Embed Size (px)
Citation preview

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-91
Pharmacokinetics: A RefresherCurtis L. Smith, Pharm.D., BCPS
Ferris State UniversityLansing, Michigan

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-92
Learning Objectives:
1. Identify and provide examples using basic phar-macokinetic concepts commonly used in clinical practice, including elimination rate constant, vol-ume of distribution, clearance, and bioavailability.
2. Describe specificpharmacokineticcharacteristicsof commonly used therapeutic agents, including aminoglycosides, vancomycin, phenytoin, and di-goxin, as well as pharmacokinetic alterations in patients with renal and hepatic disease.
3. Define important issues as they pertain to drugconcentration sampling and interpretation.
Self-Assessment Questions:Answers and explanations to these questions may be found at the end of this chapter.
1. J.H., a 65-year-old woman (65 kg), was recently ini-tiated on tobramycin and piperacillin/tazobactam for treatment of hospital-acquired pneumonia. After the first dose of tobramycin 120mg (infused fromnoonto1:00pm), serum tobramycin concentrations aredrawn.Theyare4.4mg/Lat3:00pmand1.2mg/Lat7:00pm.Whichoneofthefollowingisthebest assessment regarding calculating tobramycin pharmacokinetic parameters in this patient?A. Therearesufficientdatatodetermine
the half-life (t1/2) but not the volume of distribution (Vd).
B. Therearesufficientdatatodetermineboththe t1/2 and Vd.
C. Thereareinsufficientdatatodetermineeitherthe t1/2 or the Vd.
D. TherearesufficientdatatodeterminetheVd but not the t1/2.
2. P.L.isa60-year-oldwoman(60kg)recentlyiniti-atedongentamicinandclindamycin.Afterthefirstgentamicindoseof110mg(infusedfrom6:00pmto6:30pm),serumgentamicinconcentrationsaredrawn.Theyare3.6mg/Lat7:30pmand0.9mg/Lat11:30pm.Whichoneofthefollowingisthebestassessment of this patient’s gentamicin pharmaco-kinetic parameters?A. The t1/2 is about 2 hours.B. The t1/2 is about 3 hours.
C. The maximum concentration (Cmax) is about 3.8 mg/L.
D. The Vd is about 11.6 L.
3. R.O. is a 74-year-old woman initiated on gentami-cin 100mg intravenously every 24hours for py-elonephritis. On admission, her serum creatinine (SCr) is 1.8 mg/dL. She also has congestive heart failure and isfluidoverloadedbecauseofherdi-minished renal function and nonadherence to her angiotensin-converting enzyme inhibitor and di-uretic. A few days into her hospitalization, her SCr is down to 1.1 mg/dL, and she is reinitiated on furo-semideandenalapril.Whichoneofthefollowingmost likely happened to the gentamicin t1/2 in R.O. during her hospitalization?A. Her clearance increased, which increased her
Vd and decreased her t1/2.B. Her clearance increased, which increased her
elimination rate constant and decreased her t1/2.C. Her Vd decreased, which increased her
clearance and decreased her t1/2.D. Her Vd decreased, which increased her
elimination rate constant and increased her t1/2.
4. A patient receives vancomycin 1000mg intrave-nously every 24 hours and has a trough concentra-tion,drawn30minutesbeforethenextdose,of6mg/L.Whichoneofthefollowingregimensisbestfor this patient if the goal trough concentration is 10–15mg/L?A. Maintainthedoseat1000mgintravenously
every 24 hours.B. Lowerthedoseto500mg,butkeepthe
interval at every 24 hours.C. Keepthedoseat1000mg,butshortenthe
interval to every 12 hours.D. Lowerthedoseto500mg,andshortenthe
interval to every 12 hours.
5. A 40-year-old, 60-kg woman who smokes pre-sents to the emergency department at 2:00 pmwith an acute exacerbation of asthma. She takes theophyllinesustainedrelease300mg2times/day,withthelastdosetakenat9:00thatmorning.Hertheophylline concentration soon after presenting to theemergencydepartment is7.0mg/L.She isstabilized and is to be sent home on theophylline

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-93
sustainedrelease.Whichoneofthefollowingop-tions is the best regimen for this patient?A. Theophyllinesustainedrelease300mgby
mouth every 12 hours.B. Theophyllinesustainedrelease600mgby
mouth every 12 hours.C. Theophyllinesustainedrelease400mgby
mouth every 8 hours.D. Theophyllinesustainedrelease600mgby
mouth every 8 hours.
6. L.R.isa49-year-oldpatientwithdiabetesmellitusand renal failure. He was recently in a car accident and sustained head trauma. He currently receives phenytoin100mg intravenously3 times/day,andhis most recent concentration was 5.6 mcg/mL. You are asked to suggest a new dose to achieve a concentration within the therapeutic range. Labora-tory results include sodium 145 mEq/L, potassium 3.9mEq/L,chloride101mEq/L,carbondioxide26mEq/L,bloodureanitrogen(BUN)95mg/dL,SCr5.4mg/dL,glucose230mg/dL,andalbumin(Alb)2.8g/dL.Whichoneofthefollowingchoicesisthebest recommendation?A. Increasethedoseto200mgintravenously3
times/day.B. Increasethedoseto200mgintravenously2
times/day.C. Decreasethedoseto100mgintravenously2
times/day.D. Keep the dose the same.
7. YouareaskedhowtheTDx(fluorescencepolariza-tion immunoassay) and EMIT (enzyme multiplied immunoassay technique) assays compare with eachother.Whichoneofthefollowingstatementsis most accurate?A. Although both are immunoassays, one labels
antibody, whereas the other labels antigen.B. Although both are immunoassays, one uses
antibody as a marker, whereas the other uses a radioisotope.
C. Although both are immunoassays, one uses an enzyme label, whereas the other uses a fluorescentlabel.
D. They are both names for the same assay technique.
8. An elderly patient is seen in the morning medicine clinic for a routine follow-up. Medication history includes digoxin 0.25 mg/day by mouth, furose-mide40mg/daybymouth,andpotassiumchloride10mEq/daybymouth.Alldoseswerelasttakenat8:00amtodayathome.Thepatienthasvaguecom-plaints of stomach upset, which began 2 days ago, but is otherwise in no apparent distress. A serum digoxinconcentrationdrawntodayat10:00amis2.5mcg/L.Whichoneofthefollowingstatementsbest describes what should be done next?A. Admit the patient for administration of
digoxin Fab.B. Tell the patient to skip tomorrow’s dose of
digoxinandbegin0.125mg/daybymouth.C. Administer a dose of activated charcoal.D. Do nothing today about the digoxin.
9. Aresearchgroupisanalyzingtherelationshipbe-tween various independent patient demographics (e.g., age, height, weight, Alb, creatinine clearance [CrCl]) and phenytoin pharmacokinetics. Whichone of the following is the best statistical test to use in assessing the relationship?A. One-way analysis of variance.B. Analysis of covariance.C. Multiple logistic regression.D. Spearman rank correlation.
10. N.T.isa24-year-oldwomanreceivingvalproicacidfor tonic-clonic seizures. Her most recent trough valproic acid concentration was 22 mg/L. Her most recent Alb concentration was 4.1 g/dL. Given this serum concentration, which one of the following recommendations is best regarding her dose?A. Continue with the current dose; the
concentration is close enough to the therapeutic range.
B. Assess adherence and increase her dose; the concentration is below the therapeutic range.
C. Decrease her dose; the concentration is slightly above the therapeutic range.
D. Assess adherence and then check a free valproic acid concentration and adjust accordingly.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-94
Patient Cases1. H.R. is receiving vancomycin for a methicillin-resistant Staphylococcus aureus bacteremia. H.R. has chronic
renal failure. A 1-g intravenous dose of vancomycin is given at noon on March 21. A concentration drawn at 2:00pmonMarch21is23.8mcg/mL.Aconcentrationdrawnat2:00pmonMarch24is12.1mcg/mL.Ifyouweretogiveadoseat4:00pmonMarch24andyourgoaltroughconcentrationwas10–15mg/L,whichoneof the following represents the best time to give the next dose?A. 1 day after the dose on the 24th.B. 3 days from the dose on the 24th.C. 6 days from the dose on the 24th.D. Thereisinsufficientinformationtocalculatewhentore-dose.
2. Aftertheadministrationof100mgofadrugintravenouslyand200mgofthesamedrugbymouth,theareasunderthecurvesare50and25mg/L/hour.Whichoneofthefollowingbestdescribesthebioavailabilityofthis drug?A. 25%.B. 37.5%.C. 50%.D. 100%.
3. L.B. is receiving tobramycin for a resistant Pseudomonas aeruginosa pneumonia. L.B. has chronic renal failure.Aloadingdoseof160mgisgivenatnoonover1hour.Aconcentrationisdrawnat6:00pm,whichis6.5mg/L,andagainat6:00amthenextday,whichis5.4mg/L.WhenL.B.’sconcentrationis1mg/L,whichoneofthefollowingwillbethebestdosetoachieveapeakof9mg/L?A. 140mg.B. 160mg.C. 180mg.D. 200mg.
I. BASIC PhArmACOkInetIC reLAtIOnShIPS Table11hasdefinitionsofterms.
A. Absorption F = doseiv * AUCev
doseev * AUCiv
B. DistributionRapid intravenous (or oral) bolus: Vd =
F * doseCp0
Continuous intravenous infusion at steady state: Vd = R0
k * Css
Continuous intravenous infusion before steady state: Vd = R0
C * k(1−e−kti) and C =
R0
Vd * k(1−e−kti)
Multiple intravenous bolus at steady state: Vd = dose
Css max *(1–e–kτ)

