
fordata acquisition. The patient is placed in the
three-quarterprone position, with the head rotated to the 135 or
225position for left- or right-sided lesions, respectively.
Afterinfiltrating the skin with 1% lidocaine, a pilot hole
isdrilled at specified arc and collar angles, and a vertical
lin-ear skin incision is made. A 2-in diameter trephine cra-niotomy
is performed in line with the selected trajectory,and the dura is
opened in a cruciate fashion. The trephineis positioned so that its
diameter is two-thirds above andone-third below the lateral sinus,
approximately half thedistance between the torcular herophili and
the vein ofLabb. To avoid potential sinus laceration, extreme care
istaken to ensure that the trephine axis does not depart fromits
perpendicular orientation to the skull or inadvertentlyextend too
deeply. This routine maneuver has resulted in
no sinus injuries. Dural tack-up sutures are used to retractthe
lateral sinus inferiorly. Relaxation of the posterior tem-poral
lobe is facilitated primarily with the aid of reverseTrendelenburg
positioning, propofol-induced anesthesia,and hyperventilation to a
PCO
2of from 25 to 28 mm Hg.
Continuous drainage of small amounts of cerebrospinalfluid from
the subarachnoid space during the procedurefurther facilitates
mobilization of the temporal lobe fromthe tentorium. This maneuver
has not resulted in a signif-icant intraoperative shift of
structures with respect to theimaging data and, therefore, has not
compromised theaccuracy of the stereotactic approach in any of the
cases.The vein of Labb is identified and preserved. Smallerdraining
veins from the posterior temporal lobe to the
J. Neurosurg. / Volume 85 / August, 1996
Lateral occipitosubtemporal stereotactic approach
273
-
7/31/2019 1996 a Novel Computer-Assisted Volumetric Stereotactic
Approach for Resecting Tumors of the Posterior Parahippo
3/6
-
7/31/2019 1996 a Novel Computer-Assisted Volumetric Stereotactic
Approach for Resecting Tumors of the Posterior Parahippo
4/6
The follow-up period for this study ranged from 4months to 18
months (median 11 months; mean 8.4
months). No patient died or experienced permanent mor-bidity.
The five patients who were neurologically intactpreoperatively
experienced no new neurological deficitsafter surgery. One patient
(Case 7) who had a right hemi-paresis preoperatively was initially
worse following sur-gery. However, she experienced progressive
improvementin her power and was eventually discharged on the
7thpostoperative day neurologically unchanged. Another pa-tient
(Case 5) who presented with a superior right quad-rantanopsia
experienced transient postoperative visualworsening in the inferior
quadrant as well, which resolved1 week after surgery. Two months
after surgery, one pa-tient (Case 3) experienced a marked
progression of histumor while undergoing chemotherapy; since then
hehas required continual steroid administration. The
patientsdiagnosed with glioblastoma multiforme and
anaplasticastrocytoma were each referred for radiation therapy
andchemotherapy.
Discussion
Exposure of the posteromedial temporal lobe has long
been considered technically challenging.8 The proximityof this
region to the midbrain, crural and ambient cisterns,anterior
choroidal and posterior cerebral arteries, and thebasal vein of
Rosenthal mandates precise anatomical lo-calization and spatial
orientation by the surgeon. More-over, standard approaches to this
area have been unsatis-factory insofar as each has necessitated
either retraction orresection of lateral temporal cortex, risking
speech andvisual field disturbances or potential injury to the vein
ofLabb. Neurosurgeons have gained access to the region ofthe
posteromedial temporal lobe via transsylvian, trans-cortical, or
subtemporal approaches. The majority of ap-proaches to this area
already described have been directedat the removal of foci of
seizure activity in patients withtemporal lobe
epilepsy.3,8,1214,16,17
Wieser, Yasargil, and others8,16,17 developed the trans-sylvian
approach for selective amygdalohippocampecto-
J. Neurosurg. / Volume 85 / August, 1996
Lateral occipitosubtemporal stereotactic approach
275
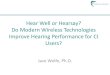
FIG. 2. Case 6. Preoperative (A and C) and postoperative (B and
D) axial and sagittal magnetic resonance imagesobtained in a
67-year-old man who underwent resection of a contrast-enhancing
glioblastoma of the right parahippo-campal gyrus.
TABLE 1
Characteristics of seven patients undergoing lateral
occipitosubtemporal computer-assisted stereotactic
volumetricresection of posterior parahippocampal gyrus tumors*
Case Age (yrs), CT/MR Imaging Type of Finding at Follow Up,No.
