Embed Size (px)
Citation preview
1660CRP-BASED CLASSIFICATION OF LOCALIZED RENAL CELLCARCINOMA PATIENTS INTO LOW, INTERMEDIATE, AND HIGHRISK OF MORTALITY
Timothy Johnson, Wayne Harris, Ammara Abbasi, Andrew Michigan,Ken Ogan, John Pattaras, Omer Kucuk, Peter Nieh, Fray Marshall,Viraj Master*, Atlanta, GA
INTRODUCTION AND OBJECTIVES: Approximately 30% ofpatients undergoing nephrectomy for localized Renal Cell Carcinoma(RCC) develop postoperative metastases. Preoperative C-reactive pro-tein (CRP) is a robust predictor of outcomes. However, CRP cut-offs forLow, Intermediate, and High Risk groups have not been rationallyderived.
METHODS: 173 patients who underwent radical nephrectomyfor localized RCC had CRP measured preoperatively. Receiver Oper-ating Characteristics (ROC) curves were constructed to assess thepotential of preoperative CRP to predict overall survival. ROC curveswere used to determine the Area Under the Curve (AUC) and relativesensitivity and specificity of cut-offs. Based on these cut-offs, patientswere categorized into Low, Intermediate, and High Risk groups. Ka-plan-Meier survival curves were constructed to assess the impact ofdifferent cut-offs on overall survival.
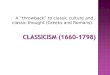
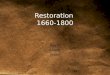
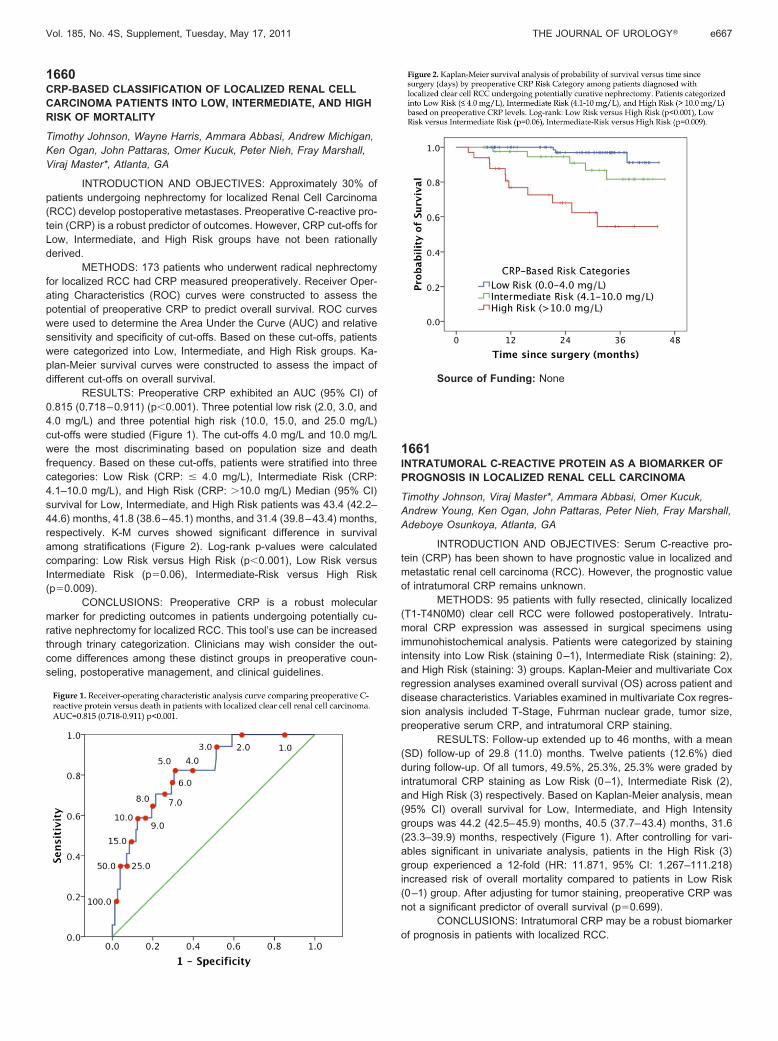
RESULTS: Preoperative CRP exhibited an AUC (95% CI) of0.815 (0.718–0.911) (p�0.001). Three potential low risk (2.0, 3.0, and4.0 mg/L) and three potential high risk (10.0, 15.0, and 25.0 mg/L)cut-offs were studied (Figure 1). The cut-offs 4.0 mg/L and 10.0 mg/Lwere the most discriminating based on population size and deathfrequency. Based on these cut-offs, patients were stratified into threecategories: Low Risk (CRP: � 4.0 mg/L), Intermediate Risk (CRP:4.1–10.0 mg/L), and High Risk (CRP: �10.0 mg/L) Median (95% CI)survival for Low, Intermediate, and High Risk patients was 43.4 (42.2–44.6) months, 41.8 (38.6–45.1) months, and 31.4 (39.8–43.4) months,respectively. K-M curves showed significant difference in survivalamong stratifications (Figure 2). Log-rank p-values were calculatedcomparing: Low Risk versus High Risk (p�0.001), Low Risk versusIntermediate Risk (p�0.06), Intermediate-Risk versus High Risk(p�0.009).