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-95
Multiple intermittent intravenous infusion at steady state: Vd = R0
k * 1−e–kt'
Cmax −(Cmin * e–kt')
Css max = R0 * (1 - ekt’)
Vd * k * (1 - ekτ) Css min = Css max * e−k(τ-t’)
C. Clearance
Clearance = doseAUC k =
C1Vd
k = (1nC1 − lnC2)
(t2−t1) t
1/2 =
0.693k
Continuous intravenous infusion at steady state: clearance = R0
Css
Continuous intravenous infusion before steady state: clearance = R0
C *(1−e−kti)
Multiple intravenous (or oral) bolus at steady state: clearance = F * dose / τ
Css–avg
τ=
(1nCmax − lnCmin)k
C1 = C0 * e−kt
II. ABSOrPtIOn
A. First-Pass Effect1. Blood that perfuses virtually all the gastrointestinal tissues passes through the liver by means of the
hepatic portal vein.a. Fifty percent of the rectal blood supply bypasses the liver (middle and inferior hemorrhoidal veins).b. Drugs absorbed in the buccal cavity bypass the liver.
2. Drugsaffectedmostbythefirst-passeffectarethosewithahighhepaticextractionratio.3. Example
AmitriptylineDesipramineDiltiazemDoxepinImipramineIsosorbide dinitrate
LabetalolLidocaineMetoprololMorphineNicardipineNifedipine
NitroglycerinPentazocinePropoxyphenePropranololVerapamil

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-96
B. Enterohepatic Recirculation1. Drugsareexcretedthroughthebileintotheduodenum,metabolizedbythenormalflorainthe
gastrointestinal tract, and reabsorbed into the portal circulation.2. Occurs with drugs that have 1) biliary (hepatic) elimination and 2) good oral absorption3. Drug is concentrated in the gallbladder and expelled on sight, smell, or ingestion of food.
table 1. Examples of Compounds Excreted in Bile and Subject to Enterohepatic Cycling
Compound entity in BileChloramphenicolDigoxinEstrogensImipramineIndomethacinNafcillinRifampinSulindacTestosteroneTiagabineValproic acidVitamin A
Glucuronide conjugateParentParentParent and desmethyl metaboliteParent and glucuronideParentParentGlucuronides of parent and metabolitesConjugatesGlucuronide conjugateGlucuronide conjugatesConjugates
Patient Case4. WhichoneofthefollowingstatementsbestdescribesP-glycoprotein?
A. It is a plasma protein that binds basic drugs.B. It transfers drugs through the gastrointestinal mucosa, increasing absorption.C. ItdiminishestheeffectofcytochromeP450(CYP)3A4inthegastrointestinalmucosa.D. Itisaneffluxpumpthatdecreasesgastrointestinalmucosalabsorption.
C. P-glycoprotein1. P-glycoproteinisaneffluxpump(locatedintheesophagus,stomach,andsmallandlargeintestines)
that pumps drugs back into the gastrointestinal lumen; it is a more important factor in drug absorption drug interactions than intestinal CYP3A4.
2. Both CYP3A4 and P-glycoprotein are located in small intestinal enterocytes and work together to decrease the absorption of xenobiotics.
3. Most CYP3A4 substrates are also P-glycoprotein substrates.4. Many CYP3A4 inhibitors/inducers also inhibit/induce P-glycoprotein, leading to increases or decreases
in bioavailability.5. Examples of P-glycoprotein absorption drug interactions include verapamil or amiodarone or
dronedaroneanddigoxinordabigatran;rifampinorSt.John’swortandhumanimmunodeficiencyvirus protease inhibitors or dabigatran.
Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-97
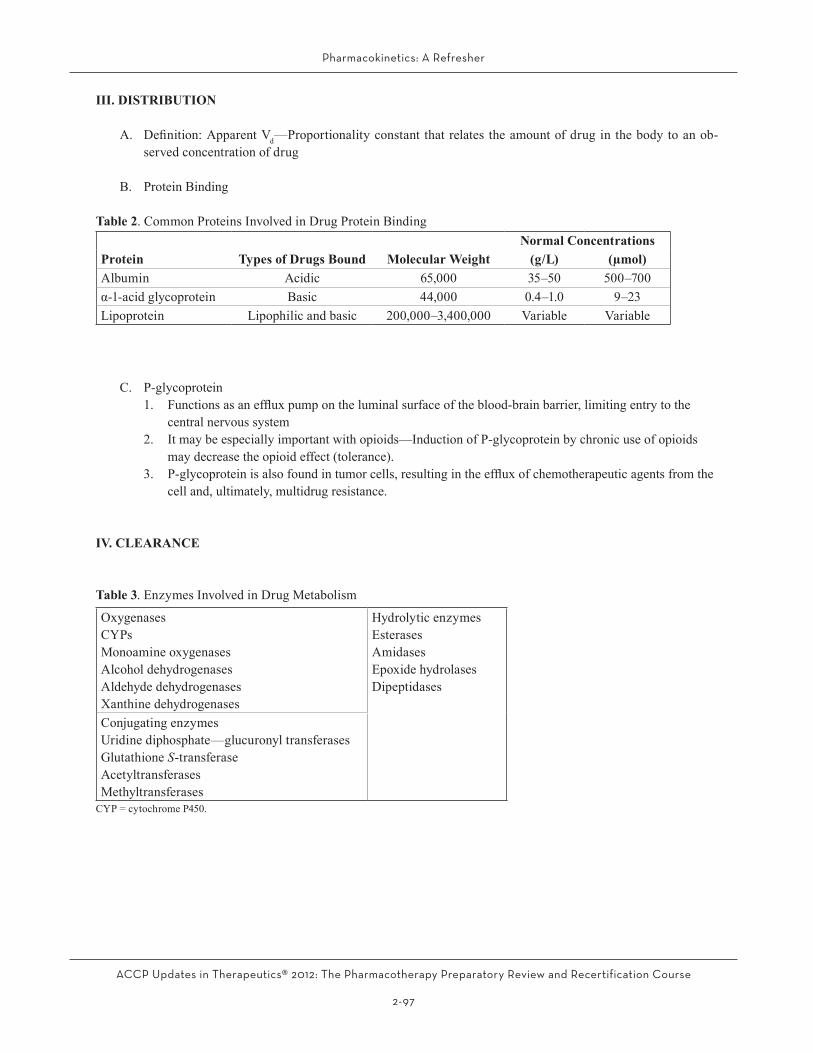
III. DIStrIButIOn
A. Definition:ApparentVd—Proportionality constant that relates the amount of drug in the body to an ob-served concentration of drug
B. Protein Binding
table 2. Common Proteins Involved in Drug Protein Bindingnormal Concentrations
Protein types of Drugs Bound molecular Weight (g/L) (µmol)Albumin Acidic 65,000 35–50 500–700α-1-acidglycoprotein Basic 44,000 0.4–1.0 9–23Lipoprotein Lipophilic and basic 200,000–3,400,000 Variable Variable
C. P-glycoprotein1. Functionsasaneffluxpumpontheluminalsurfaceoftheblood-brainbarrier,limitingentrytothe
central nervous system2. It may be especially important with opioids—Induction of P-glycoprotein by chronic use of opioids
may decrease the opioid effect (tolerance).3. P-glycoproteinisalsofoundintumorcells,resultingintheeffluxofchemotherapeuticagentsfromthe
cell and, ultimately, multidrug resistance.
IV. CLeArAnCe
table 3. Enzymes Involved in Drug Metabolism
OxygenasesCYPsMonoamine oxygenasesAlcohol dehydrogenasesAldehyde dehydrogenasesXanthine dehydrogenases
Hydrolytic enzymesEsterasesAmidasesEpoxide hydrolasesDipeptidases
Conjugating enzymesUridine diphosphate—glucuronyl transferasesGlutathione S-transferaseAcetyltransferasesMethyltransferasesCYP=cytochromeP450.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-98
table 4. Drug Transport Proteins
transport Protein Superfamily
transport Protein (Gene [Protein])
Location and Function Drugs Affected by transport Protein
SLC SLC01A2 [OATP-A] Hepatocyte: Bile acid uptake DigoxinLevofloxacinMethotrexateStatins
SLCO1B1 [OATP1B1] Hepatocyte: Hepatic uptake of drugs PravastatinRifampinValsartan
SLCO1B3 [OATP1B3] Hepatocyte: Hepatic uptake of drugs DigoxinFexofenadineRifampinStatins
SLC22A1, SLC22A2, SLC22A6, SLC22A8 [OAT and OCT]
Hepatocyte: Hepatic uptake of drugsa
Renal tubule (interstitial side): Secretion of drugsb
Salicylatea
Methotrexatea
Zidovudinea
Tetracyclinea
Organic anions and cationsb
SLCO2B1 [OATP2B1] Hepatocyte: Hepatic uptake of drugs FexofenadineGlyburideStatins
SLC15A1, SLC15A2 [PEPT1, PEPT2]
Renal tubuleIntestinal enterocytes
CephalexinCaptoprilEnalaprilValacyclovir
SLC47A1, SLC47A2 [MATE1, MATE2-K]
Renal tubule Metformin
ABC ABCB11 [BSEP] Hepatocyte: Bile acid excretion into bile PravastatinABCC2, 3, 4, and 5 [MRP2, 3, 4, and 5]
Hepatocyte: Excreting water-soluble drugs and metabolites into blooda
Renal tubule (luminal side): Secretion of drugs
Glucuronide, sulfate, and glutathione metabolitesa
Methotrexatea
Pravastatina
Rifampina
ABCB1 [MDR1] (P-glycoprotein)
Hepatocyte: See text in handoutRenal tubule (luminal side): See text in handout
See text
ABCB4 [MDR3] Hepatocyte DigoxinPaclitaxelVinblastine
ABCG2 [BCRP] Hepatocyte: Biliary excretion DaunorubicinDoxorubicinImatinibMethotrexateMitoxantroneStatins