Sex Location Diagnosis Presentation Characteristics Resection Time
Postop
1 19, M rt PHG mixed glioma GTC seizure; nonenhancing GT
neurologically intact,neurologically intact 5 mos2 61, M lt PHG
anaplastic incidental finding; ring enhancing GT neurologically
intact,
astrocytoma neurologically intact 4 mos3 29, M lt PHG
glioblastoma headache; ring enhancing ST recurrence, 7 mos
neurologically intact4 15, M lt PHG ganglioglioma GTC seizure;
nonenhancing GT neurologically intact,
neurologically intact 12 mos5 48, M lt PHG glioblastoma VF loss;
dysphasia ring enhancing GT neurologically intact,
4 mos6 67, M rt PHG glioblastoma CP seizure; contrast enhancing
GT neurologically intact,
neurologically intact 9 mos7 35, F lt PHG ganglioglioma VF loss;
hemiparesis cystic/contrast GT hemiparesis, 18 mos
enhancing
* CP = complex partial seizure; CT = computerized tomography; GT
= gross total; GTC = generalized tonicclonic seizure; MR =magnetic
resonance; PHG = parahippocampal gyrus; ST = subtotal; VF = visual
field.
-
7/31/2019 1996 a Novel Computer-Assisted Volumetric Stereotactic
Approach for Resecting Tumors of the Posterior Parahippo
5/6
my to minimize temporal neocortical resection, leavingthe
lateral surface of the temporal lobe intact and sparingspeech
functions of the dominant hemisphere. This ap-proach involves
opening of the sylvian fissure, subtotalresection of the amygdala,
and hippocampal and parahip-pocampal resection through the temporal
horn.3,16,17 Find-ing this anterior approach to the mesial temporal
struc-
tures to be encouraging in the control of complex
partialseizures of anteromedial origin, Kelly, et al.,8
nonethelessemphasized that exposure of the posterior hippocampusby
means of this anterior approach is not adequate.
Spencer and associates14 described a technique forachieving
access to posterior medial temporal lobe struc-tures in patients
with unilateral posterior hippocampal sei-zure foci. Their modified
anteromedial temporal lobecto-my consisted ofen bloc removal of the
anterior middleand inferior temporal gyri, retraction of the
remaining lat-eral temporal lobe, and resection of the posterior
hip-pocampus or posteromedial temporal intraaxial mass.3,14
However, this approach is not optimal because it requiresnot
only an anterior temporal lobectomy but also retrac-tion of the
remaining posterolateral temporal cortex witha self-retaining
retractor.
Similarly, transcorticaltransventricular approaches tomesial
temporal structures all require some resection ofcortical tissue,
as well as disruption of white matter fibersof the temporal stem.3
The transventricular amygdalo-hippocampectomy described by
Niemeyer,10 in which acortical incision was made in the middle
temporal gyrus,preserves the superior temporal gyrus; however, it
neces-sitates significant resection of middle and inferior
tem-poral white matter to gain access to the temporal
horn,amygdala, hippocampus, and parahippocampal gyrus.3,10
Olivier11 described a similar approach through the supe-
rior temporal gyrus. His technique involves resection ofthe
anterosuperior temporal gyrus, followed by aspirationof the
amygdala, opening of the temporal horn, and resec-tion of the
hippocampus.3,11 Shimizu and colleagues12 ap-proached the mesial
temporal lobe through the inferiortemporal gyrus, following removal
of the zygomatic arch.
Kelly, et al.,8 have previously described a computer-assisted
stereotactic resection of the amygdala and hip-pocampus via a
posterolateral approach in patients withmedically intractable
complex partial seizures. However,because this transcortical
approach involved disruptionof the inferior optic radiations, all
patients in their seriesdeveloped nondisabling visual field
deficits in the imme-diate postoperative period. This
posterolateraltranscorti-
cal approach, identical to that used for resection of
intra-ventricular tumors located in the temporal horn or atriumof
the lateral ventricle, was selected to spare the corticaltissue
related to speech function.8,15 The lateral occipito-subtemporal
approach, described in the present report, isessentially a
modification of the posterolateraltranscorti-cal approach, designed
specifically to avoid disruption ofthe optic radiations as well as
of the speech cortex.
The subtemporal approach, as first described by Drake2
for use in treating basilar bifurcation aneurysms,
avoidsresection of cortical tissue. However, this
procedurenecessitates use of significant brain retraction to
gainaccess to tumors located in the posterior
parahippocampalgyrus.
Smith and Spetzler13 recently described a
supratentori-alinfraoccipital approach to posteromedial temporal
lobelesions, in which they used a viewing wand
intraoperativenavigational system for guidance. Their technique
differsfrom the one described here insofar as it is a
midlineapproach, which is performed through an occipital
cra-niotomy and which requires exposure of the falx, superior
sagittal sinus, torcular herophili, both transverse sinuses,the
occipital pole, and the great vein of Galen and its trib-utaries.
As they observed, the disadvantages of the
su-pratentorialinfraoccipital approach include the need
foroccipital lobe retraction as well as wide exposure of themidline
dural venous sinuses, with the inherent risk ofblood loss, air
embolism, and delayed sinus thrombosis.