CONCLUSIONS: Preoperative CRP is a robust molecularmarker for predicting outcomes in patients undergoing potentially cu-rative nephrectomy for localized RCC. This tool’s use can be increasedthrough trinary categorization. Clinicians may wish consider the out-come differences among these distinct groups in preoperative coun-seling, postoperative management, and clinical guidelines.
Source of Funding: None
1661INTRATUMORAL C-REACTIVE PROTEIN AS A BIOMARKER OFPROGNOSIS IN LOCALIZED RENAL CELL CARCINOMA
Timothy Johnson, Viraj Master*, Ammara Abbasi, Omer Kucuk,Andrew Young, Ken Ogan, John Pattaras, Peter Nieh, Fray Marshall,Adeboye Osunkoya, Atlanta, GA
INTRODUCTION AND OBJECTIVES: Serum C-reactive pro-tein (CRP) has been shown to have prognostic value in localized andmetastatic renal cell carcinoma (RCC). However, the prognostic valueof intratumoral CRP remains unknown.
METHODS: 95 patients with fully resected, clinically localized(T1-T4N0M0) clear cell RCC were followed postoperatively. Intratu-moral CRP expression was assessed in surgical specimens usingimmunohistochemical analysis. Patients were categorized by stainingintensity into Low Risk (staining 0–1), Intermediate Risk (staining: 2),and High Risk (staining: 3) groups. Kaplan-Meier and multivariate Coxregression analyses examined overall survival (OS) across patient anddisease characteristics. Variables examined in multivariate Cox regres-sion analysis included T-Stage, Fuhrman nuclear grade, tumor size,preoperative serum CRP, and intratumoral CRP staining.
RESULTS: Follow-up extended up to 46 months, with a mean(SD) follow-up of 29.8 (11.0) months. Twelve patients (12.6%) diedduring follow-up. Of all tumors, 49.5%, 25.3%, 25.3% were graded byintratumoral CRP staining as Low Risk (0–1), Intermediate Risk (2),and High Risk (3) respectively. Based on Kaplan-Meier analysis, mean(95% CI) overall survival for Low, Intermediate, and High Intensitygroups was 44.2 (42.5–45.9) months, 40.5 (37.7–43.4) months, 31.6(23.3–39.9) months, respectively (Figure 1). After controlling for vari-ables significant in univariate analysis, patients in the High Risk (3)group experienced a 12-fold (HR: 11.871, 95% CI: 1.267–111.218)increased risk of overall mortality compared to patients in Low Risk(0–1) group. After adjusting for tumor staining, preoperative CRP wasnot a significant predictor of overall survival (p�0.699).
CONCLUSIONS: Intratumoral CRP may be a robust biomarkerof prognosis in patients with localized RCC.
Vol. 185, No. 4S, Supplement, Tuesday, May 17, 2011 THE JOURNAL OF UROLOGY� e667