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-99
Patient Case5. A renal transplant patient receiving cyclosporine receives a diagnosis of community-acquired pneumonia.
The patient is admitted to the hospital and initiated on ceftriaxone and a macrolide. A physician asks you to chooseamacrolidethatwillnotinteractwiththepatient’scyclosporine.Whichoneofthefollowingmacro-lides is the best choice to meet the physician’s criteria?A. Erythromycin.B. Clarithromycin.C. Azithromycin.D. All macrolides inhibit CYP3A4.
A. CytochromeP450
1. Introductiona. A group of heme-containing enzymes responsible for phase 1 metabolic reactionsb. Characteristicabsorbanceoflightat450nm(thus,CYP)c. Primarily located in the membranes of the smooth endoplasmic reticulum in 1) liver, 2) small
intestine, and 3) brain, lung, and kidneyd. Encoded by a supergene family and subfamily; separate genes code for different isoenzymese. DrugswillgenerallyhaveahighaffinityforoneparticularCYP,butmostdrugsalsohave
secondary pathways.
GENE for mammalian cytochrome
family(>40%identicalinaminoacidsequence)
subfamily(>70%identicalinaminoacidsequence)
specificenzyme
CYP 3 A 4
Figure 1. Nomenclature

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-100
2. Distribution of CYP isoenzymes in human liver
1A213%
2E17%
2A64%2D62%
2C18%
Other26%
3A430%
1A211%
2E14%
2B63%2A63%
2D619%
2C916%
2C198%
3A436%
Content role in CYP-mediated Drug elimination
Figure 2. Distribution of CYP isoenzymes in human liver
3. Distribution of CYP isoenzymes in human gastrointestinal tract
Other CYPs30%
CYP3A470%
Figure 3. Distribution of CYP isoenzymes in human gastrointestinal tract
4. Characteristics of CYP metabolisma. Inhibition is substrate-independent.b. Some substrates are metabolized by more than one CYP (e.g., TCAs [tricyclic antidepressants],
SSRIs [selective serotonin reuptake inhibitors]).c. Enantiomers may be metabolized by a different CYP (e.g., warfarin).d. Differencesininhibitionmayexistwithinthesameclassofagents(e.g.,fluoroquinolones,azole
antifungals, macrolides, calcium channel blockers, H2 blockers).e. Substrates can also be inhibitors (e.g., erythromycin, verapamil, diltiazem).f. Most inducers and some inhibitors can affect more than one isozyme (e.g., cimetidine, ritonavir,
fluoxetine,erythromycin).g. Inhibitorsmayaffectdifferentisozymesatdifferentdoses(e.g.,fluconazoleinhibitsCYP2C9at
dosesof100mg/dayorgreater,andinhibitsCYP3A4atdosesof400mg/dayorgreater).

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-101
B. P-glycoprotein1. P-glycoproteinisaneffluxpumpthatpumpsdrugsintothebile;theclinicaleffectofP-glycoprotein
drug interactions in the bile is unknown.2. P-glycoprotein pumps drugs from renal tubules into the urine; it also potentially limits the degree of
reabsorption.3. Examples of drug interactions: Quinidine/digoxin, cyclosporine/digoxin, and propafenone/digoxin
C. Pharmacogenetics/Polymorphic Drug Metabolism1. Population in general is divided into poor, extensive, and ultrarapid metabolizers; therefore,
metabolism is considered polymorphic.2. Definitionofpolymorphism:Coexistenceofmorethanonegeneticvariant(alleles),whicharestable
components in the population (more than 1% of population)3. Clear antimode results
Metabolic ratio of unchanged drug to metabolite → (increasing metabolic capacity)
No.
of P
atie
nts antimode
EM URMPM
Figure 4. Distribution of Patients in a Drug that Follows Polymorphic Metabolism
EM = extensive metabolizer; PM = poor metabolizer; URM = ultrarapid extensive metabolizer.
4. Phenotype: Expression of the trait; interaction of gene with environmenta. Manifestation of the trait clinicallyb. Not necessarily constant
5. Genotype: Genetic makeup

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-102
table 5. Metabolic Pathways Demonstrating Polymorphism
Pathway Substrate enzyme Drug examplesOxidation Debrisoquine,
dextromethorphanCYP2D6 Tertiary amines
FluoxetineFlecainidePropafenoneMetoprololPropranololTimololCodeineTamoxifen
Oxidation Warfarin CYP2C9 AmitriptylinePhenytoinWarfarin
Oxidation Mephenytoin CYP2C19 ClopidogrelTertiary amines (diazepam)PhenytoinOmeprazole
Acetylation Isoniazid, caffeine N-acetyltransferase ClonazepamDapsoneHydralazineInamrinoneProcainamideSulfonamides
CYP=cytochromeP450.
V. nOnLIneAr PhArmACOkInetICS
Patient Case6. C.M. is a 55-year-old man who is initiated on phenytoin after a craniotomy. His current steady-state phenytoin
concentrationis6mg/Latadoseof200mg/daybymouth.Ifhisaffinityconstant(Km) is calculated to be 5 mg/L,whichoneofthefollowingismostlikelytooccurifthedoseisdoubled(to400mg/daybymouth)?A. His concentration will double because phenytoin clearance is linear above the Km.B. His concentration will more than double because phenytoin clearance is nonlinear above the Km.C. His concentration will stay the same because phenytoin is an autoinducer, and clearance increases with time.D. Hisconcentrationwillincreasebyonly50%becausephenytoinabsorptiondecreasessignificantly
withdosesgreaterthan300mg.
A. Michaelis-Menten Pharmacokinetics
velocity = Vmax * S
Km + S
Vmax = capacity constant (amount/time)Km=affinityconstant(amount/volume)S = substrate concentration (amount/volume)