The lateral occipitosubtemporal approach has not beenpreviously
described in the neurosurgical literature. Tak-ing into
consideration the limitations of previous tech-niques for gaining
access to this region, we believe thatthis route offers several
advantages. Because of its lateraloccipitosubtemporal trajectory,
it obviates the need forboth resection and retraction of brain
tissue and thereby
avoids potential damage to vital neurovascular structures,which
include the optic radiations, anterior and lateraltemporal cortex,
vein of Labb, the occipital pole, and themidline dural sinuses. As
noted by Smith and Spetzler,13
the surgical anatomy of the medial temporooccipital junc-tion is
not familiar to most neurosurgeons, particularlyas viewed from the
posterolateral approach, and the sur-gical trajectory is long and
narrow, limiting exploration.Therefore, some form of stereotactic
guidance is essen-tial, in either the supratentorialinfraoccipital
or the later-al occipitosubtemporal approach, to maintain spatial
andanatomical orientation. Smith and Spetzler13 observed thatif a
frameless stereotactic unit were not available, a stan-dard
frame-based stereotactic instrument could be used to
place a catheter in the lesion to assure correct localization.We
believe that our computer-assisted stereotactic volu-metric
approach not only can accurately localize theselesions but offers
the additional advantage of facilitatingcomplete removal of
radiographically defined tumor vol-umes by delineating the margin
between tumor tissue andthe surrounding parenchyma.1,49
References
1. Abernathey CD, Davis DH, Kelly PJ: Treatment of colloid
cystsof the third ventricle by stereotaxic microsurgical laser
crani-otomy. J Neurosurg 70:525529, 1989
2. Drake CG: Bleeding aneurysms of the basilar artery.
Directsurgical management in four cases. J Neurosurg
18:230238,1961
3. Fried I: Anatomic temporal lobe resections for temporal
lobeepilepsy. Neurosurg Clin North Am 4:233242, 1993
4. Kelly PJ: Tumor Stereotaxis. Philadelphia: WB
Saunders,1991
5. Kelly PJ, Daumas-Duport C, Scheithauer BW, et al:
Ste-reotactic histologic correlations of computed tomography-
andmagnetic resonance imaging-defined abnormalities in patientswith
glial neoplasms. Mayo Clin Proc 62:450459, 1987
6. Kelly PJ, Kall BA, Goerss S, et al: Computer-assisted
stereo-taxic laser resection of intra-axial brain neoplasms. J
Neu-rosurg 64:427439, 1986
7. Kelly PJ, Kall BA, Goerss SJ: Results of computed
tomogra-phy-based computer-assisted stereotactic resection of
metasta-tic intracranial tumors. Neurosurgery 22:717, 1988
H. L. Weiner and P. J. Kelly
276 J. Neurosurg. / Volume 85 / August, 1996
-
7/31/2019 1996 a Novel Computer-Assisted Volumetric Stereotactic
Approach for Resecting Tumors of the Posterior Parahippo
6/6
8. Kelly PJ, Sharbrough FW, Kall BA, et al: Magnetic
resonanceimaging-based computer-assisted stereotactic resection of
thehippocampus and amygdala in patients with temporal lobeepilepsy.
Mayo Clin Proc 62:103108, 1987
9. Morita A, Kelly PJ: Resection of intraventricular tumors via
acomputer-assisted volumetric stereotactic approach.Neurosur-gery
32:920927, 1993
10. Niemeyer P: The transventricular amygdala-hippocampectomyin
temporal lobe epilepsy, in Baldwin M, Bailey P (eds): Tem-poral
Lobe Epilepsy. Springfield, Ill: Charles C Thomas,1958, pp
461482
11. Olivier A: Commentary: cortical resection, in Engel J Jr
(ed):Surgical Treatment of the Epilepsies. New York: RavenPress,
1987, pp 405416
12. Shimizu H, Suzuki I, Ishijima B: Zygomatic approach for
re-section of mesial temporal epileptic focus. Neurosurgery
25:798801, 1989
13. Smith KA, Spetzler RF: Supratentorialinfraoccipital
approachfor posteromedial temporal lobe lesions. J Neurosurg
82:940944, 1995
14. Spencer DD, Spencer SS, Mattson RH, et al: Access to the
pos-terior medial temporal lobe structures in the surgical
treatmentof temporal lobe epilepsy. Neurosurgery 15:667671,
1984
15. Talairach J, Bancaud J, Szikla G, et al: Approche nouvelle
dela neurochirurgie de lpilepsie: mthodologie strotaxique
etrsultats thrapeutiques. Neurochirurgie 20 (Suppl):1240,1974
16. Wieser HG, Yasargil MG: Selective amygdalohippocampecto-my
as a surgical treatment of mediobasal limbic epilepsy. SurgNeurol
17:445457, 1982
17. Yasargil MG, Wieser HG, Valavanis A, et al: Surgery
andresults of selective amygdala-hippocampectomy in one hun-dred
patients with nonlesional limbic epilepsy.Neurosurg ClinNorth Am
4:243261, 1993
Manuscript received October 4, 1995.Accepted in final form March
27, 1996.
Address reprint requests to: Patrick J. Kelly, M.D.,
Departmentof Neurosurgery, New York University Medical Center, 550
FirstAvenue, New York, New York 10016.
J. Neurosurg. / Volume 85 / August, 1996
Lateral occipitosubtemporal stereotactic approach
277