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-103
B. Nonlinear Elimination1. Saturation or partial saturation of the elimination pathway
rate of elimination (dose) = Vmax * C
Km + C
Vmax = maximum rate of elimination (amount/time)Km = concentration where elimination is ½ Vmax(affinityconstant)C = drug concentration
2. Note: Nonlinearity occurs when concentration is at or above Km.
Example: Phenytoina. Vmax normal = 7 mg/kg/dayb. Km normal = 5.6 mg/Lc. 50%variabilitybetweenindividuals
VI. nOn-COmPArtmentAL PhArmACOkInetICS
A. WhyNon-compartmentalPharmacokinetics?1. Identificationofthe“correct”modelisoftenimpossible.2. A compartmental view of the body is unrealistic.3. Linear regression is unnecessary—it is easier to automate analysis.4. Requires fewer and less stringent assumptions5. More general methods and equations6. There is no need to match all data sets to the same compartmental model.
B. Definitions1. Zero moment—concentration versus time curve
•Areaunderthecurve(AUC)
AUC = ∑ (Cn+1 + Cn)
2 * (tn+1−tn) ... + Clast
k2. First moment—concentration * time versus time curve
•Areaunderthefirstmomentcurve(AUMC)
AUMC = ∑ * (Cn+1 * tn+1 + Cn * tn)
2 * (tn+1−tn) +
Clast * tlast
k + Clast
k2
3. Mean residence time (MRT)
MRT = AUMCAUC
4. Mean absorption time (MAT)
MAT = MRTev−MRTiv

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-104
C. Pharmacokinetic Parameter Estimation1. Clearance
clearance = doseAUC
2. Volume of distribution at steady state
Vss = dose * AUMC
AUC2
3. Elimination rate constant
k = 1
MRT
4. Absorption rate constant
ka = 1
MAT
5. Bioavailability
F = Div * AUCev
Dev * AUCiv
VII. DAtA COLLeCtIOn AnD AnALYSIS
Patient Case7. R.K. is a 54-year-old woman with a history of diabetes mellitus and end-stage renal disease. She is receiving
gentamicin for Pseudomonas aeruginosa pneumonia. A gentamicin concentration is ordered after dialysis. Whichoneofthefollowingisthebestapproachtoobtainingthissample?A. Obtain the concentration immediately after hemodialysis.B. Waitafewhourstoobtaintheconcentrationbecauseitwilldecreasesignificantlywithinthefirstfew
hours after hemodialysis.C. Waitafewhourstoobtaintheconcentrationbecauseitwillincreasesignificantlywithinthefirstfew
hours after hemodialysis.D. Waituntilthenextdaysothatalltheeffectsofhemodialysishaveabated.
A. Timing of Collection1. Ensure completion of absorption and distribution phases (especially digoxin and vancomycin, etc.).2. Ensure completion of redistribution postdialysis (especially aminoglycosides).
B. Specimen Requirements1. Wholeblood:Useanticoagulatedtube.Examples:Cyclosporine,amiodarone2. Plasma: Use anticoagulated tube and centrifuge; clotting proteins and some blood cells are maintained.3. Serum: Use red top tube, allow to clot, and centrifuge. Examples: Most analyzed drugs including
aminoglycosides, vancomycin, phenytoin, and digoxin

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-105
Patient Case8. Adrugassayistoutedashavinghighspecificitybutlowsensitivity.Whichoneofthefollowingstatements
best describes what this means?A. The assay will not be able to distinguish the drug from like products, but it will be able to detect
extremely low concentrations.B. The assay will not be able to distinguish the drug from like products, and it will not be able to detect
extremely low concentrations.C. The assay will be able to distinguish the drug from like products and will be able to detect extremely
low concentrations.D. The assay will be able to distinguish the drug from like products but will not be able to detect
extremely low concentrations.
C. Assay Terminology1. Precision (reproducibility): Closeness of agreement among the results of repeated analyses performed
on the same samplea. Standard deviation (SD): Average difference of the individual values from the meanb. Coefficientofvariation(CV):SDasapercentageofthemean(relativeratherthanabsolute
variation)
CV = SDMean
2. Accuracy:Closenesswithwhichameasurementreflectsthetruevalueofanobject •Correlationcoefficient—Strengthoftherelationshipbetweentwovariables3. Predictive performance (accuracy)
Precision: a.k.a. root mean squared error (RMSE)
NMSE = 1
N Σ pei
2 RMSE = √mse i=1
Bias: a.k.a. mean prediction error (ME)
NME = 1
N Σ pei
i=1
•Predictionerror(pe)isthepredictionminusthetruevalue.
4. Sensitivity: Ability of an assay to quantitate low drug concentrations accurately; usually the lowest concentration an assay can differentiate from zero
5. Specificity(cross-reactivity):Abilityofanassaytodifferentiatethedruginquestionfromlikesubstances
Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-106
D. Assay Methodology1. Immunoassays
a. Radioimmunoassayi. Advantages: Extremely sensitive (picogram range)ii. Disadvantages: Radioimmunoassay kits have limited shelf life because of the short t1/2 of
labels, nuclear waste, and cross-reactivity.•Clinicaluseforassayingdigoxinandcyclosporine
b. Enzyme immunoassay; ex. EMIT (enzyme multiplied immunoassay technique)c. Fluorescenceimmunoassay:TDx(Abbott)(fluorescencepolarizationimmunoassay):Most
common therapeutic drug monitoring assayi. Advantages: Simple, automated, highly sensitive, and stable reagentsii. Disadvantages:Backgroundinterferenceattributabletoendogenousserumfluorescence
2. High-pressure liquid chromatography3. Gas chromatography-mass spectrometry and liquid chromatography-mass spectrometry4. Flame photometry5. Bioassay
E. Population Pharmacokinetics in Therapeutic Drug Monitoring1. Population pharmacokinetics useful when:
a. Drug concentrations are obtained during complicated dosing regimens.b. Drug concentrations are obtained before steady state.c. Only a few drug concentrations are feasibly obtained (limited sampling strategy).
2. Bayesian pharmacokineticsa. Priorpopulationinformationiscombinedwithpatient-specificdatatopredictthemostprobable
individual parameters.b. Whenpatient-specificdataarelimited,thereisgreaterinfluencefrompopulationparameters;when
patient-specificdataareextensive,thereislessinfluence.c. Withsmallamountsofindividualdata,Bayesianforecastinggenerallyyieldsmorepreciseresults.
Patient Cases9. K.M.,an80-year-oldwhitewoman(52kg,5′4″),isadmittedtothehospitalforpyelonephritiswithsepsis.
She has a history of myocardial infarction ×2, congestive heart failure, hypertension, osteoporosis, rheu-matoidarthritis,andcerebrovascularaccident.Onadmission,herBUNis11mg/dL,SCris0.92mg/dL,andAlbis2.9g/dL.K.M.isinitiatedonthefollowingdrugs:trimethoprim/sulfamethoxazoleintravenously,240mgoftrimethoprimevery12hours,lisinopril10mg/daybymouth,digoxin0.125mg/daybymouth,fu-rosemide40mg/daybymouth,cimetidine400mgbymouth2times/day,acetaminophen650mgbymouthevery6hours,calciumcarbonate500mgbymouth3times/day,andcarvedilol6.25mgbymouth2times/day.WhichoneofthefollowingisthebestestimateofK.M.’sglomerularfiltrationrate(GFR)?A. 10mL/minute/1.73m2.B. 30mL/minute/1.73m2.C. 60mL/minute/1.73m2.D. 120mL/minute/1.73m2.
10. WhichoneofK.M.’sdrugcombinationsismostlikelytoalterherSCrconcentrations?A. Lisinopril and digoxin.B. Trimethoprim/sulfamethoxazole and cimetidine.C. Furosemide and calcium carbonate.D. Acetaminophen and carvedilol.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-107
VIII. PhArmACOkInetICS In renAL DISeASe
A. Estimation of GFR/CrCl1. Creatinine production and elimination
a. Creatine is produced in the liver.b. Creatinine is the product of creatine metabolism in skeletal muscle.c. Creatinineisfilteredattheglomerulus,whereitundergoeslimitedsecretion.d. Creatinine is useful in approximating GFR because
i. At normal concentrations of creatinine, secretion is low.ii. The creatinine assay picks up a non-creatinine chromogen in the blood but not in the urine.
2. CrCl calculation to estimate GFR
•CrCliscalculatedfroma24-hoururinecollectionandthefollowingequation:
CrCl (mL/minute) = volumeofurine/1440minutes×urinecreatinineconcentration
serum creatinine concentration•NormalCrCl
Healthy young men = 125 mL/minute/1.73m2
Healthy young women = 115 mL/minute/1.73m2
•Afterage30,1%ofGFRislostperyear.
3. Creatinine clearance estimation to estimate GFRa. Factors affecting SCr concentrations:
i. Sexii. Ageiii. Weight/musclemassiv. Renal function. Caveats: Creatinine clearance estimations worsen as renal function worsens
(usually an overestimation).b. Jelliffe
CrCl (mL/minute/1.73m2) = 98−0.8(age−20)
SCr Women:Use90%oftheaboveequation.
•Limitations:Serum creatinine concentration must be stable.Adultsaged20–80yearsControversy:RoundingupSCrinpatientswithlowconcentrations(lessthan0.7–1mg/dL)
c. Cockcroft and Gault
CrCl (mL/minute) = (140−age)*(TBW)
72 * SCr
•Women:Use85%oftheaboveequation.•UseIBWinpatientswithBMIgreaterthan30kg/m2.
Idealbodyweight(IBW)(men)=50kg+2.3kgforeachinchover5feetIBW(women) = 45.5 kg + 2.3 kg for each inch over 5 feet

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-108
•Limitations:Serum creatinine concentration must be stable.Developed for adults onlyNot corrected for creatinine standardization (results in lower estimations)Controversy:RoundingupSCrinpatientswithlowconcentrations(lessthan0.7–1mg/dL)
d. ModificationofDietinRenalDiseasestudyequation
Full equation:
GFR (mL/minute/1.73m2) = 161.5 * (SCr)-0.999 * (age in years)-0.176*1.180 (ifpatientisAfricanAmerican)*0.762(ifpatientisawoman)*(BUN)-0.170 * (Alb)+0.318
Simplifiedfour-variableequation:
GFR (mL/minute/1.73m2) = 175 * (SCr)-1.154 * (age in years)-0.203 * 1.212 (ifpatientisAfricanAmerican)*0.742(ifpatientisawoman)
i. These equations directly estimate GFR (NOT CrCl) and were developed using standardized creatinine concentrations.
ii. These equations are recommended by the American Kidney Foundation and the European Renal Association to estimate renal function.
iii. NotasaccuratewhenGFRisgreaterthan60mL/minute/1.73m2
iv. If used for drug dosing, convert value from milliliter per minute per 1.73m2 to milliliter per minute.
v. IfusedfordrugdosingandsignificantlydifferentfromCockcroftandGault,useclinicaljudgmentandoptimizeriskversusbenefit.
e. Chronic Kidney Disease Epidemiology Collaboration equation (CKD-Epi)i. These equations directly estimate GFR (not CrCl).ii. These equations are more accurate than ModificationofDietinRenalDisease at higher GFRs
(i.e.,greaterthan60mL/minute/1.73m2).
table 6. Chronic Kidney Disease Epidemiology Collaboration equationsrace and Sex Serum Creatinine (mg/dL) equationAfrican AmericanFemale <0.7 GFR=166*(SCr/0.7)-0.329*(0.993)Age
>0.7 GFR=166*(SCr/0.7)-1.209*(0.993)Age
Male <0.9 GFR=163*(SCr/0.9)-0.411*(0.993)Age
>0.9 GFR=163*(SCr/0.9)-1.209*(0.993)Age
WhiteorotherFemale <0.7 GFR=144*(SCr/0.7)-0.329*(0.993)Age
>0.7 GFR=144*(SCr/0.7)-1.209*(0.993)Age
Male <0.9 GFR=141*(SCr/0.9)-0.411*(0.993)Age
>0.9 GFR=141*(SCr/0.9)-1.209*(0.993)Age
GFR=glomerularfiltrationrate;SCr=serumcreatinine.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-109
f. Pediatric formulas. Do not round up low SCr values in pediatric patients.
Schwartz
CrCl (mL/minute) = K * ht (cm)
SCr
table 7. Schwartz Equation Constants
Age kLowbirthweight≤1yearFullterm≤1year1 year to adolescenceMuscular adolescent males
0.330.450.550.7
Note:K=0.413for1yeartoadolescencewhenusingstandardized creatinine concentrations (other K values have not been updated)
Shull
CrCl (mL/minute/1.73m2) = (0.035*age(yrs)+0.236)*100
SCr
•Thisisonlyforthoseaged1–18years.
4. FactorsinfluencingCrClestimatesa. Patient characteristics
i. Age(↓productionofcreatininewithage)ii. Femalesex(↓productionofcreatinine)iii. Race(↑ production of creatinine in African Americans)
b. Disease states/clinical conditionsi. Spinalcordinjuries(↓musclemass;↓creatinine)ii. Amputations(↓musclemass;↓creatinine)iii. Cushingsyndrome(↓musclemass;↓creatinine)iv. Musculardystrophy(↓musclemass;↓creatinine)v. Guillain-Barrésyndrome(↓musclemass;↓creatinine)vi. Rheumatoidarthritis(↓musclemass;↓creatinine)vii. Liverdisease(↓creatine;↓creatinine)viii. Glomerulopathicdisease(greateramountofcreatininesecretioninrelationtofiltration)
c. Dieti. High-meatproteindiets(↑creatinineingestion)ii. Vegetarians(↓creatinineingestion)iii. Protein-calorie malnutrition (↓creatinineingestion)
d. Drugs/endogenous substancesi. Laboratory interaction: Kinetic alkaline picrate method
(a) Noncreatinine chromogens: In blood but not in urine(b) Cephalosporins (esp. cefoxitin): Chromogenic causing false elevations that are much greater
in urine than blood(c) Acetoacetate (increased in fasting individuals, patients with diabetic ketoacidosis):
Chromogenic causing false elevationsii. Pharmacokinetic interaction: Drugs compete with creatinine for renal secretion (causing false
elevations),trimethoprim,cimetidine,fibricacidderivatives(otherthangemfibrozil),anddronedarone.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-110
B. Drug Dosing in Renal Disease1. Loading dose
a. In general, no alteration is required, but it should be given to hasten achievement of therapeutic drug concentrations.
b. Alterations in loading dose must occur if the Vd is altered secondary to renal dysfunction. Example: Digoxin
2. Maintenance dose—Alterations should be made in either the dose or the dosing interval.a. Changing the dosing interval:
i. Use when the goal is to achieve similar steady-state concentrations.ii. Less costlyiii. Ideal for limited-dosage forms (i.e., oral medications)
b. Changing the dose:i. Use when the goal is to maintain a steady therapeutic concentration.ii. More costly
c. Changing the dose and the dosing interval:i. Often required for substantial dosage adjustment with limited-dosage formsii. Often required for narrow therapeutic index drugs with target concentrations
(a) If a drug is given more than once daily, then adjust the interval.(b) If a drug is given once daily or less often, then adjust the dose.
Patient Case11. S.J. is a 55-year-old man with hepatic dysfunction and fungemia caused by Candida krusei. He has a small
amount of ascites but is not encephalopathic. He is initiated on caspofungin, and the package insert states thatdosesshouldbedecreasedinpatientswithaChild-Pughscoreof7–9.Ifhehasthefollowinghepaticlaboratory values, which one of the following best estimates his Child-Pugh score?
Aspartatetransaminase=85U/L,alaninetransaminase=56U/L,alkalinephosphatase=190U/L,totalbilirubin=1.8mg/dL,Alb=2.9g/dL, lacticdehydrogenase=270U/L,prothrombin time/internationalnormalizedratio=14.6/1.7,γ-glutamyltransferase=60U/LA. 3.B. 5.C. 8.D. 11.
IX. PhArmACOkInetICS In hePAtIC DISeASe
A. Dosage Adjustment in Hepatic Disease1. Clinical response is the most important factor in adjusting doses in hepatic disease.2. Low hepatic extraction ratio drugs
a. Adjustment of maintenance dose is necessary only when hepatic disease alters Clint.b. Alterations in protein binding alone do not require alteration of maintenance dose, even though
total drug concentrations decline.c. Loading doses may require reduction.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-111
3. High hepatic extraction ratio drugsa. Intravenous administration
i. Usually necessary to decrease maintenance dose rateii. Consider effect of hepatic disease on protein binding.
b. Oral administration: Usually necessary to decrease maintenance dose rate
B. Rules for Dosing in Hepatic Disease1. Hepatic elimination of high extraction ratio drugs is more consistently affected by liver disease than
low extraction ratio drugs.2. The clearance of drugs that are exclusively conjugated is not substantially altered in liver disease.
table 8.Child-PughClassificationforLiverDisease
Points1 2 3
EncephalopathyAscitesBilirubin (mg/dL)Alb (g/dL)Prothrombin time (seconds over control)
00
< 1.5> 3.50–4
1 or 2+
1.5–2.32.8–3.54–6
3 or 4++
> 2.3< 2.8> 6
Pughscore:5=normal;6or7=mild(A);8or9=moderate(B);>9=severe(C).Alb = albumin.
X. PhArmACODYnAmICS
Patient Case12. Whichoneofthefollowingisthemostlikelyreasonthatadrugwillfollowclockwisehysteresis?
A. Formation of an active metabolite.B. Delay in equilibrium between the blood and the site of action.C. Tolerance.D. Increased sensitivity with time.
A. Definition:RelationshipBetweenDrugConcentrationsandthePharmacologicResponse
B. Hill Equation
E = Emax*Cγ
EC50γ+Cγ
E = pharmacologic responseEmax = maximum drug effectEC50 = concentration producing half of the maximum drug effectγ=shapefactorthataccommodatestheshapeofthecurve
Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-112
Concentration-response Plot
0
20
40
60
80
100
0 1 2 3 4
Concentration/ED50
Perc
ent o
f Max
imal
Res
pons
e
0.5125
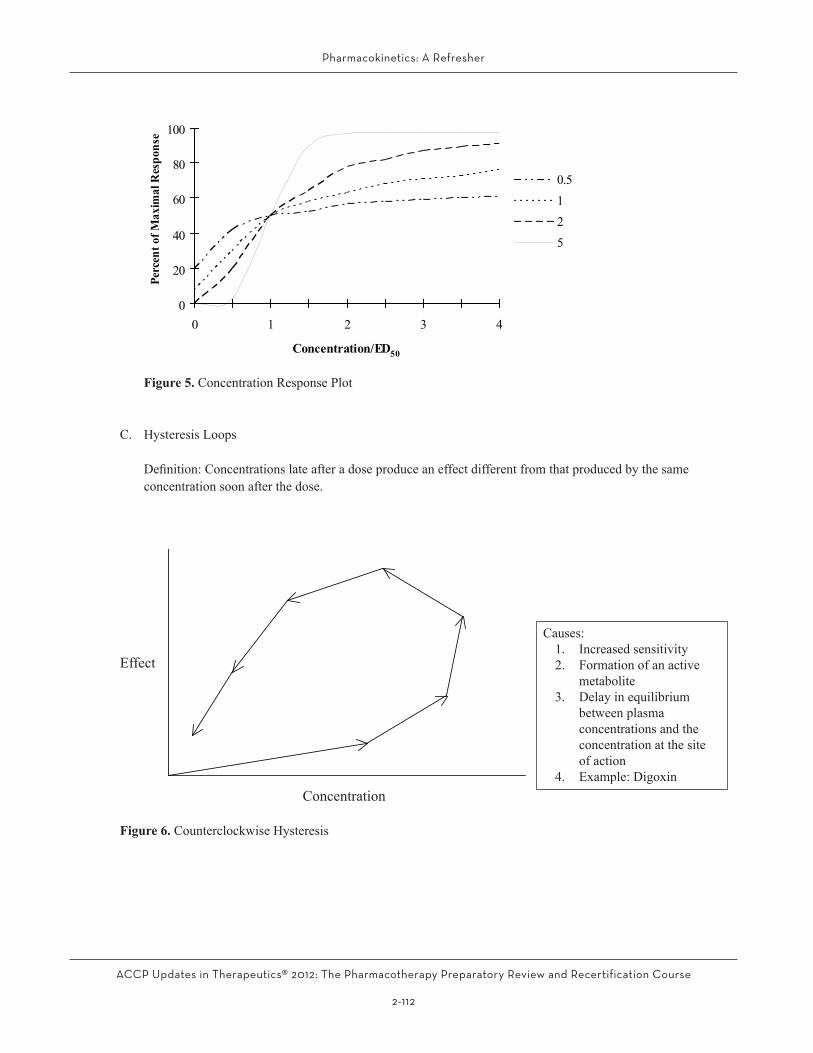
Figure 5. Concentration Response Plot
C. Hysteresis Loops
Definition:Concentrationslateafteradoseproduceaneffectdifferentfromthatproducedbythesameconcentration soon after the dose.
Causes:1. Increased sensitivity2. Formation of an active
metabolite3. Delay in equilibrium
between plasma concentrations and the concentration at the site of action
4. Example: DigoxinConcentration
Effect
Figure 6. Counterclockwise Hysteresis

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-113
Effect
Causes:1. Tolerance2. Formation of an inhibitory
metabolite3. Equilibrium reached faster
between arterial blood and site of action vs. venous blood and site of action
4. Examples: Pseudoephedrine, cocaine
ConcentrationFigure 7. Clockwise Hysteresis

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-114
Patient Cases13. P.L.,a45-year-oldmanwithchronicrenalfailure,isreceivingphenytoin400mg/dayforahistoryoftonic-
clonic seizures. His phenytoin concentration today is 13.6 mg/L, and his Alb concentration is 4.2 g/dL. Based on his current concentration, which one of the following choices should be recommended with his dose?A. Make no changes to his drug regimen.B. Keepthetotaldailydosethesame,butchangetheregimento200mg2times/day.C. Increase the dose for better seizure control.D. Decrease the dose to prevent toxicity.
14. N.R.isa63-year-oldmanwithrenalinsufficiencywhocomestotheemergencydepartmentinatrialfibril-lationwithaventricularrateof120beats/minute.Becauseofhishistoryofventriculardysfunction,itisdecidedtoinitiatehimondigoxinforratecontrol.Whichoneofthefollowingiscorrectregardingdosingin this patient?A. The loading dose should remain the same, but the maintenance dose needs to be decreased.B. The loading dose needs to be decreased, and the maintenance dose should remain the same.C. Neither the loading dose nor the maintenance dose needs to be adjusted.D. Both the loading dose and the maintenance dose need to be decreased.
15. P.P. is a 34-year-old man with a history of cerebral palsy and chronic urinary tract infections. He is admitted to the hospital with a Pseudomonas urinary tract infection that is resistant to all antibiotics but aminogly-cosides.Heisinitiatedononce-dailytobramycinat400mg/dayintravenously.Whichoneofthefollowingstatements best describes this high-dose, extended-interval aminoglycoside regimen?A. It takes advantage of the concentration-dependent killing of aminoglycoside.B. Itismoreefficaciousthanstandardaminoglycosidedosing.C. It does not require monitoring of aminoglycoside concentrations.D. It will not cause nephrotoxicity.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-115
table 9. SpecificDrugsDrug therapeutic range Sampling Issues CommentsAminoglycosides Cpmax=4–10mg/L
Amikacin=20-30mg/LCpmin < 2 mg/LAmikacin<10mg/L
Duration of infusion, timingoffirstsample post-infusion (generally should be 0.5-1 hour)
Be familiar with Sawchuk-Zaske method and high-dose, extended-interval dosing
Vancomycin Cpmin=10-15 mg/L (15–20mg/Lforcertaininfections including pneumonia, meningitis, and osteomyelitis
Controversial whether to obtain peaks or concentrations altogether
Be familiar with changes in trough concentration recommendations
Phenytoin 10-20mg/LFree: 1-2 mg/L
In general, obtain trough concentrations
Percent free increases with renal failure and hypoalbuminemia–equationstocorrect:
Change in albumin:
Cp = Cp′
(0.9*Alb4.4
)+0.1
Renal failure:
Cp = Cp′0.5
Renal failure with change in albumin:
Cp = Cp′
(0.48*0.9*Alb4.4
)+0.1
Induces liver enzymes; susceptible to metabolic drug interactions
Carbamazepine 4-12 mg/L Autoinduction;activemetabolite10,11epoxide
Phenobarbital 15-40mg/L Enzyme inducerValproic acid 50–100mg/L Saturable protein binding; percent
free increases with renal failure and hypoalbuminemia
Digoxin 0.8-2.0mcg/L Prolonged distribution period necessitates sampling > 6-12 hours postdose
Vd decreases in renal disease; susceptible to drug interactions
Cyclosporine 100-250mcg/L Wholebloodsamples Many drug interactionsLithium 0.3-1.3 mmol/L Prolonged distribution
necessitates sampling 12 hours postdose
Theophylline 10-20mg/L Treat as continuous infusion with sustained-release dosage forms
Cp = concentration of drug in plasma.
Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-116
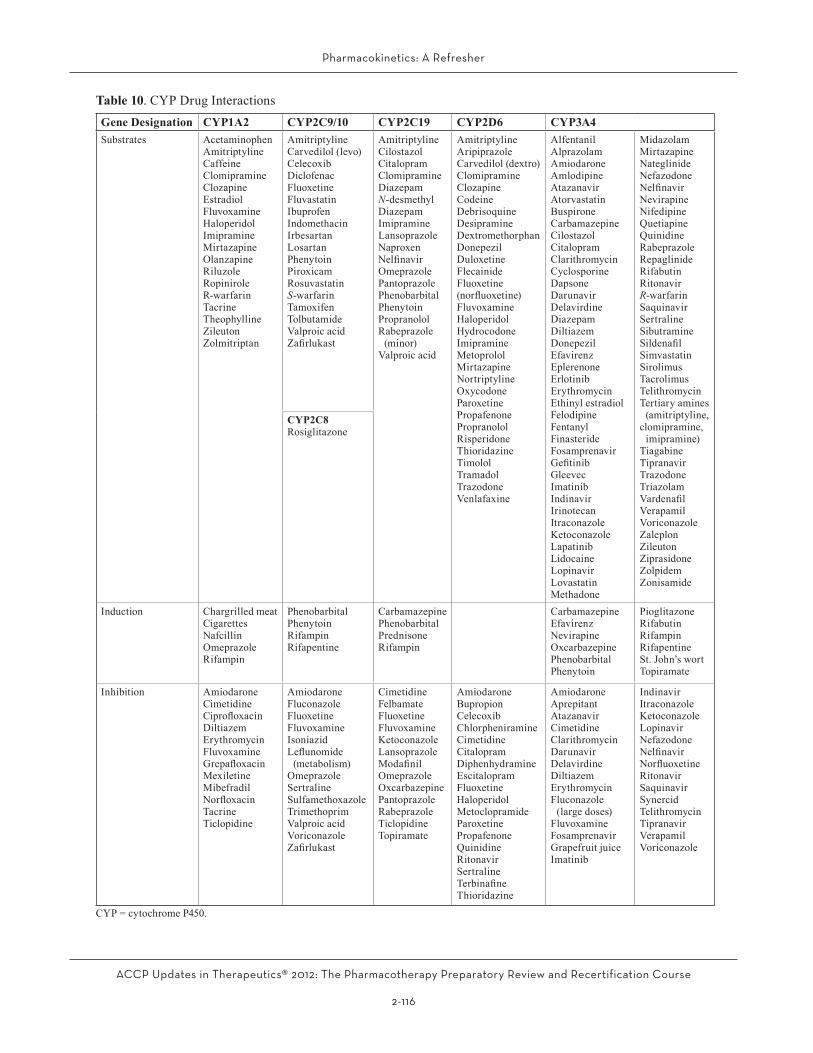
table 10. CYP Drug InteractionsGene Designation CYP1A2 CYP2C9/10 CYP2C19 CYP2D6 CYP3A4Substrates Acetaminophen
AmitriptylineCaffeineClomipramineClozapineEstradiolFluvoxamineHaloperidolImipramineMirtazapineOlanzapineRiluzoleRopiniroleR-warfarinTacrineTheophyllineZileutonZolmitriptan
AmitriptylineCarvedilol (levo)CelecoxibDiclofenacFluoxetineFluvastatinIbuprofenIndomethacinIrbesartanLosartanPhenytoinPiroxicamRosuvastatinS-warfarinTamoxifenTolbutamideValproic acidZafirlukast
AmitriptylineCilostazolCitalopramClomipramineDiazepamN-desmethylDiazepamImipramineLansoprazoleNaproxenNelfinavirOmeprazolePantoprazolePhenobarbitalPhenytoinPropranololRabeprazole
(minor)Valproic acid
AmitriptylineAripiprazoleCarvedilol (dextro)ClomipramineClozapineCodeineDebrisoquineDesipramineDextromethorphanDonepezilDuloxetineFlecainideFluoxetine(norfluoxetine)FluvoxamineHaloperidolHydrocodoneImipramineMetoprololMirtazapineNortriptylineOxycodoneParoxetinePropafenonePropranololRisperidoneThioridazineTimololTramadolTrazodoneVenlafaxine
AlfentanilAlprazolamAmiodaroneAmlodipineAtazanavirAtorvastatinBuspironeCarbamazepineCilostazolCitalopramClarithromycinCyclosporineDapsoneDarunavirDelavirdineDiazepamDiltiazemDonepezilEfavirenzEplerenoneErlotinibErythromycinEthinyl estradiolFelodipineFentanylFinasterideFosamprenavirGefitinibGleevecImatinibIndinavirIrinotecanItraconazoleKetoconazoleLapatinibLidocaineLopinavirLovastatinMethadone
MidazolamMirtazapineNateglinideNefazodoneNelfinavirNevirapineNifedipineQuetiapineQuinidineRabeprazoleRepaglinideRifabutinRitonavirR-warfarinSaquinavirSertralineSibutramineSildenafilSimvastatinSirolimusTacrolimusTelithromycinTertiary amines
(amitriptyline,clomipramine,
imipramine)TiagabineTipranavirTrazodoneTriazolamVardenafilVerapamilVoriconazoleZaleplonZileutonZiprasidoneZolpidemZonisamide
CYP2C8Rosiglitazone
Induction Chargrilled meatCigarettesNafcillinOmeprazoleRifampin
PhenobarbitalPhenytoinRifampinRifapentine
CarbamazepinePhenobarbitalPrednisoneRifampin
CarbamazepineEfavirenzNevirapineOxcarbazepinePhenobarbitalPhenytoin
PioglitazoneRifabutinRifampinRifapentineSt. John’s wortTopiramate
Inhibition AmiodaroneCimetidineCiprofloxacinDiltiazemErythromycinFluvoxamineGrepafloxacinMexiletineMibefradilNorfloxacinTacrineTiclopidine
AmiodaroneFluconazoleFluoxetineFluvoxamineIsoniazidLeflunomide
(metabolism)OmeprazoleSertralineSulfamethoxazoleTrimethoprimValproic acidVoriconazoleZafirlukast
CimetidineFelbamateFluoxetineFluvoxamineKetoconazoleLansoprazoleModafinilOmeprazoleOxcarbazepinePantoprazoleRabeprazoleTiclopidineTopiramate
AmiodaroneBupropionCelecoxibChlorpheniramineCimetidineCitalopramDiphenhydramineEscitalopramFluoxetineHaloperidolMetoclopramideParoxetinePropafenoneQuinidineRitonavirSertralineTerbinafineThioridazine
AmiodaroneAprepitantAtazanavirCimetidineClarithromycinDarunavirDelavirdineDiltiazemErythromycinFluconazole
(large doses)FluvoxamineFosamprenavirGrapefruit juiceImatinib
IndinavirItraconazoleKetoconazoleLopinavirNefazodoneNelfinavirNorfluoxetineRitonavirSaquinavirSynercidTelithromycinTipranavirVerapamilVoriconazole
CYP=cytochromeP450.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-117
table 11. PK Termsterm DefinitionAUC Area under the curveAUCEV Area under the curve following an extravascular doseAUCIV Area under the curve following an intravenous doseCmax Maximum concentrationCmin Minimum concentrationCp0 Concentration at time zeroCss Concentration at stead stateCss avg Average concentration at steady stateCss max Maximum concentration at steady stateDoseEV Dose given extravascularlyDoseIV Dose given intravenouslyF Bioavailabilityk Elimination rate constantR0 Rate of infusionτ Dosing intervalt’ Time of the infusionti Time from initiation of the infusionVd Volume of distribution

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-118
reFerenCeS
1. Burton ME, Shaw LM, Schentag JJ, eds. Applied Pharmacokinetics & Pharmacodynamics: Prin-ciples of Therapeutic Drug Monitoring, 4th ed. Baltimore,MD: LippincottWilliams&Wilkins,2006.
2. Bauer LA. Clinical pharmacokinetics and pharma-codynamics. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: A Pathophysiologic Ap-proach, 4th ed. Stamford, CT: Appleton & Lange, 1999:21–43.
3. WinterME.BasicClinicalPharmacokinetics,3rded.Vancouver:AppliedTherapeutics,1994.
4. Bauer LA. Applied Clinical Pharmacokinetics. NewYork:McGraw-HillMedical,2001.
5. Matheny CJ, LambMW,BrouwerKLR, PollackGM. Pharmacokinetic and pharmacodynamic im-plications of P-glycoprotein modulation. Pharma-cotherapy2001;21:778–96.
6. NymanHA,DowlingTC,HudsonJQ,PeterWL,Joy MS, Nolin TD. Comparative evaluation of the Cockcroft-GaultequationandtheModificationofDiet in Renal Disease (MDRD) study equation for drug dosing: an opinion of the Nephrology Practice and Research Network of the American College of Clinical Pharmacy. Pharmacotherapy 2011;31:1130–44.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-119
AnSWerS AnD eXPLAnAtIOnS tO PAtIent CASeS
1. Answer: CIn 6 days (2 t1/2), the concentration will decrease from 35.9mg/Ltoabout9mg/L;nowisthetimetore-dose.A 1-g dose given on March 24 will increase the con-centration in theblood from12.1mg/L to35.9mg/L(12.1 + 23.8 mg/L). Given that the t1/2 is about 3 days, it will take longer than 1 day to reach a concentration ofabout10mg/L. In3days (1 t1/2), the concentration willdecreasefrom35.9mg/Ltoabout18mg/L—stilltooearlytore-dose.Re-dosingcanbefiguredbecauseplenty of information exists about how to calculate when to re-dose.
2. Answer: AF=(100mg*25mg/L/hour)/(200mg*50mg/L/hour).
3. Answer: CTheeliminationrateconstantequals(ln6.5mg/L−ln5.4mg/L)/12 hours = 0.015 hour-1. The concentration at the end of the infusion equals 6.5 mg/L/e-(0.015*5) = 7 mg/L. The patient’s Vd = dose/change in concentration or160mg/7mg/L=22.9L.Ifyoudesireachangeinconcentrationfrom1mg/Lto9mg/L(or8mg/L),thendose=22.9L*8mg/L=183.2mg.Therefore,adoseof180mgisappropriate.
4. Answer: DP-glycoprotein is an efflux pump that pumps drugsback into the gastrointestinal lumen. P-glycoprotein is not a plasma protein, and it does not transfer drugs through the gastrointestinal mucosa; rather, it pumps drugs back into the gastrointestinal lumen. In addition, P-glycoprotein acts in concert with CYP3A4 to dimin-ish oral absorption.
5. Answer: CAzithromycin does not inhibit CYP3A4. Erythromycin and clarithromycin are potent inhibitors of CYP3A4 and would be expected to increase cyclosporine con-centrations.CytochromeP450inhibitionisnotadrugclass effect.
6. Answer: BBy definition, clearance becomes nonlinear once theconcentration exceeds the Km; therefore, the concen-trations will more than double. Phenytoin is not a sig-
nificant autoinducer. Although phenytoin absorptiondecreases as the dose is increased, it is not clinically significantuntilasingledoseexceeds400mg.
7. Answer: CThe correct answer, because of redistribution, is to wait a few hours to obtain the concentration because it will increase significantlywithin the first few hours afterhemodialysis.Waitingafull24hoursisnotnecessary.
8. Answer: DThe correct answer is that the assay will be able to dis-tinguish the drug from like products but will not be able todetectextremelylowconcentrations.Highspecific-ity means the assay can distinguish the drug from like products, and low sensitivity means the assay cannot detect extremely low concentrations.
9. Answer: CThecorrectanswerisabout60mL/minute/1.73m2. This valueiscalculatedusingeithertheModificationofDietin Renal Disease (study), CKD-Epi (Chronic Kidney Disease Epidemiology Collaboration [formula]), or Cockcroft and Gault equation corrected to 1.73 m2. The value is much smaller if you use the uncorrected C&G equation because the calculation is in milliliters per minute, not milliliters per minute per 1.73 m2.
10. Answer: BBoth trimethoprim/sulfamethoxazole and cimetidine compete with creatinine for secretion in the kidneys, increasing SCr concentrations. Although angiotensin-converting enzyme inhibitors may transiently increase SCr concentrations, digoxin does not affect renal func-tion. Although furosemide may secondarily affect SCr concentrations, calcium does not affect renal function. Acetaminophen and carvedilol generally will not affect SCr concentrations.
11. Answer: CS.J. has 1 point for not being encephalopathic, 2 points for mild ascites, 2 points for the bilirubin concentration, 2 points for the Alb concentration, and 1 point for the prothrombin time value, for a total of 8 points. Normal patients have a Child-Pugh score of 5, which means no hepatic dysfunction.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-120
12. Answer: CTolerance leads to a decrease in effect with time; this is clockwise hysteresis. The formation of an active me-tabolite, a delay in equilibrium between the blood and site of action, and the increased sensitivity with time would lead to an increase in effect with time; this is counterclockwise hysteresis.
13. Answer: DThe dose should be decreased to prevent toxicity. In renal failure, acidic by-products build up in the blood and compete with phenytoin for protein binding. Total concentrations need to be corrected, and this correction leads to a doubling of the concentration. Therefore, the current concentration is too high, and the dose should bedecreased.Singledosesof400mgarefine (doseshigherthan400mgshouldbedivided).
14. Answer: DBoth the loading dose and the maintenance dose need to be decreased. In general, loading doses do not need to be altered in renal dysfunction because they are pri-marily dependent on the Vd. However, the digoxin Vd
is decreased in renal dysfunction. Because digoxin is eliminated renally, the maintenance dose needs to be decreased.
15. Answer: AAminoglycosides show concentration-dependent kill-ing, and a high-dose, extended-interval aminoglycoside dose takes advantage of this characteristic. However, it hasnotproved tobemoreefficacious than traditionaldosing. Aminoglycoside concentrations still need to be monitored with high-dose, extended-interval therapy. In addition, high-dose, extended-interval aminoglycoside dosing can still cause nephrotoxicity (although the inci-dence is generally diminished).

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-121
AnSWerS AnD eXPLAnAtIOnS tO SeLF-ASSeSSment QueStIOnS
1. Answer: BWithtwoconcentrations,thereareenoughdatatocal-culate an elimination rate constant and, therefore, a t1/2. In addition, the Vd can be calculated by back extrapola-tion to the Cmax and use of appropriate equations (be-causethiswasthefirstdose,andtherefore,itisknownthat the tobramycinconcentrationwas0mg/Lbeforethe dose was given).
2. Answer: AThe t1/2 is about 2 hours. The Cmax is about 5 mg/L, and the Vdisabout20L.
3. Answer: BHer clearance increased because of the improvement in renal function, which increased her elimination rate constant and decreased her t1/2. The Vd would not be al-tered by changes in clearance (they are independent). With thediuresisandangiotensin-convertingenzymeinhibitor, her Vd probably decreased, but clearance would not be altered by changes in Vd (they are inde-pendent). In addition, if her Vd decreased, her t1/2 would decrease, not increase.
4. Answer: CBecause the trough is too low, the interval will have to be shortened to increase the concentration. Changes in dose will have the greatest effect on the peak concen-tration, and changes in interval will have the greatest effect on the trough concentration.
5. Answer: CHer dose needs to be increased, and because she is a smoker, the interval should be every 8 hours. Doubling the total daily dose will adequately increase her con-centration without causing toxic reactions.
6. Answer: DBecause of the patient’s renal failure and low Alb, the total concentration needs to be corrected. The patient’s corrected phenytoin concentration is 14.7 mcg/mL. Therefore, no changes need to be made to the dose.
7. Answer: CBoth of these are immunoassays. A brand name for the AbbottfluorescencepolarizationimmunoassayisTDx,
whichusesafluorescentlabel.ThetermEMIT stands for enzyme multiplied immunoassay technique, which is an immunoassay that uses an enzyme label.
8. Answer: DThe digoxin concentration was drawn too close to the 8:00 amdose. The digoxin had not yet had a chanceto complete its distribution phase. Once distribution is complete(generally6–12hoursafterthedose),thecon-centration will be lower and probably within the thera-peutic range. Therefore, there is no need for the digoxin antibody, activated charcoal, or lowering of the dose.
9. Answer: CThe correct statistical test is multiple logistic regres-sion. Multiple regression is used to describe the rela-tionship between a dependent variable and two or more independent variables when both the dependent and in-dependent variables are numeric. Analysis of variance is used to describe the relationship between a depen-dent variable and two or more independent variables when the dependent variable is numeric and the inde-pendent variables are nominal. Likewise, analysis of covariance is used to describe the relationship between a dependent variable and two or more independent vari-ables when the dependent variable is numeric and the independent variables are nominal with confounding factors. Spearman rank correlation is a nonparamet-ric test used to describe the relationship between one dependent and one independent variable when the data are ordinal or numeric and not normally distributed.
10. Answer: BAssessing adherence and increasing her dose, because the concentration is below the therapeutic range, is the correct answer. The valproic acid therapeutic range is50–100mg/L,andshe iswellbelow thisconcentra-tion. Although some patients are controlled at lower concentrations, this concentration is most likely too low. She definitely does not need a decrease in dose.Although total valproic acid concentrations are affected by changes in Alb, N.T.’s Alb is normal, and obtaining a free concentration is unnecessary.

Pharmacokinetics: A Refresher
ACCP Updates in Therapeutics® 2012: The Pharmacotherapy Preparatory Review and Recertification Course
2-122





























